severe sepsis & septic shock objectives - ucsf cme · severe sepsis & septic shock ... door...
TRANSCRIPT
1
Sepsis: the 1st 6 hoursIdentification
&Initial Management
Chris Fee, MDUCSF Division of Emergency Medicine
2007 Topics in Emergency Medicine
Severe Sepsis & Septic Shock
• Gain respect for severe sepsis/septic shock
• Utilize lactate to identify high risk patients & monitor resuscitation
• Understand & implement the 6 hour sepsis bundle
Objectives
What would you do?Case #1
• 66 yo man presents with anterior CP
What would you do?Case #2
• 19 yo woman with abdominal pain after a motor vehicle collision
HR 120, BP 80/50
After 1.5 L NS IV
HR 90, BP 126/76
What would you do?Case #3
• 66 yo woman with R weakness & aphasia
What would you do?Case #4
• 58 yo man with cough, fever, SOB
T 38.3 °C
HR 106
BP 110/62
RR 22
O2 sat 98% on 4L/min
Lactate 4.4 mmol/L
2
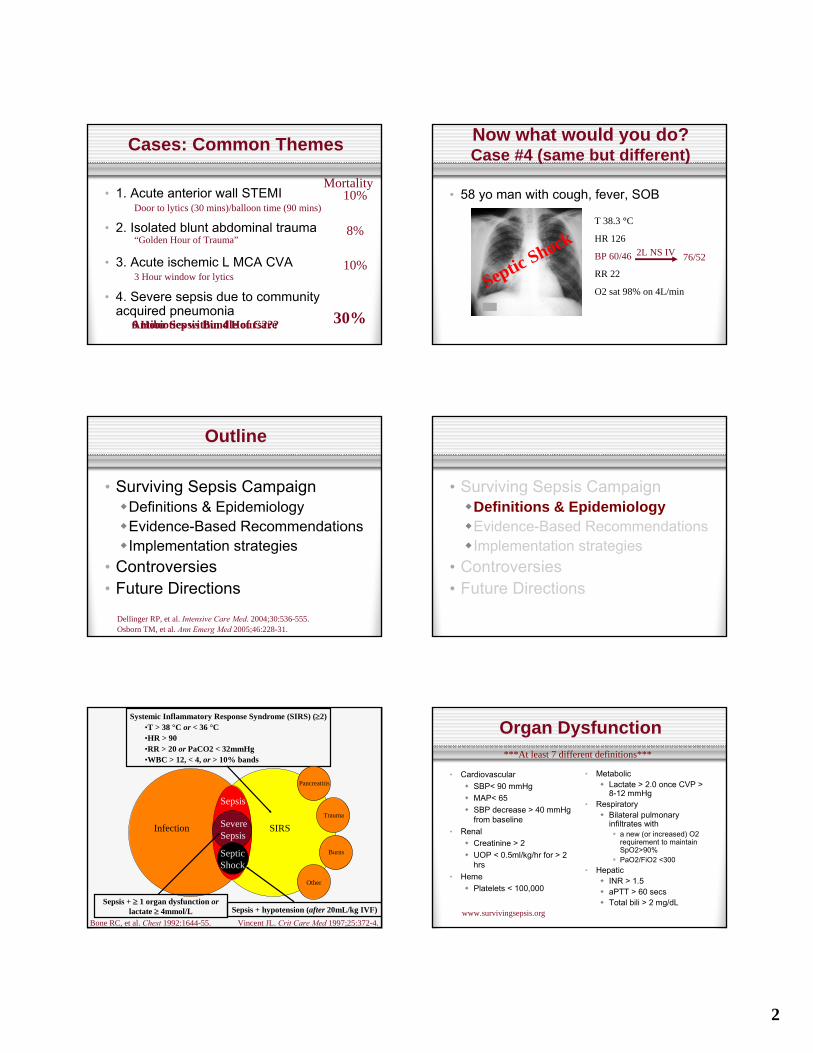
Cases: Common Themes
• 1. Acute anterior wall STEMI
• 2. Isolated blunt abdominal trauma
• 3. Acute ischemic L MCA CVA
• 4. Severe sepsis due to community acquired pneumonia
Door to lytics (30 mins)/balloon time (90 mins)
“Golden Hour of Trauma”
3 Hour window for lytics
Mortality10%
8%
10%
30%6 Hour Sepsis Bundle of CareAntibiotics within 4 Hours???
Now what would you do?Case #4 (same but different)
• 58 yo man with cough, fever, SOB
T 38.3 °C
HR 126
BP 60/46
RR 22
O2 sat 98% on 4L/min
76/522L NS IV
Septic Shock
Outline
• Surviving Sepsis CampaignDefinitions & EpidemiologyEvidence-Based RecommendationsImplementation strategies
• Controversies• Future Directions
Dellinger RP, et al. Intensive Care Med. 2004;30:536-555.Osborn TM, et al. Ann Emerg Med 2005;46:228-31.
• Surviving Sepsis CampaignDefinitions & EpidemiologyEvidence-Based RecommendationsImplementation strategies
• Controversies• Future Directions
SIRS
Systemic Inflammatory Response Syndrome (SIRS) (≥2)•T > 38 °C or < 36 °C•HR > 90•RR > 20 or PaCO2 < 32mmHg•WBC > 12, < 4, or > 10% bands
Pancreatitis
Trauma
Burns
Other
Infection
Sepsis
Severe Sepsis
Sepsis + ≥ 1 organ dysfunction orlactate ≥ 4mmol/L
Bone RC, et al. Chest 1992:1644-55. Vincent JL. Crit Care Med 1997;25:372-4.
Septic Shock
Sepsis + hypotension (after 20mL/kg IVF)
Organ Dysfunction
• CardiovascularSBP< 90 mmHgMAP< 65SBP decrease > 40 mmHg from baseline
• RenalCreatinine > 2UOP < 0.5ml/kg/hr for > 2 hrs
• HemePlatelets < 100,000
• MetabolicLactate > 2.0 once CVP > 8-12 mmHg
• RespiratoryBilateral pulmonary infiltrates with
a new (or increased) O2 requirement to maintain SpO2>90%PaO2/FiO2 <300
• HepaticINR > 1.5aPTT > 60 secsTotal bili > 2 mg/dL
***At least 7 different definitions***
www.survivingsepsis.org
3
Pathogenesis
Organism
Global Tissue Hypoxia & Organ Dysfunction
Severe Sepsis
Multiple Organ Dysfunction & Refractory Hypotension
Septic Shock
Systemic Inflammation or Inflammatory Response
Diffuse Endothelial Disruption & Microcirculation Defects
Nguyen HB, et al. Ann Emerg Med 2006;48:28-54.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Death
Pathogenesis
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Death
Organism
Global Tissue Hypoxia & Organ Dysfunction
Severe Sepsis
Multiple Organ Dysfunction & Refractory Hypotension
Septic Shock
Systemic Inflammation or Inflammatory Response
Diffuse Endothelial Disruption & Microcirculation Defects
Nguyen HB, et al. Ann Emerg Med 2006;48:28-54.
How many patients with severe sepsis/septic shock are seen in your workplace each year?
A. <5B. 6-10C. 11-15D. 16-20E. >20
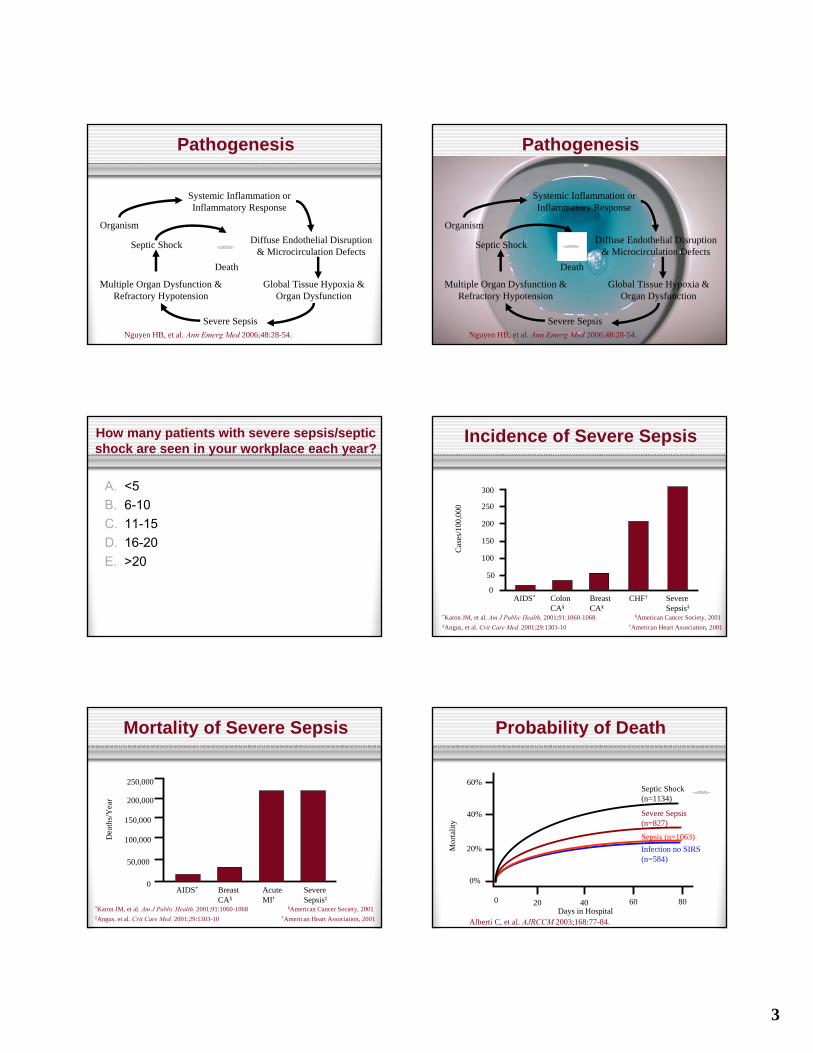
Incidence of Severe SepsisC
ases
/100
,000
300
250
200
150
100
50
0AIDS* Colon
CA§Breast CA§
CHF† Severe Sepsis‡
*Karon JM, et al. Am J Public Health. 2001;91:1060-1068 §American Cancer Society, 2001‡Angus, et al. Crit Care Med. 2001;29:1303-10 †American Heart Association, 2001
Mortality of Severe Sepsis
250,000
200,000
150,000
100,000
50,000
0
Dea
ths/
Yea
r
AIDS* Breast CA§
Acute MI†
Severe Sepsis‡
*Karon JM, et al. Am J Public Health. 2001;91:1060-1068 §American Cancer Society, 2001‡Angus, et al. Crit Care Med. 2001;29:1303-10 †American Heart Association, 2001
Probability of Death
Days in Hospital
60%
40%
20%
0%
0 20 40 60 80
Mor
talit
y
Alberti C, et al. AJRCCM 2003;168:77-84.
Infection no SIRS (n=584)
Sepsis (n=1063)
Severe Sepsis (n=827)
Septic Shock (n=1134)
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
4
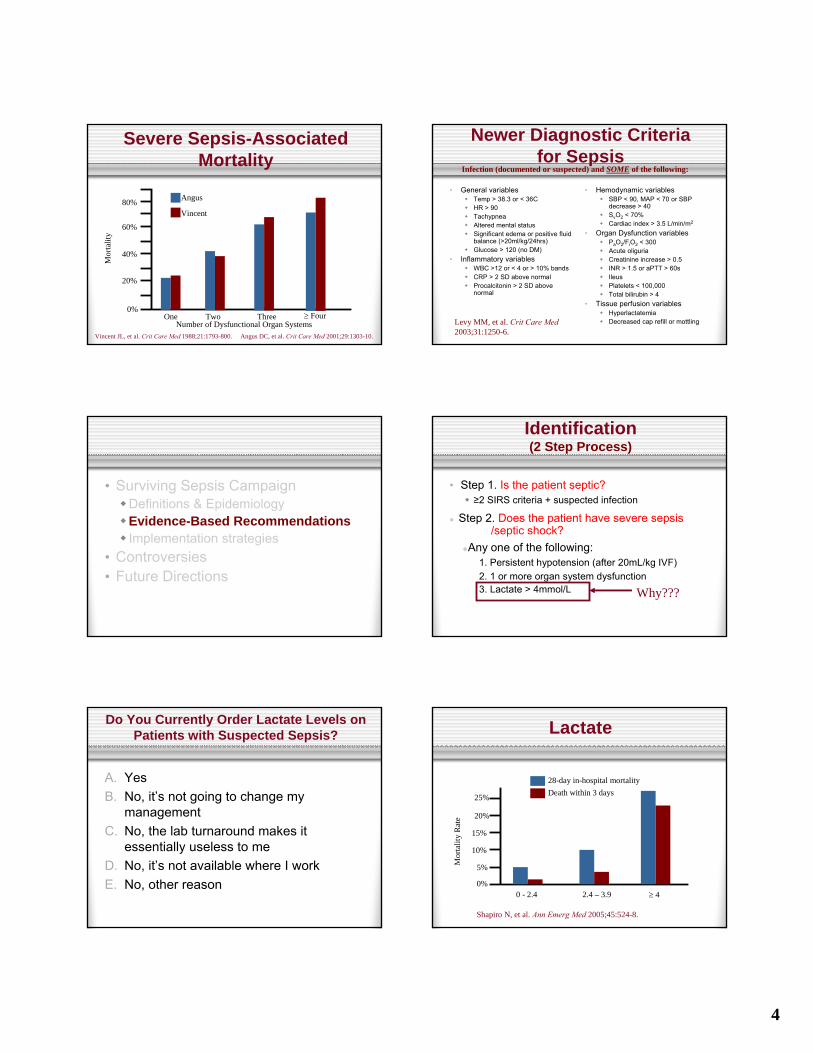
Severe Sepsis-Associated Mortality
Angus
0%
20%
40%
60%
80%
Mor
talit
y
Number of Dysfunctional Organ Systems
Vincent
One Two Three ≥ Four
Vincent JL, et al. Crit Care Med 1988;21:1793-800. Angus DC, et al. Crit Care Med 2001;29:1303-10.
Newer Diagnostic Criteriafor Sepsis
• General variablesTemp > 38.3 or < 36CHR > 90TachypneaAltered mental statusSignificant edema or positive fluid balance (>20ml/kg/24hrs)Glucose > 120 (no DM)
• Inflammatory variablesWBC >12 or < 4 or > 10% bandsCRP > 2 SD above normalProcalcitonin > 2 SD above normal
• Hemodynamic variablesSBP < 90, MAP < 70 or SBP decrease > 40SvO2 < 70%Cardiac index > 3.5 L/min/m2
• Organ Dysfunction variablesPaO2/FiO2 < 300Acute oliguriaCreatinine increase > 0.5INR > 1.5 or aPTT > 60sIleusPlatelets < 100,000Total bilirubin > 4
• Tissue perfusion variablesHyperlactatemiaDecreased cap refill or mottling
Infection (documented or suspected) and SOME of the following:
Levy MM, et al. Crit Care Med2003;31:1250-6.
• Surviving Sepsis CampaignDefinitions & EpidemiologyEvidence-Based RecommendationsImplementation strategies
• Controversies• Future Directions
Identification(2 Step Process)
• Step 1. Is the patient septic?≥2 SIRS criteria + suspected infection
Step 2. Does the patient have severe sepsis/septic shock?
Any one of the following:1. Persistent hypotension (after 20mL/kg IVF)2. 1 or more organ system dysfunction3. Lactate > 4mmol/L Why???
Do You Currently Order Lactate Levels on Patients with Suspected Sepsis?
A. YesB. No, it’s not going to change my
managementC. No, the lab turnaround makes it
essentially useless to meD. No, it’s not available where I workE. No, other reason
Lactate
Mor
talit
y R
ate
0%
5%
10%
15%
20%
25%
0 - 2.4 2.4 – 3.9 ≥ 4
Death within 3 days28-day in-hospital mortality
Shapiro N, et al. Ann Emerg Med 2005;45:524-8.
5
Lactate“Cryptic Shock”
• Tissue hypoperfusion without hypotension
• On the brink of cardiovascular collapse↓ Myocardial contractility & complianceIf not treated aggressively, leads to multiple organ failure & mortality
LactateResuscitation
• Lactate clearance inversely related to mortality (measured at 6 hrs from initiation)
• Best available marker for need of ongoing resuscitation
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Nguyen HB, et al. Crit Care Med 2004;32:1637-42.
So You Can Identify Severe Sepsis/Septic Shock, Now What?
• Step 3Source controlEarly cultures & antibioticsEarly goal-directed therapyProtective ventilation strategiesActivated protein CIntensive insulin therapyLow dose steroidsNarrowing antibiotic spectrum once sensitivities available
Grade of Recommendation
BBD
C/E?
E
ED&E
BED
ICU
Early Goal-Directed Therapy
Physical exam, vitals, urine output, CVP, mental status are
UNRELIABLE indicators of perfusion
Early Goal-Directed Therapy
• Inadequate O2 delivery = key to progressionSurrogate measure of cardiac output & oxygen extraction at the tissue level
Mixed venous (SvO2) and central venous (ScvO2) O2 saturation
• Manipulate preload, afterload, contractility Goal: balance O2 demand & delivery
Rivers E, et al. NEJM 2001;345:1368-77.
Early Goal-Directed Therapy
Sedation, paralysis (if intubated), or both
Central venous ±arterial catheterization
1. SIRS + suspected infection &
2. SBP < 90 (after 20mL/kg IVF) or lactate ≥ 4 or multiorgan
dysfunction
Supplemental O2 ±endotracheal intubation &
mechanical ventilation
Rivers E, et al. NEJM 2001;345:1368-77.

6
Early Goal-Directed Therapy
CVPColloid
<8 mm HgCrystalloid
8-12 mm Hg
Sedation, paralysis (if intubated), or both
Central venous ±arterial catheterization
1. SIRS + suspected infection &
2. SBP < 90 (after 20mL/kg IVF) or lactate ≥ 4 or multiorgan
dysfunction
Supplemental O2 ±endotracheal intubation &
mechanical ventilation
Rivers E, et al. NEJM 2001;345:1368-77.
Early Goal-Directed Therapy
MAP
CVPColloid
<8 mm HgCrystalloid
8-12 mm Hg
Sedation, paralysis (if intubated), or both
Central venous ±arterial catheterization
1. SIRS + suspected infection &
2. SBP < 90 (after 20mL/kg IVF) or lactate ≥ 4 or multiorgan
dysfunction
Supplemental O2 ±endotracheal intubation &
mechanical ventilation
Vasoactive agents<65 mm Hg>90 mm Hg
Norepinephrine pressor of choice
Rivers E, et al. NEJM 2001;345:1368-77.
>65 and <90 mm Hg
Early Goal-Directed Therapy
ScvO2Transfusion of red cells until hematocrit > 30%
<70%≥ 70%
Sedation, paralysis (if intubated), or both
CVPColloid
<8 mm HgCrystalloid
8-12 mm Hg
Central venous ±arterial catheterization
1. SIRS + suspected infection &
2. SBP < 90 (after 20mL/kg IVF) or lactate ≥ 4 or multiorgan
dysfunction
Supplemental O2 ±endotracheal intubation &
mechanical ventilation
MAP
>65 and <90 mm Hg
Vasoactive agents<65 mm Hg>90 mm Hg
Norepinephrine pressor of choice
<70%≥ 70%
Inotropic agentsDobutamine
Rivers E, et al. NEJM 2001;345:1368-77.
Early Goal-Directed Therapy
Sedation, paralysis (if intubated), or both
CVPColloid
<8 mm HgCrystalloid
8-12 mm Hg
Central venous ±arterial catheterization
1. SIRS + suspected infection &
2. SBP < 90 (after 20mL/kg IVF) or lactate ≥ 4 or multiorgan
dysfunction
Supplemental O2 ±endotracheal intubation &
mechanical ventilation
MAP
>65 and <90 mm Hg
Vasoactive agents<65 mm Hg>90 mm Hg
Norepinephrine pressor of choice
ScvO2Transfusion of red cells until hematocrit > 30%
<70%≥ 70%
<70%≥ 70%
Inotropic agentsDobutamine
Rivers E, et al. NEJM 2001;345:1368-77.
Goals achieved?
No
Hospital admission
Yes
Early Goal-Directed Therapy
Central venous ±arterial catheterization
Sedation, paralysis (if intubated), or both
CVP
MAP
ScvO2
Goals achieved?
Colloid
<8 mm HgCrystalloid
8-12 mm Hg
>65 and <90 mm HgTransfusion of red cells until hematocrit > 30%
<70%≥ 70%
No
Hospital admission
Yes
1. SIRS + suspected infection &
2. SBP < 90 (after 20mL/kg IVF) or lactate ≥ 4 or multiorgan
dysfunction
Supplemental O2 ±endotracheal intubation &
mechanical ventilation
Vasoactive agents<65 mm Hg>90 mm Hg
Norepinephrine pressor of choice
<70%≥ 70%
Inotropic agentsDobutamine
Rivers E, et al. NEJM 2001;345:1368-77.
Early Goal-Directed Therapy
• ↓ In-hospital mortality 16%46.5% controls vs 30.5% in EGDT group
Relative risk of death = 0.58
Rivers E, et al. NEJM 2001;345:1368-77.
7
Does Your ED/Practice Currently Utilize an EGDT Protocol?
A. YesB. No, lack of specialized monitoring
equipmentC. No, too many ED resources requiredD. No, need for central venous cannulationE. No, other reason(s)
• Surviving Sepsis CampaignDefinitions & EpidemiologyEvidence-Based RecommendationsImplementation strategies
• Controversies• Future Directions
Concept of the “Bundle”
• Institute for Healthcare Improvement (www.ihi.org)
Bundle: group of interventions that, when implemented together, result in better outcomes than individually
Institute for Healthcare Improvement website: as accessed on 9/2/2007.
Concept of the “Bundle”The Acute MI Model
Angiotensin-converting enzyme (ACE) inhibitors, lipid-lowering agents (statins), additional antihypertensive agents
Secondary prevention strategies
Percutaneous transluminal coronary angioplasty (PTCA), stenting, coronary artery bypass grafting (CABG)
Invasive procedures for tissue reperfusion and vessel revascularization
Angiography, intravascular ultrasound, vascular catheterization
Invasive procedures for diagnosis/monitoring
ASA, glycoprotein (GP) IIb/IIIa inhibitors, adenosine diphosphate-(ADP) receptor blockers
Antiplatelet therapies
Heparin, low-molecular-weight heparinsAnticoagulants
Streptokinase, urokinase, alteplase, retaplase, tissue plasminogen activator (tPA)
Fibrinolytics
EchocardiographyCardiac monitoring
Nitrates, analgesics (opioids), oxygen therapy, fluid resuscitation
Acute management
www.survivingsepsis.org
6 Hour (Resuscitation) BundleSteps 1-3 (ED Care)
• Prompt identificationIncludes lactate measurement
• Early cultures & appropriate antibiotics
• EGDTIncludes measurement of CVP & ScvO2
Severe sepsis (2001-2004): 2/3 present via EDAverage ED length of stay: 4.7 hours (20% spent >6 hours)
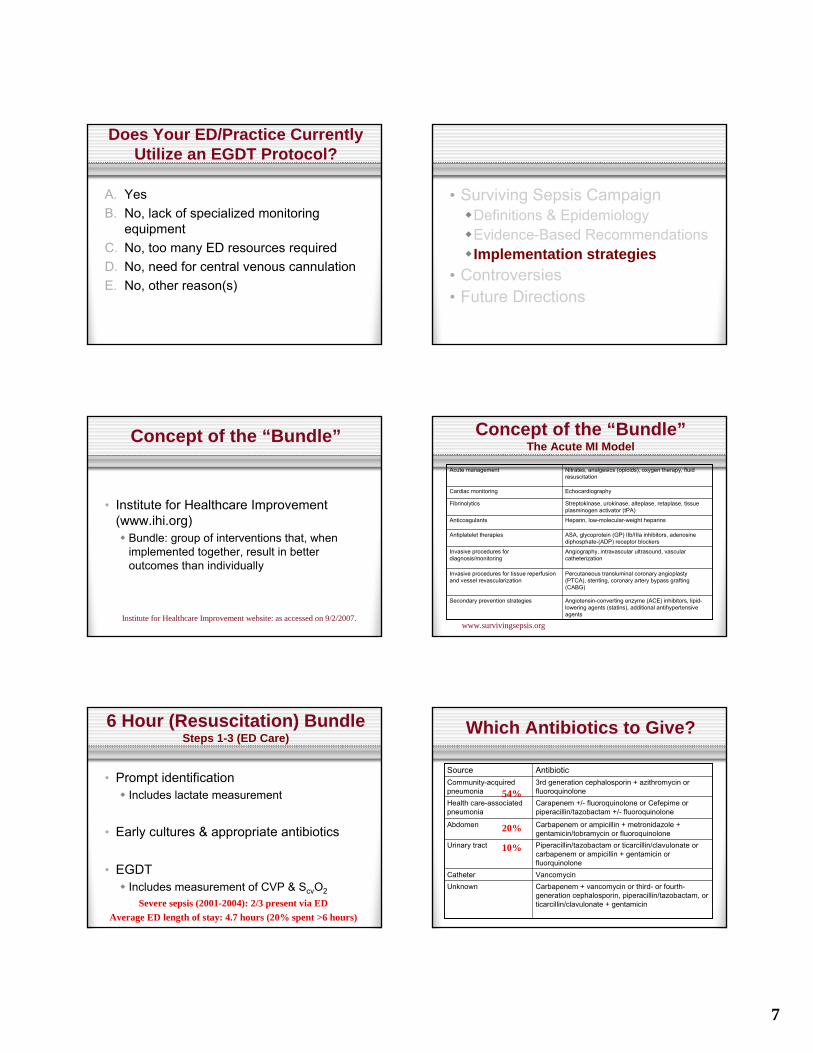
Which Antibiotics to Give?
Carbapenem + vancomycin or third- or fourth-generation cephalosporin, piperacillin/tazobactam, or ticarcillin/clavulonate + gentamicin
UnknownVancomycinCatheter
Piperacillin/tazobactam or ticarcillin/clavulonate or carbapenem or ampicillin + gentamicin or fluorquinolone
Urinary tract
Carbapenem or ampicillin + metronidazole + gentamicin/tobramycin or fluoroquinolone
Abdomen
Carapenem +/- fluoroquinolone or Cefepime or piperacillin/tazobactam +/- fluoroquinolone
Health care-associated pneumonia
3rd generation cephalosporin + azithromycin or fluoroquinolone
Community-acquired pneumonia
AntibioticSource
54%
20%
10%
8
24 Hour (Management) BundleThe 4th Step (ICU Care)…
• Source control
• Protective ventilation strategies
• Low dose steroids (???)
• Intensive insulin therapy (???)
• Activated protein C (???)
• Narrowing of antibiotic spectrum
Example Sepsis Bundles
♦ MUST (Multiple Urgent Sepsis Therapies)
♦ www.mustprotocol.com
♦ STOP (Strategies to Timely Obviate the
Progression of Sepsis in the ED)
♦ www.llu.edu//llumc/emergency/patientcare
♦ UCSF
♦ Included with syllabus
Strategies for Initiating EGDT
• ED-based
Henry Ford Hospital, MUST protocol
• Rapid response team-based
Good Samaritan Hospital (community)
• ICU-based
UCSF
If you do utilize EGDT, what model do you use?
A. ED-basedB. Rapid Response Team-basedC. ICU-basedD. Not sureE. Don’t utilize EGDT where I work
• Surviving Sepsis CampaignDefinitions & EpidemiologyEvidence-Based RecommendationsImplementation strategies
• Controversies• Future Directions
n
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

9
ControversiesLactate & “Cryptic Shock”
• Subgroup in River’s EGDT study20% (EGDT) vs 60.9% (control) mortality
• MUST Protocol Implementation37/116 in protocol had “cryptic shock”
Donnino MW. Chest 2003;90S.Shapiro NI, et al. Crit Care Med 2006;34:1025-1032.
ControversiesWhen to Order a Lactate?
• “Blood culture = lactate”
• ≥2 SIRS criteria & suspected infection (i.e. septic)
ControversiesEGDT
1st 6 Hours – Was it the volume?
3.5±2.4L
18.5%
60%
0.8%
Control
EGDT
P<0.001
P<0.001
P<0.001P<0.0015±3L
64%
95%13.7%
Fluids Red Cell Transfusion
Dobutamine ScvO2 ≥ 70%
Rivers E, et al. NEJM 2001;345:1368-77. (see accompanying Letters to the Editor. NEJM 2002;346:1025-1026.)
ControversiesEGDT
Central venous ±arterial catheterization
CVP
MAP
ScvO2
Goals achieved
Colloid
<8 mm HgCrystalloid
Transfusion of red cells until hematocrit > 30%
<70%≥ 70%
No
Supplemental O2 ±endotracheal intubation &
mechanical ventilation
Vasoactive agents<65 mm Hg>90 mm Hg
Norepinephrine pressor of choice
<70%
Inotropic agentsDobutamine
Sedation, paralysis (if intubated), or both
CVP
Dobutamine-induced
hypotension vs unmasks volume
depletion 35.9%
50.4%
13.7%
27.4%
ControversiesEGDT
1st 6 Hours – Was it the volume?
3.5±2.4L
18.5%
60%
0.8%
Control
EGDT
P<0.001
P<0.001
P<0.001P<0.0015±3L
64%
95%13.7%
Fluids Red Cell Transfusion
Dobutamine ScvO2 ≥ 70%
ControversiesStandardized Order Sets
• Cookbook or evidence-based medicine??
• Significantly reduced mortality & length of stay
Micek ST, et al. Crit Care Med 2006;34:2707.
10
ControversiesSingle Center & Small n
• Review of all published EGDT data12 trials (1298 patients)
Aggregate risk reduction of 20.3%
Did not use formal methods for meta-analyses
Otero RM, et al. Chest 2006 Nov;130:1579-95.
ControversiesHigh Cost / Resource Utilization
• 23.4% reduction in hospital costs
• Most cost effective if >16 patients/year
• True for all models (ED-, Rapid Response Team-, and ICU-based care)
Huang DT, et al. Crit Care 2003;7(suppl):S116.
ControversiesProprietary Equipment
• PreSep catheter & Vigilance monitor (Edwards Lifesciences)
• Can use central line (in RA) & drawblood gases for serial ScvO2 levels instead
ControversiesPharma Support of SSC Guidelines
• Lilly & Edwards funded Surviving Sepsis Campaign
? overstated benefits of activated protein CNo mention of ADDRESS/RESOLVE trial data
• Guidelines from other unbiased sourcesare similar
Eichacker PO, Natanson C, Danner RL. NEJM 2006;355:1640-2.
• Surviving Sepsis CampaignDefinitions & EpidemiologyEvidence-Based RecommendationsImplementation strategies
• Controversies• Future Directions
Future DirectionsDiagnostics
• More specific markers for bacterial sepsisProcalcitonin???Soluble Flt-1???
• Predicting who may progress from severe sepsis to septic shock
Heart rate variability
11
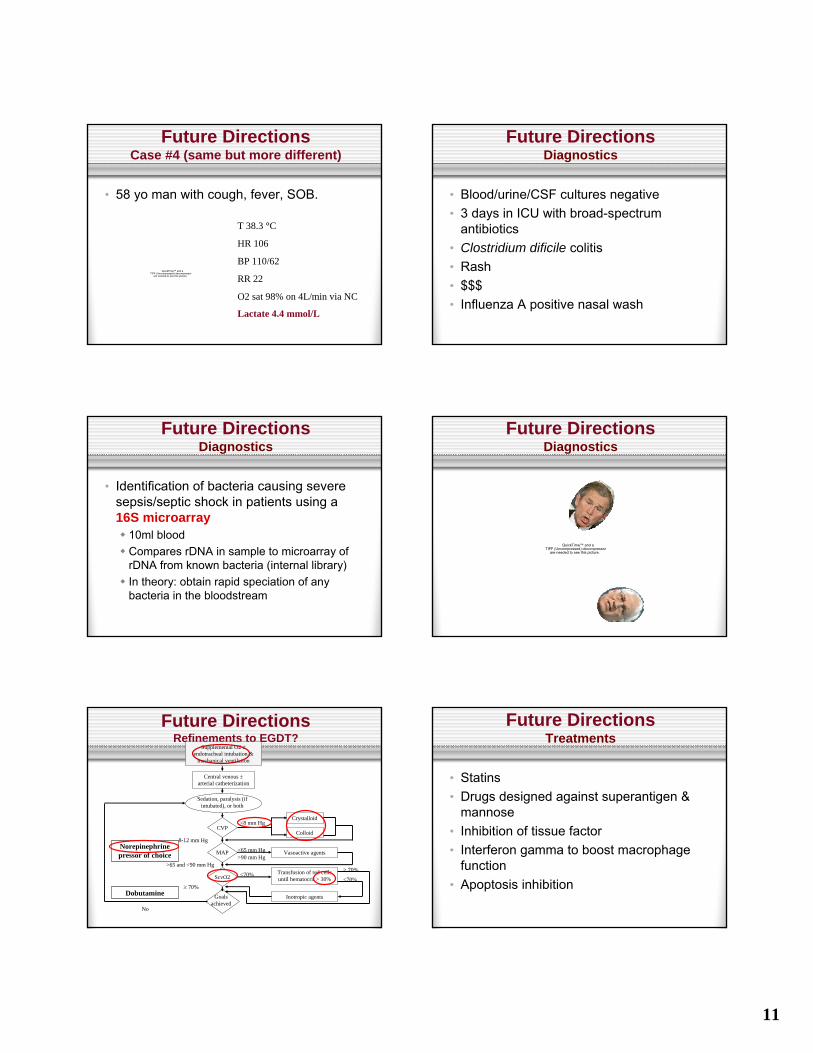
Future DirectionsCase #4 (same but more different)
• 58 yo man with cough, fever, SOB.
Lactate 4.4 mmol/L
T 38.3 °C
HR 106
BP 110/62
RR 22
O2 sat 98% on 4L/min via NC
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Future DirectionsDiagnostics
• Blood/urine/CSF cultures negative• 3 days in ICU with broad-spectrum
antibiotics• Clostridium dificile colitis• Rash• $$$• Influenza A positive nasal wash
Future DirectionsDiagnostics
• Identification of bacteria causing severe sepsis/septic shock in patients using a 16S microarray
10ml bloodCompares rDNA in sample to microarray of rDNA from known bacteria (internal library)In theory: obtain rapid speciation of anybacteria in the bloodstream
Future DirectionsDiagnostics
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Future DirectionsRefinements to EGDT?
Central venous ±arterial catheterization
Sedation, paralysis (if intubated), or both
CVP
MAP
ScvO2
Goals achieved
Colloid
<8 mm HgCrystalloid
8-12 mm Hg
>65 and <90 mm HgTransfusion of red cells until hematocrit > 30%
<70%≥ 70%
No
Supplemental O2 ±endotracheal intubation &
mechanical ventilation
Vasoactive agents<65 mm Hg>90 mm Hg
Norepinephrine pressor of choice
<70%≥ 70%
Inotropic agentsDobutamine
Future DirectionsTreatments
• Statins• Drugs designed against superantigen &
mannose• Inhibition of tissue factor• Interferon gamma to boost macrophage
function• Apoptosis inhibition
12
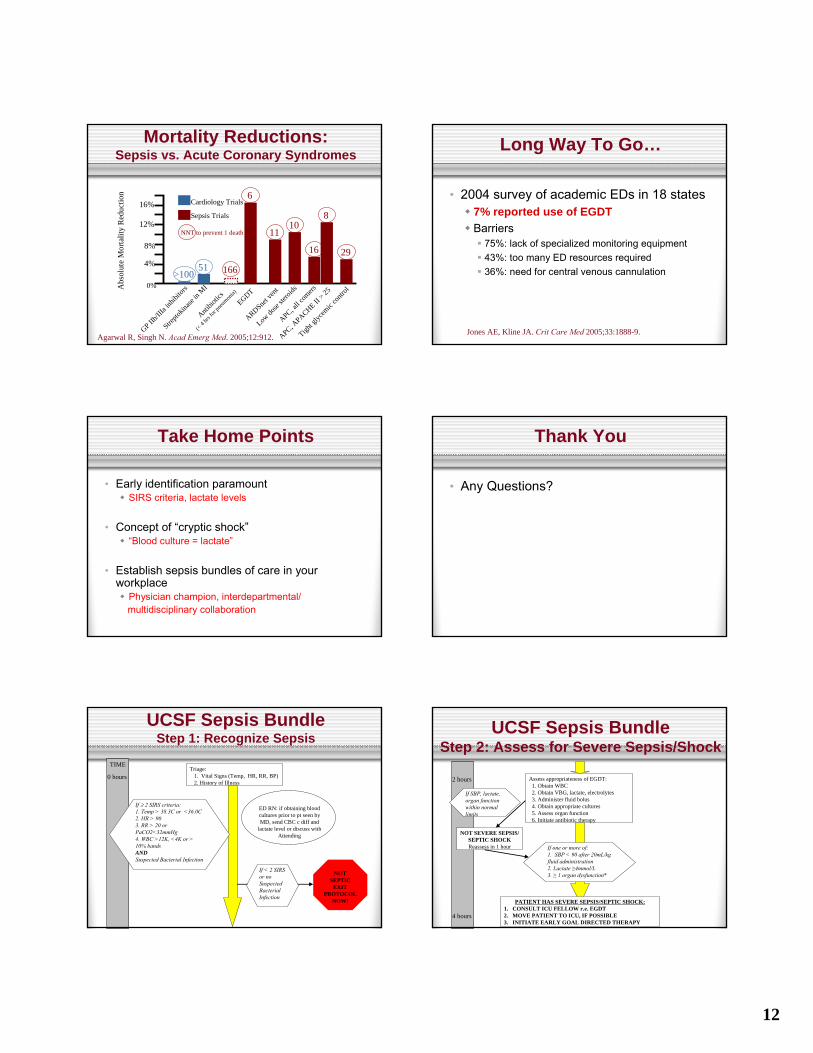
Mortality Reductions: Sepsis vs. Acute Coronary Syndromes
Abs
olut
e M
orta
lity
Red
uctio
n
16%
12%
8%
4%
0%
Cardiology Trials
Sepsis Trials
GP IIb/II
Ia inh
ibitor
s
Strepto
kinase
in M
I
APC, all c
omers
APC, APACHE II
> 25
EGDT
Low do
se ste
roids
ARDSnet v
ent
Tight g
lycem
ic co
ntrol
Antibio
tics
(< 4 hrs
for p
neumon
ia)
51>100
16
1011
29
6
8
NNT to prevent 1 death
Agarwal R, Singh N. Acad Emerg Med. 2005;12:912.
166
Long Way To Go…
• 2004 survey of academic EDs in 18 states7% reported use of EGDTBarriers
75%: lack of specialized monitoring equipment43%: too many ED resources required36%: need for central venous cannulation
Jones AE, Kline JA. Crit Care Med 2005;33:1888-9.
Take Home Points
• Early identification paramountSIRS criteria, lactate levels
• Concept of “cryptic shock”“Blood culture = lactate”
• Establish sepsis bundles of care in your workplace
Physician champion, interdepartmental/multidisciplinary collaboration
Thank You
• Any Questions?
UCSF Sepsis BundleStep 1: Recognize Sepsis
TIME
0 hoursTriage:
1. Vital Signs (Temp, HR, RR, BP)2. History of Illness
If ≥ 2 SIRS criteria:1. Temp > 38.3C or <36.0C2. HR > 903. RR > 20 or PaCO2<32mmHg4. WBC >12K, <4K or > 10% bands ANDSuspected Bacterial Infection
ED RN: if obtaining blood cultures prior to pt seen by MD, send CBC c diff and
lactate level or discuss with Attending
If < 2 SIRS or no Suspected Bacterial Infection
NOT SEPTIC
EXIT PROTOCOL
NOW!
UCSF Sepsis BundleStep 2: Assess for Severe Sepsis/Shock
Assess appropriateness of EGDT:1. Obtain WBC2. Obtain VBG, lactate, electrolytes3. Administer fluid bolus4. Obtain appropriate cultures5. Assess organ function6. Initiate antibiotic therapy
2 hours
4 hours
If SBP, lactate, organ function within normal limits
NOT SEVERE SEPSIS/ SEPTIC SHOCKReassess in 1 hour If one or more of:
1. SBP < 90 after 20mL/kg fluid administration2. Lactate ≥4mmol/L3. ≥ 1 organ dysfunction*
PATIENT HAS SEVERE SEPSIS/SEPTIC SHOCK:1. CONSULT ICU FELLOW r.e. EGDT2. MOVE PATIENT TO ICU, IF POSSIBLE3. INITIATE EARLY GOAL DIRECTED THERAPY
13
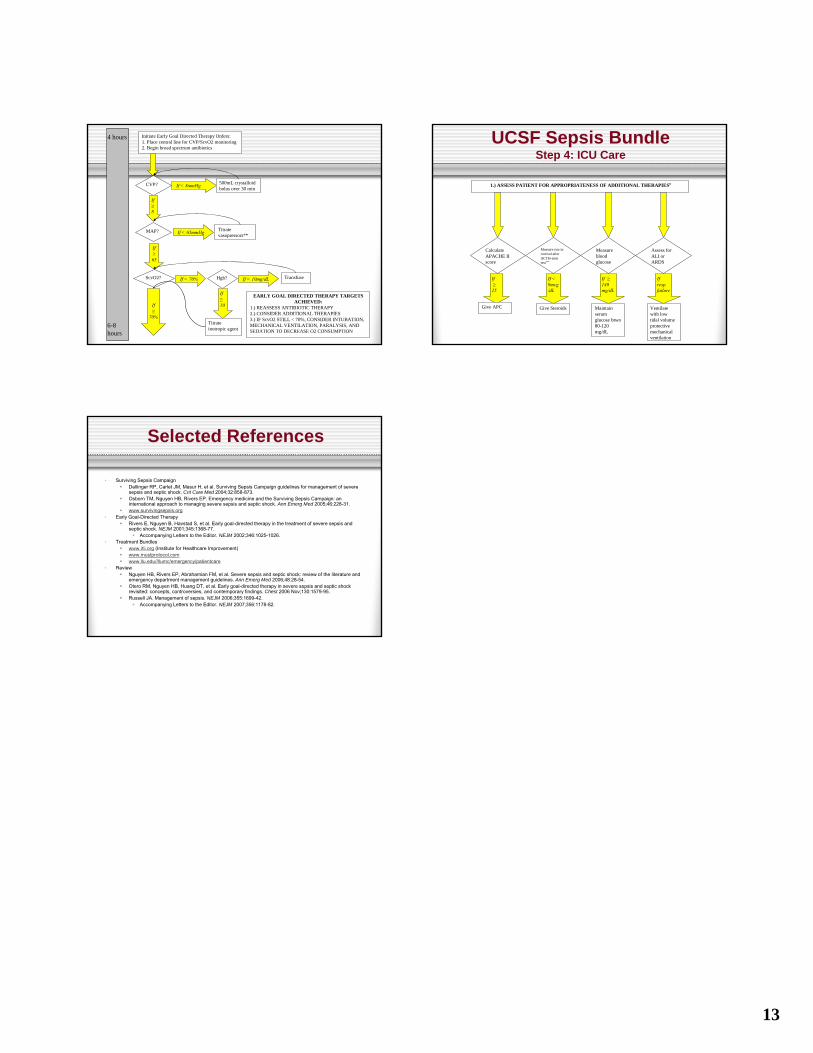
4 hours Initiate Early Goal Directed Therapy Orders:1. Place central line for CVP/ScvO2 monitoring2. Begin broad spectrum antibiotics
CVP? If < 8mmHg 500mL crystalloid bolus over 30 min
If≥8
MAP? If < 65mmHg Titratevasopressors**
ScvO2? If < 70% Hgb?
If ≥65
6-8 hours
If ≥
70%
EARLY GOAL DIRECTED THERAPY TARGETS ACHIEVED:
1.) REASSESS ANTIBIOTIC THERAPY2.) CONSIDER ADDITIONAL THERAPIES3.) IF ScvO2 STILL < 70%, CONSIDER INTUBATION, MECHANICAL VENTILATION, PARALYSIS, AND SEDATION TO DECREASE O2 CONSUMPTION
If ≥10
Titrateinotropic agent
If < 10mg/dL Transfuse
UCSF Sepsis BundleStep 4: ICU Care
1.) ASSESS PATIENT FOR APPROPRIATENESS OF ADDITIONAL THERAPIES#
Calculate APACHE II score
Measure rise incortisol after ACTH-stim test***
Measure blood glucose
Assess for ALI or ARDS
If≥
25
Give APC
If < 9mcg/dL
Give Steroids
If ≥140 mg/dL
Maintain serum glucose btwn80-120mg/dL
Ifresp. failure
Ventilate with low tidal volume protective mechanical ventilation
Selected References
• Surviving Sepsis CampaignDellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med 2004;32:858-873.Osborn TM, Nguyen HB, Rivers EP. Emergency medicine and the Surviving Sepsis Campaign: an international approach to managing severe sepsis and septic shock. Ann Emerg Med 2005;46:228-31.www.survivingsepsis.org
• Early Goal-Directed TherapyRivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. NEJM 2001;345:1368-77.
Accompanying Letters to the Editor. NEJM 2002;346:1025-1026.• Treatment Bundles
www.ihi.org (Institute for Healthcare Improvement)www.mustprotocol.comwww.llu.edu//llumc/emergency/patientcare
• ReviewNguyen HB, Rivers EP, Abrahamian FM, et al. Severe sepsis and septic shock: review of the literature and emergency department management guidelines. Ann Emerg Med 2006;48:28-54.Otero RM, Nguyen HB, Huang DT, et al. Early goal-directed therapy in severe sepsis and septic shock revisited: concepts, controversies, and contemporary findings. Chest 2006 Nov;130:1579-95.Russell JA. Management of sepsis. NEJM 2006;355:1699-42.
Accompanying Letters to the Editor. NEJM 2007;356:1178-82.