retrograde conduction from premature ventricular...
TRANSCRIPT
Retrograde Conduction from PrematureVentricular Contractions a Common
Occurrence in the Human HeartBy ALBERT D. KISTIN, M.D., AND MILTON LANDOWNE, M.D.
On the basis of studies of esophageal electrocardiograms the authors conclude that retrogradeconduction to the atria from premature ventricular beats is common and that the theory ofnormal unidirectional block in the A-V node is not tenable. In most of the cases with retrogradeconduction, the latter is not discernible in simultaneously recorded lead II, which explains why thephenomenon has previously been considered rare. Observations on the ventriculoatrial conduc-tion time and the compensatory pause are presented. In two of the cases there are two orders ofmagnitude of ventriculoatrial conduction time, which, the authors postulate, may be due to twoseparate pathways of retrograde conduction.
R RETROGRADE conduction to the atriafrom premature ventricular contrac-tions is generally believed to be rare
in the human 8,10,11,14,19, 20, 22 although Ash-man and Hu1l2 state that they have observedthis phenomenon repeatedly. We studied theesophageal leads of 33 individuals with prema-ture ventricular beats and believe there is evi-dence of retrograde conduction in 15. Theseinclude cases in which there was no evidence ofheart disease as well as cases of heart diseaseand cases in which the premature beats mayhave been related to the use of digitalis. Theesophageal leads were recorded simultaneouslywith lead II in 12 of the 15 cases and in mostof these the retrograde conduction, apparent inthe esophageal leads, is difficult or impossibleto recognize in lead II. Little attempt has beenmade to use this technic in the past. Brown'showed that retrograde P waves could be dis-cerned in esophageal leads. Kline, Conn andRosenbaum'5 used esophageal leads to demon-strate ventriculoatrial conduction in a case ofcomplete atrioventricular block; at one timethey could demonstrate the retrograde conduc-
Sponsored by the Veterans Administration andpublished with the approval of the Chief MedicalDirector. The statements and conclusions publishedby the authors are a result of their own study and donot necessarily reflect the opinion or policy of theVeterans Administration.
From the Cardiovascular Research Unit, VeteransAdministration Hospital, Washington, D. C.
738
tion in the esophageal leads but not in thesimultaneously recorded standard leads.
Technic
For esophageal exploring electrodes a modi-fied Nyboer tube* was used consisting of ringsof Monel metal about 5 mm. in diameter and3 to 5 mm. long mounted on a soft rubber tube.The optimum position of the esophageal explor-ing electrode was determined in each case bytrial, or several esophageal leads were recorded.The positions of the exploring electrodes incentimeters from the nares are designated bythe numbers following the E in the figures. Theesophageal and precordial exploring electrodeswere paired with the Wilson indifferent elec-trode. A standard recording speed of 25 mm.per second was used so that the smallest timeintervals on the illustrations represent 0.04second. All records were taken with amplifiertype instruments. A Technicon three channelelectrocardiograph was used for the simulta-neous tracings. The width of the record hasbeen reduced for some of the illustrations with-out altering the alignment. For the records ofsingle leads, the Sanborn Cardiette or Viso-Cardiette was used. An electropositive poten-tial at the precordial and esophageal electrodeswas recorded as an upward deflection.
* Manufactured by C. R. Bard Co., New York,N. Y.
Circulation, Volume III, May, 1951
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
ALBERT D. KISTIN AND MILTON LANDOWNE
There was no deliberate selection of casesavailable for study. As we became interestedin the problem, we attempted to record esopha-geal leads in all cases showing numerous pre-mature ventricular contractions. In this senseour material is a random series from a hospitalpopulation. In a few cases esophageal leads had
negative intrinsic deflection. Differences in di-rection of the atrial excitation wave may pro-duce change in contour which may be minimalor not discernible in other leads. Furthermorethe sharp positive peak of the esophageal Pwave furnishes a precise reference point fortiming from one P wave to another, even fre-quently when the latter are superimposed uponQRS or T.
XXCSjITi-rl-- 1 MktttXX
A1r, BraPi
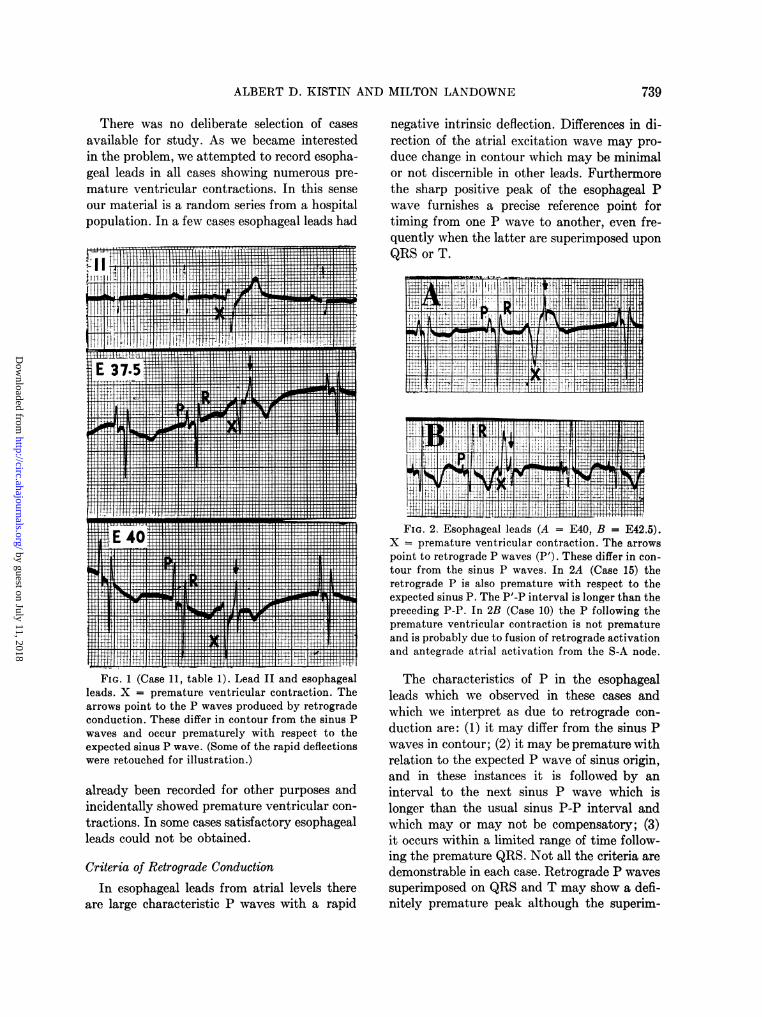
FIG. 2. Esophageal leads (A = E40, B = E42.5).X = premature ventricular contraction. The arrowspoint to retrograde P waves (P'). These differ in con-tour from the sinus P waves. In 2A (Case 15) theretrograde P is also premature with respect to theexpected sinus P. The P'-P interval is longer than thepreceding P-P. In 2B (Case 10) the P following thepremature ventricular contraction is not prematureand is probably due to fusion of retrograde activationand antegrade atrial activation from the S-A node.
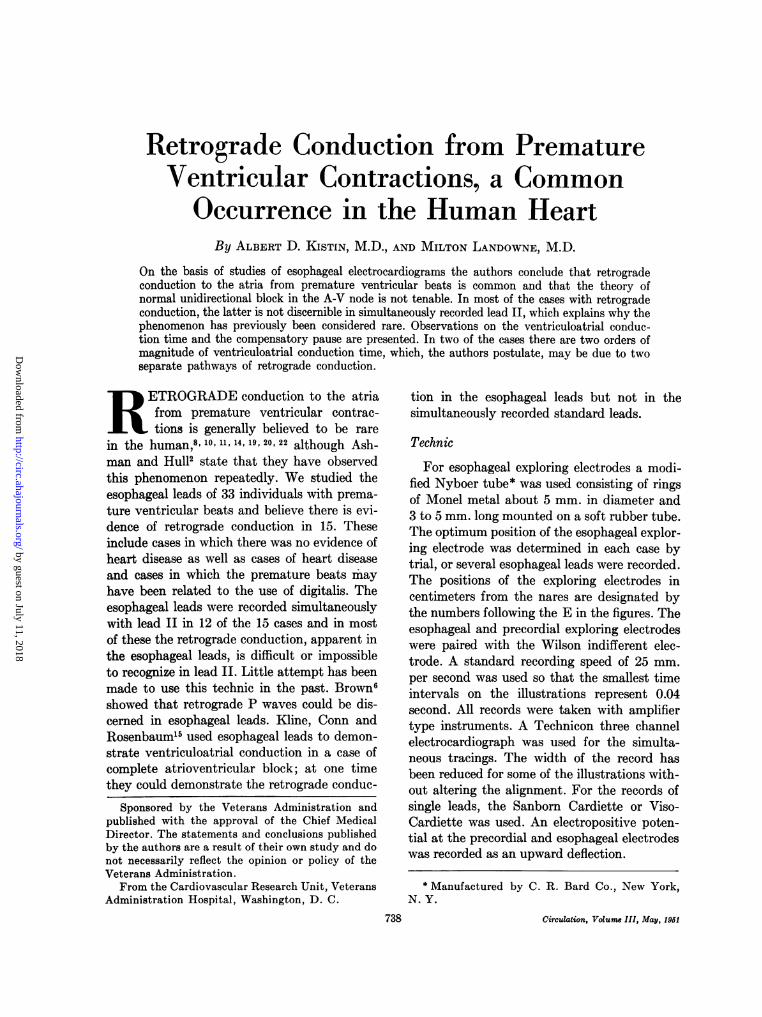
FIG. 1 (Case 11, table 1). Lead II and esophagealleads. X = premature ventricular contraction. Thearrows point to the P waves produced by retrogradeconduction. These differ in contour from the sinus Pwaves and occur prematurely with respect to theexpected sinus P wave. (Some of the rapid deflectionswere retouched for illustration.)
already been recorded for other purposes andincidentally showed premature ventricular con-
tractions. In some cases satisfactory esophagealleads could not be obtained.
Criteria of Retrograde Conduction
In esophageal leads from atrial levels thereare large characteristic P waves with a rapid
The characteristics of P in the esophagealleads which we observed in these cases andwhich we interpret as due to retrograde con-duction are: (1) it may differ from the sinus Pwaves in contour; (2) it may be premature withrelation to the expected P wave of sinus origin,and in these instances it is followed by aninterval to the next sinus P wave which islonger than the usual sinus P-P interval andwhich may or may not be compensatory; (3)it occurs within a limited range of time follow-ing the premature QRS. Not all the criteria aredemonstrable in each case. Retrograde P wavessuperimposed on QRS and T may show a defi-nitely premature peak although the superim-
739
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
RETROGRADE CONDUCTION
position makes contour analysis difficult orimpossible. In cases of fusion beats, that is.combinations of retrograde activation and ante-grade activation from the sinus node, the con-tour of the P following the premature QRS
considerably deeper negative deflection belowthe baseline than the sinus P waves.
In the esophageal leads the retrograde Pneed not be inverted or opposite in directionto the P of sinus origin, although the latter
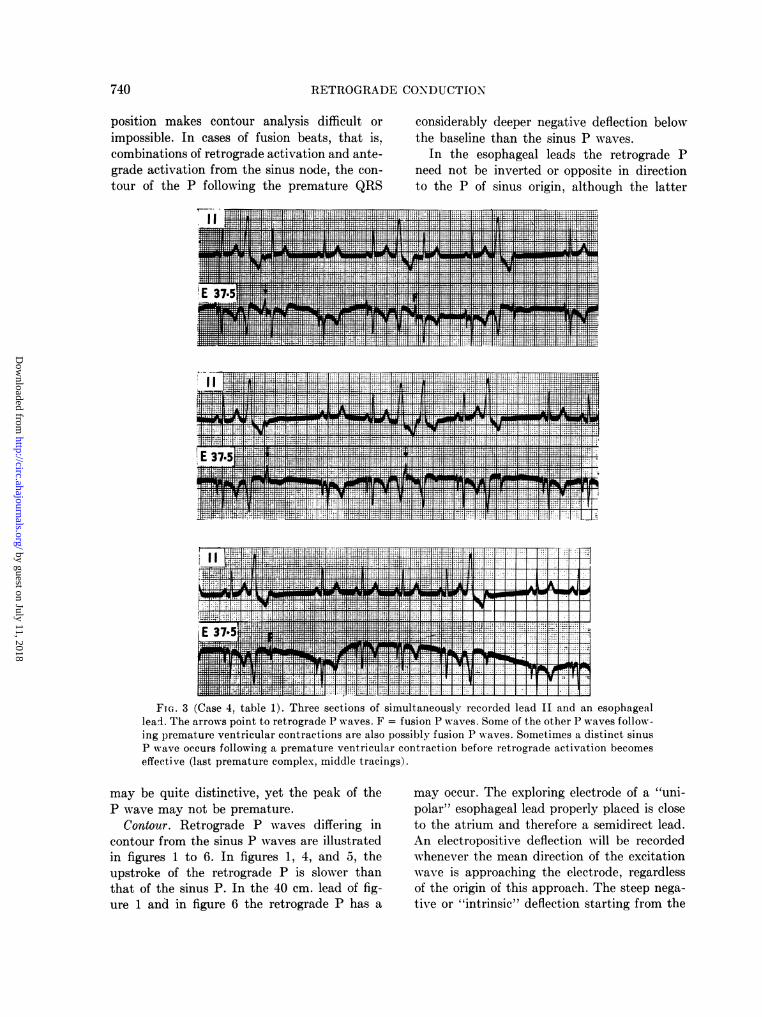
FIG. 3 (Case 4, table 1). Three sections of simultaneously recorded lead II and an esophageallead. The arrows point to retrograde P waves. F = fusion P waves. Some of the other P waves follow-ing premature ventricular contractions are also possibly fusion P waves. Sometimes a distinct sinusP wave occurs following a premature ventricular contraction before retrograde activation becomeseffective (last premature complex, middle tracings).
may be quite distinctive, yet the peak of theP wave may not be premature.
Contour. Retrograde P waves differing incontour from the sinus P waves are illustratedin figures 1 to 6. In figures 1, 4, and 5, theupstroke of the retrograde P is slower thanthat of the sinus P. In the 40 cm. lead of fig-ure 1 and in figure 6 the retrograde P has a
may occur. The exploring electrode of a "uni-polar" esophageal lead properly placed is closeto the atrium and therefore a semidirect lead.An electropositive deflection will be recordedwhenever the mean direction of the excitationwave is approaching the electrode, regardlessof the origin of this approach. The steep nega-tive or "intrinsic" deflection starting from the
740
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

ALBERT D. KISTIN AND MILTON LANDOXYWNE74
positive peak of P represents the peak arrivalof the excitation wave beneath the electrodein direct leads from the myocardium,'7 and isbelieved to approximate the same phenomenonin semidirect leads.5' 31 Deflection of the retro-grade P sometimes may appear to be opposite
tion of P and a later intrinsic deflection willocculr.
Fusion P waves are reliable evidence of retro-grade conduction. These not only differ dis-tinctly in contour from the sinus P waves(figs. 2B, and 5, upper tracings), but may be
FIG. 4 (Case 4, table 1, as in fig. 3). The arrows point to the retrograde P waves which differ incontour from the sinus P waves. In the lower tracings the retrograde P waves are also prematurewith respect to the expected sinus P wave. Il the upper tracings the first retrograde P is also pre-mature, but the second retrograde P is slightly "late" on the basis of the immediately precedingP-P interval, and this is explained by the sinus arrhythmia. In lead II of the upper tracings retro-grade conduction is clearly, indicated by the inverted P, but when the retrograde P occurs sufficiently-early after the premature ventricular contraction (last premature complex, lowter tracings), thereis no evidence of retrograde conduction in lead II. There are reciprocal beats in the upper tracings.In this case there were two discontinuous orders of magnitude of ventriculoatrial conduction times,the shorter times being illustrated in the lower tracings, and the longer times in the upper trac-ings. See text and figure 7.
in direction to that of the sinus P. For ex-ample, an electrode opposite a region of earlyantegrade activation will tend to register a rela-tively early intrinsic deflection, a small positivedeflection of the P and a large negative deflec-tion (figs. 4 and 5). Since this region may berelatively further away from the A-V node, inretrograde activation a larger positive deflec-
recognized also as intermediate in characterbetween P waves produced by retrograde ac-tivation and those produced by antegrade ac-ti-vation (fig. 3). For the recording of fusionatrial beats, lead II and other remote leadsseem to be particularly unsuitable, while anesophageal lead may be most advantageous.Two simultaneous excitation waves traveling
741
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
RETROGRADE CONDUCTION
in approximately opposite directions towardeach other, one from the S-A node and onefrom the A-V node, should tend to neutralizepotential differences between two distant pointsin such leads. This does not hold for the semi-direct esophageal lead. In fact, if the esopha-
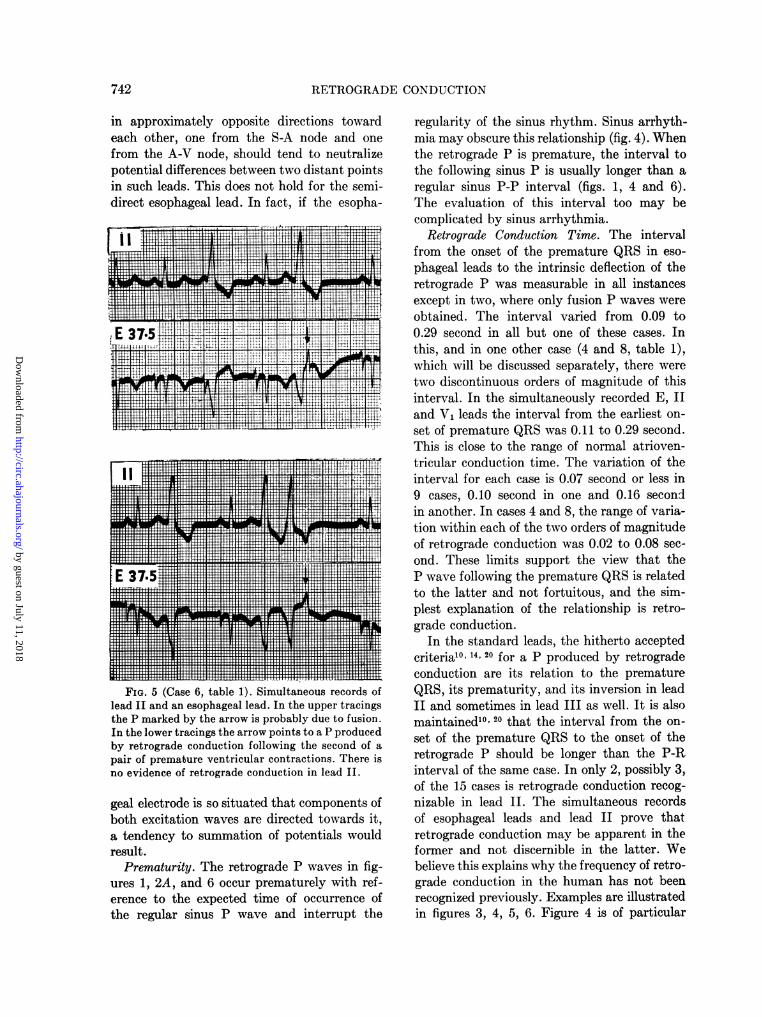
FIG:.5 (Cs 6, tal 1) Siutaeu recordsLofthe P make by the arro isprblydetfuin
Inthe lwetracingsthe maro pint to a Pprduce
geaelcrd iso siuae tha componentsobohxitaion wae arEEdHIrEcte toward itHH .
37*:
akal
411111111111111111111111:
reIXX X t 1 imultas ueLor.s of
PremdIaturity Tohaearetrgad.nte uppwaestainfg-
ure 1, 2A, an 6 aocur prematly wIthfruef
gelerenctrodte expecstutedtime ofporence ofathenrdegul sinusmPwave oand interlr oulp th
reIXsulIlIlt. .Eii aR T lTfl11LoiiLLsi!lIII*IIIIDl||E|Al~l~lflfflfl~T~sl~lrlTr~lllrrfr fllr~llrflllllllll~ln
eren SC aeto theexecedt)imultaneocusrrencrd of
Intheregulrtrainus Pth ae andop interoa rouptted
regularity of the sinus rhythm. Sinus arrhyth-mia may obscure this relationship (fig. 4). Whenthe retrograde P is premature, the interval tothe following sinus P is usually longer than aregular sinus P-P interval (figs. 1, 4 and 6).The evaluation of this interval too may becomplicated by sinus arrhythmia.
Retrograde Conduction Time. The intervalfrom the onset of the premature QRS in eso-phageal leads to the intrinsic deflection of theretrograde P was measurable in all instancesexcept in two, where only fusion P waves wereobtained. The interval varied from 0.09 to0.29 second in all but one of these cases. Inthis, and in one other case (4 and 8, table 1),which will be discussed separately, there weretwo discontinuous orders of magnitude of thisinterval. In the simultaneously recorded E, IIand V, leads the interval from the earliest on-set of premature QRS was 0.11 to 0.29 second.This is close to the range of normal atrioven-tricular conduction time. The variation of theinterval for each case is 0.07 second or less in9 cases, 0.10 second in one and 0.16 secondin another. In cases 4 and 8, the range of varia-tion within each of the two orders of magnitudeof retrograde conduction was 0.02 to 0.08 sec-ond. These limits support the view that theP wave following the premature QRS is relatedto the latter and not fortuitous, and the sim-plest explanation of the relationship is retro-grade conduction.
In the standard leads, the hitherto acceptedcriterial"' 14, 20 for a P produced by retrogradeconduction are its relation to the prematureQRS, its prematurity, and its inversion in leadII and sometimes in lead III as well. It is alsomaintained10' 20 that the interval from the on-set of the premature QRS to the onset of theretrograde P should be longer than the P-Rinterval of the same case. In only 2, possibly 3,of the 15 cases is retrograde conduction recog-nizable in lead II. The simultaneous recordsof esophageal leads and lead II prove thatretrograde conduction may be apparent in theformer and not discernible in the latter. Webelieve this explains why the frequency of retro-grade conduction in the human has not beenrecognized previously. Examples are illustratedin figures 3, 4, 5, 6. Figure 4 is of particular
742
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
ALBERT D. KISTIN AND MILTON LANDOWNE
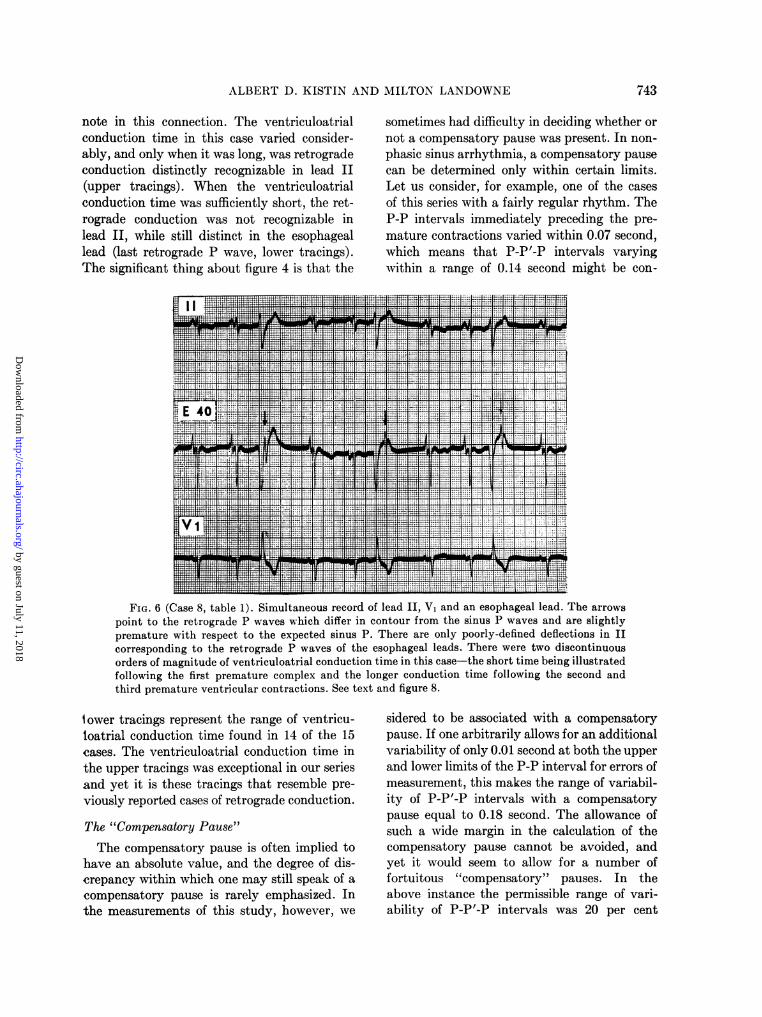
note in this connection. The ventriculoatrialconduction time in this case varied consider-ably, and only when it was long, was retrogradeconduction distinctly recognizable in lead II(upper tracings). When the ventriculoatrialconduction time was sufficiently short, the ret-rograde conduction was not recognizable inlead II, while still distinct in the esophageallead (last retrograde P wave, lower tracings).The significant thing about figure 4 is that the
sometimes had difficulty in deciding whether ornot a compensatory pause was present. In non-phasic sinus arrhythmia, a compensatory pausecan be determined only within certain limits.Let us consider, for example, one of the casesof this series with a fairly regular rhythm. TheP-P intervals immediately preceding the pre-mature contractions varied within 0.07 second,which means that P-P'-P intervals varyingwithin a range of 0.14 second might be con-
.v -m~=fl X L "__1W___ ___1
-41~~~~~point to theretor was whh d r Mincnto fro th-nut wv a sgt
.._ _
co nineto tahlretr d Pwaves reof f leXthe V, aX esophageal leeatwodctous
orders of magnitude of ventriculoatrial conduction time in this case-the short time being illustratedfollowing the first premature complex and the longer conduction time following the second andthird premature ventricular contractions. See text and figure 8.
i ower tracings represent the range of ventricu-loatrial conduction time found in 14 of the 15cases. The ventriculoatrial conduction time inthe upper tracings was exceptional in our seriesand yet it is these tracings that resemble pre-viously reported cases of retrograde conduction.
The "Compensatory Pause"The compensatory pause is often implied to
have an absolute value, and the degree of dis-crepancy within which one may still speak of acompensatory pause is rarely emphasized. Inthe measurements of this study, however, we
sidered to be associated with a compensatorypause. If one arbitrarily allows for an additionalvariability of only 0.01 second at both the upperand lower limits of the P-P interval for errors ofmeasurement, this makes the range of variabil-ity of P-P'-P intervals with a compensatorypause equal to 0.18 second. The allowance ofsuch a wide margin in the calculation of thecompensatory pause cannot be avoided, andyet it would seem to allow for a number offortuitous "compensatory" pauses. In theabove instance the permissible range of vari-ability of P-P'-P intervals was 20 per cent
743
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
44RETROGMADECI)IC'ONDIT('ION
of P-P. If wXe apply the above analysis, therewAas a compensatory pause (fig. 1) more oftenthan not (fig. 2A) following the prematureventricular contractions wvith definite retro-grade conduction in this series.
spontaneous premature atrial contractionswhich may occur much earlier in the cardiaccycle. This limited prematurity of the retro-grade stimulus (table 1) makes the spontaneousdischarge of the sinus node more likely.
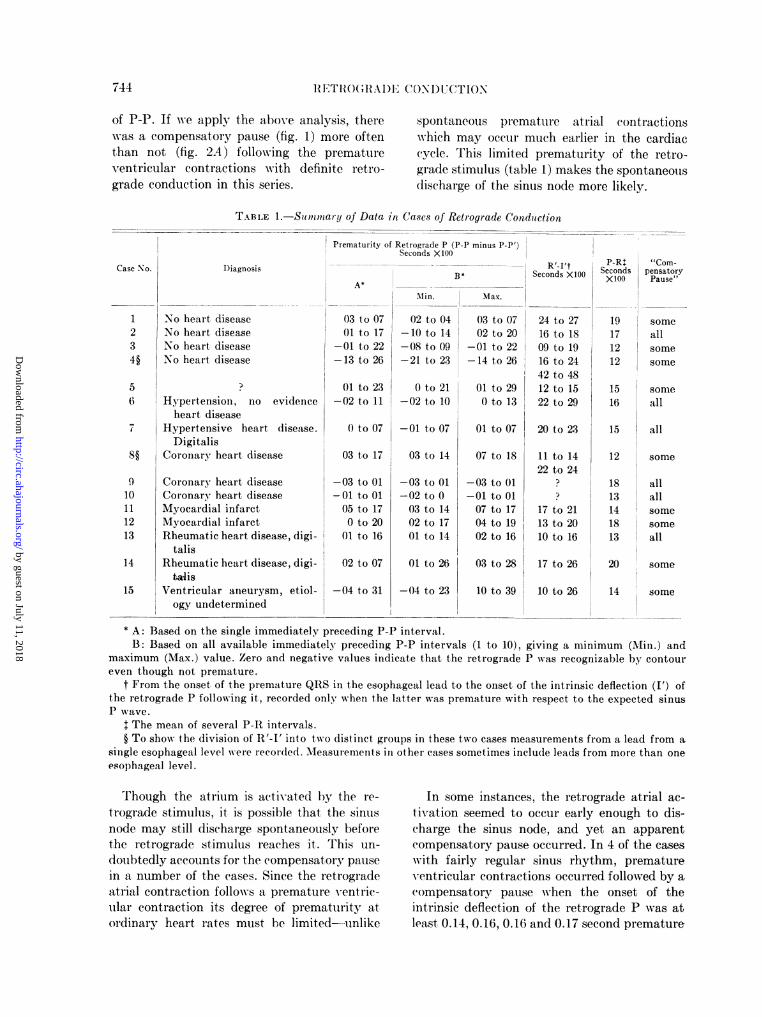
TABLE 1.-So oimnary of Data in Cases of Retrograde Conduction
Prematurity of Retrograde P (P-P minus P-P')Seconds X100
Diagnosis
Min.
No heart diseaseNo heart diseaseNo heart diseaseNo heart disease
Hypertension, no evidenceheart disease
Hypertensive heart disease.Digitalis
Coronary heart disease
Coronary heart diseaseCoronary heart diseaseMyocardial infarctMyocardial infarctRheumatic heart disease, digi-
talisRheumatic heart disease, digi-"lis
Ventricular aneurysm, etiol-ogy undetermined
03 to 0701 to 17
-01 to 22-13 to 26
01 to 23-02 to 11
0 to 07
03 to 17
-03 to 01-01 to 0105 to 170 to 20
01 to 16
02 to 07
-04 to 31
R'-I't PP-R "Com-Seconds X100 Seconds pensatorySecods 100
X100 Pause"
Ma'x.
02 to 04 03 to 07-10 to 14 02 to 20-08 to 09 -01 to 22-21 to 23 -14 to 26
Oto 21 01 to29-02 to 10 O to 13
-01 to 07
03 to 14
-03 to 01-02 to 003 to 1402 to 1701 to 14
01 to 26
-04 to 23
01 to 07
07 to 18
-03 to 01-01 to 0107 to 1704 to 1902 to 16
03 to 28
10 to 39
24 to 2716 to 1809 to 1916 to 2442 to 4812 to 1522 to 29
20 to 23
11 to 1422 to 24
17 to 2113 to 2010 to 16
17 to 26
10 to 26
19171212
1516
15
someallsomesome
someall
all
12 some
1813141813
allallsome
some
all
20 some
14 some
* A: Based on the single immediately preceding P-P interval.B: Based on all available immediately preceding P-P intervals (1 to 10), giving a minimum (Min.) and
maximum (Max.) value. Zero and negative values indicate that the retrograde P was recognizable by contoureven though not premature.
t From the onset of the premature QRS in the esophageal lead to the onset of the intrinsic deflection (I') ofthe retrograde P following it, recorded only when the latter was premature with respect to the expected sinusP wave.
$ The mean of several P-R intervals.§ To show the division of RA'-I' into two distinct groups in these two cases measurements from a lead from a,
single esophageal level were recorded. Measurements in other cases sometimes include leads from more than one
esophageal level.
Though the atrium is activated by the re-
trograde stimulus, it is possible that the sinusnode may still discharge spontaneously beforethe retrograde stimulus reaches it. This un-
doubtedly accounts for the compensatory pausein a number of the cases. Since the retrogradeatrial contraction follows a premature ventric-ular contraction its degree of prematurity atordinary heart rates must be limited-unlike
In some instances, the retrograde atrial ac-
tivation seemed to occur early enough to dis-charge the sinus node, and yet an apparentcompensatory pause occurred. In 4 of the cases
with fairly regular sinus rhythm, prematureventricular contractions occurred followed by a
(ompensatory pause when the onset of theintrinsic deflection of the retrograde P was atleast 0.14, 0.16, 0.16 and 0.17 second premature
Case No.
1234§
56
7
910111213
14
15
744
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

ALBERT D. KISTIN A-ND MILTON LANDOWNE4'
respectively, as measured on the basis of theshortest of the P-P intervals immediately pre-ceding the premature contraction. Since thenormal duration of the P wave is less than 0.14second, such excitation would be expected todischarge the sinus node unless some delay inactivation occurs at the latter. The P'-P inter-val following the retrograde atrial activationis somewhat longer than the P-P interval justas it is following spontaneous premature atrialcontractions. It is possible that a slightly de-creased P-P' interval plus a slightly increasedP'-P interval should sometimes add up to ap-proximately twice P-P by chance, even thoughthe sinus node is discharged by retrograde atrialactivation.
The Ventriculoatrial Conduiction Time
As an index of ventriculoatrial conductiontime we measured the interval from the onsetof the premature QRS to the onset of the in-trinsic deflection of the retrograde P (R'-J' in-terval). The onset of the retrograde P isfrequently impossible to time precisely in theesophageal leads. We use the designation R'-I'rather than R'-P' because the latter has beenrecorded in the literature as a measurementfrom the onset of the ectopic QRS to the onsetof the retrograde P. The over-all range of 11R-I'and the variation in a given case have alreadybeen discussed and are summarized in table 1.In 10 cases the earliest onset of the prematureQRS in the simultaneously recorded esophageallead and lead II (and often V,) was measured,and the minimum R'-' was equal to or smallerthan the P-R immediately preceding it in 5cases (cases 3, 5, 8, 13, 14, table 1). The inter-val exceeded the preceding P-R by 0.01 secondin one case, 0.05 and 0.07 second in 2 caseseach. The minimum R'-J' is an approach tothe ventriculoatrial conduction time least af-fected by the refractoriness of the conductingtissues. In cases 4 and 8, with two groups ofR'-J' intervals (see below), the minimum R'-I'was within 0.03 of P-R in the group of shorterintervals, but exceeded P-R by 0.31 and 0.10second, respectively, in the group of longerintervals. It has been stated that the R'-P'interval resulting from retrograde conductionis longer than the P-li interval in the samecase.10, 20
The P-R and li'-P' intervals are not strictlycomparable as an indication of the relativespeeds of conduction, since the pathways ofantegrade and retrograde conduction are dif-ferent. Even if it is assumed that the pathwaysare comparable in length, the two intervals donot necessarily represent relative speeds of con-duction under similar conditions, because theconduction from ventricle to atrium occurringearly in the cardiac cycle is more apt to en-counter refractoriness in the A-V node. Forcomparison with P-R the same limitations ap-ply, of course, to l'-I' as to l'-P'.
Winternitz and Langendorf32 reviewed theliterature and tabulated the R-P' intervals inreported cases of retrograde conduction occur-ring with incomplete and complete atrioven-tricular block. Of the twenty-three cases citedby these authors, the R-P' interval was 0.20second or less in sixteen. This evidence addedto our observations in cases where antegradeconduction was not abnormal does not supportthe thesis that the retrograde ventriculoatrialconduction time in the human is consistentlygreater than the normal atrioventricular con-duction time.
In experimental animals retrograde conduc-tion to the atria from artificially induced pre-mature ventricular contractions has beenobserved repeatedly.4 7, 18, 21, 23, 27, 29, 30 Someobservers found the ventriculoatrial time slowerthan the atrioventricular time,4' 27, 29 and othersfound the reverse.7 30 Comprehensive summaryand evaluation of the experimental data isdifficult. The conditions of the experiments ofthe different observers are not strictly com-parable, and sometimes the experimental con-ditions during ventriculoatrial conduction differfrom those during atrioventricular conduction.Furthermore, there may be differences amonganimal groups; von Skramlik found atrioven-tricular conduction faster than ventriculoatrialconduction in frogs,29 but the reverse in fish.30Comparative data of atrioventricular and
ventriculoatrial conduction times in mammalsare limited. Both Bayliss and Starling4 andStassen27 found the ventriculoatrial conductiontime longer than the atrioventricular time indogs. The former authors, however, were care-ful to point out that they made only few ob-servations, and the accuracy of their mechani-
745
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
RETROGRADE CONDUCTION
1.00k
az0v
0 0
0:000*I.0
0 00 0
0.90[os.oF
G.
0;*0a0.70[
-I0.55fo 0.50
z0v
0.45
^ 0.4Q
3-.
V.
0.15 0.t0 0425 030 0o-5 0.40 0.45 0.50
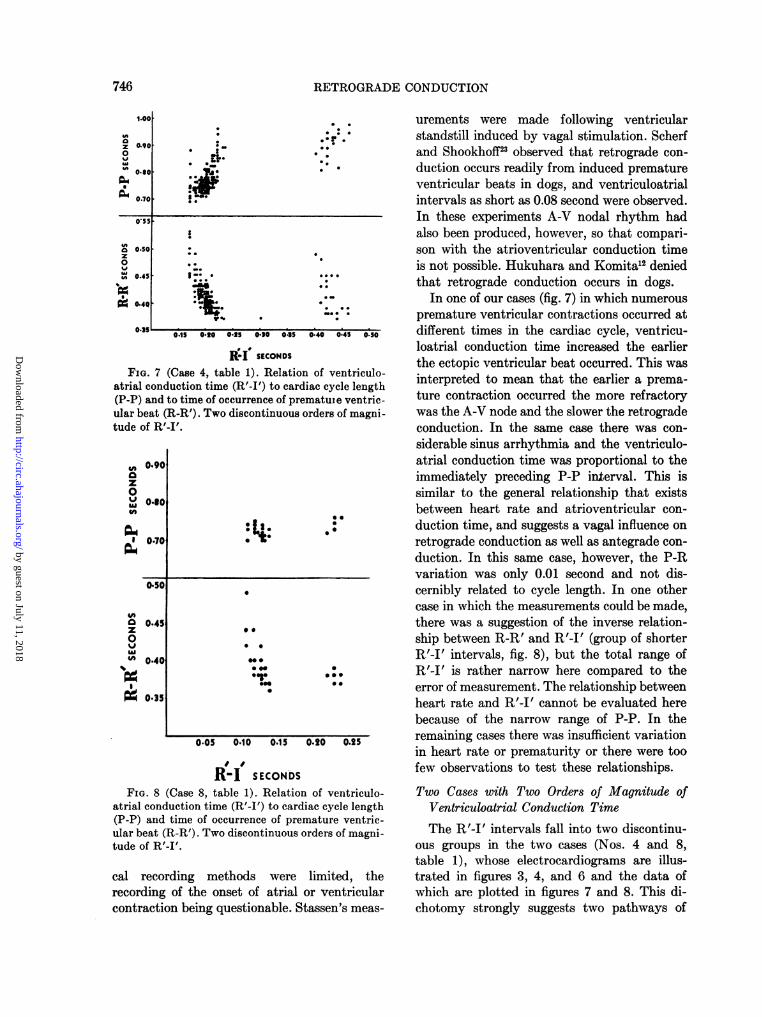
R-I SECONDSFIG. 7 (Case 4, table 1). Relation of ventriculo-
atrial conduction time (R'-I') to cardiac cycle length(P-P) and to time of occurrence of premature ventric-ular beat (R-R'). Two discontinuous orders of magni-tude of R'-I'.
., 0.90
z0
0.60
o1 0.70
040
0 0.45z
0
" 0.40
*0
090.35
.
0 0
00
0
0 0
* 0
00*
*cr 0*00 a
0.05 0.10 0.15 0.20 0.25
R-I SECONIDSFIG. 8 (Case 8, table 1). Relation of ventriculo-
atrial conduction time (R'-I') to cardiac cycle length(P-P) and time of occurrence of premature ventric-ular beat (R-R'). Two discontinuous orders of magni-tude of R'-I'.
cal recording methods were limited, therecording of the onset of atrial or ventricularcontraction being questionable. Stassen's meas-
urements were made following ventricularstandstill induced by vagal stimulation. Scherfand Shookhoff23 observed that retrograde con-duction occurs readily from induced prematureventricular beats in dogs, and ventriculoatrialintervals as short as 0.08 second were observed.In these experiments A-V nodal rhythm hadalso been produced, however, so that compari-son with the atrioventricular conduction timeis not possible. Hukuhara and Komita'2 deniedthat retrograde conduction occurs in dogs.
In one of our cases (fig. 7) in which numerouspremature ventricular contractions occurred atdifferent times in the cardiac cycle, ventricu-loatrial conduction time increased the earlierthe ectopic ventricular beat occurred. This wasinterpreted to mean that the earlier a prema-ture contraction occurred the more refractorywas the A-V node and the slower the retrogradeconduction. In the same case there was con-siderable sinus arrhythmia and the ventriculo-atrial conduction time was proportional to theimmediately preceding P-P interval. This issimilar to the general relationship that existsbetween heart rate and atrioventricular con-duction time, and suggests a vagal influence onretrograde conduction as well as antegrade con-duction. In this same case, however, the P-Rvariation was only 0.01 second and not dis-cernibly related to cycle length. In one othercase in which the measurements could be made,there was a suggestion of the inverse relation-ship between R-R' and R'-I' (group of shorterR'-I' intervals, fig. 8), but the total range ofR'-I' is rather narrow here compared to theerror of measurement. The relationship betweenheart rate and R'-I' cannot be evaluated herebecause of the narrow range of P-P. In theremaining cases there was insufficient variationin heart rate or prematurity or there were toofew observations to test these relationships.Two Cases with Two Orders of Magnitude of
Ventriculoatrial Conduction TimeThe R'-I' intervals fall into two discontinu-
ous groups in the two cases (Nos. 4 and 8,table 1), whose electrocardiograms are illus-trated in figures 3, 4, and 6 and the data ofwhich are plotted in figures 7 and 8. This di-chotomy strongly suggests two pathways of
0. 5 -.
746
s
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
ALBERT D. KISTIN AND MILTON LANDOWNE
retrograde conduction, pathways with eitherabsolute differences in rate of conduction ordifferences in duration of relative refractoriness.So far as we know this has not previously beendescribed.
Retrograde atrial activation did not followall premature ventricular contractions in thetracings from which figure 7 was charted. Some-times a regular sinus P wave occurred beforeretrograde conduction became effective. The
intervals the smaller order of magnitude ismore apt to occur. A sinus P wave or an R'-J'interval of the larger order of magnitude followsa premature beat only when the more rapid orderof conduction fails, and such failures may beexpressed as a proportion of the total numberof premature beats in a given range of heartrates. In this case this proportion was foundto be distinctly higher at slower heart ratesthan at fast rates. Exactly what factors asso
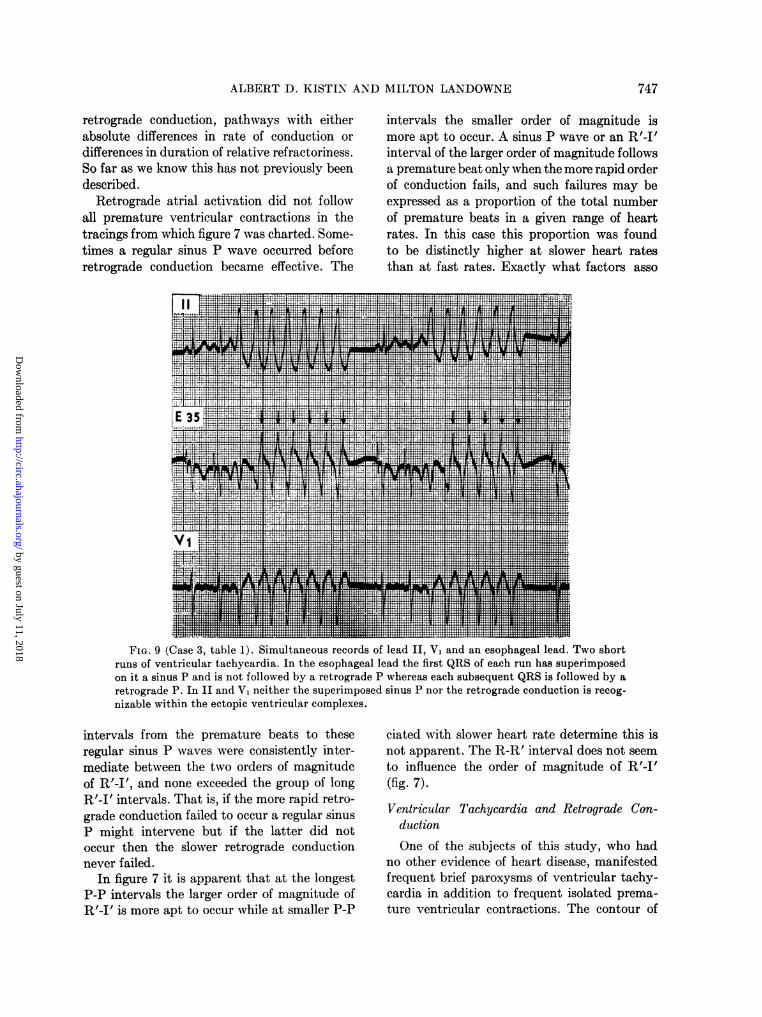
FIG. 9 (Case 3, table 1). Simultaneous records of lead II, V1 and an esophageal lead. Two shortruns of ventricular tachycardia. In the esophageal lead the first QRS of each run has superimposedon it a sinus P and is not followed by a retrograde P whereas each subsequent QRS is followed by aretrograde P. In II and V1 neither the superimposed sinus P nor the retrograde conduction is recog-nizable within the ectopic ventricular complexes.
intervals from the premature beats to theseregular sinus P waves were consistently inter-mediate between the two orders of magnitudeof R'-J', and none exceeded the group of longR'-J' intervals. That is, if the more rapid retro-grade conduction failed to occur a regular sinusP might intervene but if the latter did notoccur then the slower retrograde conductionnever failed.
In figure 7 it is apparent that at the longestP-P intervals the larger order of magnitude ofR'-I' is more apt to occur while at smaller P-P
ciated with slower heart rate determine this isnot apparent. The R-R' interval does not seemto influence the order of magnitude of R'-J'(fig. 7).Ventricular Tachycardia and Retrograde Con-
ductionOne of the subjects of this study, who had
no other evidence of heart disease, manifestedfrequent brief paroxysms of ventricular tachy-cardia in addition to frequent isolated prema-ture ventricular contractions. The contour of
747
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
8RETROGRADE CONDUCTION
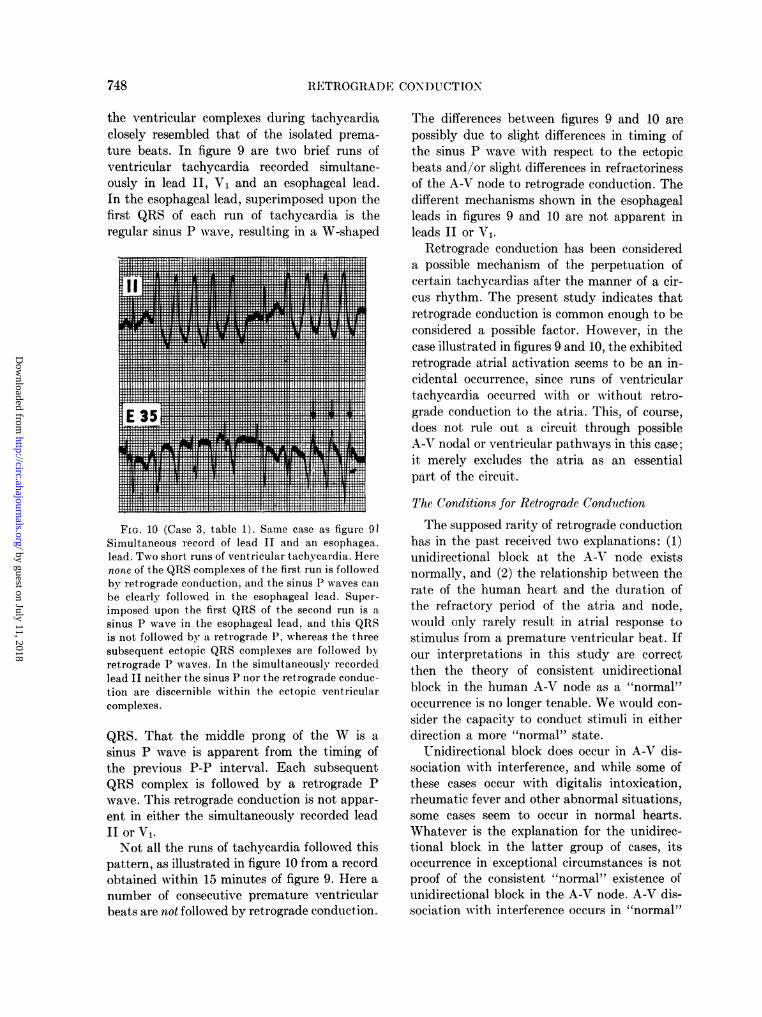
the ventricular complexes during tachycardiaclosely resembled that of the isolated prema-ture beats. In figure 9 are two brief runs ofventricular tachycardia recorded simultane-ously in lead II, V1 and an esophageal lead.In the esophageal lead, superimposed upon thefirst QRS of each run of tachycardia is theregular sinus P wave, resulting in a W-shaped
FIG. 10 (Case 3, table 1). Same case as figure 91Simultaneous record of lead II and an esophagea.lead. Two short runs of ventricular tachycardia. Herenone of the QRS complexes of the first run is followedby retrograde conduction, and the sinus P waves can
be clearly followed in the esophageal lead. Super-imposed upon the first QRS of the second run is a
sinus P wave in the esophageal lead, and this QRSis not followed by a retrograde P, whereas the threesubsequent ectopic QRS complexes are followed byretrograde P waves. In the simultaneously recordedlead II neither the sinus P nor the retrograde conduc-tion are discernible within the ectopic ventricularcomplexes.
QRS. That the middle prong of the W is a
sinus P wave is apparent from the timing ofthe previous P-P interval. Each subsequentQRS complex is follow-ed by a retrograde Pwave. This retrograde conduction is not appar-ent in either the simultaneously recorded leadII or V1.Not all the runs of tachycardia followed this
pattern, as illustrated in figure 10 from a recordobtained within 15 minutes of figure 9. Here a
number of consecutive premature ventricularbeats are not followed by retrograde conduction.
The differences between figures 9 and 10 arepossibly due to slight differences in timing ofthe sinus P wave with respect to the ectopicbeats and/or slight differences in refractorinessof the A-V node to retrograde conduction. Thedifferent mechanisms shown in the esophagealleads in figures 9 and 10 are not apparent inleads II or V,.
Retrograde conduction has been considereda possible mechanism of the perpetuation ofcertain tachyeardias after the manner of a cir-cus rhythm. The present study indicates thatretrograde conduction is common enough to beconsidered a possible factor. However, in thecase illustrated in figures 9 and 10, the exhibitedretrograde atrial activation seems to be an in-cidental occurrence, since runs of ventriculartachycardia occurred with or without retro-grade conduction to the atria. This, of course,does not rule out a circuit through possibleA-V nodal or ventricular pathways in this case;it merely excludes the atria as an essentialpart of the circuit.
The Conditions for Retrograde ConductionThe supposed rarity of retrograde conduction
has in the past received two explanations: (1)unidirectional block at the A-V node existsnormally, and (2) the relationship between therate of the human heart and the duration ofthe refractory period of the atria and node,would only rarely result in atrial response tostimulus from a premature ventricular beat. Ifour interpretations in this study are correctthen the theory of consistent unidirectionalblock in the human A-V node as a "normal"occurrence is no longer tenable. We would con-sider the capacity to conduct stimuli in eitherdirection a more "normal" state.
Unidirectional block does occur in A-V dis-sociation with interference, and while some ofthese cases occur with digitalis intoxication,rheumatic fever and other abnormal situations,some cases seem to occur in normal hearts.Whatever is the explanation for the unidirec-tional block in the latter group of cases, itsoccurrence in exceptional circumstances is notproof of the consistent "normal" existence ofunidirectional block in the A-V node. A-V dis-sociation with interference occurs in "normal"
748
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
ALBERT D. KISTIN AND MILTON LANDOWNE
cases sometimes with pronounced sinus ar-rhythmia, and possibly intense vagal stimula-tion is involved in these cases. Experimentally,it is necessary to injure the myocardium inorder to produce unidirectional block." 9, 24Englemann9 noted a long time ago in frogs thatconduction is equally rapid in either directionbut that unidirectional block sets in as theanimal is dying or as a result of nerve stimula-tion or toxins. In some cases of incomplete orcomplete atrioventricular block retrograde con-duction to the atria may occur from beats ofidioventricular origin.3 15, 25, 26, 32 In otherwords, in these cases there is unidirectionalblock in the reverse direction, and this is com-parable to the unidirectional block producedexperimentally as a result of myocardial injury.The interrelations of the heart rate, the re-
fractory periods, and the time of occurrencein the cardiac cycle of the premature ventricu-lar contraction remain to explain the cases inwhich retrograde conduction does not occur.In most of the 18 cases in which we did notfind retrograde conduction, the reason wasquite obvious. In these cases the prematureQRS occurred immediately before or after asinus P so that one might expect the atriumand/or A-V node to be refractory to retrogradeactivation. In some cases only few of manyrecorded premature ventricular contractionsshowed retrograde conduction although longrecords were obtained, and in some cases rec-ords were repeated at different times. In thesecases the relationships of the factors under dis-cussion happened to be favorable for these fewbeats, for example, adequate slowing of the heartrate and sufficient prematurity of the prema-ture ventricular contraction.
Possible Objections to the InterpretationsTwo possible objections to our interpreta-
tions must be considered: (1) The prematurebeats we have illustrated may be of nodal ori-gin with aberrant conduction. This cannot becompletely ruled out for any so-called ventricu-lar premature beat. However, this series in-cludes only those cases in which the contour ofthe QRS of the premature contractions differedsignificantly from that of the regularly occur-ring QRS complexes. In one case there were
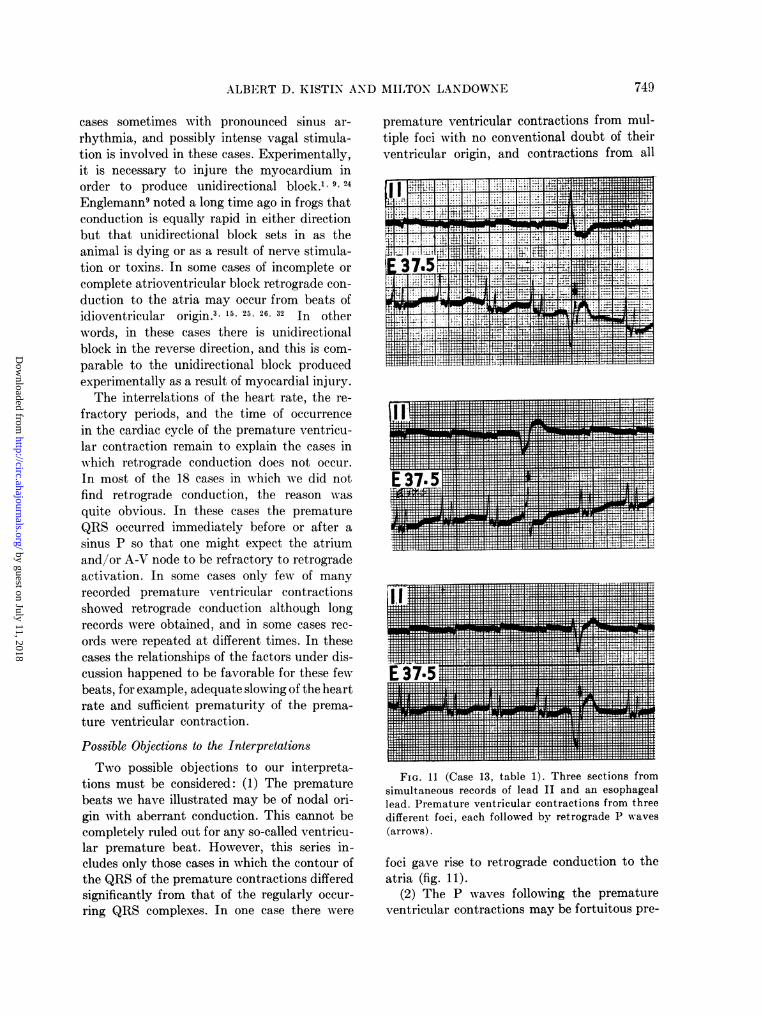
premature ventricular contractions from mul-tiple foci with no conventional doubt of theirventricular origin, and contractions from all
4n... ...M ..
Tm _f s'E;i,-
t.s .vvH ._V ,.-TE f
FIG. 11 (Case 13, table 1). Three sections fromsimultaneous records of lead II and an esophageallead. Premature ventricular contractions from threedifferent foci, each followed by retrograde P waves(arrows).
foci gave rise to retrograde conduction to theatria (fig. 11).
(2) The P waves following the prematureventricular contractions may be fortuitous pre-
749
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
RETROGRADE CONDUCTION
mature atrial contractions not due to retrogradeconduction. Against this objection, there wereat least several premature ventricular contrac-tions with retrograde conduction in each casein which this interpretation was made. In anumber of the cases many premature ventricu-lar contractions with retrograde conductionwere studied and in some of the subjects theretrograde conduction was demonstrated re-peatedly at different times. In only 2 of the15 cases, which we believe showed retrogradeconduction, did long records show prematureatrial contractions that were clearly spontane-ous and occurred at times other than immedi-ately following the premature QRS complexes.In one of these there was a single complex ofthis type, and in the second case there were anumber. The P waves which we interpreted asretrograde in these two cases were different incontour from the spontaneous premature atrialcontractions occurring at other times. It hasalready been shown that R'-I' in the 15 casesas a whole is not far from the range of normalP-R, and R'-I' in a given case falls within anarrow range. These facts also are against thefortuitous nature of the atrial contractions andfavor retrograde conduction.
SUMMARY AND CONCLUSIONS
1. Retrograde conduction to the atria frompremature ventricular contractions was dem-onstrated in 15 of 33 unselected individuals bymeans of esophageal leads. The large, peakedP waves obtained in esophageal leads from theatrial level are favorable for this study. In 12of these 15 cases the esophageal leads wererecorded simultaneously with lead II, and inmost of these cases the retrograde conductionis not recognizable in lead II.
2. The P wave due to retrograde conductionin the esophageal leads (a) may differ in con-tour from the sinus P wave, (b) may be pre-mature with respect to the expected sinus Pwave in which case the interval to the next si-nus P wave is longer than a sinus P-P interval,and (c) occurs within a limited range of timefollowing the premature QRS.
3. A compensatory pause may or may notbe present with retrograde conduction. Some of
the cases with a compensatory pause may beexplained by the spontaneous discharge of thesinus node before the retrograde impulsereaches it. The limited degree of prematurityof the retrograde atrial activation following anantecedent premature ventricular contractionfavors spontaneous discharge of the sinus node.In some cases with an apparent compensatorypause, however, the retrograde atrial activationwas sufficiently premature so that this explana-tion does not hold, and in these cases the"compensatory pause" is unexplained or for-tuitous. The range of variation which entersinto the calculation of the compensatory pauseis discussed.
4. There is no evidence that the ventriculo-atrial conduction time is consistently longerthan the atrioventricular conduction time inhuman beings. Therefore, the human A-V node"normally" conducts in either direction, andthere is no evidence for "normal" unidirec-tional block. The failure of retrograde conduc-tion to occur in some cases may be explainedby the interrelationships of heart rate, refrac-tory periods, and time within the cardiac cycleof occurrence of the premature ventricular con-traction.
5. In 2 cases in which adequate measure-ments were possible, the ventriculoatrial con-duction time increased the earlier the prema-ture ventricular contraction occurred. This wasinterpreted to indicate that the earlier a pre-mature contraction occurred, the more refrac-tory was the A-V node. In one of these caseswith pronounced sinus arrhythmia, the ven-triculoatrial conduction time was also propor-tional to the cycle length. This suggests a vagalinfluence on retrograde as well as antegradeconduction.
6. In 2 cases there were two discontinu-ous orders of magnitude of ventriculoatrial con-duction time, and it is postulated that this wasdue to two separate pathways for retrogradeconduction.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the technicalassistance of Mr. Raymond Flath and Mr. HenryG. Gillem.
750
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
ALBERT D. KISTIN AND MILTON LANDOWNE
REFERENCES1ASHMAN, R., AND HAFKESBRING, R.: Unidirec-
tional block in heart muscle. Am. J. Physiol. 91:65, 1929.
2-, AND HULL, E.: Essentials of Electrocardiogra-phy, ed. 2. New York, The Macmillan Co., 1947.P. 200.
3AVERBUCK, S. H.: Adams-Stokesscher Symptomen-komplex, Cheyne-Stokessche Atmung und rick-laufige tVberleitung in einem Fall von kom-plettem Herzblock. Wien. Arch. f. inn. Med. 22:49, 1932.
4BAYLISS, W. M., AND STARLING, E. H.: On somepoints in the innervation of the mammalianheart. J. Physiol. 13: 407, 1892.
5BROWN, W. H.: A study of the esophageal lead inclinical electrocardiography. Part I. The appli-cation of the esophageal lead to the human sub-ject with observations on the Ta-wave, extra-systoles and bundle-branch block. Am. Heart J.12: 1, 1936.
6 : A study of the esophageal lead in clinical elec-trocardiography. Part II. An electrocardio-graphic study of auricular disorders in thehuman subject by means of the esophageal lead.Am. Heart J. 12: 307, 1936.
7 CARLSON, A. J.: Contributions to the physiologyof the heart of the California hagfish (Bdello-stoma dombeyi). Ztschr. f. allg. Physiol. 4: 259,1904.
8 DRESSLER, W.: Zur Frage der Entstehung derInterferenzdissoziation und der retrogradenFortleitung ventrikularer Extrasystolen. Wien.Arch. f. inn. Med. 19: 611, 1930.
9 ENGELMANN, T. W.: tiber reciproke und irrecip-roke Reizleitung mit besonderer Beziehung aufdas Herz. Arch. f. d. ges. Physiol. 61: 275, 1895.
10 GUSSENBAUER, R.:tXber retrograde Extrasystolen.Wien. Arch. f. inn. Med. 6: 423, 1923.
11 HOFF, H. E.: Events of the cardiac cycle. In Ful-ton, J. F.: Howell's Textbook of Physiology, ed.15. Philadelphia, W. B. Saunders Co., 1946. P.726.
12HUKUHARA, T., AND KOMITA, S.: Pflanzt sich dieReizung der Kammer bei Saugetieren auf dieVorh6fe fort? Arch. f. d. ges. Physiol. 241: 444,1938.
13ISHIHAMA, F.: t~ber den Temperaturkoeffizientender recht- und riicklaufigen Erregungsleitungbeim Kaltbluiterherzen. Arch. f. d. ges. Physiol.202: 308, 1924.
14KATz, L. N.: Electrocardiography, ed. 2. Phila-delphia, Lea and Febiger, 1946. P. 570.
15KLINE, E. M., CONN, J. W., AND ROSENBAUM,F. F.: Variations in A-V and V-A conductiondependent upon the time relations of auricu-lar and ventricular systole: the supernormalphase. Am. Heart J. 17: 524, 1939.
16LANGENDORF, R., KATZ, L. N., AND SIMON, A. J.:
Reciprocal beating initiated by ventricular pre-mature systoles. Brit. Heart J. 6: 13, 1944.
17LEWIS, T., MEAKINS, J., AND WHITE. P. D.: Theexcitatory process in the dog's heart. Part I.The auricles. Phil. Trans. Roy. Soc. London,s.B. 205: 375, 1914.
18MINES, G. R.: On dynamic equilibrium in theheart. J. Physiol. 46: 349, 1913.
19 POTTS, R. H., AND ASHMAN, R.: A case of dextro-cardia with right (functional left) ventricularpredominance, ventricular ectopic beats, andretrograde conduction. Am. Heart J. 2: 152,1926.
20 SAMET, B.: tCber einen Fall von retrograden Kam-merextrasystolen. Wien. Arch. f. inn. Med. 14:11, 1927.
21 SCHERF, D.: An experimental study of reciprocat-ing rhythm. Arch. Int. Med. 67: 372, 1941.
22_, AND BOYD, L. J.: Clinical Electrocardiography,ed. 2. Philadelphia, J. B. Lippincott Co., 1946.P. 131.
23 -, AND SHOOKHOFF, C.: Experimentelle Unter-suchungen uber die "Umkehr-Extrasystole" (Re-ciprocating Beat). Wien. Arch. f. inn. Med. 12:501, 1926.
24 SCHMITT, F. 0., AND ERLANGER, J.: Directionaldifferences in the conduction of the impulsethrough heart muscle and their possible relationto extrasystolic and fibrillary contractions. Am.J. Physiol. 87: 326, 1928.
25SCHRAMM, E., AND KORTH, C.: tiber die Rick-leitung automatischer AV-Reize zum Vorhof beikomplettem AV-Block. Klin. Wchnschr. 16: 771,1937.
26SEGERS, M.: La conduction irreciproque dans lecoeur. Persistance de la transmission retrogradeau cours du bloc auriculo-ventriculaire. Actacardiol. 1: 123, 1946.
27STASSEN, M.: Sur les pulsations provoqu6es parl'6xcitation directe du coeur pendant l'arret dMa la t6tanisation du pneumogastrique. Arch.internat. de physiol. 2: 259, 1905.
2 TANCRE, E.: Untersuchungen utber kontinuerlicheBigeminie. Retrograde Extrasystolie. Ztschr. f.klin. Med. 90: 402, 1921.
29 VON SKRAMLIK, E.: Mtber die Beziehungen zwischender normalen und riucklaufigen Erregungsleitungbeim Froschherzen. Arch. f. d. ges. Physiol. 184:1, 1920.
30 VON SKRAMLIK, E.: Herzmuskel und Extrareize.Jena, Gustav Fischer, 1932.
31 WILSON, F. N.: The distribution of the potentialdifferences produced by the heart beat withinthe body and at its surfaces. Am. Heart J. 5:599, 1930.
32 WINTERNITZ, M., AND LANGENDORF, R.: Auriculo-ventricular block with ventriculoauricular re-sponse. Report of six cases and critical reviewof the literature. Am. Heart J. 27: 301, 1944.
751
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
ALBERT D. KISTIN and MILTON LANDOWNEOccurrence in the Human Heart
Retrograde Conduction from Premature Ventricular Contractions, a Common
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1951 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.3.5.738
1951;3:738-751Circulation.
http://circ.ahajournals.org/content/3/5/738the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document.
Permissions and Rights Question and Answer Further information about this process is available in therequested is located, click Request Permissions in the middle column of the Web page under Services.the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from