short pr interval and narrow qrs complex associated with ... pr interval and narrow qrs complex...
TRANSCRIPT

872
Short PR Interval and Narrow QRS Complex Associated WithPheochromocytoma: Electrophysiologic Observations
JACC Vol. 3. No.3March 1984:872-5
SHOE! K. HUANG, MD, FACC,* MICHAEL J. ROSENBERG, MD, PABLO DENES, MD, FACC
Chicago, Illinois
A patient with a short (0.10 second) PR interval, narrowQRS complex and palpitation is described. Electrophysiologic studies demonstrated the presence of accelerated atrioventricular (AV) nodal conduction. Subsequently, a pheochromocytoma was found. Surgical
In 1952, Lown, Ganong and Levine (1) described a syndrome of short PR interval, normal QRS complexes andparoxysmal rapid heart action. There has been considerablecontroversy in regard to the mechanism of the short PRinterval and the types of tachyarrhythmias associated withthis syndrome. A short PR interval has been described inpatients with chronic lung disease (2), acute myocardialinfarction (3), endocrine disorders (hyperthyroidism andCushing's disease) (4), and glycogen storage disease (Pompe'sdisease) (5). Other causes of short PR interval include abbreviated atrioventricular (AV) conduction noted in childrenand young adults, ectopic impulse formation (atria, coronarysinus or AV junction) and erroneous measurement utilizingonly one or two electrocardiographic leads (6).
Electrocardiographic changes are frequent in patients withpheochromocytoma (7); these consist of left ventricular hypertrophy, T wave changes and sinus tachycardia. Occasionally, changes suggestive of acute myocardial damage,including marked and diffuse T wave changes and transientST segment elevation or depression, have been reported(8,9). The acute changes are usually transient and revert tonormal after removal of the tumor or after pharmacologicblockade (10).
In the present report, we describe a patient who had ashort PR interval and narrow QRS complexes. Electrophysiologic studies demonstrated the presence of enhancedAV nodal conduction. Subsequently, she was found to have
From the Section of Cardiology, Department of Medicine, Rush-Presbyterian-St. Luke's Medical Center, Rush Medical College, Chicago, Illinois. Manuscript received August 8,1983, accepted September 30,1983.
*Present address and address for reprints: Shoei K. Huang, MD, Section of Cardiology, Department of Medicine, University of Arizona HealthSciences Center, Tucson, Arizona 85724.
© J984 by the American College of Cardiology
removal of the tumor resulted in normalization of thePR interval. These findings suggest that the short PRinterval and the accelerated AV nodal conduction weredue to the effect of excess catecholamines on the AVconduction system.
a left adrenal pheochromocytoma. After resection of thistumor, the PR interval returned to normal.
Case ReportThe patient, a 45 year old black woman, had a history
of labile hypertension, palpitation and atypical chest pain.On February 26, 1981, she presented to the emergency roomof a local hospital with the chief complaints of severe chestpain and dizziness. Her blood pressure was 2341140 mmHg. After admission, she had a cardiopulmonary arrest fromwhich she was successfully resuscitated. A diagnosis ofacute myocardial infarction was made based on markedelevation of cardiac serum enzymes and ST-T wave changes.She was discharged on March 28. An electrocardiogramtaken on June 25 (Fig. lA) showed a sinus rate of 75/min,a short PR interval (0.10 second) and an otherwise normaltracing.
On August 23, she was admitted to our centerfor cardiaccatheterization and electrophysiologic study. The bloodpressure was 1501100 mm Hg in both the supine and sittingpositions. Cardiac examination was normal. Chest X-rayfilm showed a normal heart size. The electrocardiogramshowed a short PR interval and was unchanged from herprevious electrocardiogram. Complete blood count, urinalysis and blood chemistry determinations including thyroidfunction studies were normal. She had a maximal treadmillexercise test that did not show electrocardiographic evidenceof ischemia; there were no arrhythmias. A 24 hour Holterelectrocardiographic recording demonstrated normal sinusrhythm with occasional ventricular premature complexesand a six beat run of ventricular tachycardia at a rate of 110to 130 beats/min. Her symptoms of palpitation and chestpain did not correlate with the presence of arrhythmias. The
0735-1097/84/$3.00
JACC Vol. 3, No, 3March 1984:872-5
HUANG ET AL.SHORT PR INTERVAL AND PHEOCHROMOCYTOMA
873
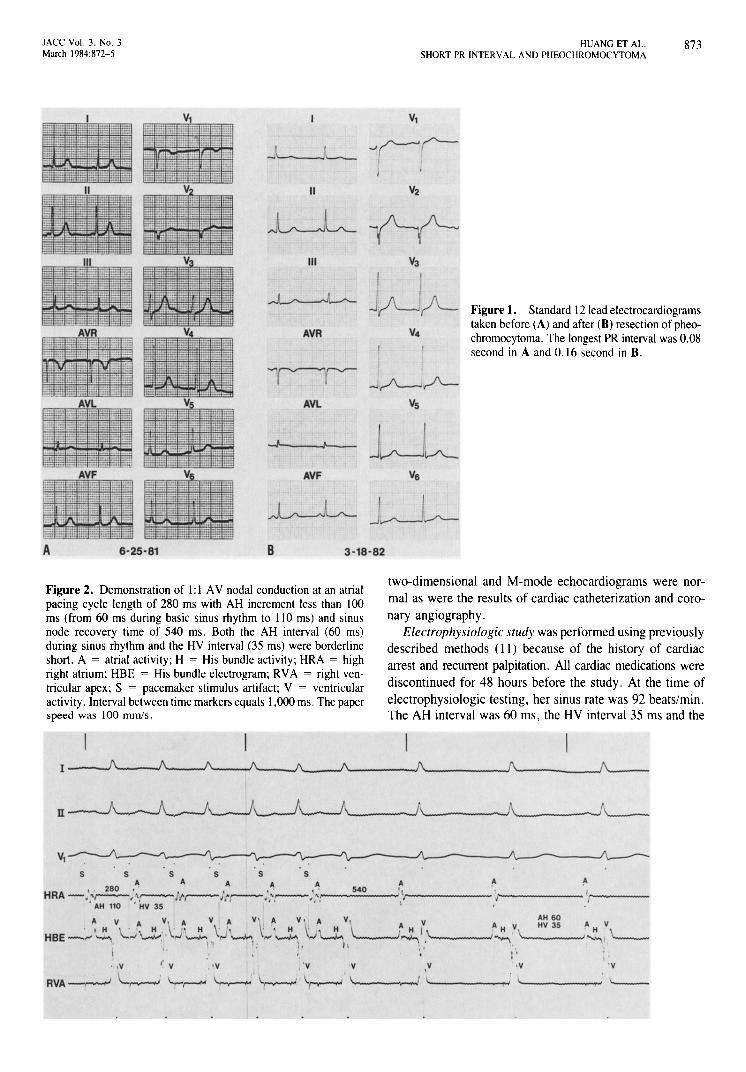
Figure 1. Standard 12 lead electrocardiogramstaken before (A) and after (B) resection of pheochromocytoma, The longest PR interval was 0,08second in A and 0.16 second in B,
Vl
3-18-82
II
III
AVF
AVR
B6-25-81A
Figure 2. Demonstration of I: I AV nodal conduction at an atrialpacing cycle length of 280 ms with AH increment less than 100ms (from 60 ms during basic sinus rhythm to 110 ms) and sinusnode recovery time of 540 ms, Both the AH interval (60 ms)during sinus rhythm and the HV interval (35 ms) were borderlineshort, A = atrial activity; H = His bundle activity; HRA = highright atrium; HBE = His bundle electrogram; RVA = right ventricular apex; S = pacemaker stimulus artifact; V = ventricularactivity, Interval between time markers equals 1,000 ms, The paperspeed was 100 mmls,
two-dimensional and M-mode echocardiograms were normal as were the results of cardiac catheterization and coronary angiography,
Electrophysiologic study was performed using previouslydescribed methods (11) because of the history of cardiacarrest and recurrent palpitation, All cardiac medications werediscontinued for 48 hours before the study, At the time ofelectrophysiologic testing, her sinus rate was 92 beats/min.The AH interval was 60 ms, the HV interval 35 ms and the
A fo fo'I .r I
J I
A yAH 60
A H V HV 35 A VI H 1\ '----., \.
H "---~. "'""". l'V .y 'y
.J li
, I.. i '---
y, 'y"y" y
I.•V
5 5 5 555A A A A A
•• 280 , . "\' 540HRA-.'r--, ,,----//'r---Jt~,,.........--,',.------...
, AH 110 . HV 35 If',I
A V A V ~ H V A V, A V A V,
HBE-.:,....·~. ',.J"~:' ~ '\~,.....l,. '-,\....!" l....__-'1" ' j. h
874 HUANG ET AL.SHORT PR INTERVAL AND PHEOCHROMOCYTOMA
JACC Vol. 3. No.3March 1984:872-5
PA interval 25 ms. Incremental atrial pacing from the highright atrium (cycle length from 600 to 300 ms) demonstrateda gradual but small increment in AH interval from 60 to110 ms (A AH = 50 ms). At an atrial pacing cycle lengthof 280 ms (rate 214 beats/min), I: I AV nodal conductionwas still present (Fig. 2). The AV nodal effective «260ms) and functional «300 ms) refractory periods at thedriven pacing cycle of 500 ms were short. Similarly, I: Iretrograde ventriculoatrial (VA) conduction was present upto a ventricular pacing rate of 200 beats/min (cycle length300 ms) with gradual prolongation of VA interval. Therewas no inducible supraventricular or ventricular tachycardiaby programmed single and double extrastimulus technique.
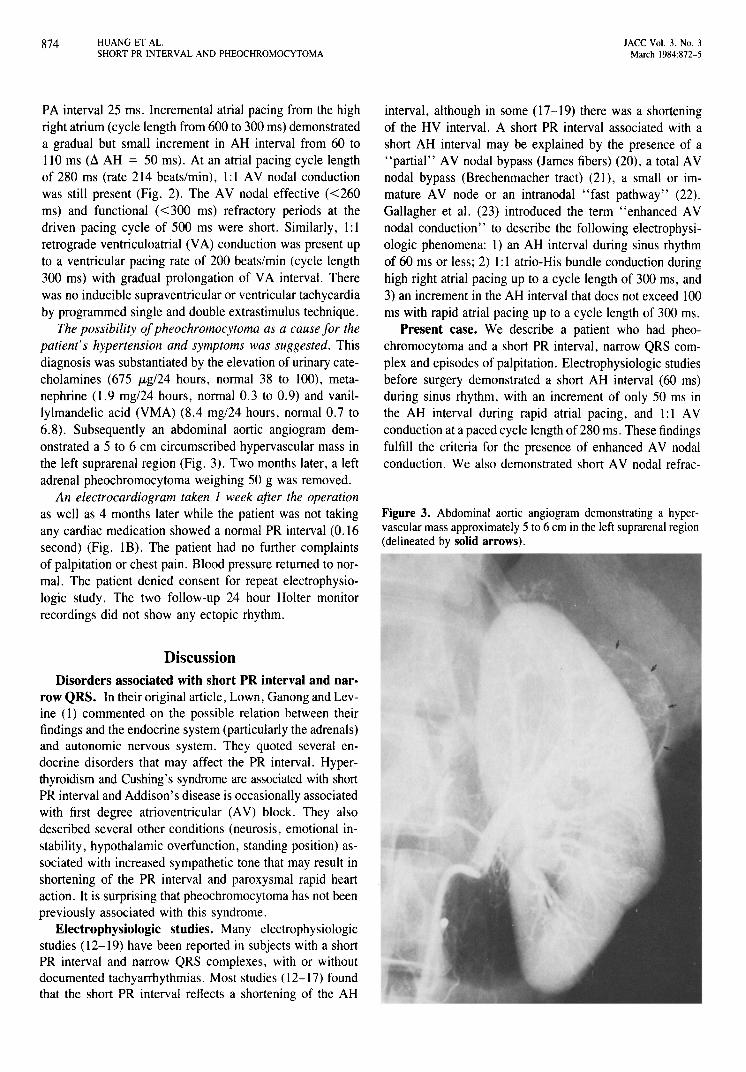
The possibility ofpheochromocytoma as a cause for thepatient's hypertension and symptoms was suggested. Thisdiagnosis was substantiated by the elevation of urinary catecholamines (675 JLg/24 hours, normal 38 to 100), metanephrine (1.9 mg124 hours, normal 0.3 to 0.9) and vanillylmandelic acid (VMA) (8.4 mg124 hours, normal 0.7 to6.8). Subsequently an abdominal aortic angiogram demonstrated a 5 to 6 cm circumscribed hypervascular mass inthe left suprarenal region (Fig. 3). Two months later, a leftadrenal pheochromocytoma weighing 50 g was removed.
An electrocardiogram taken I week after the operationas well as 4 months later while the patient was not takingany cardiac medication showed a normal PR interval (0.16second) (Fig. IB). The patient had no further complaintsof palpitation or chest pain. Blood pressure returned to normal. The patient denied consent for repeat electrophysiologic study. The two follow-up 24 hour Holter monitorrecordings did not show any ectopic rhythm.
DiscussionDisorders associated with short PR interval and nar·
row QRS. In their original article, Lown, Ganong and Levine (1) commented on the possible relation between theirfindings and the endocrine system (particularly the adrenals)and autonomic nervous system. They quoted several endocrine disorders that may affect the PR interval. Hyperthyroidism and Cushing's syndrome are associated with shortPR interval and Addison's disease is occasionally associatedwith first degree atrioventricular (AV) block. They alsodescribed several other conditions (neurosis, emotional instability, hypothalamic overfunction, standing position) associated with increased sympathetic tone that may result inshortening of the PR interval and paroxysmal rapid heartaction. It is surprising that pheochromocytoma has not beenpreviously associated with this syndrome.
Electrophysiologic studies. Many electrophysiologicstudies (12-19) have been reported in subjects with a shortPR interval and narrow QRS complexes, with or withoutdocumented tachyarrhythmias. Most studies (12-17) foundthat the short PR interval reflects a shortening of the AH
interval, although in some (17-19) there was a shorteningof the HV interval. A short PR interval associated with ashort AH interval may be explained by the presence of a"partial" AV nodal bypass (James fibers) (20), a total AVnodal bypass (Brechenmacher tract) (21), a small or immature AV node or an intranodal "fast pathway" (22).Gallagher et al. (23) introduced the term "enhanced AVnodal conduction" to describe the following electrophysiologic phenomena: I) an AH interval during sinus rhythmof 60 ms or less; 2) I: I atrio-His bundle conduction duringhigh right atrial pacing up to a cycle length of 300 ms, and3) an increment in the AH interval that does not exceed 100ms with rapid atrial pacing up to a cycle length of 300 ms.
Present case. We describe a patient who had pheochromocytoma and a short PR interval, narrow QRS complex and episodes of palpitation. Electrophysiologic studiesbefore surgery demonstrated a short AH interval (60 ms)during sinus rhythm, with an increment of only 50 ms inthe AH interval during rapid atrial pacing, and I: I AVconduction at a paced cycle length of 280 ms. These findingsfulfill the criteria for the presence of enhanced AV nodalconduction. We also demonstrated short AV nodal refrac-
Figure 3. Abdominal aortic angiogram demonstrating a hypervascular mass approximately 5 to 6 em in the left suprarenal region(delineated by solid arrows).

JACC Vol. 3, No.3March 1984:872-5
HUANG ET AL.SHORT PR INTERVAL AND PHEOCHROMOCYTOMA
875
tory periods. There was excellent retrograde ventriculoatrial(VA) conduction through the AV node (I: I VA conductionat a ventricular pacing rate of 200/min). After resection ofthe tumor, the PR interval returned to normal and the symptoms subsided. These observations confirm the role of catecholamines, particularly epinephrine and norepinephrine, inthe genesis of short PR interval and enhanced AV nodalconduction.
The short PR interval in our patient was not dependenton the presence of sinus tachycardia, but was recorded during normal sinus rates. We hypothesize that chronic sympathetic hyperstimulation resulted in a short PR intervalsecondary to enhanced AV nodal conduction. This accelerated AV nodal conduction was not accompanied by aconcomitant chronic increase in sinus nodal discharge rate,suggesting a differential adaptation process between the sinusand AV nodes to chronic catecholamine excess. Resectionof the pheochromocytoma resulted in normalization of AVconduction time.
We deeply appreciate the secretarial assistance of Cheryl Bahrychuk.
ReferencesI. Lown B, Ganong W, Levine S. The syndrome of short P-R interval,
normal QRS complex and paroxysmal rapid heart action. Circulation1952;5:693-706.
2. Katz LN, Pick A. Clinical Electrocardiography. Part I. The Arrhythmias. Philadelphia: Lea & Febiger, 1956:102.
3. Mathew G, Raftery EB. Accelerated atrioventricular conduction aftermyocardial infarction. A study using His bundle electrograms. BrHeart J 1973;35:985-90.
4. Lown B, Arons WL, Ganong WF, et al. Adrenal steroids and auriculoventricular conduction. Am Heart J 1955;50:760-9.
5. Ehlers KH, Hagstrom JW, Lukes OS, Redo SF, Engle MA. Glycogenstorage disease of the myocardium with obstruction of left ventricularoutflow. Circulation 1962;25:96-109.
6. Castellanos A, Zaman L, Moleiro F. Aranda J, Myerburg R. TheLown-Ganong-Levine syndrome. PACE 1982;5:715-40.
7. Surawicz B, Mangiard ML. Electrocardiogram in endocrine and metabolic disorders. In: Rios JC, ed. Clinical Electrocardiographic Correlations. Philadelphia: FA Davis, 1977:254.
8. Van Vliet PO, Burchell HB, Titus JL. Focal myocarditis associatedwith pheochromocytoma. N Engl J Med 1966;274: 1102-8.
9. Manger WM, Gifford RW. Pheochromocytoma. New York: SpringerVerlag, 1977:184-92.
10. Cheng RO, Bashour TT. Striking electrocardiographic changes associated with pheochromocytoma masquerading as ischemic heart disease. Chest 1976;70:397-9.
II. Dhingra RC, Rosen KM, Rahimtoola SH. Normal conduction intervalsand response in sixty-one patients using His bundle recording andatrial pacing. Chest 1973;64:55-9.
12. Castellanos A, Castillo CA, Agha AS, Tessler M. His bundle electrograms in patients with short P-R intervals, narrow QRS complexes,and paroxysmal tachycardias. Circulation 1971 ;43:667-78.
13. Bissett JK, Thompson AJ, DeSoyza H, Murphy Me. Atrioventricularconduction in patients with short P-R intervals and normal QRS complexes. Br Heart J 1973;35:123-7.
14. Aranda J, Castellanos A, Molerio F, Befeler B. Effects of the pacingsite on A-H conduction and refractoriness in patients with short P-Rintervals. Circulation 1976;53:33-9.
15. Caracta AR, Damato AN, Gallagher JJ, et al. Electrophysiologic studies in the syndrome of short P-R interval, normal QRS complex. AmJ Cardiol 1973;31 :245-53.
16. Benditt DG, Pritchett ELC, Smith WM, Wallace AG, Gallagher J1.Characteristics of atrioventricular conduction and the spectrum of arrhythmias in Lown-Ganong-Levine syndrome. Circulation1978;57:454-65.
17. Moro C, Cosio F. Electrophysiologic study of patients with shortP-R interval and normal QRS complex. Eur J Cardiol 1980; 11:81-90.
18. Mandel WJ, Danzig R, Hayakawa H. Lown-Ganong-Levine syndrome: a study using His bundle electrogram. Circulation1971 ;44:696-708.
19. Moleiro F, Mendoza IJ, Medina-Ravell V, et al. One-to-one A-Vconduction during atrial pacing at rate of 300/minute in absence ofWolff-Parkinson-White syndrome. A review of the literature. Am JCardiol 1981;48:789-96.
20. James TN. The connecting pathways between the sinus node and AVnode and between the right and left atrium in the human heart. AmHeart J 1963;66:498-508.
21. Brechenmacher e. Atrio-His bundle tracts. Br Heart J 1975;37:853-5.
22. Anderson RH, Becker AE. Gross anatomy and microscopy of theconducting system. In: Mandel WJ, ed. Cardiac Arrhythmias. TheirMechanisms, Diagnosis and Management. Philadelphia: Lippincott,1980:12.
23. Gallagher 11, Sealy WC, Kansell J, et al. Multiple accessory pathwaysin patients with the pre-excitation syndrome. Circulation1976;54:571-91.