rheumatoid arthritis
TRANSCRIPT
Rheumatoid Arthritis
By : Hammad
2
History of Rheumatoid Arthritis (RA)
• 123 AD first text describes symptoms very similar to RA
• 1800 first recognised description of RA by French physician Dr A J Landré-Beauvais (1772-1840)
• 1859 name “rheumatoid arthritis" itself was coined by British Dr A B Garrod.
3
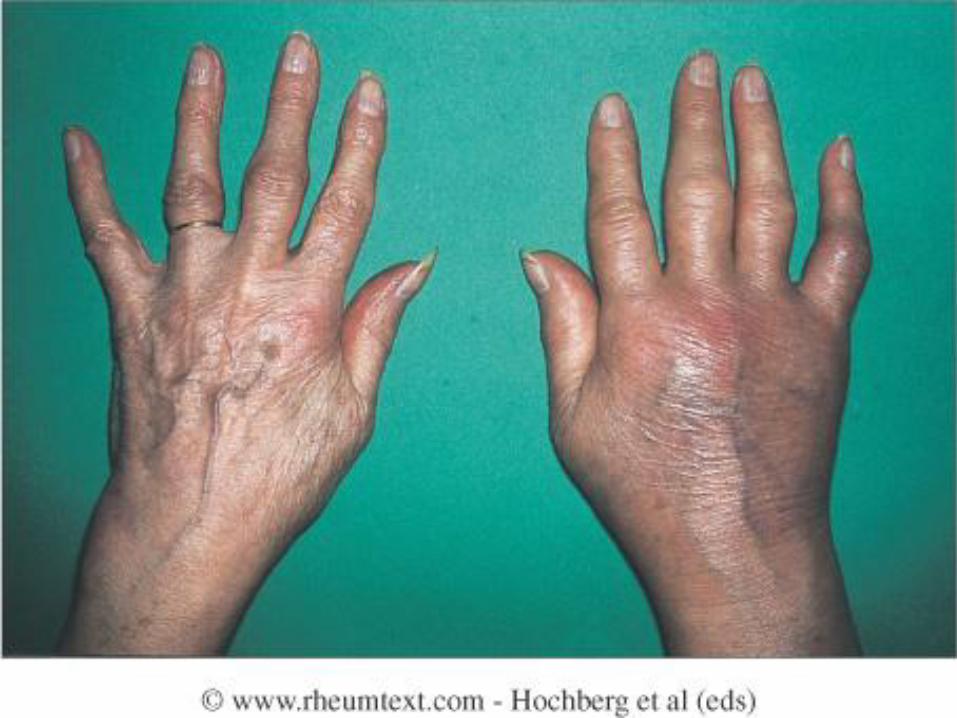
What is it?
• Chronic, progressive, autoimmune disease
• Causes inflammation in joints (especially hands, wrists, feet)
• Systemic condition
4
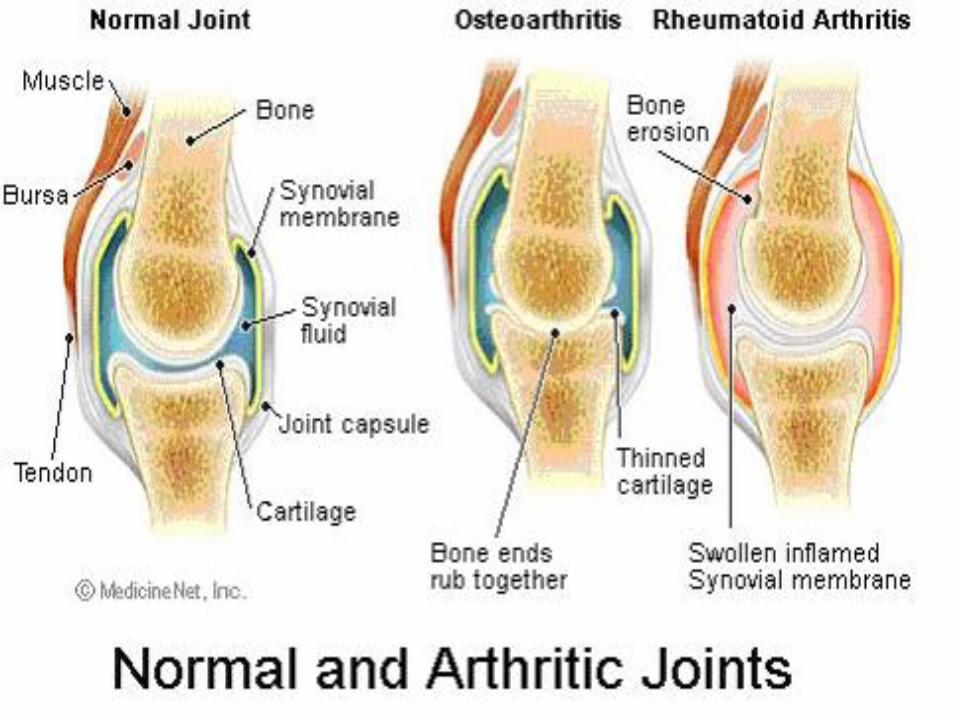
What is inflammation?
• Normal body defence mechanism
• Increased blood flow
• Blood cells produce chemical messengers to continue the process
• Heat, swelling, redness, pain, loss of function
5
6
7
8
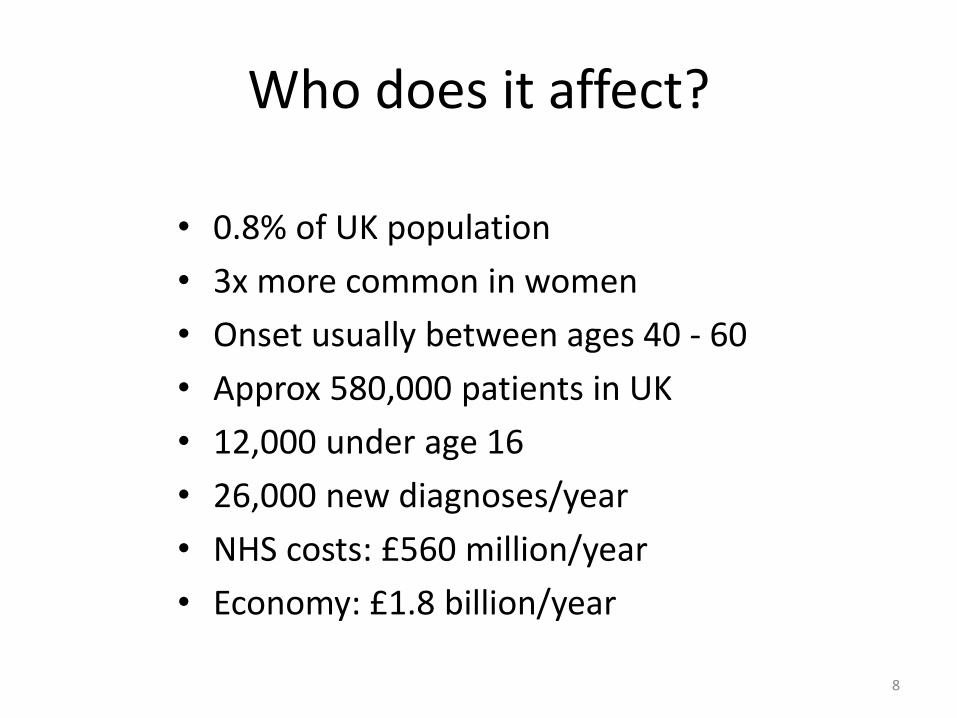
Who does it affect?
• 0.8% of UK population
• 3x more common in women
• Onset usually between ages 40 - 60
• Approx 580,000 patients in UK
• 12,000 under age 16
• 26,000 new diagnoses/year
• NHS costs: £560 million/year
• Economy: £1.8 billion/year
9
What causes RA?
• Genetics
• Environment
10
Genetics
• 1st degree relative: 2-7 fold risk
• Identical twin: 16% chance of RA
• Need an environmental trigger as well
11
Environment
• Geography
• Hormones
• Infection
• Smoking
• Diet

12
13
Symptoms
• Joint pain
• Joint swelling
• Morning stiffness
• Fatigue
• Weight loss
• Flu-like symptoms

14
What else does RA do?
• Eyes: dryness, inflammation
• Lungs: fluid, inflammation, nodules
• Skin: nodules, ulcers
• Heart: fluid, inflammation, ischaemic heart disease
• Blood: anaemia, low counts
15
How is RA treated?
General Principles:
• Patient education/self-management
• Multi-professional team care
• Medication
• Surgery

16
Symptomatic Treatments
• Education/support
• Rest/relaxation
• Joint protection
• Physiotherapy
• Painkillers
• Anti-inflammatory drugs
• Steroids
• Joint injections
• Pain Management Clinics
17
Reduction of Joint Damage
Disease-modifying Anti-Rheumatic Drugs (DMARDS)
•Methotrexate
•Sulfasalazine
•Leflunomide
•Hydroxychloroquine
•Azathioprine
•Ciclosporin
•Gold
•Penicillamine
Biologic drugs
• Anti-TNF therapy:
Infliximab
Etanercept
Adalimumab
Certolizumab
Golimumab
• Rituximab
• Abatacept
• Tocilizumab
Drug Therapy
• Drugs remain cornerstone of treatment
• DMARDs (Disease-modifying antirheumatic drug) can lessen permanent effects of RA
• Choice of drug is based on
– Disease activity
– Patient’s level of function
– Lifestyle considerations
Drug Therapy
• Many of the drugs used to treat RA are expensive
• Methotrexate (Rheumatrex) is drug of choice – Rapid antiinflammatory effect decreases clinical
symptoms in days to weeks
– Inexpensive
– Lower toxicity compared to other drugs
Drug Therapy
• Effective DMARDs for mild to moderate disease
– Sulfasalazine (Azulfidine)
– Antimalarial drug hydroxychloroquine
• Leflunomide (Arava) is a newer synthetic DMARD that blocks immune cell overproduction
Drug Therapy
• Use of combination therapy can slow symptoms and joint damage while improving function
• Drug combinations are individualized and often include – A DMARD
– An NSAID
– A corticosteroid
Drug Therapy
• Biologic/targeted drug therapies can also slow disease progression in RA
• Can be used in patients with moderate to severe disease who have not responded to DMARDs or in combination therapy with an established DMARD
Drug Therapy
• Corticosteroid therapy can aid in symptom control – Intraarticular injections may relieve pain and
inflammation associated with flare-ups • Long-term use should not be a mainstay
– Risk osteoporosis, avascular necrosis
– Low-dose prednisone for a limited time to decrease disease activity until DMARD effect is seen
Drug Therapy
• Various NSAIDs and salicylates to treat arthritis pain and inflammation
• Aspirin is often used in high dosages of 4 to 6 g/day (10 to 18 tablets)
• NSAIDs have antiinflammatory, analgesic, and antipyretic properties

Drug Therapy
• NSAIDs
– Do not alter natural history of RA
– Full effectiveness may take 2 to 3 weeks
• Some relief may be noted within days
– May be used when patient cannot tolerate high doses of aspirin
26
Goals of Therapy
• To relieve pain, stiffness, swelling, fatigue
• To prevent joint damage/disability
• To improve quality of life
• ? To achieve disease remission
27
Principles of Treatment
• Early diagnosis
• Early initiation of treatment
• Regular assessment (Disease Activity Scores)
• “Treat to Target”
• Annual review

28
Nursing Implementation Acute Intervention
• Usually treated on an outpatient basis
• Hospitalization may be necessary for patients with extraarticular complications or advancing disease – Reconstructive surgery for disabling deformities
• Nursing intervention begins with a careful physical assessment
Nursing Management Assessment
• Nurse must also
– Evaluate psychosocial needs and environmental concerns
– After problem identification, coordinate a carefully planned program for rehabilitation and education for interdisciplinary health care team
Nursing Management Problems
• Chronic pain
• Impaired physical mobility
• Activity intolerance
• Self-care deficit
• Ineffective therapeutic regimen management
• Disturbed body image
Nursing Management Planning
• Overall goals – Satisfactory pain relief
– Minimal loss of functional ability of affected joints
– Perform self-care
– Participate in planning and carrying out therapeutic regimen
– Maintain a positive self-image
Nursing Management Planning
• Primary goals in managing RA
– Decrease inflammation
– Manage pain
– Maintain joint function
– Prevent or correct joint deformity
Nursing Management Interventions
• Goals may be met through a comprehensive program
– Drug therapy – pain control, antiinflammatory
– Rest
– Joint protection
– Heat and cold applications – pain control
– Exercise
– Patient and family teaching
Nursing Management Interventions
• Suppression of inflammation
– NSAIDs
– DMARDs
– Biologic therapies
• Careful attention to timing is critical to
– Sustain a therapeutic drug level
– Decrease early morning stiffness
Nursing Management Interventions
• Discuss with patient – Action and side effects of each prescribed drug
– Importance of laboratory monitoring
• Many RA patients take several different drugs so the nurse must make the drug regimen as understandable as possible
Nursing Management Interventions
• Nonpharmacologic relief of pain – Therapeutic heat and cold
– Rest
– Relaxation techniques
– Joint protection
– Biofeedback
– Transcutaneous electrical stimulation
– Hypnosis
Nursing Management Interventions
• Lightweight splints may be prescribed to rest an inflamed joint and prevent deformity – Should be removed regularly to perform skin care
and ROM exercises
– Should be reapplied as prescribed
– Occupational therapist may help identify additional self-help devices to assist in activities of daily living
Nursing Management Interventions
• Morning care and procedures should be planned around morning stiffness
• To relieve joint stiffness and increase comfort
– Sitting or standing in a warm shower
– Sitting a tub with warm towels around shoulders
– Simply soaking hands in a basin of warm water