scompenso cardiaco, albuminuria e diabete mellitotigulliocardio.com/slide/mangili.pdf · scompenso...
TRANSCRIPT

Scompenso Cardiaco, Albuminuria e Diabete Mellito
Ruggero Mangili
Key points:
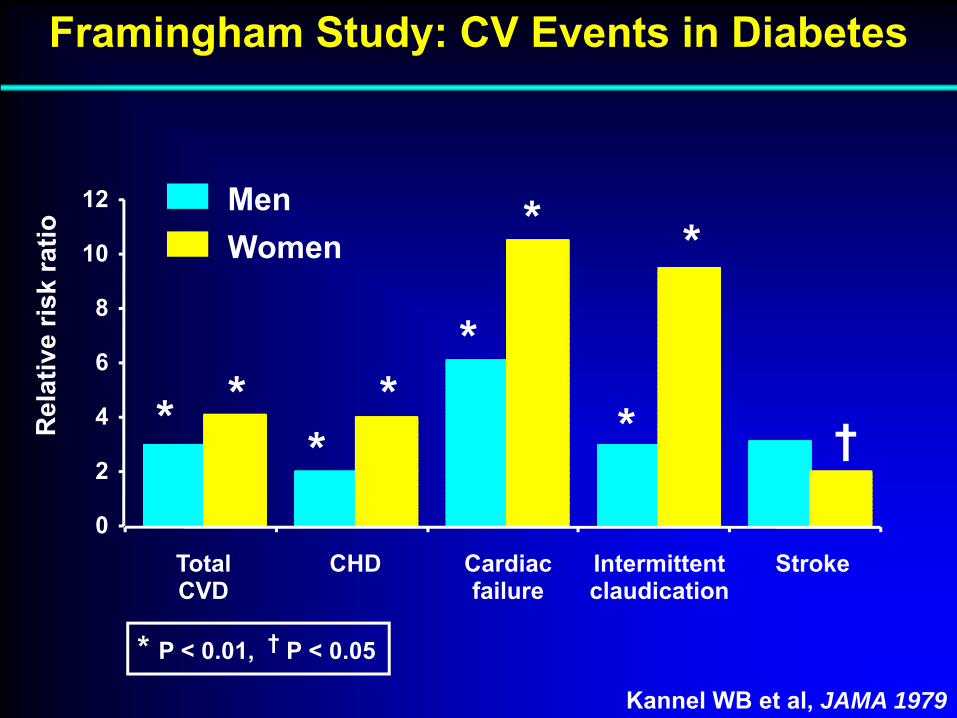
• 1‐ Diabetes begets excess heart failure (HF)
• 2‐ Raised AER is a risk factor for HF
• 3‐ Raised AER independently predicts death in HF
0
2
4
6
8
10
12
Intermittentclaudication
TotalCVD
CHD Cardiacfailure
Stroke
MenWomen
* **
**
*
*
*
†
Kannel WB et al, JAMA 1979
* P < 0.01, † P < 0.05
Framingham Study: CV Events in Diabetes
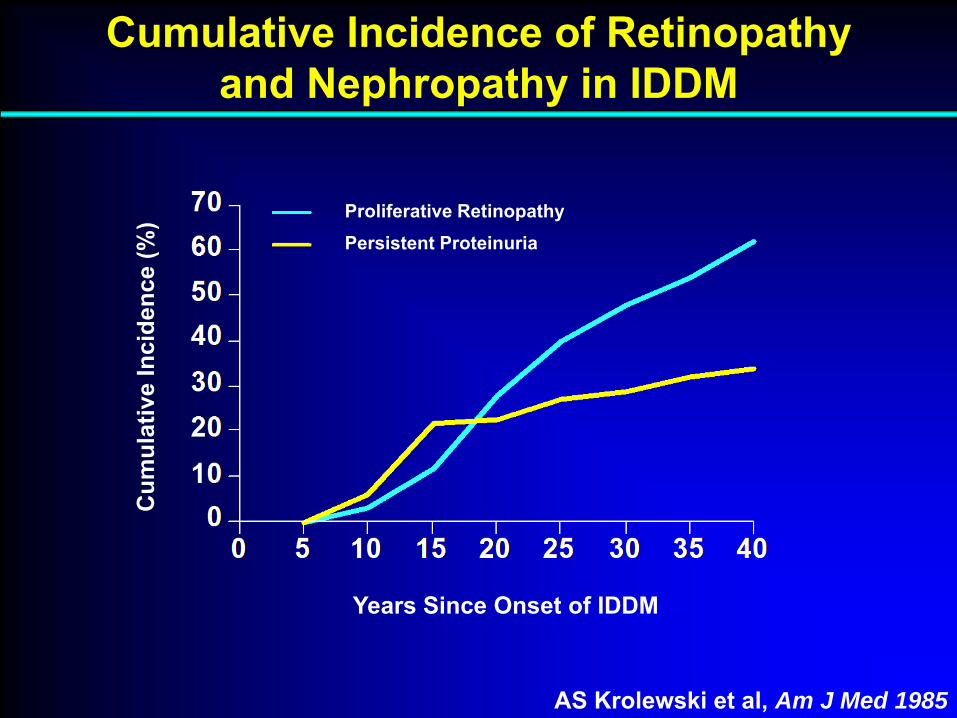
Years Since Onset of IDDM
Cum
ulat
ive
Inci
denc
e (%
) Proliferative RetinopathyPersistent Proteinuria
Cumulative Incidence of Retinopathyand Nephropathy in IDDM
AS Krolewski et al, Am J Med 1985
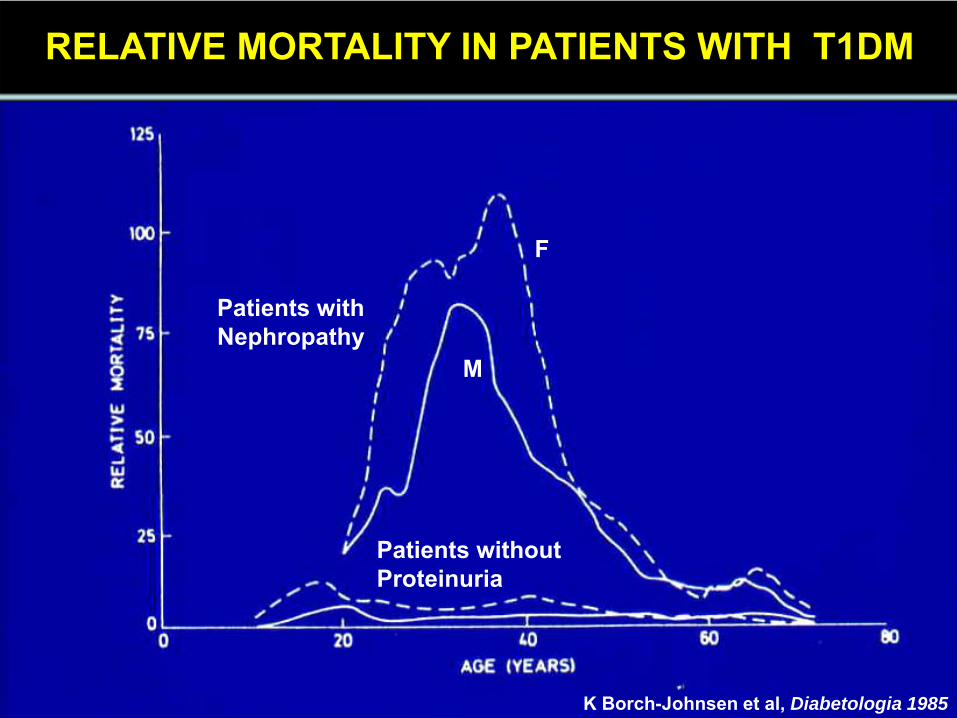
RELATIVE MORTALITY IN PATIENTS WITH T1DM
Patients with Nephropathy
Patients without Proteinuria
F
M
K Borch-Johnsen et al, Diabetologia 1985

The concomitants of raised blood sugar: studies in newly-detected hyperglycaemics. II. Urinary albumin excretion, blood pressure and their
relation to blood sugar levels.Keen H, Chlouverakis C, Fuller J, Jarrett RJ.
Guy’s Hosp Rep 118:247-54, 1969
Rosalyn Yalow1977 Nobel Prize
Harry KeenWHO Diabetes Committee
The Inception of Microalbuminuria
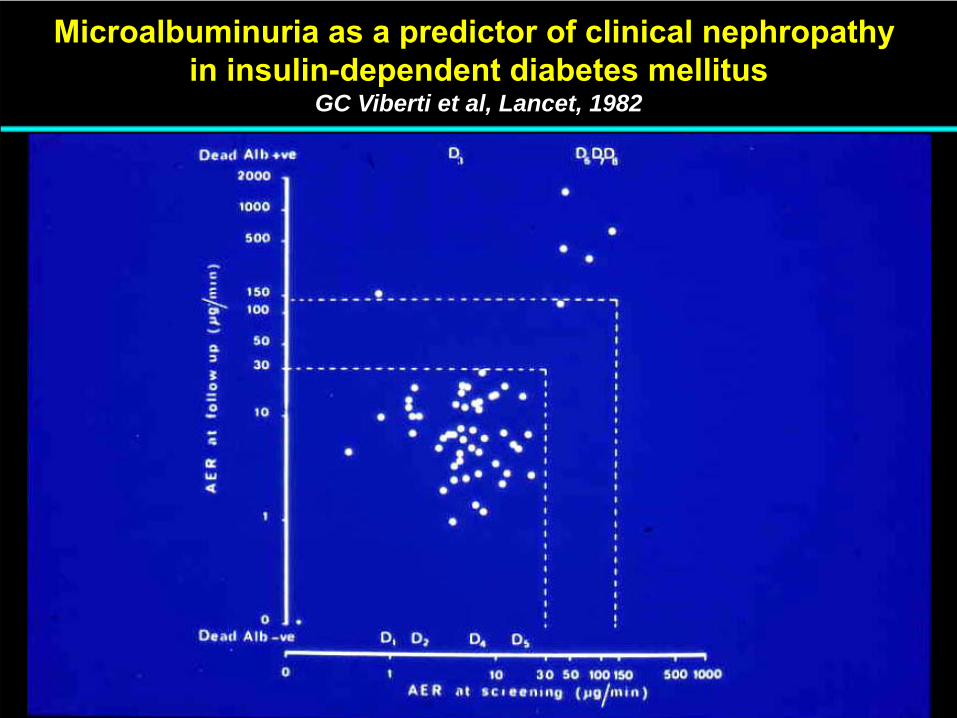
Microalbuminuria as a predictor of clinical nephropathy in insulin-dependent diabetes mellitus
GC Viberti et al, Lancet, 1982
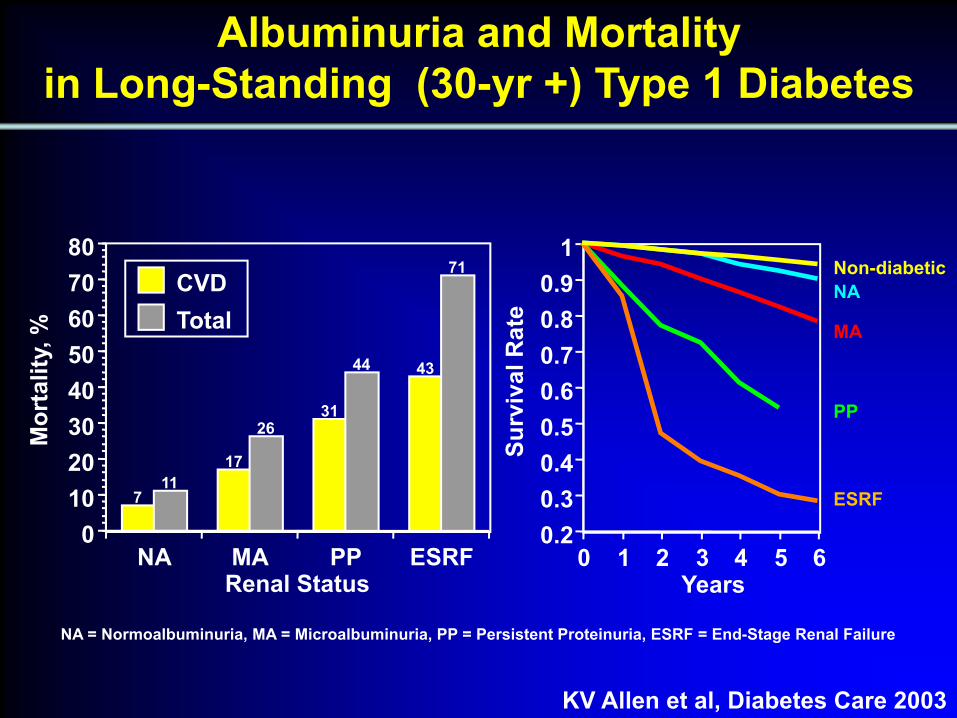
NA MA PP ESRF0
1020304050607080
Renal Status
711
17
2631
44 43
71CVDTotal
Albuminuria and Mortalityin Long-Standing (30-yr +) Type 1 Diabetes
0.20.30.40.50.60.70.80.9
1
0 1 2 3 4 5 6
NA
MA
PP
ESRF
Non-diabetic
Years
Surv
ival
Rat
e
NA = Normoalbuminuria, MA = Microalbuminuria, PP = Persistent Proteinuria, ESRF = End-Stage Renal Failure
KV Allen et al, Diabetes Care 2003
Mor
talit
y, %
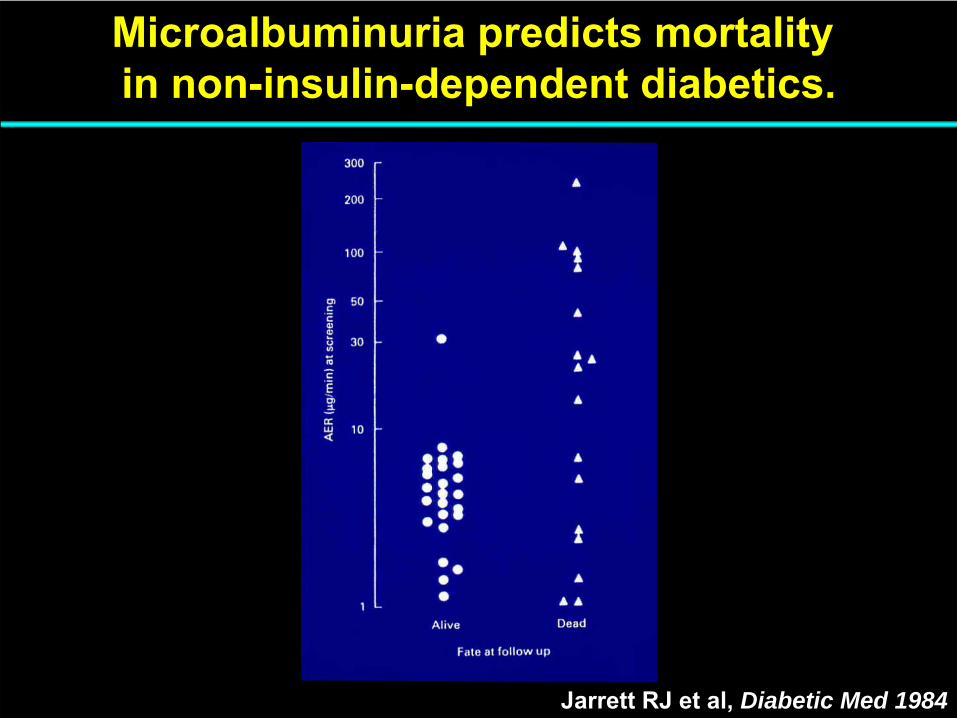
Jarrett RJ et al, Diabetic Med 1984
Microalbuminuria predicts mortality in non-insulin-dependent diabetics.
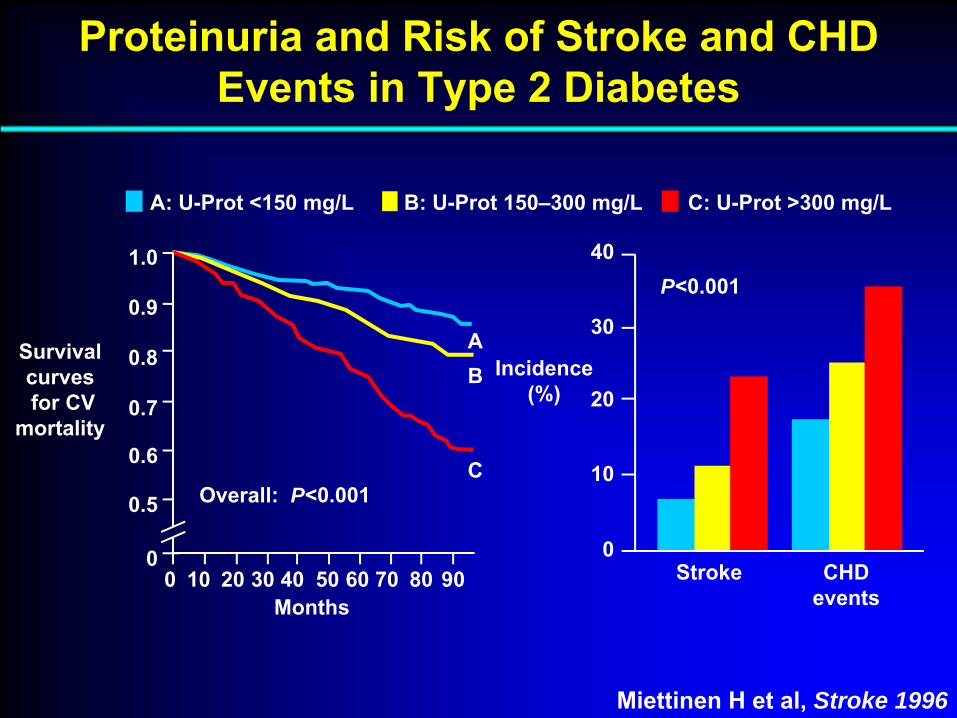
Proteinuria and Risk of Stroke and CHD Events in Type 2 Diabetes
1.0
0.9
0.8
0.7
0.6
0.5
00 10 20 30 40 50 60 70 80 90 Stroke CHD
events
P<0.001
Incidence (%)
Survival curvesfor CV
mortality
Months
AB
COverall: P<0.001
0
10
20
30
40
A: U-Prot <150 mg/L B: U-Prot 150–300 mg/L C: U-Prot >300 mg/L
Miettinen H et al, Stroke 1996
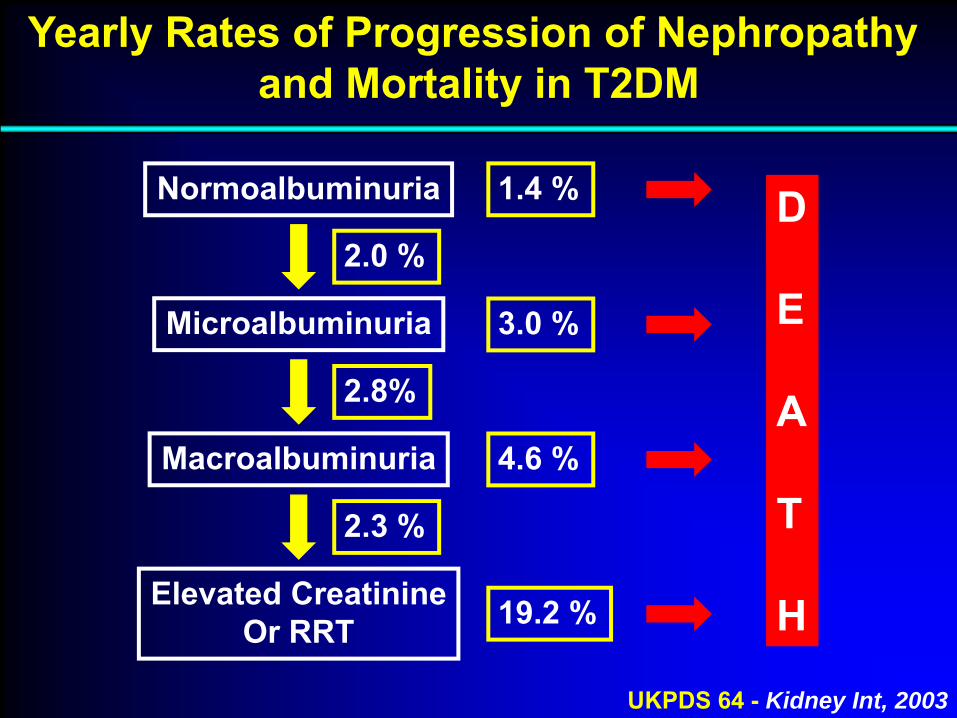
Yearly Rates of Progression of Nephropathy and Mortality in T2DM
UKPDS 64 - Kidney Int, 2003
D
E
A
T
H
2.0 %
2.8%
2.3 %
Elevated CreatinineOr RRT 19.2 %
Macroalbuminuria 4.6 %
Microalbuminuria 3.0 %
Normoalbuminuria 1.4 %
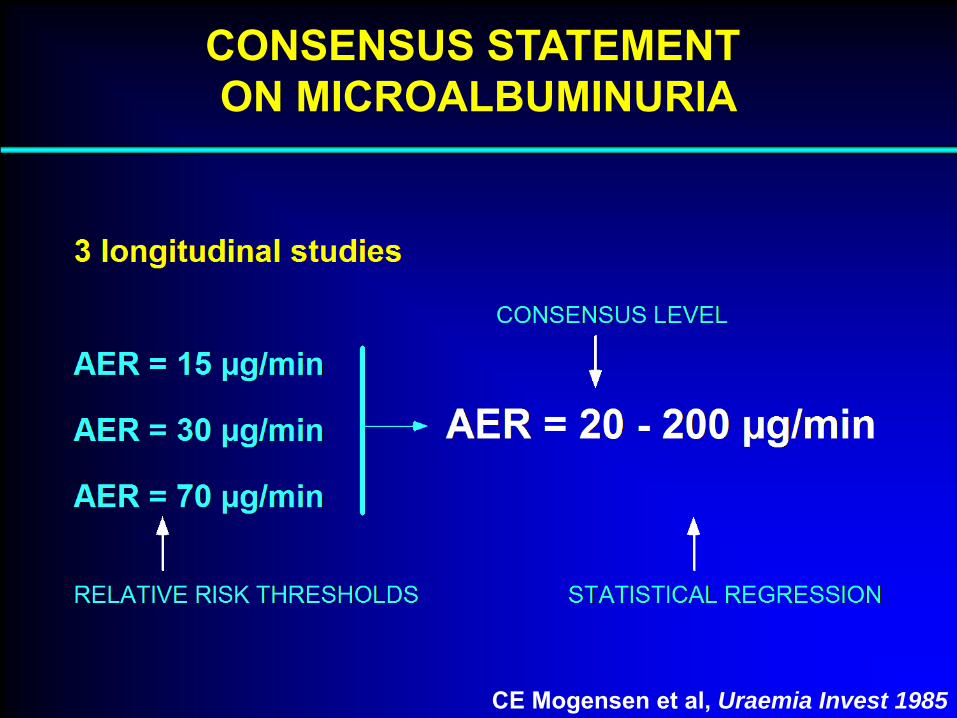
CONSENSUS STATEMENT ON MICROALBUMINURIA
CE Mogensen et al, Uraemia Invest 1985
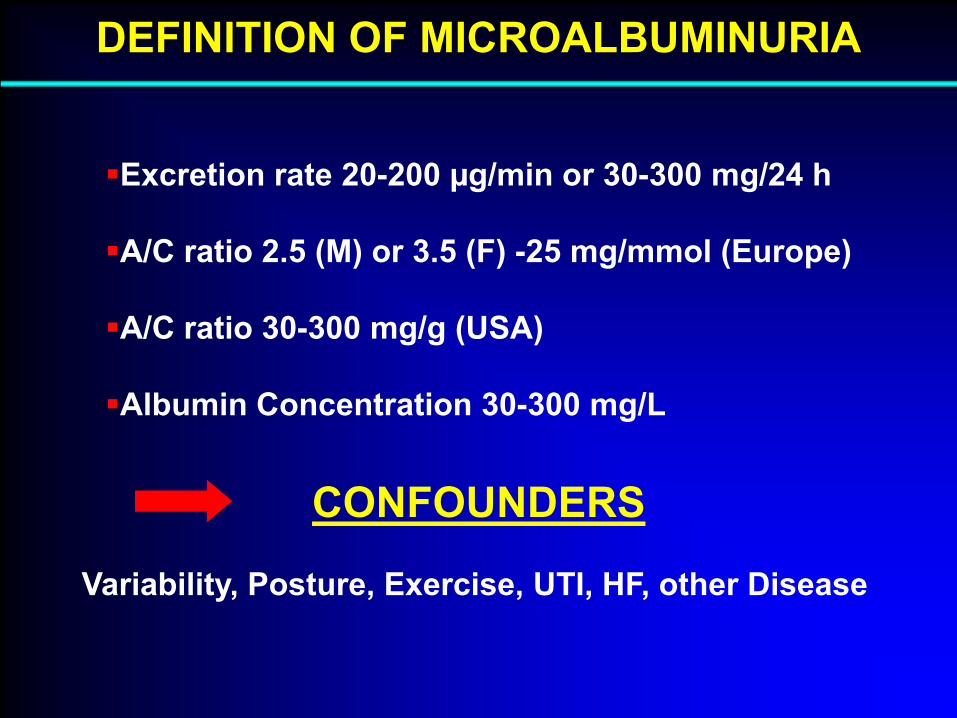
DEFINITION OF MICROALBUMINURIA
Excretion rate 20-200 µg/min or 30-300 mg/24 h
A/C ratio 2.5 (M) or 3.5 (F) -25 mg/mmol (Europe)
A/C ratio 30-300 mg/g (USA)
Albumin Concentration 30-300 mg/L
CONFOUNDERS
Variability, Posture, Exercise, UTI, HF, other Disease
Q 1:
Does hyperglycaemia beget heart failure?

0
2
4
6
8
10
12
Intermittentclaudication
TotalCVD
CHD Cardiacfailure
Stroke
MenWomen
* **
**
*
*
*
†
Kannel WB et al, JAMA 1979
* P < 0.01, † P < 0.05
Framingham Study: CV Events in Diabetes
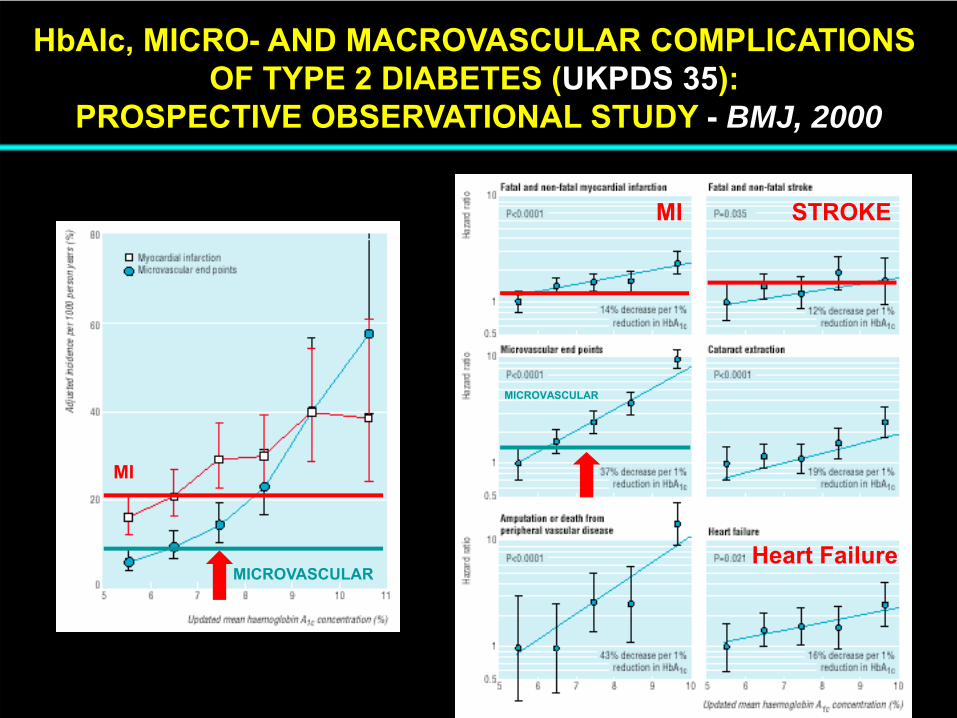
HbAIc, MICRO- AND MACROVASCULAR COMPLICATIONS OF TYPE 2 DIABETES (UKPDS 35):
PROSPECTIVE OBSERVATIONAL STUDY - BMJ, 2000
MI STROKE
MICROVASCULAR
MI
MICROVASCULAR
Heart Failure
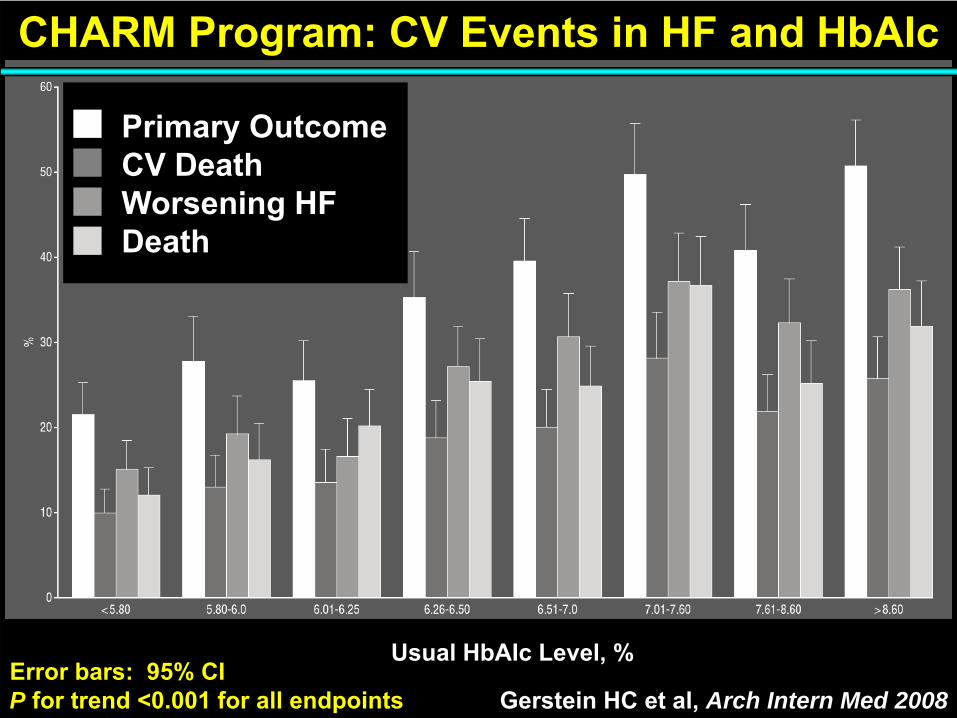
Usual HbAIc Level, %
CHARM Program: CV Events in HF and HbAIc
Gerstein HC et al, Arch Intern Med 2008
Primary OutcomeCV DeathWorsening HFDeath
Error bars: 95% CIP for trend <0.001 for all endpoints
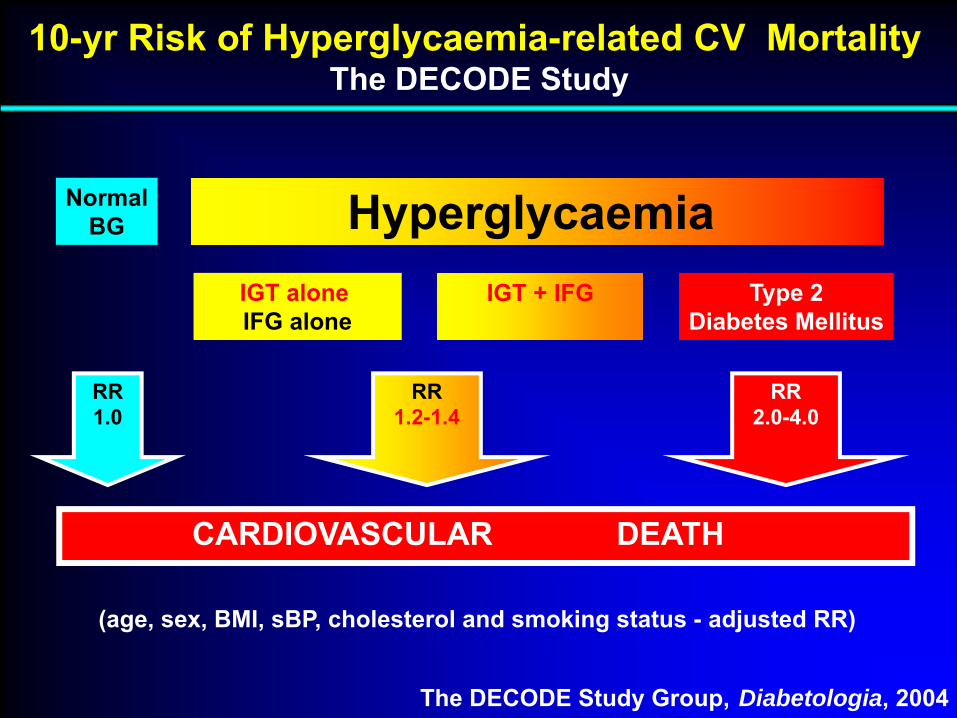
Type 2Diabetes Mellitus
IGT aloneIFG alone
NormalBG Hyperglycaemia
CARDIOVASCULAR DEATH
RR2.0-4.0
RR1.2-1.4
RR1.0
10-yr Risk of Hyperglycaemia-related CV MortalityThe DECODE Study
The DECODE Study Group, Diabetologia, 2004
(age, sex, BMI, sBP, cholesterol and smoking status - adjusted RR)
IGT + IFG
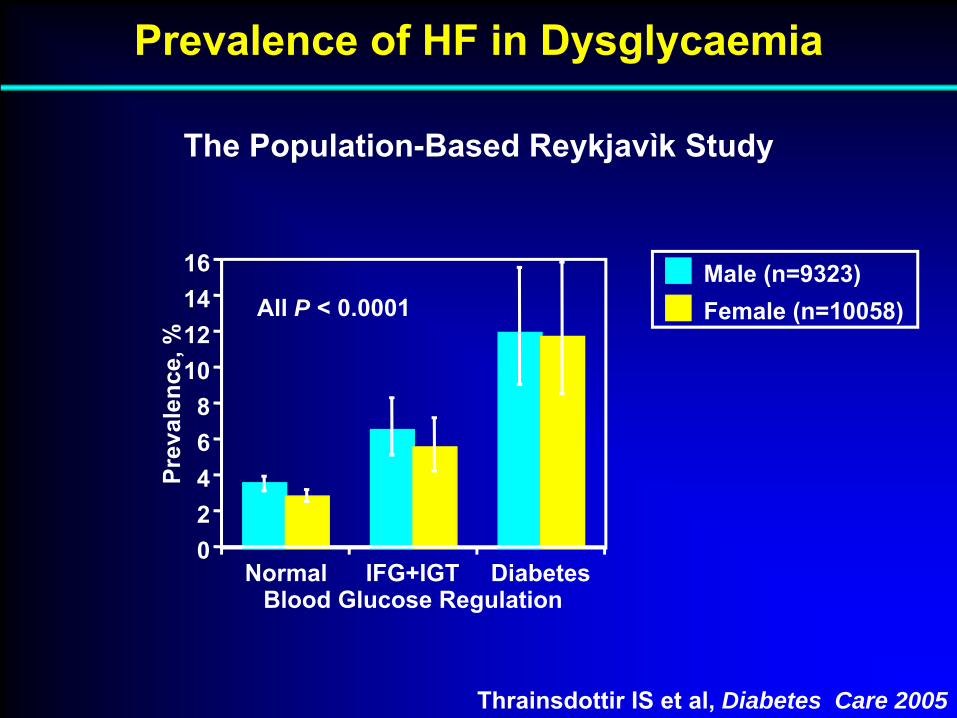
Prevalence of HF in Dysglycaemia
The Population-Based Reykjavìk Study
Normal IFG+IGT Diabetes02468
10121416
Prev
alen
ce, %
Blood Glucose Regulation
Male (n=9323)Female (n=10058)All P < 0.0001
Thrainsdottir IS et al, Diabetes Care 2005

Low-normal
High-normal
IFG
New DM
DM
0 0.5 1 1.5 2 2.5 3 3.5 4Age and Sex Adjusted Relative Risk
368 / 11708
24 / 1006
116 / 6650
91 / 6298
69 / 513
Events / Patient #
P for Trend < 0.0001
Held C et al, Circulation 2009
Glucose Levels and 4.5-yr Incidence of HF
The ONTARGET/TRANSCEND Cohort
Q 2:
Does microalbuminuria beget heart failure?
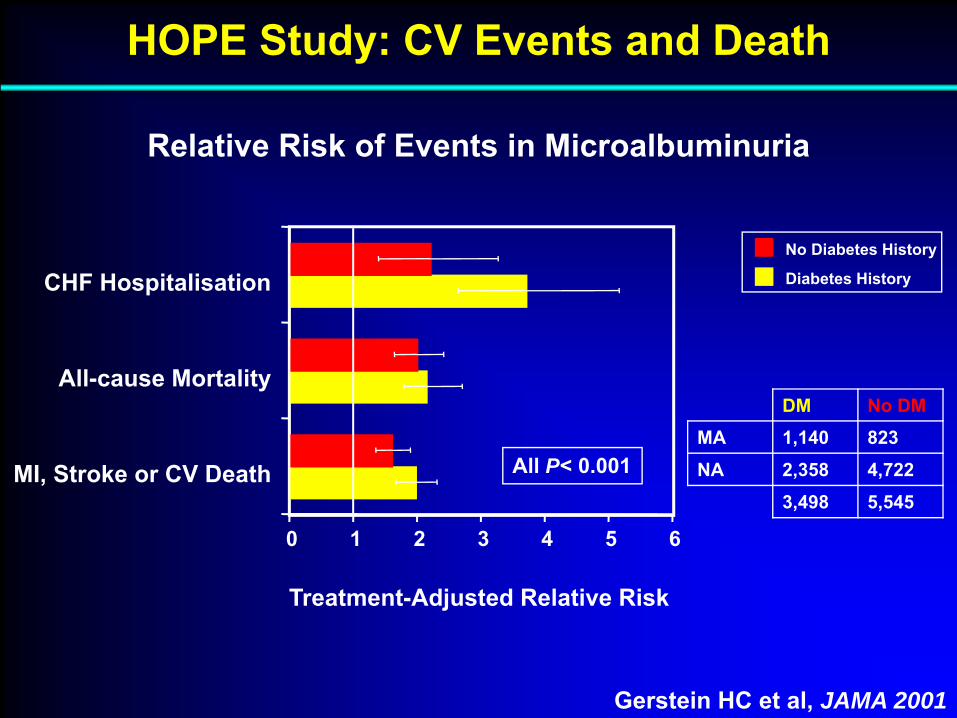
MI, Stroke or CV Death
All-cause Mortality
CHF Hospitalisation
HOPE Study: CV Events and Death
0 1 2 3 4 5 6
Diabetes History
No Diabetes History
Treatment-Adjusted Relative Risk
Gerstein HC et al, JAMA 2001
Relative Risk of Events in Microalbuminuria
DM No DMMA 1,140 823NA 2,358 4,722
3,498 5,545
All P< 0.001

HOPE Study: Incidence of HF by ACR
Gerstein HC et al, JAMA 2001
Incidence of Heart Failure Hospitalisation by ACR
Albumin to Creatinine Ratio Decile
%
ACR quartiledistribution:<0.220.22-0.570.58-1.62>1.62 mg/mmol
MICROALBUMINURIA
P for trend =0.05without MA only
for all participants
Q 3:
Is heart failure always ischemic in origin among patients with microalbuminuria?
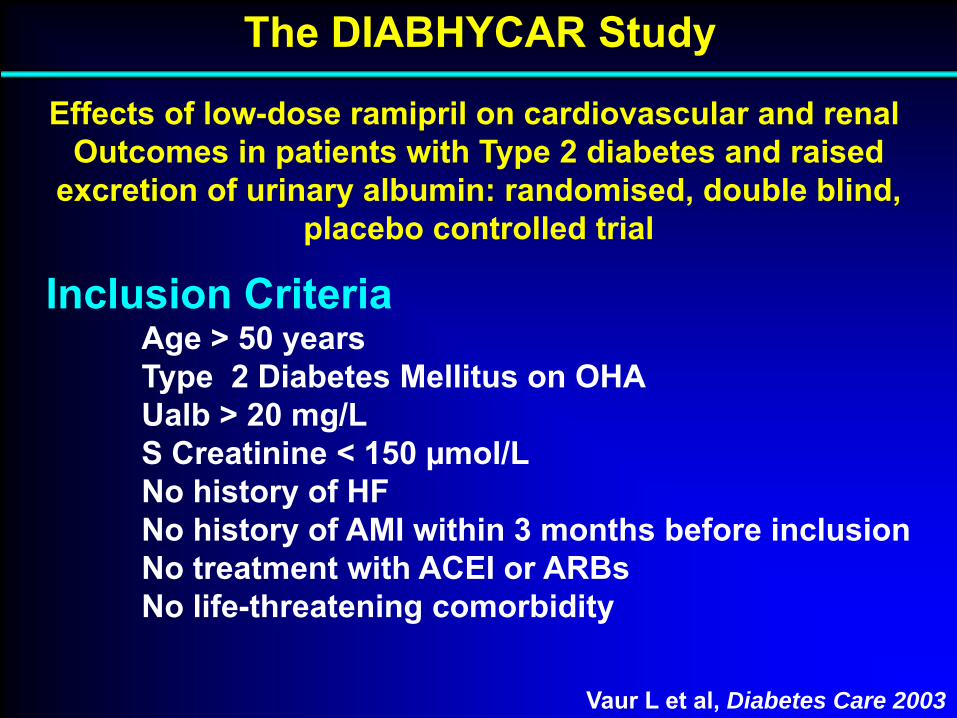
The DIABHYCAR Study
Vaur L et al, Diabetes Care 2003
Inclusion CriteriaAge > 50 yearsType 2 Diabetes Mellitus on OHAUalb > 20 mg/LS Creatinine < 150 µmol/LNo history of HFNo history of AMI within 3 months before inclusionNo treatment with ACEI or ARBsNo life-threatening comorbidity
Effects of low-dose ramipril on cardiovascular and renal Outcomes in patients with Type 2 diabetes and raised
excretion of urinary albumin: randomised, double blind,placebo controlled trial

The DIABHYCAR Study
Vaur L et al, Diabetes Care 2003
STUDY DESIGN4,937 patients randomised to 1.25 mg/day ramipril vs placebofollowed for 3-6 years
PRIMARY ENDPOINTCombined incidence of:
Cardiovascular deathNon-fatal AMIStrokeHF requiring hospital admissionESRF (requiring HD or RT)

Development of CHF Type 2 Diabetic Patientswith Microalbuminuria or Proteinuria
Observations from the DIABHYCAR Study
Vaur L et al, Diabetes Care 2003
187 of 4,912 patients
developed CHF during the study
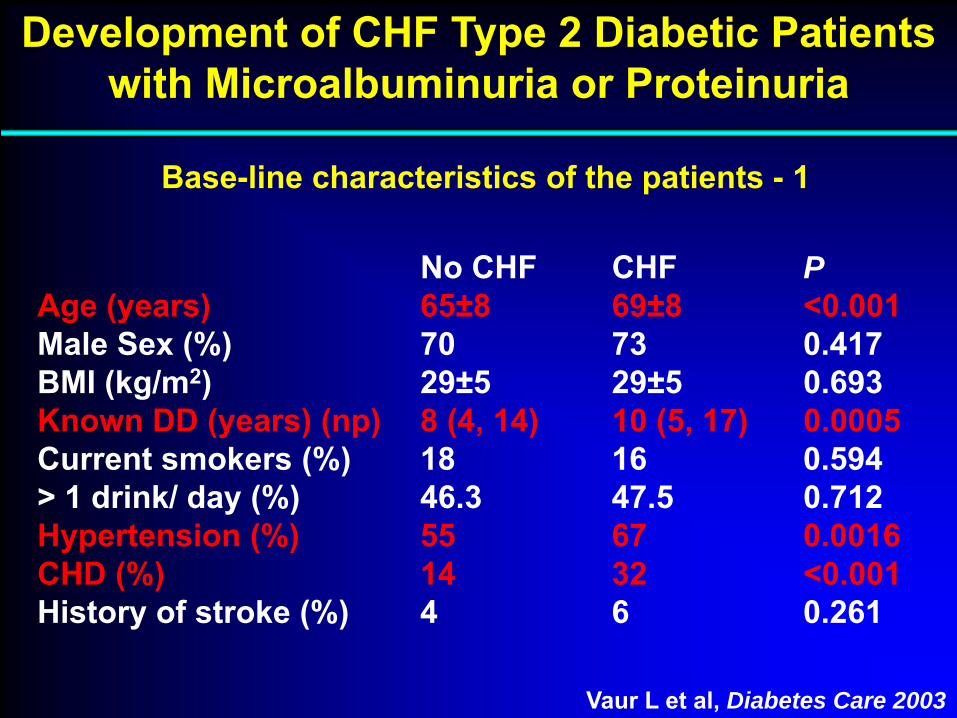
Development of CHF Type 2 Diabetic Patientswith Microalbuminuria or Proteinuria
Vaur L et al, Diabetes Care 2003
Base-line characteristics of the patients - 1
No CHF CHF PAge (years) 65±8 69±8 <0.001Male Sex (%) 70 73 0.417BMI (kg/m2) 29±5 29±5 0.693Known DD (years) (np) 8 (4, 14) 10 (5, 17) 0.0005Current smokers (%) 18 16 0.594> 1 drink/ day (%) 46.3 47.5 0.712Hypertension (%) 55 67 0.0016CHD (%) 14 32 <0.001History of stroke (%) 4 6 0.261

Development of CHF Type 2 Diabetic Patientswith Microalbuminuria or Proteinuria
Vaur L et al, Diabetes Care 2003
Base-line characteristics of the patients - 2
No CHF CHF PHistory of PVD (%) 10 23 <0.001sCreatinine (µmol/L) 89±20 96±21 <0.001Fasting BG (mmol/L) 9.8±3.2 9.8±3.1 0.926HbAIc (%) 7.9±1.8 8.3±1.9 0.0032UAC>200 mg/L (%) 25 44 <0.001UAC mg/L (np) 74 (37, 206) 155 (48, 493) 0.0001sBP (mm Hg) 145±15 148±16 0.045dBP (mm Hg) 82±9 82±8 0.831Ramipril treatment (%) 49.9 45.5 0.232

Vaur L et al, Diabetes Care 2003
Characteristics of the patients at the onset of CHF
CHD No CHD P
N 101 86Age (years) 71±8 72±8 0.52Male Sex (%) 77 67 0.14Hypertension (%) 59 74 0.043Prior MI (%) 53 0 NAValvulopathy (%) 13 10 0.66LVEF<40% (%) (44 miss) 61 37 0.018Atrial fibrillation (%) 28 36 0.27
The DIABHYCAR StudySubgroup analysis of new CHF by coronary status
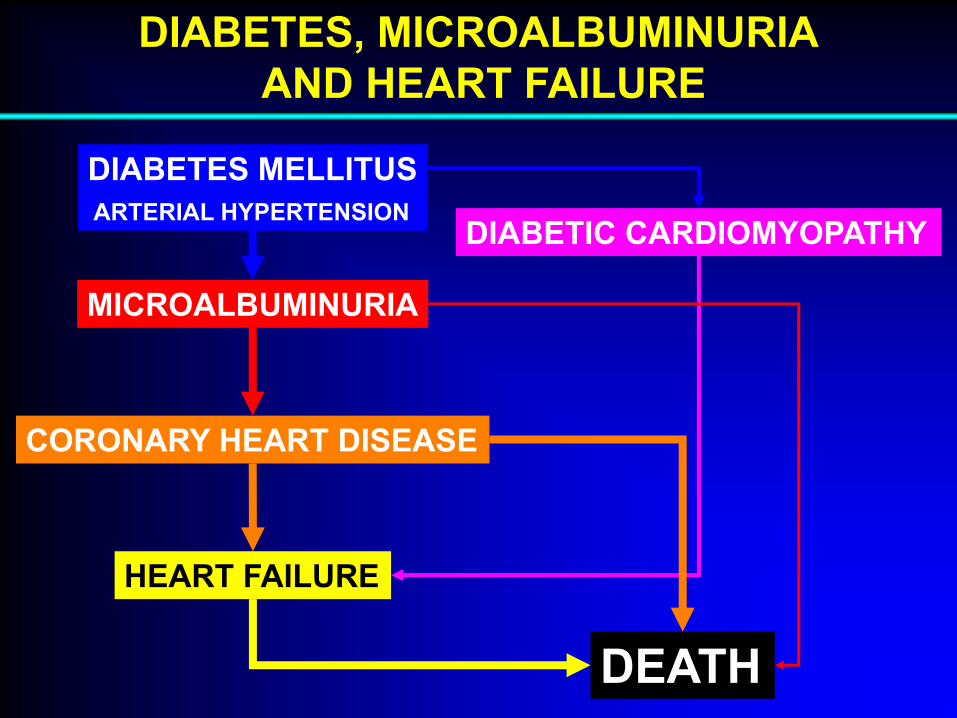
DIABETES MELLITUS
MICROALBUMINURIA
HEART FAILURE
DEATH
CORONARY HEART DISEASE
DIABETIC CARDIOMYOPATHYARTERIAL HYPERTENSION
DIABETES, MICROALBUMINURIAAND HEART FAILURE
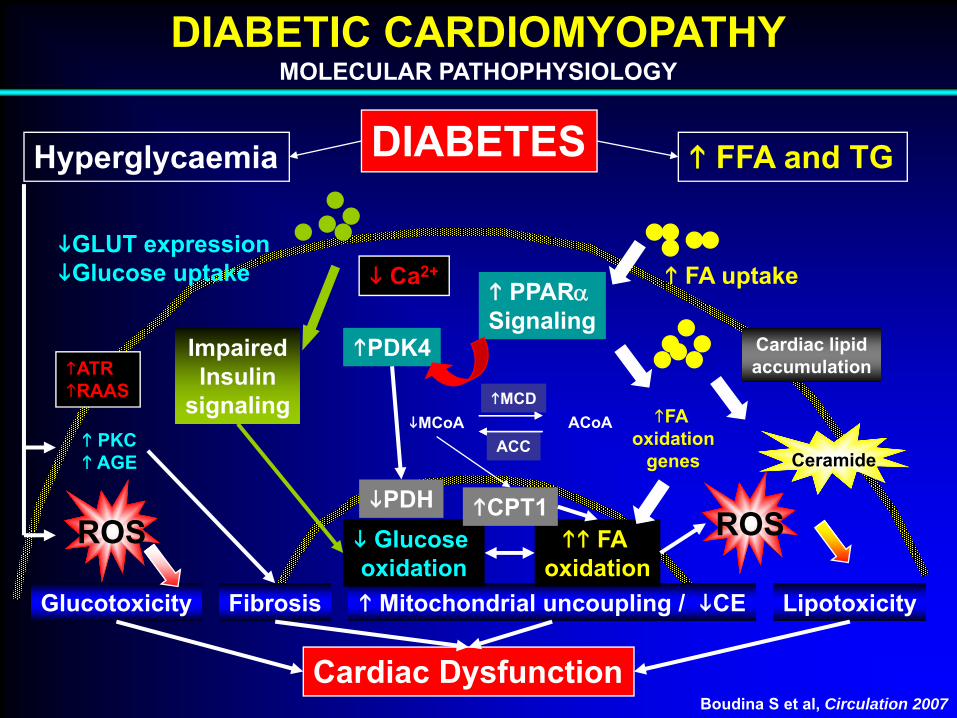
DIABETIC CARDIOMYOPATHYMOLECULAR PATHOPHYSIOLOGY
ImpairedInsulin
signaling
GLUT expressionGlucose uptake
Cardiac Dysfunction
Glucotoxicity Fibrosis Mitochondrial uncoupling / CE Lipotoxicity
Cardiac lipidaccumulation
FA uptake
Hyperglycaemia FFA and TGDIABETES
PPARαSignaling
PDK4
PKCAGE Ceramide
ROS ROSFA oxidation
Glucose oxidation
PDH CPT1
MCDMCoA
ACCACoA FA
oxidationgenes
Boudina S et al, Circulation 2007
ATRRAAS
Ca2+

THE STAGES OF DIABETIC CARDIOMYOPATHYEARLY STAGE
Fang ZY et al, Endocrine Reviews 2004
CharacteristicsDepletion of GLUT4Increased FFACarnitine deficiencyCa2+ homeostasis changesInsulin resistance
Functional featuresIf any, slight diastolic dysfunction but normal EF
Structural featuresNormal LV size, thickness and mass
Study methodsStrain rateMyocardial tissue velocity

THE STAGES OF DIABETIC CARDIOMYOPATHYMIDDLE STAGE
Fang ZY et al, Endocrine Reviews 2004
CharacteristicsApoptosis and necrosisIncreased AT IIReduced IGF-IIncreased TGF-β1Mild CAN
Functional featuresDiastolic dysfunction but normal or slightly EF
Structural featuresSlightly increased LV size, thickness or mass
Study methodsStrain rate, Myocardial tissue velocityConventional echocardiography
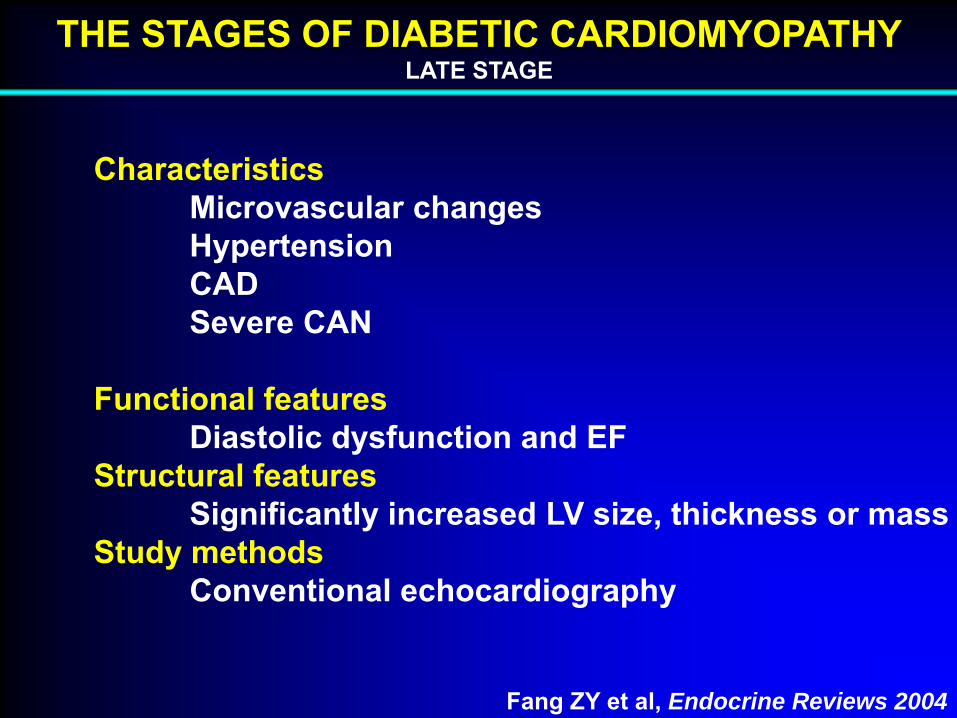
THE STAGES OF DIABETIC CARDIOMYOPATHYLATE STAGE
Fang ZY et al, Endocrine Reviews 2004
CharacteristicsMicrovascular changesHypertensionCADSevere CAN
Functional featuresDiastolic dysfunction and EF
Structural featuresSignificantly increased LV size, thickness or mass
Study methodsConventional echocardiography
Q 4:
Is microalbuminuria relevant to prognosisamong patients with heart failure?
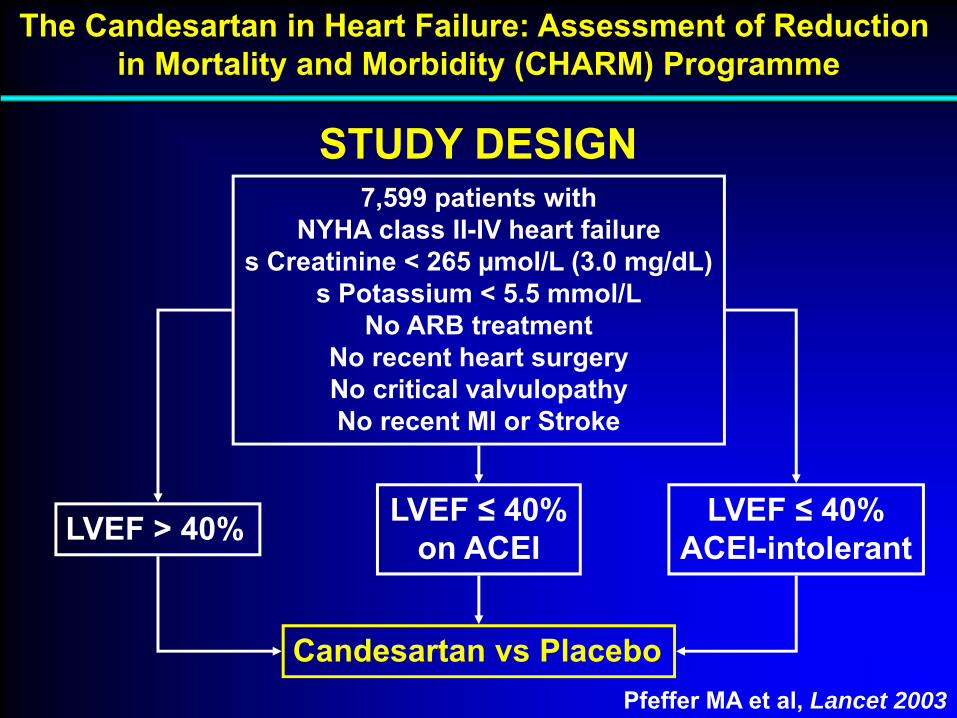
The Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) Programme
Pfeffer MA et al, Lancet 2003
STUDY DESIGN7,599 patients with
NYHA class II-IV heart failures Creatinine < 265 µmol/L (3.0 mg/dL)
s Potassium < 5.5 mmol/LNo ARB treatment
No recent heart surgeryNo critical valvulopathyNo recent MI or Stroke
LVEF > 40% LVEF ≤ 40%on ACEI
LVEF ≤ 40%ACEI-intolerant
Candesartan vs Placebo
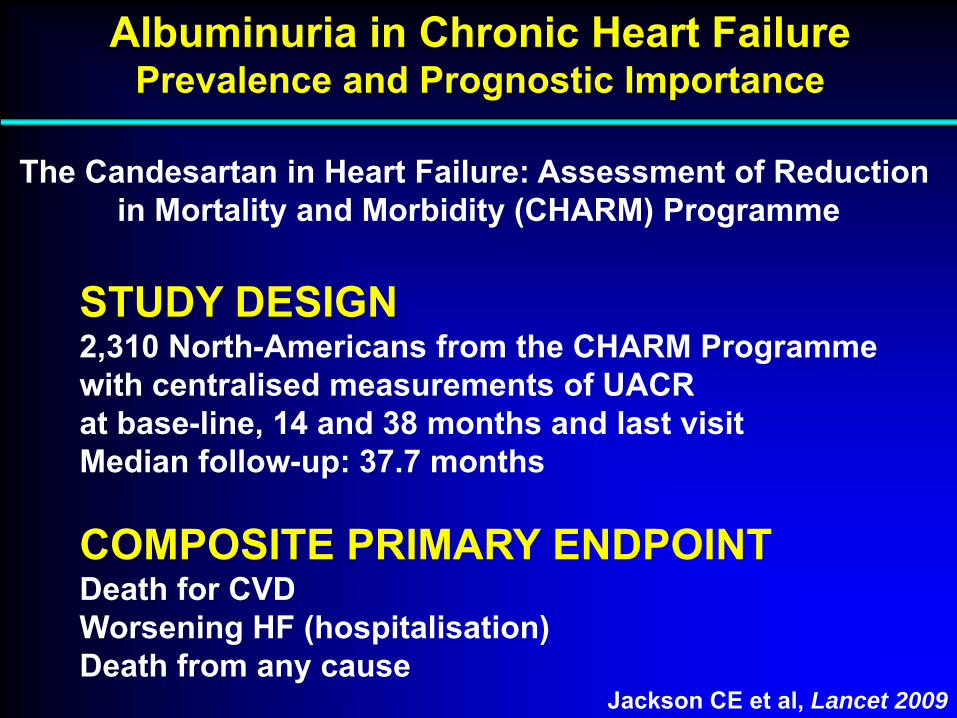
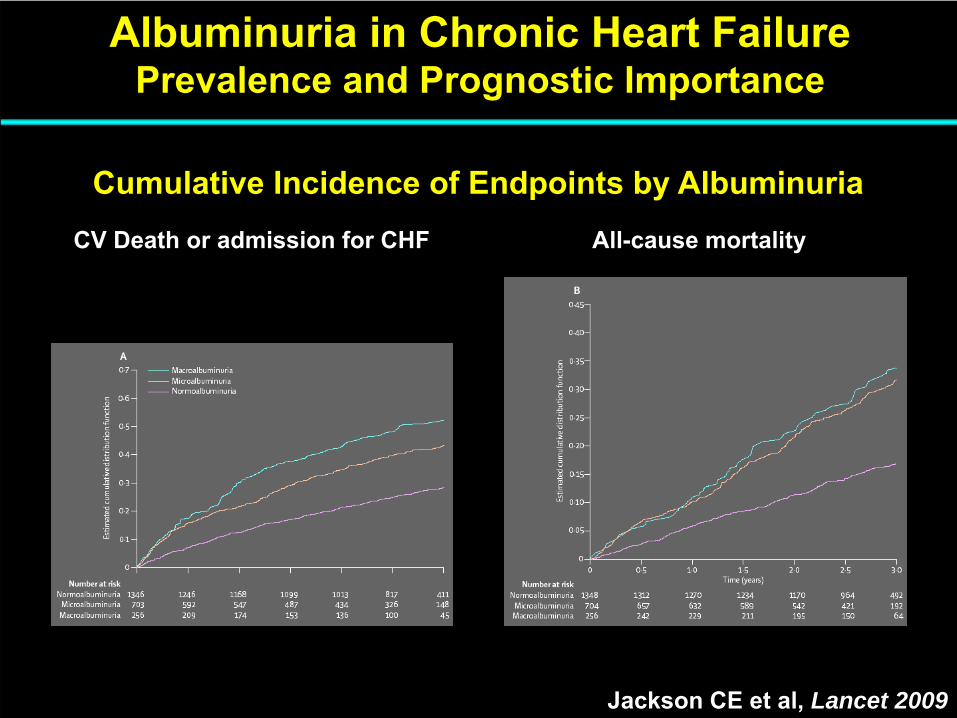
Albuminuria in Chronic Heart FailurePrevalence and Prognostic Importance
The Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) Programme
Jackson CE et al, Lancet 2009
STUDY DESIGN2,310 North-Americans from the CHARM Programmewith centralised measurements of UACRat base-line, 14 and 38 months and last visitMedian follow-up: 37.7 months
COMPOSITE PRIMARY ENDPOINTDeath for CVDWorsening HF (hospitalisation)Death from any cause

Albuminuria in Chronic Heart FailurePrevalence and Prognostic Importance
Jackson CE et al, Lancet 2009
Normo- Micro- Macro-0
10
20
30
40
50
60
70 All patients
No DM
No HT
No DM No HT
PREVALENCE OF RAISED ALBUMINURIA
MICROALBUMINURIA: UACR = 2.5/3.5 (M/W) -25.0 mg/mmolMACROALBUMINURIA: UACR > 25.0 mg/mmol
%
N = 1,447
N = 1,714
N = 796
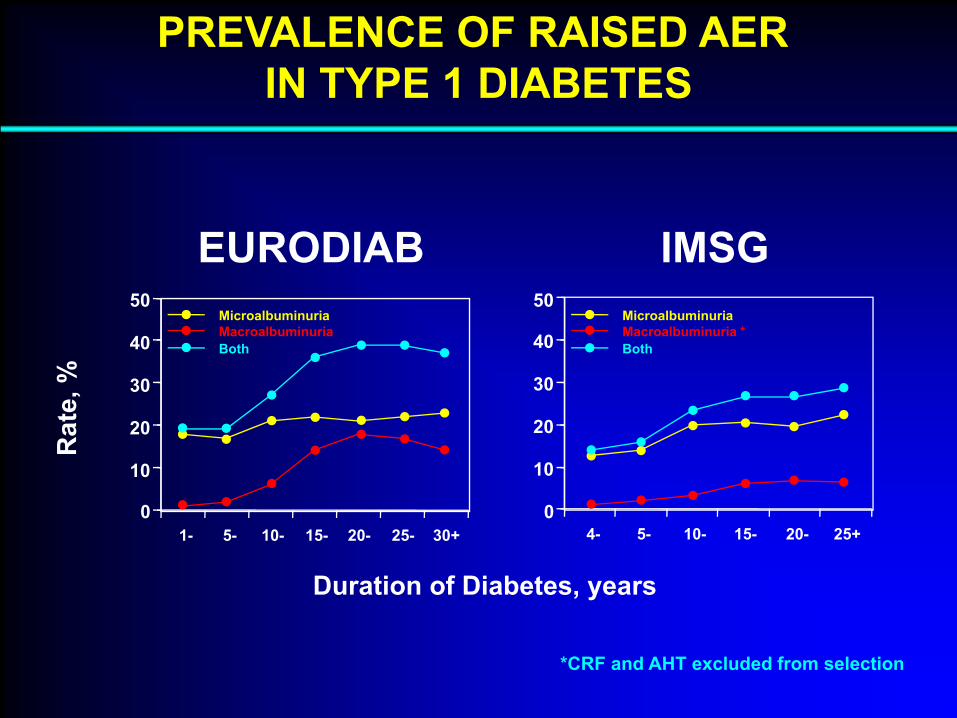
PREVALENCE OF RAISED AER IN TYPE 1 DIABETESR
ate,
%
Duration of Diabetes, years
0
10
20
30
40
50
1- 5- 10- 15- 20- 25- 30+
MicroalbuminuriaMacroalbuminuriaBoth
EURODIAB IMSG
0
10
20
30
40
50
5-4- 10- 15- 20- 25+
MicroalbuminuriaMacroalbuminuria *Both
*CRF and AHT excluded from selection
Albuminuria in Chronic Heart FailurePrevalence and Prognostic Importance
Jackson CE et al, Lancet 2009
CV Death or admission for CHF All-cause mortality
Cumulative Incidence of Endpoints by Albuminuria

Albuminuria in Chronic Heart FailurePrevalence and Prognostic Importance
Jackson CE et al, Lancet 2009
Multivariate Analysis of UACR with 33 Baseline Covariates
CV Death or CHFAll-cause mortalityAdmission for HF
* HR increase per 100 mg/mmol
Micro- vs NA Macro- vs NA UACR cont.*0
0.5
1
1.5
2
2.5
HR
P<0.0001 P<0.0001 P<0.02

Prevalence and Prognostic Value of Raised Urinary Albumin Excretion in Patients with Heart Failure
The GISSI-Heart Failure Trial
Masson S et al, Circ Heart Fail 2010
STUDY DESIGNRandomised ω-3 PUFA or rosuvastatin2,131 patients with heart failure and base-line ACR
PRIMARY ENDPOINTAll cause mortality
Prevalence and Prognostic Value of Raised Urinary Albumin Excretion in Patients with Heart Failure
The GISSI-Heart Failure Trial
Masson S et al, Circ Heart Fail 2010
PREVALENCE DATAMicroalbuminuria 19.9%Macroalbuminuria 5.4%
MAJOR FINDINGSOther RF-adjusted HR 1.12 (95% CI: 1.05-1.18) per 1 U increase log 10ACRboth in the study populationand in the subset without diabetes and hypertension
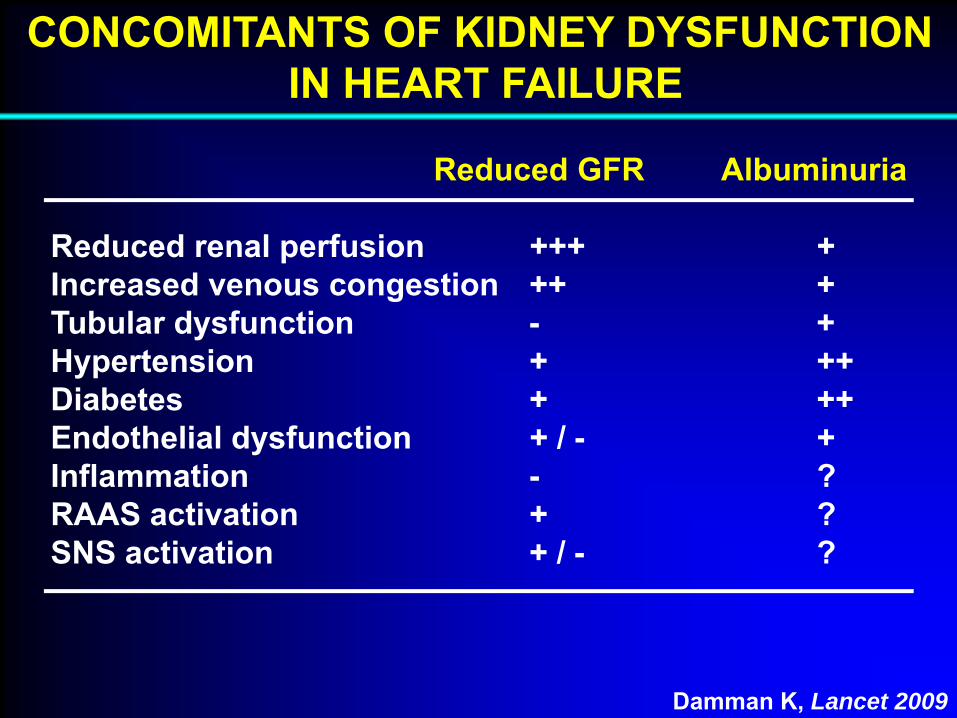
CONCOMITANTS OF KIDNEY DYSFUNCTIONIN HEART FAILURE
Reduced GFR Albuminuria
Reduced renal perfusion +++ +Increased venous congestion ++ +Tubular dysfunction - +Hypertension + ++Diabetes + ++Endothelial dysfunction + / - +Inflammation - ?RAAS activation + ?SNS activation + / - ?
Damman K, Lancet 2009

MICROALBUMINURIA 1969 - 2009:5400+ Papers - 9 Major Clinical Settings
Diabetes MellitusArterial HypertensionRenal Disease and TransplantationPre-eclampsiaSLEICBDHaemochromatosisNormotensive IndividualsHeart Failure
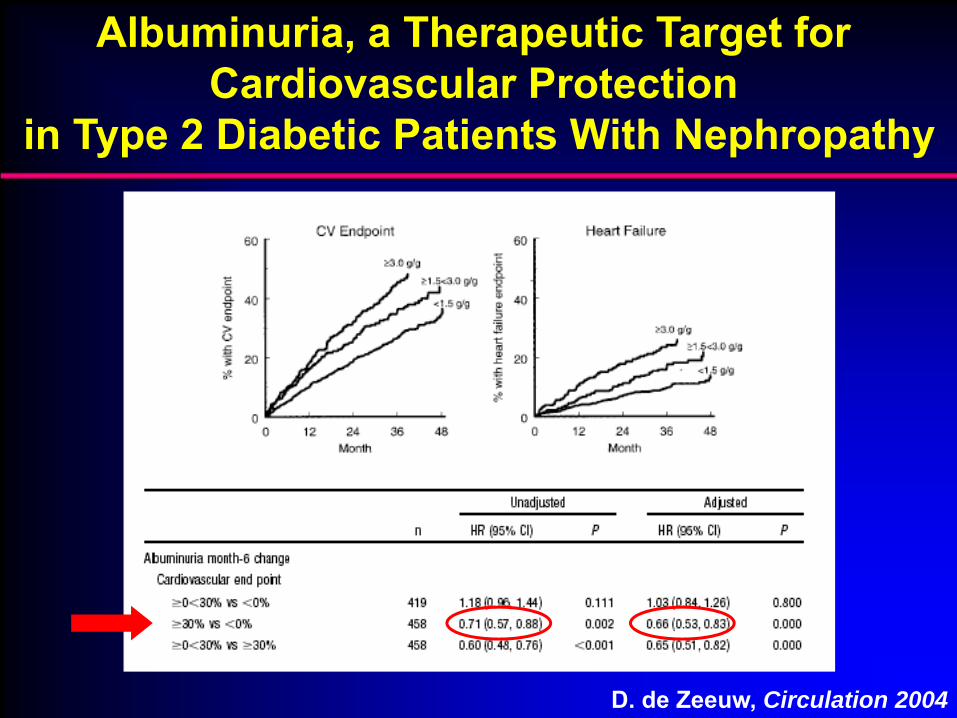
Albuminuria, a Therapeutic Target for Cardiovascular Protection
in Type 2 Diabetic Patients With Nephropathy
D. de Zeeuw, Circulation 2004