september 1, 2016 company presentation - hansa...
TRANSCRIPT

1
September 1, 2016 Company presentation
Forward-looking statements This presentation may contain certain forward-looking statements and forecasts based on uncertainty, since they relate to
events and depend on circumstances that will occur in the future and which, by their nature, will have an impact on Hansa
Medical’s business, financial condition and results of operations. The terms “anticipates”, “assumes”, “believes”, “can”,
“could”, “estimates”, “expects”, “forecasts”, “intends”, “may”, “might”, “plans”, “should”, “projects”, “will”, “would” or, in
each case, their negative, or other variations or comparable terminology are used to identify forward-looking statement.
There are a number of factors that could cause actual results and developments to differ materially from those expressed
or implied in a forward-looking statement or affect the extent to which a particular projection is realized. Factors that could
cause these differences include, but are not limited to, implementation of Hansa Medical’s strategy and its ability to further
grow, risks associated with the development and/or approval of Hansa Medical’s products candidates, ongoing clinical
trials and expected trial results, the ability to commercialize IdeS, technology changes and new products in Hansa
Medical’s potential market and industry, the ability to develop new products and enhance existing products, the impact of
competition, changes in general economy and industry conditions and legislative, regulatory and political factors.
No assurance can be given that such expectations will prove to have been correct. Hansa Medical disclaims any obligation
to update or revise any forward-looking statements, whether as a result of new information, future events or otherwise.
2

3
› Biopharma company founded 2007
› Develops immunomodulatory enzymes for treatment of rare and severe immunological diseases
› 20+ employees in Lund, Sweden
› Listed at Nasdaq Stockholm
› Significant collaborations:
Hansa Medical snapshot
· Cedars-Sinai Medical Center
· NYU Langone Medical Center
· Johns Hopkins Medicine
· Lund University
· Uppsala University Hospital
· Karolinska University Hospital
› IgG antibody modulating enzymes – Lead candidate IdeS in Phase II
› Strong IP protection and orphan drug designation
Proprietary technology
Immediate antibody inactivation to patients in acute need
4
Clinical proof-of-concept in 30+ patients › Phase I and Phase II finalized
› HighdeS multicenter study initiated – Potential BLA filing 2018
› Initial focus on turning non-transplantable patients transplantable
› Unmet medical need in acute rare autoimmune diseases
Significant unmet need in many rare acute diseases
› Potentially a 1BUSD market for lead product
› Current market cap: 275 MUSD
Substantial value creation potential
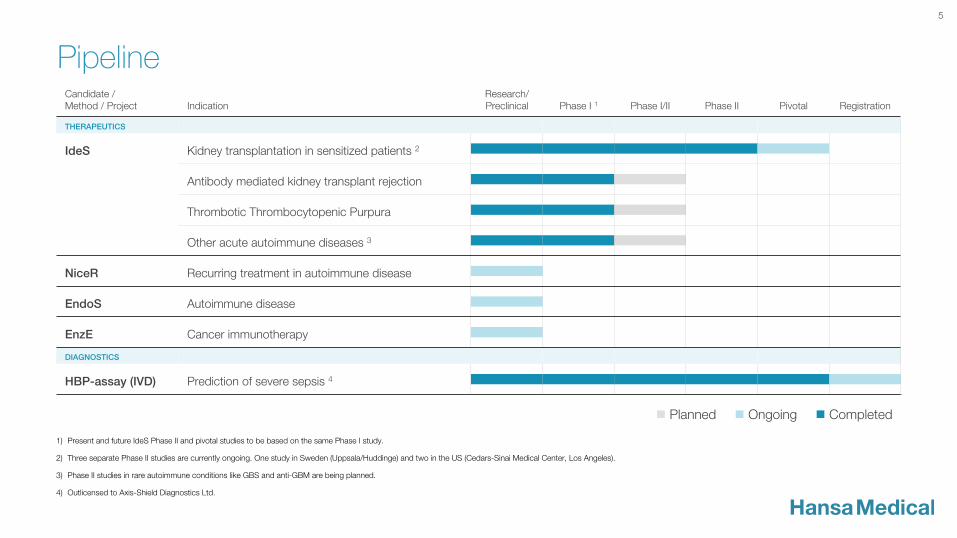
Pipeline
5
Candidate / Method / Project Indication
Research/ Preclinical Phase I 1 Phase I/II Phase II Pivotal Registration
THERAPEUTICS
IdeS Kidney transplantation in sensitized patients 2
Antibody mediated kidney transplant rejection
Thrombotic Thrombocytopenic Purpura
Other acute autoimmune diseases 3
NiceR Recurring treatment in autoimmune disease
EndoS Autoimmune disease
EnzE Cancer immunotherapy
DIAGNOSTICS
HBP-assay (IVD) Prediction of severe sepsis 4
n Planned n Ongoing n Completed
1) Present and future IdeS Phase II and pivotal studies to be based on the same Phase I study.
2) Three separate Phase II studies are currently ongoing. One study in Sweden (Uppsala/Huddinge) and two in the US (Cedars-Sinai Medical Center, Los Angeles).
3) Phase II studies in rare autoimmune conditions like GBS and anti-GBM are being planned.
4) Outlicensed to Axis-Shield Diagnostics Ltd.
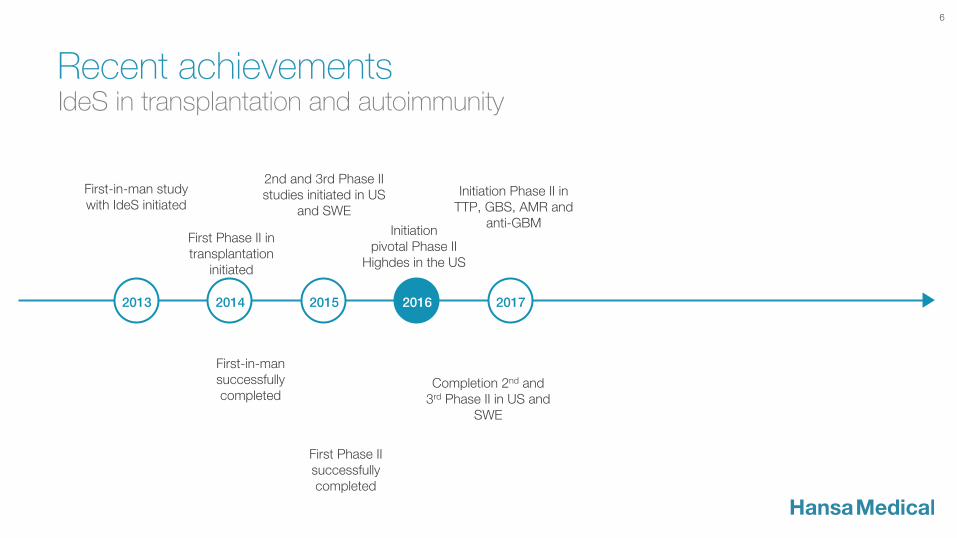
First Phase II in transplantation
initiated
First-in-man study with IdeS initiated
2nd and 3rd Phase II studies initiated in US
and SWE
Initiation pivotal Phase II
Highdes in the US
6
Recent achievements
Initiation Phase II in TTP, GBS, AMR and
anti-GBM
IdeS in transplantation and autoimmunity
2014 2016 2015 2017 2013
Completion 2nd and 3rd Phase II in US and
SWE
First Phase II successfully completed
First-in-man successfully completed
IdeS
8
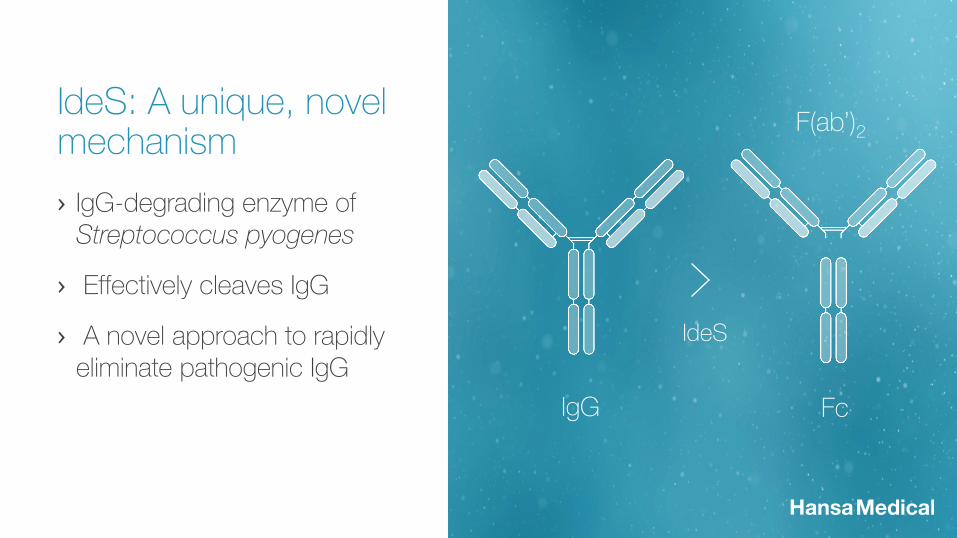
IgG Fc
F(ab’)2
IdeS
› IgG-degrading enzyme of Streptococcus pyogenes
› Effectively cleaves IgG
› A novel approach to rapidly eliminate pathogenic IgG
IdeS: A unique, novel mechanism
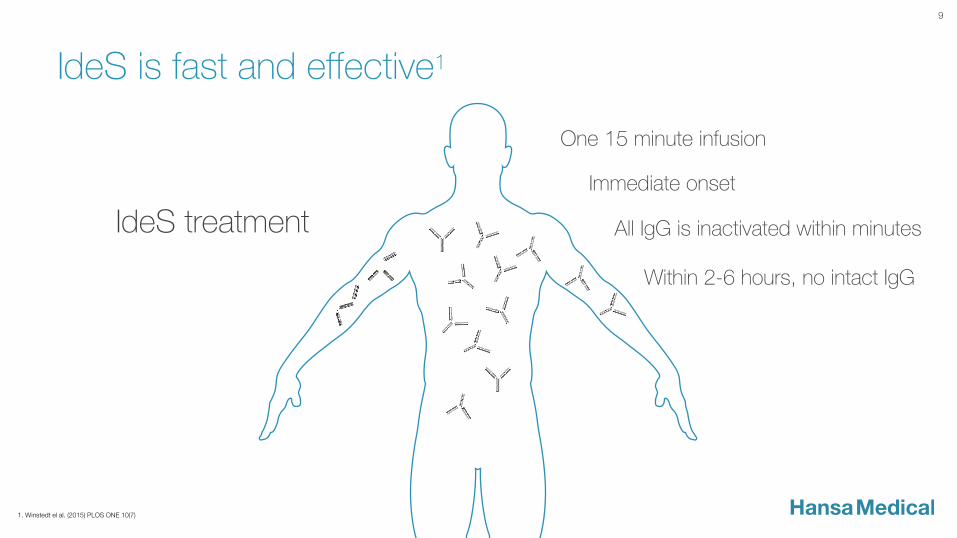
IdeS is fast and effective1
IdeS treatment
Immediate onset
All IgG is inactivated within minutes
One 15 minute infusion
Within 2-6 hours, no intact IgG
9
1. Winstedt el al. (2015) PLOS ONE 10(7)
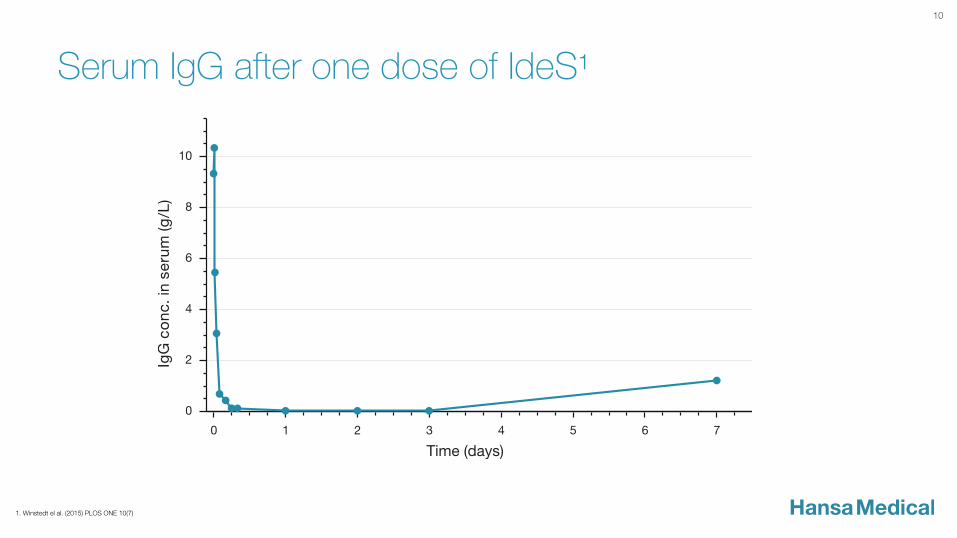
Serum IgG after one dose of IdeS1
10
1. Winstedt el al. (2015) PLOS ONE 10(7)
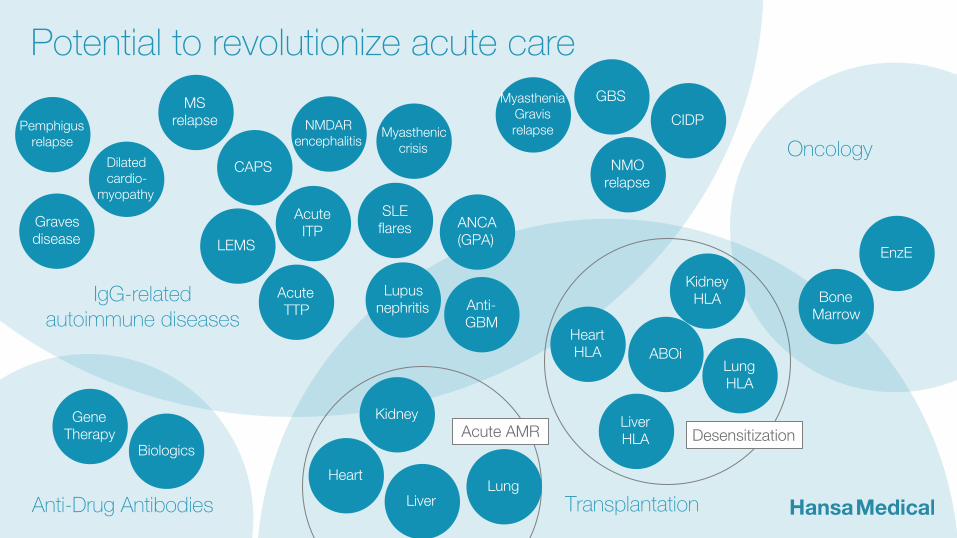
Gene Therapy
Biologics
Anti-Drug Antibodies
Myasthenia Gravis relapse
MS relapse
Acute ITP
Myasthenic crisis
Dilated cardio-
myopathy
Pemphigus relapse
CIDP
GBS
SLE flares Graves
disease
NMO relapse
NMDAR encephalitis
LEMS
CAPS
Acute TTP
IgG-related autoimmune diseases
Lupus nephritis Anti-
GBM
ANCA (GPA)
Heart HLA
Liver HLA
Kidney HLA
ABOi
Heart
Liver
Kidney
Transplantation
Desensitization Acute AMR
Potential to revolutionize acute care
Bone Marrow
EnzE
Oncology
Lung
Lung HLA
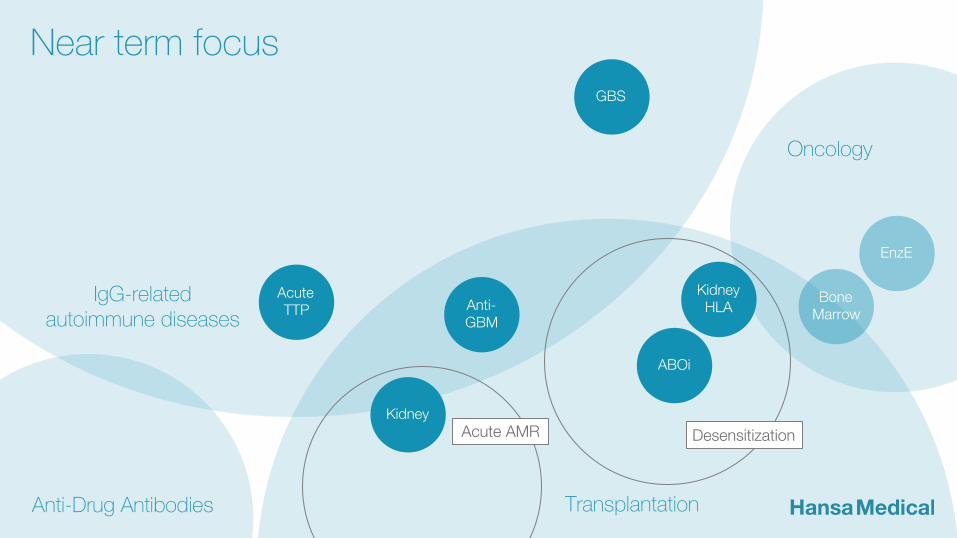
Anti-Drug Antibodies
GBS
Acute TTP
IgG-related autoimmune diseases
Anti- GBM
Kidney HLA
ABOi
Kidney
Transplantation
Desensitization Acute AMR
Bone Marrow
Oncology
Near term focus
EnzE
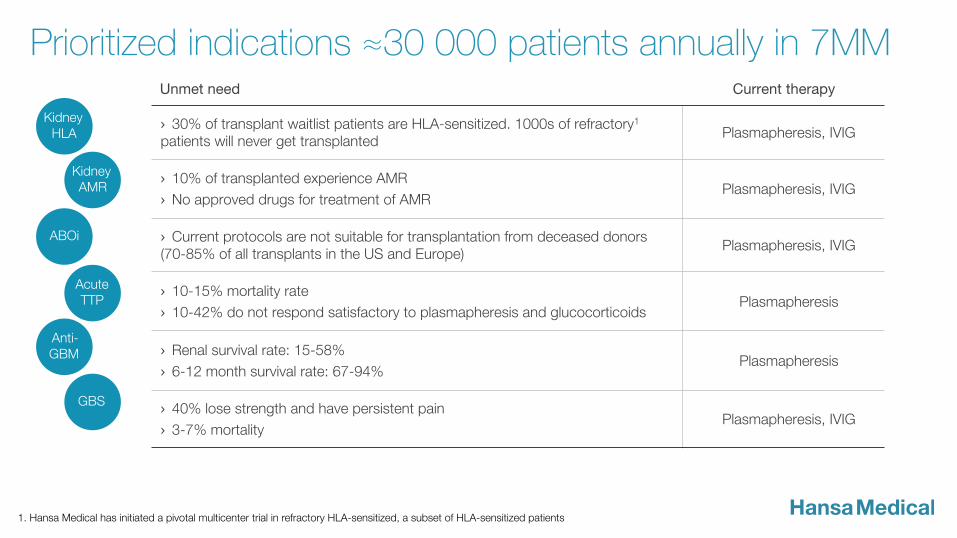
GBS
Acute TTP
Anti- GBM
Kidney HLA
ABOi
Kidney AMR
Prioritized indications ≈30 000 patients annually in 7MM Unmet need Current therapy
› 30% of transplant waitlist patients are HLA-sensitized. 1000s of refractory1 patients will never get transplanted
Plasmapheresis, IVIG
› 10% of transplanted experience AMR
› No approved drugs for treatment of AMR Plasmapheresis, IVIG
› Current protocols are not suitable for transplantation from deceased donors (70-85% of all transplants in the US and Europe)
Plasmapheresis, IVIG
› 10-15% mortality rate
› 10-42% do not respond satisfactory to plasmapheresis and glucocorticoids Plasmapheresis
› Renal survival rate: 15-58%
› 6-12 month survival rate: 67-94% Plasmapheresis
› 40% lose strength and have persistent pain
› 3-7% mortality Plasmapheresis, IVIG
1. Hansa Medical has initiated a pivotal multicenter trial in refractory HLA-sensitized, a subset of HLA-sensitized patients
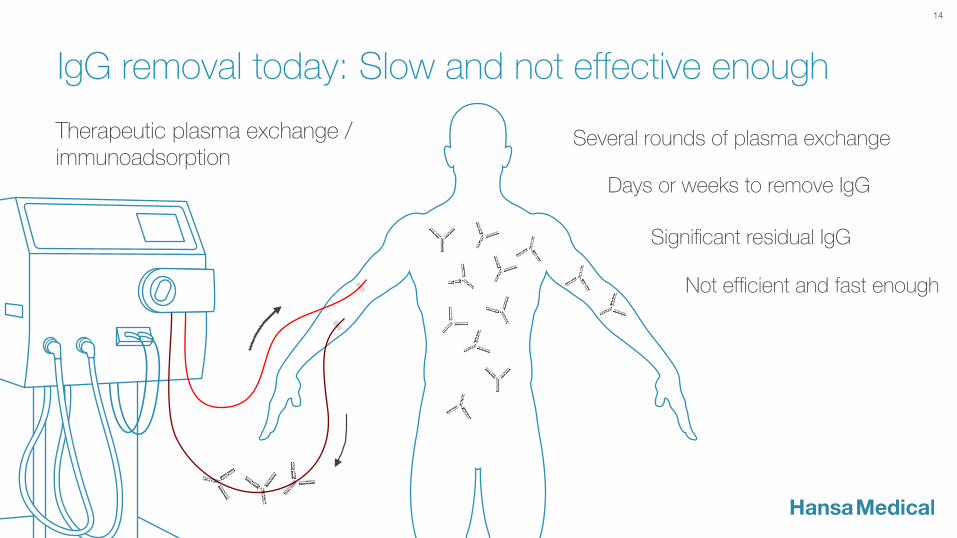
Therapeutic plasma exchange / immunoadsorption
Days or weeks to remove IgG
Significant residual IgG
Several rounds of plasma exchange
Not efficient and fast enough
IgG removal today: Slow and not effective enough
14
IdeS key differentiators in all acute IgG mediated conditions
IdeS treatment
Immediate onset
All IgG is inactivated within minutes
One 15 minute infusion
Within 2-6 hours, no intact IgG
15
1. Winstedt el al. (2015) PLOS ONE 10(7)

16
IdeS in transplantation
Prioritized transplantation indications
Kidney HLA-sens.
Kidney ABOi
Kidney AMR
› HLA-antibodies against potential donors prevents transplantation
› ≈ 10 000 patients in need of desensitization annually on 7 MM
› Blood group antigen antibodies needs to be removed prior to transplantation
› ≈ 2600 patients in need annually on 7MM
› Antibody Mediated Rejection post transplantation
› ≈ 3000 patients in need annually on 7MM
18
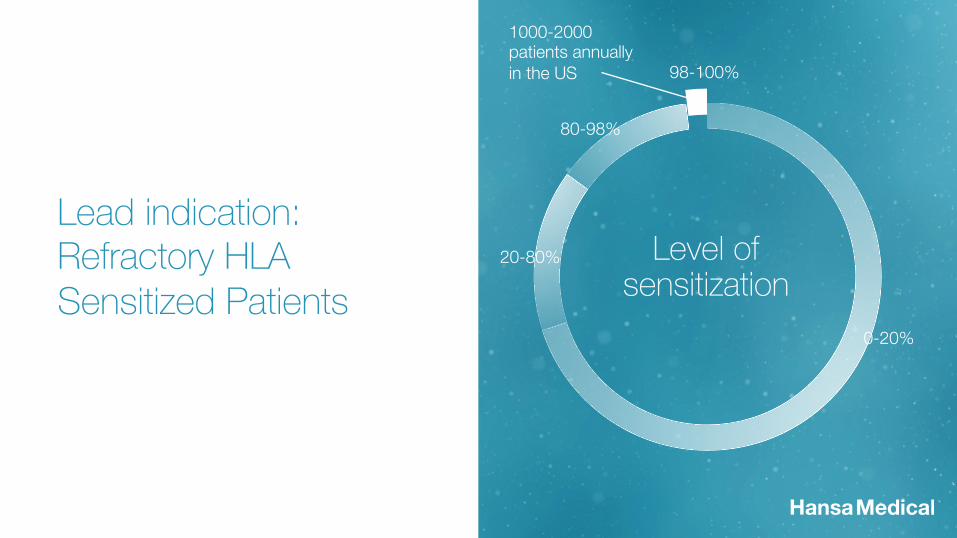
Lead indication: Refractory HLA Sensitized Patients
1. Jordan et al. British Medical Bulletin, 2015, 114:113-125 2. Orandi et al. NEJM, 2016;374:940-50
Level of sensitization
0-20%
20-80%
80-98%
98-100%
1000-2000 patients annually in the US
19
1. Orandi et al, NEJM,, 374;10, March 10, 2016
› A recent study (1,025 patients1) demonstrate the survival benefit of desensitization
› 8 year survival rate for transplanted sensitized patients: 76.5%
› 8 year survival rate for non-transplanted sensitized patients: 43.9%
› Long-term dialysis results in cardiovascular complications
The importance of desensitization
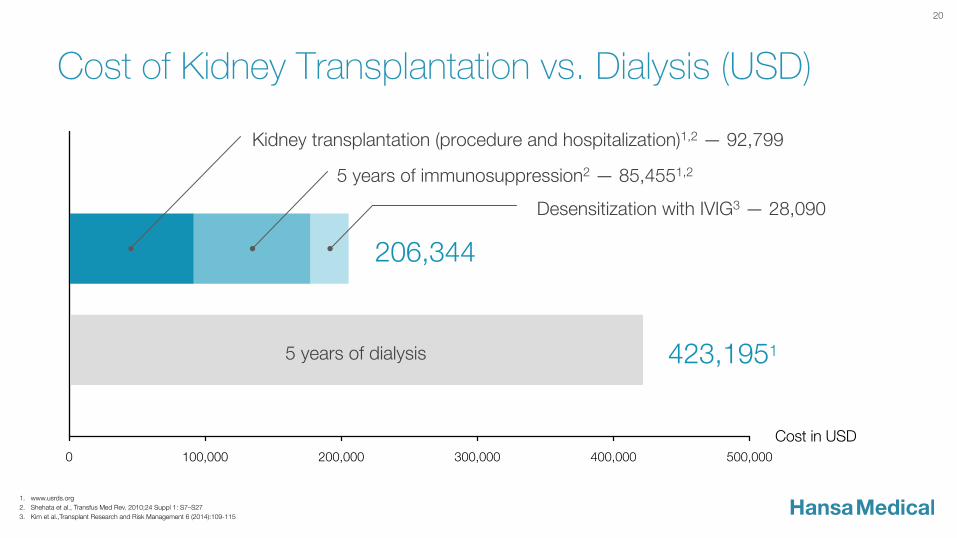
Cost of Kidney Transplantation vs. Dialysis (USD)
Cost in USD
Kidney transplantation (procedure and hospitalization) 92,799
5 years of immunosuppression 85,455
Desensitization with IVIG 28,090
In Total 206,344
For comparison: 5 years of dialysis 423,195
20
206,344
423,1951
Kidney transplantation (procedure and hospitalization)1,2 — 92,799
5 years of immunosuppression2 — 85,4551,2
Desensitization with IVIG3 — 28,090
5 years of dialysis
1. www.usrds.org 2. Shehata et al., Transfus Med Rev. 2010;24 Suppl 1: S7–S27 3. Kim et al.,Transplant Research and Risk Management 6 (2014):109-115

Completed clinical trials
Phase I
› 29 healthy subjects in 4 dose groups + placebo
› Safe and well tolerated – no SAEs
› Fully effective dose identified (0.12 and 0.24 mg/kg BW)
Phase II
› 8 sensitized patients at Uppsala University Hospital
› Patients made transplantable after IdeS treatment
› Four infections and one case of myalgia possibly related to IdeS were reported in the study
› Conclusion: Manageable safety profile with excellent risk benefit profile
21
1. Winstedt el al. (2015) PLOS ONE 10(7)
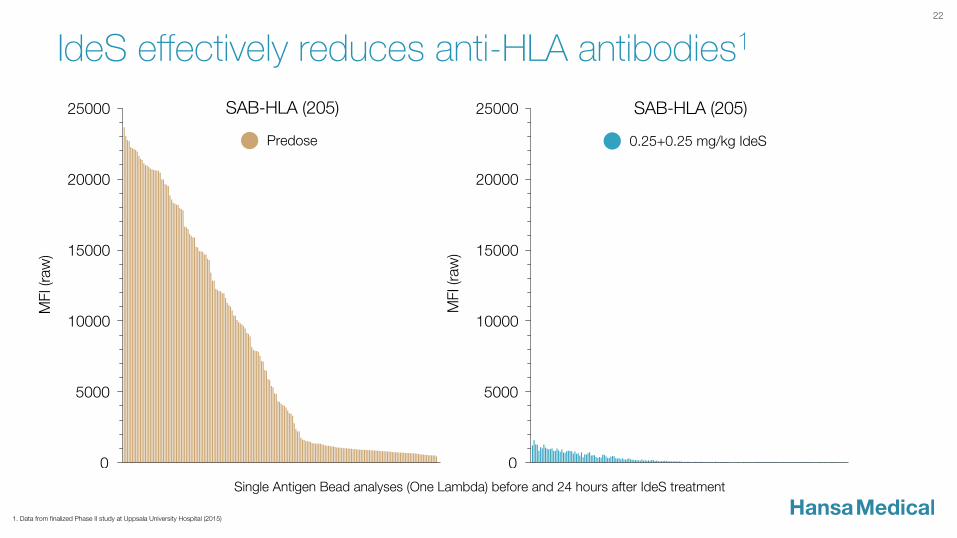
IdeS effectively reduces anti-HLA antibodies1 22
Single Antigen Bead analyses (One Lambda) before and 24 hours after IdeS treatment
1. Data from finalized Phase II study at Uppsala University Hospital (2015)
Status of ongoing Phase II trials (SWE and US)
› All 10 patients recruited in the Swedish study
› Topline results: IdeS enabled transplantation in 10/10 patients with very good creatinine levels
› Data from 10 patients in US study presented at 2016 American Transplant Congress (ATC) in Boston in June. Recruitment according to plan.
› 6 months follow up in both studies
› Results expected from Swedish study in Q4 2016
23

24
Initiated pivotal trial
› HighdeS – Refractory HLA sensitized patients
› Initiated in July 2016
› Primary endpoint: transplantability
› 20 patients, 6 months follow-up, target completion: H2 2017
At:
› Cedars-Sinai Medical Center, Los Angeles
› NYU Langone Transplant Institute, New York
› The Johns Hopkins Medicine, Baltimore
› Two European sites to be announced
The Johns Hopkins Hospital
NYU Langone Transplant Institute
Cedars-Sinai Medical Center
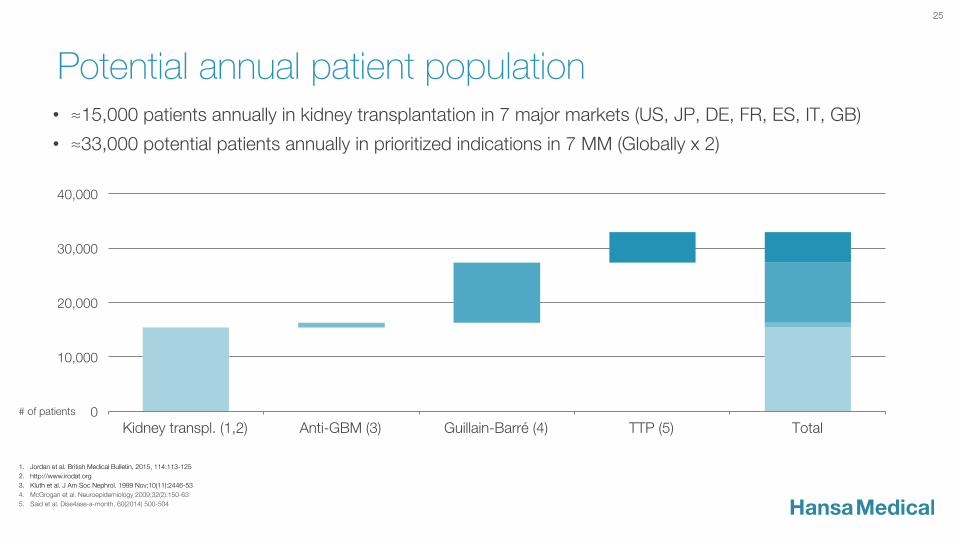
Potential annual patient population
25
• ≈15,000 patients annually in kidney transplantation in 7 major markets (US, JP, DE, FR, ES, IT, GB)
• ≈33,000 potential patients annually in prioritized indications in 7 MM (Globally x 2)
1. Jordan et al. British Medical Bulletin, 2015, 114:113-125 2. http://www.irodat.org 3. Kluth et al. J Am Soc Nephrol. 1999 Nov;10(11):2446-53 4. McGrogan et al. Neuroepidemiology 2009;32(2):150-63 5. Said et al. Dise4ase-a-month, 60(2014) 500-504
0
10,000
20,000
30,000
40,000
Kidney transpl. (1,2) Anti-GBM (3) Guillain-Barré (4) TTP (5) Total # of patients
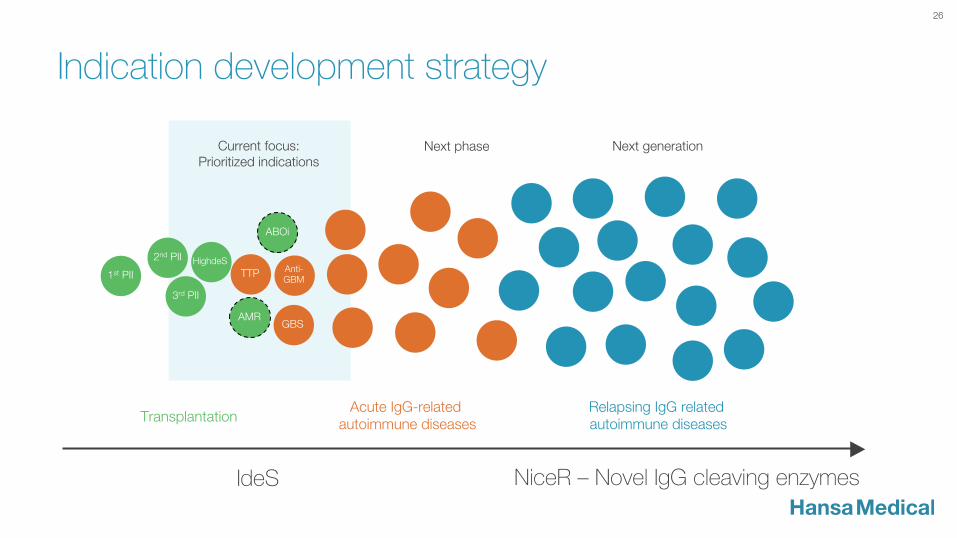
Indication development strategy
26
NiceR – Novel IgG cleaving enzymes IdeS
1st PII
HighdeS Anti- GBM
GBS
2nd PII
3rd PII
AMR
Relapsing IgG related autoimmune diseases
Transplantation Acute IgG-related
autoimmune diseases
TTP
ABOi
Current focus: Prioritized indications
Next phase Next generation
NiceR – Novel immunoglobulin cleaving enzymes for repeat dosing
› Creation of novel IgG cleaving enzymes ongoing
› Lowered immunogenicity
› Increased efficacy
› Aim: Repeat dosing
› Highly relevant in a number of autoimmune conditions
27
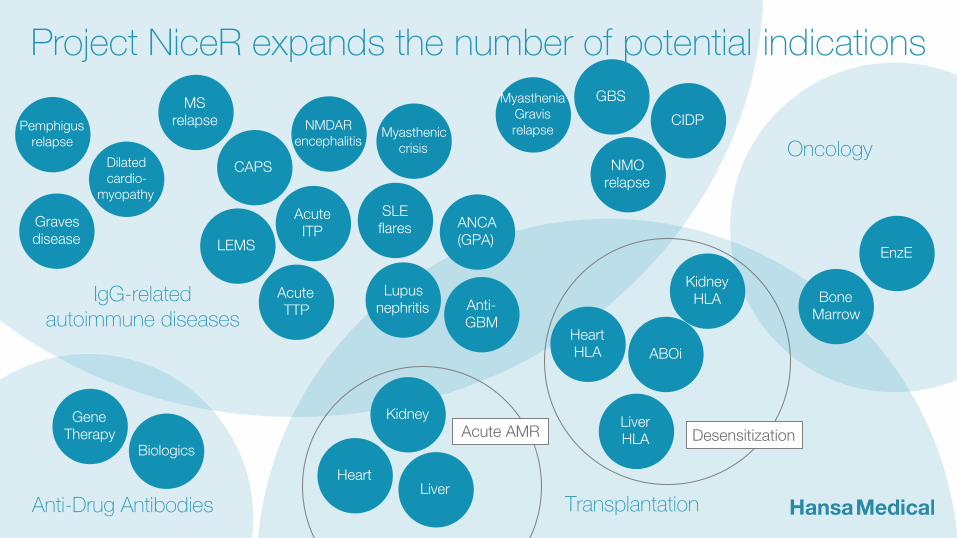
Gene Therapy
Biologics
Anti-Drug Antibodies
Myasthenia Gravis relapse
MS relapse
Acute ITP
Myasthenic crisis
Dilated cardio-
myopathy
Pemphigus relapse
CIDP
GBS
SLE flares Graves
disease
NMO relapse
NMDAR encephalitis
LEMS
CAPS
Acute TTP
IgG-related autoimmune diseases
Lupus nephritis Anti-
GBM
ANCA (GPA)
Heart HLA
Liver HLA
Kidney HLA
ABOi
Heart Liver
Kidney
Transplantation
Desensitization Acute AMR
Project NiceR expands the number of potential indications
Bone Marrow
EnzE
Oncology
EnzE – Enzyme based antibody Enhancement
29
› Enhancement of the efficacy of antibody based cancer treatments with IdeS
› In vitro data published in Journal of Molecular Biology, 2012 Jun 29;420(1-2):1-7. Crispin et al, University of Oxford
› Hansa Medical to publish confirmatory in vitro and in vivo data soon
› Potential: Presently available antibody based cancer therapies could be made more effective
› Global market for monoclonal antibodies for cancer is estimated at $23 billion, and is expected to grow to $33 billion by 2017
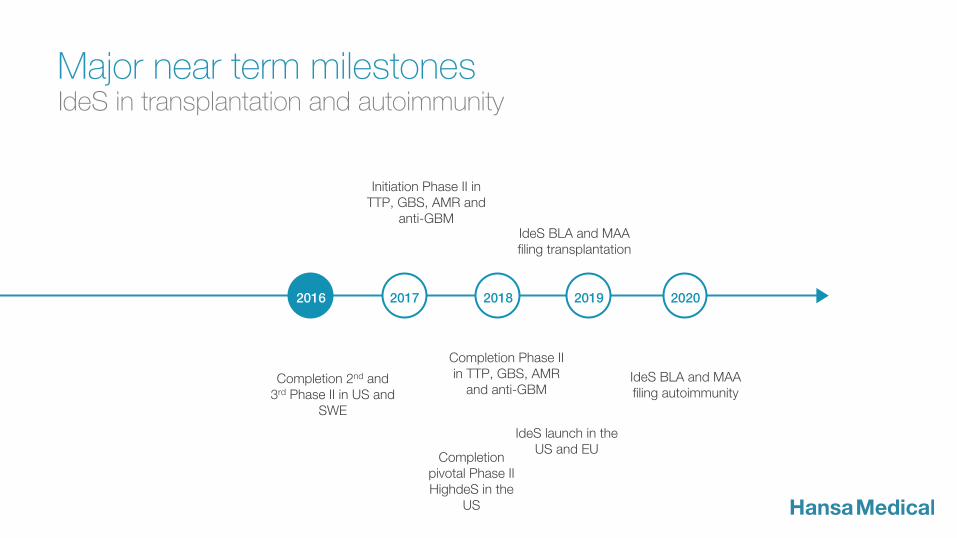
IdeS BLA and MAA filing transplantation
30
Major near term milestones
Initiation Phase II in TTP, GBS, AMR and
anti-GBM
IdeS launch in the US and EU
IdeS BLA and MAA filing autoimmunity
IdeS in transplantation and autoimmunity
2016 2017 2018 2020 2019
Completion 2nd and 3rd Phase II in US and
SWE
Completion pivotal Phase II HighdeS in the
US
Completion Phase II in TTP, GBS, AMR
and anti-GBM

31
Q&A
Appendix

33
› Use of isolated IdeS to create Fc and Fab
› Medical use of IdeS in IgG mediated conditions
› Use of isolated IdeS for immune response
› Dose regime of IdeS in combination with other therapy such as transplantation
› New versions of IdeS
Granted and pending IdeS patents (2022-2035)
34
› Orphan Drug Designation Solid Organ Transplantation – Approved (FDA) – 10 and 7 years post authorization (EU, USA)
› Orphan Drug Designation Autoimmune disease – To be filed – 10 years post authorization
› Biologics and data exclusivity – 11-12 years post authorization
Additional market exclusivity
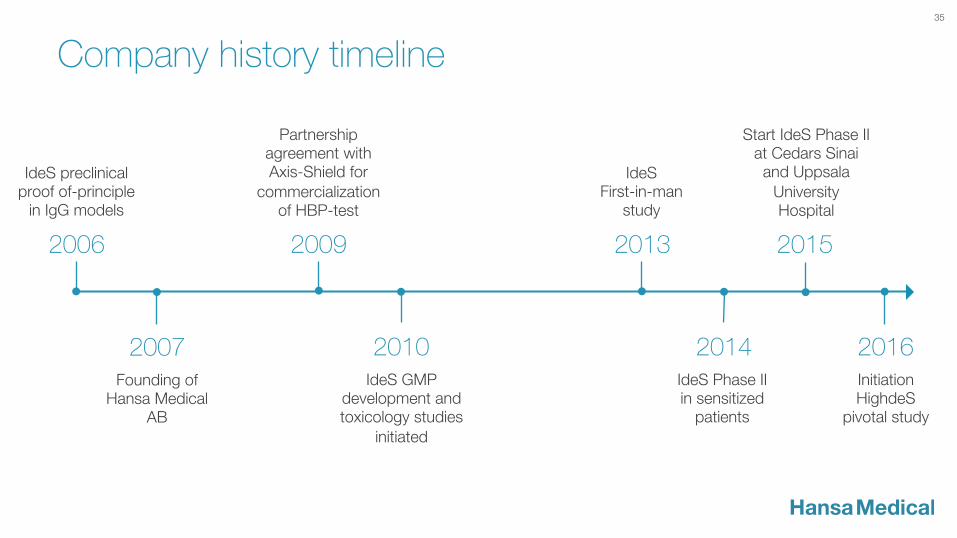
IdeS preclinical proof of-principle
in IgG models
IdeS Phase II in sensitized
patients
Founding of Hansa Medical
AB
2006
2007
Partnership agreement with Axis-Shield for
commercialization of HBP-test
2009
IdeS GMP development and toxicology studies
initiated
2010
IdeS First-in-man
study
2013
2014
Start IdeS Phase II at Cedars Sinai and Uppsala
University Hospital
2015
Initiation HighdeS
pivotal study
2016
35
Company history timeline

Management Team Göran Arvidson, President and CEO Executive Vice President and CFO of Swedish Orphan Biovitrum AB (publ), Co-founder of Biovitrum and has held senior positions with Procordia AB and Pharmacia AB. Göran holds a B.Sc. in Business Administration from Stockholm School of Economics.
Emanuel Björne, Vice President Business Development and Investor Relations Joined Hansa Medical in 2007 - experience from Biolin Scientific and Polypeptide Labs. Emanuel holds an M.Sc. in Engineering Physics (biophysics core) from Lund University and the University of California at Santa Barbara
Dr. Christian Kjellman, Senior Vice President Research and Development Joined Hansa Medical in 2008 after serving at BioInvent AB and Cartela AB. Assistant Professor in Molecular Genetics at Lund University. Christian holds an M.Sc. in Chemical Biology and a Ph.D. in Tumour Immunology from Lund University.
Dr. Lena Winstedt, Vice President Project Management Before joining Hansa Medical in 2011, she served at BioInvent International AB, Genmab A/S and H. Lundbeck AB. Lena holds an M.Sc. in Molecular Biology from Lund University and the University of Glasgow and a Ph.D. in Microbiology from Lund University.
Eva-Maria Joed, Vice President, Chief Financial Officer Eva-Maria joined Hansa Medical in 2015. She has held positions both as Chief Accountant and CFO at Kemira Kemi AB, Johns Manville AB within the Berkshire Hathaway group and Procordia Food AB Eva-Maria holds an M. Sc. in Business and Economics from Lund University.
Steven Glazer, Vice President, Chief Medical Officer Steven joined Hansa Medical in August 2015. He served at BioInvent AB, Zealand Pharma and NovoNordisk. Steven holds a Doctor of Medicine from the University of Copenhagen and was trained in Internal Medicine.
Henk Doude van Troostwijk, Vice President, Commercial Operations Henk joined Hansa Medical in May 2016. He has extensive management experience in sales and marketing in the areas of transplantation and orphan drugs. from Raptor Pharmaceuticals and Genzyme Europe BV. Henk holds an MBA from Henley Management College, UK.
36
Board of Directors
Ulf Wiinberg, Chairman of the board (2016) Former CEO of H Lundbeck A/S. Also served as president of global consumer health care business and European pharma business at Wyeth.
Dr. Angelica Loskog (2016) Professor at the Department of Immunology, Genetics and Pathology at Uppsala University. Scientific advisor to Nexttobe AB.
Hans Schikan (2015) Sobi (Swedish Orphan Biovitrum, publ), InteRNA, Dutch Top Sector Life Sciences & Health and Asceneuron.
Birgit Stattin Norinder (2012) Prolifix Ltd, Pharmacia & Upjohn, Glaxo Group Research Ltd.
Per Olof Wallström (2011) Merck, Astra, Pharmacia and Bristol-Myers Squibb, Q-Med AB, Melacure Therapeutics AB, Karo Bio AB and Camurus AB
Dr. Stina Gestrelius (2007) Biora AB, Medicon Valley Alliance, BioActive Polymers, Biogaia AB (publ.), Clavis Pharma ASA (publ.) and Lipopeptide AB
37
US Medical Advisory Board
Professor Stanley Jordan (Chairman) M.D, Ph.D., Director of Kidney Transplantation and Transplant Immunology, Kidney and Pancreas Transplant Center and Director of Division of Pediatric and Adult Nephrology, Cedars-Sinai Medical Center, Los Angeles, California
Professor Robert Montgomery M.D, DPhil, FACS, Director at NYU Langone Transplant Institute, New York, NY, USA
Professor Kathryn Wood Ph.D. Fellow of the Academy of Medical Sciences, Professor of Immunology in the Nuffield Department of Surgical Sciences, University of Oxford, England, runs the Transplantation Research Immunology Group
38
European Medical Advisory Board
Professor Kathryn Wood Ph.D. Fellow of the Academy of Medical Sciences, Professor of Immunology in the Nuffield Department of Surgical Sciences, University of Oxford, England, runs the Transplantation Research Immunology Group
Professor Christophe Legendre M.D, Ph.D. Professor at Paris Descartes University and Head of the Adult Nephrology and Transplantation unit at Necker Hospital in Paris.
Professor Gunnar Tufveson (Chairman) M.D., Ph.D., Professor of Transplant Surgery at Uppsala University and Chief Physician at the Department of Surgical Sciences at Uppsala University Hospital
39
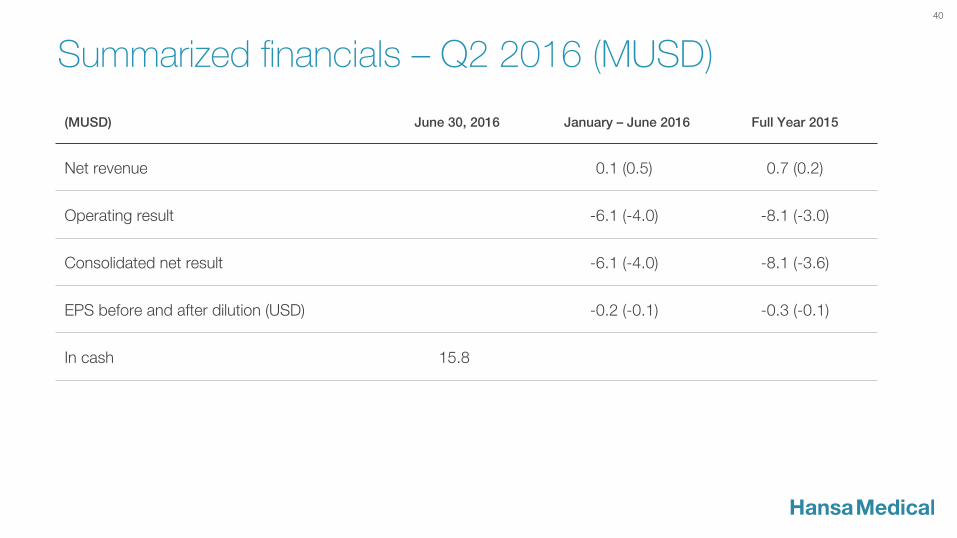
Summarized financials – Q2 2016 (MUSD)
40
(MUSD) June 30, 2016 January – June 2016 Full Year 2015
Net revenue 0.1 (0.5) 0.7 (0.2)
Operating result -6.1 (-4.0) -8.1 (-3.0)
Consolidated net result -6.1 (-4.0) -8.1 (-3.6)
EPS before and after dilution (USD) -0.2 (-0.1) -0.3 (-0.1)
In cash 15.8