reversion of ventricular tachycardia by pacemaker stimulation
TRANSCRIPT

British Heart Journal, 1971, 33, 922-927.
Reversion of ventricular tachycardia bypacemaker stimulation
M. A. Bennett and B. L. PentecostFrom the General Hospital, Birmingham 4
Reversion of ventricular tachycardia to either sinus rhythm or atrialfibrillation has been achievedin a group ofpatients by rapid ventricular pacing. The standard technique involved pacing at a
rate slightly in excess of the existing tachycardia until ventricular capture was achieved. Cessationofpacing after afew seconds was usuallyfollowed by a supraventricular rhythm, though pacing ata lower rate might be required to suppress completely ventricular ectopic activity. In the event ofa return to ventricular tachycardia, ventricular capture was again achieved and the pacing rategradually slowed to the point where ventricular premature beats first appeared; the heart was
then paced slightly in excess of this critical rate.
Rapid transvenous pacing of the heart is ofvalue in stabilizing the cardiac rhythm whenrecurrent episodes of ventricular tachycardiaand fibrillation persist in spite of conventionaldrug treatment (Swedberg and Malm, I964;Sowton, Leatham, and Carson, I964; Fried-berg, Lyon, and Donoso, 1970; Bennett andPentecost, 1970). Ventricular tachycardla may,however, return after cessation of pacing oreven during the manoeuvre. It seems probablethat ventricular tachycardia could be ter-minated by pacemaker stimulation in a similarway to that described in paroxysmal atrialtachycardia, junctional tachycardia, and atrialflutter (Haft et al., I967; Lister et al., I968;Hunt et al., I968. Ventricular tachycardiawhich progresses rapidly to fibrillation doesnot offer sufficient time to test this hypothesisbut the opportunity does arise when a pace-maker catheter is already in situ after a pre-vious period of prophylactic pacing. Thispaper describes our initial experience in theattempted reversion of ventricular tachy-cardia to supraventricular rhythm in a groupof patients by means of transvenous pacing ofthe right ventricle.
MethodsAll pacing procedures were performed in theHospital's Coronary Care Unit. A transvenousbipolar catheter and a fixed rate pacemaker wereused (United Birmingham Hospitals). Thecatheter was introduced into a medial arm vein atthe antecubital fossa and guided to the apex of theright ventricle under fluoroscopic control withinthe Unit. The electrocardiogram was continuouslyrecorded on electromagnetic tape and permanentpaper records made from the tape using an electro-
Received 8 March I97I.
cardiograph (Mingograph 243) at a paper speedof 25 mm/sec.The patients in this study had all suffered acute
myocardial infarction complicated by recurrentventricular tachyarrhythmias in spite of anti-arrhythmic drug therapy. In the majority ofpatients prophylactic transvenous right ventricu-lar pacing had been employed in an attempt tosuppress further ventricular tachycardia, but thisrhythm returned either during or after cessationofpacing. It was during a recurrence of ventriculartachycardia that the technique of conversion byrapid pacing was tried. In two further patients thepacing technique was attempted during the firstepisode of ventricular tachycardia after arrival inthe Unit, as described in the relevant casehistories.
Reversion of ventricular tachycardia was begunby capturing the ventricle by pacing at a rateslightly in excess of the existing rhythm, with anexception when a slower rate was found to beeffective. When the initial rate of pacemakerstimulation failed to capture the ventricle the ratewas gradually increased until capture wasachieved. Pacing rates in excess of 300/min werenot used. After successful capture, pacing wasdiscontinued abruptly after a few seconds. Ifsupraventricular rhythm was restored no furtherpacing was performed. In the event of a return toventricular tachycardia pacing was begun again atthe previous capture rate; the paced rate was thengradually reduced until the appearance of ven-tricular premature beats was observed. The heartwas subsequently paced at a rate marginallyabove this level as a prophylactic measure againstfurther episodes of ventricular tachycardia.
ResultsCase I A 62-year-old woman was admittedwith an extensive anterior myocardial infarc-tion. She experienced 12 episodes of ventricu-lar tachyarrhythmia which required DC

Reversion of ventricular tachycardia by pacemaker stimulation 923
shock. These occurred over a period of 36hours during which time she received a totalof 2-4 g intravenous lignocaine and I-5 gquinidine as well as 500 mg procainamideduring the final 8 hours. The cardiac rhythmwas satisfactorily stabilized for 48 hours bytransvenous pacing but upon cessation ofpacing ventricular tachycardia returned.
Pacing was reinstituted at 3 volts and 192beats/min (Fig. i). This rate was 6 beats/minfaster than the existing ventricular tachy-cardia. Ventricular capture occurred after 3-68seconds, pacing was continued for a further3-68 seconds, and then stopped. Two sinusbeats followed, the first associated with aventricular premature beat and the secondimmediately followed by ventricular tachy-cardia initiated by a similar premature beat.Pacing was restarted at 3 volts and 192beats/min. Ventricular capture was immediate(Fig. 2). The pacing rate was reduced inapproximately 2 minutes to 138 beats/minand over the following 4 hours to 9I beats/min. Pacing was continued at 9I beats/minfor 5 days, after which sinus rhythm withoutectopic activity was established.
Case 2 This 47-year-old man had beenpaced after i i episodes of cardiac arrestnecessitating DC countershock over thecourse of 2 hours. These episodes had occur-red in spite of the administration of a total of300 mg lignocaine and 250 mg procainamide.The paced rhythm remained stable for 48hours but ventricular tachycardia returnedwithin a short period of discontinuing pacing.The catheter had been left in situ and
pacing was restarted at 3 volts and a rate ofI29 beats/min; this was considerably slowerthan the ventricular tachycardia of 300 beats/min (Fig. 3). Ventricular capture was achievedin i-84 seconds. Pacing at I29 beats/min wascontinued for approximately 3 minutes andthen stopped. Sinus rhythm with ectopic
ventricular beats followed. The ectopic beatswere abolished by ventricular pacing at II5beats/min. Pacing at this rate was maintainedfor 5 days without recurrence of ventriculartachycardia. Uncomplicated sinus rhythmfollowed the cessation of pacing.
Case 3 After suffering an inferior infarctionthis 47-year-old man developed I4 episodesof ventricular tachycardia over the first 2hours of admission in spite of intravenouslignocaine (66o mg) and procainamide (250mg). Though pacing produced a stablerhythm for a short period, 6 further episodesof ventricular tachycardia occurred, the first4 of which were treated with DC shock. Thefifth was managed by rapid pacing at 270beats/min and ventricular capture was achie-ved in ii seconds. Pacing at 270 beats/minwas continued for 2-2 seconds and thenstopped. Sinus rhythm with ventricularpremature beats followed. A pacing rate of150 beats/min was needed to suppress theventricular ectopic beats. However, afterapproximately I5 hours ventricular tachy-cardia recurred at a rate of 270 beats/min.Rapid ventricular pacing at 275 beats/minresulted in fusion beats but failed to capturethe ventricle. The pacemaker rate wasincreased to 284 beats/min and ventricularcapture was achieved. Pacing was continuedat 284 beats/min for 2-42 seconds and thenstopped. Ventricular tachycardia at 270beats/min immediately recurred withoutpreceding sinus beats. Pacing was againinitiated but at a rate of 300 beats/min; it wascontinued for 2 seconds and then stopped.Sinus rhythm with ventricular prematurebeats followed. Prophylactic pacing at I50beats/min was again required to suppresspremature beats in spite of concurrentadministration of intravenous lignocaine. Thepatient developed ventricular fibrillation 3days later, while being paced, and died.
FIG. I Case i. Ventricular tachycardia in lead Vi. Pacing was begun at 'on' and ventricularcapture (c) achieved with a pacing rate of 192 beats/min after 3y68 sec. On cessation of pacing(off) sinus rhythm returned with coupled ventricular premature beats leading into the originalventricular tachycardia after only two sinus beats.
*01

924 Bennett and Pentecost
FIG. 2 Case i. Pacing restarted (on) at 192 beats/min with immediate ventricular capture.Lower trace - pacing rate slowed to approximately 138 beats/min with no return of ventricularpremature beats.
Case 4 This patient was already in ven-tricular tachycardia on admission to theCoronary Care Unit. He was a 65-year-oldman with an acute anterior infarction. Nine-teen episodes of ventricular tachycardia hadbeen treated with DC shock during his shortsojourn in the hospital's Accident andEmergency Service, in spite of lignocaine480 mg which had been administered overapproximately 30 minutes. In view of therecurrent nature of the dysrhythmia a pace-maker catheter was introduced into the rightventricle and pacing begun at 2 volts and 250beats/min. This was 34 beats/min faster thanthe intrinsic ventricular tachycardia (Fig. 4).Ventricular capture was achieved after 4o8sec. Pacing at 250 beats/min was continuedfor approximately ii seconds and thenstopped. Sinus rhythm was re-established;ventricular premature beats appeared withinminutes and were suppressed by ventricular
pacing at I45 beats/min. Pacing in its thirdday was intermittent due to instability of thecatheter in the right ventricle and during aperiod of spontaneous sinus rhythm ventricu-lar fibrillation developed which proved fatal.
Case 5 The clinical picture here wassimilar to that of the previous patient. A 57-year-old man with a recent anterior infarctionhad received DC shock on I7 occasions duringi hour in the Casualty Department. The fre-quency of ventricular tachycardia deteriora-ting into fibrillation had not been influencedby the intravenous administration of ligno-caine 6oo mg. Between episodes of ventriculartachycardia the underlying rhythm was seento be atrial fibrillation. A pacemaker catheterwas inserted and during an episode ofventricular tachycardia pacing was begun at3 volts and 2I5 beats/min, a rate of 29 beats/min faster than the existing ventricular
FIG. 3 Case 2. Ventricular tachycardia of approximately 300 beats/min. Pacing at I29beats/min (on) resulted in ventricular capture (c) after I-84 sec.
0N A
\~~~~~~~~~~~~~~~~~MI~~!!!f!

Reversion of ventricular tachycardia by pacemaker stimulation 925
jS.li, ,,,,,,. ,, . ,:I.
FIG. 4 Case 4. Ventricular tachycardia in lead VI. Pacing begun at 250 beats/min (on), severalfusion beats (F) follow, with eventual ventricular capture (c) achieved after 40o8 sec. Aftercessation ofpacing (off) there is a return of sinus rhythm - the first sinus beat may have beenconducted aberrantly.
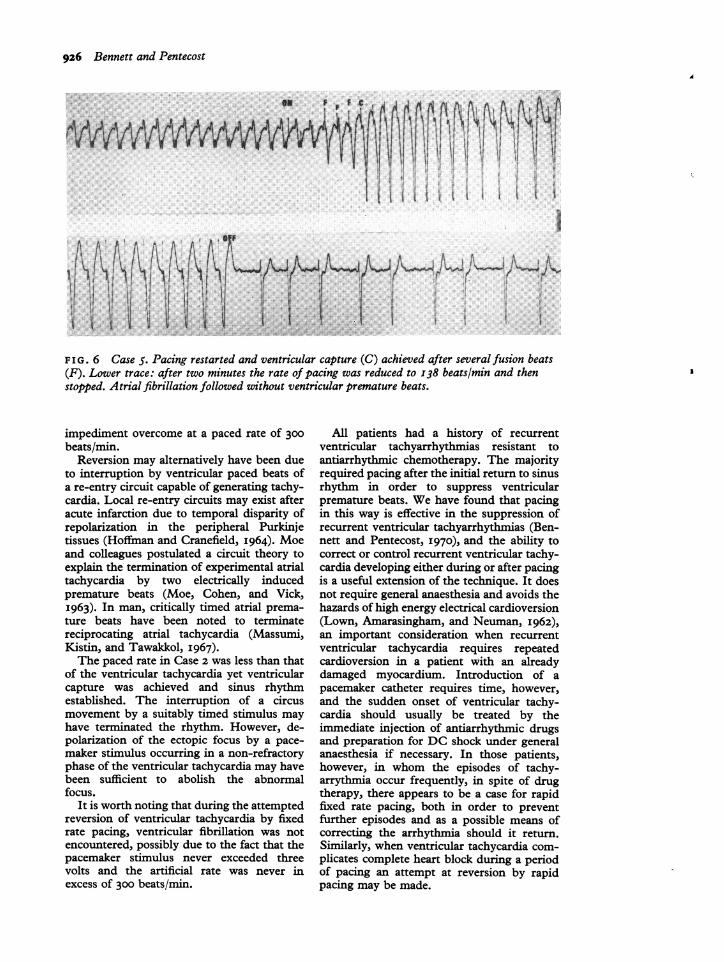
tachycardia (Fig. 5). Ventricular capture wasachieved after i 68 seconds. Pacing wasstopped after two capture beats. Supra-ventricular initiated beats followed, but afterfour such beats ventricular tachycardia re-curred. Pacing was restarted at 2I5 beats/min. The ventricle was again captured afterir68 seconds (Fig. 6). After ventricular cap-ture the rate was rapidly reduced over twominutes to I38 beats/min and then stopped.Atrial fibrillation followed without interrup-tion.
DiscussionIn four patients return to supraventricularrhythm was achieved by pacing at a ratefaster than that of the intrinsic tachycardia.
Reversion in Cases I, 3, 4, and 5 followedpacing at the respective ventricular capturerates for a short period. Case 3, however, onone occasion required a rate in excess of theventricular capture rate before suppression ofthe ectopic focus occurred. Ventricularstimulation at a rate in excess of the existingventricular tachycardia may have permittedreturn to supraventricular rhythm by suppres-sion of the ectopic ventricular focus by afaster, in this instance artificial, pacemaker - aphenomenon known as overdrive suppression(Lange, I965). The fact that pacing at a rateof 284 beats was sufficient to capture theventricles but failed to achieve return tosupraventricular rhythm on one occasion inCase 3 may have been related to a critical rate-dependent entry block to the ectopic focus, an
FIG. 5 Case 5. Ventricular tachycardia in lead VI. Ventricular capture rapidly achievedafter pacing was begun (on). After cessation of pacing (off) there were 4 supraventricularinitiated beats then a return of the original ventricular tachycardia.
I ,
% I.
w
926 Bennett and Pentecost
FIG. 6 Case 5. Pacing restarted and ventricular capture (C) achieved after several fusion beats(F). Lower trace: after two minutes the rate of pacing was reduced to 138 beats/min and thenstopped. Atrial fibrillation followed without ventricular premature beats.
impediment overcome at a paced rate of 300beats/min.
Reversion may alternatively have been dueto interruption by ventricular paced beats ofa re-entry circuit capable of generating tachy-cardia. Local re-entry circuits may exist afteracute infarction due to temporal disparity ofrepolarization in the peripheral Purkinjetissues (Hoffman and Cranefield, I964). Moeand colleagues postulated a circuit theory toexplain the termination of experimental atrialtachycardia by two electrically inducedpremature beats (Moe, Cohen, and Vick,I963). In man, critically timed atrial prema-ture beats have been noted to terminatereciprocating atrial tachycardia (Massumi,Kistin, and Tawakkol, I967).The paced rate in Case 2 was less than that
of the ventricular tachycardia yet ventricularcapture was achieved and sinus rhythmestablished. The interruption of a circusmovement by a suitably timed stimulus mayhave terminated the rhythm. However, de-polarization of the ectopic focus by a pace-maker stimulus occurring in a non-refractoryphase of the ventricular tachycardia may havebeen sufficient to abolish the abnormalfocus.
It is worth noting that during the attemptedreversion of ventricular tachycardia by fixedrate pacing, ventricular fibrillation was notencountered, possibly due to the fact that thepacemaker stimulus never exceeded threevolts and the artificial rate was never inexcess of 300 beats/min.
All patients had a history of recurrentventricular tachyarrhythmias resistant toantiarrhythmic chemotherapy. The majorityrequired pacing after the initial return to sinusrhythm in order to suppress ventricularpremature beats. We have found that pacingin this way is effective in the suppression ofrecurrent ventricular tachyarrhythmias (Ben-nett and Pentecost, 1970), and the ability tocorrect or control recurrent ventricular tachy-cardia developing either during or after pacingis a useful extension of the technique. It doesnot require general anaesthesia and avoids thehazards of high energy electrical cardioversion(Lown, Amarasingham, and Neuman, I962),an important consideration when recurrentventricular tachycardia requires repeatedcardioversion in a patient with an alreadydamaged myocardium. Introduction of apacemaker catheter requires time, however,and the sudden onset of ventricular tachy-cardia should usually be treated by theimmediate injection of antiarrhythmic drugsand preparation for DC shock under generalanaesthesia if necessary. In those patients,however, in whom the episodes of tachy-arrythmia occur frequently, in spite of drugtherapy, there appears to be a case for rapidfixed rate pacing, both in order to preventfurther episodes and as a possible means ofcorrecting the arrhythmia should it return.Similarly, when ventricular tachycardia com-plicates complete heart block during a periodof pacing an attempt at reversion by rapidpacing may be made.
I
i

Reversion of ventricular tachycardia by pacemaker stimulation 927
ReferencesBennett, M. A., and Pentecost, B. L. (1970). The
suppression of ventricular tachyarrhythmias bytransvenous intracardiac pacing after acute myo-cardial infarction. British Medical Journal, 4, 468.
Friedberg, C. K., Lyon, L. J., and Donoso, E. (I970).Suppression of refractory recurrent ventriculartachycardia by transvenous rapid cardiac pacingand antiarrhythmic drugs. Report of seven cases.American Heart journal, 79, 44.
Haft, J. I., Kosowsky, B. D., Lau, S. H., Stein, E., andDamato, A. N. (I967). Termination of atrial flutterby rapid electrical pacing of the atrium. AmericanJ'ournal of Cardiology, 20, 239.
Hoffman, B. F., and Cranefield, P. F. (I964). Thephysiological basis of cardiac arrhythmias. AmericanJournal of Medicine, 37, 670.
Hunt, N. C., Cobb, F. R., Waxman, M. B., Zeft, H. J.,Peter, R. H., and Morris, J. J. (I968). Conversionof supraventricular tachycardias with atrial stim-ulation. Evidence for re-entry mechanisms. Circu-lation, 38, io6o.
Lange, G. (I965). Action of driving stimuli fromintrinsic and extrinsic sources on in situ cardiacpacemaker tissues. Circulation Research, 17, 449.
Lister, J. W., Cohen, L. S., Bernstein, W. H., andSamet, P. (I968). Treatment of supraventriculartachycardias by rapid atrial stimulation. Circulation,38, 1044.
Lown, B., Amarasingham, R., and Neuman, J. (i962).New method for terminating cardiac arrhythmias;use of synchronized capacitor discharge. J'ournal ofthe American Medical Association, I82, 548.
Massumi, R. A., Kistin, A. D., and Tawakkol, A. A.(I967). Termination of reciprocating tachycardiaby atrial stimulation. Circulation, 36, 637.
Moe, G. K., Cohen, W., and Vick, R. L. (I963).Experimentally induced paroxysmal A-V nodaltachycardia in the dog: a 'case report'. AmericanHeart_Journal, 65, 87.
Sowton, E., Leatham, A., and Carson, P. (I964). Thesuppression ofarrhythmias by artificial pacemaking.Lancet, 2, I098.
Swedberg, J., and Malm, A. (I964). Pacemakerstimulation in ventricular paroxysmal tachycardia.Acta Chirurgica Scandinavica, I28, 6I0.
Requests for reprints to Dr. B. L. Pentecost, TheGeneral Hospital, Steelhouse Lane, Birmingham,B4 6NH.