seronegative arthritis 111226134709-phpapp02
TRANSCRIPT

(Seronegative arthritis)
DR. PRUTHVIRAJ NISTANE
Post-Graduate student
Deptt. Of Orthopaedics,
Govt. Medical College and
Rajindra Hospital, Patiala
Objectives
Gain a basic understanding of the Spondylo-
Arthritis
Learn specific Characteristics of SpA
Differentiate SpA from other chronic Arthritis
( RA, OA )
Become familiar with articular and extra-articular
manifestations of SpA
Understand the current treatment paradigm and
medications used


Introduction
Are a diverse group of chronic, systemic inflammatory conditions linked by distinctive clinical, radiographic, and genetic features
Refers to inflammatory changes involving the spine and the spinal joints.
subtypes often overlap
may be considered one heterogeneous and phenotypically diverse disease that has the potential to evolve into AS.

Introduction
Absence of Rheumatoid Factor or other
autoantibody serologic abnormalities
includes
○Ankylosing Spondylitis
○Psoriatic Arthritis
○Reactive Arthritis
○Enteropathic Arthritis-IBD
○Undifferentiated Spondyloarthropathy

ESSG (Europian SpA Study
Group)Criteria for diagnosis of
spondyloarthropathy Inflammatory spinal pain or synovitis (asymmetric or
predominantly in lower limbs) plus more than 1 of the
following:
Positive family history
Psoriasis
Inflammatory bowel disease
Urethritis, cervicitis, or acute diarrhea < 1 mo. before arthritis
Buttock pain alternating between right and left gluteal areas
Enthesities
Sacroiliitis
Sensitivity 78.4% and specificity 89.6%
RA SpA
• UE>LE
• Often polyarticular
• Sacroiliitis absent
• RF usually pos
• No HLA-B27 assoc
• Sicca, scleritis
• Nodules
• LE>UE
• Oligoarticular
• Sacroiliitis often +
• RF neg
• + HLA-B27 assoc
• Anterior uveitis
• Mucocutaneous

Confusion
Can often see peripheral joint symptoms in
the absence of spinal symptoms

Pathology immune
The pathology of spondyloarthropathies is
very different from that of RA. In RA, it is
the synovitis that plays the major role, and
the synovitis leads to bony erosions.
In spondyloarthritis there is some synovitis,
but it's the enthesitis that is the major
problem, especially in the axial disease.

Pathology
Osteitis follows
reactive bone sclerosis and
bone absorption, but then
more bone remodeling sets in
and it goes on to result in
new bone formation that can
result in ankylosis


Pathology In RA, the cytokines lead to excessive
osteoclastic activity resulting in bone erosions,
In spondyloarthritis, the cytokines that are
playing a major role result in osteoblastic activity
Gradual bony bridging follows after being
initiated by the inflammation


Hallmarks
Inflammatory back pain (IBP)
Enthesitis - inflammation at sites where
tendons, ligaments, and joint capsule
fibers attach to bone, with a strong
tendency to produce fibrosis and
calcifications.

Inflammatory Back Pain
Worse in the late night and early morning
Pain interferes with sleep to the point that the
patient gets up to walk in the middle of the night
The discomfort can be characterized by
alternating buttock pain.
prolonged morning stiffness of greater than 30
minutes.

Inflammatory Back Pain
Exercise alleviates the pain rest makes it
worse.
Affects younger patients
Peaking during the mid-20s
onset before the age of 40
Spondyloarthropathies
IBP persists for at least 3 months.
detrimental effects on quality of life
increased disability, and morbidity --
equal, and in some cases
exceeding, that seen in RA

Spondyloarthropathies
Also associated with osteoporosis and low bone
mineral density
Ectopic bone formation occurs within the inflamed
vertebral enthesis
Bone resorption, (increased osteoclast activity),
occurs at an unregulated rate within the vertebra
and promotes weakening of the spinal column.

Clinical course
The spine in the patient with AS fuses through:
ligamentous ossification and
syndesmophytosis,
Rigid hyperkyphotic deformity develops.
Biomechanically, the fused spine acts as a long
bone incapable of appropriately dissipating the
energy of a traumatic event.

Spondyloarthropathies
Altered spinal biomechanics
Combined with the brittle quality of the
osteoporotic bone
Increase susceptibility to vertebral column
factures, and Spinal Cord injury, even after minor,
often trivial, trauma
Significantly impaired mobility and peripheral joint
arthritis

Sagittal reformatted CT scan showing a highly displaced
thoracic fracture. Asterisk indicates apposition of the
caudal fracture fragment on the thoracic aorta

Extra-articular
manifestations psoriasis,
anterior uveitis,
IBD,
as well as rarer cardiac, renal, and
pulmonary manifestations
a wide range of clinical manifestations.

Ocular Manifestations
Uveitis is one of the most common
occurring in 25% to 40% of patients.
there appears to be no correlation
between the course of inflammatory
eye disease and that of the arthritis.

Ocular Manifestations
Presents as acute unilateral pain and photophobia
Blurring of vision may also occur.
Cataracts
Glaucoma
Increased intraocular pressure
Posterior synechiae
Conjuctivities

Cutaneous Manifestations
Plaque psoriasis
Characterized by scaly,
erythematous, hyperkeratotic lesions
most common form of psoriasis and
is an important component of
diagnosing PsA.

Cutaneous Manifestations
assessment of less
conspicuous areas
including
gluteal cleft
scalp
scalp line
groin
posterior
auricular regions
should be performed.

Nail Changes
Diffuse and numerous nail pitting (plate
depressions)
Onicholysis (separation of the nail from
underlying nail bed)
Crumbling of the nail plate can be observed in
both psoriasis and PsA.
The extent of nail involvement parallels both
skin and joint disease

Nail Pitting

Onicholysis toe nails

Crumbling nail/DIP joint involvement
Other Extra- articular Manifestations
Apical pulmonary fibrosis : mostly asymptomatic
and typically observed in patients with substantial
disease duration
Renal disease : beyond analgesic and nonsteroidal
anti-inflammatory drug adverse effects
IgA nephropathy : proteinuria and hematuria
secondary amyloidosis : nephrotic syndrome
renal failure : a poor prognosis.

Gene association
Up to 70% of individuals suffering from
SpA carry the HLA-B27 gene
Strength of the association between HLA-
B27 and disease susceptibility varies
among SpA subtypes and ethnic groups

Associations with HLA-B27
Rheumatic diseases
Ankylosing spondylitis
Reiter’s syndrome/reactive arthritis
IBD related arthritis
Psoriatic arthritis
Normal Associations
Native Americans
Caucasians
Blacks
Degree of associations
>90%
>80%
~75%
~50%
13%
8%
4%

(MARIE-STRUMPELL DISEASE)
(BECHTEREW DISEASE)

A chronic, progressively inflammatory
disease of the spine and axial joints leading
to fibrous or bony ankylosis and deformity.
Systemic disease
Age – late adolescence or early childhood
(20-40 yrs)
Sex - 3:1 men: women
Affects about 6 in 10,000


Etiology
Not completely understood
Auto-immune
HLA-B27 : seen in 90 % patients
Autosomal inheritance with 70 %
penetration in males
some family history

Pathology Most striking feature - high degree of fibrosis,
bony ankylosis, and inflammation that focus
on bone, cartilage, and tendon-bone
junction.
Early lesions include subchondral
granulation tissue that erodes the joint and is
replaced gradually by FIBROCARTILAGE
and then OSSIFICATION.
Occurs in ligaments, fibrocartilage,disc and
capsular attachment sites to bone,called
“enthesitis” )

Gross Pathology
Start from SI joint
Destruction of cartilage and articular cortex
Fibrous or bony bridging
Para-articular – degeneration and
ossification in spine
ossification of anterior longitudinal ligaments
“bamboo spine”

HistoPathologyInflammatory cells in ligamentous and periosteal area
Subchondral marrow oedema
Pannus and new bone formation
Bony erosion
Fibrocartilagenous regeneration and ossification

Clinical features Insidious onset
Begins in the Sacroiliac Joints –
backache and morning stiffness
radiation
U/L or B/L
subsides with activity
returns after sitting in one position for long
period
Flexor spasm predominateforward
flexion
Progresses upwards and can involve the entire
spine

Axial joints(a poor prognostic )
Shoulders
Hips
Knees
Painful,swollon,
effusion,
muscle spasms
Flexion,
adduction
deformities
Peripheral jointsOsteoporosis
Blurring of margins
Joint space narrowing
Bony ankylosis
• Kyphosis
• Loss of spinal mobility
• Decreased chest expansion

Systemic features
Fatigue
Weight loss
Anorexia
Night sweats
Anemia

Diagnosis
Modified New York criteria (1984)
1. Limited lumbar motion
2. Low back pain for 3 months improved with exercise
not relieved by rest with morning stiffness
3. Reduced chest expansion
4. Definite radiological sacroilitis
Criteria 4 plus any of 1, 2, or 3.

Juvenile Ankylosing Spondylitis
Onset 8 to 14
Sex Ratio M:F 7 to 1
HLA-B27 91 %
Systemic symptoms rare
Polyarticular 97%
Prognosis good
Peripheral joint involvement is more to begin with; later axial symptoms supervene

Physical Examination
Loss of spinal mobility
Para spinal spasm

Spinal Involvement
Tenderness – SI joints
SI Compression Testing
Modified Schober Test
Potentially useful diagnostically
Limitation of motion

•Occiput to Wall distance
•Chest Expansion at the xiphisternum Normally > 5 cm Measurement is age and sex dependant Useful for following patients over time

Spinal Involvement
Finger Tip to Floor Distance
Measure fingertips to floor
Useful for following patients over time
Lateral Flexion
Ask the patient to flex laterally and
mark at the maximal extent of the
fingertips
Useful for following patients over time
Cervical Spine
Can result in Atlanto-Axial Instability

Radiological features
Within 3 to 6 months
SI joints – earliest
Patchy osteoporosis
Margins ill defined
Widened
Later subchondral sclerosis
Finally bridging and obliteration of joint


Sacroiliitis grading
0-normal
1-possible
2-minimal
3-moderate
4-ankylosing

The Spine
Sharp squaring of anterior portion of
vertebral body
Loss of concavity
Loss of lardosis
Subluxation of atlanto-axial joint
destruction of transverse
ligament and odontoid


•The reparative process formsvertical linear bone ossificationalong the outer fibers of the annulus fibrosus of the disc,called syndesmophyte formation.
•Ossification of anterior longitudinal ligament and annulus –“bamboo spine”
•Vertebral bodies tend to become osteoporotic (dorsal spine appears to become wedge-shaped)

MRI – Early changes

Progression and complications
Early stage(inflammatory)
Intermittent, low-grade fever
Fatigue
Anorexia
Sacroilitis (inflammation, pain, and tenderness in the sacroiliac joint)
Spasm of the vertebral muscles
Intermittent, low back pain (non-traumatic, insidious onset)
Rarely remission within 2 years


Advanced stage(ankylosis)
Constant low back pain
Ankylosis , decreased ROM
Muscle wasting in shoulder and pelvic girdle
Loss of lumbar lordosis
Marked dorsocervical kyphosis
Ultimately in 3 to 5 years – SI joints are
fused, spine , hips ankylosed in forward
flexion, single rounded immobile spinal curve
, residual motion in knees and shoulder.


Complications
Fractures - Stiff osteoporotic spine is prone to
fracture and minor trauma. Most common
site of fracture is the lower cervical spine.
Progressive myelopathy - develops from
cord compression leading to motor/sensory
disturbance.
Cauda equina syndrome – late complication
Initial deficit is loss of sensation on the
lower extremity

Spinal stenosis – rare ; Result of bony
overgrowth of the spinal ligament and
facet joint.Symptoms are pain and
numbness of the lower extremities
brought on by walking and relieved by
rest.
Subluxation of atlanto-axial joint -
chin-on-chest deformity
Reduced vital capacity

Associated symptoms
Aortitis
Aortic dilatation
Aortic regurgitation – scar tissue in aortic
valves
Conduction abnormalities
Apical pulmonary fibrobullous lesion
Iritis
Non-granulomatous anterior uveitis
Colitis

Laboratory Investigations
• Elevated ESR/CRP
HLA-B27 - found in 90-95% of patients
( 6% of general population)
• Synovial fluid – mononuclear leukocytes
CBC
Normochromic normocytic anemia
Reactive thrombocytosis
• Elevated serum IgA
• Increased ALP
• Decreased vital capacity

Differential diagnosis
Ankylosing form of RA
Other spondyloarthropathies
Other causes of LBA
Ochronosis
DISH

Treatment - Goals
Rehabilitation.
Initiated before the disease fuses the
vertebrae and involves other organ.
Directed toward maintaining function
and strength.

Conservative management
Corticosteroids – reduces inflammation
and relieves pain may overcome
deformity to some extent
NSAIDS - mainstay of treatment
Radiation – relieves muscle spasm
given with caution
Methotrexate
Sulfasalazine

Latest revolution
Anti TNF-α therapy
Infliximab
Etanercept
Rapid, profound and sustained response to
all aspects of disease
Serious complications
Very expensive

Posture and exercise Recumbence
Hyperextension , abduction
Deep breathing exercises
Traction to lower extremities to overcome
deformity
Surgical management To relieve from disabling deformities
Total hip replacement Neck osteotomy and head removed
piecemeal
Accurately identify acetabular margins
Over come flexion, stooping
Motion
Relieve pain
Restore upright posture
Prevent spinal osteotomy
90 % good results
Spinal osteotomyDone at L2-3 or L3-4 level
Wedge of posterior spinal
column excised and
straightening of spine done.
Multiple complications


Thank you

(Seronegative arthritis)
II
Moderated by - Dr. K. S. SandhuPresented by - Dr. Pruthviraj Nistane

“Recap”
Are a diverse group of chronic, systemic
inflammatory conditions linked by
distinctive clinical, radiographic, and
genetic features
Refers to inflammatory changes involving
the spine and the spinal joints.
subtypes often overlap


ESSG (Europian SpA Study
Group)Criteria for diagnosis of
spondyloarthropathy Inflammatory spinal pain or synovitis (asymmetric or
predominantly in lower limbs) plus more than 1 of the
following:
Positive family history
Psoriasis
Inflammatory bowel disease
Urethritis, cervicitis, or acute diarrhea < 1 mo. before arthritis
Buttock pain alternating between right and left gluteal areas
Enthesities
Sacroiliitis
Sensitivity 78.4% and specificity 89.6%

Hallmarks
Immune mediated enthesitis and other
changes
IBP
Extra-skeletal manifestations
Association with HLA – B27

ANKYLOSING
SPONDYLITIS PROTOTYPE
Most common
Crippling disease affecting young population
Inflammatory back pain
From sacro-ilitis to complete fusion on the spine
Large peripheral joints may be involved
Anti TNF agents have revolutionised treatment


(Reiter’s syndrome)

What is it ???
Acute non-purulent arthritis complicating
an infection elsewhere in body
Clinical syndrome triggered by specific
etiological agent in genetically susceptible
host
Infection – mostly enteric or urogenital

“Reactive”
viable micro-organisms do not enter the
joints and synovial fluid cultures are thus
negative.
There is no universal agreement about
the classification and diagnostic criteria
for reactive arthritis.

Reiter’s syndrome –old aponym for reactive
arthritis
clinical triad of arthritis, urethritis and
conjunctivitis.
Reactive arthritis belongs to the family of
spondyloarthropathies because they share
cardinal clinical features together.

Epidemiology
age - is 18–40 years
gender ratio in ReA following enteric infection is
nearly 1:1, whereas venereally acquired ReA
occurs mainly in men
60–85% of patients were found to be B27-
positive - its presence contributes to the
chronicity of the disease.

Triggering infections
• Reactive arthritis is an arthritis induced by one of
the following bacteria:
Urogenital:
• Chlamydia trachomatis
Enteric:• Shigella (S. flexneri has most often)
• Salmonella
• Yersinia
• Campylobacter
• At least presumptive evidence for a related
antecedent infection is a must

Form of post infection arthritis that share
same clinical features as SpA.
Whereas arthritis caused by or related to
other infections is termed “infection-
related/ associated arthritis”

Pathology• Synovial histology - is similar to that of other SpA
• Enthesitis - increased vascularity
Macrophage infiltration of fibro
cartilage
• Histopathology evidence of
inflammation has occasionally been noted in the colon
and ileum

PathogenesisBacterias
• produce lipopolysaccharide (LPS)
• capacity to attack mucosal surfaces,
• survive intracellularly
HLA-B27 - prolongs the intracellular survival
Trafficking of infected leukocytes from the site of primary infection to joints, where an innate and adaptive immune response to persistent bacterial antigens promote arthritis.
synovial T cells that specifically responded to antigens of the inciting organism were reported and characterized as predominantly CD4+ with a TH2 or T regulatory phenotype. More recent work has documented high levels of IL-17

confusion ????
• Antigens from these bacterias have
been shown to be present in the
synovium and/or synovial fluid
leukocytes
• So atleast in some cases,it may be
chronic form of infection rather than
solely reactive

Clinical picture
Usually there is a delay of 1-4 wks from
infection till start of arthritis
ranges from an isolated, transient
monarthritis or enthesitis to severe
multisystem disease
History suggestive of infection

Musculoskeletal symptoms
Peripheral
• Typically there is asymmetric additive, oligoarthritis,
mainly of Lower limbs.
• Most common are knees, ankles, subtalar , toe IP and
MTP joints.
• Quite painful, and tense joint effusions.
• Dactylitis, or "sausage digit " a diffuse swelling of a
solitary finger or toe, is a distinctive feature of
peripheral SpA


Axial
• Inflammatory low back pain
o Acute sacroiliitis
o insertional inflammation,
o muscle spasm
o arthritis in intervertebral joints.
• Enthesitis
• Plantar fasciitis
• Achilles tendinitis

Extra-articular features in ReA
Mucocutaneous
• Keratoderma Blennorrhagica (20%)
palms and soles
• Circinate balantitis (30%)
• Painless oral ulcers (25%)
• Erythema nodosum
Nail changes
• onycholysis,
• distal yellowish discoloration
• heaped-up hyperkeratosis.
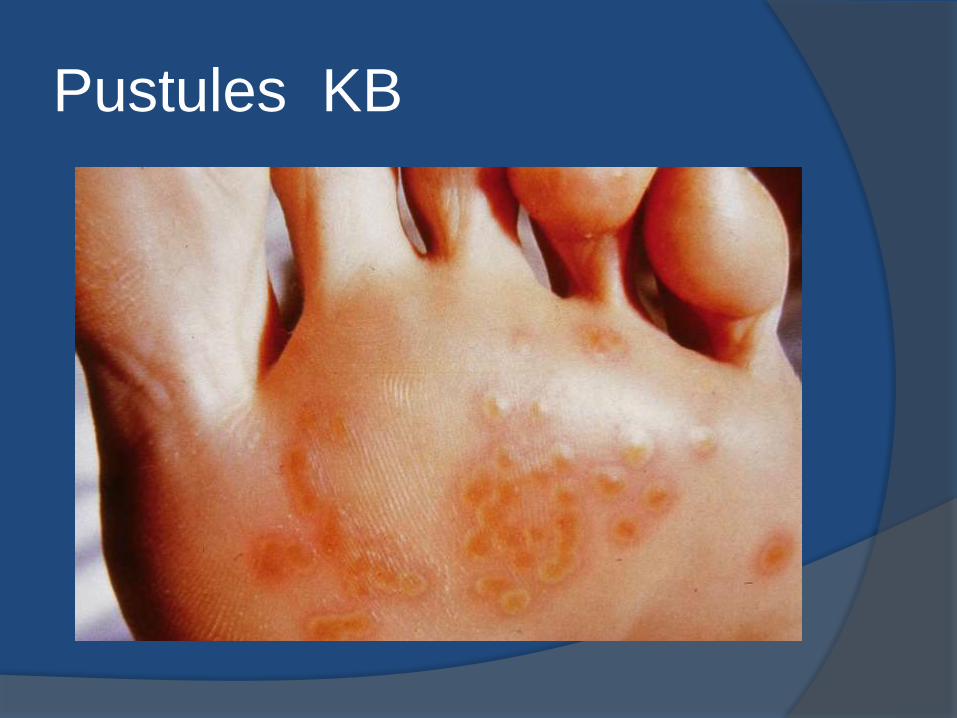
Pustules KB

Keratoderma
Blenorrhagicum

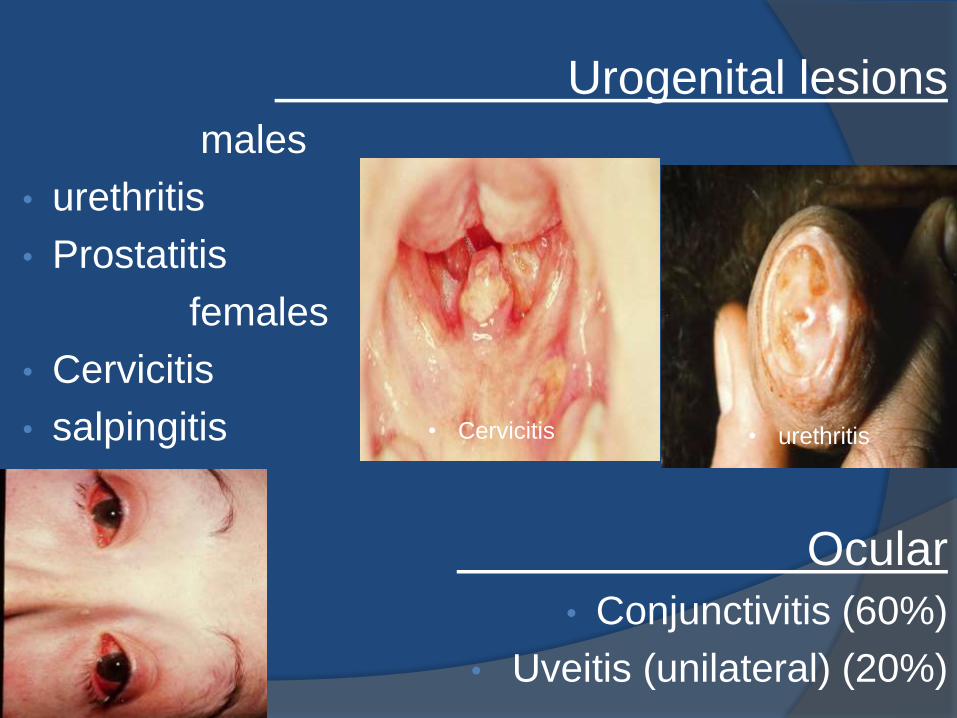
Urogenital lesions
males
• urethritis
• Prostatitis
females
• Cervicitis
• salpingitis
Ocular
• Conjunctivitis (60%)
• Uveitis (unilateral) (20%)
• urethritis• Cervicitis

Constitutional symptoms
Fatigue
Malaise
Fever
Weight loss
Cardiac conduction defects
Aortic insufficiency
Central or peripheral nervous system lesions
Pleuropulmonary infiltrates.
Diagnostic Criteria• Seronegative asymmetric arthropathy
and at least 1 of the following:
• Urethritis or cervicitis
• Diarrhea
• Inflammatory eye disease
• Mucocutaneous disease
• Balanitis, oral ulceration or keratoderma
• Other spondyloarthropathies and rheumatic disease
excluded

Prognosis
Persists 3–5 months, but courses up to 1 year
can occur.
Chronic joint symptoms persist in about 15% of
patients.
Recurrences of the acute syndrome are also
common
Low-back pain, sacroiliitis, and frank AS are
also common sequelae

Laboratory investigations
Demonsration of the urogenital tract or bowel infections
During the acute phase:
• urine culture,
• genital swabs,
• stool culture
After arthritis developed:
• Serodiagnosis to detect antibodies
• PCR

inflammatory arthritis:
• ↑ESR, CRP
• leucocytosis
• Synovial fluid analysis and culture
HLA B27 (especially in chronic arthritis)-85 %
Imaging :
MRI, CT, Plane x-ray for detection of
• Sacroilitis – asymmetrical
• Enthesopathy
• Juxtaarticular osteoporosis
• Marginal erosions
• Loss of joint space
• Spondylitis – can begin anywhere in lumbar spine
• Reactive new bone formation
Laboratory investigations

Differintial diagnosis
Disseminated gonococcal
disease
psoriatic arthropathy
Other spondyloarthropathies

Treatment
Eradicate triggering infection (antibiotics)
Treat extra-articular manifestations:
Topical steroid
Uveitis - topical steroids, mydriatics
Skin lesions ordinarily require only
symptomatic treatment

1. NSAIDs: in full doses
Indomethacin, 75–150 mg/d in divided doses is the initial
treatment of choice
2. Local steroids injections
in mono/oligo arthritis, enthesopathy
3.Immuno-suppresants
• Sulfasalazine
• Azathioprine
• methotrexate
4. Biologics: anti-TNF- α
in resistant disease
Treatment of arthritis:


PSORIATIC
ARTHRITIS

What is it ???
Psoriatic arthritis (PsA) refers to an
inflammatory arthritis that
characteristically occurs in individuals with
psoriasis.

Who Gets Psoriatic
Arthritis? Age of onset - 30-50 years
1-3% of the population has psoriasis
5 – 10 % of people with psoriasis get psoriatic
arthritis
Family studies suggest a 50-fold increase in the risk
of psoriatic arthritis in 1st degree relatives
HLA-Cw6 gene is directly associated with psoriasis
HLA-B27 is associated with psoriatic spondylitis

Pathology
shares pathogenic mechanisms with psoriasis
immune-mediated
Infiltration with T cells, B cells, macrophages,
and NK receptor–expressing cells
Resembles that of RA - less hyperplasia and
cellularity than in RA, & greater vascularity

Pathology synovial overexpression of proinflammatory
cytokines
• Interleukin 2
• Interferon
• TNF
marked increase in osteoclastic precursors in
peripheral blood and upregulation of receptor
activator of nuclear factor ligand (RANKL) in the
synovial lining layer.

Clinical Features
Psoriasis present before the onset of joint disease
(70%)
Psoriasis comes with the arthritis (15%)
Psoriasis comes after the arthritis (15%)

Confusion
Psoriatic Arthritis is a heterogenous disease
which can present in a multitude of ways

Wright and Moll Classification
(1) Arthritis of the DIP joints; 15 %
(2) Asymmetric oligoarthritis; 30 %
(3) Symmetric polyarthritis similar to RA; 40 %
(4) Axial involvement (spine and sacroiliac joints);5%
(5) Arthritis mutilans, a highly destructive form of
disease5 %

Arthritis of the DIP joints

Arthritis of the DIP joints

Asymmetric oligoarthritis

Asymmetric oligoarthritis

Symmetric polyarthritis

Axial involvement

Arthritis Mutilans

Arthritis Mutilans

Presentation Typical presentation is a peripheral inflammatory joint
disease – usually a mono or oligo arthritis
Knees
Wrists
May occasionally present with polyarthritis
Initial presentation of inflammatory spinal disease is
rare

Progression -- later stages
Sacroiliac Involvement
Sacroiliitis in 1/3 of patients
Usually asymmetric (unilateral)
May be asymptomatic
Spinal Involvement
May affect any part of the spine in a random fashion
Different from ankylosing spondylitis

Other features Mucocutaneous Involvement
Psoriatic skin lesions
Psoriatic Nail lesions
Entheseal Involvement
Tenosynovities
Dactylitis ->30 %• Shortening of digits because of underlying osteolysis
• Both fibrous and bony ankylosis of small joints
• Ankylosis of one or more PIP joint
Ocular Involvement - uveitis - bilateral, chronic, and/or posterior,
- conjuctivitis
Aortic valve insufficiency

Dactylitis


Nail changes Occur in 90% of patients with PsA
Pitting
Horizontal ridging
Onycholysis
Yellowish discoloration of the nail margins
Dystrophic hyperkeratosis
Combinations

Psoriasis/Nail changes/arthritis DIPs
and Sausage deformity

Classification of Psoriatic
Arthritis (CASPAR) criteria; 2006
A patient must have inflammatory articular disease (joint,
spine, or entheseal) with 3 points from any of the following
five categories:
1) Evidence of current psoriasis,or history of it
2) Typical psoriatic nail dystrophy
3) A negative test result for rheumatoid factor
4) Either current dactylitisf or a history of it
5) Radiographic evidence of juxtaarticular new bone formation in
the hand or foot

Physical Examination
Skin and Nail Involvement
Peripheral Joint Involvement
Peripheral Entheseal Involvement
Spinal Involvement
Schober Test
Occiput to Wall Distance
Spine ROM
Finger tip to floor distance
Lateral flexion

assessment of less
conspicuous areas
including
gluteal cleft
scalp
scalp line
groin
posterior
auricular regions
should be performed.

Peripheral Joint Involvement
Inflammatory Joint Count
Number of Joints Involved
○ Prognostic Importance
○ Therapeutic Importance
Pattern of Joints Involved
○ Diagnostic Importance
Evidence of Damage
Dactylitis

Laboratory investigations
ESR and CRP elevated
Uric acid may be elevated in the
presence of extensive psoriasis
HLA-B27 is found in 50–70% of patients
with axial disease, but 20% in patients
with only peripheral joint involvement.

Radiographic featuresSmall joints involvement
classic "pencil-in-cup" deformity
marginal erosions
adjacent bony proliferation(whiskering)
small-joint ankylosis
osteolysis of phalangeal and metacarpal bone
telescoping of digits
Periostitis
proliferative new bone at sites of enthesitis.

Fusion
Pencil in Cup
deformity
•Subchondral bone resorption of
the distal interphalangeal joint of
the thumb and middle fingers
has resulted in the "pencil-in-
cup" appearance.
•A flexion deformity of the distal
interphalangeal joint of the small
finger is present
•corresponding joint of the ring
finger has fused.

Radiology

Axial involvement Asymmetric sacroiliitis
Syndesmophytes
Fluffy hyperperiostosis on anterior vertebral bodies
Severe cervical spine involvement, with a
tendency to atlantoaxial subluxation
Sparing of the thoracolumbar spine
paravertebral ossification

Prognosis
Erosive disease develops in the majority
Progressive disease with deformity and disability
is common
Mortality was found to be significantly increased
compared with the general population
The psoriasis and associated arthropathy seen
with HIV infection both tend to be severe and can
occur in populations with very little psoriasis

Indicators of Bad
Prognosis Younger age at onset
Presence of certain HLA antigens:
o HLA-B27 correlates with spondylitic involvement
o HLA-DR3, DR4 correlates with erosive disease
Extensive skin involvement
Polyarticular involvement
Lack of clinical response to NSAIDs
Association with HIV infection

Differntial diagnosis
Gout
Inflammatory Osteoarthritis
Multicentric reticulohistiocutosis
Other forms of SpA

How to Tell the Difference

Treatment coordinated therapy is directed at both the skin and
joints
anti-TNFagents - revolution• Etanercept
• Infliximab
• Adalimumab
• Golimumab.
Methotrexate
Sulfasalazine
leflunomide
PUVA
7 % of patients with PsA required musculoskeletal surgery



A relationship between arthritis and IBD
Ulcerative colitis (UC) as well as
Crohn's disease (CD)
prevalence of IBD is 0.05–0.1%,
AS was diagnosed in 1–10%, and peripheral
arthritis in 10–50% of patients with IBD
one-third to two-thirds of patients with AS have
subclinical intestinal inflammation

tendency to familial aggregation, more so for
CD
HLA-B27 - 70% of patients with IBD and AS
-15% of patients with IBD and
peripheral arthritis
alleles of the NOD2/CARD15 gene in SpA
patients with chronic inflammatory gut lesions

Pathology
Similar to other spondyloarthritides
1. Enthesiopathy (7%)
2. Spondylitis (2%)
3. Peripheral arthritis (10%)
Pathogenesis
The specific pathogenic mechanisms are
poorly understood
Immune-mediated
Trafficking of leukocytes between the gut and
the joint
Mucosal leukocytes from IBD patients have
been shown to bind avidly to synovial
vasculature

Clinical Features
AS - clinically indistinguishable from idiopathic AS
course independent of the bowel disease
peripheral arthritis - includes acute self-limited
attacks of oligoarthritis (4-6 weeks) of LL
chronic and symmetric polyarticular arthritis
course parallel to disease
Enthesitis , arthralgias or fibromyalgia symptoms.

Extraintestinal
manifestations
Uveitis
Pyoderma gangrenosum
Erythema nodosum
Finger clubbing

In IBD-associated SpA, erythema nodosum can be
observed in Crohn's disease

Laboratory Findings
inflammatory and metabolic
manifestations of IBD
Joint fluid is usually at least mildly
inflammatory
30–70% carry the HLA-B27 gene,

Radiographic
Findings axial skeleton are the same as in
uncomplicated AS.
Erosions are uncommon in peripheral
arthritis but may occur, particularly in the
metatarsophalangeal joints.
Isolated destructive hip disease has
been described.

Differential diagnosis(Diarrhea and arthritis)
Reactive arthritis
Celiac disease
Blind loop syndromes
Whipple's disease

Treatmentanti-TNF agents
• Infliximab
• adalimumab
Other treatment for IBD
sulfasalazine and related drugs,
systemic glucocorticoids
immunosuppressive drugs
usually of benefit for associated peripheral arthritis.



Approximately one-half of the patients with
undifferentiated SpA are HLA-B27-positive
often eventual progression to classical AS

In juvenile-onset SpA - begins between ages 7 and 16
o most commonly in boys (60–80%)
o an asymmetric, predominantly lower-extremity
oligoarthritis and enthesitis without extraarticular
Features
The prevalence of B27 in this condition, which has
been termed the seronegative enthesopathy and
arthropathy (SEA) syndrome, is approximately 80%.

management
anti-TNF- therapy
Newer - doxycycline and rifampin



SYNOVITIS
ACNE -CONGLOBATA,
FULMINANS,
HIDRAENITIS SUPURATIVA
PUSTULOSIS -PALMO PLANTAR
HYPEROSTOSIS - STERNO-CLAVICULAR
SPINAL
OSTEOMIELITIS - STERIL MULTIFOCAL
RECURRENT

In some cases, bacteria, most often
Propionibacterium acnes, have been cultured
ESR is usually elevated, sometimes
dramatically
Inflammatory bowel disease was coexistent in
8%
B27 is not associated

Management
High-dose NSAIDs
Pamidronate or other
bisphosphonates
Anti-TNF therapy



Rare chronic bacterial infection, mostly
of middle-aged white men, caused by
Tropheryma whipplei
75% of affected individuals develop an
oligo- or polyarthritis.
Joint manifestations usually precede
other symptoms of the disease by 5
years or more
Large and small peripheral joints and
sacroiliac joints may be involved.
abrupt in onset, migratory, usually lasts
hours to a few days

systemic disease
PCR amplification
penicillin (or ceftriaxone) and Streptomycin for
2 weeks
followed by
trimethoprim-sulfamethoxazole for 1–2 years



SPONDYLOARTHOPATHIES
A summary Absence of rheumatoid factor
Involvement of sacroiliac and spinal joints
Peripheral arthritis (predominantly lower limb)
Enthesopathy
Familial clustering
Increased incidence of HLA-B27
Common spectrum of extra-articular features
(predominantly muco-cultaneous)
Anti TNF agents are the latest revolution !
