school mental health/ pbis integration: funding and policy nancy lever, center for school mental...
TRANSCRIPT

School Mental Health/PBIS Integration: Funding and Policy
Nancy Lever, Center for School Mental HealthMariola Rosser, IDEA Partnership
Joanne Cashman, IDEA PartnershipMark Weist, University of South Carolina
National PBIS Leadership ForumOctober 30, 2014
“Expanded” School Mental Health• Full continuum of effective mental health
promotion and intervention for students in general and special education
• Reflecting a “shared agenda” involving school-family-community system partnerships
• Collaborating community professionals (not outsiders) augment the work of school-employed staff
Advantages• Improved access• Improved early identification/intervention• Reduced barriers to learning, and
achievement of valued outcomes• WHEN DONE WELL
But• SMH programs and services continue to
develop in an ad hoc manner, and• LACK AN IMPLEMENTATION STRUCTURE
Positive Behavior Intervention and Support (www.pbis.org)
• In 18,000 plus schools• Decision making framework to guide best
practices for improving academic and behavioral functioning– Data based decision making– Measurable outcomes– Evidence-based practices– Systems to support effective implementation
Advantages• Promotes effective decision making• Reduces punitive approaches• Improves student behavior• Improves student academic performance• WHEN DONE WELL
But• Many schools implementing PBIS lack
resources and struggle to implement effective interventions at Tiers 2 and 3
Key Rationale• PBIS and SMH systems are operating separately• Results in ad hoc, disorganized delivery of SMH
and contributes to lack of depth in programs at Tiers 2 and 3 for PBIS
• By joining together synergies are unleashed and the likelihood of achieving depth and quality in programs at all three tiers is greatly enhanced
Tier 1 Tier 2 Tier 3
Mental Health
Education
Not two, but one
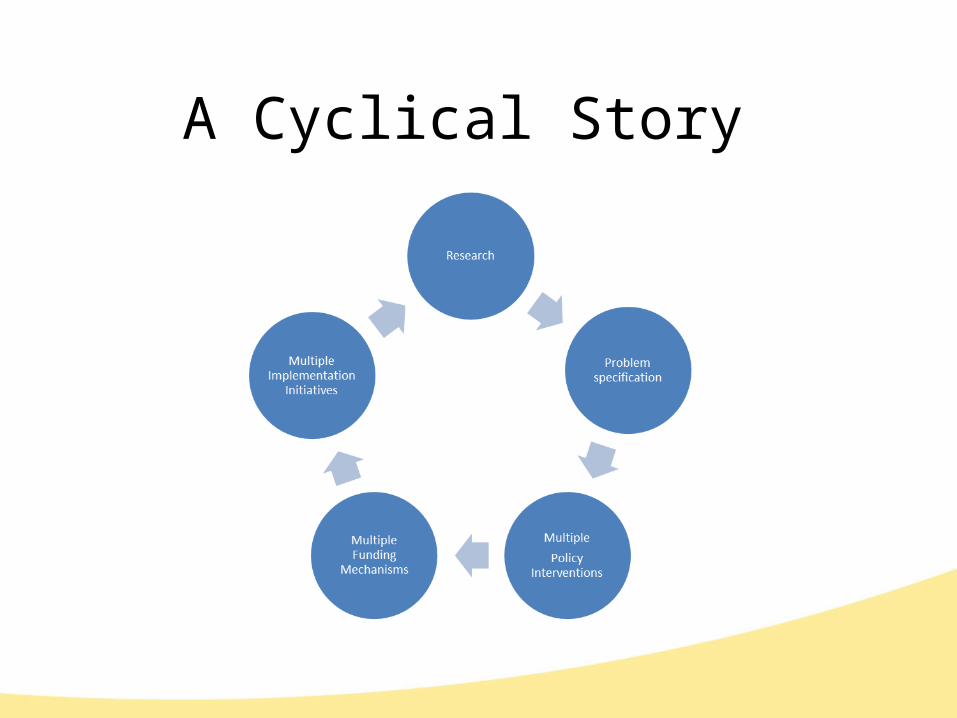
A Cyclical Story
Insights in the Cycle• Many agencies have goals related to behavioral
health• Each has specific initiatives aligned to its mission and
goals• Each initiative reaches a specific group of
implementers• Each is targeted to a specific unit for scale for
intervention: Federal, state, local, site, individuals• Sometimes implementers find their commonalities…
sometimes they don’t!
Emerging ApproachesNew insights link interventions at varying levels of scale
o New initiatives create interventions linking the state and local level
Safe Schools Healthy Students –State grant must include local pilots as a core feature
Project AWARE -State grant must include local pilots as a core feature
• New initiatives link MH and Education Interventionso Project AWARE grants required submission of the School Climate
Granto New Juvenile Justice grants will require similar coordination
A Word to the Wise …..
• Technical strategies to coordination and increased funding ‘open’ as we understand more about options that exist in policy
• Never forget…..people make it happen!
• We need a technical and an adaptive approach for real progress in practice!
Persistent Challenges
• Technical ChallengeRequires information, knowledge or tools
• Adaptive (Relationship) Challenges Requires understanding and a willingness to make behavior changes
Source: Heifetz and Linsky, Leadership on the Line, 2002
Learning that technical solutions are necessary but often not sufficient
Knowing when a persistent problem needs a adaptive (relationship) solution
Building adaptive (relationship) skills as a part of strategy
The Leadership Challenge
• Let’s explore some options for funding School Based Mental Health…
Funding Sources• School level
– Principal discretionary dollars– Funding from PTA/PTO for supplies/EBP purchase
• Local level– General Revenue (education purposes) – Categorical Revenue (targeted for specific for specific
student population in need of supplemental services– Tax levies– Private Foundations
• More Flexible with Prevention/Mental Health Promotion
– Community Businesses
State Funding
– Mental Health Block Grants– Grant Programs to develop SMH infrastructure
(Minnesota)– Children’s Health Insurance Program
• Provides health coverage to nearly eight million children in families with incomes too high to quality for Medicaid but who can’t afford private coverage
Federal Funding– Block Grants (fixed amount of funding based on
population, unemployment, and demographics)• Maternal and Child Health Block Grant• Social Services Block Grant• Preventive Health and Health Services Block Grant
– Project Grants – Discretionary grants awarded through a competitive process to fund discrete projects over a specified period of time
– Legislative Earmarks- Provide funding over one fiscal year and are not competitive
– Direct Payments (Medicaid) – Federal Assistance provided directly to individuals who meet eligibility requirements
Best Practice Funding Considerations• Use Diverse Funding Sources• Use Funding Strategies that Rely on Shared
Funding and Promote Sustainability– Braided/Pooled/Blended Funding– Increase reliance on more permanent
versus short-term funding• Leveraging of Funding• Return on Investment • Seed Money
Best Practice Funding Considerations (Cont.)
• Matching Funding to Service Delivery Across Multiple Tiers
• Utilize Evidence-Based Practices and Programs• Evaluate and Document Outcomes• Demonstrate Connections Between Mental Health
and Academic Functioning• Cross-Training and Sharing of Professional Development Expenses
EXAMPLES OF SCHOOL MENTAL FUNDING
SMH in Baltimore
• 1989: 4 schools• 2014: 114 schools
Serving elementary, middle, and high schools across the City of Baltimore
Led by 4 Outpatient Clinic Programs each Leading 1 Quadrant of the City’s SMH Services
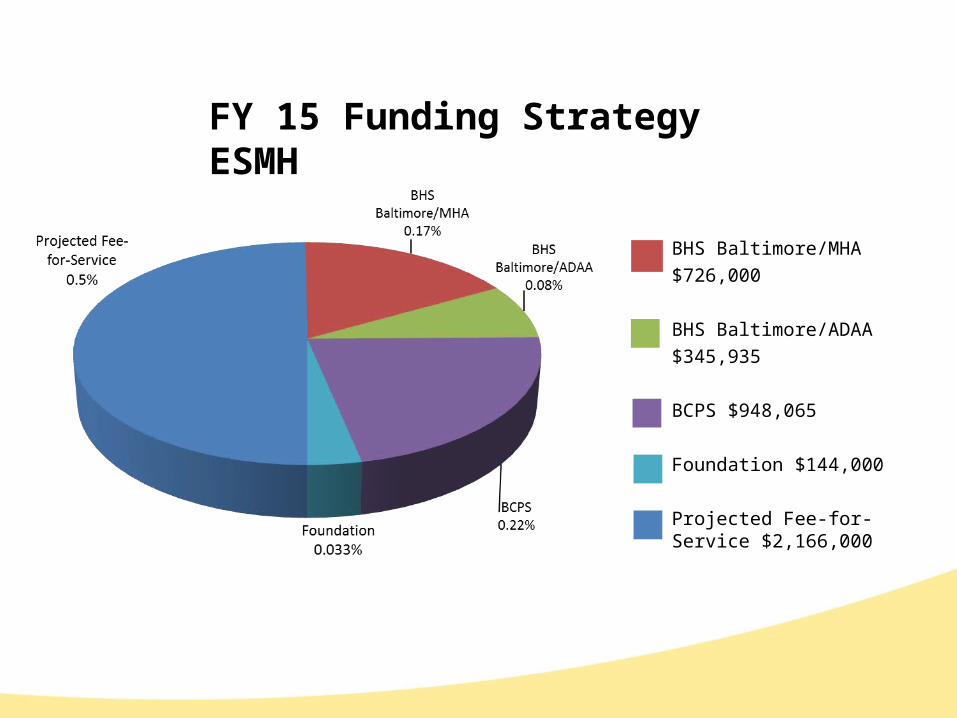
FY 15 Funding Strategy ESMH
BHS Baltimore/MHA $726,000
BHS Baltimore/ADAA $345,935
BCPS $948,065
Foundation $144,000
Projected Fee-for-Service $2,166,000
PGSMHI Goals
• Divert students who are at risk for entering non-public educational settings.
• Complement existing special education programs with a mental health component.
• Improve student functioning
• Improve school climate
• Increase knowledge of community resources
• Provide training and support to PGCPS school staff
PGSMHI Target Population and Enrollment • Students in Transition ED Programs who are at
risk of entering non-public settings due to an increase in behavioral and/or emotional problems
• Students in non-public settings who are returning to the Transition ED Programs
• 2013-2014 School Year: – 8 Schools (Elementary/Middle/High)– 160 enrolled– 495 students seen
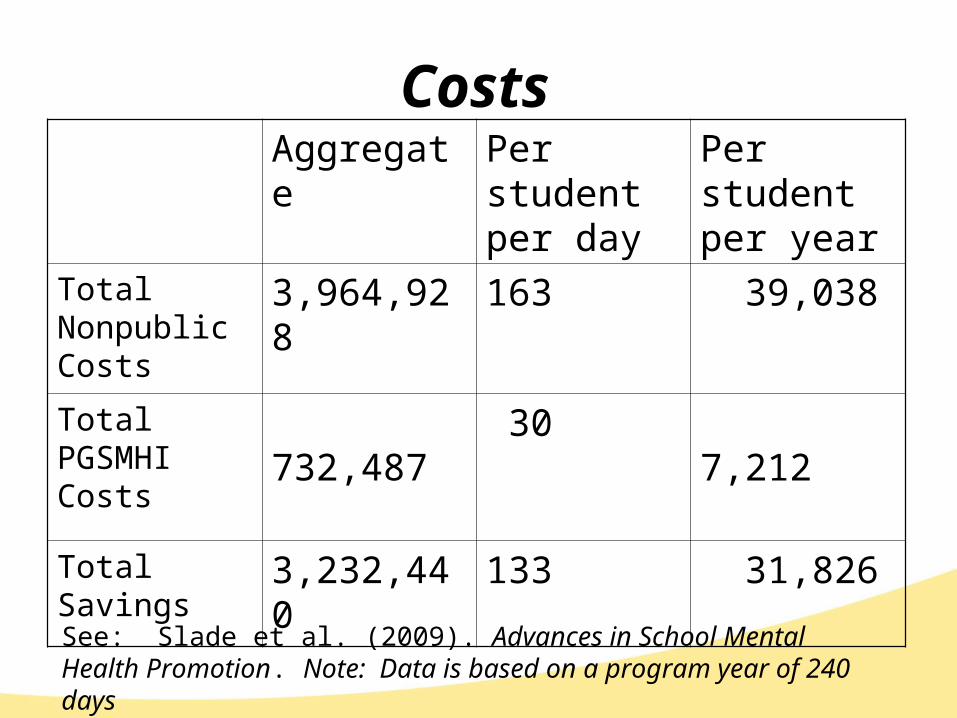
CostsAggregate Per student
per dayPer student per year
Total Nonpublic Costs
3,964,928 163 39,038
Total PGSMHI Costs
732,487 30 7,212
Total Savings 3,232,440 133 31,826
See: Slade et al. (2009). Advances in School Mental Health Promotion. Note: Data is based on a program year of 240 days
Syracuse Promise ZoneModel for Funding District Wide Mental
Health Supports April 7, 2014
Jennifer Parmalee, MPAOnondaga County Dept of Children & Family ServicesDirector of School Based Initiatives
Syracuse City School District Urban district in Central New York 95,000 residents 31 schools in the SCSD 5 High Schools
6 Kindergarten – 8th grade buildings6 Middle Schools (6th – 8th)10 Elementary Schools
21, 000 students75% Free and Reduced Lunch (4th highest in
state)20% Listed as Special Education Syracuse Promise Zone is a district wide
approach
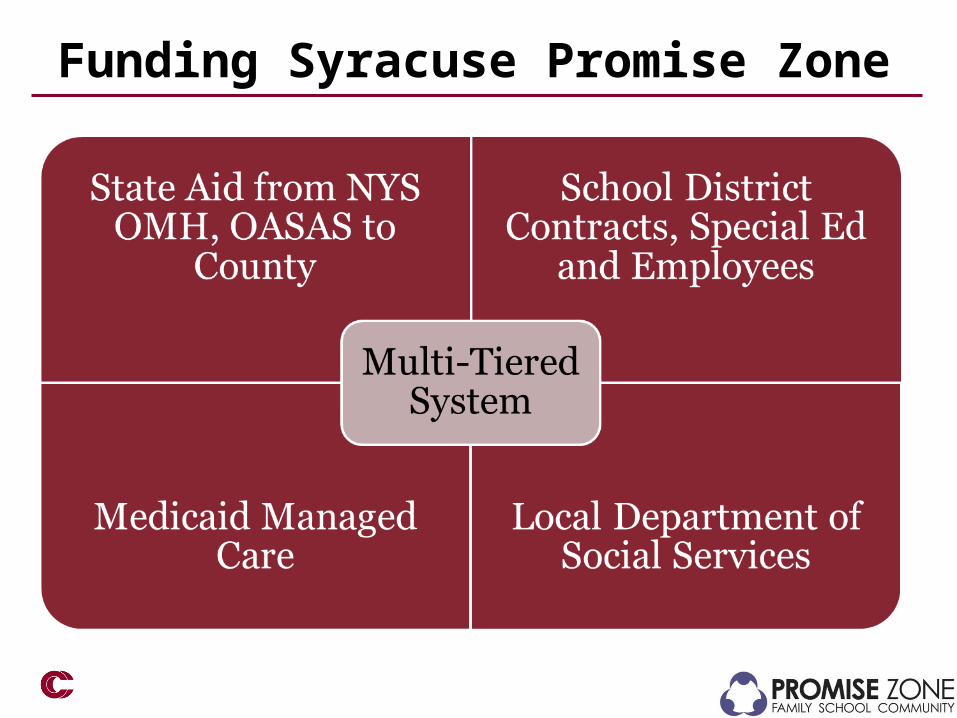
Funding Syracuse Promise Zone
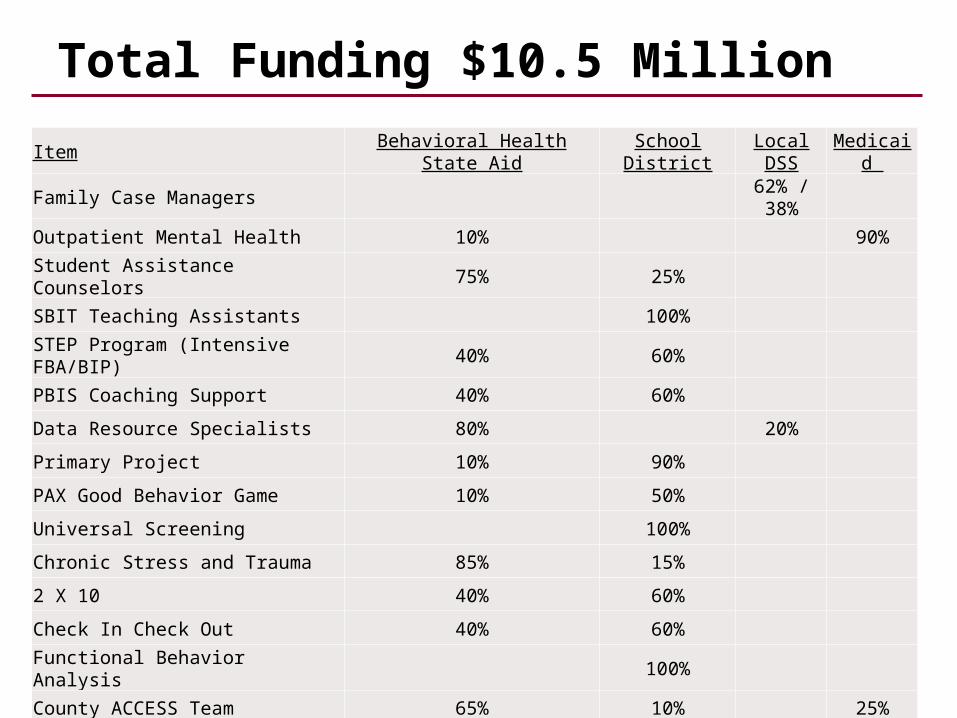
Total Funding $10.5 Million
ItemBehavioral Health State
AidSchool District
Local DSS
Medicaid
Family Case Managers62% / 38%
Outpatient Mental Health 10% 90%
Student Assistance Counselors 75% 25%
SBIT Teaching Assistants 100%STEP Program (Intensive FBA/BIP)
40% 60%
PBIS Coaching Support 40% 60%
Data Resource Specialists 80% 20%
Primary Project 10% 90%
PAX Good Behavior Game 10% 50%
Universal Screening 100%
Chronic Stress and Trauma 85% 15%
2 X 10 40% 60%
Check In Check Out 40% 60%
Functional Behavior Analysis 100%
County ACCESS Team 65% 10% 25%
Let’s look at the adaptive side of your funding effort using a tool from….
Leading By Convening: A Blueprint for Authentic Engagement
Four Simple Questions
34© 2014 Community Care Behavioral Health Organization
Convening in the Landscape of Practice on SBBH
• Coalescing around issuesAsk yourself: Who cares about this issue and why?
• Ensuring relevant participationAsk yourself: What work is already underway?
• Doing work together Ask yourself: What shared work could unite us?
• Leading by convening Ask yourself: Can you successfully lead on this issue without the other stakeholders? How can we deepen our connections?
Source: IDEA Partnership