seminar burkholderia 1
TRANSCRIPT
Burkholderia
Dr Sandhya Kulkarni
OUTLINE• Introduction
• History & Diversity and taxonomy
• Epidemiology – Agent
• Morphology and cultural characteristics
• Virulence factors and pathogenesis, immunopathogenesis
– Environment
– Host • Risk factors
• Clinical syndromes
• Laboratory diagnosis
• Management and Prevention
INTRODUCTION
Introduction
• Complex group of organisms exhibiting extreme diversity in• Genus contains over 40 species
• Host specificity
• Biochemical and physiologic activity
• Nonfermenting gram negative bacteria - NFGNB– ? Emerging bacterial pathogens / often missed either as contaminants or reported as
Pseudomonas species across the world
• Burkholderia pseudomallei
• Burkholderia mallei
• Burkholderia cepacia complex – BCC – HETEROGENOUS GROUP OF nine genomovars
• Burkholderia gladioli
• Key microbial constituents of rhizosphere
– Role in environment
Emerging pathogens
• Burkholderia pseudomallei
– Causative microbe of Meliodosis / Whitmore's disease
– Recent recognition southeast Asia, Australia
– Possibly under-diagnosed in India
• Burkholderia cepacia complex – BCC
– Increasingly common nosocomial pathogen & recent reports of community aquired infections
• high intrinsic and acquired antimicrobial resistance, lack of effective antibiotics, and survival ability in the environment for prolonged periods of time
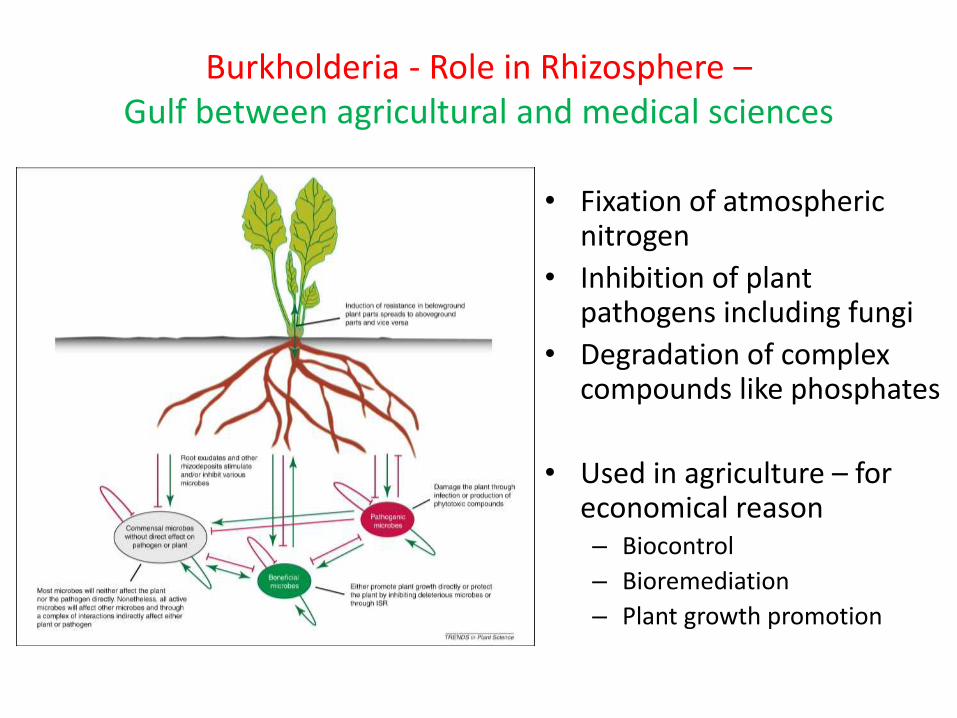
Burkholderia - Role in Rhizosphere –Gulf between agricultural and medical sciences
• Fixation of atmospheric nitrogen
• Inhibition of plant pathogens including fungi
• Degradation of complex compounds like phosphates
• Used in agriculture – for economical reason– Biocontrol
– Bioremediation
– Plant growth promotion
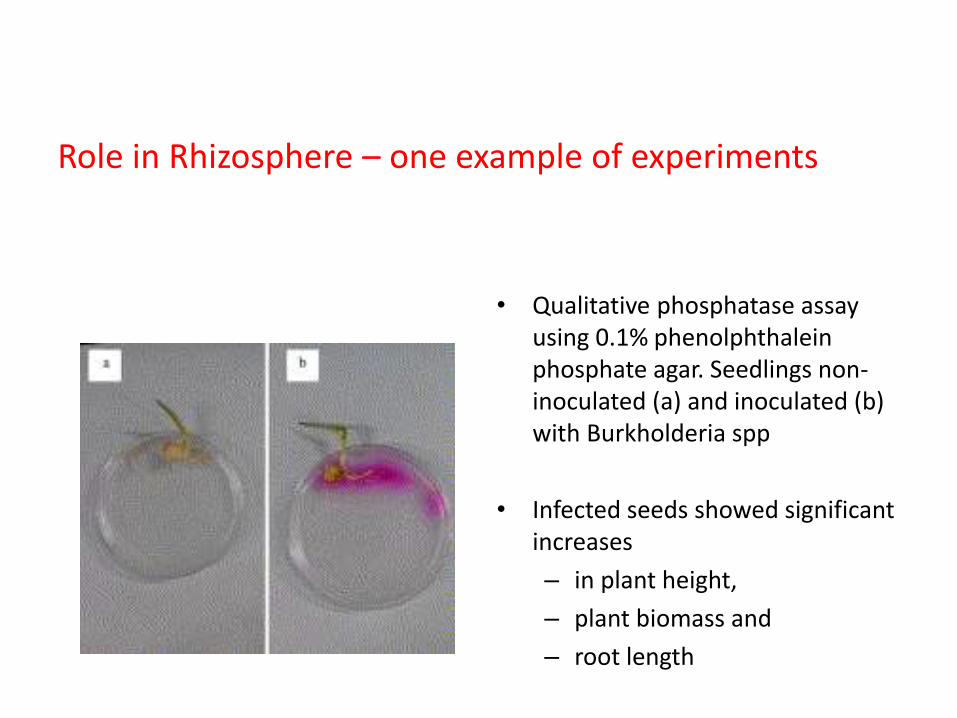
Role in Rhizosphere – one example of experiments
• Qualitative phosphatase assay using 0.1% phenolphthalein phosphate agar. Seedlings non-inoculated (a) and inoculated (b) with Burkholderia spp
• Infected seeds showed significant increases
– in plant height,
– plant biomass and
– root length
History
&
Diversity and taxonomy
Interest arose as MELIODOSIS emerged
History • 1882 – Loeffler & Schultz Glanders ..isolation of Bacillus mallei
• 1912 – Alfred Whitmore & Krishnaswamy
Glanders-like: in morphia addicts ..Rangoon
• 1932 – Stanton & Fletcher .. Bacillus whitmorii
Greek - Melis: distemper of asses, eidos: resemblance
• 1970 – Public health importance
– thailand and other SE Asia countries, Northern Australia
Fatal CAP , 20 % in Thailand
» Bacillus pseudomallei,, Malleomyces pseudomallei, Pseudomonas pseudomallei
– Vietnam Time Bomb – In Returning soldiers
• 1973 – Pellaroni work – Pseudomonas Genus Dissection into 5 clusters
• 1970 - 80’ s – Cepacia syndrome– Isolation of these species (now under BCC) from Cystic fibrosis patients - Selective agars
• 1992 – Yabuuchi et al – Cluster II dissected further Genus Burkholder ..
– named after Walter Burkholder
Walter Hagemeyer Burkholder, 1891–1983Phytopathologist
• Ph.D. degree from Cornell University
• Pioneer in bacterial taxonomy - major genera of plant-pathogenic bacteria that had been lumped into the genus Phytomonas.
• Burkholder’s classification scheme -Bergey’s Manual of Determinative Bacteriology - served as editor of the phytopathogenic bacteria section for many years.
• First described Pseudomonas cepacia (Burkholderia cepacia) in 1949 as a cause of rot on onion bulbs. The genus Burkholderia is named in his honor.
REVIEW ARTICLEBurkholderia cepacia: medical, taxonomic andecological issuesJ. R. W. GOVAN - J. Med. Microbiol. - Vol. 45 (1996), 395407
http://www.apsnet.org/about/history/pioneeringplantpathologists/Pages/BurkholderWalterHagemeyer.aspx
History - Taxonomy• Burkholderia cepacia complex - BCC
– a clinical laboratory differentiation of species within the Bcc is lacking
– Phenotypically similar but genotypically distinct groups
– 1997 Vandamme et al, 2001 Coenye et al - Nine genomovars
– Novel genomovars - expanding knolwedge
– Genomovars - By recA gene amplification
Why we need to know?
Cause of concern for in India .. Antimicrobial resistance, person-to-person transmission and hospital outbreaks
I. B. cepacia
II. B. multivorans
III. B. cenocepacia
IV. B. stabilis
V. B. vietnamiensis
VI. B. dolosa
VII. B. ambifaria
VIII. B. anthina
IX. B. pyrrocinia
MOST common in cystic fibrosis / outbreaksIn UK and USAB. cenocepacia BCC – IIIB. multivorans BCC - II
Epidemiology - Agents
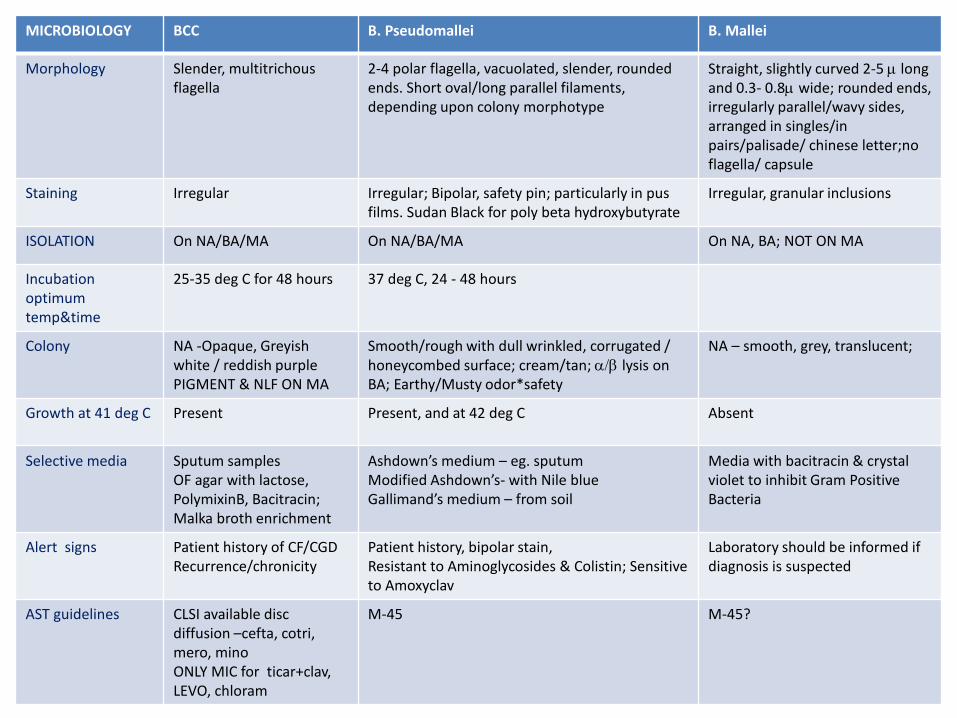
MICROBIOLOGY BCC B. Pseudomallei B. Mallei
Morphology Slender, multitrichousflagella
2-4 polar flagella, vacuolated, slender, rounded ends. Short oval/long parallel filaments,depending upon colony morphotype
Straight, slightly curved 2-5 m long and 0.3- 0.8m wide; rounded ends, irregularly parallel/wavy sides, arranged in singles/in pairs/palisade/ chinese letter;noflagella/ capsule
Staining Irregular Irregular; Bipolar, safety pin; particularly in pus films. Sudan Black for poly beta hydroxybutyrate
Irregular, granular inclusions
ISOLATION On NA/BA/MA On NA/BA/MA On NA, BA; NOT ON MA
Incubation optimum temp&time
25-35 deg C for 48 hours 37 deg C, 24 - 48 hours
Colony NA -Opaque, Greyishwhite / reddish purplePIGMENT & NLF ON MA
Smooth/rough with dull wrinkled, corrugated / honeycombed surface; cream/tan; a/b lysis on BA; Earthy/Musty odor*safety
NA – smooth, grey, translucent;
Growth at 41 deg C Present Present, and at 42 deg C Absent
Selective media Sputum samplesOF agar with lactose, PolymixinB, Bacitracin; Malka broth enrichment
Ashdown’s medium – eg. sputum Modified Ashdown’s- with Nile blueGallimand’s medium – from soil
Media with bacitracin & crystal violet to inhibit Gram Positive Bacteria
Alert signs Patient history of CF/CGDRecurrence/chronicity
Patient history, bipolar stain,Resistant to Aminoglycosides & Colistin; Sensitive to Amoxyclav
Laboratory should be informed ifdiagnosis is suspected
AST guidelines CLSI available disc diffusion –cefta, cotri,mero, minoONLY MIC for ticar+clav, LEVO, chloram
M-45 M-45?
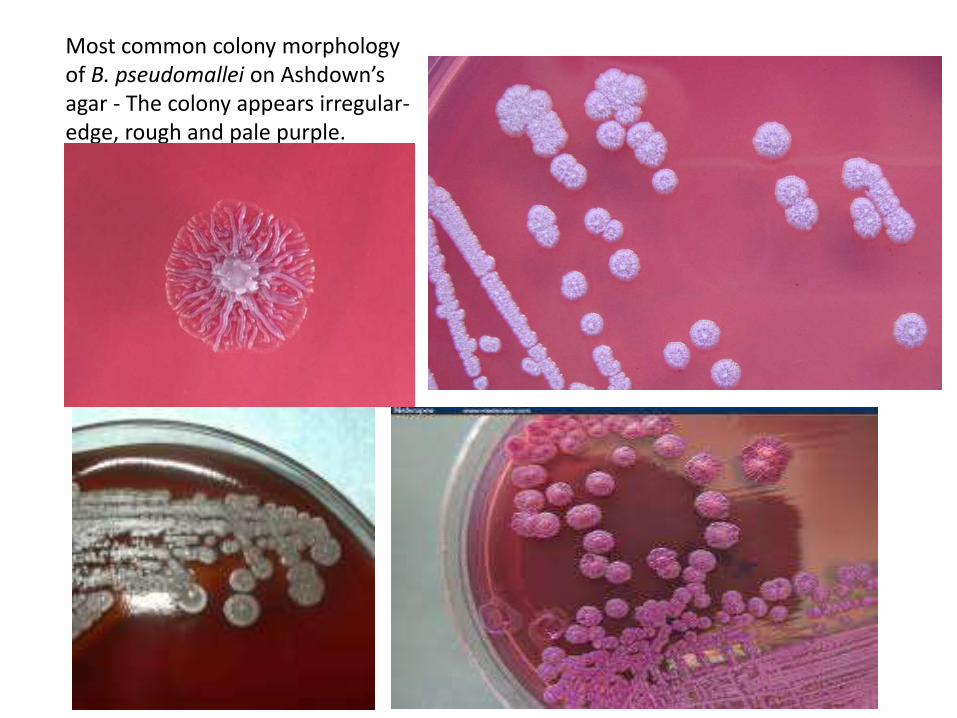
Most common colony morphology of B. pseudomallei on Ashdown’s agar - The colony appears irregular-edge, rough and pale purple.
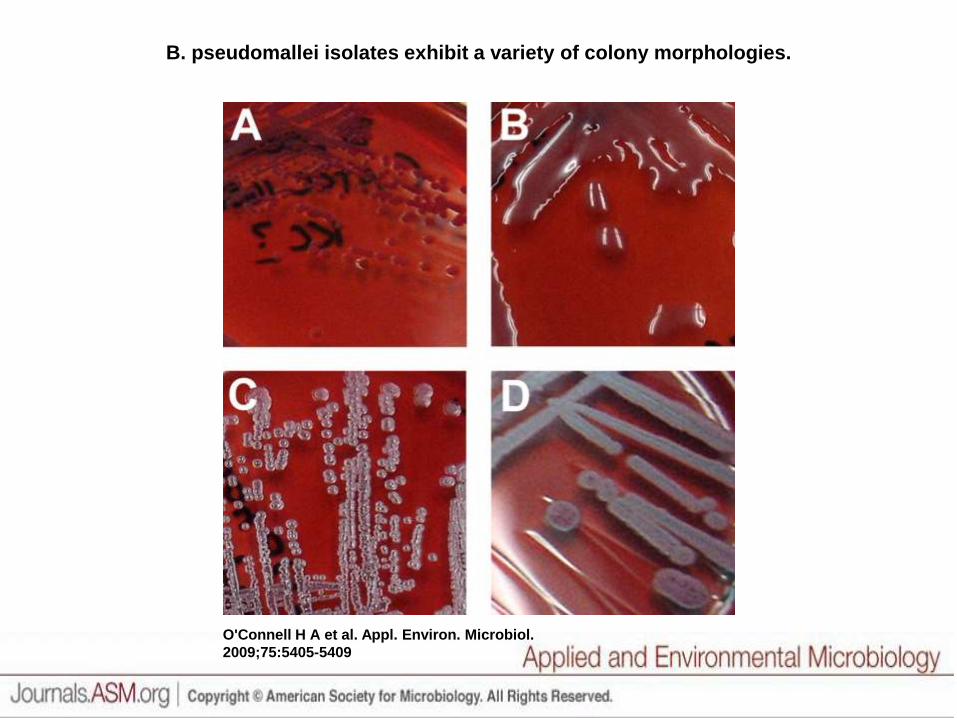
B. pseudomallei isolates exhibit a variety of colony morphologies.
O'Connell H A et al. Appl. Environ. Microbiol.
2009;75:5405-5409
Biological Relevance of Colony Morphology and Phenotypic Switching by Burkholderia pseudomallei
J. Bacteriol. February 2007 vol. 189 no. 3 807-817
• Morphotypes were divided into seven types (denoted I to VII).
• Type I gave rise to other morphotypes (most commonly type II or III) by a process of switching in response to environmental stress, including starvation, iron limitation, and growth at 42°C.
• Switching was associated with complex shifts in phenotype, one of which (type I to type II) was associated with a marked increase in production of factors putatively associated with in vivo concealment.
• Mixed B. pseudomallei morphologies were common in individual clinical specimens and were significantly more frequent in samples of
– blood, pus, and respiratory secretions than in urine and surface swabs.
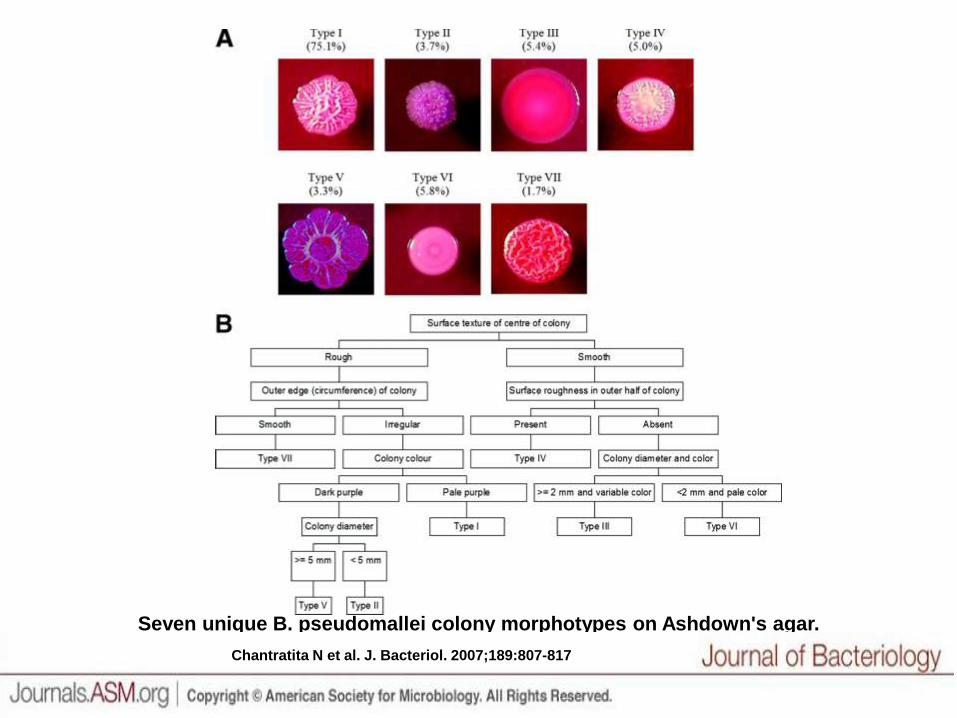
Seven unique B. pseudomallei colony morphotypes on Ashdown's agar.
Chantratita N et al. J. Bacteriol. 2007;189:807-817
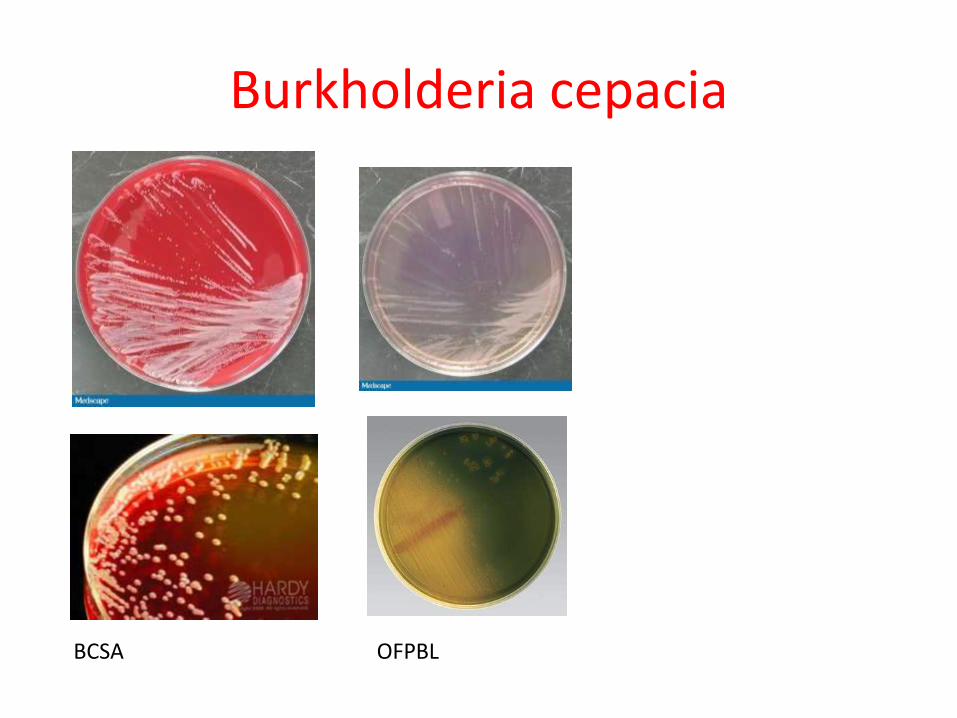
Burkholderia cepacia
OFPBLBCSA
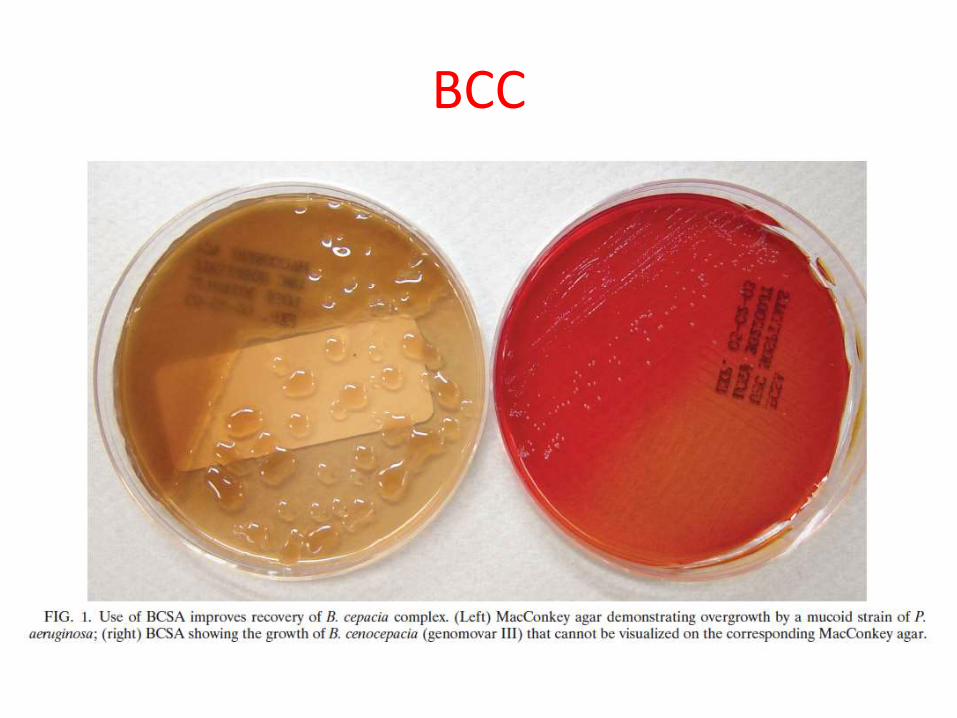
BCC
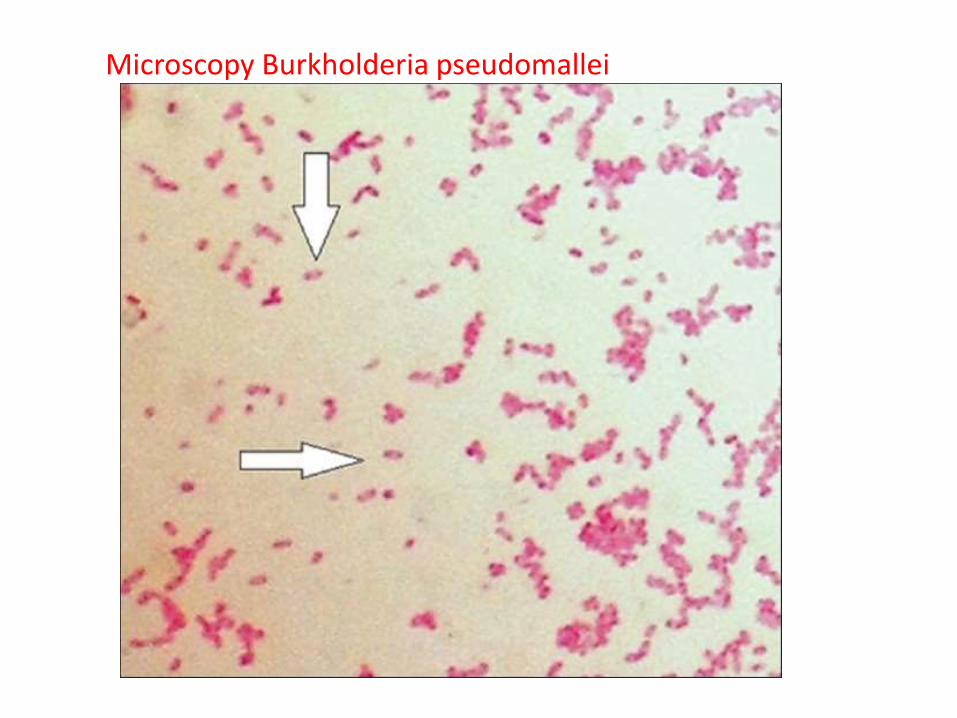
Microscopy Burkholderia pseudomallei
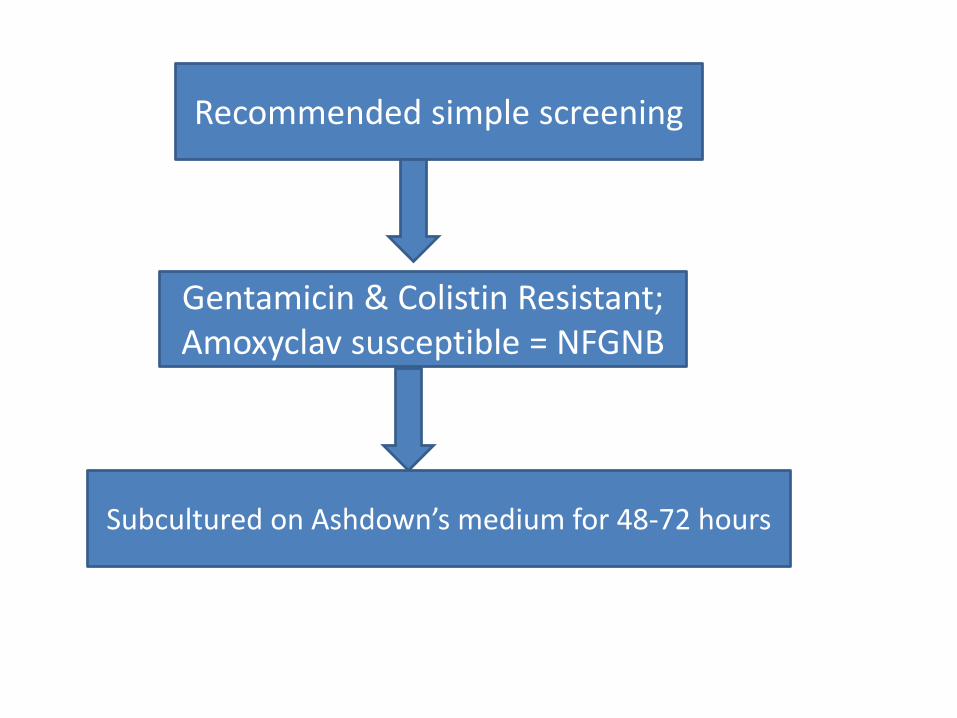
Recommended simple screening
Gentamicin & Colistin Resistant;Amoxyclav susceptible = NFGNB
Subcultured on Ashdown’s medium for 48-72 hours

Biochemical BCC Gladioli B. Pseudomallei B. Mallei
Motility + + + Nonmotile
Oxidase +/v V + +
Growth MA + + + +
Lysine + - - -
Arginine - NA + +
Ornithine + - - -
Maltose + - + +
Lactose + - + +
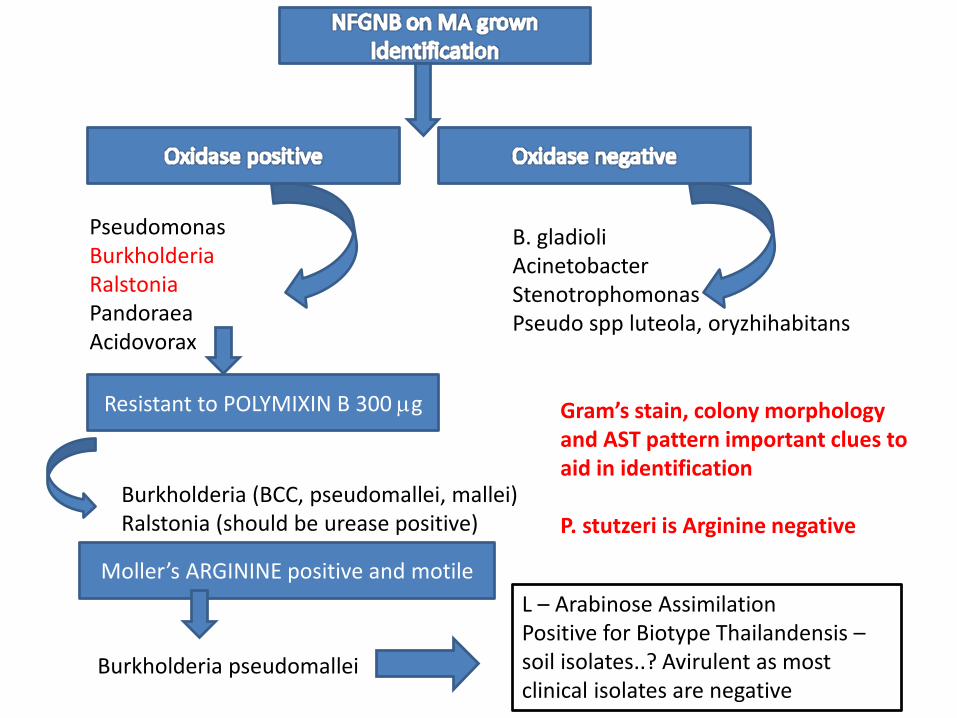
PseudomonasBurkholderiaRalstoniaPandoraeaAcidovorax
B. gladioliAcinetobacterStenotrophomonasPseudo spp luteola, oryzhihabitans
Resistant to POLYMIXIN B 300 mg
Burkholderia (BCC, pseudomallei, mallei)Ralstonia (should be urease positive)
Moller’s ARGININE positive and motile
Burkholderia pseudomallei
L – Arabinose AssimilationPositive for Biotype Thailandensis –soil isolates..? Avirulent as most clinical isolates are negative
Gram’s stain, colony morphology and AST pattern important clues to aid in identification
P. stutzeri is Arginine negative
Agents continued… - Virulence markers
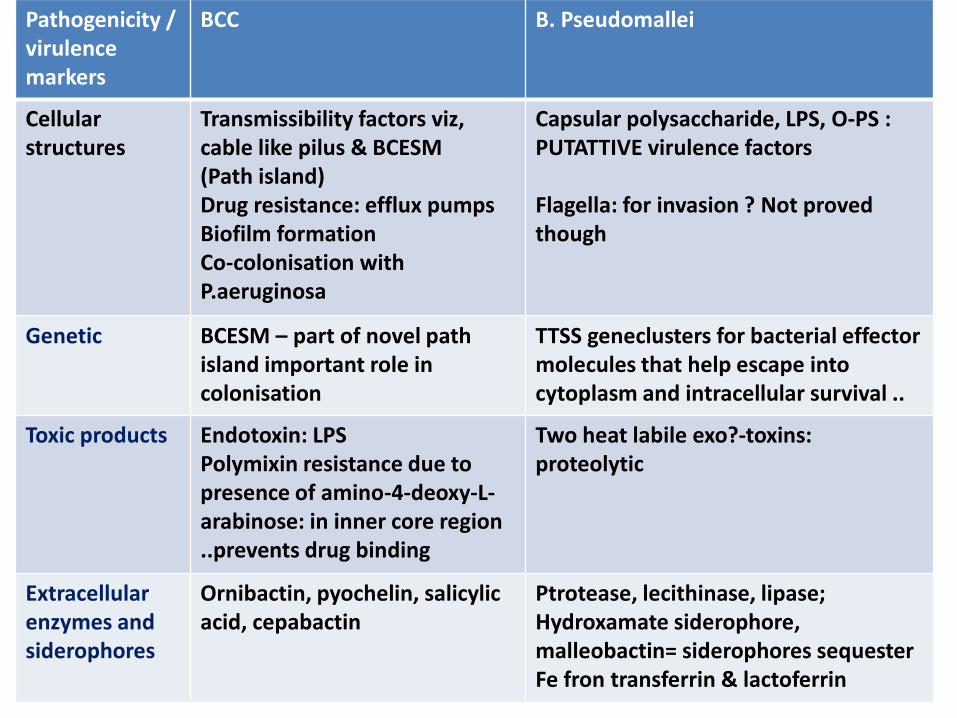
Pathogenicity / virulence markers
BCC B. Pseudomallei
Cellularstructures
Transmissibility factors viz, cable like pilus & BCESM(Path island) Drug resistance: efflux pumpsBiofilm formationCo-colonisation with P.aeruginosa
Capsular polysaccharide, LPS, O-PS :PUTATTIVE virulence factors
Flagella: for invasion ? Not proved though
Genetic BCESM – part of novel path island important role in colonisation
TTSS geneclusters for bacterial effectormolecules that help escape into cytoplasm and intracellular survival ..
Toxic products Endotoxin: LPSPolymixin resistance due to presence of amino-4-deoxy-L-arabinose: in inner core region ..prevents drug binding
Two heat labile exo?-toxins:proteolytic
Extracellular enzymes and siderophores
Ornibactin, pyochelin, salicylic acid, cepabactin
Ptrotease, lecithinase, lipase;Hydroxamate siderophore, malleobactin= siderophores sequester Fe fron transferrin & lactoferrin
Typing
• Pseudomallei
– Phages, chromosomal DNA analysis
• BCC
– Bacteriocin, phage, Chromosomal DNA analysis, and plasmid
Melioidosis – Pathology & Pathogenesis
• Poorly understood• Pyogenic organism
– Histopath: acute & or chronic..mixed• Intracellular globi of Gram Neg Bacilli combine with giant
cells in a background of acute necrotising inflammation• Outcome depends on
– Host’s immune system – Virulence of the strain– Size and route of initial inoculum
• Host defence– 50-70% underlying predisposition; probably altered host CMI impact
manifestations
• Host response– Ab to O-PSII higher in survivors
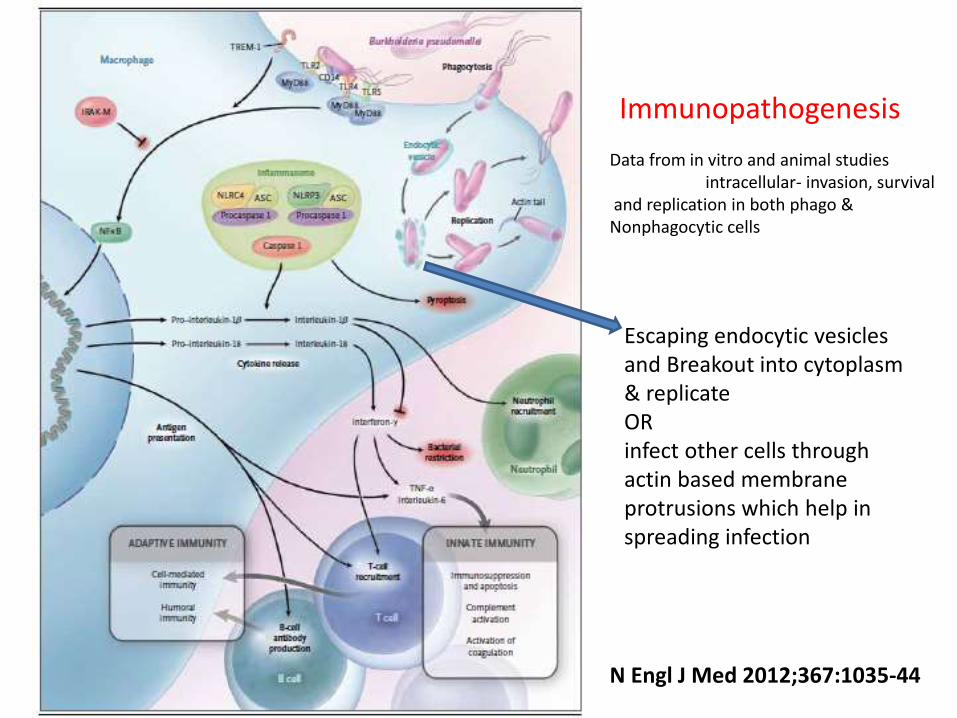
Immunopathogenesis
N Engl J Med 2012;367:1035-44
Data from in vitro and animal studiesintracellular- invasion, survival
and replication in both phago & Nonphagocytic cells
Escaping endocytic vesicles and Breakout into cytoplasm & replicateOR infect other cells through actin based membrane protrusions which help in spreading infection

Environment
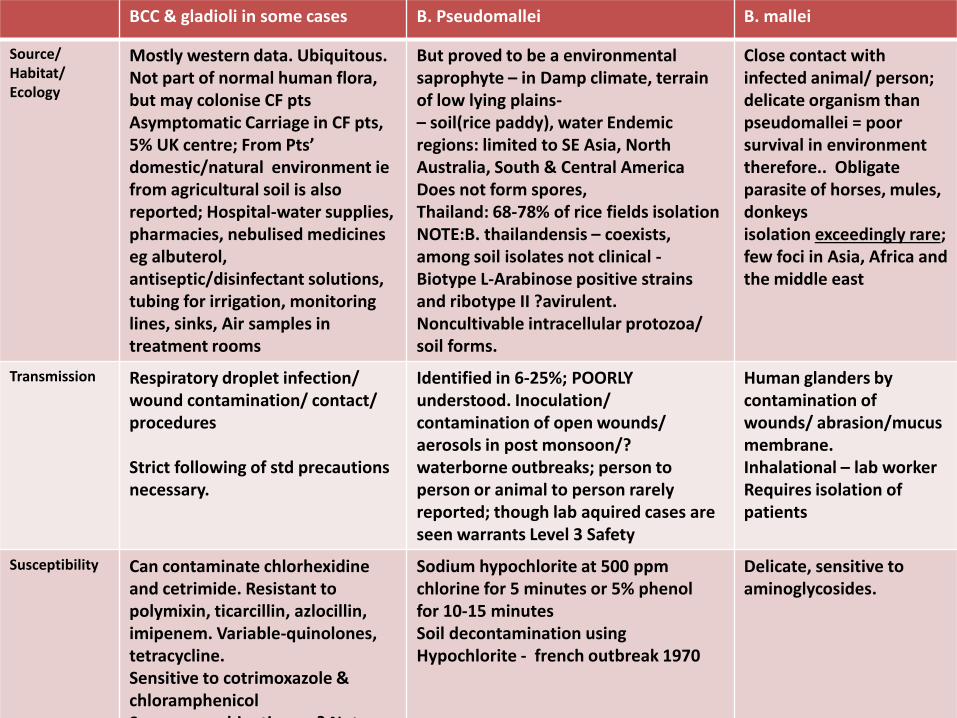
BCC & gladioli in some cases B. Pseudomallei B. mallei
Source/ Habitat/ Ecology
Mostly western data. Ubiquitous. Not part of normal human flora, but may colonise CF pts Asymptomatic Carriage in CF pts, 5% UK centre; From Pts’ domestic/natural environment iefrom agricultural soil is also reported; Hospital-water supplies, pharmacies, nebulised medicines eg albuterol, antiseptic/disinfectant solutions, tubing for irrigation, monitoring lines, sinks, Air samples in treatment rooms
But proved to be a environmentalsaprophyte – in Damp climate, terrain of low lying plains-– soil(rice paddy), water Endemic regions: limited to SE Asia, North Australia, South & Central AmericaDoes not form spores,Thailand: 68-78% of rice fields isolationNOTE:B. thailandensis – coexists, among soil isolates not clinical -Biotype L-Arabinose positive strains and ribotype II ?avirulent. Noncultivable intracellular protozoa/ soil forms.
Close contact with infected animal/ person;delicate organism than pseudomallei = poor survival in environment therefore.. Obligate parasite of horses, mules, donkeysisolation exceedingly rare; few foci in Asia, Africa and the middle east
Transmission Respiratory droplet infection/ wound contamination/ contact/ procedures
Strict following of std precautions necessary.
Identified in 6-25%; POORLY understood. Inoculation/ contamination of open wounds/ aerosols in post monsoon/? waterborne outbreaks; person to person or animal to person rarely reported; though lab aquired cases are seen warrants Level 3 Safety
Human glanders by contamination of wounds/ abrasion/mucus membrane.Inhalational – lab workerRequires isolation of patients
Susceptibility Can contaminate chlorhexidineand cetrimide. Resistant topolymixin, ticarcillin, azlocillin, imipenem. Variable-quinolones, tetracycline.Sensitive to cotrimoxazole & chloramphenicolSynergy combinations – ? Not rec
Sodium hypochlorite at 500 ppmchlorine for 5 minutes or 5% phenolfor 10-15 minutesSoil decontamination using Hypochlorite - french outbreak 1970
Delicate, sensitive to aminoglycosides.
Epidemiology - HostPseudomallei - Melioidosis
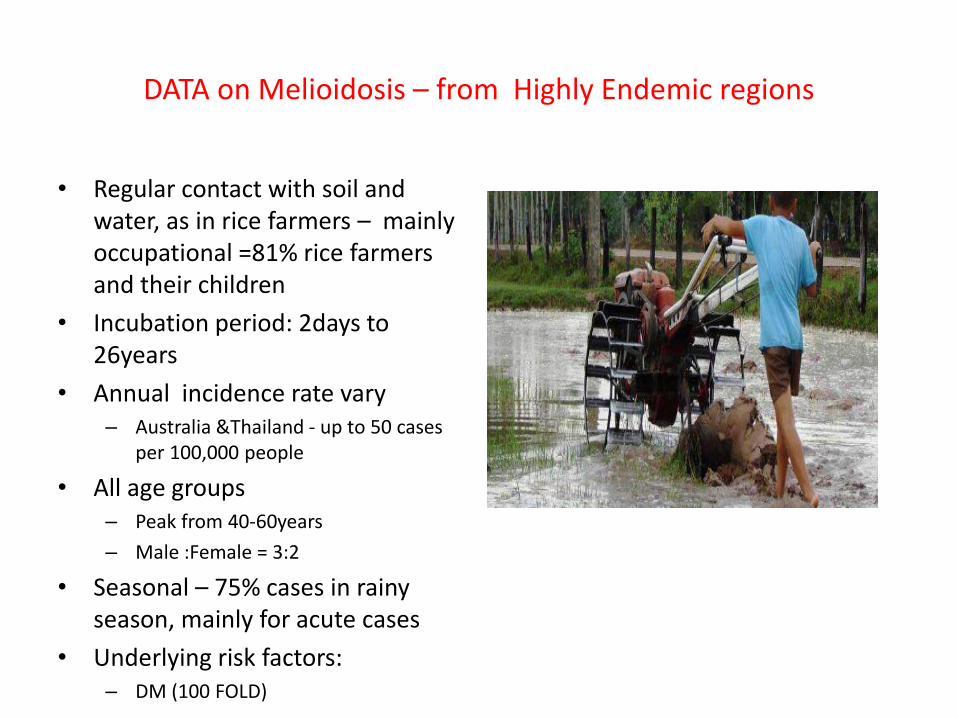
DATA on Melioidosis – from Highly Endemic regions
• Regular contact with soil and water, as in rice farmers – mainly occupational =81% rice farmers and their children
• Incubation period: 2days to 26years
• Annual incidence rate vary– Australia &Thailand - up to 50 cases
per 100,000 people
• All age groups– Peak from 40-60years
– Male :Female = 3:2
• Seasonal – 75% cases in rainy season, mainly for acute cases
• Underlying risk factors:– DM (100 FOLD)
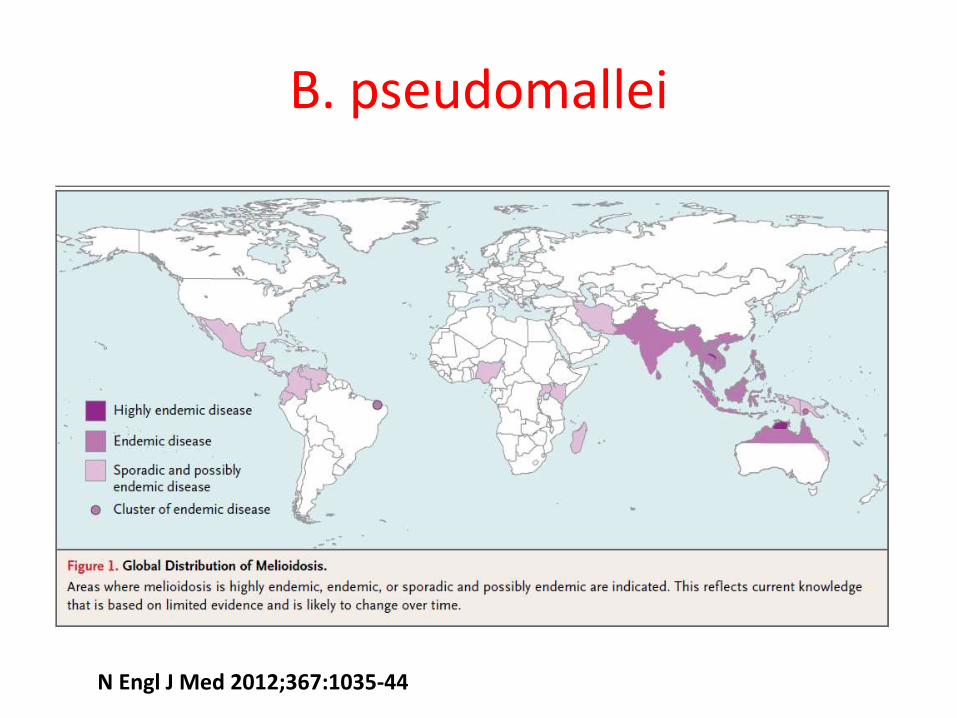
B. pseudomallei
N Engl J Med 2012;367:1035-44
Indian literature - Pseudomallei
• 1991 first reported from Bombay– Raghavan KR, Shenoi RP, Zaer F, Aiyer R, Ramamoorthy P, Mehta MN. Melioidosis in India. Indian
Pediatr 1991;28:184-8
• Later onwards several case reports/series from CMC/JIPMER/MANGLORE/St Johns
2003 - AIMS
2008 - From SJMC
Emergence of Burkholderia pseudomallei and pandrug-resistant non-fermenters from southern Karnataka, India
C. Mukhopadhyay et al Trans R Soc Trop Med Hyg (2008)
Summary points
• ………..outcome of 25 patients with melioidosis and 46 patients with MDR non-fermenters (Pseudomonas aeruginosa and Acinetobacter spp.) infection were documented during the period 2005 2007.
• Skin and soft-tissue involvement (16%), liver abscess (16%) and bone and joint involvement (16%) were the most common presentations of melioidosis in diabetic patients. The presence of septicaemia (44%) and major organ failure (48%) resulted in death. Relapse was seen in patients with inappropriate treatment. …
• More awareness among clinicians and laboratory staff, and environmental investigations of soil are required for accurate diagnosis and prompt treatment of melioidosis.
Neonatal melioidosis: A case report from India..JIPMER
• Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 260-263
• Melioidosis, caused by Burkholderia pseudomallei , is an infectious disease of major public health importance in Southeast Asia and Australia. ..
• A pre-term female baby developed respiratory distress soon after birth. The child was febrile, had tachypnea, grunting, normal heart rate with a low pulse volume and poor peripheral perfusion. Chest X-ray revealed right-sided bronchopneumonia. B. pseudomallei was isolated from the blood culture of the neonate collected aseptically. The neonate was successfully treated with meropenem.
Last year – 2012
Western coast in India – endemic
KMC Manipal study
As it is one study with highest no patient population = 95
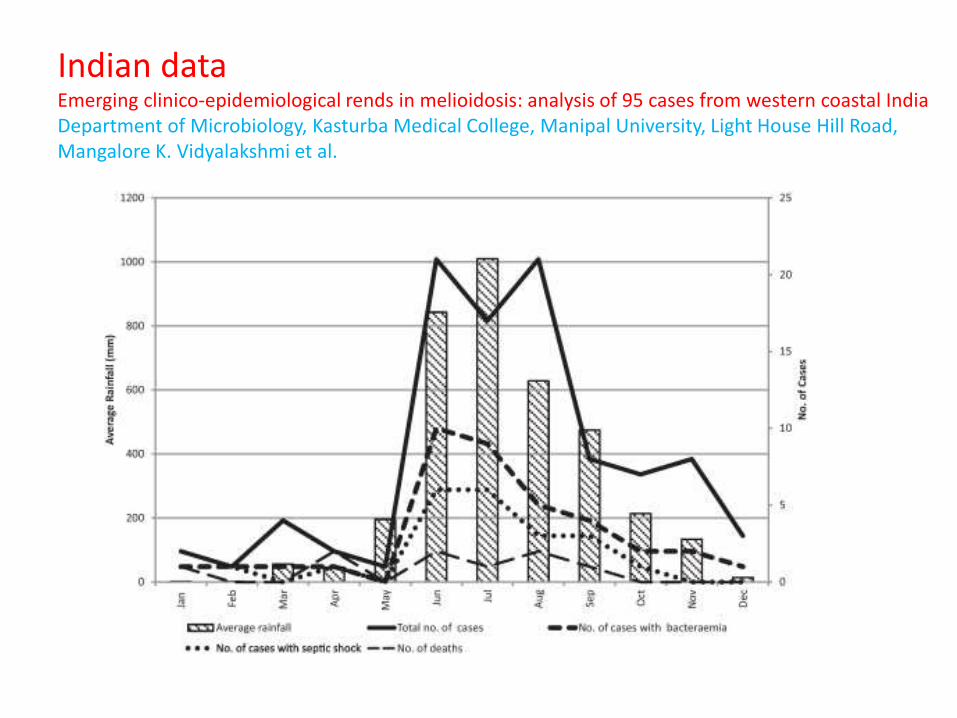
Indian dataEmerging clinico-epidemiological rends in melioidosis: analysis of 95 cases from western coastal IndiaDepartment of Microbiology, Kasturba Medical College, Manipal University, Light House Hill Road, Mangalore K. Vidyalakshmi et al.
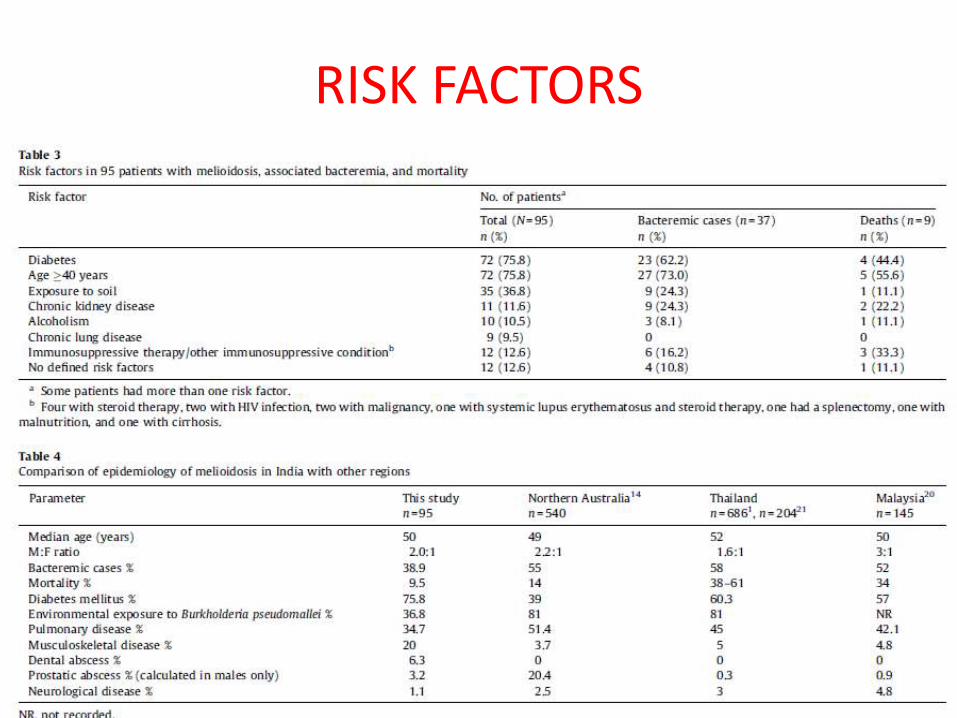
RISK FACTORS
Epidemiology – Host - BCC
BCC – Cystic fibrosis and HAI
• Hospital outbreaks
• Candian outbreak – ET12 strain with cable like pilus
• 5% colonisation – mainly adult population low rates overall
• But spectrum of disease• Asymptomatic carriage to rapid decline of lung function
• Higher mortality among colonised
• Lung transplants – higher mortality
• CROSS INFECTIONS– With infection control measures - transmission can be brought under control
between CF patients eg in treatment rooms
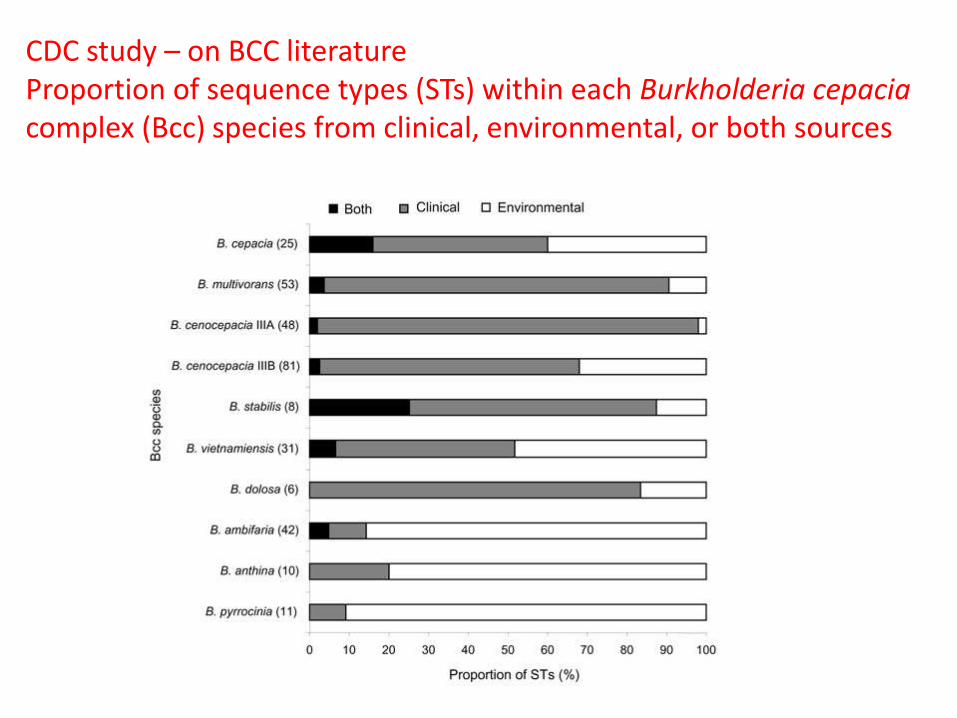
CDC study – on BCC literatureProportion of sequence types (STs) within each Burkholderia cepaciacomplex (Bcc) species from clinical, environmental, or both sources
Clinical features
Melioidosis• Remarkable imitator
– Staph/MTB
Spectrum
• Mild & subclinical infections - seroepidemiology
• Latent infections ie why its called as…
• Clinical disease - small proportion of cases
– Septicemic – prothrombotic state, multiorgan failure, multiple foci in lung/liver and most pathognomonic spleen later neurologic
» Peripheral motor weakness, Brainstem encephelitis, Aseptic meningitis, Respiratory failure
– Localised melioidosis
» Lung/Acute suppurative parotitis in children

Details @
Outcome and follow up
• Mortality 40-50%in thailand
– Australia 19%
Relapse? 1-26%
= Chronic morbidity with both disease & underlying conditions
= longterm follow up needed
= clues for relapse: CRP
Important as emergence of resistance during treatment period is known
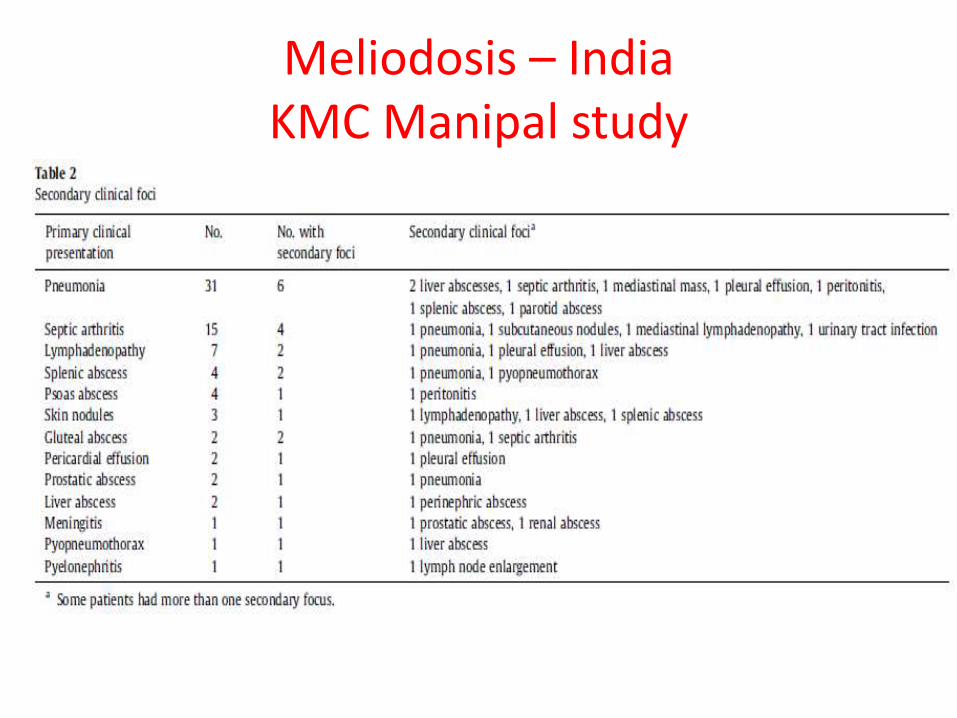
Meliodosis – IndiaKMC Manipal study
Glanders
Clinical features
Burkholderia mallei• Glanders –
– primarily affects horses, mules, and donkeys.
– can infect humans
• Cause of concern
– likely candidate for biological warfare and bioterrorism
– World War I, German forces reportedly spread glanders to debilitate enemy cavalries.
• Transmission
– enter the body through cuts in the skin or the membranes of the eyes and nose; also can be inhaled, and as an aerosol glanders would be a deadly weapon
• Incubation period before symptoms - 1-14 days
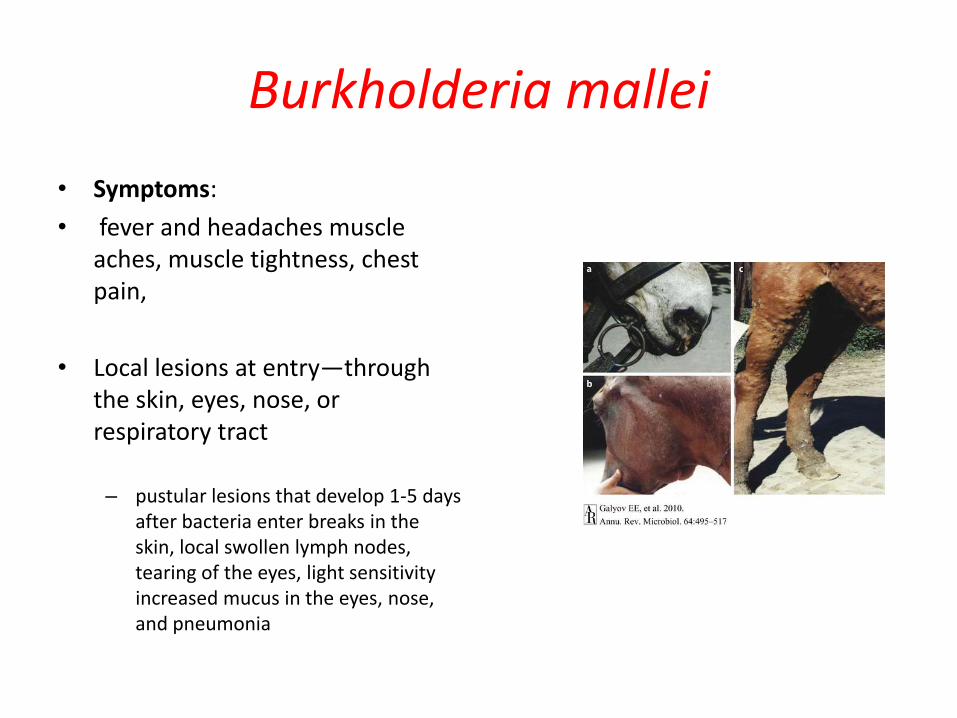
Burkholderia mallei
• Symptoms:
• fever and headaches muscle aches, muscle tightness, chest pain,
• Local lesions at entry—through the skin, eyes, nose, or respiratory tract
– pustular lesions that develop 1-5 days after bacteria enter breaks in the skin, local swollen lymph nodes, tearing of the eyes, light sensitivity increased mucus in the eyes, nose, and pneumonia

DIAGNOSIS
Meliodosis – Diagnosis
• Clinical features, patient from endemic area or with h/o travel
• Radiological – splenic/hepatic abscess swiss cheese
• Microbiological – Gold Standard – Culture
• Confirmatory even with single colony– Confirmation by latex agglutination
• Serological - IHA
• Molecular– Real-Time PCR Assay Targeting the Type III Secretion System of Burkholderia
pseudomallei
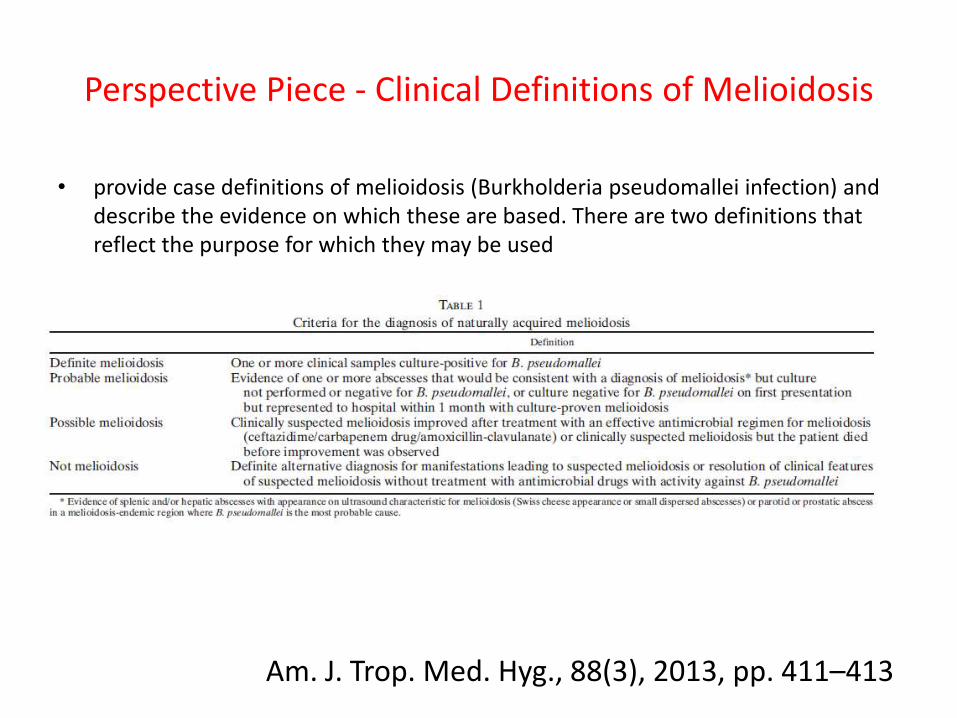
Perspective Piece - Clinical Definitions of Melioidosis
• provide case definitions of melioidosis (Burkholderia pseudomallei infection) and describe the evidence on which these are based. There are two definitions that reflect the purpose for which they may be used
Am. J. Trop. Med. Hyg., 88(3), 2013, pp. 411–413
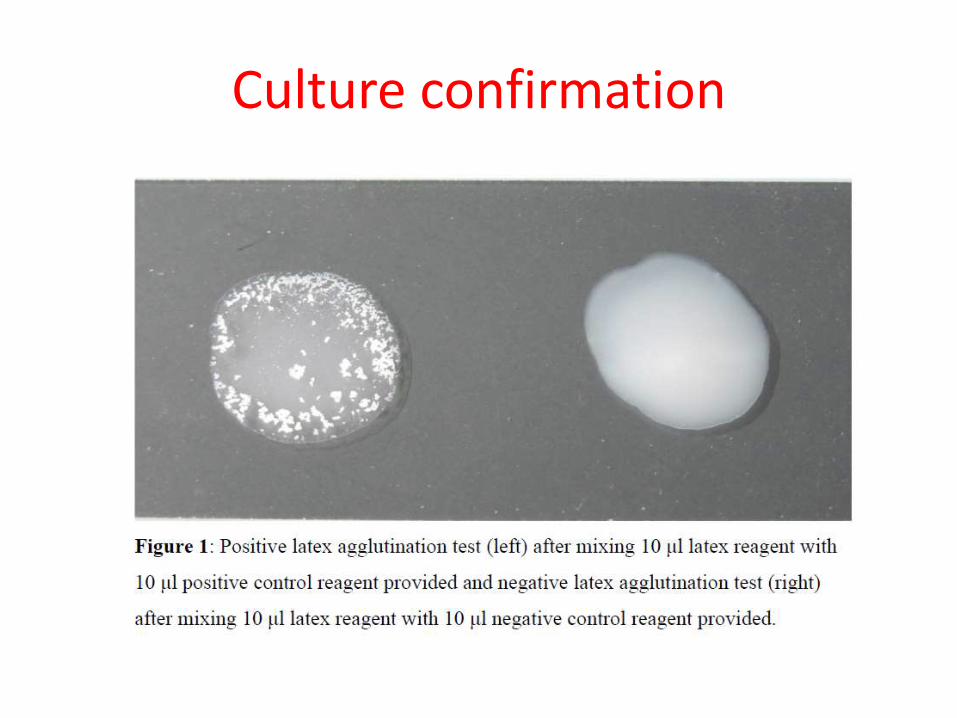
Culture confirmation
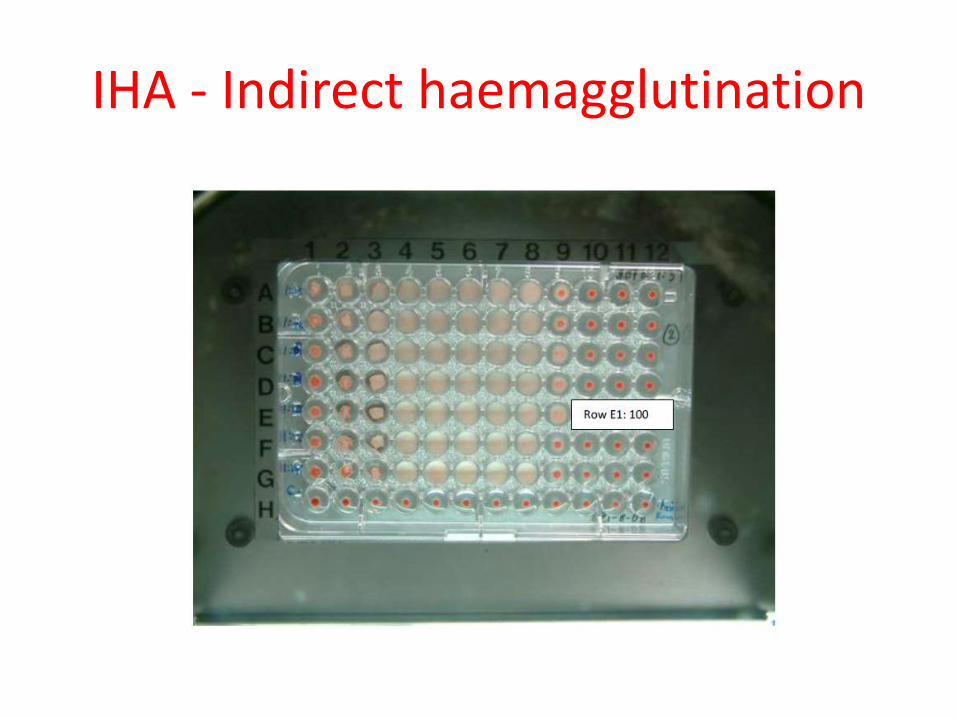
IHA - Indirect haemagglutination
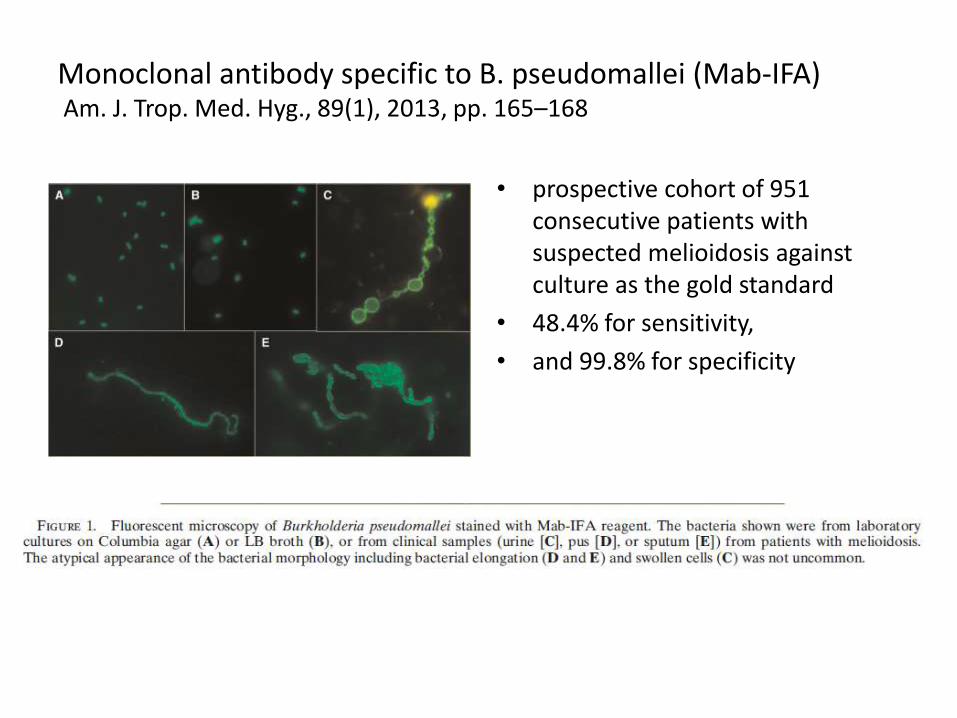
Monoclonal antibody specific to B. pseudomallei (Mab-IFA) Am. J. Trop. Med. Hyg., 89(1), 2013, pp. 165–168
• prospective cohort of 951 consecutive patients with suspected melioidosis against culture as the gold standard
• 48.4% for sensitivity,
• and 99.8% for specificity
Management
Management & Prevention
• Improved diagnostics and training of health care workers
• Intensive treatment and mantainace with follow ups – Aiming for cure of meliodosis
• Among Laboratory workers – Awareness – Using biosafety cabinets as recommended to be used; standard
precautions – Prophylaxis in exposed individuals
• Vaccine research
• Soil testing, awareness among patient population
Treatment
Prevention & Vaccine
• Potentially preventable, but no evidence for development of guidelines for prevention
• Recommended for high risk:
– Stay indoors during monsoon /wind/rain
• Aerosolisation avoid
• No evidence to support human-to-human transmission through respiratory route
• No vaccine available to date
– Research
• Using live attennuated, subunit, plasmid based, and killed whole –cell candidates

Preventive measures: Thailand
• Thailand Laos Melioidosis Network Meeting II
– 17 September 2012, meet twice a year
• Update from 2nd TLMNM - Melioidosis
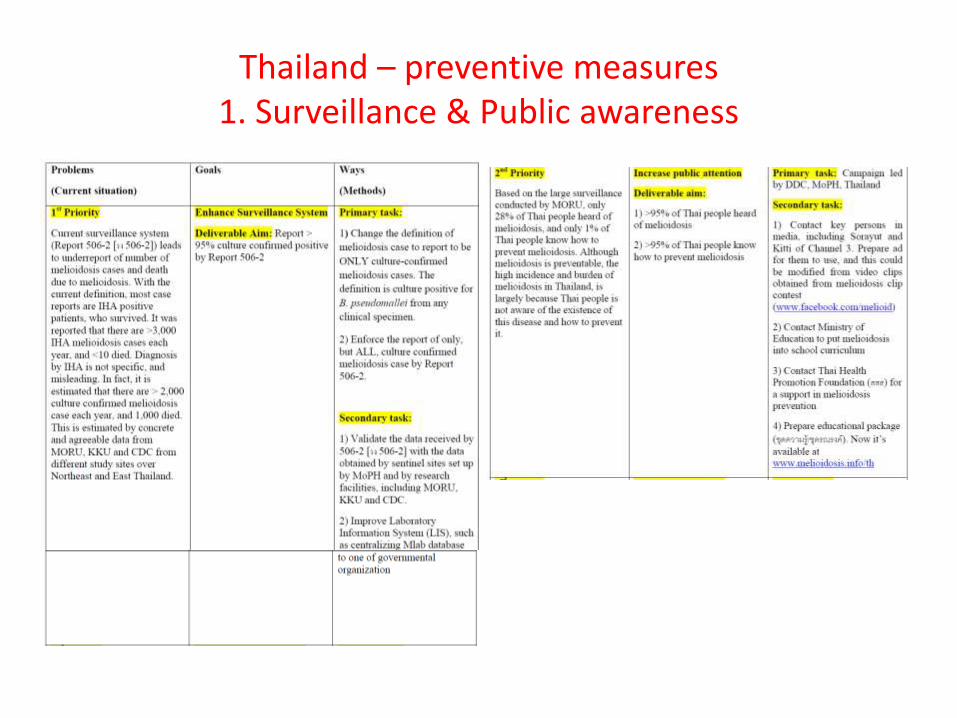
Thailand – preventive measures 1. Surveillance & Public awareness
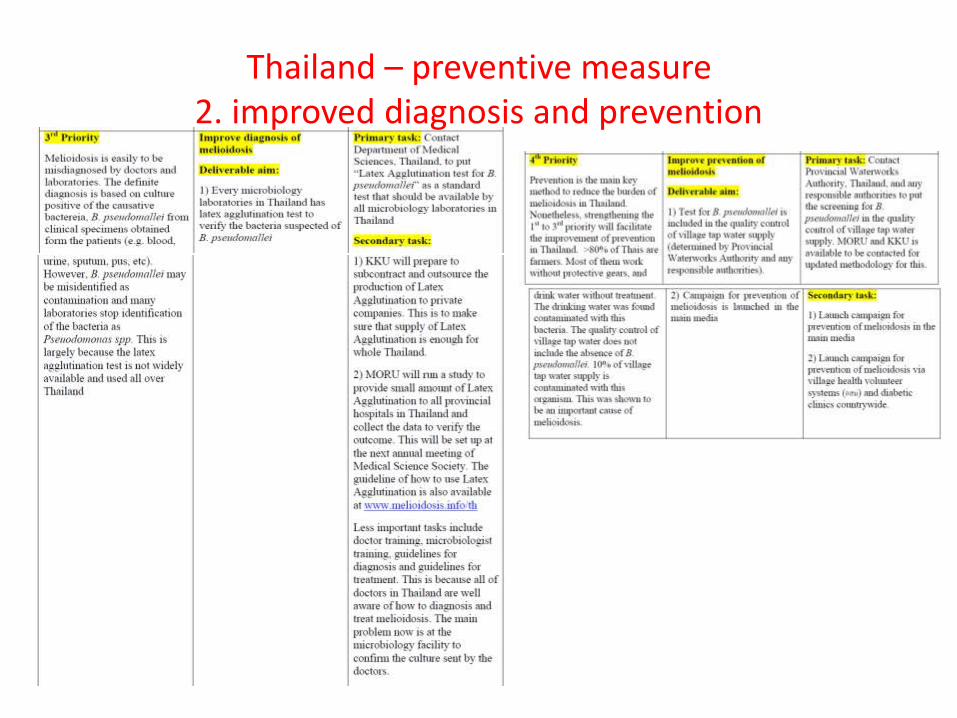
Thailand – preventive measure2. improved diagnosis and prevention
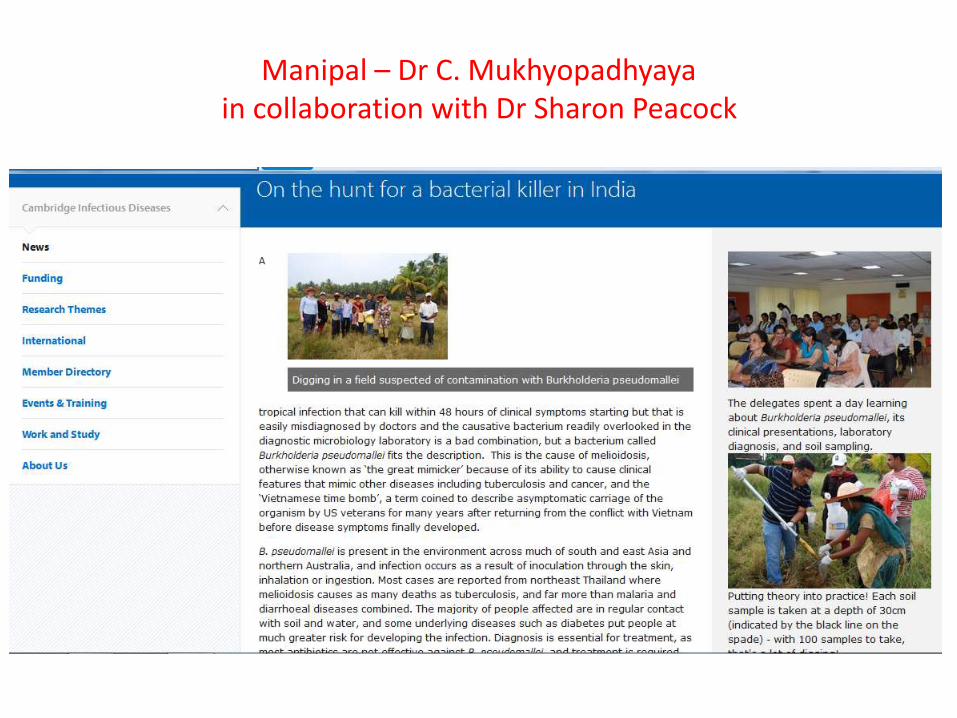
Manipal – Dr C. Mukhyopadhyayain collaboration with Dr Sharon Peacock

Mahidol university, Thailand
Major References
• Topley Wilson
• Mandel
• CMR – Melioidosis
• NEJM review2012
Acknowledgement
• Dr H. Srinivasa
• Dr Sharon Peacock
• Dr David Dance
Thank you