risk of secondary cancer induced by radiotherapy
TRANSCRIPT
Risk of secondary cancer induced by radiotherapy
Iuliana Toma-Dasu
Medical Radiation Physics Stockholm University and Karolinska Institutet
Radiation - the two-edged sword
I. Toma-Dasu 2015
Risk of secondary cancer induced by radiotherapy – a cross cutting theme
The point of view of the medical physicist
How dangerous is a particular type of treatment ?
Is the risk from treatment A larger than the risk from treatment B?
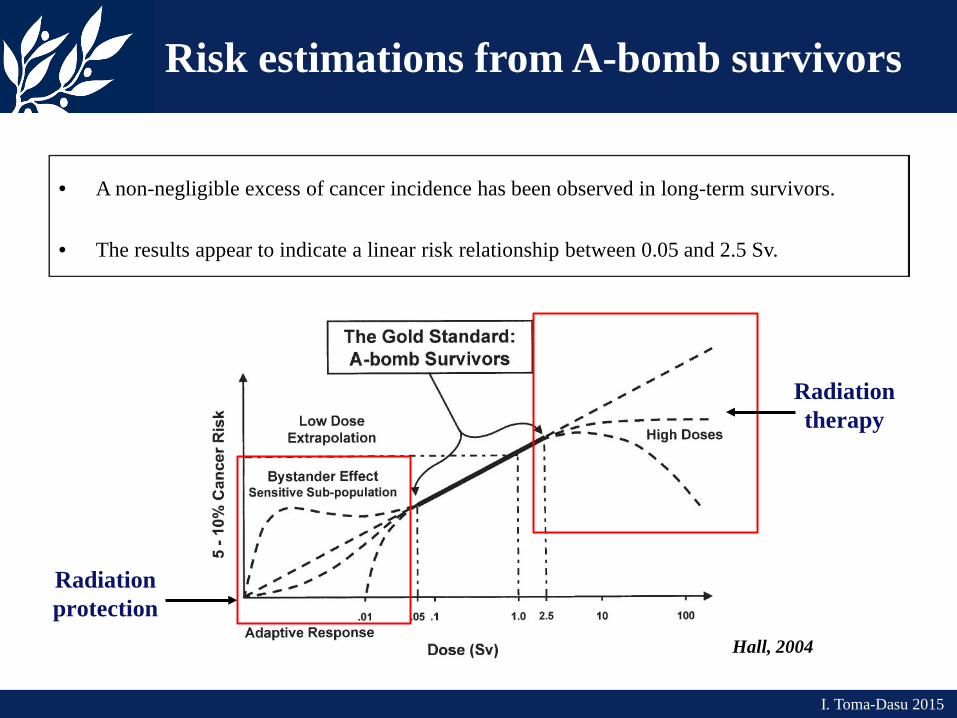
• A non-negligible excess of cancer incidence has been observed in long-term survivors.
• The results appear to indicate a linear risk relationship between 0.05 and 2.5 Sv.
Hall, 2004
Risk estimations from A-bomb survivors
I. Toma-Dasu 2015
Radiation protection
Radiation therapy
Risk of secondary cancer
I. Toma-Dasu 2015
• Extrapolations of risks from general populations to radiotherapy patients are
not straightforward. Age distribution and the genetic features of the patients may differ from
the general population.
• Best risk estimates would probably be obtained from long term survivors of radiotherapy. Control populations may be difficult to establish.
• Irradiation techniques have changed over the years.
The relevance of the results from 30-year old treatments to modern techniques is questionable.
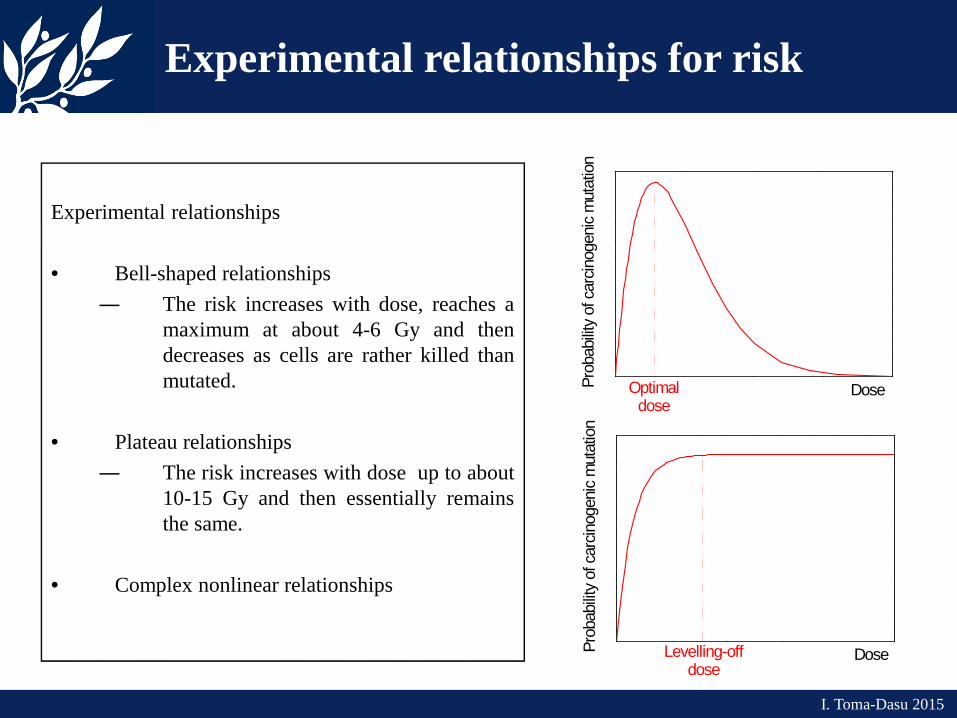
Experimental relationships • Bell-shaped relationships
― The risk increases with dose, reaches a maximum at about 4-6 Gy and then decreases as cells are rather killed than mutated.
• Plateau relationships ― The risk increases with dose up to about
10-15 Gy and then essentially remains the same.
• Complex nonlinear relationships
Experimental relationships for risk
I. Toma-Dasu 2015
Prob
abilit
y of
car
cinog
enic
mut
atio
n
DoseOptimaldose
Prob
abilit
y of
car
cinog
enic
mut
atio
n
DoseLevelling-offdose
I. Toma-Dasu 2015
Risk of secondary cancer
• It would be useful to use risk predictions as a complementary criterion for the selection of successful plans.
• Risk calculations however require reliable models and accurate parameters which
may not always be available from experimental studies!
• Most models aim to describe on mechanistic bases the shapes of the dose-response relationships for risk observed in epidemiological studies: UNSCEAR (1993, 2000)
Davis 2004, Dasu et al 2005, Sachs and Brenner 2005, Schneider 2005,
Schneider and Walsh 2008, Schneider 2009, etc
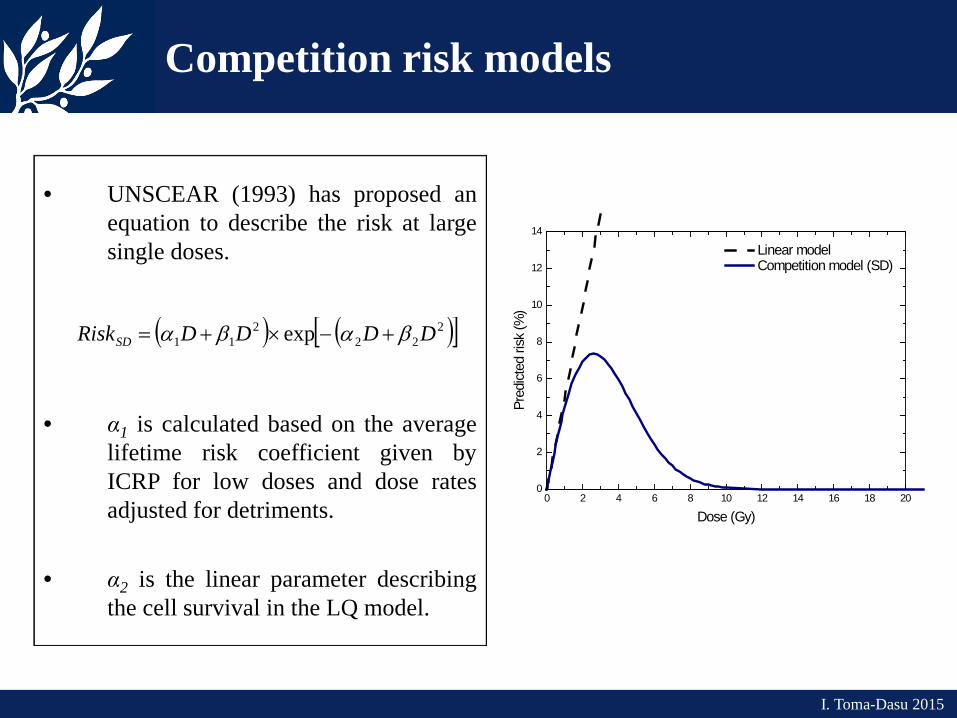
• UNSCEAR (1993) has proposed an equation to describe the risk at large single doses.
• α1 is calculated based on the average lifetime risk coefficient given by ICRP for low doses and dose rates adjusted for detriments.
• α2 is the linear parameter describing the cell survival in the LQ model.
( ) ( )[ ]222
211 exp DDDDRiskSD βαβα +−×+=
Competition risk models
I. Toma-Dasu 2015
0 2 4 6 8 10 12 14 16 18 200
2
4
6
8
10
12
14
Linear model Competition model (SD)
Pred
icted
risk
(%)
Dose (Gy)
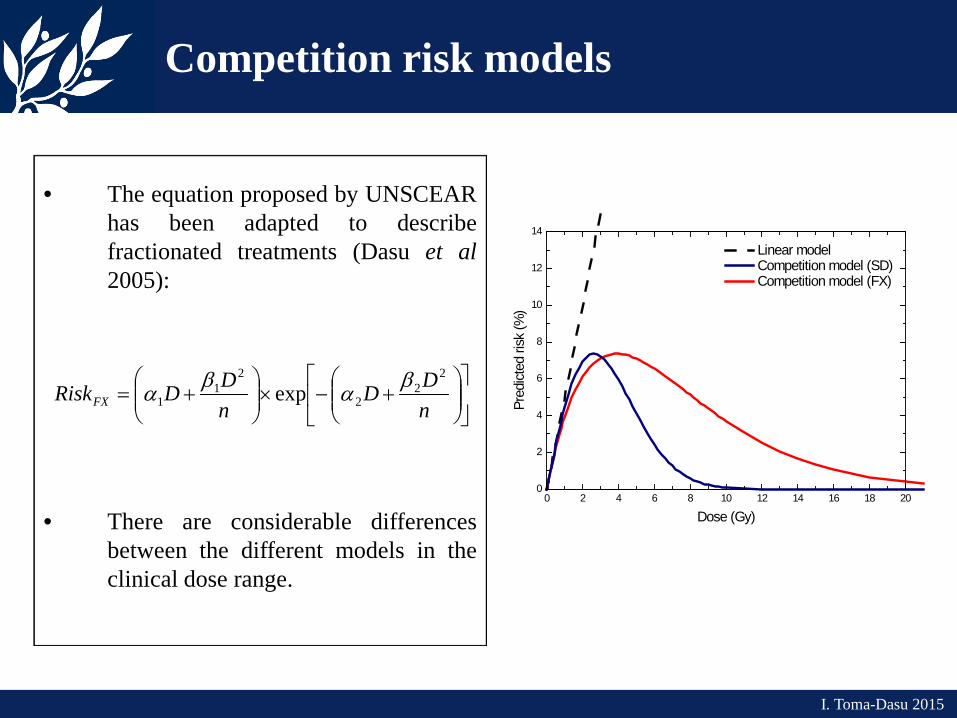
• The equation proposed by UNSCEAR has been adapted to describe fractionated treatments (Dasu et al 2005):
• There are considerable differences between the different models in the clinical dose range.
+−×
+=
nDD
nDDRiskFX
22
2
21
1 exp βαβα
0 2 4 6 8 10 12 14 16 18 200
2
4
6
8
10
12
14
Linear model Competition model (SD) Competition model (FX)
Pred
icted
risk
(%)
Dose (Gy)
Competition risk models
I. Toma-Dasu 2015
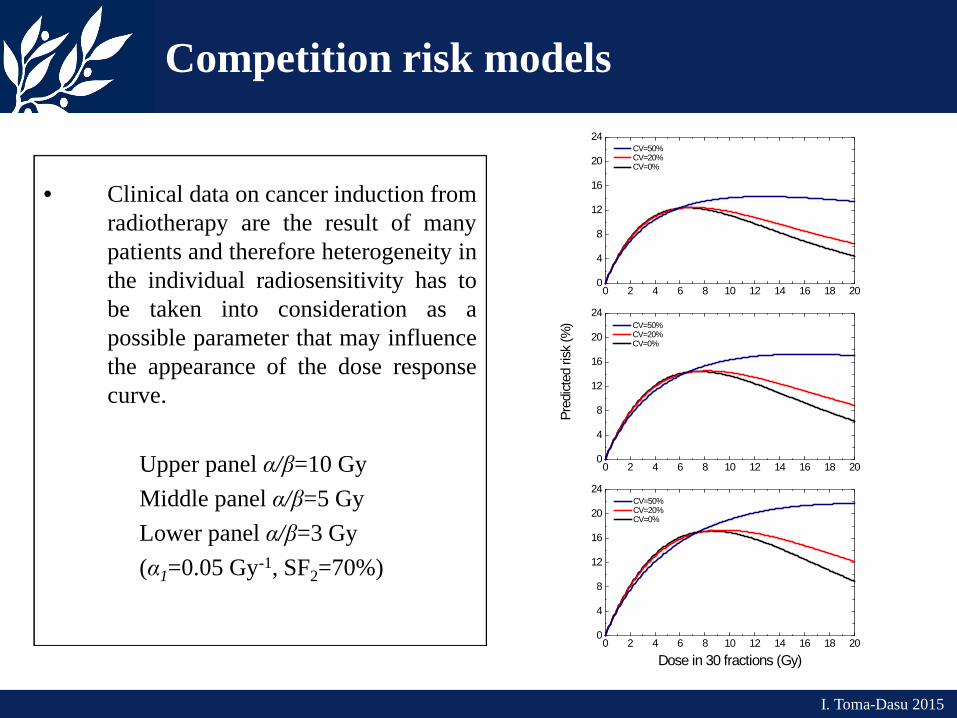
• Clinical data on cancer induction from radiotherapy are the result of many patients and therefore heterogeneity in the individual radiosensitivity has to be taken into consideration as a possible parameter that may influence the appearance of the dose response curve.
Upper panel α/β=10 Gy Middle panel α/β=5 Gy Lower panel α/β=3 Gy (α1=0.05 Gy-1, SF2=70%)
0 2 4 6 8 10 12 14 16 18 200
4
8
12
16
20
24
Dose in 30 fractions (Gy)
CV=50% CV=20% CV=0%
0 2 4 6 8 10 12 14 16 18 200
4
8
12
16
20
24
Pred
icted
risk
(%) CV=50%
CV=20% CV=0%
0 2 4 6 8 10 12 14 16 18 200
4
8
12
16
20
24 CV=50% CV=20% CV=0%
Competition risk models
I. Toma-Dasu 2015
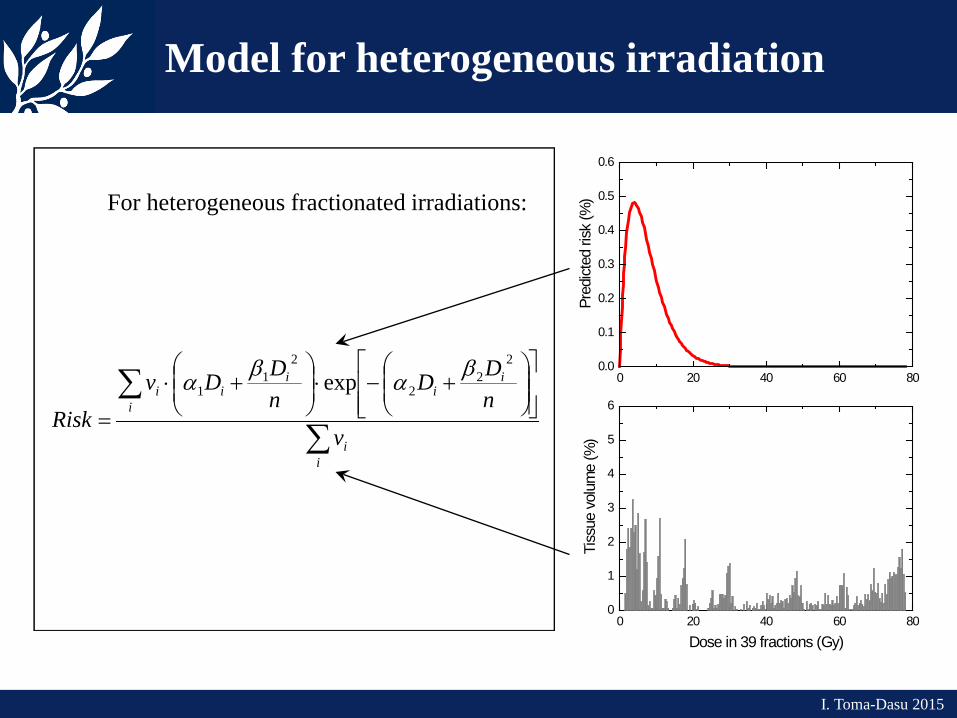
For heterogeneous fractionated irradiations:
∑
∑
+−⋅
+⋅
=
ii
i
ii
iii
vnDD
nDDv
Risk
22
2
21
1 exp βαβα
0 20 40 60 800
1
2
3
4
5
6
Tiss
ue v
olum
e (%
)
Dose in 39 fractions (Gy)
0 20 40 60 800.0
0.1
0.2
0.3
0.4
0.5
0.6
Pred
icted
risk
(%)
Model for heterogeneous irradiation
I. Toma-Dasu 2015
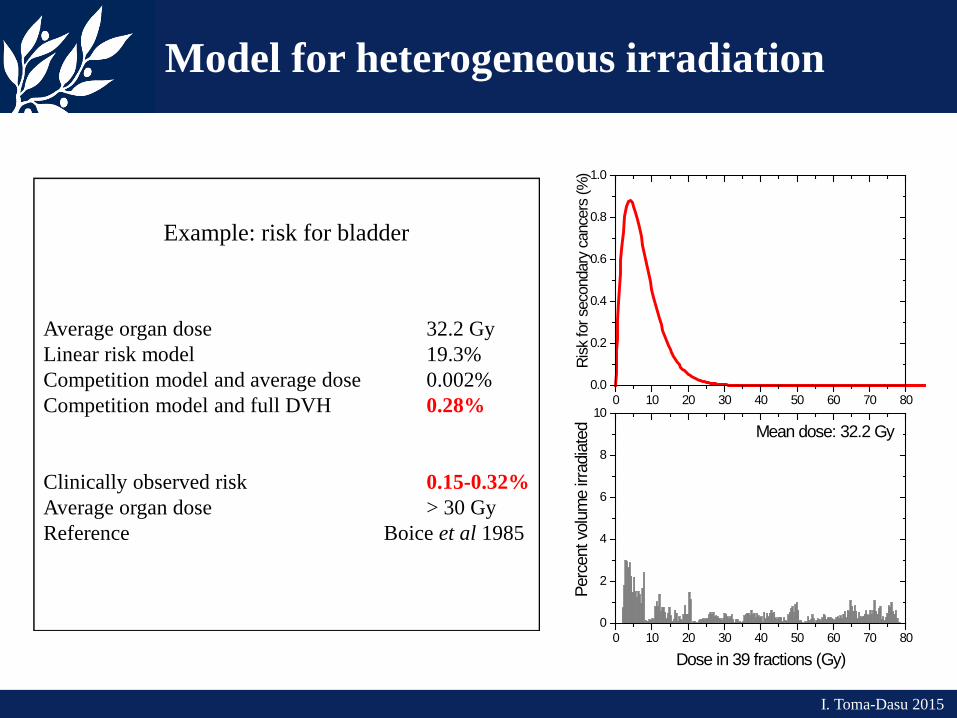
Example: risk for bladder
Average organ dose 32.2 Gy Linear risk model 19.3% Competition model and average dose 0.002% Competition model and full DVH 0.28% Clinically observed risk 0.15-0.32% Average organ dose > 30 Gy Reference Boice et al 1985
0 10 20 30 40 50 60 70 800
2
4
6
8
10
Mean dose: 32.2 Gy
Perc
ent v
olum
e irr
adia
ted
Dose in 39 fractions (Gy)
0 10 20 30 40 50 60 70 800.0
0.2
0.4
0.6
0.8
1.0
Risk
for s
econ
dary
can
cers
(%)
Model for heterogeneous irradiation
I. Toma-Dasu 2015
I. Toma-Dasu 2015
Risk of secondary cancer
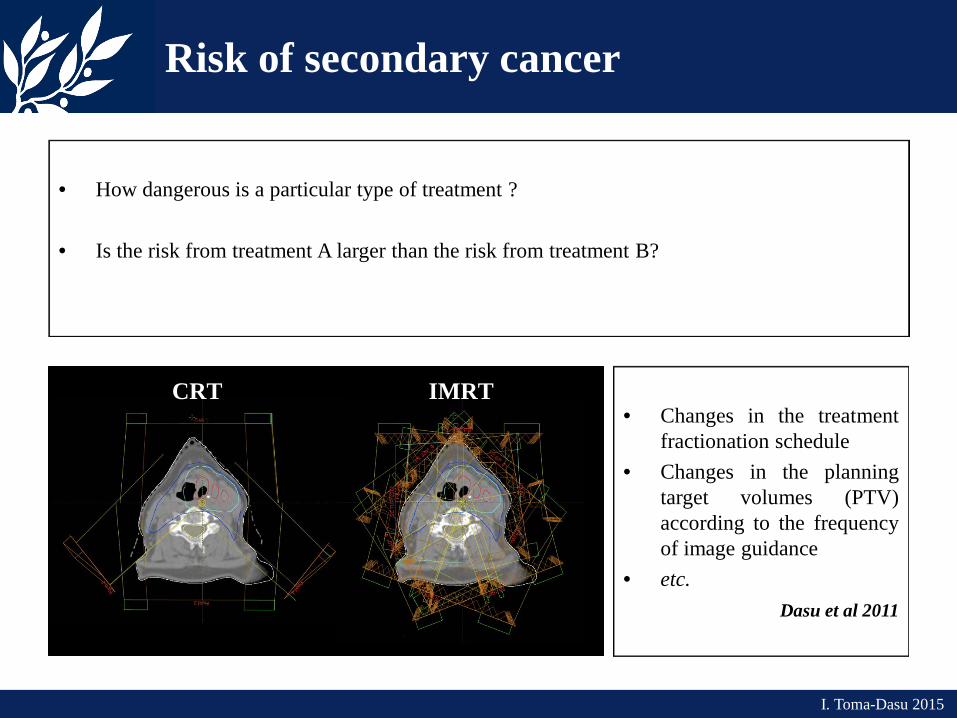
• How dangerous is a particular type of treatment ?
• Is the risk from treatment A larger than the risk from treatment B?
CRT
IMRT
• Changes in the treatment
fractionation schedule • Changes in the planning
target volumes (PTV) according to the frequency of image guidance
• etc. Dasu et al 2011
Clinical application of the risk models
• Risk assessments were carried out for 10 H&N patients.
• Two plans for each patient: an IMRT plan and a clinically equivalent CRT
plan.
• The prescribed dose to the tumour was 68 Gy in 2 Gy fractions.
• Four tissues of interest were included in the risk calculations: parotid glands, oesophagus, lungs and the remaining tissues.
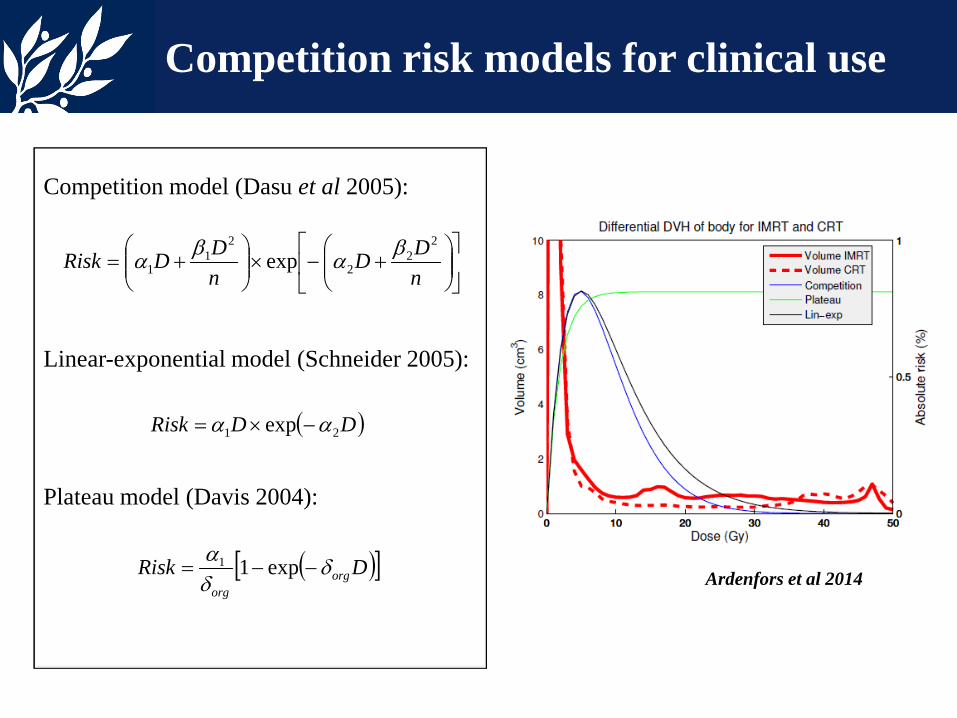
Competition model (Dasu et al 2005):
Linear-exponential model (Schneider 2005): Plateau model (Davis 2004):
+−×
+=
nDD
nDDRisk
22
2
21
1 exp βαβα
Competition risk models for clinical use
( )DDRisk 21 exp αα −×=
( )[ ]DRisk orgorg
δδα
−−= exp11Ardenfors et al 2014
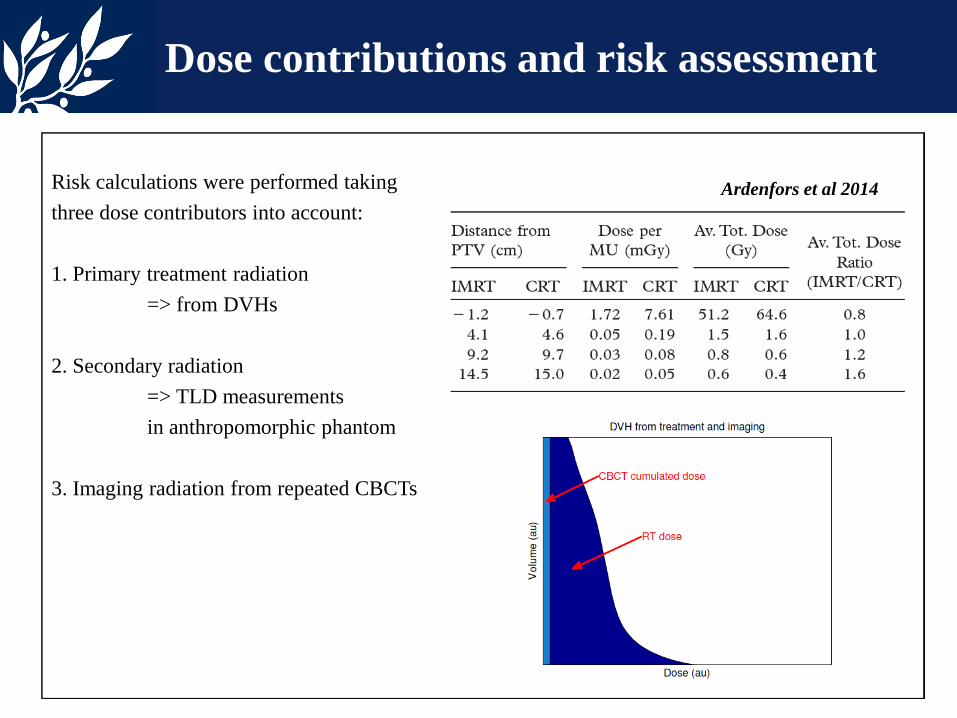
Risk calculations were performed taking three dose contributors into account:
1. Primary treatment radiation => from DVHs
2. Secondary radiation => TLD measurements in anthropomorphic phantom
3. Imaging radiation from repeated CBCTs
Dose contributions and risk assessment
Ardenfors et al 2014
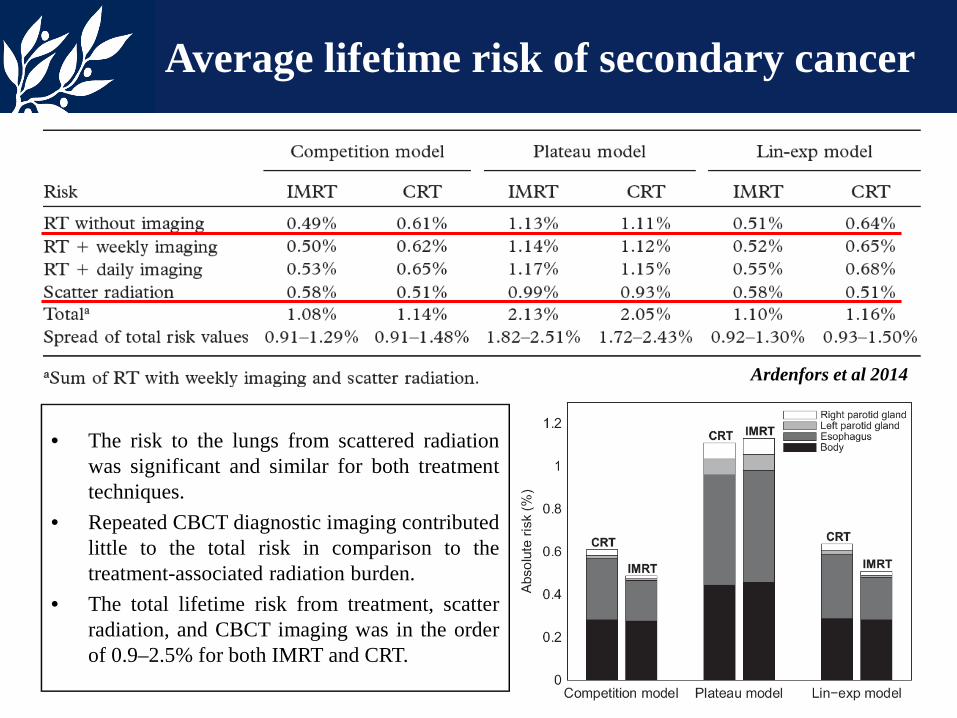
Average lifetime risk of secondary cancer
• The risk to the lungs from scattered radiation was significant and similar for both treatment techniques.
• Repeated CBCT diagnostic imaging contributed little to the total risk in comparison to the treatment-associated radiation burden.
• The total lifetime risk from treatment, scatter radiation, and CBCT imaging was in the order of 0.9–2.5% for both IMRT and CRT.
Ardenfors et al 2014
Conclusions
I. Toma-Dasu 2015
• Quantification of the risks for cancer induction from RT becomes increasingly
necessary as the life expectancy of patients increases.
• Conventional risk estimates might not be appropriate for radiotherapy applications due to differences in the irradiation pattern.
• Knowledge about risk is in a continuous update. Models rely on epidemiological studies for parameters. Epidemiological studies may in turn benefit from theoretical modelling to
highlight aspects of interest.
• Current knowledge indicate that radiotherapy might result in a small but significant risk of inducing cancers.
Considerations for the future
I. Toma-Dasu 2015
• Irradiation techniques change continuously.
How could the results from epidemiological studies analysing data from patients irradiated in the 1970s and 1980s be extrapolated to modern therapy techniques?
How could the results from current treatment methods (CRT, IMRT, TT) be extrapolated to the treatments of the 2040s and 2050s?
How much of the information available nowadays must we record for the future?
• The use of particle therapy employing protons and heavier ions is on the increase.
How could the results from photon therapy be extrapolated to particle therapy?
Acknowledgements
OSCAR ARDENFORS Stockholm University and Karolinska Institutet IRENA GUDOWSKA ALEXANDRU DASU Linköping University and Linköping University Hospital This work was partially supported by the Swedish Radiation Safety Authority under the contract SSM2014-2593.