responding to disasters - winnipeg regional health … · responding to disasters ... • typhoid...
TRANSCRIPT

Responding to Disasters Preparing for humanitarian and disaster
relief work

Responding to Disasters Preparing for humanitarian and disaster
relief work
Dr. Pierre J. PlourdeMedical Officer of Health
Winnipeg Regional Health Authority
Associate Professor, Departments of Medical Microbiology and Community Health Sciences, University of Manitoba

•
Honoraria from GSK for presentations on travel health and tropical medicine
Responding to Disasters Preparing for humanitarian and disaster
relief work
Disclosure

Not all travellers are the same

Humanitarian/Disaster Response Worker
Haiti 2010 Earthquake
Plan Your Trip in AdvanceStart ASAP – may not have much timeInform yourself of:
• destination (currentsituation, political)
• health care system• local tropical diseases• www.cdc.gov/travel• www.cia.gov/cia/publications/factbook/index.html

Plan Your Trip in Advance
www.travelhealth.gc.ca

Plan Your Trip in Advance
www.travel.gc.ca

HCW Fears
Haiti –
Most Common Diagnoses• Malaria (falciparum)
• Typhoid fever• GERD• Helminths
(hookworm, ascariasis)
• Hypertension• Scabies• Ringworm (Tinea)
• Gastroenteritis• Tuberculosis
• Asthma• STI/PID• UTI• Viral URTI

• Routine– Childhood/adult immunizations
• Recommended– According to specific risks
• Required– To cross international borders
Immunization Categories
• Incidence/Outbreaks of VPD at destination
•Risk behaviours•Vaccine Efficacy•Vaccine-associated
adverse events•Vaccine Cost
Travel Vaccine Considerations
• Incidence/Outbreaks of VPD at destination
•Risk behaviours•Vaccine Efficacy•Vaccine-associated
adverse events•Vaccine Cost
Travel Vaccine Considerations
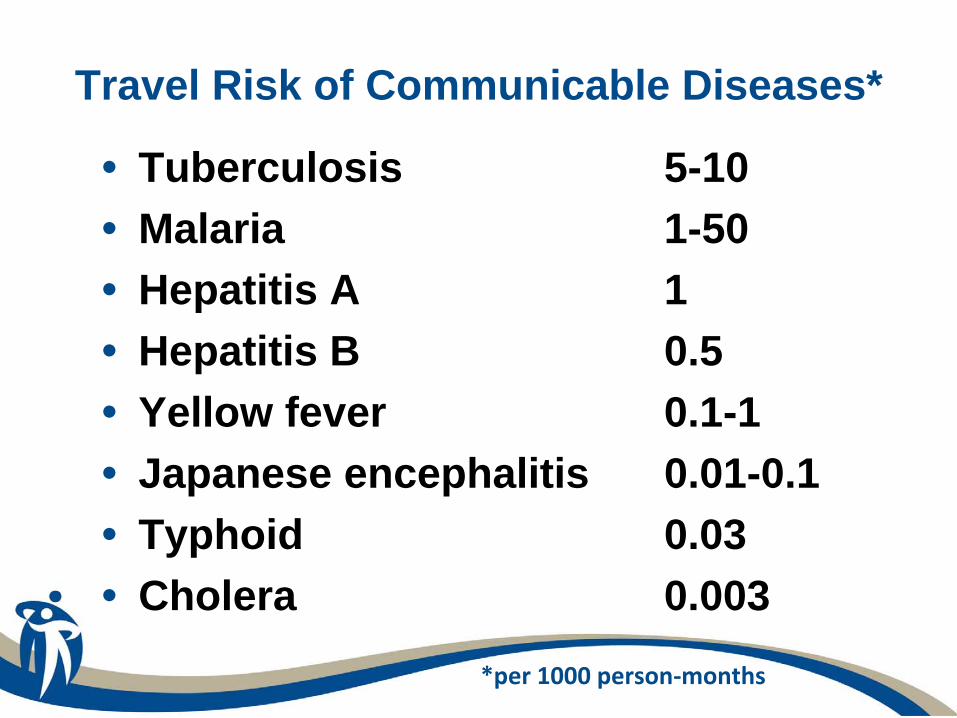
Travel Risk of Communicable Diseases*
• Tuberculosis 5-10• Malaria 1-50• Hepatitis A 1• Hepatitis B 0.5• Yellow fever 0.1-1• Japanese encephalitis 0.01-0.1• Typhoid 0.03• Cholera 0.003
*per 1000 person‐months


Outbreaks of VPD in Haiti following Jan 2010 earthquake
Pathogen Date(s) Location (N) SourceDiphtheria May 2010 Camp Batimat –
Cité Soleil (??)ProMED
Typhoid June 2010 Camp Acra –
Delmas (82)Haiti Operational Biosurveillance Blog
Cholera Oct 2010 –Aug 2011
St. Marc (Artibonite) (439,000) (>6200 deaths)
ProMED; MMWR; MSPP; PAHO

Don’t Forget IPV
Pathogen Date(s) Location (N) Source
Polio type 1 2000-2001 Haiti/DR (21)(AFP = 208)
MMWR 2001;50(39):855-856

• Incidence/Outbreaks of VPD at destination
•Risk behaviours•Vaccine Efficacy•Vaccine-associated
adverse events•Vaccine Cost
Travel Vaccine Considerations

High travel risk** 95% CI
Europeans 8.3% (2000) Americans 8% (2004/5) 18-40 yrs 1.9 0.8-4.9 Male 3.4 1.7-7.0 Single 2.4 1.2-5.0 Travel alone 2.0 1.0-4.2 >20 d duration 4.6 1.7-12.6
Risk Behaviours*
* Zuckerman JN, et al. J Travel Med 2000;7:170-174; Connor BA, et al. J Travel Med 2006;13:273-280** invasive medical intervention, dental, tattoo, body piercing, acupuncture, sex contact
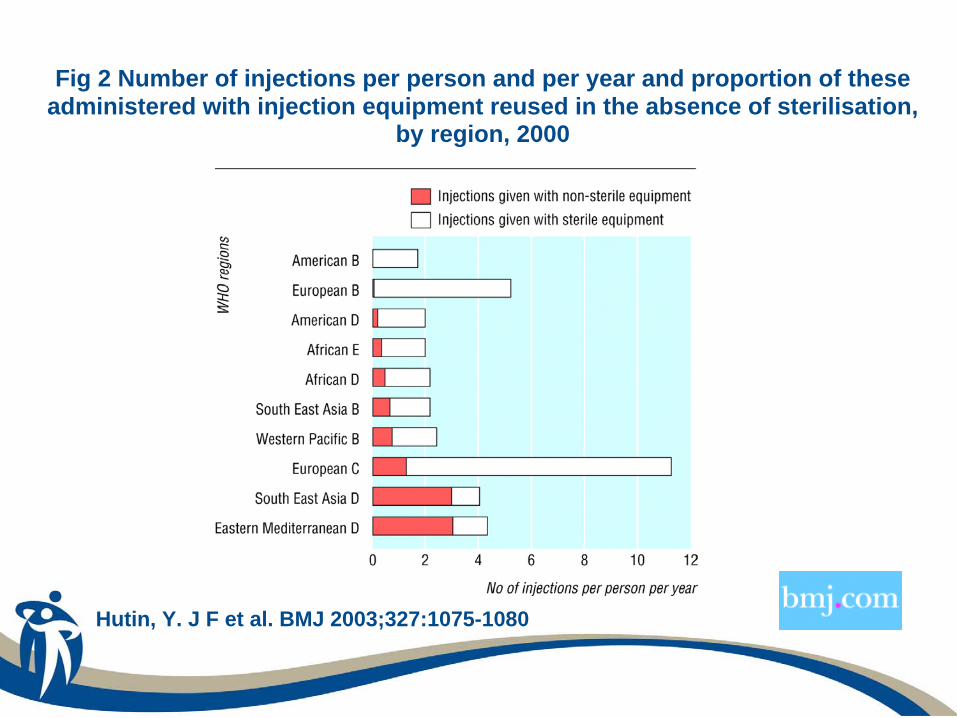
Fig 2 Number of injections per person and per year and proportion of these administered with injection equipment reused in the absence of sterilisation,
by region, 2000
Hutin, Y. J F et al. BMJ 2003;327:1075-1080

Dental Sterilization - Haiti

Hepatitis B Risks vs Benefits
• Exposure risks–sex contacts–unexpected/planned health care (blood
products, nonsterile equipment, acupuncture)–personal services (tattoo, body piercing,
manicures, hair cut/shave)• Potential vaccine benefits
–vaccine efficacy >90% after 3 doses–vaccine adverse events minimal–“catch up”
universal immunization

Don’t Forget HAV•Hepatitis A vaccine
–$120 for vaccine–$70 for admin fees
•HAV/HBV vaccine–$190 for vaccine–$90 for admin fees
• Incremental cost of ~$90

• Incidence/Outbreaks of VPD at destination
•Risk behaviours•Vaccine Efficacy•Vaccine-associated
adverse events•Vaccine Cost
Travel Vaccine Considerations

Oral (Ty21a)
Injectable (Typhim Vi)
Dose 4 capsules 1 IM
Immunity Local IgA Systemic IgG
Efficacy 50%* 55%*
Onset 2 wks 1 wk
Duration 3-4 yrs (vs 5-7 yrs)
2-3 yrs
Typhoid Vaccine Efficacy
*J Trav Med 2009;16:46-52

Vaccine Efficacy –
Cholera (Dukoral™)*
• 62% 1 year after third dose• RRR = 41/20,705 ÷ 110/20,837 = 38%
or PE = 1 - RRR = 62%• ARR = 0.3% or 3/1,000 or NNT = 333• Need to give vaccine to >300 persons
to prevent one case of cholera* 89,596 adults and children >2 yrs in Bangladesh (Clemens JD, et al. JID 1988[Jul];158:60-69)

• Incidence/Outbreaks of VPD at destination
•Risk behaviours•Vaccine Efficacy•Vaccine-associated
adverse events•Vaccine Cost
Travel Vaccine Considerations

• Yf primary vaccine (not booster):–Viscerotropic AE ~ 3/million doses–Viscerotropic AE ~ 20/million doses (if >60 yrs)
• Risk of Yf disease exceeds risk of Yf vaccine for travel to endemic/epidemic countries
• JE primary vaccine:–Delayed systemic allergic reactions ~ 6/100,000 doses–Severe neurologic AE ~ 2/million doses
• Risk of JE disease is less than 1/million for most travel to endemic countries
Vaccine-related Adverse Events – Yf and JE Vaccines

• Incidence/Outbreaks of VPD at destination
•Risk behaviours•Vaccine Efficacy•Vaccine-associated
adverse events•Vaccine Cost
Travel Vaccine Considerations

Vaccine Cost - Rabies Vaccine
• $500-600 for pre-exposure prophylaxis 3 injection IM series
• Alternative “off label” ID 0.1 mL dosing schedule (0,7,21-28 d @ $120+)
• Advantages of ID– Cheaper– Antibody response is very good
• Disadvantages of ID– Not licensed indication in Canada– Follow-up requires time to measure antibodies

Rabies ID Vaccine Seroconversion
• Australian study – “modified” ID –pre- exposure rabies vaccine schedule
• Completed 420 ID rabies vaccine series (2 X 0.1 mL Day 0 & 7; 0.1 mL Day 21-28)
• Of 420 participants:– 397 good immune response (95%) at Day 21-28– 5 non-responders LTF– 18 non-responders (16 responded with ID dose at
Day 21-28; 2 responded after ID booster at Day 35-42)
– Total seroresponders (415 of 415 = 100%)
*J Trav Med 2011;18:327-332
Rabies ID Vaccine Seroconversion
• WRHA Clinic Jan 2009 to June 2011• Completed 75 ID rabies vaccine series• 5 post vaccine serology results not
done (LTF); 8 serology results pending• Of 62 remaining:
– 54 good immune response (87%)– 8 non-responders (3 responded with IM
booster; 1 LTF; 4 declined booster)– Total seroresponders (57 of 57 = 100%)

Algorithm for Travel Immunizations
• Childhood immunizations UTD? (Routine)– If no; TdaP, MMR, varicella, HBV, TIV
• Food/water risk? (Recommended)– If yes; HAV, typhoid
• Humanitarian work? (Recommended)– If yes; cholera, polio
• Long-term/repeated stay? (Recommended)– If yes; JEV, rabies
• Border crossing? (Required)– If yes; Yellow fever, meningococcal
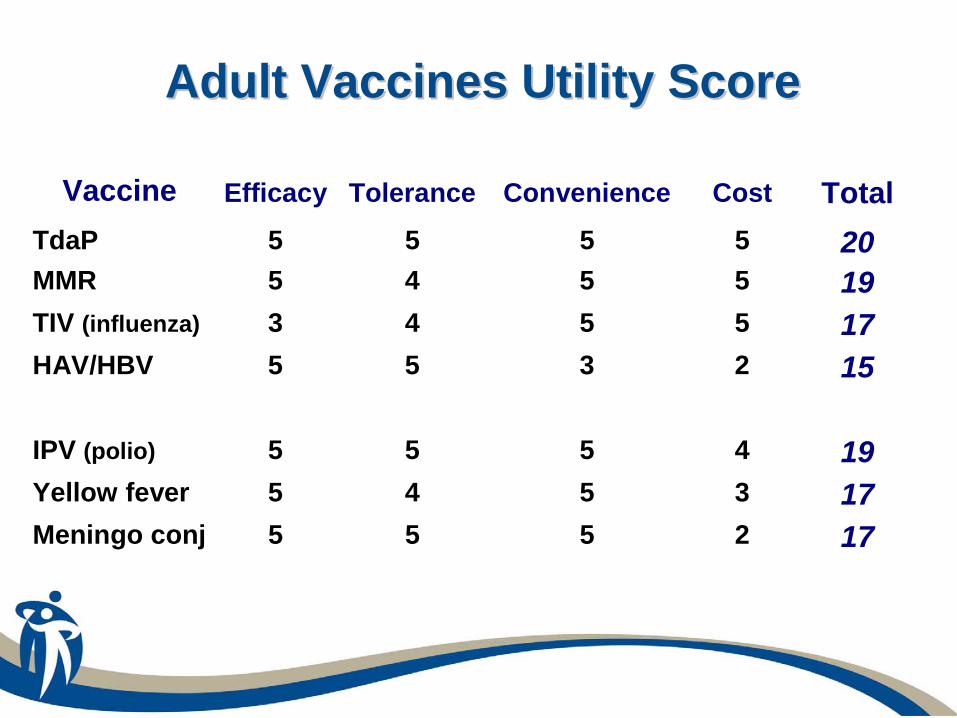
Adult Vaccines Utility ScoreAdult Vaccines Utility Score
Vaccine Efficacy Tolerance Convenience Cost Total TdaP 5 5 5 5 20MMR 5 4 5 5 19TIV (influenza) 3 4 5 5 17HAV/HBV 5 5 3 2 15 IPV (polio) 5 5 5 4 19Yellow fever 5 4 5 3 17Meningo conj 5 5 5 2 17
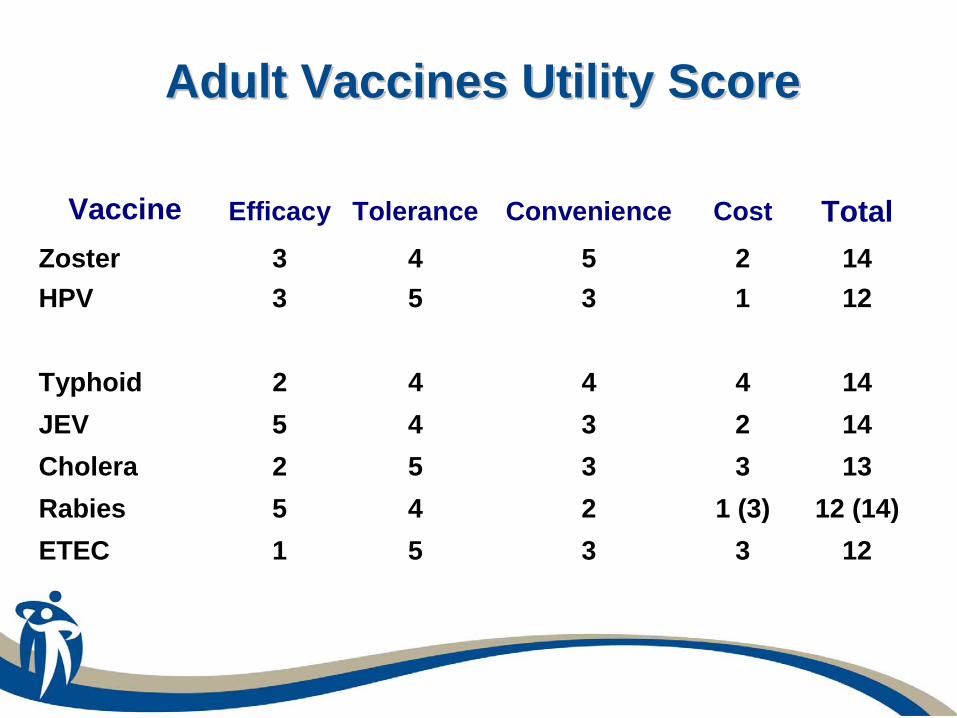
Vaccine Efficacy Tolerance Convenience Cost Total Zoster 3 4 5 2 14HPV 3 5 3 1 12 Typhoid 2 4 4 4 14 JEV 5 4 3 2 14 Cholera 2 5 3 3 13 Rabies 5 4 2 1 (3) 12 (14)ETEC 1 5 3 3 12
Adult Vaccines Utility ScoreAdult Vaccines Utility Score

Infection Control Practices• Routine Practices
• Bring your own supplies•gloves/gowns not routinely required (for
contact with blood/body fluids only)•gloves not a substitute for handwashing•masks not routinely required
(fit tested N-95 primarily for TB)•handwashing is routinely required!

Travel Risk of TB*• Incidence rate of TB infection and disease
• 3.5/1000 person-months of travel (Mantoux conversion)• 0.6/1000 person-months of travel (abnormal CXR)
• Incidence rate by region of travel (/1000 person-mos)
• Africa 4.5; Central America 5.3; South Asia 3.0; Southeast Asia 4.3
• Incidence rate by occupation• health care worker - 7.9/1000 person-months• health care work with TB patients - 9.8/1000 p-mos
*Cobelens FGJ et al, Lancet 2000;356:461-5 and Cobelens FGJ et al, CID 2001;33:300-4
Canadian TB Standards• Post-travel single-step TST testing for
• travel >3 mos to “high risk” setting (200/100,000)
• travel >6 mos to “moderate risk” setting (100-199/100,000)
• travel >12 mos to “lower risk” setting (50-99/100,000)
• travel any duration if HCW, refugee worker, backpacker, chronic medical conditions
• Pre-travel two-step plus post-travel (8 wks) single-step TST only for• HCWs, refugee worker, born/living in TB endemic
area, Hx of TB exposure, Hx of BCG, Hx of liver disease

HIV PEP Starter Kit
*MMWR 2005;54(RR-9):1-17
• Check CIA World Fact Book forestimated population prevalence of HIV
• Canada/Mexico 0.3% (2009)• Haiti 1.9% (2009)• Kenya 6.3% (2009)• Zambia 13.5% (2009)• Thailand 1.3% (2009)
• Basic regimen* (AZT/3-TC - Combivir™ X5 d) – Cost $125
• Expanded regimen* (Combivir™ + lopinavir/ ritonavir - Kaletra® X5 d) – Cost $250
Never, never, never recap a needle!

Infection Control Supplies

Choose your partner carefully
• Short-term should only refer to the time you have available to offer
• Long-term should refer to the impact you and the organization you partner with will have

Education, Medical Aid and Service
www.emascanada.org
To heal, teach and serve, those in need, … by building capacity through partnerships with national groups
Christian Medical and Dental Society
www.cmdscanada.org
Physicians, dentists, and students … who seek to honour God by integrating faith with professional
practice

Medical Teams International
www.medicalteams.org
To demonstrate the love of Christ to people affected by disaster, conflict and poverty around
the world

Mercy Ships Canada
www.mercyships.ca
Deliver medical excellence with integrity and compassion to the world's forgotten poor

Medical Ministry International
www.mmint.org
To meet the need for medical care among the world's poor with lasting solutions through
excellence in medicine, patient care, and health education

Médecins Sans Frontières (Doctors Without Borders)
www.msf.ca
To offer assistance to populations in distress, to victims of natural or man-made disasters and to victims of
armed conflict, without discrimination and irrespective of race, religion, creed or political affiliation
Final Thoughts• Camera (share their suffering first)
• Ethnocentrism (what seems “dumb” to you isn’t to them)
• Judgmentalism (let them see your “log” first)
• Solutions (join with them in problem solving)
• Charity (they need your friendship more than your money and skills)
- Put Away Your:
Final Thoughts• Self (exercise, yoga)
• Emotions (mental health, brief and debrief often)
• Time (reflection, contemplation, meditation)
• Giving (time, talent and treasure, know your limits)
- Take Care of Your:

Responding to Disasters Preparing for humanitarian and disaster relief
work
THANK YOUTHANK YOU