respiration dr. zainab h.h dept. of physiology lec.11,12
TRANSCRIPT
RESPIRATION
Dr. Zainab H.HDept. of Physiology
Lec.11,12
Objectives
List the types of respiratory controls
List the types of chemoreceptors and the main stimulants for each
List the effects of pulmonary receptors on ventilation
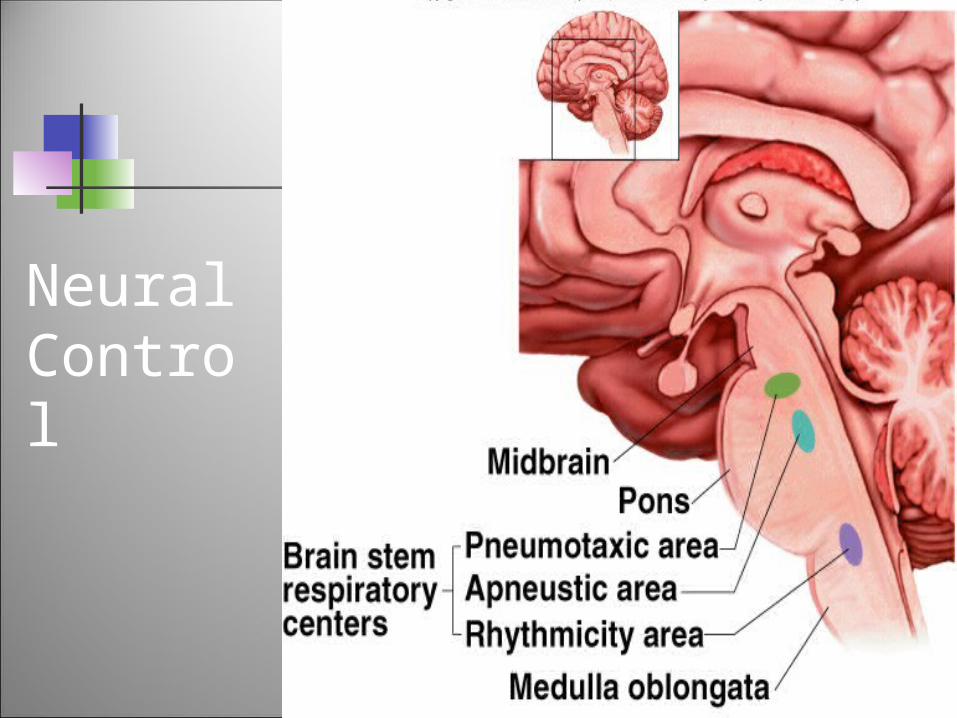
Neural Control
Control of Respiration
The respiratory rate changes:i. When active - respiratory rate goes upii. When less active or sleeping - the rate goes down. The respiratory muscles are voluntary BUT you can't
consciously control them when you're sleeping. So, how is respiratory rate altered & how is
respiration controlled when you're not consciously thinking about respiration? This is by:
A. Neural ControlB. Chemical Control
Two Neurogenic Systems (both CNS)
1) Involuntary (automatic): involve medulla and pons limbic systems (emotional response) hypothalamus (temperature
regulation) other subcortical structures
2) Voluntary: initiated by the cerebral cortex

Two Neurogenic Systems (both CNS)
Notes: Systems are independent Both systems require intact innervation of
respiratory muscles (descending pathways and alpha motorneurons)
The muscles of respiratory ventilation are controlled by somatic motor system and not the autonomic system
The autonomic system controls airway smooth muscle contraction and secretion
Neural Control
Ventilation is matched to the body’s needs for O2 uptake and CO2 removal Medullary respiratory center receives input Appropriate signals sent to motor neurons Rate and depth of ventilation adjusted
Reticular Activating System (RAS)
Located in the reticular system of the brain stem
Activity is associated with the “awake” or conscious state
When active, stimulates respiratory ventilation
When RAS activity is reduced, as during sleep, ventilation is reduced and the PCO2 increases by a few mmHg
Sleep Apnea Ventilation ceases temporarily (10+ seconds)
during sleep. types of sleep apnea
central apnea - reduced CNS respiratory drive
obstructive apnea - increased upper airway resistance (lyryngospasm, bronchospasm, snoring)
In infants - can lead to SIDS (sudden infant Death Syndrome).
Other Neural Structures
Hypothalamus - change in inspiration associated with temperature regulation
Limbic system - respiratory changes in emotion
Cerebral cortex - voluntary control
Chemical Control
This is achieved through the following stimuli:
A. Arterial PO2 level.
B. Arterial PCO2 level.
C. Arterial H+ Concentration. CO2 & [H+] act centrally while the O2 levels
act on the peripheral chemoreceptors.
Chemoreceptors 2 groups of chemo-receptors that monitor
changes in blood PCO2, PO2, and pH. Central:
Highly sensitive to PCO2 and [H+] Located in the medulla oblongata. Functions by stimulating the respiratory centers
Peripheral: Monitors PO2 and arterial H+
Located in the Carotid and aortic bodies. Control breathing indirectly via sensory nerve fibers to
the medulla (X, IX).
Central Chemoreceptors
Their input modifies the rate and depth of breathing to maintain arterial PCO2 of 40 mm Hg.
The primary stimulus is [H+] But [H+] can not cross the Blood Brain
Barrier the blood PCO2 level has more effect as
CO2 readily crosses the BBB.
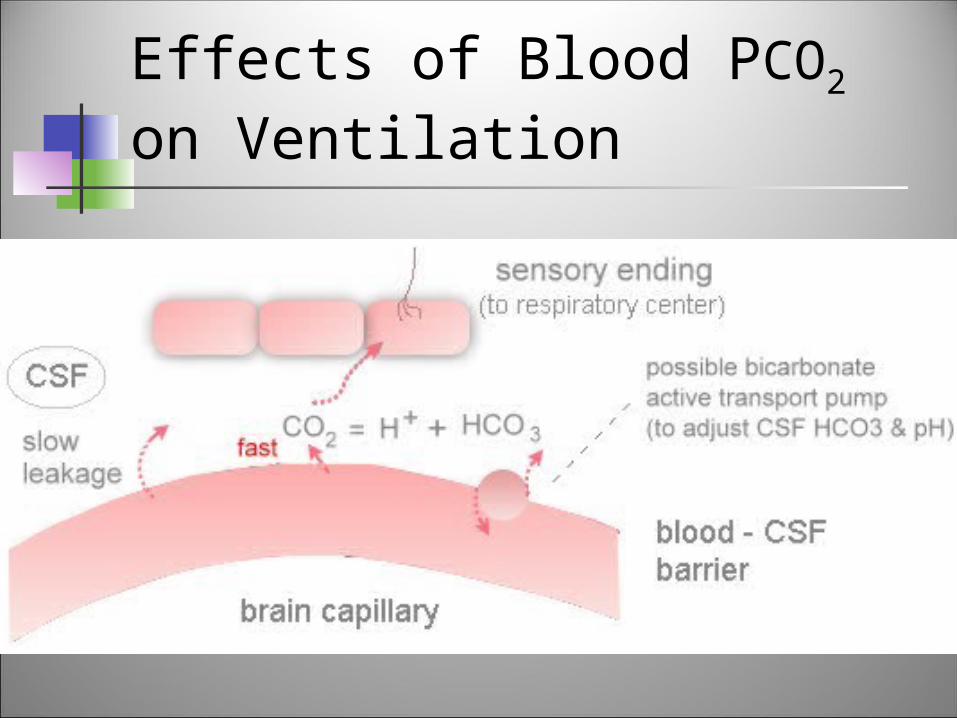
Effects of Blood PCO2 on Ventilation
Is not direct. Even the indirect effect of CO2 is most
potent. Why? Because CO2 easily crosses the BBB. Once it is across the BBB, CO2 + H2O H2CO3 H+ + HCO3
-
These increased H+ ions in the brain stimulate the medullary chemoreceptors.
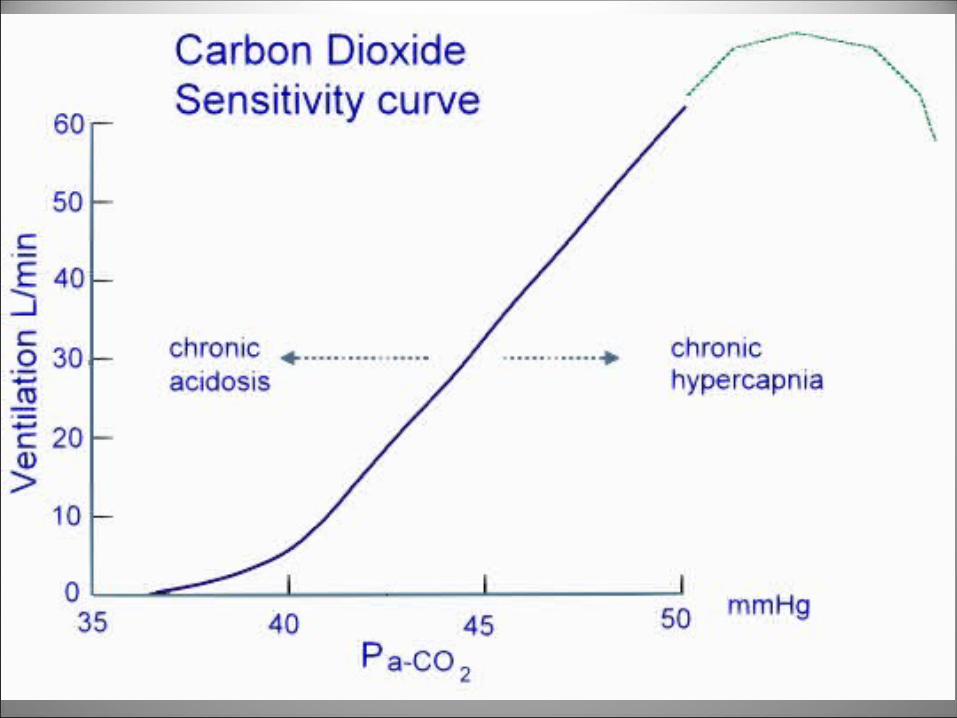
Effects of Blood PCO2 on Ventilation
very large effect sensitive in the normal range of 40
mmHg low PCO2 depresses ventilation very high CO2 is a respiratory
depressant

Effects of Blood PCO2 on Ventilation
The afferent sensory receptors located in the CNS and affected by CSF.
Carotid bodies also have CO2 receptors, but these are less important than the CNS CO2 receptors
The main stimulus is H+ of CSF, which in turn controlled by PCO2 of blood and to a smaller extent, blood pH
Effects of Blood PCO2 on Ventilation
Effects of Blood PCO2 on Ventilation
Physiological Significance homeostatic: maintains PCO2 within the
normal range (38-42 mmHg), thus helps to maintain brain pH
synergistic with O2: hypercapnia increases sensitivity to hypoxemia
Effects of Blood H+ on
Ventilation
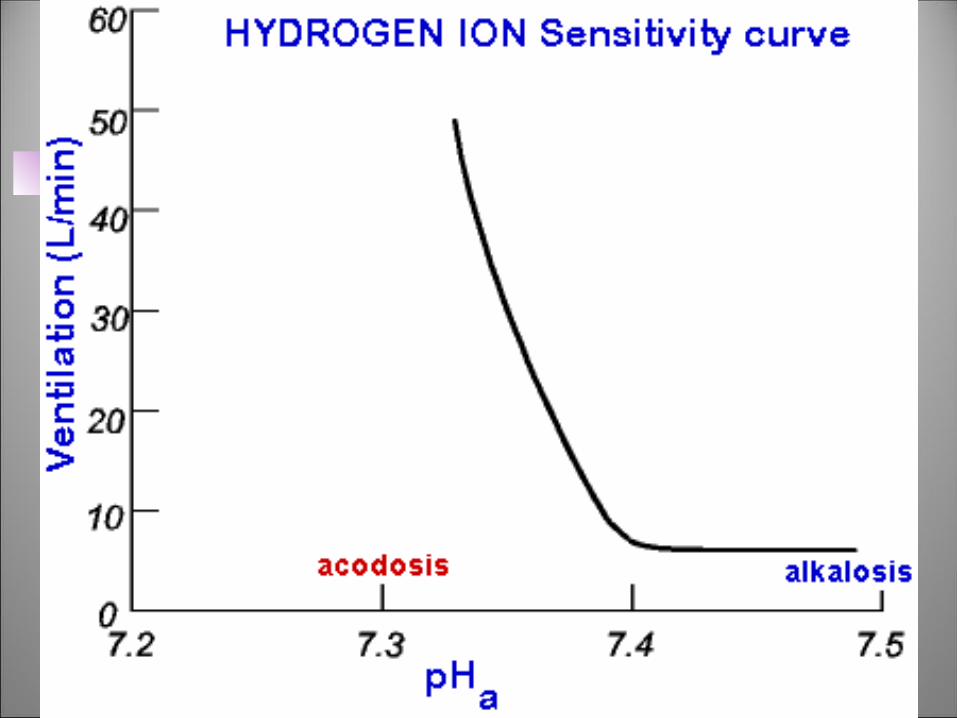
Response as a function of pH especially marked at acidic pH The afferent endings are carotid body and
aortic body H+ sensitive receptors (rapid response)
CNS medullary H+ receptors (slow H+ leakage across the BBB, so slow response
Stimulus is pHa and pH CSF
Quantitative Effect of H+ Ions
The stimulatory effect of H+ ions increases in the first few hours.
It then decreases in the next 1 to 2 days.
It comes down to about 1/5th the initial effect.
This is due to Renal readjustment of [H+] in the circulating blood.
Quantitative Effect of H+ Ions
The kidneys increase blood HCO3-.
This HCO3- binds with the free H+ ions in
the blood & decreases their concentration.
HCO3- also diffuses slowly past the BBB
and decreases the H+ ions in the brain. Therefore the effect of H+ ions is:
Potent: Acutely Weak: Chronically.
Effect of O2
The partial pressure of O2 has no effect on the central (medullary) chemoreceptors.
It only has an effect on the peripheral chemoreceptors.
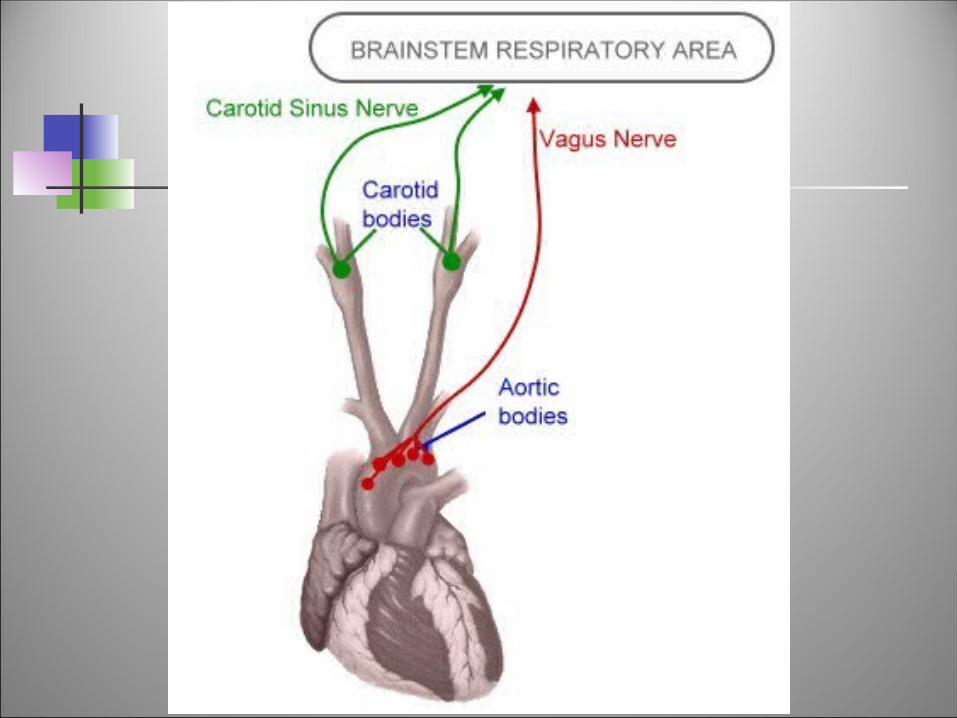
Peripheral Chemoreceptors
There are two pairs of O2 chemoreceptors: Aortic Bodies: located at the arch of aorta. Carotid bodies (mainly): located at the
branching of the common carotid arteries. Their functions are:
To detect changes in the PO2 & H+ To transmit nervous signals to the
Respiratory Centers.
Peripheral Chemoreceptors
These bodies have two types of special cells called glomus cells.
The type 1 glomus cells have special ion channels sensitive to PO2.
They fire the nerve endings and send signals via: Aortic bodies: Vagi. Carotid bodies: Glossopharyngeal
nerve.
Peripheral Chemoreceptors
Both these bodies receive their own special blood supply through minute arteries, directly from the trunk.
Their blood flow is roughly 20 times their own weight.
They are all the time exposed only to arterial blood.
PO2 stimulates these chemoreceptors strongly.
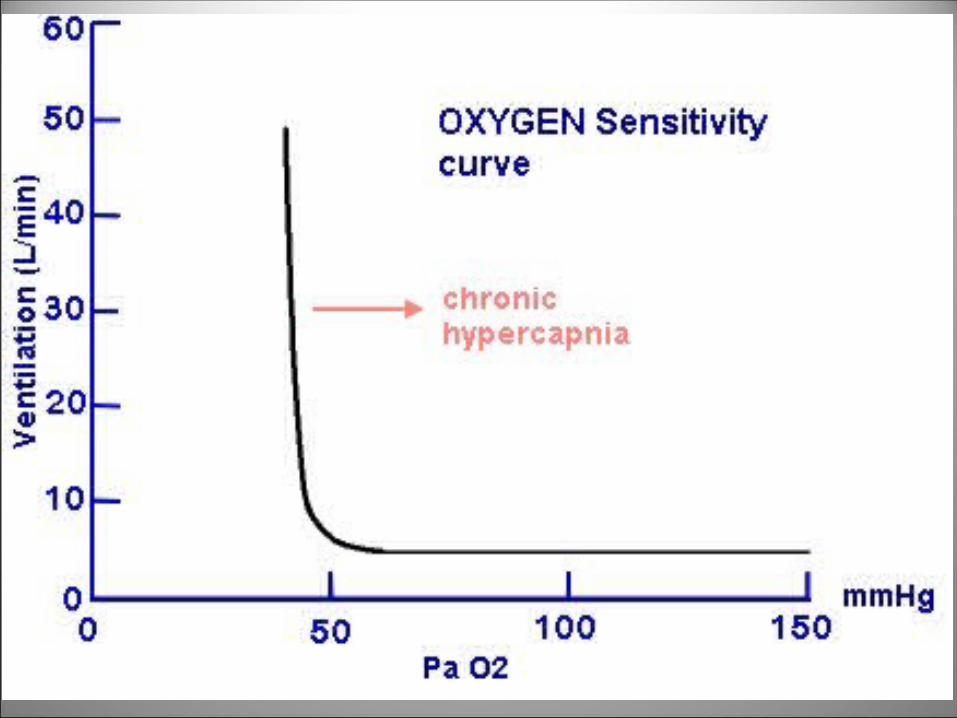
Effects of Blood PO2 on Ventilation
Relatively small effect in the normal range (PO2 > 70 mmHg)
Only important in pronounced hypoxemia (PO2 < 60 mmHg)
High PO2 does not depress ventilation (except for chronic hypercapnia)
Peripheral chemoreceptors respond to the PO2 and not the total O2 content.
Physiological Significance
helps to maintain PO2 in conditions of severe hypoxia (homeostatic)
remain when other chemostimulation is lost synergistic with CO2 response (hypoxia
increases sensitivity to hypercapnia) NOTE: If PO2 is very low, then all CNS
neurons including respiratory neurons, become depressed, so respiratory ventilation is reduced or ceases activity.
Effects of Blood PO2 on Ventilation
Hypoxic drive: Emphysema blunts the chemoreceptor
response to PCO2. Choroid plexus secrete more HCO3
- into CSF, buffering the fall in CSF pH.
Abnormally high PCO2 enhances sensitivity of carotid bodies to fall in PO2.
Effect of CO2 & H+
They also stimulate the peripheral chemoreceptors.
But their effects on the central or medullary chemoreceptors are more powerful.
PCO2 stimulates the peripheral chemoreceptors 5 times as rapidly as it stimulates the central ones.
So this is responsible for the rapid response to CO2 at the onset of exercise.
Effects of Pulmonary Receptors on Ventilation
Lungs contain receptors that influence the brain stem respiratory control centers via sensory fibers in vagus.i. Pulmonary stretch (mechano-)
receptorsii. Lung irritant receptors - airway
receptors responding to inhaled irritating substances; cause hyperpnea and bronchoconstriction
Effects of Pulmonary Receptors on Ventilation
iii. Proprioceptors (Respiratory muscle spindle receptors and joint receptors) may contribute to respiratory drive in exercise.
Along with the chemoreceptors, they send information to the respiratory centers.
Factors Influencing Respiratory Rate and Depth
A. Physical factorsi. Increased body temperatureii. Exerciseiii. Talkingiv. Coughing
B. Volition (conscious control) - emotional factorsC. Chemical factors
i. CO2 levelsii. O2 levels
Chemoreceptors in aorta and carotid arteries
Respiratory Rate Changes Throughout Life
Newborns: 40 to 80 respirations per minute
Infants: 30 respirations per minute
Age 5: 25 respirations per minute
Adults: 12 to 18 respirations per minute
Rate often increases somewhat with old age
A 36-year-old man visits his doctor because his wife has long complained of his snoring, but recently observed that his breathing stops for a couple of minutes at a time while he is sleeping. He undergoes polysomnography and ventilatory response testing to ascertain the extent and cause of his sleep apnea.
The activity of the central chemoreceptors is stimulated by which of the following?
a. A decrease in the metabolic rate of the surrounding brain tissue
b. A decrease in the PO2 of blood flowing through the brain
c. An increase in the PCO2 of blood flowing through the brain
d. An increase in the pH of the CSF e. Hypoxemia, hypercapnia, and metabolic acidosis
Every day it’s the same old thing:
BreatheBreatheBreathe