seronegative arthritis or spondyloartropaties. introduction spondyloarthritis or seronegative...
TRANSCRIPT
Seronegative ArthritisSeronegative ArthritisOrOr
SpondyloartropatiesSpondyloartropaties
Introduction
Spondyloarthritis or Seronegative Spondyloarthritis
– Refers to inflammatory changes involving the spine and the spinal joints.
– Absence of Rheumatoid Factor and ANA
Spondyloarthritis • A group of autoimmune
diseases that in common appear mediated by activation of autoreactive CD8 T cells
• Primarily affect joints, skin, eyes and mucous membranes
• Physical stress, inflammation and infection with specific microorganisms trigger the immune response
Spondyloarthropathies (SpA)
Frequent – prevalence ~ 0.5% Chronic Inflammatory With potential disabling outcomes Consist of several disorders
SpA consist of several disorders
• Ankylosing spondylitis (ASp)• Reiter’s syndrome (RS) / reactive arthritis
(ReA)• Psoriatic arthritis (PsA)• Undifferentiated spondyloarthritis (USpA)• Enteropathic arthritis (ulcerative colitis,
regional enteritis)
Spondyloarthritis Diseases-features common to all
1. Clinical:• - Affect joints, skin, eyes and mucous
membranes in varying proportions with characteristic joint involvement: – Spondylitis(inflammation of vertebral
discs), – sacroiliitis (sacroiliac joints) and – enthesitis (tendon insertions).
• All with granulomatous fibrosis and newbone formation
Spondyloarthritis Diseases-features common to all
peripheral articular involvement– asymmetric mono-oligoarticular
Common in male
Sausage digits
Spondyloarthritis Diseases-features common to all
Enthesopathy– Achilles tenosynovitis
Extra-articular manifestationsOral aphtae, Erythema nodosum, uveitis
Absence of RF and Rheumatoid nodules
Absence of Raynoud’s phenomenon
Spondyloarthritis Diseases-features common to all
• 2. Genetic:– Susceptibility to develop disease is
associated with inheritance of certain MHC class I alleles, notably HLA-B27
– Positive family history
• 3. Pathogenesis:– Effector/ memoryCD8 T cells are activated
and clonally expanded while CD4 T cells or B cells are not involved
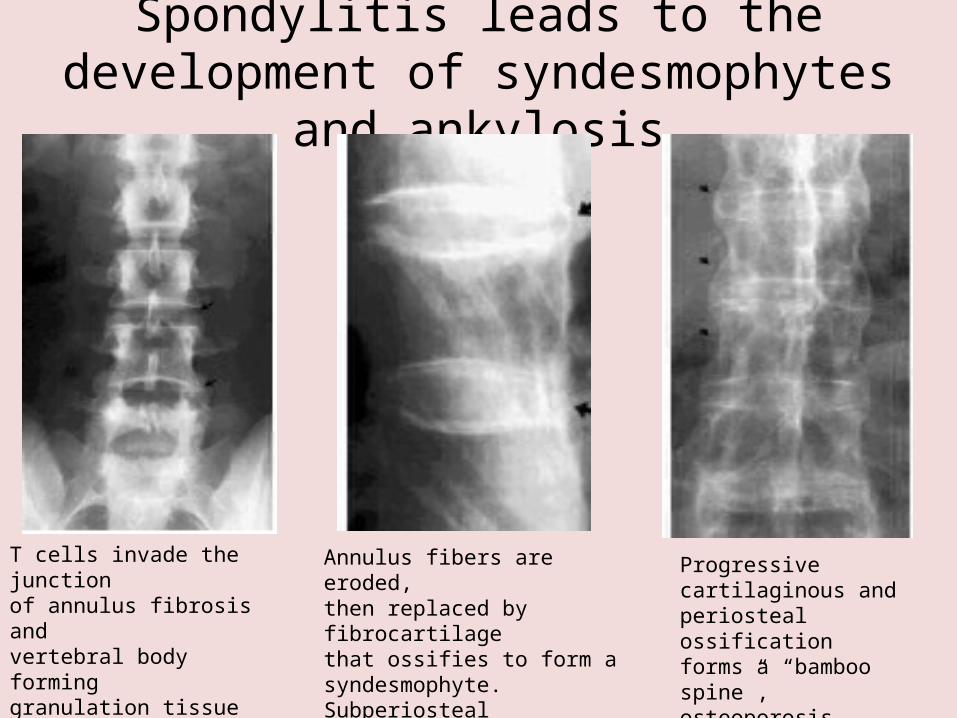
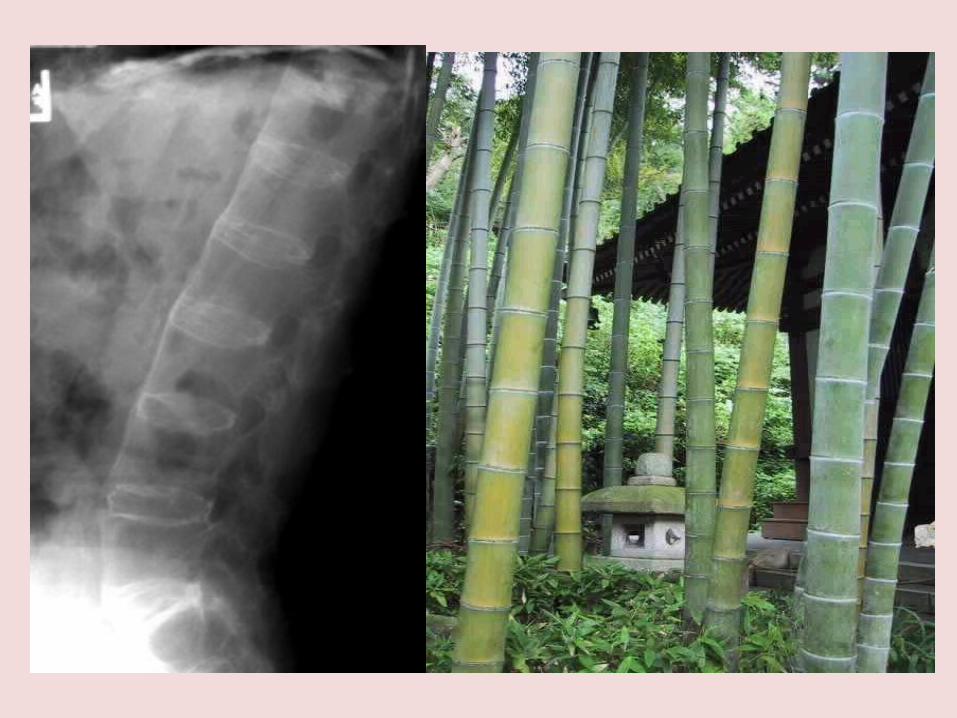
Spondylitis leads to the development of syndesmophytes
and ankylosis
T cells invade the junctionof annulus fibrosis andvertebral body forminggranulation tissue(activated macrophages, Tcells and fibroblasts)
Annulus fibers are eroded,then replaced by fibrocartilagethat ossifies to form asyndesmophyte. Subperiostealnew bone formation ensues
Progressivecartilaginous andperiosteal ossificationforms a “bamboo spine”,osteoporosis develops
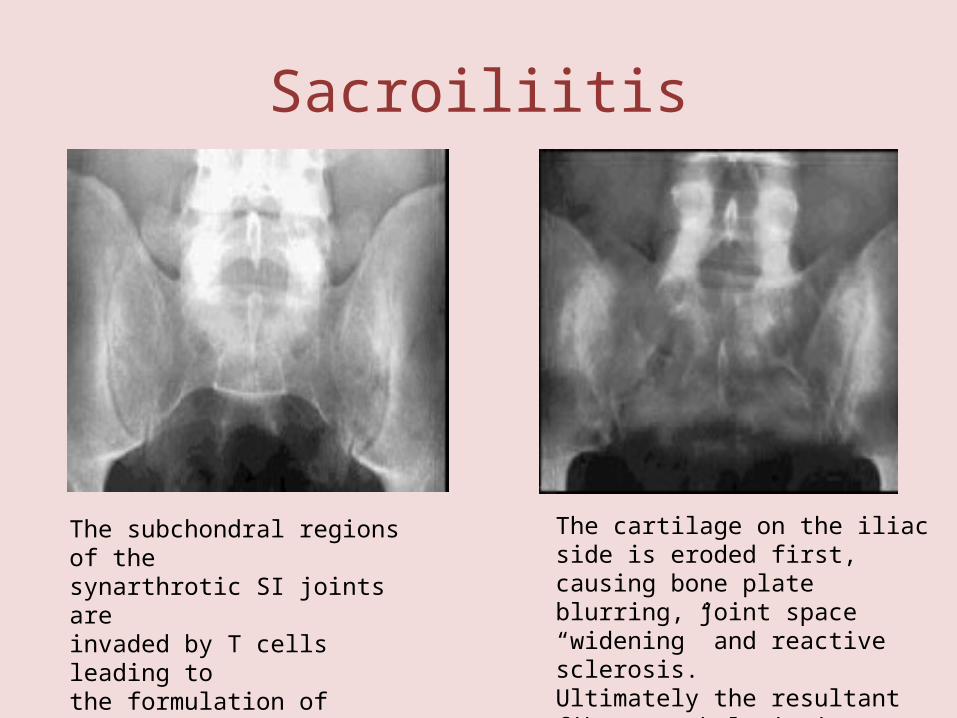
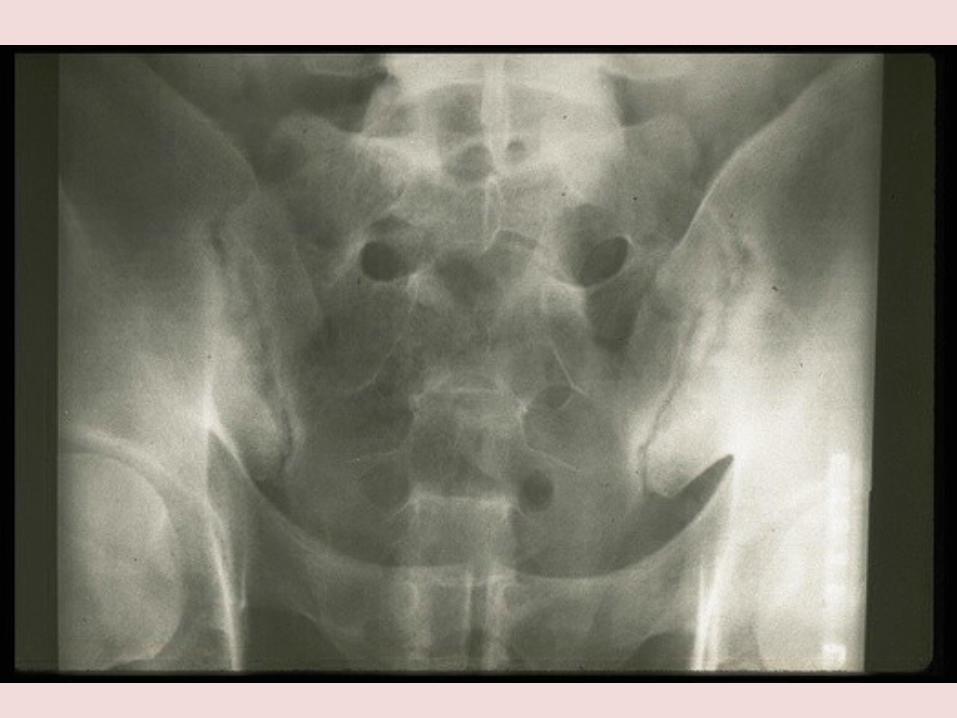
Sacroiliitis
The subchondral regions of thesynarthrotic SI joints areinvaded by T cells leading tothe formulation of granulationTissue
The cartilage on the iliac side is eroded first, causing bone plate blurring, joint space “widening” and reactive sclerosis.Ultimately the resultant fibrous ankylosis is replaced by bone, obliterating the SI joint
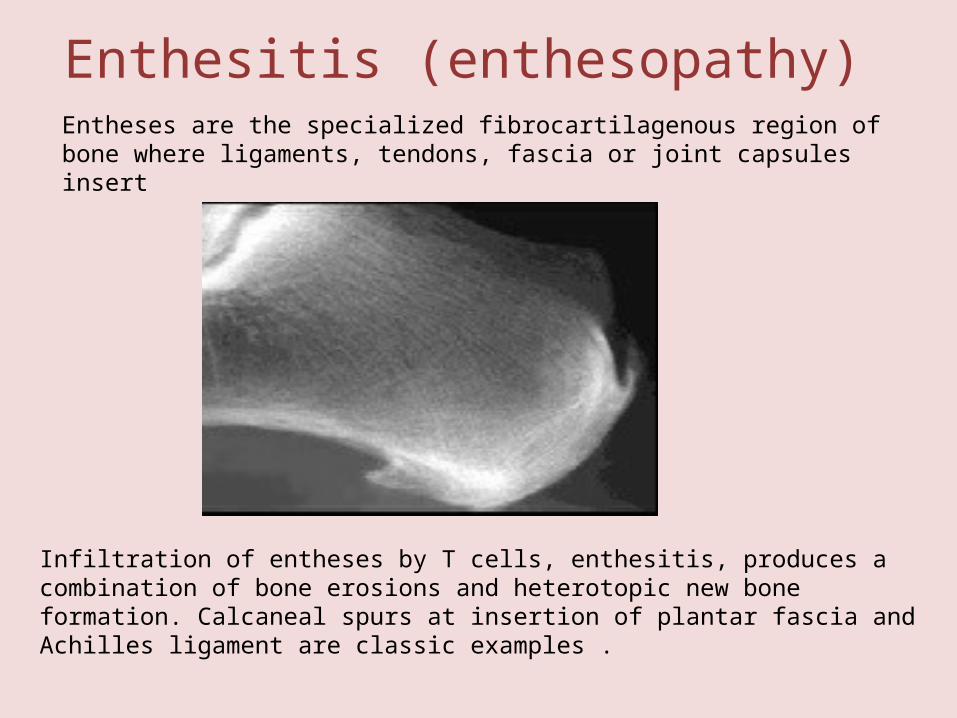
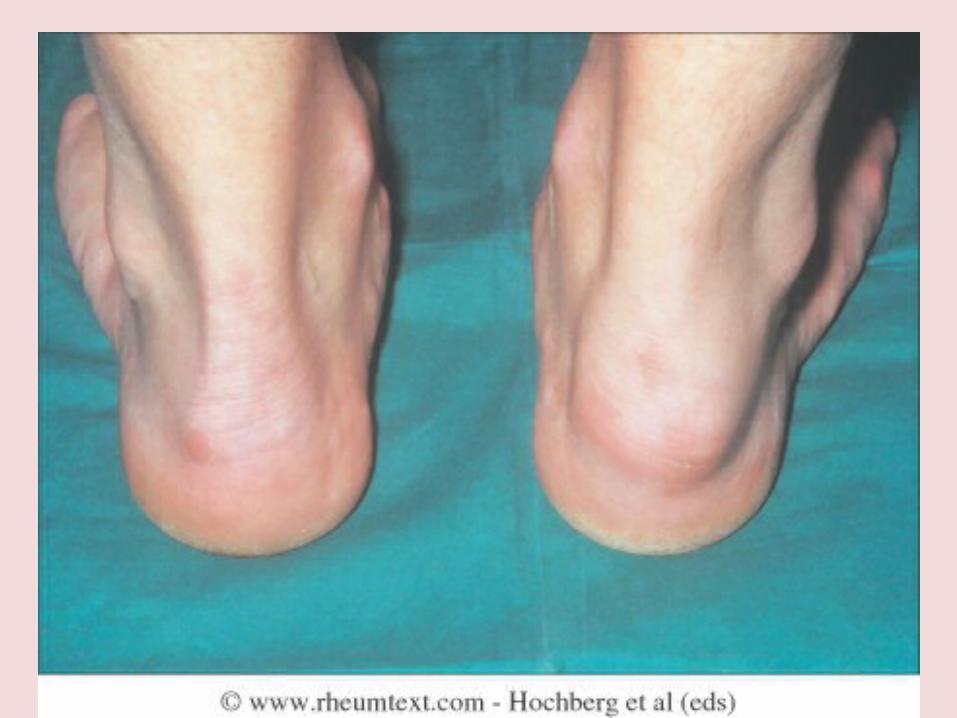
Enthesitis (enthesopathy) Entheses are the specialized fibrocartilagenous region of bone where ligaments, tendons, fascia or joint capsules insert
Infiltration of entheses by T cells, enthesitis, produces a combination of bone erosions and heterotopic new bone formation. Calcaneal spurs at insertion of plantar fascia and Achilles ligament are classic examples .
• Inflammatory back pain
• Onset before age 40• Insidious persistent (> 3 mo) dull deep
buttock or low back pain• Stiffness/pain upon arising in the morning,
or during sleep• Improvement with exercise Due to the
initial inflammation of enthesitis, spondylitis or sacroiliitis
• Poorly localized, does not follow nerve root
Genetic epidemiology
• HLA-B27 increased, but unevenly, among spondylitis diseases
HLA-B27 frequency (%)
• Ankylosing spondylitis 95• Reiter’s syndrome (reactive arthritis) 70• Psoriatic arthritis 20-40• Ethnically matched controls 8
• Other class I alleles may also be involved, especially in PsA
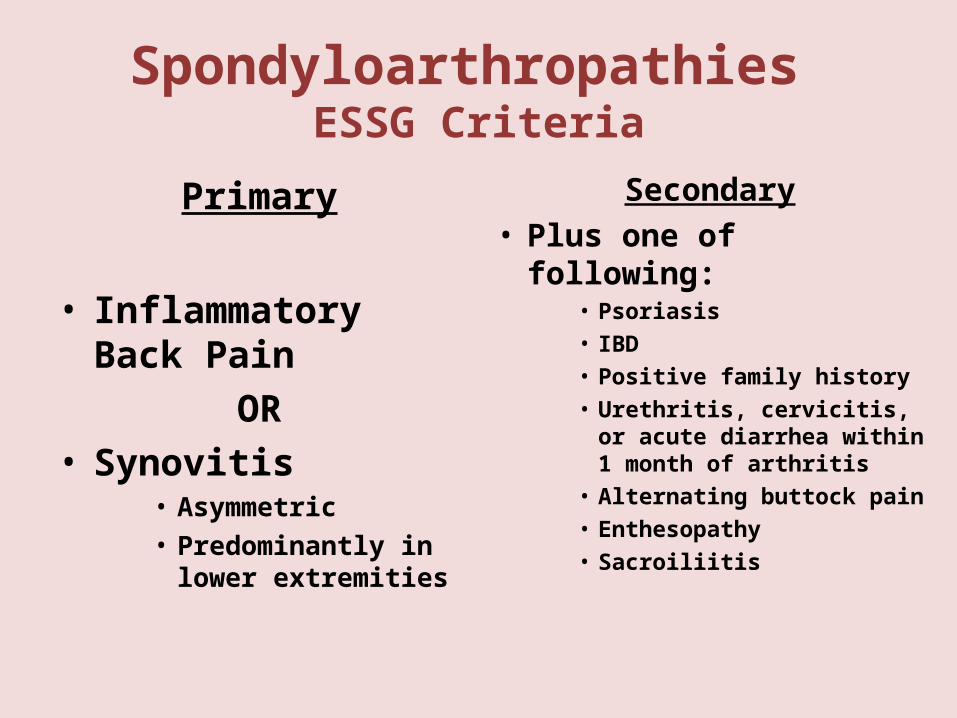
Spondyloarthropathies ESSG Criteria
Primary
• Inflammatory Back Pain
OR• Synovitis
• Asymmetric• Predominantly in lower
extremities
Secondary• Plus one of following:
• Psoriasis• IBD• Positive family history• Urethritis, cervicitis, or
acute diarrhea within 1 month of arthritis
• Alternating buttock pain• Enthesopathy• Sacroiliitis
Ankylosing Spondylitis
Ankylosing Spondylitis
• A progressive autoimmune inflammatory disease characterized by widespread spondylitis and sacroiliitis
• Onset, age 10-35 with dull pain in lumbar or gluteal regions
• Hip, shoulder, knee arthritis in ~30%
• Epidemiology: >95% of those affected are positive for HLA-B27
• Affects 1-3% of HLA-B27 individuals,
• Begins in the Sacroiliac Joints and progresses upwards and can involve the entire spine


Ankylosing Spondylitis
• Inflammatory Stages– Can be extremely painful (flares)– Prolonged morning stiffness (hours)– Fatigue (pain & lack of sleep)
• Ankylosis– Stiffness increases – Significantly reduced ROM– Abnormal posture
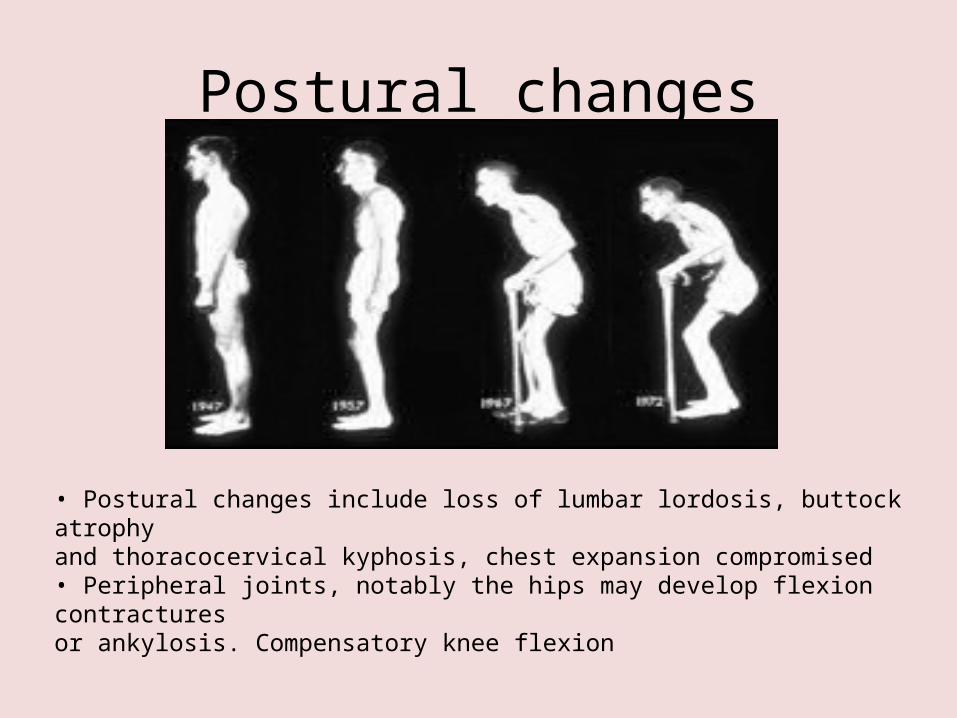
Postural changes
• Postural changes include loss of lumbar lordosis, buttock atrophyand thoracocervical kyphosis, chest expansion compromised• Peripheral joints, notably the hips may develop flexion contracturesor ankylosis. Compensatory knee flexion
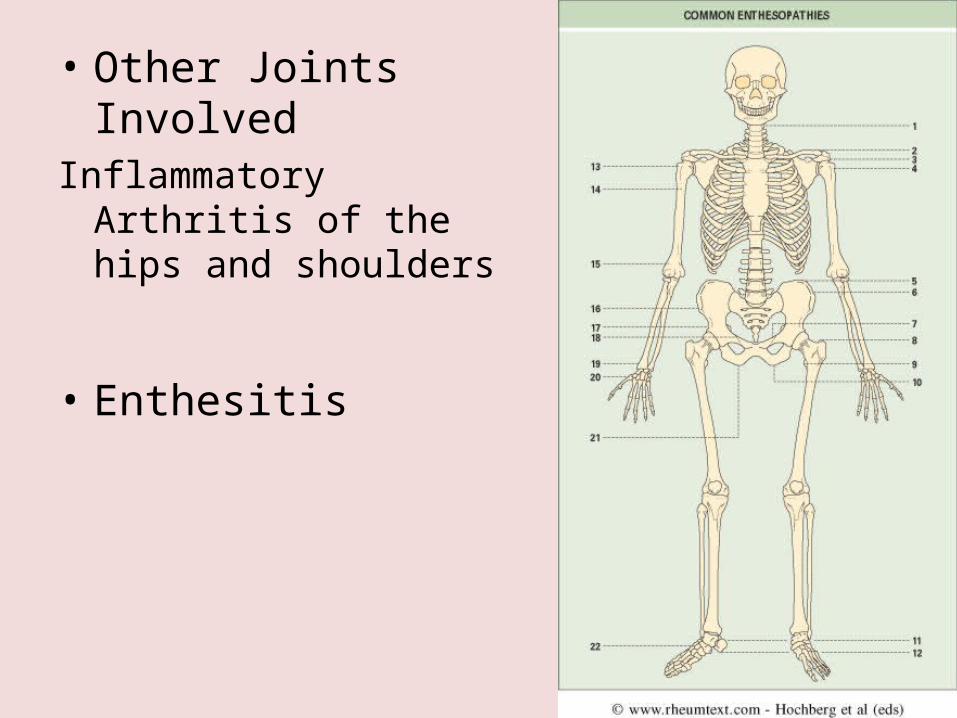
• Other Joints InvolvedInflammatory Arthritis of the
hips and shoulders
• Enthesitis
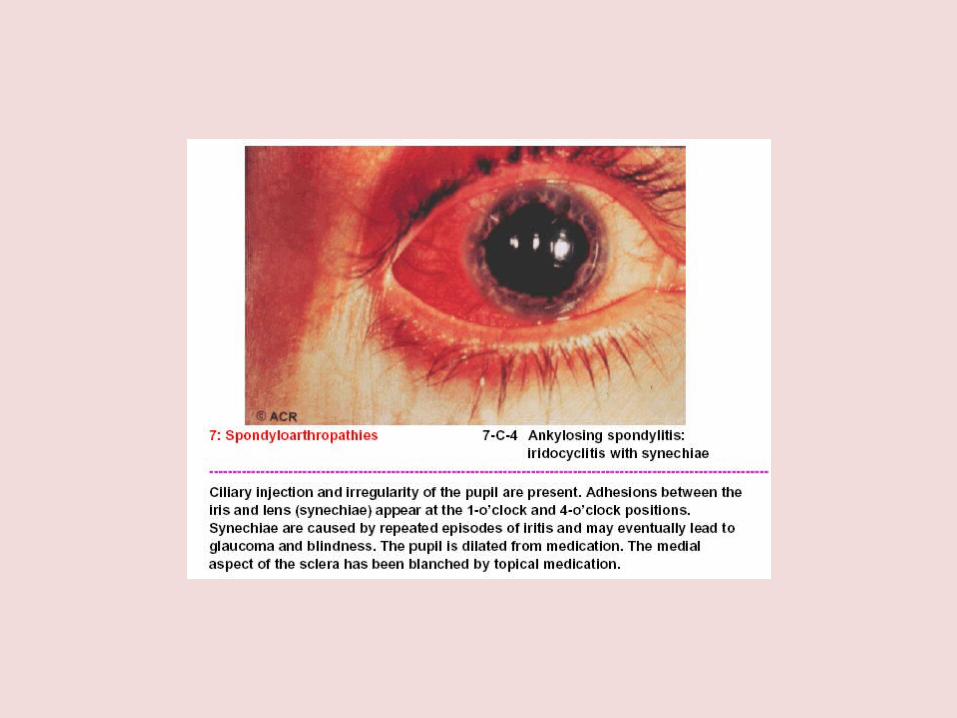
Extra-Articular Features• Eyes: Acute anterior uveitis (40%)
– most common extraarticular features of AS– Anterior uveitis can precede the onset of AS by
several years– Strongly associated with HLA B27
• Lungs: Rigidity of the chest wall and fibrosis in the upper lungs
• Kidneys: IgA nephropathy (rare)
• Heart: Aortitis (dilation of aortic root), aortic regurgitation
Laboratory Investigations
• Evidence of Inflammation– Normochromic normocytic anemia– Elevated ESR/CRP– Reactive thrombocytosis
• HLA-B27 found in 90-95% of patients with Ank Spond vs 6-8% of general population
Imaging Studies
• Sacroiliac joints:– Standard anteroposterior radiograph of the pelvis– Ferguson view-15 degree angle to the prone pelvis– Erosions-pseudowidening of SI Joint– Obliteration of SI joint
• Scintigraphy• MRI-visualization of acute sacroiliitis• CT-erosions


Psoriatic Arthritis
Psoriatic arthritis
• Psoriatic arthritis: an often clinically distinctive complex of enthesitis and arthritis that occurs in the setting of psoriasis
• It may involve the spine or peripheral joints in a variety of patterns,and is initiated or exacerbated by stress or non specific infection
Progression
• Polyarticular in 30-50%– Like Rheumatoid Arthritis
• Oligoarticular in 40-50%• Predominant Spinal Disease in 5%
– Spinal symptoms usually occur after many years of peripheral arthritis
• DIP involvement in 5%• Arthritis Mutilans in 5%
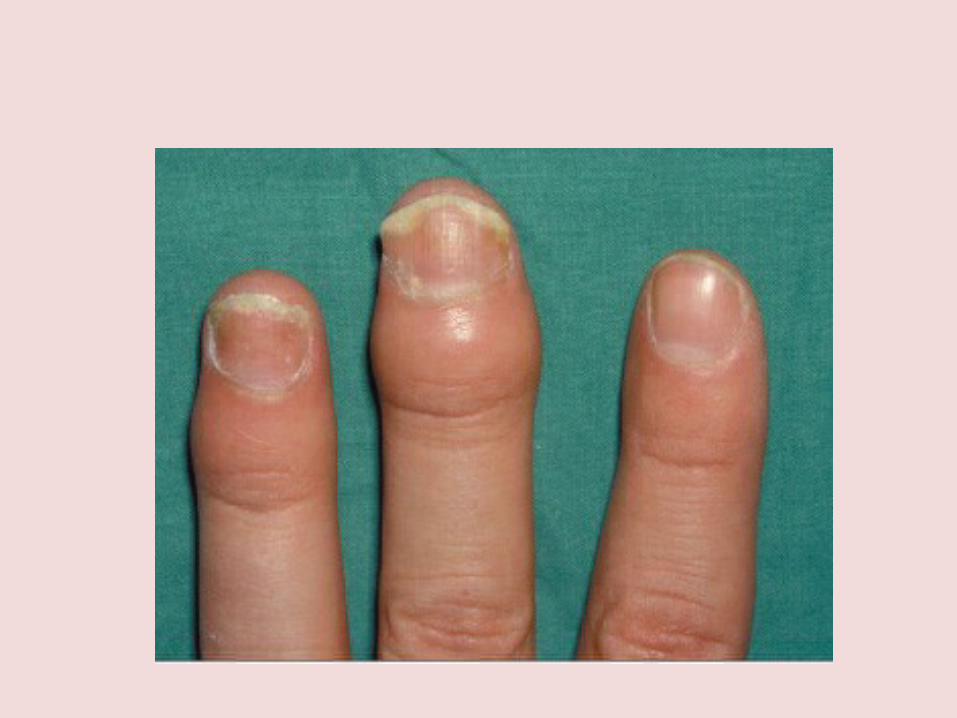
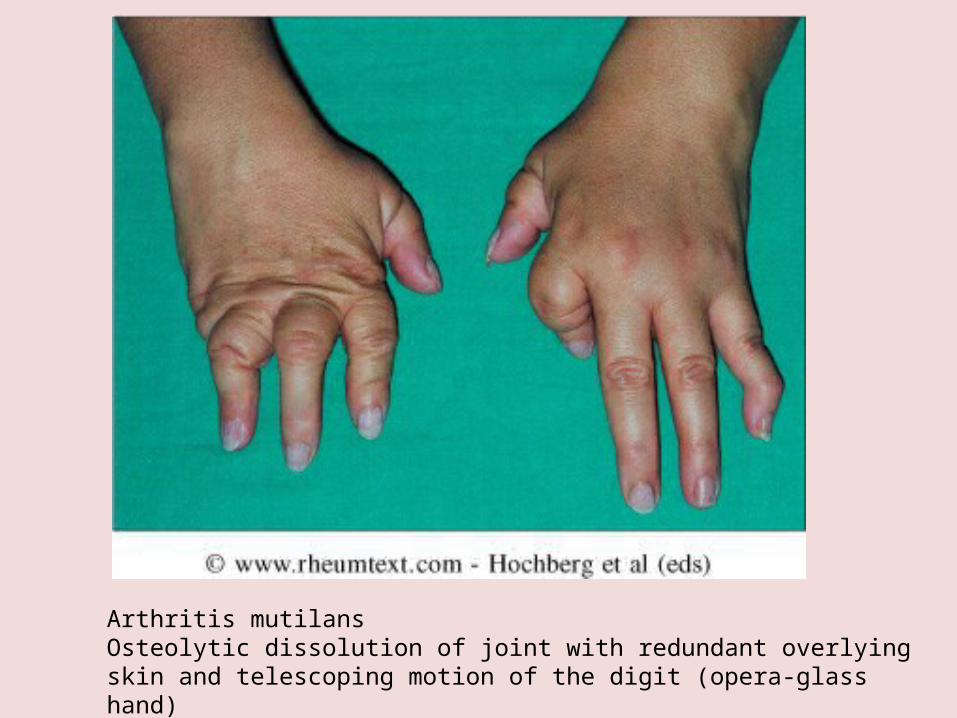
Arthritis mutilansOsteolytic dissolution of joint with redundant overlyingskin and telescoping motion of the digit (opera-glass hand)
• Sacroiliac Involvement– Sacroiliitis in 1/3 of patients– Usually asymmetric (unilateral)– May be asymptomatic
• Spinal Involvement– May affect any part of the spine in a
random fashion– Different from ankylosing spondylitis
Rheumatologic Review of Systems
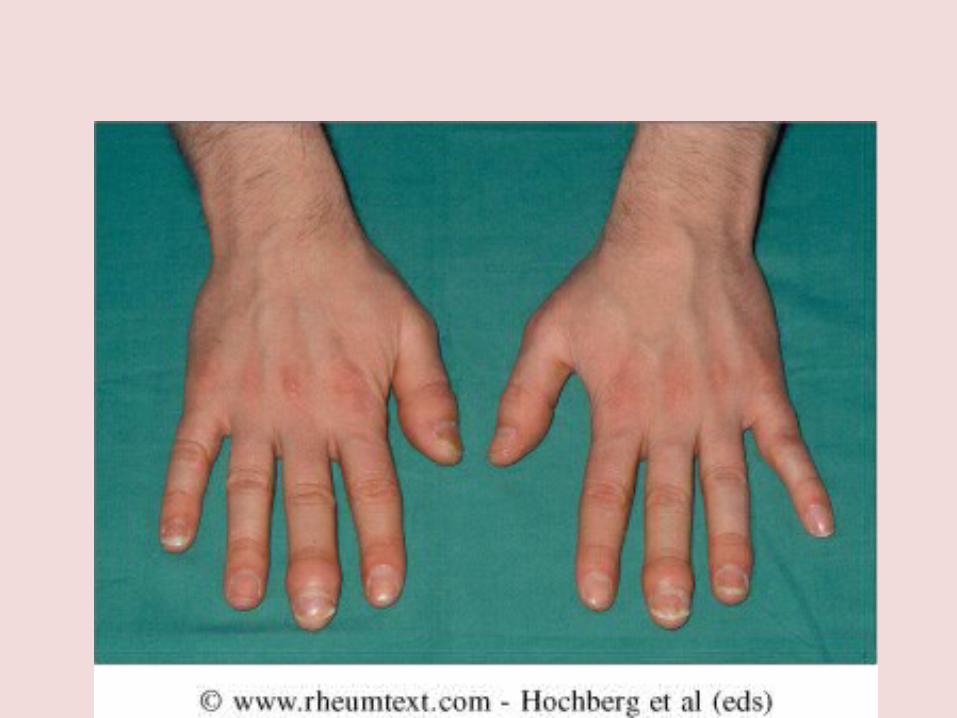
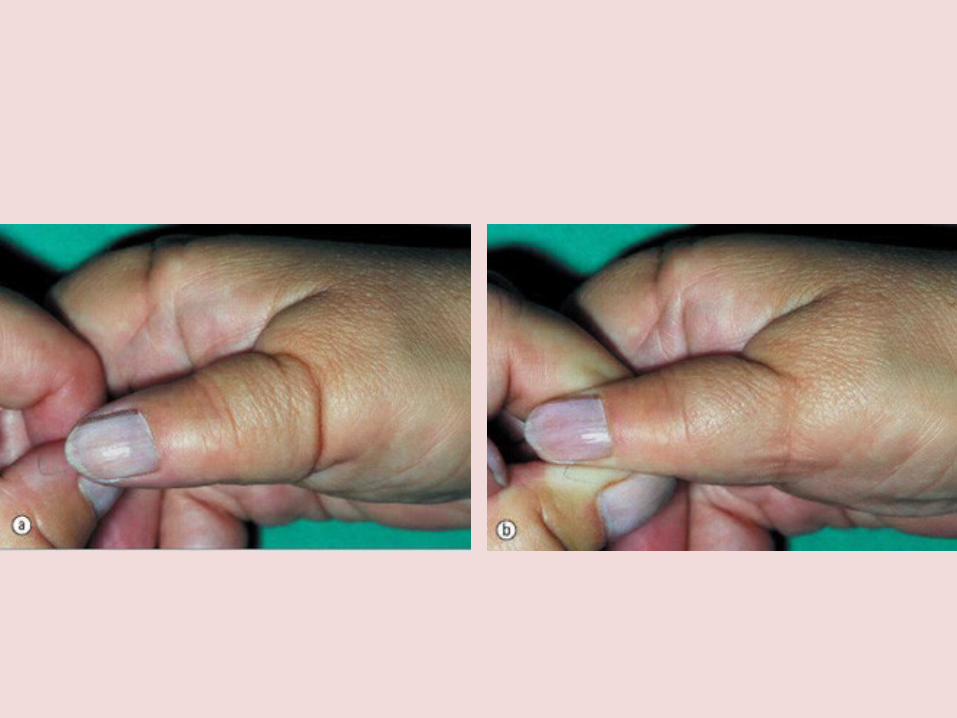
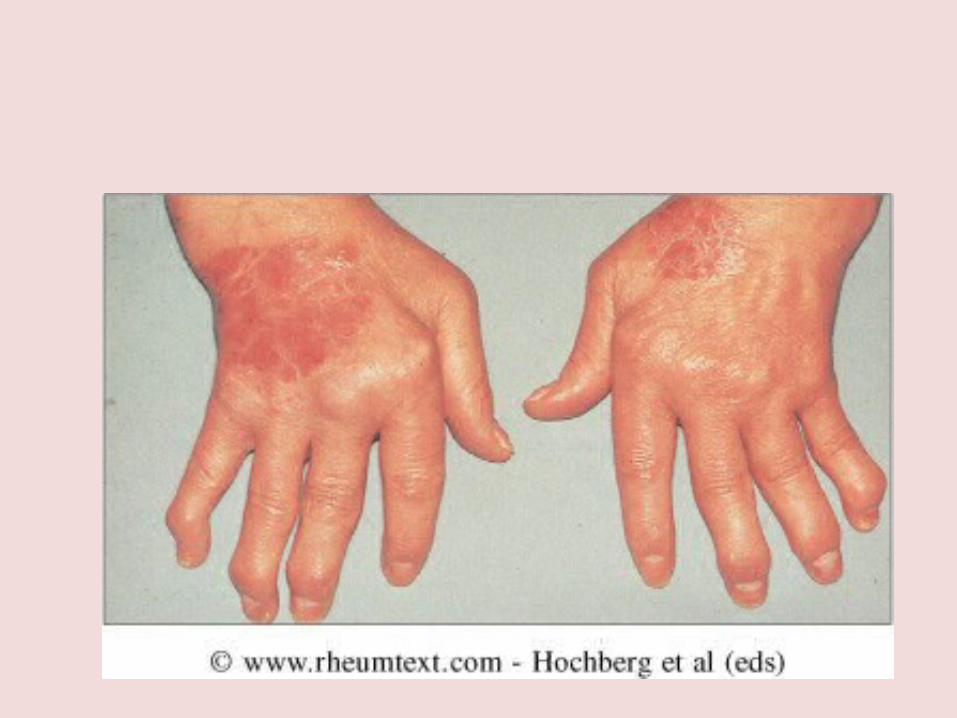
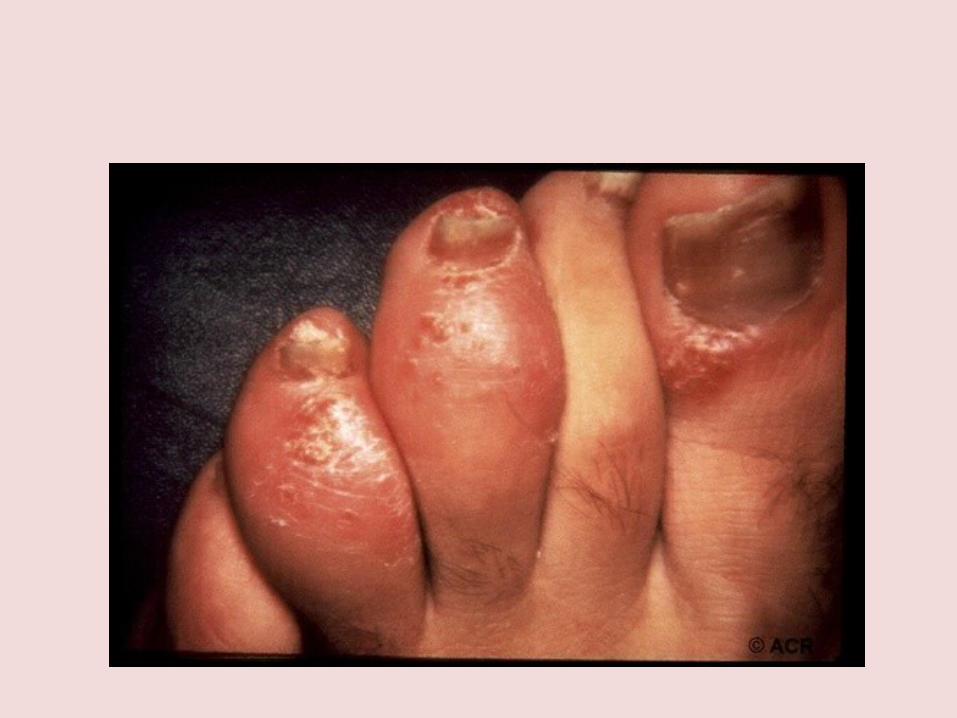
• Mucocutaneous Involvement– Psoriatic skin lesions– Psoriatic Nail lesions
• Entheseal Involvement• Dactylitis• Ocular Involvement
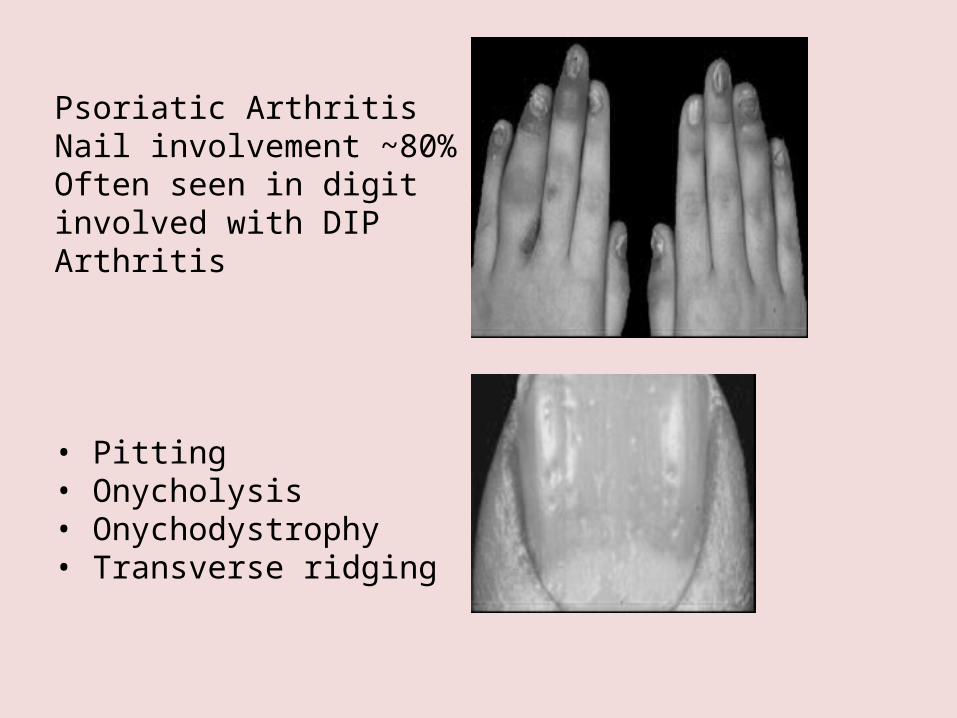
Psoriatic ArthritisNail involvement ~80%Often seen in digitinvolved with DIPArthritis
• Pitting• Onycholysis• Onychodystrophy• Transverse ridging
History - Psoriasis
– Psoriasis present before the onset of joint disease (70%)
– Psoriasis comes with the arthritis (15%)
– Psoriasis comes after the arthritis (15%)

Psoriatic Plaque Under the Knee
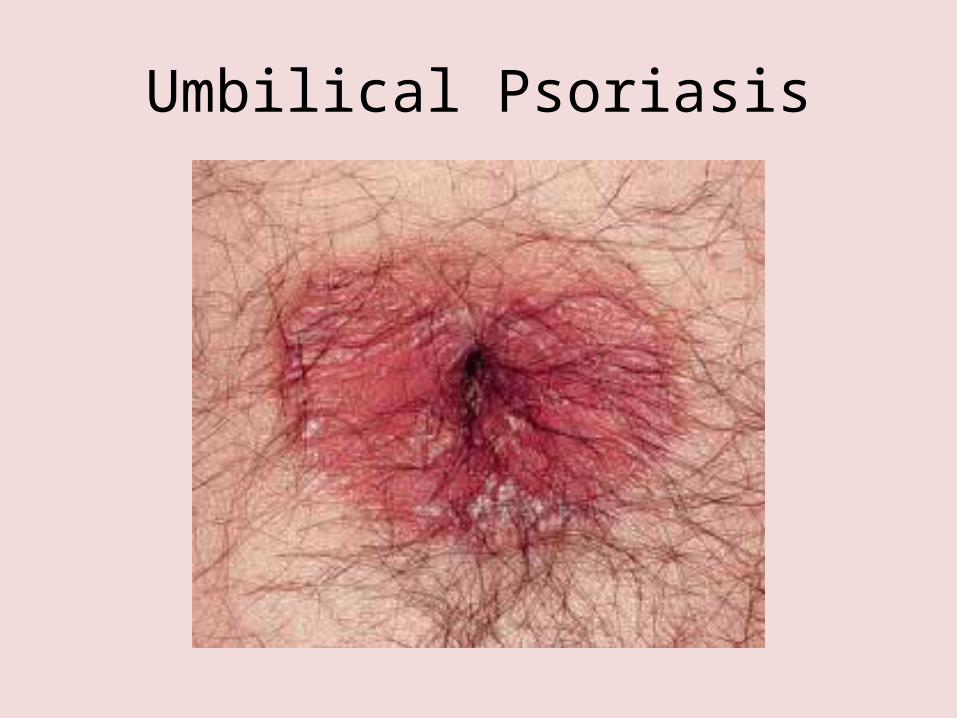
Umbilical Psoriasis
Dactylitis
• Entire digit is involved compared to “fusiform” swelling around a joint
• Dactylitis – represents inflammation of the flexor tenosynovium – “flexor tenosynovitis”

Progression of DIP arthritisNarrowed joint space & condylar erosionsReactive sub periosteal new bonePencil in cup appearance
Management AS and Psoriatic Arthritis
• Goals of Treatment– Improve pain– Improve Function– Prevent Long-term Damage– Safely
• Psoriatic arthritis can lead to a deforming and destructive arthropathy in 20-30%
• Ankylosing spondylitis can result in significant disability
Management
• NSAIDs– Can be useful in some cases of
mono/oligo arthritis– Useful for enthesitis– Useful for spinal disease
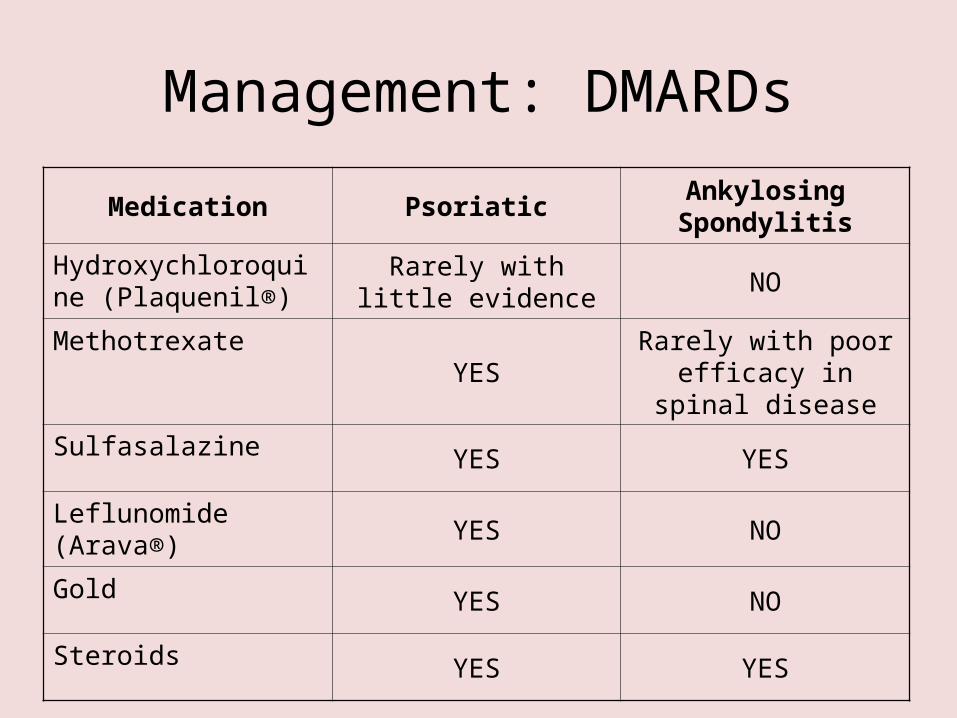
Management: DMARDs
Medication PsoriaticAnkylosing Spondylitis
Hydroxychloroquine (Plaquenil®)
Rarely with little evidence
NO
MethotrexateYES
Rarely with poor efficacy in spinal
disease
Sulfasalazine YES YES
Leflunomide (Arava®)YES NO
Gold YES NO
Steroids YES YES
Management: Biologics
• Biologics Approved for Psoriatic Arthritis and Ankylosing Spondylitis– Etanercept (Enbrel®) – Infliximab (Remicade®)– Adalimumab (Humira®)
• Biggest advance in the treatment of spondyloarthropathies in decades!
• REACTİVE ARTHRITIS
• Reactive arthritis has generally beendefined as sterile synovitis developingafter a distant infection.
• Occurs 2-4 weeks after inciting infection
• Most responsible organisms have an affinity for mucous membranes
• Terms Reactive Arthritis & Reiter’s Syndrome Synonamous
• 1916, Hans Reiter– Arthritis, Conjunctivitis, Non
Gonococcal Urethritis
Reiter Syndrome ?
Classic triad: Arthritis, Urethritis, Conjunktivitis
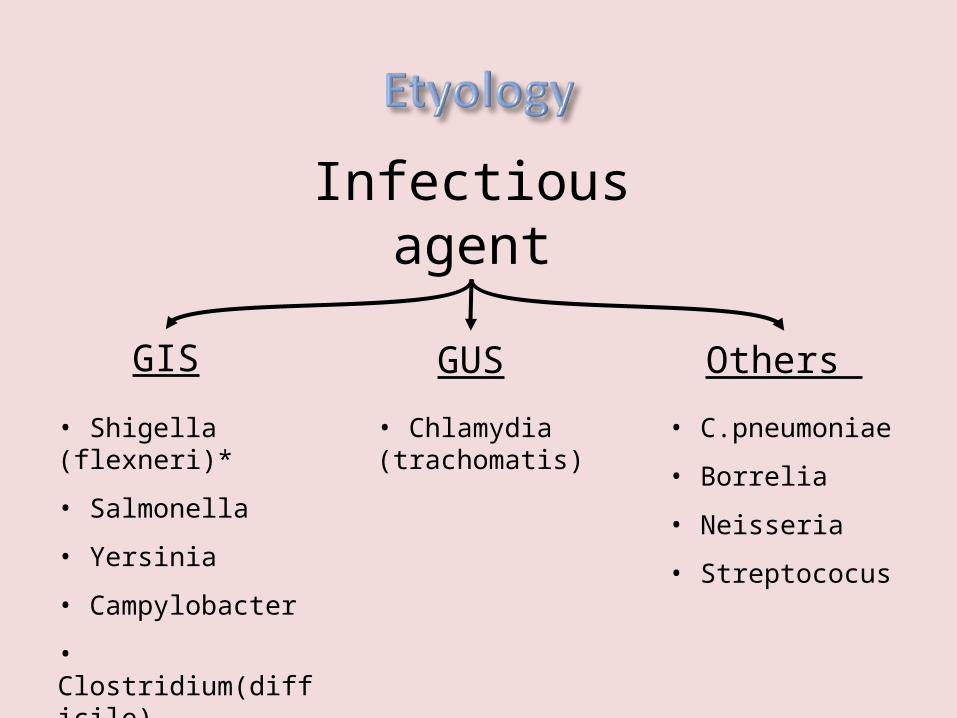
Infectious agent
GIS GUS Others
• Shigella (flexneri)*
• Salmonella
• Yersinia
• Campylobacter
• Clostridium(difficile)
• C.pneumoniae
• Borrelia
• Neisseria
• Streptococus
• Chlamydia (trachomatis)
- symptoms of the triggering infection haveoften been mild and, in about 10% ofcases, the infection has passed unnoticed- Symptoms• malaise,• fatigue• fever• mild arthralgias to severely disabling polyarthritis
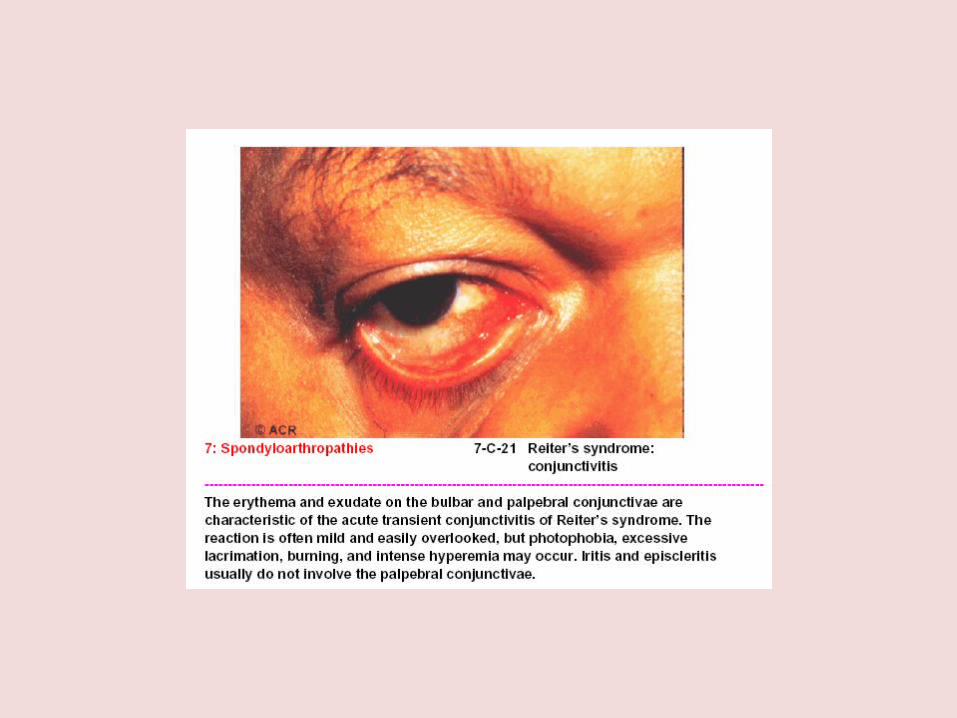
• Conjunctivitis– follows urethritis by several days– Sx often mild and transient– acute anterior Uveitis possible

• Starts 2-4 weeks after the initial infection
• Articular symptoms typically appear last
• additive• oligoarticular• lower limbs most common
• Knee • Ankle• Foot joints • Occasionally
– Wrist, Elbow, Shoulder, SIE
asymetric, oligoarticular
• Chronic cases– Dactilitis– Entesopathy. tenosynovitis, plantar facitis,
achill tendinitis, bursit
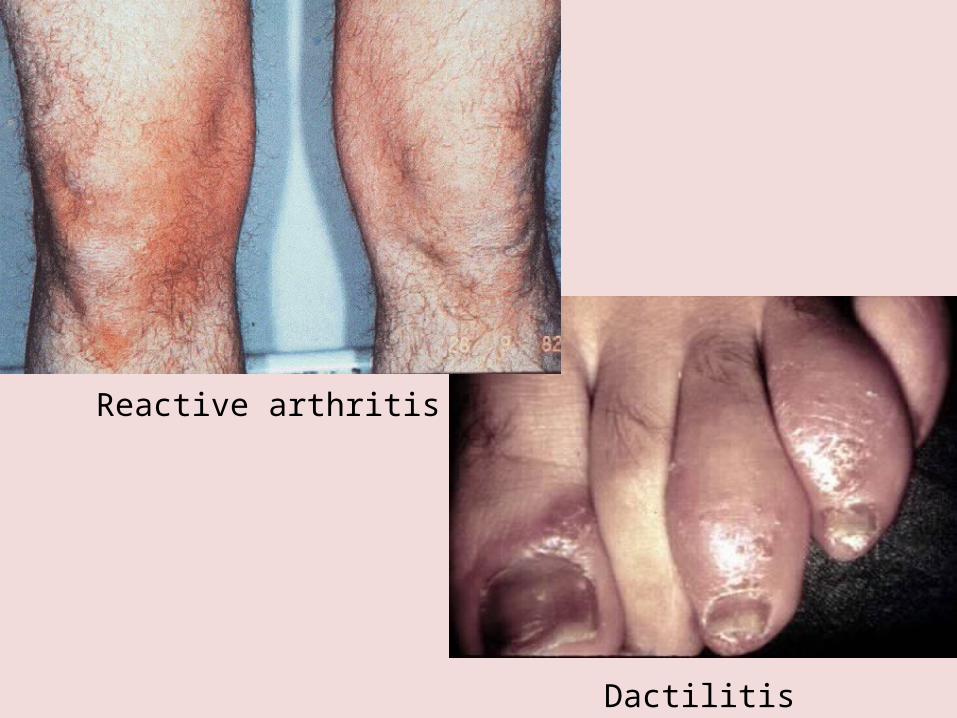
Dactilitis
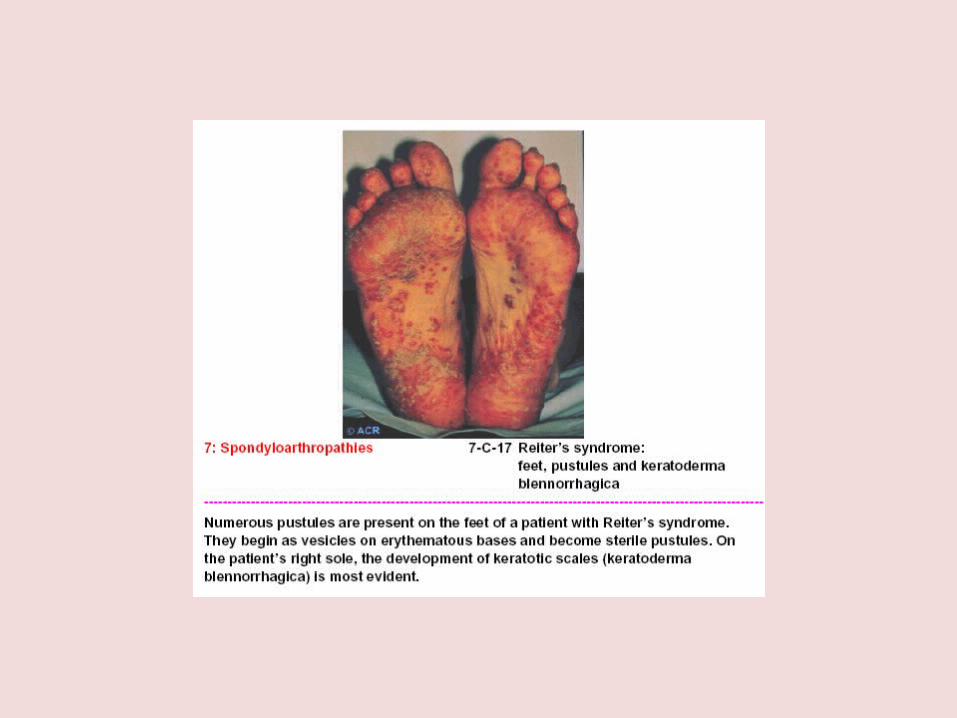
Reactive arthritis
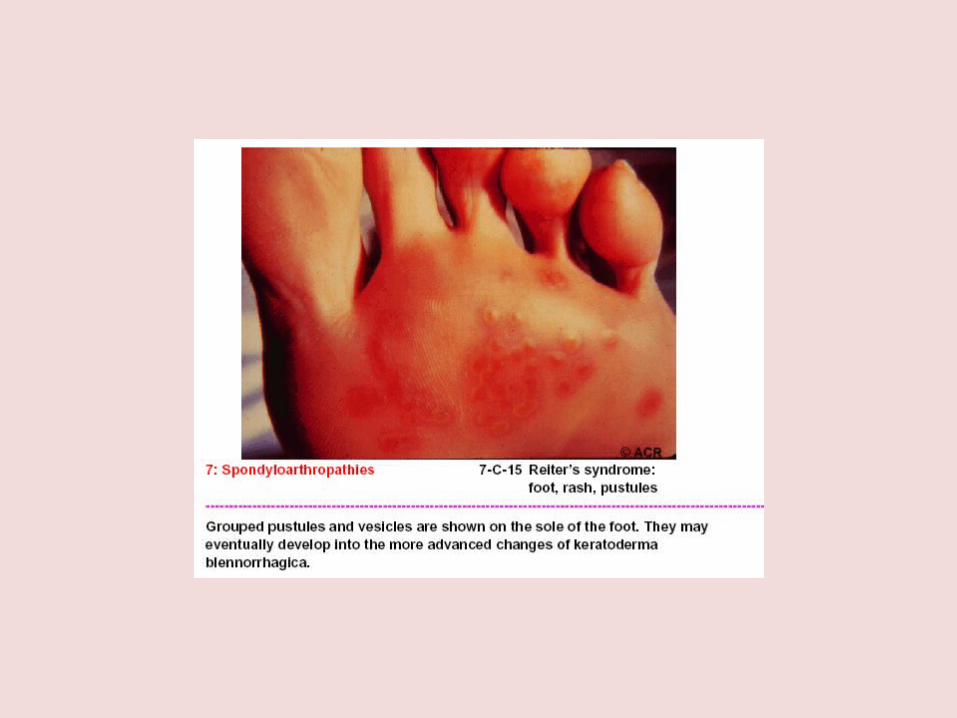
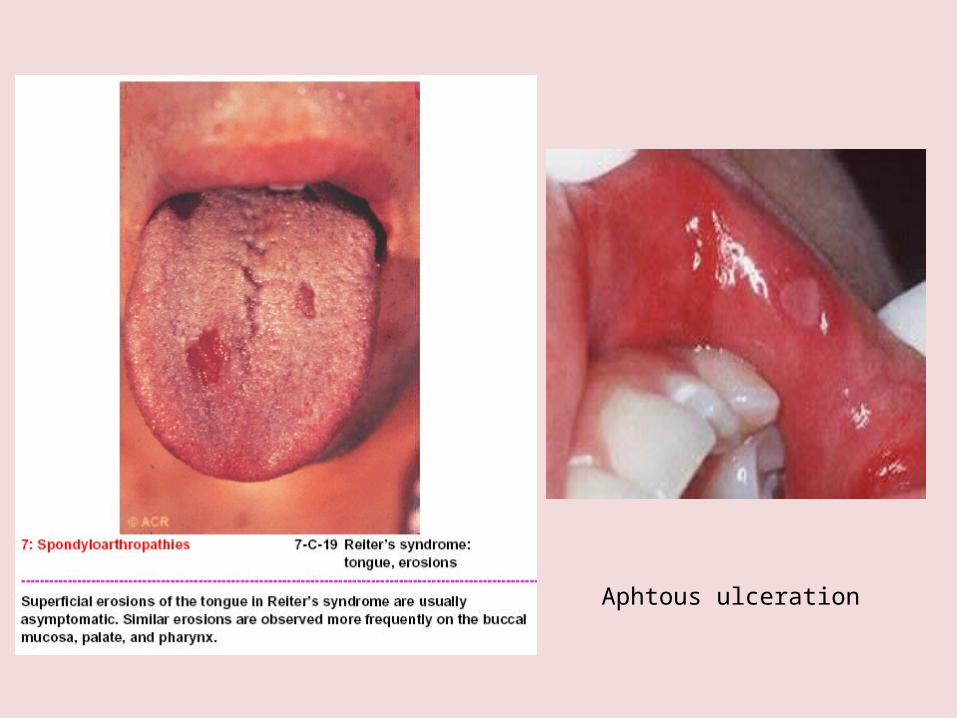
Aphtous ulceration

Erithema nodosum
• Clinical course– Normally limited course running 3-12 months– 15% with prolonged relapsing arthritis
• ? Relapse• ?Reinfection
– Ankylosing Spondylitis in 10% of cases
• Laboratory findings– Normochromic, normocytic anemia– Leukocytosis– Acute phase reactants:
• ESR • C-reactive Protein
– Patients with genitourinary symptoms should be tested for infection with C trachomatis
• Treatment: Antibiotics?-chlamydia-tetracyclines Rest NSAIDs Methotrexate and sulphasalazine Intralesional and intraarticular
glucocorticoids Uveitis-glucocorticoids
Enteropathic ArthritisOr
SpA associated with inflammatory bowel disease
Arthropathy associated with IBD – (5-20%) Peripheral arthritis Axial involvement – sacroiliitis w/o
spondylitis HLA-B27 not implicated here
Acute, oligoarticular onset Predominantly lower extremities Non-deforming, self-limiting arthritis Association with active bowel symptoms
Periarticular features Enthesopathy Tendonitis
Extraarticular features Erytema nodosum Uveitis
NSAID Sulphasalazine Methotrexate
Biologic agents – Anti TNF therapy
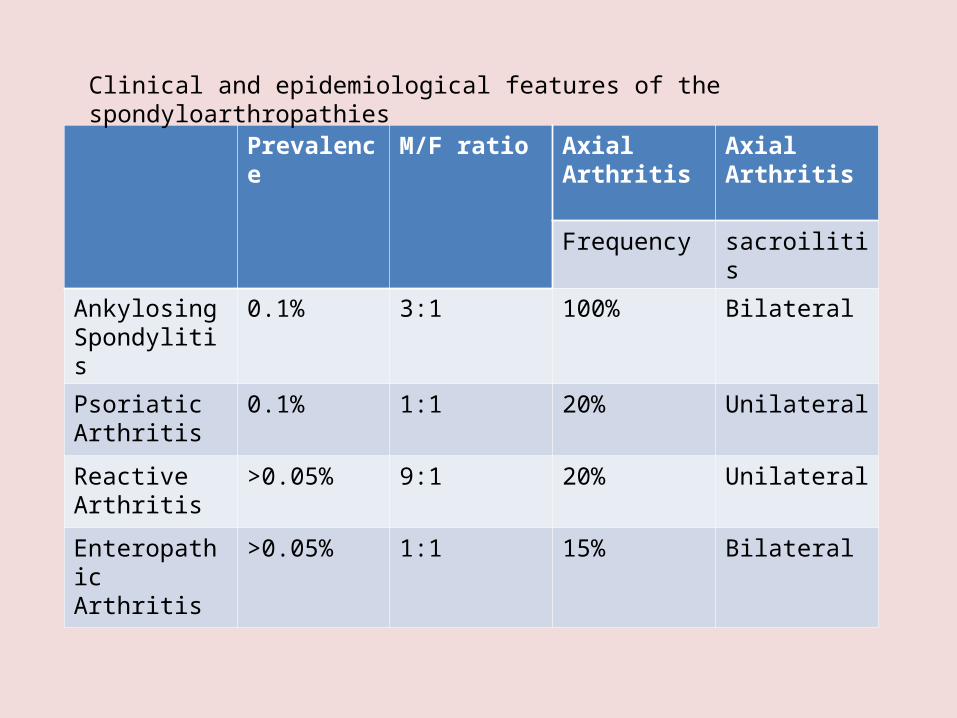
Prevalence M/F ratio Axial Arthritis Axial Arthritis
Frequency sacroilitis
Ankylosing Spondylitis
0.1% 3:1 100% Bilateral
Psoriatic Arthritis
0.1% 1:1 20% Unilateral
Reactive Arthritis
>0.05% 9:1 20% Unilateral
Enteropathic Arthritis
>0.05% 1:1 15% Bilateral
Clinical and epidemiological features of the spondyloarthropathies
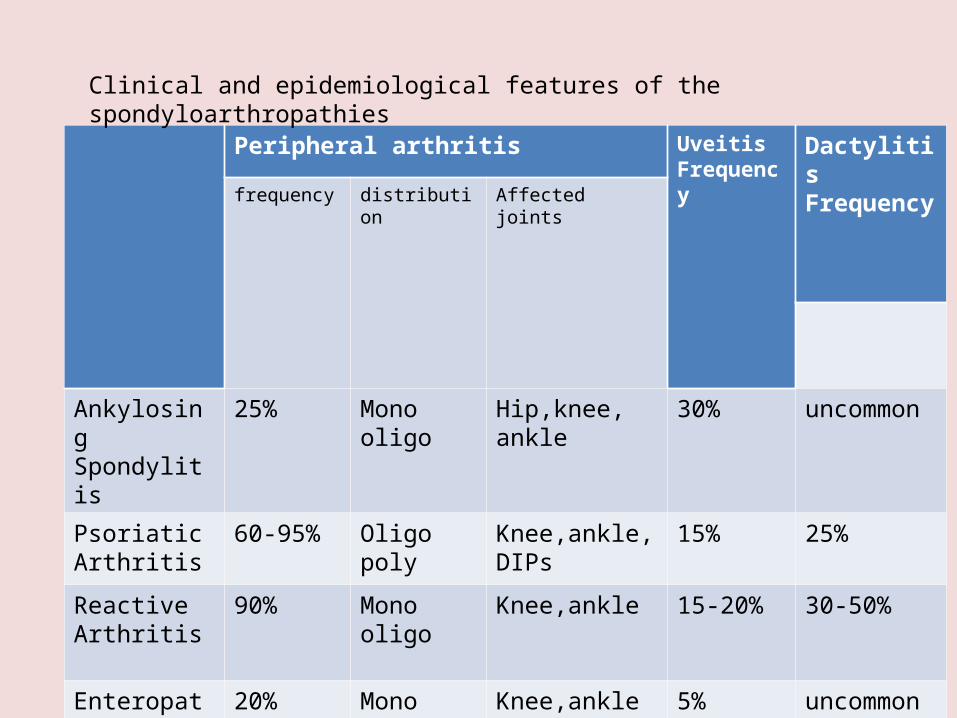
Peripheral arthritis Uveitis Frequency
Dactylitis Frequencyfrequency distribution Affected
joints
Ankylosing Spondylitis
25% Monooligo
Hip,knee,ankle
30% uncommon
Psoriatic Arthritis
60-95% Oligopoly
Knee,ankle,DIPs 15% 25%
Reactive Arthritis
90% Monooligo
Knee,ankle 15-20% 30-50%
Enteropathic Arthritis
20% Monooligo
Knee,ankle 5% uncommon
Clinical and epidemiological features of the spondyloarthropathies