research article surveillance of food- and smear...
TRANSCRIPT

Research ArticleSurveillance of Food- and Smear-TransmittedPathogens in European Soldiers with Diarrhea onDeployment in the Tropics Experience fromthe European Union Training Mission (EUTM) Mali
Hagen Frickmann12 Philipp Warnke2 Claudia Frey1 Salvatore Schmidt3
Christian Janke3 Kay Erkens3 Ulrich Schotte4 Thomas Koumlller2 Winfried Maaszligen1
Andreas Podbielski2 Alfred Binder4 Rebecca Hinz1 Benjamin Queyriaux5
Dorothea Wiemer1 Norbert Georg Schwarz6 and Ralf Matthias Hagen1
1Department of Tropical Medicine at the Bernhard Nocht Institute German Armed Forces Hospital of Hamburg20359 Hamburg Germany2Institute for Medical Microbiology Virology and Hygiene University Medicine Rostock 18057 Rostock Germany3Sub-Department VI2 Department A Military Medical Command 56070 Koblenz Germany4Department II (Veterinary Medicine) Central Institute of the German Armed Forces Medical Service Kiel-Kronshagen24119 Kiel-Kronshagen Germany5Deployment Health Surveillance CapabilityNATO MilMed COE 80637 Munich Germany6Department of InfectiousDisease Epidemiology BernhardNocht Institute for TropicalMedicineHamburg 20359Hamburg Germany
Correspondence should be addressed to Hagen Frickmann frickmannbnitmde
Received 2 December 2014 Revised 5 June 2015 Accepted 8 June 2015
Academic Editor Pierre Colin
Copyright copy 2015 Hagen Frickmann et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Introduction Since 2013 European soldiers have been deployed on the European Union Training Mission (EUTM) in Mali Fromthe beginning diarrhea has been among the most ldquourgentrdquo concerns Diarrhea surveillance based on deployable real-time PCRequipment was conducted betweenDecember 2013 andAugust 2014Material andMethods In total 53 stool samples were obtainedfrom 51 soldiers with acute diarrhea Multiplex PCR panels comprised enteroinvasive bacteria diarrhea-associated Escherichia coli(EPEC ETEC EAEC and EIEC) enteropathogenic viruses and protozoa Noroviruses were characterized by sequencing Culturalscreening for Enterobacteriaceae with extended-spectrum beta-lactamases (ESBL) with subsequent repetitive sequence-based PCR(rep-PCR) typingwas performed Clinical informationwas assessedResults Positive PCR results for diarrhea-associated pathogenswere detected in 4353 samples comprising EPEC (119899 = 21) ETEC (119899 = 19) EAEC (119899 = 15) Norovirus (119899 = 10) ShigellasppEIEC (119899 = 6) Cryptosporidium parvum (119899 = 3) Giardia duodenalis (119899 = 2) Salmonella spp (119899 = 1) Astrovirus (119899 = 1)Rotavirus (119899 = 1) and Sapovirus (119899 = 1) ESBL-positive Enterobacteriaceae were grown from 13 out of 48 samples Simultaneousinfections with several enteropathogenic agents were observed in 23 instances Symptoms were mild to moderate There werehints of autochthonous transmission Conclusions Multiplex real-time PCR proved to be suitable for diarrhea surveillance ondeployment Etiological attribution is challenging in cases of detection of multiple pathogens
1 IntroductionDiarrhea due to food- and smear-transmitted pathogensremains a scourge of military deployments in tropical set-tings Potential deleterious consequences of this problem
were first described more than 3000 years ago in the OldTestament (Deuteronomy 23 9ndash14) detailing basic hygieneprocedures such as isolation of infected soldiers and eradica-tion of infectiousmaterial in timeswhen therewas no concept
Hindawi Publishing CorporationBioMed Research InternationalVolume 2015 Article ID 573904 15 pageshttpdxdoiorg1011552015573904
2 BioMed Research International
of microbial pathogens Recently described deployment-associated outbreaks of gastrointestinal infections confirmthe relevance of the issue [1 2]
As previously described [3] infections with food- orwaterborne enteric pathogens can be efficiently preventedby elaborate hygiene precautions in military field campson deployment In German field camps these precautionscomprise compliance with European general principles andrequirements of food law European procedures regardingfood safety (Regulation EC number 1782002) and theGerman Food and Feed Law (ldquoLebensmittel- und Futter-mittelgesetzbuchrdquo LFBG) production and delivery of foodand drinking water by German soldiers or under their directsupervision whenever possible implementation of HACCP(hazard analysis and critical control points) systems fromdelivery to disposal including cleaning and disinfectionmeasures in conjunctionwith food production as well as han-dling procedures by operators of dining and water treatmentfacilities and instructions in accordance with the Germaninfection prevention law (ldquoInfektionsschutzgesetzrdquo IfSG) formilitary and civilian staffs of facilities supplying food andwater Military public health officials such as veterinariansor hygiene officers are in charge of all food and drinkingwater control procedures Laboratory surveillance generallyfocused on infectious and noninfectious threats that mightendanger themission is carried out with samples of deliveredand prepared food and treated water prior to release and alsoincludes the screening of local staffs for pathogens accordingto relevant directives from the hygiene department Gener-ally all deployed soldiers are by order forbidden to consumeother than safety-approved food and drinking water from thecountry of deployment Such safety approval requires thatlocal producers are audited and controlled by military foodspecialists
If such high hygiene standards can be maintained infec-tion rates with enteric pathogens are comparably low tothose in Germany as shown for chronic infestations withenteropathogenic protozoa in German soldiers returningfromGermanmilitary field camps in various subtropical andtropical deployment sites [3] If these standards cannot bemaintained for logistic reasons for example during smallor multinational deployments infection rates increase [3]Further in spite of training and education in basic hygienicmeasures that are implemented before deployment soldiersmay tend to noncompliance if the temptation of appealinglocal foods coincides with monotonous food in the fieldcanteen or perhaps delivery problems during the first phasesof deployment A previous study described noncomplianceproblems with antimalarial chemoprophylaxis on deploy-ment [4]
German hygiene standards for military field camps can-not always be maintained during multinational militaryoperations German soldiers have for example participatedin the European Union Training Mission (EUTM) in Malisince March 2013 with the field camp in Koulikoro near thecapital Bamako as the major site of deployment Diarrhea hasbeen among the most ldquourgentrdquo infectious concerns from thebeginning Consequently deployable real-time PCR equip-ment was transferred to Koulikoro to study the molecular
epidemiology of diarrhea in the camp from December 2013until March 2014 Subsequently the surveillance of food- andsmear-transmitted pathogens was continued until August2014 by transferring sample material to Germany Here wedescribe results that were obtained in a 9-month observationperiod
2 Materials and Methods
21 Study Population Between the 49th calendar week inDecember 2013 and the 34th calendar week in August 2014microbiological surveillance was carried out on Europeansoldiers with acute diarrhea deployed in Mali in the courseof the European Union Training Mission (EUTM) Diarrheawas defined as the deposition by the subject of amorphousstools and distinguished according to frequency as lt3 orge3 stools per day Accordingly low-frequency diarrhea wasconsidered as of potential infectiological relevance as wellThe field doctor in charge subjectively decided whether ornot he or she considered the symptoms of the patients tobe relevant and incapacitating enough for an inclusion intothe surveillance All diarrhea patients were asked by the fielddoctor in camp Koulikoro to provide a sample of native stoolfor molecular and cultural diagnostic analysis Investigationsof diseased local military or civilian personnel were not partof the surveillance
In addition to providing the samples the field doctorcollected data on diarrhea patients in a standardized way onthe delivery note that was sent together with the sample Theitems on these notes were as follows age gender nationalitymode of food intake site of deployment stool frequencystool consistency as described by the patient accompa-nying symptoms presence of fever type of antimalarialprophylaxis vaccination status against cholera and typhoidfever medication with antibiotic drugs any previous staysin high-endemicity settings regarding diarrhea (includingAfghanistan Bahrain Bolivia Colombia Kosovo Lebanonand Turkey [3]) and participation in counseling regardinghygiene on tropical deployments prior to the onset of diar-rhea In addition stool consistency of the samples providedwas assessed by the analyzing laboratory technician
While providing stool samples and thus participatingin the surveillance were voluntary all cases of diarrheaamong EUTM personnel that were registered by the fielddoctor were further routinely reported to the DeploymentHealth Surveillance Capability (DHSC) of the North AtlanticTreaty Organization (NATO) Military Medicine Center ofExcellence Again the diagnosis diarrhea was based on thefield doctorrsquos subjective decision whether or not he or sheconsidered the symptoms of the patients to be relevantand incapacitating These data and the number of deployedEUTM forces were used to calculate a weekly incidencerate as a passive surveillance procedure DHSC reports werecompared with the number of patients that were included inthe surveillance to estimate the achieved coverage
22 Laboratory Testing FromDecember 2013 toMarch 2014collected stool samples were analyzed by PCR directly in the
BioMed Research International 3
laboratory of the field hospital in Camp Koulikoro in MaliFrom April until August 2014 the samples were frozen atminus20∘C and shipped to Germany for further investigationAll culture-based diagnostic approaches were performed inGermany
221 Sample Preparation Prior to PCR analysis nucleicacids were extracted from all stool samples using the Qiampstool kit (Qiagen Hamburg Germany) The nucleic acidextraction was performed as described by the manufacturer
222 PCR Testing All samples were analyzed with a panelof real-time multiplex PCRs comprising two in-houseprotocols One of those in-house PCR tests targets theinvasive enteropathogenic bacteria Salmonella spp Shigellasppenteroinvasive Escherichia coli (EIEC) Campylobacterjejuni andYersinia spp [5 6]The diagnostic reliability of thisprocedure has been shown previously in comparison withcultural approaches [5] The other in-house PCR which isused for routine diagnostic analyses by the German NationalReferenceCentre for Tropical Diseases BernhardNocht Insti-tute Hamburg amplifies DNA of the enteropathogenic pro-tozoa Entamoeba histolytica Giardia duodenalis Cyclosporacayetanensis and Cryptosporidium parvum [3 6 7] Thepreviously described primer-probe-sets for Entamoeba his-tolytica Giardia duodenalis and Cryptosporidium parvumwere complemented by a primer-probe-set for Cyclosporacayetanensis that was adapted froma previous publication [7]No further changes to the described protocols [3 5 6 8] wereapplied The primer-probe-sets used are detailed in Table 1
In addition to the in-house multiplex real-time PCRassays described above three commercial RidaGene (R-Bio-pharm Darmstadt Germany) PCR kits ldquoEAECrdquo ldquoEHEC-EPECrdquo and ldquoETEC-EIECrdquo were applied targeting enteroag-gregative E coli (EAEC) enterohemorrhagic E coli (EHEC)enteropathogenic E coli (EPEC) enterotoxic E coli (ETEC)and Shigella sppEIEC Finally analyses using the commer-cial Fast-track Diagnostics (Sliema Malta) PCR kit ldquoviralgastroenteritisrdquo targeting Norovirus genogroups I (G1) and II(G2) Astrovirus Rotavirus Adenovirus and Sapovirus wereadded
Phocid herpesvirus DNA was chosen as the target forinhibition control PCR The procedure was performed asdescribed previously [8ndash10] The primer-probe-set is pre-sented in Table 1
223 Norovirus Sequencing Samples testing positive byNorovirus genogroup I (GI) or II (GII) PCR were subjectedto further sequence analysis In detail a 213-base-pair (bp)part of the open reading frame 1 (ORF1) was amplified usingdegenerate multiplex primers MON432MON434 (GI) andMON431MON433 (GII) as described [11] Amplified DNAwas sent for sequencing (Seqlab Gottingen Germany) afternucleic acid gel extraction and cleanup with a QIAquickGel Extraction Kit (QIAGEN Hilden Germany) Sequenceassembly and analysis were performed with the softwareDNAStar Lasergene 121 genomics suite (DNASTAR IncMadisonWI USA) Subsequent genotyping was based uponthe Norovirus genotyping tool as described [12]
224 Cultural Growth Identification and Resistance TestingIf sufficient stool material was available cherry-pit-sized vol-umes were used for broth enrichment in thioglycolate broth(Heipha Eppelheim Germany) This was the case for a totalof 48 out of 53 samples Incubation was performed for 16ndash24hours at 37∘C Broth enrichment increases the yield of ESBL-expressing bacteria after swabbing for example by a factorof 2 in upper respiratory tract samples [13] Subsequently10 120583L preincubated broth was cultured on Brilliance ESBLselective agar (Oxoid Basingstoke UK) This agar is madefor selective growth of ESBL-positive EnterobacteriaceaeSensitivity of 949ndash979 and specificity of 957ndash100 havebeen described for Brilliance ESBL selective agar [14 15]Agar plates were incubated at 37∘C for 40ndash48 hours Allcolonies that looked suspicious for Enterobacteriaceae (bluegreen and brown colonies) were isolated while suspectedGram-negative nonfermentative rod-shaped bacteria (ieyellow or yellowish-brown or greenish-brown colonies) werediscarded All isolates were frozen at minus80∘C in Microbanktubes (Pro-LabDiagnostics Bromborough UK) until furtherassessment
Identification was performed by VITEK-II GN-cards(bioMerieux Marcy-lrsquoEtoile France) and matrix-assistedlaser-desorption-ionization time-of-flight mass spectrome-try (MALDI-TOF-MS) using a ShimadzuKratos ldquoAXIMAAssurancerdquo MALDI-TOF mass spectrometer (ShimadzuGermany Ltd Duisburg Germany) [16] For MALDI-TOFanalyses isolates were prepared using alpha-cyano-4-hydroxycinnamic acid (bioMerieux) as matrix Spectralfingerprints were analyzed using Vitek MS IVD V2 databaseMS-CE versionCLI 200 (bioMerieux) Automated antibioticsusceptibility testing was performed with VITEK-II AST-N263-cards (bioMerieux) In case of uncertain resultsE-testing (bioMerieux) was added Interpretation of resist-ance testing results was based on the EUCAST guideline(version 40 2014 httpwwweucastorgfileadminsrcme-diaPDFsEUCAST filesBreakpoint tablesBreakpoint tab-le v 40pdf)
225 Rep-PCR Typing of Extended-Spectrum Beta-LactamasePositive E coli All confirmed ESBL-positive E coli strainsfromESBL selective agar were grown overnight in brain heartinfusion broth DNA was extracted using the MoBio Ultr-aClean Microbial DNA Isolation Kit (Mo Bio LaboratoriesInc Carlsbad CA USA) Purified DNA samples were ampli-fied using the DiversiLab Escherichia DNA fingerprinting kit(reference number 410 980 bioMerieux) on a T-personalthermal cycler (Biometra Gottingen Germany) Rep-PCRproducts were detected by chip-based DNA separation onanAgilent 2100 Bioanalyzer (Agilent Technologies Inc SantaClara CA USA) All techniques were executed according tothe manufacturersrsquo instructions
Documentation and band-pattern analysis were per-formed using the DiversiLab software version 33 (bioMeri-eux) A correlation cutoff of 95 for confirmation or exclu-sion of clonal identity of analyzed strains was applied asrecommended by the manufacturer All library entries wereanalyzed in duplicate
4 BioMed Research International
Table1Sequ
enceso
fthe
prim
er-probe-setsu
sedin
thea
ppliedreal-timeP
CRassays
[5ndash9
]
Targetorganism
Forw
ardprim
erRe
versep
rimer
TaqM
anprob
eMultip
lex-PC
Rtargetinginvasiv
eentericbacteria
Salm
onellaspp
51015840-ATT
-GTT
-GAT
-TCA
-GGT-AC
A-AAC
-31015840
51015840-AAT
-TAG
-CCA
-TGT-TG
T-AAT
-CTC
-31015840
51015840-C
AA-
GTT
-CAA-
CGC-
GCA
-ATT
-TA-
31015840ShigellasppEIEC
51015840-C
AG-AAG
-AGC-AG
A-AG
T-AT
G-AG-31015840
51015840-C
AG-TAC
-CTC
-GTC
-AGT-CA
G-31015840
51015840-ACA
-GGT-GAT
-GCG
-TGA-
GAC
-TG-31015840
Campylobacterjejun
i51015840-C
TA-TAA-
CAA-
CTG-C
AC-C
TA-C
TA-AT-31015840
51015840-AAG
-TGT-AAG
-CAC
-ACA
-AGG-TA-
3101584051015840-C
TT-AAT
-AGC-
CGT-CA
C-CC
C-AC
-31015840
Yersiniaspp
51015840-G
CA-TTA
-ACG
-AAT
-ATG
-TTA
-GC-
3101584051015840-ATC
-GAG
-TTT
-GGA-
GTA
-TTC
-AT-31015840
51015840-C
CG-C
TT-C
CA-AAT
-TTT
-GTC
-AT-31015840
Multip
lex-PC
Rtargetingenteric
protozoa
Entamoeba
histo
lytica
51015840-ATT
-GTC
-GTG
-GCA
-TCC
-TAA-
CTC-A-
3101584051015840-G
CG-G
AC-G
GC-TC
A-TT
A-TA
A-CA
-31015840
51015840-TCA
-TTG
-AAT
-GAA-TT
G-G
CC-ATT
-T-31015840
Giardiadu
odenalis
51015840-G
AC-G
GC-TC
A-GGA-
CAA-
CGG-TT-31015840
51015840-TTG
-CCA
-GCG
-GTG
-TCC
-G-31015840
51015840-C
CC-G
CG-G
CG-G
TC-C
CT-G
CT-AG-31015840
Cyclo
spora
cayetanensis
51015840-TAG
-TAA-
CCG-AAC
-GGA-TC
G-C
AT-T-31015840
51015840-AAT
-GCC
-ACG
-GTA
-GGC-
CAA-TA
-31015840
51015840-C
CG-G
CG-ATA
-GAT
-CAT
-TCA
-AGT-TT
C-TG
A-CC
-31015840
Cryptosporidium
parvum
51015840-C
GC-TT
C-TC
T-AG
C-CT
T-TC
A-TG
A-31015840
51015840-C
TT-C
AC-G
TG-TGT-TT
G-C
CA-AT-31015840
51015840-C
CA-ATC
-ACA
-GAA-TC
A-TC
A-GAA-TC
G-ACT
-GGT-AT
C-31015840
InternalcontrolP
CRtargetingph
ocid
herpesvirusD
NA
Phocid
herpes
virus
51015840-G
GG-C
GA-AT
C-AC
A-GAT
-TGA-AT
C-31015840
51015840-G
CG-G
TT-C
CA-AAC
-GTA
-CCA
-A-31015840
51015840-TTT
-TTA
-TGT-GTC
-CGC-
CAC-
CAT-CT
G-G
ATC-
31015840
BioMed Research International 5
Table 2 Median and mean cycle threshold (Ct) values of pathogens that were detected by PCR
Detected pathogen Median Ct-value Mean Ct-value Standard deviationSalmonella spp 27 27 mdashShigella sppEIEC1 175 18 30Shigella sppEIEC2 135 147 27Shigella sppEIEC3 125 137 24EPEC 22 214 40STEC4 14 159 39STEC5 19 182 43EAEC 19 192 35Giardia duodenalis 255 255 35Cryptosporidium parvum 27 277 60Norovirus G1 20 243 84Norovirus G2 17 166 43Astrovirus 30 30 mdashRotavirus 22 22 mdashSapovirus 32 32 mdash1As detected by in-house PCR 2As detected by RidaGene PCR targeting EHECEPECShigella sppEIEC 3As detected by RidaGene PCR targeting ETEC andShigella sppEIEC 4As detected by PCR targeting the stable toxin 5As detected by PCR targeting the labile toxin
23 Ethics The surveillance described here was ordered asa preventive medical procedure by the German command-ing hygiene officer of the EUTM Mali mission Respectiveorders are legally covered by the self-administrative rightsldquoEigenvollzugskompetenzrdquo of the German Armed ForcesMedical Service regarding infectious disease prevention andcontrol ldquoInfektionsschutzrdquo Collected data were assessedanonymously thus avoiding any violation of sect25 of theDeclaration of Helsinki (DoHOct 2008) or national dataprotection laws ldquoBundesdatenschutzgesetzrdquo
3 Results
31 Frequency of Diarrhea and Coverage Based on thereports of the field doctors to the NATO Deployment HealthSurveillance Capability (DHSC) an average weekly incidenceof diarrhea among EUTM soldiers of 58 patients per weekwas calculated The average number of deployed soldiers atrisk was 480 the resulting average weekly incidence rate per1000 soldiers was 121 During the surveillance period of 37weeks a total of 53 stool samples from 51 EUTM soldiers withdiarrheawere collected resulting in an average of 14 cases perweek Accordingly the coverage of the surveillance was about241 of the registered diarrhea cases
32 Diagnostic Results Positive PCR results for diarrhea-associated pathogens could be detected in 4353 patientsamples The five quantitatively dominating pathogenswere EPEC (119899 = 21) ETEC (119899 = 19) EAEC (119899 = 15)Norovirus (119899 = 10) and ShigellaEIEC (119899 = 6) followed byCryptosporidium parvum (119899 = 3)Giardia duodenalis (119899 = 2)Salmonella spp (119899 = 1) Astrovirus (119899 = 1) Rotavirus(119899 = 1) and Sapovirus (119899 = 1) Of note both detections ofGiardia duodenalis were in the same patient so copy-strainassessment occurred here Median and mean cycle threshold
(Ct) values as well as calculated standard deviations (SD)are given in Table 2 Of note the lowest Ct values weredetected for bacteria Ct-values for Shigella sppEIEC variedconsiderably depending on the primer-probe compositionused with lowest Ct-values in the RidaGene ETECEIEC kitand highest in the in-house approach
DNA of two and more pathogens was detected in 23 ofthe samples of three and more pathogens in 11 samples offour and more pathogens in 2 samples and of as many as fivepathogens in 1 sample Measured Ct values for the respectivecases are given in Table 3 In several cases low Ct-values aremeasured for more than one pathogen
33 Norovirus Genotyping Sequence analysis and genotyp-ing verified the detection of Norovirus GII in six out ofseven initially PCR-positive cases The procedure failed forthe seventh Norovirus GII detection and for all three casespositive for Norovirus GI At least two out of three NorovirusGI-positive cases were confirmed by a separate real-time RT-PCR [17 18] (data not shown)
Genotyping of the six sequenced Norovirus G2 strainsrevealed GIIP7 in four instances Three out of those fourstrains showed identical sequences suggesting either noso-comial transmission or a common source of infection Epi-demiological assessment showed that the respective sampleswere collected from three patients within a single weekmaking a mini-outbreak highly likely In two out of sixinstances Norovirus GIIP16 and GIIP4 var New Orleanswere identified respectively
The underlying sequence information has been depositedand is freely accessible via httpwwwrivmnlmpfnoro-virustypingtooljob1197792283
34 Cultural Approach From 13 out of the 48 analyzed stoolsamples ESBL-positive Enterobacteriaceae were isolated by
6 BioMed Research International
Table 3 Ct-values in cases of multiple pathogen detections (in brackets) If both stable and labile toxin of STEC were detected two Ct-valuesare given otherwise only one In case of Shigella sppEIEC detections three Ct-values are shown reflecting the three applied PCR approachesIn several cases low Ct-values are measured for more than one pathogen
Case Pathogen 1 Pathogen 2 Pathogen 3 Pathogen 4 Pathogen 5
1 Shigella sppEIEC (Ct13 14 16) EPEC (Ct 18) ETEC (Ct 13 16) EAEC (Ct 19) Norovirus G1 (Ct 20)
2 Salmonella spp (Ct 27) EPEC (Ct 15) Norovirus G2 (Ct 11) Astrovirus (Ct 30) mdash
3 EPEC (Ct 29) EAEC (Ct 19) Norovirus G2 (Ct 17) mdash mdash
4 ETEC (Ct 17 20) EAEC (Ct 19) Norovirus G2 (Ct 14) mdash mdash
5 ETEC (Ct 13 20) EAEC (Ct 18) Norovirus G2 (Ct 21) mdash mdash
6 Shigella sppEIEC (Ct12 13 14) EPEC (Ct 21) ETEC (Ct 21) mdash mdash
7 EPEC (Ct 17) ETEC (Ct 20) EAEC (Ct 19) mdash mdash
8 EPEC (Ct 20) ETEC (Ct 13) EAEC (Ct 21) mdash mdash
9 EPEC (Ct 16) ETEC (Ct 13) EAEC (Ct 22) mdash mdash
10 ETEC (Ct 15) EAEC (Ct 15) Cryptosporidiumparvum (Ct 34) mdash mdash
11 EPEC (Ct 23) ETEC (Ct 16 21) EAEC (Ct 22) mdash mdash
12 Shigella sppEIEC (Ct18 20 21) EPEC (Ct 26) mdash mdash mdash
13 EPEC (Ct 28) Giardia duodenalis(Ct 28) mdash mdash mdash
14 EPEC (Ct 21) ETEC (Ct 17) mdash mdash mdash
15 EPEC (Ct 25) ETEC (Ct 12) mdash mdash mdash
16 EPEC (Ct 22) Norovirus G2 (Ct 17) mdash mdash mdash
17 ETEC (Ct 11 18) EAEC (Ct 14) mdash mdash mdash
18 ETEC (Ct 15) EAEC (Ct 23) mdash mdash mdash
19 EAEC (Ct 18) Cryptosporidiumparvum (Ct 22) mdash mdash mdash
20 EPEC (Ct 22) Sapovirus (Ct 32) mdash mdash mdash
21 Shigella sppEIEC (Ct12 23 18) EPEC (Ct 19) mdash mdash mdash
22 EPEC (Ct 22) ETEC (Ct 19 19) mdash mdash mdash
23 EPEC (Ct 21) ETEC (Ct 24 29) mdash mdash mdash
thioglycolate broth enrichment with subsequent growthon ESBL selective agar From 12 samples ESBL-positiveEscherichia coli were isolated with proof of more than onestrain in two instances The total number of ESBL-positive Ecoli strainswas 15One of those strainswas identified as EAECby RidaGene PCR An ESBL-positive Klebsiella pneumoniaestrain was isolated from another sample
For the 13 samples containing ESBL-positive Enterobac-teriaceae sensitivity against nonpenicillin noncephalosporinantibiotics was determined by VITEK-II- and E-test-basedresistance testing If several ESBL-positive E coli weresimultaneously isolated the most resistant strain with theresulting highest risk of selection under antibiotic pressurewas chosen Sensitivity for carbapenems tigecycline and
fosfomycin was shown in all 13 cases in 12 for nitrofurantoinwhich is only suitable for urinary tract infections in 11for fluoroquinolones and in 10 for gentamicin Resistanceagainst trimethoprimsulfamethoxazole which is frequentlyencountered in tropical settings was demonstrated in all 13cases
35 Rep-PCR of ESBL-Positive Enterobacteriaceae In total15 E coli strains from 12 patients were subjected to rep-PCR-based DiversiLab typing Within the 95 cutoff rangefor clonal identity three clonal clusters comprising 7 strainsfrom 6 patients were observed (Figure 1) This suggests thepresence of common sources of infection or nosocomial
BioMed Research International 7
10
5
11
4ndash2
3
6ndash1
2
1
12
13
8
4ndash3
7
4ndash1
6ndash2
Similarity ()
Dendrogram Strain Band pattern
10090 958580757065
Figure 1 Dendrogram of the DiversiLab typing results of 15 ESBL-positive E coli strains from 12 patients The strainsrsquo labeling consistsof the patient number (number before the ldquondashrdquo) and the strainnumber in case ofmore than one isolated ESBL-positive E coli strainper patient (number following the ldquondashrdquo) The strain of patient 9 ismissing as the respective ESBL-positive isolate was not E coli butK pneumoniae Three clusters of clonal identity beyond the 95-similarity cutoff (dotted red line) are detectable
transmission within the camp One patient was even colo-nized by E coli strains from two different clusters (Figure 1)For the remaining 8 strains from 6 patients clonal identitywas excluded
36 Clinical and Epidemiological Assessment Clinical datawere provided for 49 patients The completeness of clinicaldata varied missing data are characterized as ldquono datardquo in thetables in the following In those 49 diarrhea patients bacterialpathogens were detected in 34 instances viral pathogens in 12instances and parasitic pathogens in 3 instances No entericpathogen was detectable in 9 out of these 49 patients with theapplied procedures DNA of more than one enteric pathogenwas detectable in 23 of the soldiers with acute diarrhea
361 Age Gender Nationality Sites of Deployment andPrevious Stays in High-Endemicity Regions for Diarrhea-Associated Pathogens No particular distribution pattern ofbacterial viral and parasitic enteric pathogens was observedwith respect to gender and nationality of the soldiers withdiarrhea Soldiers who were younger than 30 years of age
showed coinfections with multiple enteric pathogens lessfrequently than older soldiers Of note all assessed diarrheapatients who were deployed to Bapho were infected by viralpathogens Previous stays in high-endemicity settings did nothave any notable effects on the acquisition of bacterial viraland parasitic pathogens (Table 4)
362 Mode of Food Intake As few as 2 out of 15 diarrheapatients who claimed to have eaten exclusively in the fieldkitchen were free of enteric pathogens in the PCR analysesBacterial pathogens dominated in this group Soldiers whorestricted their diet to hotel food were prone to both bacterialand viral enteric infections There was not a single diarrheapatient in this assessment who had eaten field rations aloneprior to the onset of diarrhea (Table 5)
363 Stool Frequency andConsistency A small proportion of11 patients showed less severe symptomswith fewer than threeunformed stools per day Of note no enteric pathogens weredetected in only one of these patients There was no obviousdistribution pattern of bacterial viral or parasitic pathogensin these less severe diarrhea cases
The observed stool consistency of collected samples asreported by the laboratory technician was considerably lessunformed than the reported stool consistency A total of 13out of 49 stool samples were already hard at the time ofsample collection suggesting that the symptoms had alreadyimproved In contrast no patient reported formed stools tothe field doctor Only 3 out of these 13 formed stools werewithout detectable pathogen DNA at the time of assessment(Table 6)
364 Accompanying Symptoms including Fever Light tomoderate symptoms including nausea and vomiting crampsabdominal pain and flatulence were frequent in the assesseddiarrhea patients Cramps abdominal pain and flatulencewere particularly often detectable in diarrhea patients withbacterial infections while nausea and vomiting were equallylikely for both bacterial and viral infections Only oneinstance of bloody diarrhea was observed in a patient withShigella sppEIEC as the only detectable pathogen in stoolFever was confirmed in only three instances without anydetectable association with a particular pathogen group(Table 7)
Of note the distribution of accompanying symptoms didnot change considerably if only the 34 patients who reportedge3 stools per day were included into the assessment (Table 7)
Only one enteric pathogen per patient was detected in 16patients who reported accompanying symptoms comprising4 cases with STEC 2 cases with EAEC 2 cases with EPEC 2cases with Norovirus G1 2 cases with Norovirus G2 2 caseswith Shigella sppEIEC 1 case withCryptosporidium parvumand 1 case with Rotavirus respectively Bacterial infectionswere associated with a broad distribution of symptoms(Table 7) As expected patients infected with enteroinvasiveShigella sppEIEC showed a particularly wide spectrumof symptoms Norovirus infections and Cryptosporidiumparvum infections were associated with nausea vomiting
8 BioMed Research International
Table 4 Age gender nationality sites of deployment and previous stays in high-endemicity regions for diarrhea-associated pathogens ofdiarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Agelt30 years 1015 615 015 215 51530ndash50 years 1015 315 115 315 815gt50 years 22 12 02 02 22No data 1217 217 217 417 717
GenderMale 3144 1144 344 744 2044Female 35 15 05 25 25
NationalityAustria 11 11 01 01 11Belgium 79 29 19 19 39Colombia 11 01 01 01 01Germany 1725 825 025 425 1225Greece 33 03 13 03 33Ireland 01 01 01 11 01Italy 01 01 01 11 01Portugal 01 01 01 11 01Romania 01 11 01 01 01Spain 44 04 04 04 24SpainBolivia 01 01 01 11 01No data 11 01 11 01 11
Site of deploymentKoulikoro 3141 741 341 641 1941Koulikoro and Bamako 12 12 02 12 12Bamako 01 01 01 11 01Bapho 24 44 04 04 24No data 01 01 01 11 01
Previous stays in high endemicitysettings
Yes 813 313 113 213 413No 2636 936 236 736 1836
and abdominal pain and Norovirus G1 infections also wereassociated with cramps and flatulence (Table 7)
365 Antimalarial Prophylaxis Hygiene Counseling Vacci-nation against Cholera and Typhoid Fever and MedicationLow-dose doxycycline-monohydrate antimalarial prophy-laxis at 100mgday did not provide any protection againstbacterial enteric infections Among the diarrhea patientsunder doxycycline prophylaxis 7 out of 10 were positive forDNA of bacterial enteric pathogens
The vast majority of diarrhea patients were properlycounseled regarding hygiene on tropical deployments andwere vaccinated against typhoid fever Infections with bacte-rial enteric pathogens were particularly frequent in patientswho were vaccinated against cholera and typhoid fever Useof anti-infective drugs was documented for three patients
all three took rifaximin and one in addition metronidazoleDNA of bacterial enteric pathogens was detectable in onlyone of these patients no pathogen DNA was observed in twoof them (Table 8)
4 Discussion
Risk assessment by standardized monitoring and surveil-lance of deployed soldiers in subtropical or tropical coun-tries contributes to evaluation of both individual risk andpreventive measures As previously shown infection riskswith enteric pathogens increase if sophisticated hygieneprecautions regarding food and drinking water cannot bemaintained on military deployments for example in thecase of small missions [3] Considering an average clinicalincidence of diarrhea between 5 and 7 per 100 per month
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

2 BioMed Research International
of microbial pathogens Recently described deployment-associated outbreaks of gastrointestinal infections confirmthe relevance of the issue [1 2]
As previously described [3] infections with food- orwaterborne enteric pathogens can be efficiently preventedby elaborate hygiene precautions in military field campson deployment In German field camps these precautionscomprise compliance with European general principles andrequirements of food law European procedures regardingfood safety (Regulation EC number 1782002) and theGerman Food and Feed Law (ldquoLebensmittel- und Futter-mittelgesetzbuchrdquo LFBG) production and delivery of foodand drinking water by German soldiers or under their directsupervision whenever possible implementation of HACCP(hazard analysis and critical control points) systems fromdelivery to disposal including cleaning and disinfectionmeasures in conjunctionwith food production as well as han-dling procedures by operators of dining and water treatmentfacilities and instructions in accordance with the Germaninfection prevention law (ldquoInfektionsschutzgesetzrdquo IfSG) formilitary and civilian staffs of facilities supplying food andwater Military public health officials such as veterinariansor hygiene officers are in charge of all food and drinkingwater control procedures Laboratory surveillance generallyfocused on infectious and noninfectious threats that mightendanger themission is carried out with samples of deliveredand prepared food and treated water prior to release and alsoincludes the screening of local staffs for pathogens accordingto relevant directives from the hygiene department Gener-ally all deployed soldiers are by order forbidden to consumeother than safety-approved food and drinking water from thecountry of deployment Such safety approval requires thatlocal producers are audited and controlled by military foodspecialists
If such high hygiene standards can be maintained infec-tion rates with enteric pathogens are comparably low tothose in Germany as shown for chronic infestations withenteropathogenic protozoa in German soldiers returningfromGermanmilitary field camps in various subtropical andtropical deployment sites [3] If these standards cannot bemaintained for logistic reasons for example during smallor multinational deployments infection rates increase [3]Further in spite of training and education in basic hygienicmeasures that are implemented before deployment soldiersmay tend to noncompliance if the temptation of appealinglocal foods coincides with monotonous food in the fieldcanteen or perhaps delivery problems during the first phasesof deployment A previous study described noncomplianceproblems with antimalarial chemoprophylaxis on deploy-ment [4]
German hygiene standards for military field camps can-not always be maintained during multinational militaryoperations German soldiers have for example participatedin the European Union Training Mission (EUTM) in Malisince March 2013 with the field camp in Koulikoro near thecapital Bamako as the major site of deployment Diarrhea hasbeen among the most ldquourgentrdquo infectious concerns from thebeginning Consequently deployable real-time PCR equip-ment was transferred to Koulikoro to study the molecular
epidemiology of diarrhea in the camp from December 2013until March 2014 Subsequently the surveillance of food- andsmear-transmitted pathogens was continued until August2014 by transferring sample material to Germany Here wedescribe results that were obtained in a 9-month observationperiod
2 Materials and Methods
21 Study Population Between the 49th calendar week inDecember 2013 and the 34th calendar week in August 2014microbiological surveillance was carried out on Europeansoldiers with acute diarrhea deployed in Mali in the courseof the European Union Training Mission (EUTM) Diarrheawas defined as the deposition by the subject of amorphousstools and distinguished according to frequency as lt3 orge3 stools per day Accordingly low-frequency diarrhea wasconsidered as of potential infectiological relevance as wellThe field doctor in charge subjectively decided whether ornot he or she considered the symptoms of the patients tobe relevant and incapacitating enough for an inclusion intothe surveillance All diarrhea patients were asked by the fielddoctor in camp Koulikoro to provide a sample of native stoolfor molecular and cultural diagnostic analysis Investigationsof diseased local military or civilian personnel were not partof the surveillance
In addition to providing the samples the field doctorcollected data on diarrhea patients in a standardized way onthe delivery note that was sent together with the sample Theitems on these notes were as follows age gender nationalitymode of food intake site of deployment stool frequencystool consistency as described by the patient accompa-nying symptoms presence of fever type of antimalarialprophylaxis vaccination status against cholera and typhoidfever medication with antibiotic drugs any previous staysin high-endemicity settings regarding diarrhea (includingAfghanistan Bahrain Bolivia Colombia Kosovo Lebanonand Turkey [3]) and participation in counseling regardinghygiene on tropical deployments prior to the onset of diar-rhea In addition stool consistency of the samples providedwas assessed by the analyzing laboratory technician
While providing stool samples and thus participatingin the surveillance were voluntary all cases of diarrheaamong EUTM personnel that were registered by the fielddoctor were further routinely reported to the DeploymentHealth Surveillance Capability (DHSC) of the North AtlanticTreaty Organization (NATO) Military Medicine Center ofExcellence Again the diagnosis diarrhea was based on thefield doctorrsquos subjective decision whether or not he or sheconsidered the symptoms of the patients to be relevantand incapacitating These data and the number of deployedEUTM forces were used to calculate a weekly incidencerate as a passive surveillance procedure DHSC reports werecompared with the number of patients that were included inthe surveillance to estimate the achieved coverage
22 Laboratory Testing FromDecember 2013 toMarch 2014collected stool samples were analyzed by PCR directly in the
BioMed Research International 3
laboratory of the field hospital in Camp Koulikoro in MaliFrom April until August 2014 the samples were frozen atminus20∘C and shipped to Germany for further investigationAll culture-based diagnostic approaches were performed inGermany
221 Sample Preparation Prior to PCR analysis nucleicacids were extracted from all stool samples using the Qiampstool kit (Qiagen Hamburg Germany) The nucleic acidextraction was performed as described by the manufacturer
222 PCR Testing All samples were analyzed with a panelof real-time multiplex PCRs comprising two in-houseprotocols One of those in-house PCR tests targets theinvasive enteropathogenic bacteria Salmonella spp Shigellasppenteroinvasive Escherichia coli (EIEC) Campylobacterjejuni andYersinia spp [5 6]The diagnostic reliability of thisprocedure has been shown previously in comparison withcultural approaches [5] The other in-house PCR which isused for routine diagnostic analyses by the German NationalReferenceCentre for Tropical Diseases BernhardNocht Insti-tute Hamburg amplifies DNA of the enteropathogenic pro-tozoa Entamoeba histolytica Giardia duodenalis Cyclosporacayetanensis and Cryptosporidium parvum [3 6 7] Thepreviously described primer-probe-sets for Entamoeba his-tolytica Giardia duodenalis and Cryptosporidium parvumwere complemented by a primer-probe-set for Cyclosporacayetanensis that was adapted froma previous publication [7]No further changes to the described protocols [3 5 6 8] wereapplied The primer-probe-sets used are detailed in Table 1
In addition to the in-house multiplex real-time PCRassays described above three commercial RidaGene (R-Bio-pharm Darmstadt Germany) PCR kits ldquoEAECrdquo ldquoEHEC-EPECrdquo and ldquoETEC-EIECrdquo were applied targeting enteroag-gregative E coli (EAEC) enterohemorrhagic E coli (EHEC)enteropathogenic E coli (EPEC) enterotoxic E coli (ETEC)and Shigella sppEIEC Finally analyses using the commer-cial Fast-track Diagnostics (Sliema Malta) PCR kit ldquoviralgastroenteritisrdquo targeting Norovirus genogroups I (G1) and II(G2) Astrovirus Rotavirus Adenovirus and Sapovirus wereadded
Phocid herpesvirus DNA was chosen as the target forinhibition control PCR The procedure was performed asdescribed previously [8ndash10] The primer-probe-set is pre-sented in Table 1
223 Norovirus Sequencing Samples testing positive byNorovirus genogroup I (GI) or II (GII) PCR were subjectedto further sequence analysis In detail a 213-base-pair (bp)part of the open reading frame 1 (ORF1) was amplified usingdegenerate multiplex primers MON432MON434 (GI) andMON431MON433 (GII) as described [11] Amplified DNAwas sent for sequencing (Seqlab Gottingen Germany) afternucleic acid gel extraction and cleanup with a QIAquickGel Extraction Kit (QIAGEN Hilden Germany) Sequenceassembly and analysis were performed with the softwareDNAStar Lasergene 121 genomics suite (DNASTAR IncMadisonWI USA) Subsequent genotyping was based uponthe Norovirus genotyping tool as described [12]
224 Cultural Growth Identification and Resistance TestingIf sufficient stool material was available cherry-pit-sized vol-umes were used for broth enrichment in thioglycolate broth(Heipha Eppelheim Germany) This was the case for a totalof 48 out of 53 samples Incubation was performed for 16ndash24hours at 37∘C Broth enrichment increases the yield of ESBL-expressing bacteria after swabbing for example by a factorof 2 in upper respiratory tract samples [13] Subsequently10 120583L preincubated broth was cultured on Brilliance ESBLselective agar (Oxoid Basingstoke UK) This agar is madefor selective growth of ESBL-positive EnterobacteriaceaeSensitivity of 949ndash979 and specificity of 957ndash100 havebeen described for Brilliance ESBL selective agar [14 15]Agar plates were incubated at 37∘C for 40ndash48 hours Allcolonies that looked suspicious for Enterobacteriaceae (bluegreen and brown colonies) were isolated while suspectedGram-negative nonfermentative rod-shaped bacteria (ieyellow or yellowish-brown or greenish-brown colonies) werediscarded All isolates were frozen at minus80∘C in Microbanktubes (Pro-LabDiagnostics Bromborough UK) until furtherassessment
Identification was performed by VITEK-II GN-cards(bioMerieux Marcy-lrsquoEtoile France) and matrix-assistedlaser-desorption-ionization time-of-flight mass spectrome-try (MALDI-TOF-MS) using a ShimadzuKratos ldquoAXIMAAssurancerdquo MALDI-TOF mass spectrometer (ShimadzuGermany Ltd Duisburg Germany) [16] For MALDI-TOFanalyses isolates were prepared using alpha-cyano-4-hydroxycinnamic acid (bioMerieux) as matrix Spectralfingerprints were analyzed using Vitek MS IVD V2 databaseMS-CE versionCLI 200 (bioMerieux) Automated antibioticsusceptibility testing was performed with VITEK-II AST-N263-cards (bioMerieux) In case of uncertain resultsE-testing (bioMerieux) was added Interpretation of resist-ance testing results was based on the EUCAST guideline(version 40 2014 httpwwweucastorgfileadminsrcme-diaPDFsEUCAST filesBreakpoint tablesBreakpoint tab-le v 40pdf)
225 Rep-PCR Typing of Extended-Spectrum Beta-LactamasePositive E coli All confirmed ESBL-positive E coli strainsfromESBL selective agar were grown overnight in brain heartinfusion broth DNA was extracted using the MoBio Ultr-aClean Microbial DNA Isolation Kit (Mo Bio LaboratoriesInc Carlsbad CA USA) Purified DNA samples were ampli-fied using the DiversiLab Escherichia DNA fingerprinting kit(reference number 410 980 bioMerieux) on a T-personalthermal cycler (Biometra Gottingen Germany) Rep-PCRproducts were detected by chip-based DNA separation onanAgilent 2100 Bioanalyzer (Agilent Technologies Inc SantaClara CA USA) All techniques were executed according tothe manufacturersrsquo instructions
Documentation and band-pattern analysis were per-formed using the DiversiLab software version 33 (bioMeri-eux) A correlation cutoff of 95 for confirmation or exclu-sion of clonal identity of analyzed strains was applied asrecommended by the manufacturer All library entries wereanalyzed in duplicate
4 BioMed Research International
Table1Sequ
enceso
fthe
prim
er-probe-setsu
sedin
thea
ppliedreal-timeP
CRassays
[5ndash9
]
Targetorganism
Forw
ardprim
erRe
versep
rimer
TaqM
anprob
eMultip
lex-PC
Rtargetinginvasiv
eentericbacteria
Salm
onellaspp
51015840-ATT
-GTT
-GAT
-TCA
-GGT-AC
A-AAC
-31015840
51015840-AAT
-TAG
-CCA
-TGT-TG
T-AAT
-CTC
-31015840
51015840-C
AA-
GTT
-CAA-
CGC-
GCA
-ATT
-TA-
31015840ShigellasppEIEC
51015840-C
AG-AAG
-AGC-AG
A-AG
T-AT
G-AG-31015840
51015840-C
AG-TAC
-CTC
-GTC
-AGT-CA
G-31015840
51015840-ACA
-GGT-GAT
-GCG
-TGA-
GAC
-TG-31015840
Campylobacterjejun
i51015840-C
TA-TAA-
CAA-
CTG-C
AC-C
TA-C
TA-AT-31015840
51015840-AAG
-TGT-AAG
-CAC
-ACA
-AGG-TA-
3101584051015840-C
TT-AAT
-AGC-
CGT-CA
C-CC
C-AC
-31015840
Yersiniaspp
51015840-G
CA-TTA
-ACG
-AAT
-ATG
-TTA
-GC-
3101584051015840-ATC
-GAG
-TTT
-GGA-
GTA
-TTC
-AT-31015840
51015840-C
CG-C
TT-C
CA-AAT
-TTT
-GTC
-AT-31015840
Multip
lex-PC
Rtargetingenteric
protozoa
Entamoeba
histo
lytica
51015840-ATT
-GTC
-GTG
-GCA
-TCC
-TAA-
CTC-A-
3101584051015840-G
CG-G
AC-G
GC-TC
A-TT
A-TA
A-CA
-31015840
51015840-TCA
-TTG
-AAT
-GAA-TT
G-G
CC-ATT
-T-31015840
Giardiadu
odenalis
51015840-G
AC-G
GC-TC
A-GGA-
CAA-
CGG-TT-31015840
51015840-TTG
-CCA
-GCG
-GTG
-TCC
-G-31015840
51015840-C
CC-G
CG-G
CG-G
TC-C
CT-G
CT-AG-31015840
Cyclo
spora
cayetanensis
51015840-TAG
-TAA-
CCG-AAC
-GGA-TC
G-C
AT-T-31015840
51015840-AAT
-GCC
-ACG
-GTA
-GGC-
CAA-TA
-31015840
51015840-C
CG-G
CG-ATA
-GAT
-CAT
-TCA
-AGT-TT
C-TG
A-CC
-31015840
Cryptosporidium
parvum
51015840-C
GC-TT
C-TC
T-AG
C-CT
T-TC
A-TG
A-31015840
51015840-C
TT-C
AC-G
TG-TGT-TT
G-C
CA-AT-31015840
51015840-C
CA-ATC
-ACA
-GAA-TC
A-TC
A-GAA-TC
G-ACT
-GGT-AT
C-31015840
InternalcontrolP
CRtargetingph
ocid
herpesvirusD
NA
Phocid
herpes
virus
51015840-G
GG-C
GA-AT
C-AC
A-GAT
-TGA-AT
C-31015840
51015840-G
CG-G
TT-C
CA-AAC
-GTA
-CCA
-A-31015840
51015840-TTT
-TTA
-TGT-GTC
-CGC-
CAC-
CAT-CT
G-G
ATC-
31015840
BioMed Research International 5
Table 2 Median and mean cycle threshold (Ct) values of pathogens that were detected by PCR
Detected pathogen Median Ct-value Mean Ct-value Standard deviationSalmonella spp 27 27 mdashShigella sppEIEC1 175 18 30Shigella sppEIEC2 135 147 27Shigella sppEIEC3 125 137 24EPEC 22 214 40STEC4 14 159 39STEC5 19 182 43EAEC 19 192 35Giardia duodenalis 255 255 35Cryptosporidium parvum 27 277 60Norovirus G1 20 243 84Norovirus G2 17 166 43Astrovirus 30 30 mdashRotavirus 22 22 mdashSapovirus 32 32 mdash1As detected by in-house PCR 2As detected by RidaGene PCR targeting EHECEPECShigella sppEIEC 3As detected by RidaGene PCR targeting ETEC andShigella sppEIEC 4As detected by PCR targeting the stable toxin 5As detected by PCR targeting the labile toxin
23 Ethics The surveillance described here was ordered asa preventive medical procedure by the German command-ing hygiene officer of the EUTM Mali mission Respectiveorders are legally covered by the self-administrative rightsldquoEigenvollzugskompetenzrdquo of the German Armed ForcesMedical Service regarding infectious disease prevention andcontrol ldquoInfektionsschutzrdquo Collected data were assessedanonymously thus avoiding any violation of sect25 of theDeclaration of Helsinki (DoHOct 2008) or national dataprotection laws ldquoBundesdatenschutzgesetzrdquo
3 Results
31 Frequency of Diarrhea and Coverage Based on thereports of the field doctors to the NATO Deployment HealthSurveillance Capability (DHSC) an average weekly incidenceof diarrhea among EUTM soldiers of 58 patients per weekwas calculated The average number of deployed soldiers atrisk was 480 the resulting average weekly incidence rate per1000 soldiers was 121 During the surveillance period of 37weeks a total of 53 stool samples from 51 EUTM soldiers withdiarrheawere collected resulting in an average of 14 cases perweek Accordingly the coverage of the surveillance was about241 of the registered diarrhea cases
32 Diagnostic Results Positive PCR results for diarrhea-associated pathogens could be detected in 4353 patientsamples The five quantitatively dominating pathogenswere EPEC (119899 = 21) ETEC (119899 = 19) EAEC (119899 = 15)Norovirus (119899 = 10) and ShigellaEIEC (119899 = 6) followed byCryptosporidium parvum (119899 = 3)Giardia duodenalis (119899 = 2)Salmonella spp (119899 = 1) Astrovirus (119899 = 1) Rotavirus(119899 = 1) and Sapovirus (119899 = 1) Of note both detections ofGiardia duodenalis were in the same patient so copy-strainassessment occurred here Median and mean cycle threshold
(Ct) values as well as calculated standard deviations (SD)are given in Table 2 Of note the lowest Ct values weredetected for bacteria Ct-values for Shigella sppEIEC variedconsiderably depending on the primer-probe compositionused with lowest Ct-values in the RidaGene ETECEIEC kitand highest in the in-house approach
DNA of two and more pathogens was detected in 23 ofthe samples of three and more pathogens in 11 samples offour and more pathogens in 2 samples and of as many as fivepathogens in 1 sample Measured Ct values for the respectivecases are given in Table 3 In several cases low Ct-values aremeasured for more than one pathogen
33 Norovirus Genotyping Sequence analysis and genotyp-ing verified the detection of Norovirus GII in six out ofseven initially PCR-positive cases The procedure failed forthe seventh Norovirus GII detection and for all three casespositive for Norovirus GI At least two out of three NorovirusGI-positive cases were confirmed by a separate real-time RT-PCR [17 18] (data not shown)
Genotyping of the six sequenced Norovirus G2 strainsrevealed GIIP7 in four instances Three out of those fourstrains showed identical sequences suggesting either noso-comial transmission or a common source of infection Epi-demiological assessment showed that the respective sampleswere collected from three patients within a single weekmaking a mini-outbreak highly likely In two out of sixinstances Norovirus GIIP16 and GIIP4 var New Orleanswere identified respectively
The underlying sequence information has been depositedand is freely accessible via httpwwwrivmnlmpfnoro-virustypingtooljob1197792283
34 Cultural Approach From 13 out of the 48 analyzed stoolsamples ESBL-positive Enterobacteriaceae were isolated by
6 BioMed Research International
Table 3 Ct-values in cases of multiple pathogen detections (in brackets) If both stable and labile toxin of STEC were detected two Ct-valuesare given otherwise only one In case of Shigella sppEIEC detections three Ct-values are shown reflecting the three applied PCR approachesIn several cases low Ct-values are measured for more than one pathogen
Case Pathogen 1 Pathogen 2 Pathogen 3 Pathogen 4 Pathogen 5
1 Shigella sppEIEC (Ct13 14 16) EPEC (Ct 18) ETEC (Ct 13 16) EAEC (Ct 19) Norovirus G1 (Ct 20)
2 Salmonella spp (Ct 27) EPEC (Ct 15) Norovirus G2 (Ct 11) Astrovirus (Ct 30) mdash
3 EPEC (Ct 29) EAEC (Ct 19) Norovirus G2 (Ct 17) mdash mdash
4 ETEC (Ct 17 20) EAEC (Ct 19) Norovirus G2 (Ct 14) mdash mdash
5 ETEC (Ct 13 20) EAEC (Ct 18) Norovirus G2 (Ct 21) mdash mdash
6 Shigella sppEIEC (Ct12 13 14) EPEC (Ct 21) ETEC (Ct 21) mdash mdash
7 EPEC (Ct 17) ETEC (Ct 20) EAEC (Ct 19) mdash mdash
8 EPEC (Ct 20) ETEC (Ct 13) EAEC (Ct 21) mdash mdash
9 EPEC (Ct 16) ETEC (Ct 13) EAEC (Ct 22) mdash mdash
10 ETEC (Ct 15) EAEC (Ct 15) Cryptosporidiumparvum (Ct 34) mdash mdash
11 EPEC (Ct 23) ETEC (Ct 16 21) EAEC (Ct 22) mdash mdash
12 Shigella sppEIEC (Ct18 20 21) EPEC (Ct 26) mdash mdash mdash
13 EPEC (Ct 28) Giardia duodenalis(Ct 28) mdash mdash mdash
14 EPEC (Ct 21) ETEC (Ct 17) mdash mdash mdash
15 EPEC (Ct 25) ETEC (Ct 12) mdash mdash mdash
16 EPEC (Ct 22) Norovirus G2 (Ct 17) mdash mdash mdash
17 ETEC (Ct 11 18) EAEC (Ct 14) mdash mdash mdash
18 ETEC (Ct 15) EAEC (Ct 23) mdash mdash mdash
19 EAEC (Ct 18) Cryptosporidiumparvum (Ct 22) mdash mdash mdash
20 EPEC (Ct 22) Sapovirus (Ct 32) mdash mdash mdash
21 Shigella sppEIEC (Ct12 23 18) EPEC (Ct 19) mdash mdash mdash
22 EPEC (Ct 22) ETEC (Ct 19 19) mdash mdash mdash
23 EPEC (Ct 21) ETEC (Ct 24 29) mdash mdash mdash
thioglycolate broth enrichment with subsequent growthon ESBL selective agar From 12 samples ESBL-positiveEscherichia coli were isolated with proof of more than onestrain in two instances The total number of ESBL-positive Ecoli strainswas 15One of those strainswas identified as EAECby RidaGene PCR An ESBL-positive Klebsiella pneumoniaestrain was isolated from another sample
For the 13 samples containing ESBL-positive Enterobac-teriaceae sensitivity against nonpenicillin noncephalosporinantibiotics was determined by VITEK-II- and E-test-basedresistance testing If several ESBL-positive E coli weresimultaneously isolated the most resistant strain with theresulting highest risk of selection under antibiotic pressurewas chosen Sensitivity for carbapenems tigecycline and
fosfomycin was shown in all 13 cases in 12 for nitrofurantoinwhich is only suitable for urinary tract infections in 11for fluoroquinolones and in 10 for gentamicin Resistanceagainst trimethoprimsulfamethoxazole which is frequentlyencountered in tropical settings was demonstrated in all 13cases
35 Rep-PCR of ESBL-Positive Enterobacteriaceae In total15 E coli strains from 12 patients were subjected to rep-PCR-based DiversiLab typing Within the 95 cutoff rangefor clonal identity three clonal clusters comprising 7 strainsfrom 6 patients were observed (Figure 1) This suggests thepresence of common sources of infection or nosocomial
BioMed Research International 7
10
5
11
4ndash2
3
6ndash1
2
1
12
13
8
4ndash3
7
4ndash1
6ndash2
Similarity ()
Dendrogram Strain Band pattern
10090 958580757065
Figure 1 Dendrogram of the DiversiLab typing results of 15 ESBL-positive E coli strains from 12 patients The strainsrsquo labeling consistsof the patient number (number before the ldquondashrdquo) and the strainnumber in case ofmore than one isolated ESBL-positive E coli strainper patient (number following the ldquondashrdquo) The strain of patient 9 ismissing as the respective ESBL-positive isolate was not E coli butK pneumoniae Three clusters of clonal identity beyond the 95-similarity cutoff (dotted red line) are detectable
transmission within the camp One patient was even colo-nized by E coli strains from two different clusters (Figure 1)For the remaining 8 strains from 6 patients clonal identitywas excluded
36 Clinical and Epidemiological Assessment Clinical datawere provided for 49 patients The completeness of clinicaldata varied missing data are characterized as ldquono datardquo in thetables in the following In those 49 diarrhea patients bacterialpathogens were detected in 34 instances viral pathogens in 12instances and parasitic pathogens in 3 instances No entericpathogen was detectable in 9 out of these 49 patients with theapplied procedures DNA of more than one enteric pathogenwas detectable in 23 of the soldiers with acute diarrhea
361 Age Gender Nationality Sites of Deployment andPrevious Stays in High-Endemicity Regions for Diarrhea-Associated Pathogens No particular distribution pattern ofbacterial viral and parasitic enteric pathogens was observedwith respect to gender and nationality of the soldiers withdiarrhea Soldiers who were younger than 30 years of age
showed coinfections with multiple enteric pathogens lessfrequently than older soldiers Of note all assessed diarrheapatients who were deployed to Bapho were infected by viralpathogens Previous stays in high-endemicity settings did nothave any notable effects on the acquisition of bacterial viraland parasitic pathogens (Table 4)
362 Mode of Food Intake As few as 2 out of 15 diarrheapatients who claimed to have eaten exclusively in the fieldkitchen were free of enteric pathogens in the PCR analysesBacterial pathogens dominated in this group Soldiers whorestricted their diet to hotel food were prone to both bacterialand viral enteric infections There was not a single diarrheapatient in this assessment who had eaten field rations aloneprior to the onset of diarrhea (Table 5)
363 Stool Frequency andConsistency A small proportion of11 patients showed less severe symptomswith fewer than threeunformed stools per day Of note no enteric pathogens weredetected in only one of these patients There was no obviousdistribution pattern of bacterial viral or parasitic pathogensin these less severe diarrhea cases
The observed stool consistency of collected samples asreported by the laboratory technician was considerably lessunformed than the reported stool consistency A total of 13out of 49 stool samples were already hard at the time ofsample collection suggesting that the symptoms had alreadyimproved In contrast no patient reported formed stools tothe field doctor Only 3 out of these 13 formed stools werewithout detectable pathogen DNA at the time of assessment(Table 6)
364 Accompanying Symptoms including Fever Light tomoderate symptoms including nausea and vomiting crampsabdominal pain and flatulence were frequent in the assesseddiarrhea patients Cramps abdominal pain and flatulencewere particularly often detectable in diarrhea patients withbacterial infections while nausea and vomiting were equallylikely for both bacterial and viral infections Only oneinstance of bloody diarrhea was observed in a patient withShigella sppEIEC as the only detectable pathogen in stoolFever was confirmed in only three instances without anydetectable association with a particular pathogen group(Table 7)
Of note the distribution of accompanying symptoms didnot change considerably if only the 34 patients who reportedge3 stools per day were included into the assessment (Table 7)
Only one enteric pathogen per patient was detected in 16patients who reported accompanying symptoms comprising4 cases with STEC 2 cases with EAEC 2 cases with EPEC 2cases with Norovirus G1 2 cases with Norovirus G2 2 caseswith Shigella sppEIEC 1 case withCryptosporidium parvumand 1 case with Rotavirus respectively Bacterial infectionswere associated with a broad distribution of symptoms(Table 7) As expected patients infected with enteroinvasiveShigella sppEIEC showed a particularly wide spectrumof symptoms Norovirus infections and Cryptosporidiumparvum infections were associated with nausea vomiting
8 BioMed Research International
Table 4 Age gender nationality sites of deployment and previous stays in high-endemicity regions for diarrhea-associated pathogens ofdiarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Agelt30 years 1015 615 015 215 51530ndash50 years 1015 315 115 315 815gt50 years 22 12 02 02 22No data 1217 217 217 417 717
GenderMale 3144 1144 344 744 2044Female 35 15 05 25 25
NationalityAustria 11 11 01 01 11Belgium 79 29 19 19 39Colombia 11 01 01 01 01Germany 1725 825 025 425 1225Greece 33 03 13 03 33Ireland 01 01 01 11 01Italy 01 01 01 11 01Portugal 01 01 01 11 01Romania 01 11 01 01 01Spain 44 04 04 04 24SpainBolivia 01 01 01 11 01No data 11 01 11 01 11
Site of deploymentKoulikoro 3141 741 341 641 1941Koulikoro and Bamako 12 12 02 12 12Bamako 01 01 01 11 01Bapho 24 44 04 04 24No data 01 01 01 11 01
Previous stays in high endemicitysettings
Yes 813 313 113 213 413No 2636 936 236 736 1836
and abdominal pain and Norovirus G1 infections also wereassociated with cramps and flatulence (Table 7)
365 Antimalarial Prophylaxis Hygiene Counseling Vacci-nation against Cholera and Typhoid Fever and MedicationLow-dose doxycycline-monohydrate antimalarial prophy-laxis at 100mgday did not provide any protection againstbacterial enteric infections Among the diarrhea patientsunder doxycycline prophylaxis 7 out of 10 were positive forDNA of bacterial enteric pathogens
The vast majority of diarrhea patients were properlycounseled regarding hygiene on tropical deployments andwere vaccinated against typhoid fever Infections with bacte-rial enteric pathogens were particularly frequent in patientswho were vaccinated against cholera and typhoid fever Useof anti-infective drugs was documented for three patients
all three took rifaximin and one in addition metronidazoleDNA of bacterial enteric pathogens was detectable in onlyone of these patients no pathogen DNA was observed in twoof them (Table 8)
4 Discussion
Risk assessment by standardized monitoring and surveil-lance of deployed soldiers in subtropical or tropical coun-tries contributes to evaluation of both individual risk andpreventive measures As previously shown infection riskswith enteric pathogens increase if sophisticated hygieneprecautions regarding food and drinking water cannot bemaintained on military deployments for example in thecase of small missions [3] Considering an average clinicalincidence of diarrhea between 5 and 7 per 100 per month
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 3
laboratory of the field hospital in Camp Koulikoro in MaliFrom April until August 2014 the samples were frozen atminus20∘C and shipped to Germany for further investigationAll culture-based diagnostic approaches were performed inGermany
221 Sample Preparation Prior to PCR analysis nucleicacids were extracted from all stool samples using the Qiampstool kit (Qiagen Hamburg Germany) The nucleic acidextraction was performed as described by the manufacturer
222 PCR Testing All samples were analyzed with a panelof real-time multiplex PCRs comprising two in-houseprotocols One of those in-house PCR tests targets theinvasive enteropathogenic bacteria Salmonella spp Shigellasppenteroinvasive Escherichia coli (EIEC) Campylobacterjejuni andYersinia spp [5 6]The diagnostic reliability of thisprocedure has been shown previously in comparison withcultural approaches [5] The other in-house PCR which isused for routine diagnostic analyses by the German NationalReferenceCentre for Tropical Diseases BernhardNocht Insti-tute Hamburg amplifies DNA of the enteropathogenic pro-tozoa Entamoeba histolytica Giardia duodenalis Cyclosporacayetanensis and Cryptosporidium parvum [3 6 7] Thepreviously described primer-probe-sets for Entamoeba his-tolytica Giardia duodenalis and Cryptosporidium parvumwere complemented by a primer-probe-set for Cyclosporacayetanensis that was adapted froma previous publication [7]No further changes to the described protocols [3 5 6 8] wereapplied The primer-probe-sets used are detailed in Table 1
In addition to the in-house multiplex real-time PCRassays described above three commercial RidaGene (R-Bio-pharm Darmstadt Germany) PCR kits ldquoEAECrdquo ldquoEHEC-EPECrdquo and ldquoETEC-EIECrdquo were applied targeting enteroag-gregative E coli (EAEC) enterohemorrhagic E coli (EHEC)enteropathogenic E coli (EPEC) enterotoxic E coli (ETEC)and Shigella sppEIEC Finally analyses using the commer-cial Fast-track Diagnostics (Sliema Malta) PCR kit ldquoviralgastroenteritisrdquo targeting Norovirus genogroups I (G1) and II(G2) Astrovirus Rotavirus Adenovirus and Sapovirus wereadded
Phocid herpesvirus DNA was chosen as the target forinhibition control PCR The procedure was performed asdescribed previously [8ndash10] The primer-probe-set is pre-sented in Table 1
223 Norovirus Sequencing Samples testing positive byNorovirus genogroup I (GI) or II (GII) PCR were subjectedto further sequence analysis In detail a 213-base-pair (bp)part of the open reading frame 1 (ORF1) was amplified usingdegenerate multiplex primers MON432MON434 (GI) andMON431MON433 (GII) as described [11] Amplified DNAwas sent for sequencing (Seqlab Gottingen Germany) afternucleic acid gel extraction and cleanup with a QIAquickGel Extraction Kit (QIAGEN Hilden Germany) Sequenceassembly and analysis were performed with the softwareDNAStar Lasergene 121 genomics suite (DNASTAR IncMadisonWI USA) Subsequent genotyping was based uponthe Norovirus genotyping tool as described [12]
224 Cultural Growth Identification and Resistance TestingIf sufficient stool material was available cherry-pit-sized vol-umes were used for broth enrichment in thioglycolate broth(Heipha Eppelheim Germany) This was the case for a totalof 48 out of 53 samples Incubation was performed for 16ndash24hours at 37∘C Broth enrichment increases the yield of ESBL-expressing bacteria after swabbing for example by a factorof 2 in upper respiratory tract samples [13] Subsequently10 120583L preincubated broth was cultured on Brilliance ESBLselective agar (Oxoid Basingstoke UK) This agar is madefor selective growth of ESBL-positive EnterobacteriaceaeSensitivity of 949ndash979 and specificity of 957ndash100 havebeen described for Brilliance ESBL selective agar [14 15]Agar plates were incubated at 37∘C for 40ndash48 hours Allcolonies that looked suspicious for Enterobacteriaceae (bluegreen and brown colonies) were isolated while suspectedGram-negative nonfermentative rod-shaped bacteria (ieyellow or yellowish-brown or greenish-brown colonies) werediscarded All isolates were frozen at minus80∘C in Microbanktubes (Pro-LabDiagnostics Bromborough UK) until furtherassessment
Identification was performed by VITEK-II GN-cards(bioMerieux Marcy-lrsquoEtoile France) and matrix-assistedlaser-desorption-ionization time-of-flight mass spectrome-try (MALDI-TOF-MS) using a ShimadzuKratos ldquoAXIMAAssurancerdquo MALDI-TOF mass spectrometer (ShimadzuGermany Ltd Duisburg Germany) [16] For MALDI-TOFanalyses isolates were prepared using alpha-cyano-4-hydroxycinnamic acid (bioMerieux) as matrix Spectralfingerprints were analyzed using Vitek MS IVD V2 databaseMS-CE versionCLI 200 (bioMerieux) Automated antibioticsusceptibility testing was performed with VITEK-II AST-N263-cards (bioMerieux) In case of uncertain resultsE-testing (bioMerieux) was added Interpretation of resist-ance testing results was based on the EUCAST guideline(version 40 2014 httpwwweucastorgfileadminsrcme-diaPDFsEUCAST filesBreakpoint tablesBreakpoint tab-le v 40pdf)
225 Rep-PCR Typing of Extended-Spectrum Beta-LactamasePositive E coli All confirmed ESBL-positive E coli strainsfromESBL selective agar were grown overnight in brain heartinfusion broth DNA was extracted using the MoBio Ultr-aClean Microbial DNA Isolation Kit (Mo Bio LaboratoriesInc Carlsbad CA USA) Purified DNA samples were ampli-fied using the DiversiLab Escherichia DNA fingerprinting kit(reference number 410 980 bioMerieux) on a T-personalthermal cycler (Biometra Gottingen Germany) Rep-PCRproducts were detected by chip-based DNA separation onanAgilent 2100 Bioanalyzer (Agilent Technologies Inc SantaClara CA USA) All techniques were executed according tothe manufacturersrsquo instructions
Documentation and band-pattern analysis were per-formed using the DiversiLab software version 33 (bioMeri-eux) A correlation cutoff of 95 for confirmation or exclu-sion of clonal identity of analyzed strains was applied asrecommended by the manufacturer All library entries wereanalyzed in duplicate
4 BioMed Research International
Table1Sequ
enceso
fthe
prim
er-probe-setsu
sedin
thea
ppliedreal-timeP
CRassays
[5ndash9
]
Targetorganism
Forw
ardprim
erRe
versep
rimer
TaqM
anprob
eMultip
lex-PC
Rtargetinginvasiv
eentericbacteria
Salm
onellaspp
51015840-ATT
-GTT
-GAT
-TCA
-GGT-AC
A-AAC
-31015840
51015840-AAT
-TAG
-CCA
-TGT-TG
T-AAT
-CTC
-31015840
51015840-C
AA-
GTT
-CAA-
CGC-
GCA
-ATT
-TA-
31015840ShigellasppEIEC
51015840-C
AG-AAG
-AGC-AG
A-AG
T-AT
G-AG-31015840
51015840-C
AG-TAC
-CTC
-GTC
-AGT-CA
G-31015840
51015840-ACA
-GGT-GAT
-GCG
-TGA-
GAC
-TG-31015840
Campylobacterjejun
i51015840-C
TA-TAA-
CAA-
CTG-C
AC-C
TA-C
TA-AT-31015840
51015840-AAG
-TGT-AAG
-CAC
-ACA
-AGG-TA-
3101584051015840-C
TT-AAT
-AGC-
CGT-CA
C-CC
C-AC
-31015840
Yersiniaspp
51015840-G
CA-TTA
-ACG
-AAT
-ATG
-TTA
-GC-
3101584051015840-ATC
-GAG
-TTT
-GGA-
GTA
-TTC
-AT-31015840
51015840-C
CG-C
TT-C
CA-AAT
-TTT
-GTC
-AT-31015840
Multip
lex-PC
Rtargetingenteric
protozoa
Entamoeba
histo
lytica
51015840-ATT
-GTC
-GTG
-GCA
-TCC
-TAA-
CTC-A-
3101584051015840-G
CG-G
AC-G
GC-TC
A-TT
A-TA
A-CA
-31015840
51015840-TCA
-TTG
-AAT
-GAA-TT
G-G
CC-ATT
-T-31015840
Giardiadu
odenalis
51015840-G
AC-G
GC-TC
A-GGA-
CAA-
CGG-TT-31015840
51015840-TTG
-CCA
-GCG
-GTG
-TCC
-G-31015840
51015840-C
CC-G
CG-G
CG-G
TC-C
CT-G
CT-AG-31015840
Cyclo
spora
cayetanensis
51015840-TAG
-TAA-
CCG-AAC
-GGA-TC
G-C
AT-T-31015840
51015840-AAT
-GCC
-ACG
-GTA
-GGC-
CAA-TA
-31015840
51015840-C
CG-G
CG-ATA
-GAT
-CAT
-TCA
-AGT-TT
C-TG
A-CC
-31015840
Cryptosporidium
parvum
51015840-C
GC-TT
C-TC
T-AG
C-CT
T-TC
A-TG
A-31015840
51015840-C
TT-C
AC-G
TG-TGT-TT
G-C
CA-AT-31015840
51015840-C
CA-ATC
-ACA
-GAA-TC
A-TC
A-GAA-TC
G-ACT
-GGT-AT
C-31015840
InternalcontrolP
CRtargetingph
ocid
herpesvirusD
NA
Phocid
herpes
virus
51015840-G
GG-C
GA-AT
C-AC
A-GAT
-TGA-AT
C-31015840
51015840-G
CG-G
TT-C
CA-AAC
-GTA
-CCA
-A-31015840
51015840-TTT
-TTA
-TGT-GTC
-CGC-
CAC-
CAT-CT
G-G
ATC-
31015840
BioMed Research International 5
Table 2 Median and mean cycle threshold (Ct) values of pathogens that were detected by PCR
Detected pathogen Median Ct-value Mean Ct-value Standard deviationSalmonella spp 27 27 mdashShigella sppEIEC1 175 18 30Shigella sppEIEC2 135 147 27Shigella sppEIEC3 125 137 24EPEC 22 214 40STEC4 14 159 39STEC5 19 182 43EAEC 19 192 35Giardia duodenalis 255 255 35Cryptosporidium parvum 27 277 60Norovirus G1 20 243 84Norovirus G2 17 166 43Astrovirus 30 30 mdashRotavirus 22 22 mdashSapovirus 32 32 mdash1As detected by in-house PCR 2As detected by RidaGene PCR targeting EHECEPECShigella sppEIEC 3As detected by RidaGene PCR targeting ETEC andShigella sppEIEC 4As detected by PCR targeting the stable toxin 5As detected by PCR targeting the labile toxin
23 Ethics The surveillance described here was ordered asa preventive medical procedure by the German command-ing hygiene officer of the EUTM Mali mission Respectiveorders are legally covered by the self-administrative rightsldquoEigenvollzugskompetenzrdquo of the German Armed ForcesMedical Service regarding infectious disease prevention andcontrol ldquoInfektionsschutzrdquo Collected data were assessedanonymously thus avoiding any violation of sect25 of theDeclaration of Helsinki (DoHOct 2008) or national dataprotection laws ldquoBundesdatenschutzgesetzrdquo
3 Results
31 Frequency of Diarrhea and Coverage Based on thereports of the field doctors to the NATO Deployment HealthSurveillance Capability (DHSC) an average weekly incidenceof diarrhea among EUTM soldiers of 58 patients per weekwas calculated The average number of deployed soldiers atrisk was 480 the resulting average weekly incidence rate per1000 soldiers was 121 During the surveillance period of 37weeks a total of 53 stool samples from 51 EUTM soldiers withdiarrheawere collected resulting in an average of 14 cases perweek Accordingly the coverage of the surveillance was about241 of the registered diarrhea cases
32 Diagnostic Results Positive PCR results for diarrhea-associated pathogens could be detected in 4353 patientsamples The five quantitatively dominating pathogenswere EPEC (119899 = 21) ETEC (119899 = 19) EAEC (119899 = 15)Norovirus (119899 = 10) and ShigellaEIEC (119899 = 6) followed byCryptosporidium parvum (119899 = 3)Giardia duodenalis (119899 = 2)Salmonella spp (119899 = 1) Astrovirus (119899 = 1) Rotavirus(119899 = 1) and Sapovirus (119899 = 1) Of note both detections ofGiardia duodenalis were in the same patient so copy-strainassessment occurred here Median and mean cycle threshold
(Ct) values as well as calculated standard deviations (SD)are given in Table 2 Of note the lowest Ct values weredetected for bacteria Ct-values for Shigella sppEIEC variedconsiderably depending on the primer-probe compositionused with lowest Ct-values in the RidaGene ETECEIEC kitand highest in the in-house approach
DNA of two and more pathogens was detected in 23 ofthe samples of three and more pathogens in 11 samples offour and more pathogens in 2 samples and of as many as fivepathogens in 1 sample Measured Ct values for the respectivecases are given in Table 3 In several cases low Ct-values aremeasured for more than one pathogen
33 Norovirus Genotyping Sequence analysis and genotyp-ing verified the detection of Norovirus GII in six out ofseven initially PCR-positive cases The procedure failed forthe seventh Norovirus GII detection and for all three casespositive for Norovirus GI At least two out of three NorovirusGI-positive cases were confirmed by a separate real-time RT-PCR [17 18] (data not shown)
Genotyping of the six sequenced Norovirus G2 strainsrevealed GIIP7 in four instances Three out of those fourstrains showed identical sequences suggesting either noso-comial transmission or a common source of infection Epi-demiological assessment showed that the respective sampleswere collected from three patients within a single weekmaking a mini-outbreak highly likely In two out of sixinstances Norovirus GIIP16 and GIIP4 var New Orleanswere identified respectively
The underlying sequence information has been depositedand is freely accessible via httpwwwrivmnlmpfnoro-virustypingtooljob1197792283
34 Cultural Approach From 13 out of the 48 analyzed stoolsamples ESBL-positive Enterobacteriaceae were isolated by
6 BioMed Research International
Table 3 Ct-values in cases of multiple pathogen detections (in brackets) If both stable and labile toxin of STEC were detected two Ct-valuesare given otherwise only one In case of Shigella sppEIEC detections three Ct-values are shown reflecting the three applied PCR approachesIn several cases low Ct-values are measured for more than one pathogen
Case Pathogen 1 Pathogen 2 Pathogen 3 Pathogen 4 Pathogen 5
1 Shigella sppEIEC (Ct13 14 16) EPEC (Ct 18) ETEC (Ct 13 16) EAEC (Ct 19) Norovirus G1 (Ct 20)
2 Salmonella spp (Ct 27) EPEC (Ct 15) Norovirus G2 (Ct 11) Astrovirus (Ct 30) mdash
3 EPEC (Ct 29) EAEC (Ct 19) Norovirus G2 (Ct 17) mdash mdash
4 ETEC (Ct 17 20) EAEC (Ct 19) Norovirus G2 (Ct 14) mdash mdash
5 ETEC (Ct 13 20) EAEC (Ct 18) Norovirus G2 (Ct 21) mdash mdash
6 Shigella sppEIEC (Ct12 13 14) EPEC (Ct 21) ETEC (Ct 21) mdash mdash
7 EPEC (Ct 17) ETEC (Ct 20) EAEC (Ct 19) mdash mdash
8 EPEC (Ct 20) ETEC (Ct 13) EAEC (Ct 21) mdash mdash
9 EPEC (Ct 16) ETEC (Ct 13) EAEC (Ct 22) mdash mdash
10 ETEC (Ct 15) EAEC (Ct 15) Cryptosporidiumparvum (Ct 34) mdash mdash
11 EPEC (Ct 23) ETEC (Ct 16 21) EAEC (Ct 22) mdash mdash
12 Shigella sppEIEC (Ct18 20 21) EPEC (Ct 26) mdash mdash mdash
13 EPEC (Ct 28) Giardia duodenalis(Ct 28) mdash mdash mdash
14 EPEC (Ct 21) ETEC (Ct 17) mdash mdash mdash
15 EPEC (Ct 25) ETEC (Ct 12) mdash mdash mdash
16 EPEC (Ct 22) Norovirus G2 (Ct 17) mdash mdash mdash
17 ETEC (Ct 11 18) EAEC (Ct 14) mdash mdash mdash
18 ETEC (Ct 15) EAEC (Ct 23) mdash mdash mdash
19 EAEC (Ct 18) Cryptosporidiumparvum (Ct 22) mdash mdash mdash
20 EPEC (Ct 22) Sapovirus (Ct 32) mdash mdash mdash
21 Shigella sppEIEC (Ct12 23 18) EPEC (Ct 19) mdash mdash mdash
22 EPEC (Ct 22) ETEC (Ct 19 19) mdash mdash mdash
23 EPEC (Ct 21) ETEC (Ct 24 29) mdash mdash mdash
thioglycolate broth enrichment with subsequent growthon ESBL selective agar From 12 samples ESBL-positiveEscherichia coli were isolated with proof of more than onestrain in two instances The total number of ESBL-positive Ecoli strainswas 15One of those strainswas identified as EAECby RidaGene PCR An ESBL-positive Klebsiella pneumoniaestrain was isolated from another sample
For the 13 samples containing ESBL-positive Enterobac-teriaceae sensitivity against nonpenicillin noncephalosporinantibiotics was determined by VITEK-II- and E-test-basedresistance testing If several ESBL-positive E coli weresimultaneously isolated the most resistant strain with theresulting highest risk of selection under antibiotic pressurewas chosen Sensitivity for carbapenems tigecycline and
fosfomycin was shown in all 13 cases in 12 for nitrofurantoinwhich is only suitable for urinary tract infections in 11for fluoroquinolones and in 10 for gentamicin Resistanceagainst trimethoprimsulfamethoxazole which is frequentlyencountered in tropical settings was demonstrated in all 13cases
35 Rep-PCR of ESBL-Positive Enterobacteriaceae In total15 E coli strains from 12 patients were subjected to rep-PCR-based DiversiLab typing Within the 95 cutoff rangefor clonal identity three clonal clusters comprising 7 strainsfrom 6 patients were observed (Figure 1) This suggests thepresence of common sources of infection or nosocomial
BioMed Research International 7
10
5
11
4ndash2
3
6ndash1
2
1
12
13
8
4ndash3
7
4ndash1
6ndash2
Similarity ()
Dendrogram Strain Band pattern
10090 958580757065
Figure 1 Dendrogram of the DiversiLab typing results of 15 ESBL-positive E coli strains from 12 patients The strainsrsquo labeling consistsof the patient number (number before the ldquondashrdquo) and the strainnumber in case ofmore than one isolated ESBL-positive E coli strainper patient (number following the ldquondashrdquo) The strain of patient 9 ismissing as the respective ESBL-positive isolate was not E coli butK pneumoniae Three clusters of clonal identity beyond the 95-similarity cutoff (dotted red line) are detectable
transmission within the camp One patient was even colo-nized by E coli strains from two different clusters (Figure 1)For the remaining 8 strains from 6 patients clonal identitywas excluded
36 Clinical and Epidemiological Assessment Clinical datawere provided for 49 patients The completeness of clinicaldata varied missing data are characterized as ldquono datardquo in thetables in the following In those 49 diarrhea patients bacterialpathogens were detected in 34 instances viral pathogens in 12instances and parasitic pathogens in 3 instances No entericpathogen was detectable in 9 out of these 49 patients with theapplied procedures DNA of more than one enteric pathogenwas detectable in 23 of the soldiers with acute diarrhea
361 Age Gender Nationality Sites of Deployment andPrevious Stays in High-Endemicity Regions for Diarrhea-Associated Pathogens No particular distribution pattern ofbacterial viral and parasitic enteric pathogens was observedwith respect to gender and nationality of the soldiers withdiarrhea Soldiers who were younger than 30 years of age
showed coinfections with multiple enteric pathogens lessfrequently than older soldiers Of note all assessed diarrheapatients who were deployed to Bapho were infected by viralpathogens Previous stays in high-endemicity settings did nothave any notable effects on the acquisition of bacterial viraland parasitic pathogens (Table 4)
362 Mode of Food Intake As few as 2 out of 15 diarrheapatients who claimed to have eaten exclusively in the fieldkitchen were free of enteric pathogens in the PCR analysesBacterial pathogens dominated in this group Soldiers whorestricted their diet to hotel food were prone to both bacterialand viral enteric infections There was not a single diarrheapatient in this assessment who had eaten field rations aloneprior to the onset of diarrhea (Table 5)
363 Stool Frequency andConsistency A small proportion of11 patients showed less severe symptomswith fewer than threeunformed stools per day Of note no enteric pathogens weredetected in only one of these patients There was no obviousdistribution pattern of bacterial viral or parasitic pathogensin these less severe diarrhea cases
The observed stool consistency of collected samples asreported by the laboratory technician was considerably lessunformed than the reported stool consistency A total of 13out of 49 stool samples were already hard at the time ofsample collection suggesting that the symptoms had alreadyimproved In contrast no patient reported formed stools tothe field doctor Only 3 out of these 13 formed stools werewithout detectable pathogen DNA at the time of assessment(Table 6)
364 Accompanying Symptoms including Fever Light tomoderate symptoms including nausea and vomiting crampsabdominal pain and flatulence were frequent in the assesseddiarrhea patients Cramps abdominal pain and flatulencewere particularly often detectable in diarrhea patients withbacterial infections while nausea and vomiting were equallylikely for both bacterial and viral infections Only oneinstance of bloody diarrhea was observed in a patient withShigella sppEIEC as the only detectable pathogen in stoolFever was confirmed in only three instances without anydetectable association with a particular pathogen group(Table 7)
Of note the distribution of accompanying symptoms didnot change considerably if only the 34 patients who reportedge3 stools per day were included into the assessment (Table 7)
Only one enteric pathogen per patient was detected in 16patients who reported accompanying symptoms comprising4 cases with STEC 2 cases with EAEC 2 cases with EPEC 2cases with Norovirus G1 2 cases with Norovirus G2 2 caseswith Shigella sppEIEC 1 case withCryptosporidium parvumand 1 case with Rotavirus respectively Bacterial infectionswere associated with a broad distribution of symptoms(Table 7) As expected patients infected with enteroinvasiveShigella sppEIEC showed a particularly wide spectrumof symptoms Norovirus infections and Cryptosporidiumparvum infections were associated with nausea vomiting
8 BioMed Research International
Table 4 Age gender nationality sites of deployment and previous stays in high-endemicity regions for diarrhea-associated pathogens ofdiarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Agelt30 years 1015 615 015 215 51530ndash50 years 1015 315 115 315 815gt50 years 22 12 02 02 22No data 1217 217 217 417 717
GenderMale 3144 1144 344 744 2044Female 35 15 05 25 25
NationalityAustria 11 11 01 01 11Belgium 79 29 19 19 39Colombia 11 01 01 01 01Germany 1725 825 025 425 1225Greece 33 03 13 03 33Ireland 01 01 01 11 01Italy 01 01 01 11 01Portugal 01 01 01 11 01Romania 01 11 01 01 01Spain 44 04 04 04 24SpainBolivia 01 01 01 11 01No data 11 01 11 01 11
Site of deploymentKoulikoro 3141 741 341 641 1941Koulikoro and Bamako 12 12 02 12 12Bamako 01 01 01 11 01Bapho 24 44 04 04 24No data 01 01 01 11 01
Previous stays in high endemicitysettings
Yes 813 313 113 213 413No 2636 936 236 736 1836
and abdominal pain and Norovirus G1 infections also wereassociated with cramps and flatulence (Table 7)
365 Antimalarial Prophylaxis Hygiene Counseling Vacci-nation against Cholera and Typhoid Fever and MedicationLow-dose doxycycline-monohydrate antimalarial prophy-laxis at 100mgday did not provide any protection againstbacterial enteric infections Among the diarrhea patientsunder doxycycline prophylaxis 7 out of 10 were positive forDNA of bacterial enteric pathogens
The vast majority of diarrhea patients were properlycounseled regarding hygiene on tropical deployments andwere vaccinated against typhoid fever Infections with bacte-rial enteric pathogens were particularly frequent in patientswho were vaccinated against cholera and typhoid fever Useof anti-infective drugs was documented for three patients
all three took rifaximin and one in addition metronidazoleDNA of bacterial enteric pathogens was detectable in onlyone of these patients no pathogen DNA was observed in twoof them (Table 8)
4 Discussion
Risk assessment by standardized monitoring and surveil-lance of deployed soldiers in subtropical or tropical coun-tries contributes to evaluation of both individual risk andpreventive measures As previously shown infection riskswith enteric pathogens increase if sophisticated hygieneprecautions regarding food and drinking water cannot bemaintained on military deployments for example in thecase of small missions [3] Considering an average clinicalincidence of diarrhea between 5 and 7 per 100 per month
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
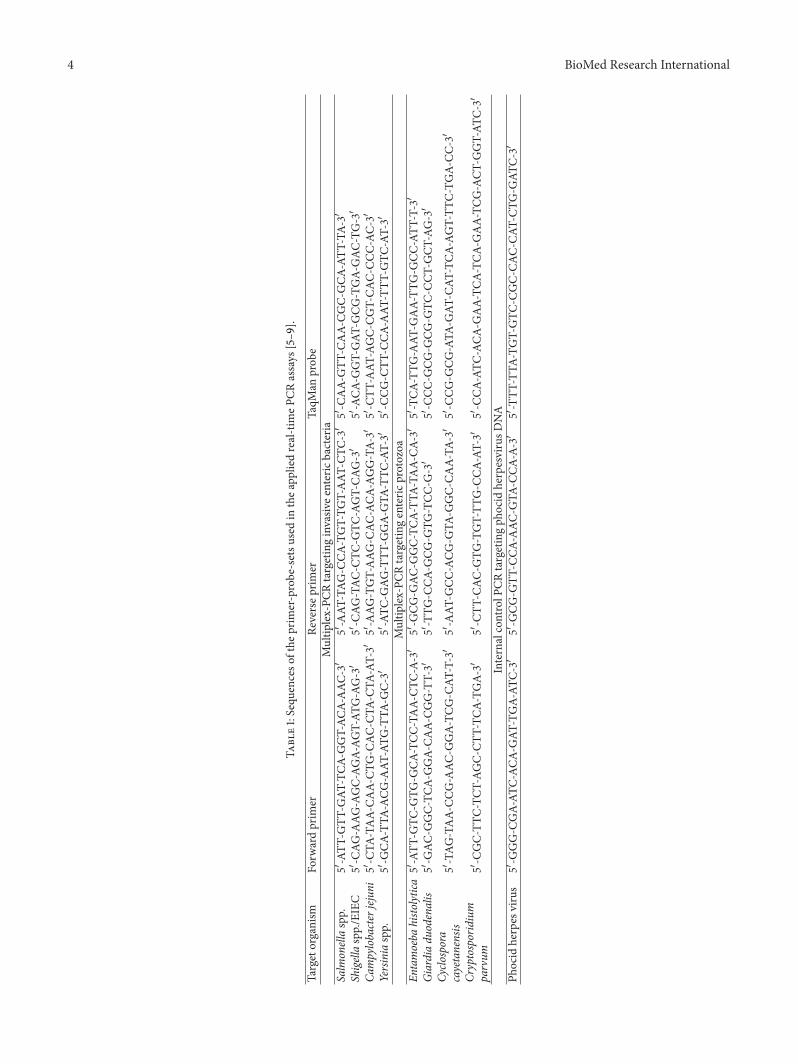
4 BioMed Research International
Table1Sequ
enceso
fthe
prim
er-probe-setsu
sedin
thea
ppliedreal-timeP
CRassays
[5ndash9
]
Targetorganism
Forw
ardprim
erRe
versep
rimer
TaqM
anprob
eMultip
lex-PC
Rtargetinginvasiv
eentericbacteria
Salm
onellaspp
51015840-ATT
-GTT
-GAT
-TCA
-GGT-AC
A-AAC
-31015840
51015840-AAT
-TAG
-CCA
-TGT-TG
T-AAT
-CTC
-31015840
51015840-C
AA-
GTT
-CAA-
CGC-
GCA
-ATT
-TA-
31015840ShigellasppEIEC
51015840-C
AG-AAG
-AGC-AG
A-AG
T-AT
G-AG-31015840
51015840-C
AG-TAC
-CTC
-GTC
-AGT-CA
G-31015840
51015840-ACA
-GGT-GAT
-GCG
-TGA-
GAC
-TG-31015840
Campylobacterjejun
i51015840-C
TA-TAA-
CAA-
CTG-C
AC-C
TA-C
TA-AT-31015840
51015840-AAG
-TGT-AAG
-CAC
-ACA
-AGG-TA-
3101584051015840-C
TT-AAT
-AGC-
CGT-CA
C-CC
C-AC
-31015840
Yersiniaspp
51015840-G
CA-TTA
-ACG
-AAT
-ATG
-TTA
-GC-
3101584051015840-ATC
-GAG
-TTT
-GGA-
GTA
-TTC
-AT-31015840
51015840-C
CG-C
TT-C
CA-AAT
-TTT
-GTC
-AT-31015840
Multip
lex-PC
Rtargetingenteric
protozoa
Entamoeba
histo
lytica
51015840-ATT
-GTC
-GTG
-GCA
-TCC
-TAA-
CTC-A-
3101584051015840-G
CG-G
AC-G
GC-TC
A-TT
A-TA
A-CA
-31015840
51015840-TCA
-TTG
-AAT
-GAA-TT
G-G
CC-ATT
-T-31015840
Giardiadu
odenalis
51015840-G
AC-G
GC-TC
A-GGA-
CAA-
CGG-TT-31015840
51015840-TTG
-CCA
-GCG
-GTG
-TCC
-G-31015840
51015840-C
CC-G
CG-G
CG-G
TC-C
CT-G
CT-AG-31015840
Cyclo
spora
cayetanensis
51015840-TAG
-TAA-
CCG-AAC
-GGA-TC
G-C
AT-T-31015840
51015840-AAT
-GCC
-ACG
-GTA
-GGC-
CAA-TA
-31015840
51015840-C
CG-G
CG-ATA
-GAT
-CAT
-TCA
-AGT-TT
C-TG
A-CC
-31015840
Cryptosporidium
parvum
51015840-C
GC-TT
C-TC
T-AG
C-CT
T-TC
A-TG
A-31015840
51015840-C
TT-C
AC-G
TG-TGT-TT
G-C
CA-AT-31015840
51015840-C
CA-ATC
-ACA
-GAA-TC
A-TC
A-GAA-TC
G-ACT
-GGT-AT
C-31015840
InternalcontrolP
CRtargetingph
ocid
herpesvirusD
NA
Phocid
herpes
virus
51015840-G
GG-C
GA-AT
C-AC
A-GAT
-TGA-AT
C-31015840
51015840-G
CG-G
TT-C
CA-AAC
-GTA
-CCA
-A-31015840
51015840-TTT
-TTA
-TGT-GTC
-CGC-
CAC-
CAT-CT
G-G
ATC-
31015840
BioMed Research International 5
Table 2 Median and mean cycle threshold (Ct) values of pathogens that were detected by PCR
Detected pathogen Median Ct-value Mean Ct-value Standard deviationSalmonella spp 27 27 mdashShigella sppEIEC1 175 18 30Shigella sppEIEC2 135 147 27Shigella sppEIEC3 125 137 24EPEC 22 214 40STEC4 14 159 39STEC5 19 182 43EAEC 19 192 35Giardia duodenalis 255 255 35Cryptosporidium parvum 27 277 60Norovirus G1 20 243 84Norovirus G2 17 166 43Astrovirus 30 30 mdashRotavirus 22 22 mdashSapovirus 32 32 mdash1As detected by in-house PCR 2As detected by RidaGene PCR targeting EHECEPECShigella sppEIEC 3As detected by RidaGene PCR targeting ETEC andShigella sppEIEC 4As detected by PCR targeting the stable toxin 5As detected by PCR targeting the labile toxin
23 Ethics The surveillance described here was ordered asa preventive medical procedure by the German command-ing hygiene officer of the EUTM Mali mission Respectiveorders are legally covered by the self-administrative rightsldquoEigenvollzugskompetenzrdquo of the German Armed ForcesMedical Service regarding infectious disease prevention andcontrol ldquoInfektionsschutzrdquo Collected data were assessedanonymously thus avoiding any violation of sect25 of theDeclaration of Helsinki (DoHOct 2008) or national dataprotection laws ldquoBundesdatenschutzgesetzrdquo
3 Results
31 Frequency of Diarrhea and Coverage Based on thereports of the field doctors to the NATO Deployment HealthSurveillance Capability (DHSC) an average weekly incidenceof diarrhea among EUTM soldiers of 58 patients per weekwas calculated The average number of deployed soldiers atrisk was 480 the resulting average weekly incidence rate per1000 soldiers was 121 During the surveillance period of 37weeks a total of 53 stool samples from 51 EUTM soldiers withdiarrheawere collected resulting in an average of 14 cases perweek Accordingly the coverage of the surveillance was about241 of the registered diarrhea cases
32 Diagnostic Results Positive PCR results for diarrhea-associated pathogens could be detected in 4353 patientsamples The five quantitatively dominating pathogenswere EPEC (119899 = 21) ETEC (119899 = 19) EAEC (119899 = 15)Norovirus (119899 = 10) and ShigellaEIEC (119899 = 6) followed byCryptosporidium parvum (119899 = 3)Giardia duodenalis (119899 = 2)Salmonella spp (119899 = 1) Astrovirus (119899 = 1) Rotavirus(119899 = 1) and Sapovirus (119899 = 1) Of note both detections ofGiardia duodenalis were in the same patient so copy-strainassessment occurred here Median and mean cycle threshold
(Ct) values as well as calculated standard deviations (SD)are given in Table 2 Of note the lowest Ct values weredetected for bacteria Ct-values for Shigella sppEIEC variedconsiderably depending on the primer-probe compositionused with lowest Ct-values in the RidaGene ETECEIEC kitand highest in the in-house approach
DNA of two and more pathogens was detected in 23 ofthe samples of three and more pathogens in 11 samples offour and more pathogens in 2 samples and of as many as fivepathogens in 1 sample Measured Ct values for the respectivecases are given in Table 3 In several cases low Ct-values aremeasured for more than one pathogen
33 Norovirus Genotyping Sequence analysis and genotyp-ing verified the detection of Norovirus GII in six out ofseven initially PCR-positive cases The procedure failed forthe seventh Norovirus GII detection and for all three casespositive for Norovirus GI At least two out of three NorovirusGI-positive cases were confirmed by a separate real-time RT-PCR [17 18] (data not shown)
Genotyping of the six sequenced Norovirus G2 strainsrevealed GIIP7 in four instances Three out of those fourstrains showed identical sequences suggesting either noso-comial transmission or a common source of infection Epi-demiological assessment showed that the respective sampleswere collected from three patients within a single weekmaking a mini-outbreak highly likely In two out of sixinstances Norovirus GIIP16 and GIIP4 var New Orleanswere identified respectively
The underlying sequence information has been depositedand is freely accessible via httpwwwrivmnlmpfnoro-virustypingtooljob1197792283
34 Cultural Approach From 13 out of the 48 analyzed stoolsamples ESBL-positive Enterobacteriaceae were isolated by
6 BioMed Research International
Table 3 Ct-values in cases of multiple pathogen detections (in brackets) If both stable and labile toxin of STEC were detected two Ct-valuesare given otherwise only one In case of Shigella sppEIEC detections three Ct-values are shown reflecting the three applied PCR approachesIn several cases low Ct-values are measured for more than one pathogen
Case Pathogen 1 Pathogen 2 Pathogen 3 Pathogen 4 Pathogen 5
1 Shigella sppEIEC (Ct13 14 16) EPEC (Ct 18) ETEC (Ct 13 16) EAEC (Ct 19) Norovirus G1 (Ct 20)
2 Salmonella spp (Ct 27) EPEC (Ct 15) Norovirus G2 (Ct 11) Astrovirus (Ct 30) mdash
3 EPEC (Ct 29) EAEC (Ct 19) Norovirus G2 (Ct 17) mdash mdash
4 ETEC (Ct 17 20) EAEC (Ct 19) Norovirus G2 (Ct 14) mdash mdash
5 ETEC (Ct 13 20) EAEC (Ct 18) Norovirus G2 (Ct 21) mdash mdash
6 Shigella sppEIEC (Ct12 13 14) EPEC (Ct 21) ETEC (Ct 21) mdash mdash
7 EPEC (Ct 17) ETEC (Ct 20) EAEC (Ct 19) mdash mdash
8 EPEC (Ct 20) ETEC (Ct 13) EAEC (Ct 21) mdash mdash
9 EPEC (Ct 16) ETEC (Ct 13) EAEC (Ct 22) mdash mdash
10 ETEC (Ct 15) EAEC (Ct 15) Cryptosporidiumparvum (Ct 34) mdash mdash
11 EPEC (Ct 23) ETEC (Ct 16 21) EAEC (Ct 22) mdash mdash
12 Shigella sppEIEC (Ct18 20 21) EPEC (Ct 26) mdash mdash mdash
13 EPEC (Ct 28) Giardia duodenalis(Ct 28) mdash mdash mdash
14 EPEC (Ct 21) ETEC (Ct 17) mdash mdash mdash
15 EPEC (Ct 25) ETEC (Ct 12) mdash mdash mdash
16 EPEC (Ct 22) Norovirus G2 (Ct 17) mdash mdash mdash
17 ETEC (Ct 11 18) EAEC (Ct 14) mdash mdash mdash
18 ETEC (Ct 15) EAEC (Ct 23) mdash mdash mdash
19 EAEC (Ct 18) Cryptosporidiumparvum (Ct 22) mdash mdash mdash
20 EPEC (Ct 22) Sapovirus (Ct 32) mdash mdash mdash
21 Shigella sppEIEC (Ct12 23 18) EPEC (Ct 19) mdash mdash mdash
22 EPEC (Ct 22) ETEC (Ct 19 19) mdash mdash mdash
23 EPEC (Ct 21) ETEC (Ct 24 29) mdash mdash mdash
thioglycolate broth enrichment with subsequent growthon ESBL selective agar From 12 samples ESBL-positiveEscherichia coli were isolated with proof of more than onestrain in two instances The total number of ESBL-positive Ecoli strainswas 15One of those strainswas identified as EAECby RidaGene PCR An ESBL-positive Klebsiella pneumoniaestrain was isolated from another sample
For the 13 samples containing ESBL-positive Enterobac-teriaceae sensitivity against nonpenicillin noncephalosporinantibiotics was determined by VITEK-II- and E-test-basedresistance testing If several ESBL-positive E coli weresimultaneously isolated the most resistant strain with theresulting highest risk of selection under antibiotic pressurewas chosen Sensitivity for carbapenems tigecycline and
fosfomycin was shown in all 13 cases in 12 for nitrofurantoinwhich is only suitable for urinary tract infections in 11for fluoroquinolones and in 10 for gentamicin Resistanceagainst trimethoprimsulfamethoxazole which is frequentlyencountered in tropical settings was demonstrated in all 13cases
35 Rep-PCR of ESBL-Positive Enterobacteriaceae In total15 E coli strains from 12 patients were subjected to rep-PCR-based DiversiLab typing Within the 95 cutoff rangefor clonal identity three clonal clusters comprising 7 strainsfrom 6 patients were observed (Figure 1) This suggests thepresence of common sources of infection or nosocomial
BioMed Research International 7
10
5
11
4ndash2
3
6ndash1
2
1
12
13
8
4ndash3
7
4ndash1
6ndash2
Similarity ()
Dendrogram Strain Band pattern
10090 958580757065
Figure 1 Dendrogram of the DiversiLab typing results of 15 ESBL-positive E coli strains from 12 patients The strainsrsquo labeling consistsof the patient number (number before the ldquondashrdquo) and the strainnumber in case ofmore than one isolated ESBL-positive E coli strainper patient (number following the ldquondashrdquo) The strain of patient 9 ismissing as the respective ESBL-positive isolate was not E coli butK pneumoniae Three clusters of clonal identity beyond the 95-similarity cutoff (dotted red line) are detectable
transmission within the camp One patient was even colo-nized by E coli strains from two different clusters (Figure 1)For the remaining 8 strains from 6 patients clonal identitywas excluded
36 Clinical and Epidemiological Assessment Clinical datawere provided for 49 patients The completeness of clinicaldata varied missing data are characterized as ldquono datardquo in thetables in the following In those 49 diarrhea patients bacterialpathogens were detected in 34 instances viral pathogens in 12instances and parasitic pathogens in 3 instances No entericpathogen was detectable in 9 out of these 49 patients with theapplied procedures DNA of more than one enteric pathogenwas detectable in 23 of the soldiers with acute diarrhea
361 Age Gender Nationality Sites of Deployment andPrevious Stays in High-Endemicity Regions for Diarrhea-Associated Pathogens No particular distribution pattern ofbacterial viral and parasitic enteric pathogens was observedwith respect to gender and nationality of the soldiers withdiarrhea Soldiers who were younger than 30 years of age
showed coinfections with multiple enteric pathogens lessfrequently than older soldiers Of note all assessed diarrheapatients who were deployed to Bapho were infected by viralpathogens Previous stays in high-endemicity settings did nothave any notable effects on the acquisition of bacterial viraland parasitic pathogens (Table 4)
362 Mode of Food Intake As few as 2 out of 15 diarrheapatients who claimed to have eaten exclusively in the fieldkitchen were free of enteric pathogens in the PCR analysesBacterial pathogens dominated in this group Soldiers whorestricted their diet to hotel food were prone to both bacterialand viral enteric infections There was not a single diarrheapatient in this assessment who had eaten field rations aloneprior to the onset of diarrhea (Table 5)
363 Stool Frequency andConsistency A small proportion of11 patients showed less severe symptomswith fewer than threeunformed stools per day Of note no enteric pathogens weredetected in only one of these patients There was no obviousdistribution pattern of bacterial viral or parasitic pathogensin these less severe diarrhea cases
The observed stool consistency of collected samples asreported by the laboratory technician was considerably lessunformed than the reported stool consistency A total of 13out of 49 stool samples were already hard at the time ofsample collection suggesting that the symptoms had alreadyimproved In contrast no patient reported formed stools tothe field doctor Only 3 out of these 13 formed stools werewithout detectable pathogen DNA at the time of assessment(Table 6)
364 Accompanying Symptoms including Fever Light tomoderate symptoms including nausea and vomiting crampsabdominal pain and flatulence were frequent in the assesseddiarrhea patients Cramps abdominal pain and flatulencewere particularly often detectable in diarrhea patients withbacterial infections while nausea and vomiting were equallylikely for both bacterial and viral infections Only oneinstance of bloody diarrhea was observed in a patient withShigella sppEIEC as the only detectable pathogen in stoolFever was confirmed in only three instances without anydetectable association with a particular pathogen group(Table 7)
Of note the distribution of accompanying symptoms didnot change considerably if only the 34 patients who reportedge3 stools per day were included into the assessment (Table 7)
Only one enteric pathogen per patient was detected in 16patients who reported accompanying symptoms comprising4 cases with STEC 2 cases with EAEC 2 cases with EPEC 2cases with Norovirus G1 2 cases with Norovirus G2 2 caseswith Shigella sppEIEC 1 case withCryptosporidium parvumand 1 case with Rotavirus respectively Bacterial infectionswere associated with a broad distribution of symptoms(Table 7) As expected patients infected with enteroinvasiveShigella sppEIEC showed a particularly wide spectrumof symptoms Norovirus infections and Cryptosporidiumparvum infections were associated with nausea vomiting
8 BioMed Research International
Table 4 Age gender nationality sites of deployment and previous stays in high-endemicity regions for diarrhea-associated pathogens ofdiarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Agelt30 years 1015 615 015 215 51530ndash50 years 1015 315 115 315 815gt50 years 22 12 02 02 22No data 1217 217 217 417 717
GenderMale 3144 1144 344 744 2044Female 35 15 05 25 25
NationalityAustria 11 11 01 01 11Belgium 79 29 19 19 39Colombia 11 01 01 01 01Germany 1725 825 025 425 1225Greece 33 03 13 03 33Ireland 01 01 01 11 01Italy 01 01 01 11 01Portugal 01 01 01 11 01Romania 01 11 01 01 01Spain 44 04 04 04 24SpainBolivia 01 01 01 11 01No data 11 01 11 01 11
Site of deploymentKoulikoro 3141 741 341 641 1941Koulikoro and Bamako 12 12 02 12 12Bamako 01 01 01 11 01Bapho 24 44 04 04 24No data 01 01 01 11 01
Previous stays in high endemicitysettings
Yes 813 313 113 213 413No 2636 936 236 736 1836
and abdominal pain and Norovirus G1 infections also wereassociated with cramps and flatulence (Table 7)
365 Antimalarial Prophylaxis Hygiene Counseling Vacci-nation against Cholera and Typhoid Fever and MedicationLow-dose doxycycline-monohydrate antimalarial prophy-laxis at 100mgday did not provide any protection againstbacterial enteric infections Among the diarrhea patientsunder doxycycline prophylaxis 7 out of 10 were positive forDNA of bacterial enteric pathogens
The vast majority of diarrhea patients were properlycounseled regarding hygiene on tropical deployments andwere vaccinated against typhoid fever Infections with bacte-rial enteric pathogens were particularly frequent in patientswho were vaccinated against cholera and typhoid fever Useof anti-infective drugs was documented for three patients
all three took rifaximin and one in addition metronidazoleDNA of bacterial enteric pathogens was detectable in onlyone of these patients no pathogen DNA was observed in twoof them (Table 8)
4 Discussion
Risk assessment by standardized monitoring and surveil-lance of deployed soldiers in subtropical or tropical coun-tries contributes to evaluation of both individual risk andpreventive measures As previously shown infection riskswith enteric pathogens increase if sophisticated hygieneprecautions regarding food and drinking water cannot bemaintained on military deployments for example in thecase of small missions [3] Considering an average clinicalincidence of diarrhea between 5 and 7 per 100 per month
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 5
Table 2 Median and mean cycle threshold (Ct) values of pathogens that were detected by PCR
Detected pathogen Median Ct-value Mean Ct-value Standard deviationSalmonella spp 27 27 mdashShigella sppEIEC1 175 18 30Shigella sppEIEC2 135 147 27Shigella sppEIEC3 125 137 24EPEC 22 214 40STEC4 14 159 39STEC5 19 182 43EAEC 19 192 35Giardia duodenalis 255 255 35Cryptosporidium parvum 27 277 60Norovirus G1 20 243 84Norovirus G2 17 166 43Astrovirus 30 30 mdashRotavirus 22 22 mdashSapovirus 32 32 mdash1As detected by in-house PCR 2As detected by RidaGene PCR targeting EHECEPECShigella sppEIEC 3As detected by RidaGene PCR targeting ETEC andShigella sppEIEC 4As detected by PCR targeting the stable toxin 5As detected by PCR targeting the labile toxin
23 Ethics The surveillance described here was ordered asa preventive medical procedure by the German command-ing hygiene officer of the EUTM Mali mission Respectiveorders are legally covered by the self-administrative rightsldquoEigenvollzugskompetenzrdquo of the German Armed ForcesMedical Service regarding infectious disease prevention andcontrol ldquoInfektionsschutzrdquo Collected data were assessedanonymously thus avoiding any violation of sect25 of theDeclaration of Helsinki (DoHOct 2008) or national dataprotection laws ldquoBundesdatenschutzgesetzrdquo
3 Results
31 Frequency of Diarrhea and Coverage Based on thereports of the field doctors to the NATO Deployment HealthSurveillance Capability (DHSC) an average weekly incidenceof diarrhea among EUTM soldiers of 58 patients per weekwas calculated The average number of deployed soldiers atrisk was 480 the resulting average weekly incidence rate per1000 soldiers was 121 During the surveillance period of 37weeks a total of 53 stool samples from 51 EUTM soldiers withdiarrheawere collected resulting in an average of 14 cases perweek Accordingly the coverage of the surveillance was about241 of the registered diarrhea cases
32 Diagnostic Results Positive PCR results for diarrhea-associated pathogens could be detected in 4353 patientsamples The five quantitatively dominating pathogenswere EPEC (119899 = 21) ETEC (119899 = 19) EAEC (119899 = 15)Norovirus (119899 = 10) and ShigellaEIEC (119899 = 6) followed byCryptosporidium parvum (119899 = 3)Giardia duodenalis (119899 = 2)Salmonella spp (119899 = 1) Astrovirus (119899 = 1) Rotavirus(119899 = 1) and Sapovirus (119899 = 1) Of note both detections ofGiardia duodenalis were in the same patient so copy-strainassessment occurred here Median and mean cycle threshold
(Ct) values as well as calculated standard deviations (SD)are given in Table 2 Of note the lowest Ct values weredetected for bacteria Ct-values for Shigella sppEIEC variedconsiderably depending on the primer-probe compositionused with lowest Ct-values in the RidaGene ETECEIEC kitand highest in the in-house approach
DNA of two and more pathogens was detected in 23 ofthe samples of three and more pathogens in 11 samples offour and more pathogens in 2 samples and of as many as fivepathogens in 1 sample Measured Ct values for the respectivecases are given in Table 3 In several cases low Ct-values aremeasured for more than one pathogen
33 Norovirus Genotyping Sequence analysis and genotyp-ing verified the detection of Norovirus GII in six out ofseven initially PCR-positive cases The procedure failed forthe seventh Norovirus GII detection and for all three casespositive for Norovirus GI At least two out of three NorovirusGI-positive cases were confirmed by a separate real-time RT-PCR [17 18] (data not shown)
Genotyping of the six sequenced Norovirus G2 strainsrevealed GIIP7 in four instances Three out of those fourstrains showed identical sequences suggesting either noso-comial transmission or a common source of infection Epi-demiological assessment showed that the respective sampleswere collected from three patients within a single weekmaking a mini-outbreak highly likely In two out of sixinstances Norovirus GIIP16 and GIIP4 var New Orleanswere identified respectively
The underlying sequence information has been depositedand is freely accessible via httpwwwrivmnlmpfnoro-virustypingtooljob1197792283
34 Cultural Approach From 13 out of the 48 analyzed stoolsamples ESBL-positive Enterobacteriaceae were isolated by
6 BioMed Research International
Table 3 Ct-values in cases of multiple pathogen detections (in brackets) If both stable and labile toxin of STEC were detected two Ct-valuesare given otherwise only one In case of Shigella sppEIEC detections three Ct-values are shown reflecting the three applied PCR approachesIn several cases low Ct-values are measured for more than one pathogen
Case Pathogen 1 Pathogen 2 Pathogen 3 Pathogen 4 Pathogen 5
1 Shigella sppEIEC (Ct13 14 16) EPEC (Ct 18) ETEC (Ct 13 16) EAEC (Ct 19) Norovirus G1 (Ct 20)
2 Salmonella spp (Ct 27) EPEC (Ct 15) Norovirus G2 (Ct 11) Astrovirus (Ct 30) mdash
3 EPEC (Ct 29) EAEC (Ct 19) Norovirus G2 (Ct 17) mdash mdash
4 ETEC (Ct 17 20) EAEC (Ct 19) Norovirus G2 (Ct 14) mdash mdash
5 ETEC (Ct 13 20) EAEC (Ct 18) Norovirus G2 (Ct 21) mdash mdash
6 Shigella sppEIEC (Ct12 13 14) EPEC (Ct 21) ETEC (Ct 21) mdash mdash
7 EPEC (Ct 17) ETEC (Ct 20) EAEC (Ct 19) mdash mdash
8 EPEC (Ct 20) ETEC (Ct 13) EAEC (Ct 21) mdash mdash
9 EPEC (Ct 16) ETEC (Ct 13) EAEC (Ct 22) mdash mdash
10 ETEC (Ct 15) EAEC (Ct 15) Cryptosporidiumparvum (Ct 34) mdash mdash
11 EPEC (Ct 23) ETEC (Ct 16 21) EAEC (Ct 22) mdash mdash
12 Shigella sppEIEC (Ct18 20 21) EPEC (Ct 26) mdash mdash mdash
13 EPEC (Ct 28) Giardia duodenalis(Ct 28) mdash mdash mdash
14 EPEC (Ct 21) ETEC (Ct 17) mdash mdash mdash
15 EPEC (Ct 25) ETEC (Ct 12) mdash mdash mdash
16 EPEC (Ct 22) Norovirus G2 (Ct 17) mdash mdash mdash
17 ETEC (Ct 11 18) EAEC (Ct 14) mdash mdash mdash
18 ETEC (Ct 15) EAEC (Ct 23) mdash mdash mdash
19 EAEC (Ct 18) Cryptosporidiumparvum (Ct 22) mdash mdash mdash
20 EPEC (Ct 22) Sapovirus (Ct 32) mdash mdash mdash
21 Shigella sppEIEC (Ct12 23 18) EPEC (Ct 19) mdash mdash mdash
22 EPEC (Ct 22) ETEC (Ct 19 19) mdash mdash mdash
23 EPEC (Ct 21) ETEC (Ct 24 29) mdash mdash mdash
thioglycolate broth enrichment with subsequent growthon ESBL selective agar From 12 samples ESBL-positiveEscherichia coli were isolated with proof of more than onestrain in two instances The total number of ESBL-positive Ecoli strainswas 15One of those strainswas identified as EAECby RidaGene PCR An ESBL-positive Klebsiella pneumoniaestrain was isolated from another sample
For the 13 samples containing ESBL-positive Enterobac-teriaceae sensitivity against nonpenicillin noncephalosporinantibiotics was determined by VITEK-II- and E-test-basedresistance testing If several ESBL-positive E coli weresimultaneously isolated the most resistant strain with theresulting highest risk of selection under antibiotic pressurewas chosen Sensitivity for carbapenems tigecycline and
fosfomycin was shown in all 13 cases in 12 for nitrofurantoinwhich is only suitable for urinary tract infections in 11for fluoroquinolones and in 10 for gentamicin Resistanceagainst trimethoprimsulfamethoxazole which is frequentlyencountered in tropical settings was demonstrated in all 13cases
35 Rep-PCR of ESBL-Positive Enterobacteriaceae In total15 E coli strains from 12 patients were subjected to rep-PCR-based DiversiLab typing Within the 95 cutoff rangefor clonal identity three clonal clusters comprising 7 strainsfrom 6 patients were observed (Figure 1) This suggests thepresence of common sources of infection or nosocomial
BioMed Research International 7
10
5
11
4ndash2
3
6ndash1
2
1
12
13
8
4ndash3
7
4ndash1
6ndash2
Similarity ()
Dendrogram Strain Band pattern
10090 958580757065
Figure 1 Dendrogram of the DiversiLab typing results of 15 ESBL-positive E coli strains from 12 patients The strainsrsquo labeling consistsof the patient number (number before the ldquondashrdquo) and the strainnumber in case ofmore than one isolated ESBL-positive E coli strainper patient (number following the ldquondashrdquo) The strain of patient 9 ismissing as the respective ESBL-positive isolate was not E coli butK pneumoniae Three clusters of clonal identity beyond the 95-similarity cutoff (dotted red line) are detectable
transmission within the camp One patient was even colo-nized by E coli strains from two different clusters (Figure 1)For the remaining 8 strains from 6 patients clonal identitywas excluded
36 Clinical and Epidemiological Assessment Clinical datawere provided for 49 patients The completeness of clinicaldata varied missing data are characterized as ldquono datardquo in thetables in the following In those 49 diarrhea patients bacterialpathogens were detected in 34 instances viral pathogens in 12instances and parasitic pathogens in 3 instances No entericpathogen was detectable in 9 out of these 49 patients with theapplied procedures DNA of more than one enteric pathogenwas detectable in 23 of the soldiers with acute diarrhea
361 Age Gender Nationality Sites of Deployment andPrevious Stays in High-Endemicity Regions for Diarrhea-Associated Pathogens No particular distribution pattern ofbacterial viral and parasitic enteric pathogens was observedwith respect to gender and nationality of the soldiers withdiarrhea Soldiers who were younger than 30 years of age
showed coinfections with multiple enteric pathogens lessfrequently than older soldiers Of note all assessed diarrheapatients who were deployed to Bapho were infected by viralpathogens Previous stays in high-endemicity settings did nothave any notable effects on the acquisition of bacterial viraland parasitic pathogens (Table 4)
362 Mode of Food Intake As few as 2 out of 15 diarrheapatients who claimed to have eaten exclusively in the fieldkitchen were free of enteric pathogens in the PCR analysesBacterial pathogens dominated in this group Soldiers whorestricted their diet to hotel food were prone to both bacterialand viral enteric infections There was not a single diarrheapatient in this assessment who had eaten field rations aloneprior to the onset of diarrhea (Table 5)
363 Stool Frequency andConsistency A small proportion of11 patients showed less severe symptomswith fewer than threeunformed stools per day Of note no enteric pathogens weredetected in only one of these patients There was no obviousdistribution pattern of bacterial viral or parasitic pathogensin these less severe diarrhea cases
The observed stool consistency of collected samples asreported by the laboratory technician was considerably lessunformed than the reported stool consistency A total of 13out of 49 stool samples were already hard at the time ofsample collection suggesting that the symptoms had alreadyimproved In contrast no patient reported formed stools tothe field doctor Only 3 out of these 13 formed stools werewithout detectable pathogen DNA at the time of assessment(Table 6)
364 Accompanying Symptoms including Fever Light tomoderate symptoms including nausea and vomiting crampsabdominal pain and flatulence were frequent in the assesseddiarrhea patients Cramps abdominal pain and flatulencewere particularly often detectable in diarrhea patients withbacterial infections while nausea and vomiting were equallylikely for both bacterial and viral infections Only oneinstance of bloody diarrhea was observed in a patient withShigella sppEIEC as the only detectable pathogen in stoolFever was confirmed in only three instances without anydetectable association with a particular pathogen group(Table 7)
Of note the distribution of accompanying symptoms didnot change considerably if only the 34 patients who reportedge3 stools per day were included into the assessment (Table 7)
Only one enteric pathogen per patient was detected in 16patients who reported accompanying symptoms comprising4 cases with STEC 2 cases with EAEC 2 cases with EPEC 2cases with Norovirus G1 2 cases with Norovirus G2 2 caseswith Shigella sppEIEC 1 case withCryptosporidium parvumand 1 case with Rotavirus respectively Bacterial infectionswere associated with a broad distribution of symptoms(Table 7) As expected patients infected with enteroinvasiveShigella sppEIEC showed a particularly wide spectrumof symptoms Norovirus infections and Cryptosporidiumparvum infections were associated with nausea vomiting
8 BioMed Research International
Table 4 Age gender nationality sites of deployment and previous stays in high-endemicity regions for diarrhea-associated pathogens ofdiarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Agelt30 years 1015 615 015 215 51530ndash50 years 1015 315 115 315 815gt50 years 22 12 02 02 22No data 1217 217 217 417 717
GenderMale 3144 1144 344 744 2044Female 35 15 05 25 25
NationalityAustria 11 11 01 01 11Belgium 79 29 19 19 39Colombia 11 01 01 01 01Germany 1725 825 025 425 1225Greece 33 03 13 03 33Ireland 01 01 01 11 01Italy 01 01 01 11 01Portugal 01 01 01 11 01Romania 01 11 01 01 01Spain 44 04 04 04 24SpainBolivia 01 01 01 11 01No data 11 01 11 01 11
Site of deploymentKoulikoro 3141 741 341 641 1941Koulikoro and Bamako 12 12 02 12 12Bamako 01 01 01 11 01Bapho 24 44 04 04 24No data 01 01 01 11 01
Previous stays in high endemicitysettings
Yes 813 313 113 213 413No 2636 936 236 736 1836
and abdominal pain and Norovirus G1 infections also wereassociated with cramps and flatulence (Table 7)
365 Antimalarial Prophylaxis Hygiene Counseling Vacci-nation against Cholera and Typhoid Fever and MedicationLow-dose doxycycline-monohydrate antimalarial prophy-laxis at 100mgday did not provide any protection againstbacterial enteric infections Among the diarrhea patientsunder doxycycline prophylaxis 7 out of 10 were positive forDNA of bacterial enteric pathogens
The vast majority of diarrhea patients were properlycounseled regarding hygiene on tropical deployments andwere vaccinated against typhoid fever Infections with bacte-rial enteric pathogens were particularly frequent in patientswho were vaccinated against cholera and typhoid fever Useof anti-infective drugs was documented for three patients
all three took rifaximin and one in addition metronidazoleDNA of bacterial enteric pathogens was detectable in onlyone of these patients no pathogen DNA was observed in twoof them (Table 8)
4 Discussion
Risk assessment by standardized monitoring and surveil-lance of deployed soldiers in subtropical or tropical coun-tries contributes to evaluation of both individual risk andpreventive measures As previously shown infection riskswith enteric pathogens increase if sophisticated hygieneprecautions regarding food and drinking water cannot bemaintained on military deployments for example in thecase of small missions [3] Considering an average clinicalincidence of diarrhea between 5 and 7 per 100 per month
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
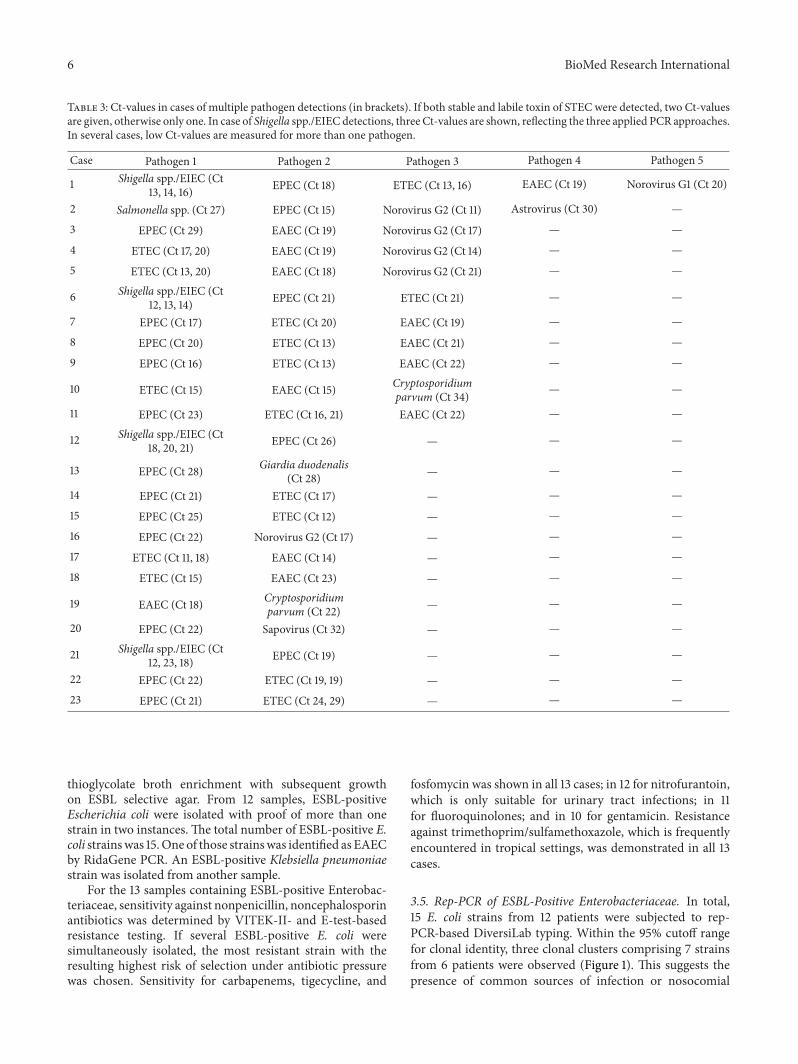
6 BioMed Research International
Table 3 Ct-values in cases of multiple pathogen detections (in brackets) If both stable and labile toxin of STEC were detected two Ct-valuesare given otherwise only one In case of Shigella sppEIEC detections three Ct-values are shown reflecting the three applied PCR approachesIn several cases low Ct-values are measured for more than one pathogen
Case Pathogen 1 Pathogen 2 Pathogen 3 Pathogen 4 Pathogen 5
1 Shigella sppEIEC (Ct13 14 16) EPEC (Ct 18) ETEC (Ct 13 16) EAEC (Ct 19) Norovirus G1 (Ct 20)
2 Salmonella spp (Ct 27) EPEC (Ct 15) Norovirus G2 (Ct 11) Astrovirus (Ct 30) mdash
3 EPEC (Ct 29) EAEC (Ct 19) Norovirus G2 (Ct 17) mdash mdash
4 ETEC (Ct 17 20) EAEC (Ct 19) Norovirus G2 (Ct 14) mdash mdash
5 ETEC (Ct 13 20) EAEC (Ct 18) Norovirus G2 (Ct 21) mdash mdash
6 Shigella sppEIEC (Ct12 13 14) EPEC (Ct 21) ETEC (Ct 21) mdash mdash
7 EPEC (Ct 17) ETEC (Ct 20) EAEC (Ct 19) mdash mdash
8 EPEC (Ct 20) ETEC (Ct 13) EAEC (Ct 21) mdash mdash
9 EPEC (Ct 16) ETEC (Ct 13) EAEC (Ct 22) mdash mdash
10 ETEC (Ct 15) EAEC (Ct 15) Cryptosporidiumparvum (Ct 34) mdash mdash
11 EPEC (Ct 23) ETEC (Ct 16 21) EAEC (Ct 22) mdash mdash
12 Shigella sppEIEC (Ct18 20 21) EPEC (Ct 26) mdash mdash mdash
13 EPEC (Ct 28) Giardia duodenalis(Ct 28) mdash mdash mdash
14 EPEC (Ct 21) ETEC (Ct 17) mdash mdash mdash
15 EPEC (Ct 25) ETEC (Ct 12) mdash mdash mdash
16 EPEC (Ct 22) Norovirus G2 (Ct 17) mdash mdash mdash
17 ETEC (Ct 11 18) EAEC (Ct 14) mdash mdash mdash
18 ETEC (Ct 15) EAEC (Ct 23) mdash mdash mdash
19 EAEC (Ct 18) Cryptosporidiumparvum (Ct 22) mdash mdash mdash
20 EPEC (Ct 22) Sapovirus (Ct 32) mdash mdash mdash
21 Shigella sppEIEC (Ct12 23 18) EPEC (Ct 19) mdash mdash mdash
22 EPEC (Ct 22) ETEC (Ct 19 19) mdash mdash mdash
23 EPEC (Ct 21) ETEC (Ct 24 29) mdash mdash mdash
thioglycolate broth enrichment with subsequent growthon ESBL selective agar From 12 samples ESBL-positiveEscherichia coli were isolated with proof of more than onestrain in two instances The total number of ESBL-positive Ecoli strainswas 15One of those strainswas identified as EAECby RidaGene PCR An ESBL-positive Klebsiella pneumoniaestrain was isolated from another sample
For the 13 samples containing ESBL-positive Enterobac-teriaceae sensitivity against nonpenicillin noncephalosporinantibiotics was determined by VITEK-II- and E-test-basedresistance testing If several ESBL-positive E coli weresimultaneously isolated the most resistant strain with theresulting highest risk of selection under antibiotic pressurewas chosen Sensitivity for carbapenems tigecycline and
fosfomycin was shown in all 13 cases in 12 for nitrofurantoinwhich is only suitable for urinary tract infections in 11for fluoroquinolones and in 10 for gentamicin Resistanceagainst trimethoprimsulfamethoxazole which is frequentlyencountered in tropical settings was demonstrated in all 13cases
35 Rep-PCR of ESBL-Positive Enterobacteriaceae In total15 E coli strains from 12 patients were subjected to rep-PCR-based DiversiLab typing Within the 95 cutoff rangefor clonal identity three clonal clusters comprising 7 strainsfrom 6 patients were observed (Figure 1) This suggests thepresence of common sources of infection or nosocomial
BioMed Research International 7
10
5
11
4ndash2
3
6ndash1
2
1
12
13
8
4ndash3
7
4ndash1
6ndash2
Similarity ()
Dendrogram Strain Band pattern
10090 958580757065
Figure 1 Dendrogram of the DiversiLab typing results of 15 ESBL-positive E coli strains from 12 patients The strainsrsquo labeling consistsof the patient number (number before the ldquondashrdquo) and the strainnumber in case ofmore than one isolated ESBL-positive E coli strainper patient (number following the ldquondashrdquo) The strain of patient 9 ismissing as the respective ESBL-positive isolate was not E coli butK pneumoniae Three clusters of clonal identity beyond the 95-similarity cutoff (dotted red line) are detectable
transmission within the camp One patient was even colo-nized by E coli strains from two different clusters (Figure 1)For the remaining 8 strains from 6 patients clonal identitywas excluded
36 Clinical and Epidemiological Assessment Clinical datawere provided for 49 patients The completeness of clinicaldata varied missing data are characterized as ldquono datardquo in thetables in the following In those 49 diarrhea patients bacterialpathogens were detected in 34 instances viral pathogens in 12instances and parasitic pathogens in 3 instances No entericpathogen was detectable in 9 out of these 49 patients with theapplied procedures DNA of more than one enteric pathogenwas detectable in 23 of the soldiers with acute diarrhea
361 Age Gender Nationality Sites of Deployment andPrevious Stays in High-Endemicity Regions for Diarrhea-Associated Pathogens No particular distribution pattern ofbacterial viral and parasitic enteric pathogens was observedwith respect to gender and nationality of the soldiers withdiarrhea Soldiers who were younger than 30 years of age
showed coinfections with multiple enteric pathogens lessfrequently than older soldiers Of note all assessed diarrheapatients who were deployed to Bapho were infected by viralpathogens Previous stays in high-endemicity settings did nothave any notable effects on the acquisition of bacterial viraland parasitic pathogens (Table 4)
362 Mode of Food Intake As few as 2 out of 15 diarrheapatients who claimed to have eaten exclusively in the fieldkitchen were free of enteric pathogens in the PCR analysesBacterial pathogens dominated in this group Soldiers whorestricted their diet to hotel food were prone to both bacterialand viral enteric infections There was not a single diarrheapatient in this assessment who had eaten field rations aloneprior to the onset of diarrhea (Table 5)
363 Stool Frequency andConsistency A small proportion of11 patients showed less severe symptomswith fewer than threeunformed stools per day Of note no enteric pathogens weredetected in only one of these patients There was no obviousdistribution pattern of bacterial viral or parasitic pathogensin these less severe diarrhea cases
The observed stool consistency of collected samples asreported by the laboratory technician was considerably lessunformed than the reported stool consistency A total of 13out of 49 stool samples were already hard at the time ofsample collection suggesting that the symptoms had alreadyimproved In contrast no patient reported formed stools tothe field doctor Only 3 out of these 13 formed stools werewithout detectable pathogen DNA at the time of assessment(Table 6)
364 Accompanying Symptoms including Fever Light tomoderate symptoms including nausea and vomiting crampsabdominal pain and flatulence were frequent in the assesseddiarrhea patients Cramps abdominal pain and flatulencewere particularly often detectable in diarrhea patients withbacterial infections while nausea and vomiting were equallylikely for both bacterial and viral infections Only oneinstance of bloody diarrhea was observed in a patient withShigella sppEIEC as the only detectable pathogen in stoolFever was confirmed in only three instances without anydetectable association with a particular pathogen group(Table 7)
Of note the distribution of accompanying symptoms didnot change considerably if only the 34 patients who reportedge3 stools per day were included into the assessment (Table 7)
Only one enteric pathogen per patient was detected in 16patients who reported accompanying symptoms comprising4 cases with STEC 2 cases with EAEC 2 cases with EPEC 2cases with Norovirus G1 2 cases with Norovirus G2 2 caseswith Shigella sppEIEC 1 case withCryptosporidium parvumand 1 case with Rotavirus respectively Bacterial infectionswere associated with a broad distribution of symptoms(Table 7) As expected patients infected with enteroinvasiveShigella sppEIEC showed a particularly wide spectrumof symptoms Norovirus infections and Cryptosporidiumparvum infections were associated with nausea vomiting
8 BioMed Research International
Table 4 Age gender nationality sites of deployment and previous stays in high-endemicity regions for diarrhea-associated pathogens ofdiarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Agelt30 years 1015 615 015 215 51530ndash50 years 1015 315 115 315 815gt50 years 22 12 02 02 22No data 1217 217 217 417 717
GenderMale 3144 1144 344 744 2044Female 35 15 05 25 25
NationalityAustria 11 11 01 01 11Belgium 79 29 19 19 39Colombia 11 01 01 01 01Germany 1725 825 025 425 1225Greece 33 03 13 03 33Ireland 01 01 01 11 01Italy 01 01 01 11 01Portugal 01 01 01 11 01Romania 01 11 01 01 01Spain 44 04 04 04 24SpainBolivia 01 01 01 11 01No data 11 01 11 01 11
Site of deploymentKoulikoro 3141 741 341 641 1941Koulikoro and Bamako 12 12 02 12 12Bamako 01 01 01 11 01Bapho 24 44 04 04 24No data 01 01 01 11 01
Previous stays in high endemicitysettings
Yes 813 313 113 213 413No 2636 936 236 736 1836
and abdominal pain and Norovirus G1 infections also wereassociated with cramps and flatulence (Table 7)
365 Antimalarial Prophylaxis Hygiene Counseling Vacci-nation against Cholera and Typhoid Fever and MedicationLow-dose doxycycline-monohydrate antimalarial prophy-laxis at 100mgday did not provide any protection againstbacterial enteric infections Among the diarrhea patientsunder doxycycline prophylaxis 7 out of 10 were positive forDNA of bacterial enteric pathogens
The vast majority of diarrhea patients were properlycounseled regarding hygiene on tropical deployments andwere vaccinated against typhoid fever Infections with bacte-rial enteric pathogens were particularly frequent in patientswho were vaccinated against cholera and typhoid fever Useof anti-infective drugs was documented for three patients
all three took rifaximin and one in addition metronidazoleDNA of bacterial enteric pathogens was detectable in onlyone of these patients no pathogen DNA was observed in twoof them (Table 8)
4 Discussion
Risk assessment by standardized monitoring and surveil-lance of deployed soldiers in subtropical or tropical coun-tries contributes to evaluation of both individual risk andpreventive measures As previously shown infection riskswith enteric pathogens increase if sophisticated hygieneprecautions regarding food and drinking water cannot bemaintained on military deployments for example in thecase of small missions [3] Considering an average clinicalincidence of diarrhea between 5 and 7 per 100 per month
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
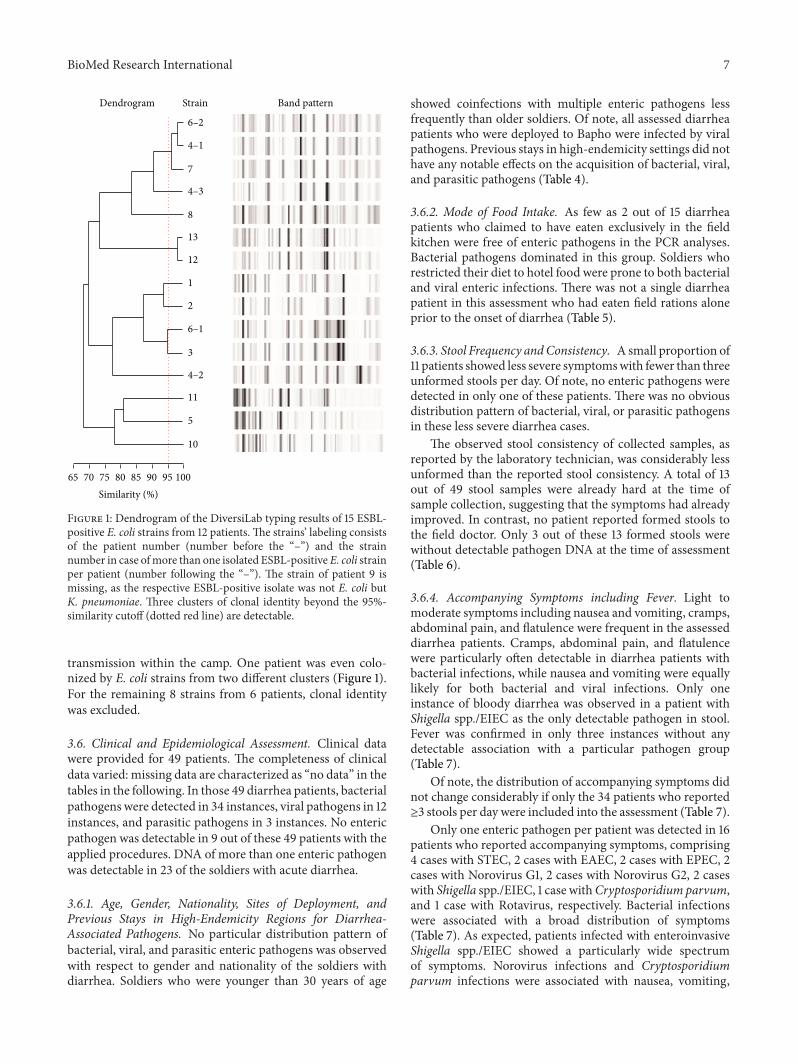
BioMed Research International 7
10
5
11
4ndash2
3
6ndash1
2
1
12
13
8
4ndash3
7
4ndash1
6ndash2
Similarity ()
Dendrogram Strain Band pattern
10090 958580757065
Figure 1 Dendrogram of the DiversiLab typing results of 15 ESBL-positive E coli strains from 12 patients The strainsrsquo labeling consistsof the patient number (number before the ldquondashrdquo) and the strainnumber in case ofmore than one isolated ESBL-positive E coli strainper patient (number following the ldquondashrdquo) The strain of patient 9 ismissing as the respective ESBL-positive isolate was not E coli butK pneumoniae Three clusters of clonal identity beyond the 95-similarity cutoff (dotted red line) are detectable
transmission within the camp One patient was even colo-nized by E coli strains from two different clusters (Figure 1)For the remaining 8 strains from 6 patients clonal identitywas excluded
36 Clinical and Epidemiological Assessment Clinical datawere provided for 49 patients The completeness of clinicaldata varied missing data are characterized as ldquono datardquo in thetables in the following In those 49 diarrhea patients bacterialpathogens were detected in 34 instances viral pathogens in 12instances and parasitic pathogens in 3 instances No entericpathogen was detectable in 9 out of these 49 patients with theapplied procedures DNA of more than one enteric pathogenwas detectable in 23 of the soldiers with acute diarrhea
361 Age Gender Nationality Sites of Deployment andPrevious Stays in High-Endemicity Regions for Diarrhea-Associated Pathogens No particular distribution pattern ofbacterial viral and parasitic enteric pathogens was observedwith respect to gender and nationality of the soldiers withdiarrhea Soldiers who were younger than 30 years of age
showed coinfections with multiple enteric pathogens lessfrequently than older soldiers Of note all assessed diarrheapatients who were deployed to Bapho were infected by viralpathogens Previous stays in high-endemicity settings did nothave any notable effects on the acquisition of bacterial viraland parasitic pathogens (Table 4)
362 Mode of Food Intake As few as 2 out of 15 diarrheapatients who claimed to have eaten exclusively in the fieldkitchen were free of enteric pathogens in the PCR analysesBacterial pathogens dominated in this group Soldiers whorestricted their diet to hotel food were prone to both bacterialand viral enteric infections There was not a single diarrheapatient in this assessment who had eaten field rations aloneprior to the onset of diarrhea (Table 5)
363 Stool Frequency andConsistency A small proportion of11 patients showed less severe symptomswith fewer than threeunformed stools per day Of note no enteric pathogens weredetected in only one of these patients There was no obviousdistribution pattern of bacterial viral or parasitic pathogensin these less severe diarrhea cases
The observed stool consistency of collected samples asreported by the laboratory technician was considerably lessunformed than the reported stool consistency A total of 13out of 49 stool samples were already hard at the time ofsample collection suggesting that the symptoms had alreadyimproved In contrast no patient reported formed stools tothe field doctor Only 3 out of these 13 formed stools werewithout detectable pathogen DNA at the time of assessment(Table 6)
364 Accompanying Symptoms including Fever Light tomoderate symptoms including nausea and vomiting crampsabdominal pain and flatulence were frequent in the assesseddiarrhea patients Cramps abdominal pain and flatulencewere particularly often detectable in diarrhea patients withbacterial infections while nausea and vomiting were equallylikely for both bacterial and viral infections Only oneinstance of bloody diarrhea was observed in a patient withShigella sppEIEC as the only detectable pathogen in stoolFever was confirmed in only three instances without anydetectable association with a particular pathogen group(Table 7)
Of note the distribution of accompanying symptoms didnot change considerably if only the 34 patients who reportedge3 stools per day were included into the assessment (Table 7)
Only one enteric pathogen per patient was detected in 16patients who reported accompanying symptoms comprising4 cases with STEC 2 cases with EAEC 2 cases with EPEC 2cases with Norovirus G1 2 cases with Norovirus G2 2 caseswith Shigella sppEIEC 1 case withCryptosporidium parvumand 1 case with Rotavirus respectively Bacterial infectionswere associated with a broad distribution of symptoms(Table 7) As expected patients infected with enteroinvasiveShigella sppEIEC showed a particularly wide spectrumof symptoms Norovirus infections and Cryptosporidiumparvum infections were associated with nausea vomiting
8 BioMed Research International
Table 4 Age gender nationality sites of deployment and previous stays in high-endemicity regions for diarrhea-associated pathogens ofdiarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Agelt30 years 1015 615 015 215 51530ndash50 years 1015 315 115 315 815gt50 years 22 12 02 02 22No data 1217 217 217 417 717
GenderMale 3144 1144 344 744 2044Female 35 15 05 25 25
NationalityAustria 11 11 01 01 11Belgium 79 29 19 19 39Colombia 11 01 01 01 01Germany 1725 825 025 425 1225Greece 33 03 13 03 33Ireland 01 01 01 11 01Italy 01 01 01 11 01Portugal 01 01 01 11 01Romania 01 11 01 01 01Spain 44 04 04 04 24SpainBolivia 01 01 01 11 01No data 11 01 11 01 11
Site of deploymentKoulikoro 3141 741 341 641 1941Koulikoro and Bamako 12 12 02 12 12Bamako 01 01 01 11 01Bapho 24 44 04 04 24No data 01 01 01 11 01
Previous stays in high endemicitysettings
Yes 813 313 113 213 413No 2636 936 236 736 1836
and abdominal pain and Norovirus G1 infections also wereassociated with cramps and flatulence (Table 7)
365 Antimalarial Prophylaxis Hygiene Counseling Vacci-nation against Cholera and Typhoid Fever and MedicationLow-dose doxycycline-monohydrate antimalarial prophy-laxis at 100mgday did not provide any protection againstbacterial enteric infections Among the diarrhea patientsunder doxycycline prophylaxis 7 out of 10 were positive forDNA of bacterial enteric pathogens
The vast majority of diarrhea patients were properlycounseled regarding hygiene on tropical deployments andwere vaccinated against typhoid fever Infections with bacte-rial enteric pathogens were particularly frequent in patientswho were vaccinated against cholera and typhoid fever Useof anti-infective drugs was documented for three patients
all three took rifaximin and one in addition metronidazoleDNA of bacterial enteric pathogens was detectable in onlyone of these patients no pathogen DNA was observed in twoof them (Table 8)
4 Discussion
Risk assessment by standardized monitoring and surveil-lance of deployed soldiers in subtropical or tropical coun-tries contributes to evaluation of both individual risk andpreventive measures As previously shown infection riskswith enteric pathogens increase if sophisticated hygieneprecautions regarding food and drinking water cannot bemaintained on military deployments for example in thecase of small missions [3] Considering an average clinicalincidence of diarrhea between 5 and 7 per 100 per month
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
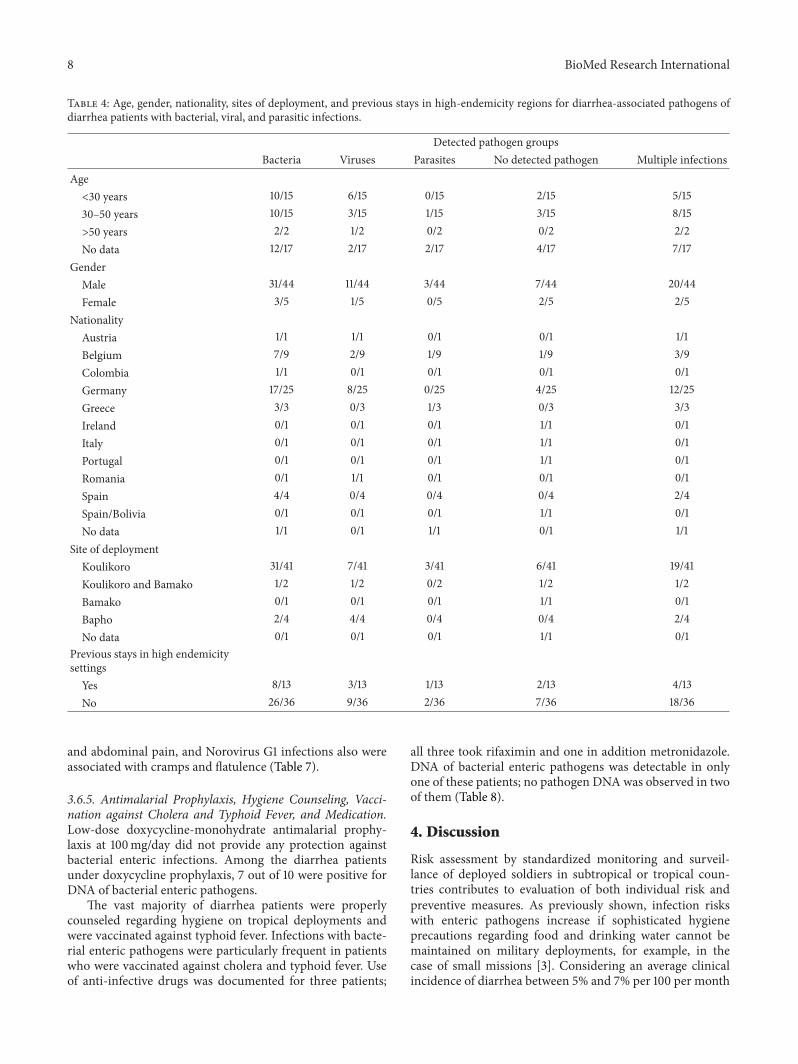
8 BioMed Research International
Table 4 Age gender nationality sites of deployment and previous stays in high-endemicity regions for diarrhea-associated pathogens ofdiarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Agelt30 years 1015 615 015 215 51530ndash50 years 1015 315 115 315 815gt50 years 22 12 02 02 22No data 1217 217 217 417 717
GenderMale 3144 1144 344 744 2044Female 35 15 05 25 25
NationalityAustria 11 11 01 01 11Belgium 79 29 19 19 39Colombia 11 01 01 01 01Germany 1725 825 025 425 1225Greece 33 03 13 03 33Ireland 01 01 01 11 01Italy 01 01 01 11 01Portugal 01 01 01 11 01Romania 01 11 01 01 01Spain 44 04 04 04 24SpainBolivia 01 01 01 11 01No data 11 01 11 01 11
Site of deploymentKoulikoro 3141 741 341 641 1941Koulikoro and Bamako 12 12 02 12 12Bamako 01 01 01 11 01Bapho 24 44 04 04 24No data 01 01 01 11 01
Previous stays in high endemicitysettings
Yes 813 313 113 213 413No 2636 936 236 736 1836
and abdominal pain and Norovirus G1 infections also wereassociated with cramps and flatulence (Table 7)
365 Antimalarial Prophylaxis Hygiene Counseling Vacci-nation against Cholera and Typhoid Fever and MedicationLow-dose doxycycline-monohydrate antimalarial prophy-laxis at 100mgday did not provide any protection againstbacterial enteric infections Among the diarrhea patientsunder doxycycline prophylaxis 7 out of 10 were positive forDNA of bacterial enteric pathogens
The vast majority of diarrhea patients were properlycounseled regarding hygiene on tropical deployments andwere vaccinated against typhoid fever Infections with bacte-rial enteric pathogens were particularly frequent in patientswho were vaccinated against cholera and typhoid fever Useof anti-infective drugs was documented for three patients
all three took rifaximin and one in addition metronidazoleDNA of bacterial enteric pathogens was detectable in onlyone of these patients no pathogen DNA was observed in twoof them (Table 8)
4 Discussion
Risk assessment by standardized monitoring and surveil-lance of deployed soldiers in subtropical or tropical coun-tries contributes to evaluation of both individual risk andpreventive measures As previously shown infection riskswith enteric pathogens increase if sophisticated hygieneprecautions regarding food and drinking water cannot bemaintained on military deployments for example in thecase of small missions [3] Considering an average clinicalincidence of diarrhea between 5 and 7 per 100 per month
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
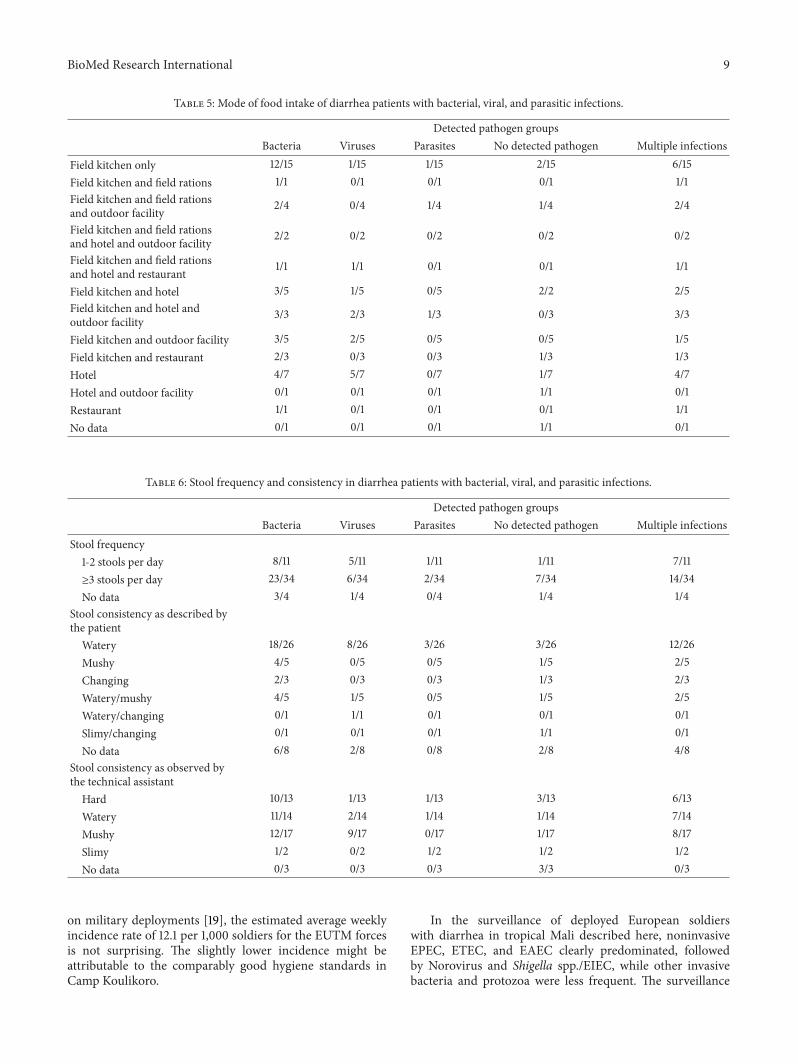
BioMed Research International 9
Table 5 Mode of food intake of diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Field kitchen only 1215 115 115 215 615Field kitchen and field rations 11 01 01 01 11Field kitchen and field rationsand outdoor facility 24 04 14 14 24
Field kitchen and field rationsand hotel and outdoor facility 22 02 02 02 02
Field kitchen and field rationsand hotel and restaurant 11 11 01 01 11
Field kitchen and hotel 35 15 05 22 25Field kitchen and hotel andoutdoor facility 33 23 13 03 33
Field kitchen and outdoor facility 35 25 05 05 15Field kitchen and restaurant 23 03 03 13 13Hotel 47 57 07 17 47Hotel and outdoor facility 01 01 01 11 01Restaurant 11 01 01 01 11No data 01 01 01 11 01
Table 6 Stool frequency and consistency in diarrhea patients with bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Stool frequency1-2 stools per day 811 511 111 111 711ge3 stools per day 2334 634 234 734 1434No data 34 14 04 14 14
Stool consistency as described bythe patient
Watery 1826 826 326 326 1226Mushy 45 05 05 15 25Changing 23 03 03 13 23Waterymushy 45 15 05 15 25Waterychanging 01 11 01 01 01Slimychanging 01 01 01 11 01No data 68 28 08 28 48
Stool consistency as observed bythe technical assistant
Hard 1013 113 113 313 613Watery 1114 214 114 114 714Mushy 1217 917 017 117 817Slimy 12 02 12 12 12No data 03 03 03 33 03
on military deployments [19] the estimated average weeklyincidence rate of 121 per 1000 soldiers for the EUTM forcesis not surprising The slightly lower incidence might beattributable to the comparably good hygiene standards inCamp Koulikoro
In the surveillance of deployed European soldierswith diarrhea in tropical Mali described here noninvasiveEPEC ETEC and EAEC clearly predominated followedby Norovirus and Shigella sppEIEC while other invasivebacteria and protozoa were less frequent The surveillance
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
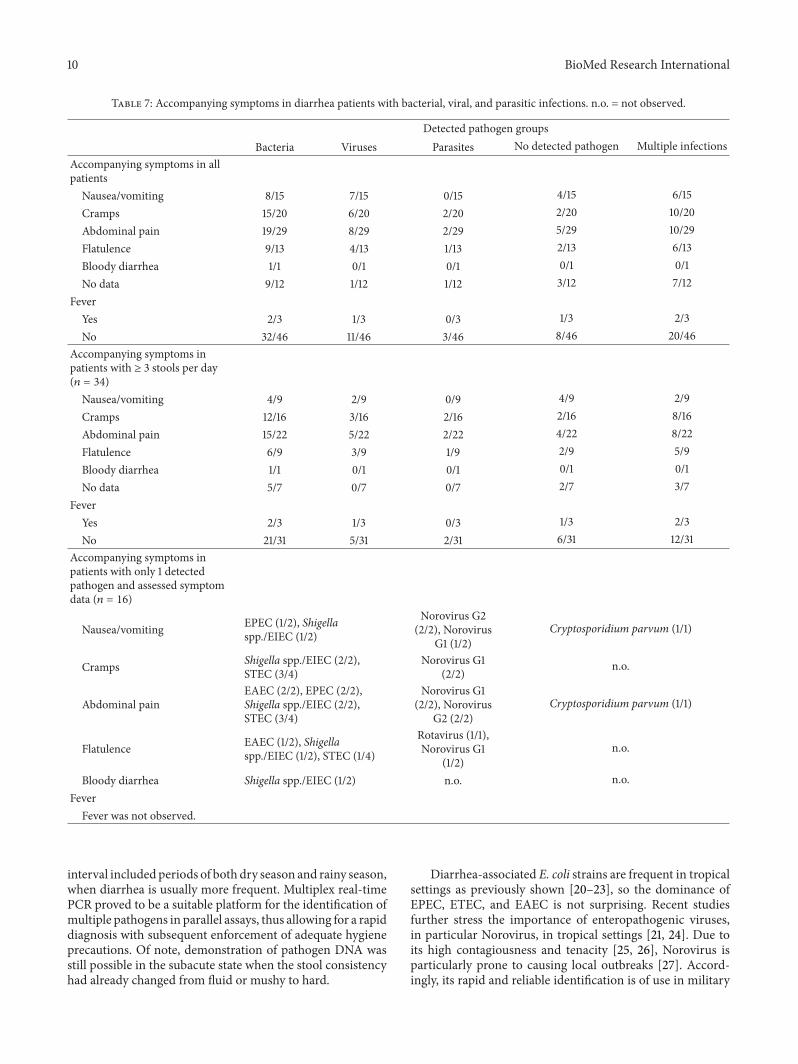
10 BioMed Research International
Table 7 Accompanying symptoms in diarrhea patients with bacterial viral and parasitic infections no = not observed
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Accompanying symptoms in allpatients
Nauseavomiting 815 715 015 415 615Cramps 1520 620 220 220 1020Abdominal pain 1929 829 229 529 1029Flatulence 913 413 113 213 613Bloody diarrhea 11 01 01 01 01No data 912 112 112 312 712
FeverYes 23 13 03 13 23No 3246 1146 346 846 2046
Accompanying symptoms inpatients with ge 3 stools per day(119899 = 34)
Nauseavomiting 49 29 09 49 29Cramps 1216 316 216 216 816Abdominal pain 1522 522 222 422 822Flatulence 69 39 19 29 59Bloody diarrhea 11 01 01 01 01No data 57 07 07 27 37
FeverYes 23 13 03 13 23No 2131 531 231 631 1231
Accompanying symptoms inpatients with only 1 detectedpathogen and assessed symptomdata (119899 = 16)
Nauseavomiting EPEC (12) ShigellasppEIEC (12)
Norovirus G2(22) Norovirus
G1 (12)Cryptosporidium parvum (11)
Cramps Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) no
Abdominal painEAEC (22) EPEC (22)Shigella sppEIEC (22)STEC (34)
Norovirus G1(22) Norovirus
G2 (22)Cryptosporidium parvum (11)
Flatulence EAEC (12) ShigellasppEIEC (12) STEC (14)
Rotavirus (11)Norovirus G1
(12)no
Bloody diarrhea Shigella sppEIEC (12) no noFever
Fever was not observed
interval included periods of both dry season and rainy seasonwhen diarrhea is usually more frequent Multiplex real-timePCR proved to be a suitable platform for the identification ofmultiple pathogens in parallel assays thus allowing for a rapiddiagnosis with subsequent enforcement of adequate hygieneprecautions Of note demonstration of pathogen DNA wasstill possible in the subacute state when the stool consistencyhad already changed from fluid or mushy to hard
Diarrhea-associated E coli strains are frequent in tropicalsettings as previously shown [20ndash23] so the dominance ofEPEC ETEC and EAEC is not surprising Recent studiesfurther stress the importance of enteropathogenic virusesin particular Norovirus in tropical settings [21 24] Due toits high contagiousness and tenacity [25 26] Norovirus isparticularly prone to causing local outbreaks [27] Accord-ingly its rapid and reliable identification is of use in military
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
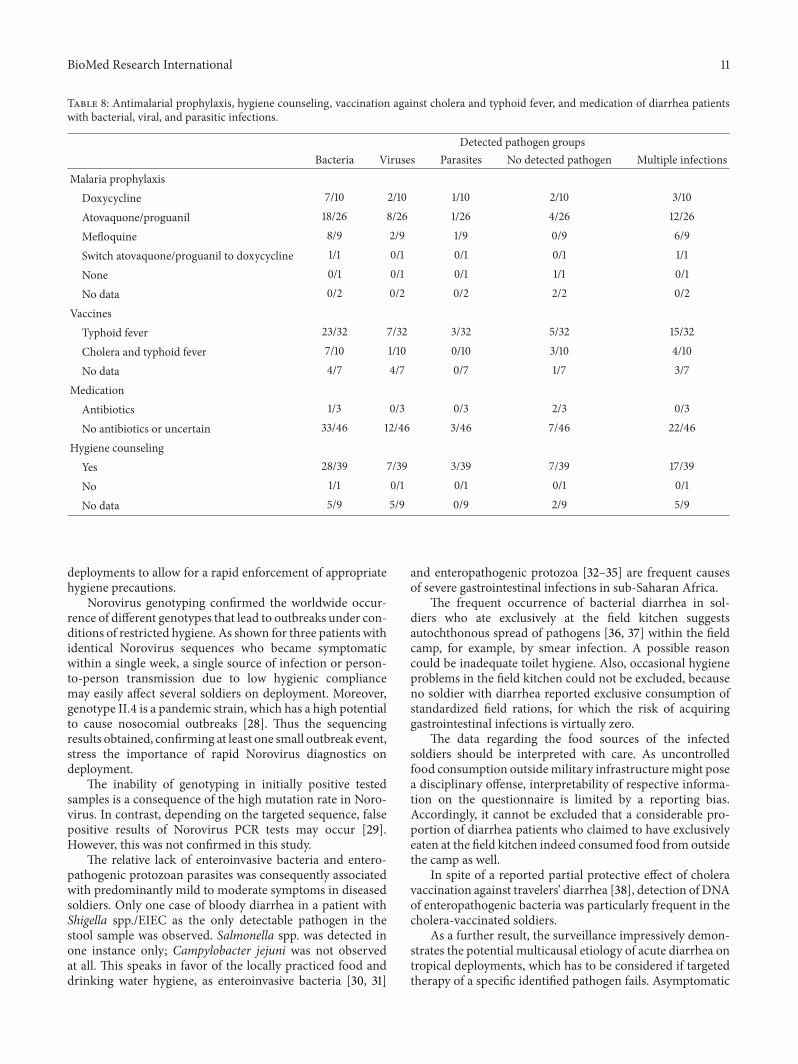
BioMed Research International 11
Table 8 Antimalarial prophylaxis hygiene counseling vaccination against cholera and typhoid fever and medication of diarrhea patientswith bacterial viral and parasitic infections
Detected pathogen groupsBacteria Viruses Parasites No detected pathogen Multiple infections
Malaria prophylaxisDoxycycline 710 210 110 210 310
Atovaquoneproguanil 1826 826 126 426 1226
Mefloquine 89 29 19 09 69
Switch atovaquoneproguanil to doxycycline 11 01 01 01 11
None 01 01 01 11 01
No data 02 02 02 22 02
VaccinesTyphoid fever 2332 732 332 532 1532
Cholera and typhoid fever 710 110 010 310 410
No data 47 47 07 17 37
MedicationAntibiotics 13 03 03 23 03
No antibiotics or uncertain 3346 1246 346 746 2246
Hygiene counselingYes 2839 739 339 739 1739
No 11 01 01 01 01
No data 59 59 09 29 59
deployments to allow for a rapid enforcement of appropriatehygiene precautions
Norovirus genotyping confirmed the worldwide occur-rence of different genotypes that lead to outbreaks under con-ditions of restricted hygiene As shown for three patients withidentical Norovirus sequences who became symptomaticwithin a single week a single source of infection or person-to-person transmission due to low hygienic compliancemay easily affect several soldiers on deployment Moreovergenotype II4 is a pandemic strain which has a high potentialto cause nosocomial outbreaks [28] Thus the sequencingresults obtained confirming at least one small outbreak eventstress the importance of rapid Norovirus diagnostics ondeployment
The inability of genotyping in initially positive testedsamples is a consequence of the high mutation rate in Noro-virus In contrast depending on the targeted sequence falsepositive results of Norovirus PCR tests may occur [29]However this was not confirmed in this study
The relative lack of enteroinvasive bacteria and entero-pathogenic protozoan parasites was consequently associatedwith predominantly mild to moderate symptoms in diseasedsoldiers Only one case of bloody diarrhea in a patient withShigella sppEIEC as the only detectable pathogen in thestool sample was observed Salmonella spp was detected inone instance only Campylobacter jejuni was not observedat all This speaks in favor of the locally practiced food anddrinking water hygiene as enteroinvasive bacteria [30 31]
and enteropathogenic protozoa [32ndash35] are frequent causesof severe gastrointestinal infections in sub-Saharan Africa
The frequent occurrence of bacterial diarrhea in sol-diers who ate exclusively at the field kitchen suggestsautochthonous spread of pathogens [36 37] within the fieldcamp for example by smear infection A possible reasoncould be inadequate toilet hygiene Also occasional hygieneproblems in the field kitchen could not be excluded becauseno soldier with diarrhea reported exclusive consumption ofstandardized field rations for which the risk of acquiringgastrointestinal infections is virtually zero
The data regarding the food sources of the infectedsoldiers should be interpreted with care As uncontrolledfood consumption outsidemilitary infrastructuremight posea disciplinary offense interpretability of respective informa-tion on the questionnaire is limited by a reporting biasAccordingly it cannot be excluded that a considerable pro-portion of diarrhea patients who claimed to have exclusivelyeaten at the field kitchen indeed consumed food from outsidethe camp as well
In spite of a reported partial protective effect of choleravaccination against travelersrsquo diarrhea [38] detection of DNAof enteropathogenic bacteria was particularly frequent in thecholera-vaccinated soldiers
As a further result the surveillance impressively demon-strates the potential multicausal etiology of acute diarrhea ontropical deployments which has to be considered if targetedtherapy of a specific identified pathogen fails Asymptomatic
12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

12 BioMed Research International
pathogen carriage was not excluded but is unlikely becausethe deployed soldiers analyzed did not arrive from high-endemicity settings As is typical for surveillance analysesno stool samples were collected prior to deployment whichwould have allowed for comparison testing this is an unde-niable limitation of the data presented
The inclusion of patients into the surveillance merelybased on the subjective assessment of the local field doctoris a major limitation of the study This limitation does notallow direct comparisons with studies using standardizeddefinitions of travelersrsquo diarrhea for example including stoolquality assessments like the Bristol stool scale [39ndash42] Ofnote the assessment of symptoms of patients with ge3 stoolsper day led to similar results as observed for the whole studypopulationThe focus of the surveillance was on patients withgastrointestinal symptoms leading to incapacitation frommilitary duty not on patients meeting a standard definitionof travelersrsquo diarrhea Therefore such a nonconventionalinclusion strategy was chosen
PCR is a highly sensitive method for the detection ofenteric pathogens in stool outperforming alternative app-roaches such as microscopy regarding the detection limit[5 43] However the problem of simultaneously detectingseveral enteric pathogens by PCR in stool samples in high-endemicity settings for diarrheal disease is a constant stum-bling block because it hinders etiological attribution andsubsequent targeted antimicrobial therapy in case of severedisease Here we could demonstrate that this problem alsoapplies to European soldiers deployed in the tropics
Quantitative PCR tests have been suggested as useful toolsfor a more reliable attribution of etiological significance todetected enteric pathogens [44 45] discriminating activeinfection from asymptomatic carrier status or sheddingof residual pathogen DNA after previous already clearedinfections However no generally accepted standards for suchquantitative approaches have been established so far DNAquantification in complex materials like stool samples is fur-ther limited by various degrees of PCR inhibition [46] In thissurveillance low Ct-values potentially suggesting etiologicalrelevance were observed for more than one pathogen inseveral instances Sufficiently powered future studies will benecessary to evaluate the usefulness of quantitative stool PCRand the definition of reliable cut-off values for the diagnosticroutine
However etiological attribution is not the only aspectthat makes calculated antimicrobial therapy challenging incase of severe diarrhea in soldiers on deployment Knowl-edge about the local antimicrobial-resistance situation indiarrhea-associated bacteria is crucial to allow for a tailoredantimicrobial therapy Next to standard recommendationsregarding the therapy of acute gastroenteritis [47] and trav-elerrsquos diarrhea [48ndash52] the British and US military medicalservices also intend studies on the optimization of single-doseantibiotic treatment regimens [19]
High rates of colonization with atypically resistant oreven multidrug-resistant bacteria in returnees from tropicalsettings have recently been described [53ndash55] Increasedcolonization with multidrug-resistant bacteria in the tropicscan be triggered by prescribing antibiotics for travelersrsquo
diarrhea [56 57] However during the International SecurityAssistance Force (ISAF)mission inAfghanistan colonizationof German soldiers with ESBL-positive Enterobacteriaceaewas as low as 5 [58] despite considerably higher coloniza-tion rates in Afghan patients In contrast nearly every fourthstool sample of European soldiers demonstrated ESBL colo-nization in our present surveillance during the EUTM Malideployment Although rep-PCR suggests a moderate degreeof clonal diversity of ESBL-positive strains fromMali severalclonal mini-clusters suggest either fecal contamination ofcommon sources of infection or nosocomial spreadingwithinthe field camp
In persons of weakened immunological state (eg afterpolytrauma on deployment) transition of enteric bacteriathrough the gut tissue with resulting sepsis may occur Ifresistant bacteria enter blood circulation in this way [59ndash61] antibiotic therapy becomes challenging The probabilityof such events rises in case of high colonization rates withresistant bacteria and selective pressure due to antibiotictherapy or prophylaxis It is a well-documented phenomenonthat colonizing resistant bacteria can cause blood streaminfections under the selective pressure of antibiotics [62ndash66]
The high incidence of ESBL-positive Enterobacteriaceaein deployed soldiers in Mali suggests the use of alternativeantibiotic drugs in case of systemic infections According toGerman recommendations oxyimino-cephalosporins (egceftazidime) or aminoacyl penicillin-beta-lactamase combi-nations (eg piperacillintazobactam) are appropriate sub-stances for calculated initial therapy of sepsis [67] Howeverthese substances will fail in case of sepsis due to ESBL-positive Enterobacteriaceae Furthermore resistance againstthe orally administrable fluoroquinolones was observed inseveral instances making the use of intravenous reserve sub-stances such as carbapenems unavoidable if severe systemicbacterial infections occur
Of note increasing antibiotic resistance has recently beendescribed for diarrhea-associated E coli and Shigella spp aswell [68] In this study only one ESBL-positive EAEC wasisolated
No efficient procedures for reliable eradication of entericcolonization with ESBL-positive Enterobacteriaceae havebeen described so far Accordingly a high probability of suchcolonization in returnees fromMali has to be considered bothfor hygienic reasons and for the choice of antibiotic drugs incase of future systemic infections
5 Conclusions
Real-time multiplex-PCR systems proved to be useful fordiarrhea surveillance in the tropical deployment settingallowing the detection of enteric pathogens in more than80 of the analyzed stool samples of European soldiers inMali However the frequent detection of DNA of severalpathogens in high-endemicity settings impedes the etiolog-ical attribution Noninvasive enteropathogenic bacteria andNorovirus dominated quantitatively andwere associatedwithmild to moderate symptoms The reported mode of foodintake suggests the presence of transmission routes in the fieldcamp
BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 13
Conflict of Interests
The authors declare that there is no conflict of interestsaccording to the guidelines of the International Committeeof Medical Journal Editors
Authorsrsquo Contribution
Hagen Frickmann and PhilippWarnke contributed equally tothis work
Acknowledgments
The authors thank all field doctors from the EUTMMali mis-sion who contributed to the surveillance Behruz ForoutanClas Oltmanns and Philipp Schroder The authors are alsograteful to Fabien Flament from the Deployment HealthSurveillance Capability Munich (DHSC) Simone Priesnitzand Karin Lubbert are gratefully acknowledged for excellenttechnical assistance
References
[1] M R Kasper A G Lescano C Lucas et al ldquoDiarrhea outbreakduring US military training in El Salvadorrdquo PLoS ONE vol 7no 7 Article ID e40404 2012
[2] S O Brockmann C Dreweck C Wagner-Wiening et alldquoSerological and epidemiological analysis of an outbreak ofgastroenteritis among military recruits in Germany caused byCryptosporidium parvumrdquo Infection vol 36 no 5 pp 450ndash4572008
[3] H Frickmann N G Schwarz D F Wiemer et al ldquoFood anddrinking water hygiene and intestinal protozoa in deployedGerman soldiersrdquo European Journal of Microbiology andImmunology vol 3 no 1 pp 53ndash60 2013
[4] H Frickmann N G Schwarz H-U Holtherm et al ldquoCompli-ance with antimalarial chemoprophylaxis in German soldiers a6-year surveyrdquo Infection vol 41 no 2 pp 311ndash320 2013
[5] D Wiemer U Loderstaedt H von Wulffen et al ldquoReal-timemultiplex PCR for simultaneous detection of Campylobacterjejuni Salmonella Shigella andYersinia species in fecal samplesrdquoInternational Journal of Medical Microbiology vol 301 no 7 pp577ndash584 2011
[6] H Frickmann DDekker K Boahen et al ldquoIncreased detectionof invasive enteropathogenic bacteria in pre-incubated bloodculture materials by real-time PCR in comparison with auto-mated incubation in Sub-Saharan Africardquo Scandinavian Journalof Infectious Diseases vol 45 no 8 pp 616ndash622 2013
[7] J J Verweij D Laeijendecker E A T Brienen L Van Lieshoutand A M Polderman ldquoDetection of Cyclospora cayetanensisin travellers returning from the tropics and subtropics usingmicroscopy and real-time PCRrdquo International Journal of Medi-cal Microbiology vol 293 no 2-3 pp 199ndash202 2003
[8] J J Verweij R A Blange K Templeton et al ldquoSimultaneousdetection of Entamoeba histolytica Giardia lamblia and Cryp-tosporidium parvum in fecal samples by using multiplex real-time PCRrdquo Journal of Clinical Microbiology vol 42 no 3 pp1220ndash1223 2004
[9] H G M Niesters ldquoQuantitation of viral load using real-timeamplification techniquesrdquo Methods vol 25 no 4 pp 419ndash4292001
[10] H Frickmann K Tenner-Racz P Eggert et al ldquoInfluence ofparasite density and sample storage time on the reliability ofentamoeba histolytica-specific PCR from formalin-fixed andparaffin-embedded tissuesrdquo Diagnostic Molecular Pathologyvol 22 no 4 pp 236ndash244 2013
[11] G P Richards M A Watson R L Fankhauser and S S Mon-roe ldquoGenogroup I and II noroviruses detected in stool samplesby real-time reverse transcription-PCR using highly degenerateuniversal primersrdquo Applied and Environmental Microbiologyvol 70 no 12 pp 7179ndash7184 2004
[12] A Kroneman H Vennema K Deforche et al ldquoAn automatedgenotyping tool for enteroviruses and norovirusesrdquo Journal ofClinical Virology vol 51 no 2 pp 121ndash125 2011
[13] J-L A N Murk E R Heddema D L J Hess J A BogaardsC M J E Vandenbroucke-Grauls and Y J Debets-OssenkoppldquoEnrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveil-lance cultures of samples from patients in intensive care unitsrdquoJournal of Clinical Microbiology vol 47 no 6 pp 1885ndash18872009
[14] T-D Huang P Bogaerts C Berhin A Guisset and YGlupczynski ldquoEvaluation of brilliance ESBL agar a novel chro-mogenic medium for detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceaerdquo Journal of ClinicalMicrobiology vol 48 no 6 pp 2091ndash2096 2010
[15] G Ongut A E Daloglu B O Baysan et al ldquoEvaluation ofa chromogenic medium for detection of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneu-moniae strainsrdquoClinical Laboratory vol 60 no 7 pp 1213ndash12152014
[16] H Frickmann M Christner M Donat et al ldquoRapid discrim-ination of Haemophilus influenzae H parainfluenzae and Hhaemolyticus by fluorescence in situ hybridization (FISH) andtwo matrix-assisted laser-desorption-ionization time-of-flightmass spectrometry (MALDI-TOF-MS) platformsrdquo PLoS ONEvol 8 no 4 Article ID e63222 2013
[17] A K da Silva J-C Le Saux S Parnaudeau M PommepuyM Elimelech and F S Le Guyader ldquoEvaluation of removalof noroviruses during wastewater treatment using real-timereverse transcription-PCR different behaviors of genogroups Iand IIrdquoApplied and Environmental Microbiology vol 73 no 24pp 7891ndash7897 2007
[18] S Svraka E Duizer H Vennema et al ldquoEtiological role ofviruses in outbreaks of acute gastroenteritis inThe Netherlandsfrom 1994 through 2005rdquo Journal of Clinical Microbiology vol45 no 5 pp 1389ndash1394 2007
[19] P Connor C K Porter B Swierczewski and M S RiddleldquoDiarrhoea during military deployment current concepts andfuture directionsrdquo Current Opinion in Infectious Diseases vol25 no 5 pp 546ndash554 2012
[20] I N Okeke ldquoDiarrheagenic Escherichia coli in sub-SaharanAfrica status uncertainties and necessitiesrdquo Journal of Infectionin Developing Countries vol 3 no 11 pp 817ndash842 2009
[21] R E Black ldquoPathogens that cause travelersrsquo diarrhea in LatinAmerica and Africardquo Reviews of infectious diseases vol 8supplement 2 pp S131ndashS135 1986
[22] R E Black ldquoEpidemiology of travelersrsquo diarrhea and relativeimportance of various pathogensrdquo Reviews of Infectious Dis-eases vol 12 supplement 1 pp S73ndashS79 1990
[23] C A Hart R M Batt and J R Saunders ldquoDiarrhoea caused byEscherichia colirdquoAnnals of Tropical Paediatrics vol 13 no 2 pp121ndash131 1993
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
14 BioMed Research International
[24] S L Becker J Vogt S Knopp et al ldquoPersistent digestivedisorders in the tropics causative infectious pathogens andreference diagnostic testsrdquo BMC Infectious Diseases vol 13article 37 2013
[25] F Kundig P Chevalley andD Genne ldquoNorovirus gastroenteri-tis frequent often epidemic with potentially severe complica-tionsrdquo RevueMedicale Suisse vol 9 no 401 pp 1806ndash1808 2013(French)
[26] L Barclay G Park E Vega et al ldquoInfection control fornorovirusrdquoClinicalMicrobiology and Infection vol 20 no 8 pp731ndash740 2014
[27] M Iturriza-Gomara and B Lopman ldquoNorovirus in healthcaresettingsrdquo Current Opinion in Infectious Diseases vol 27 no 5pp 437ndash443 2014
[28] P Godoy G Ferrrus N Torner et al ldquoHigh incidence ofnorovirus GII4 outbreaks in hospitals and nursing homes inCatalonia (Spain) 2010-2011rdquo Epidemiology and Infection vol43 no 4 pp 725ndash733 2014
[29] F R Lin Y H Shen C W Fang et al ldquoIncidence of andfactors associated with false positives in laboratory diagnosisof norovirus infection by amplification of the RNA-dependentRNA polymerase generdquo PLoS ONE vol 9 no 9 Article IDe109876 2014
[30] M S Riddle J W Sanders S D Putnam and D R TribbleldquoIncidence etiology and impact of diarrhea among long-termtravelers (US military and similar populations) a systematicreviewrdquoAmerican Journal of TropicalMedicine andHygiene vol74 no 5 pp 891ndash900 2006
[31] H K de Jong C M Parry T van der Poll andW J WiersingaldquoHost-pathogen interaction in invasive salmonellosisrdquo PLoSPathogens vol 8 no 10 Article ID e1002933 2012
[32] B Gryseels and P L Gigase ldquoThe prevalence of intestinalparasites in two suburbs ofKinshasa (Zaire) and their relation todomestic water suppliesrdquo Tropical and Geographical Medicinevol 37 no 2 pp 129ndash132 1985
[33] R Wumba A Enache-Angoulvant M Develoux et al ldquoPreva-lence of opportunistic digestive parasitic infections in KinshasaDemocratic Republic of Congo Results of a preliminary studyin 50 aids patientsrdquo Medecine Tropicale vol 67 no 2 pp 145ndash148 2007
[34] M A Babiker M S M Ali and E S Ahmed ldquoFrequency ofintestinal parasites among food-handlers in Khartoum SudanrdquoEastern Mediterranean Health Journal vol 15 no 5 pp 1098ndash1104 2009
[35] H A Saeed and H H Hamid ldquoBacteriological and parasito-logical assessment of food handlers in the Omdurman area ofSudanrdquo Journal of Microbiology Immunology and Infection vol43 no 1 pp 70ndash73 2010
[36] J Bowen-Jones ldquoInfection and cross-infection in a paediatricgastro-enteritis unitrdquoCurationis vol 12 no 3-4 pp 30ndash33 1989
[37] C N Kamalaratnam G Kang C Kirubakaran et al ldquoAprospective study of nosocomial enteric pathogen acquisitionin hospitalized children in South Indiardquo Journal of TropicalPediatrics vol 47 no 1 pp 46ndash49 2001
[38] R Lopez-Gigosos M CampinsM J Calvo et al ldquoEffectivenessof the WCrBS oral cholera vaccine in the prevention oftravelerrsquos diarrhea a prospective cohort studyrdquoHuman Vaccinesand Immunotherapeutics vol 9 no 3 pp 692ndash698 2013
[39] D Pares M Comas D Dorcaratto et al ldquoAdaptation andvalidation of the Bristol scale stool form translated into theSpanish language among health professionals and patientsrdquo
Revista Espanola de Enfermedades Digestivas vol 101 no 5 pp312ndash316 2009
[40] B P Chumpitazi M M Lane D I Czyzewski E M WeidlerP R Swank and R J Shulman ldquoCreation and initial evaluationof a stool form scale for childrenrdquoThe Journal of Pediatrics vol157 no 4 pp 594ndash597 2010
[41] M M Lane D I Czyzewski B P Chumpitazi and R JShulman ldquoReliability and validity of a modified bristol stoolform scale for childrenrdquo The Journal of Pediatrics vol 159 no3 pp 437e1ndash441e1 2011
[42] A P Martinez and G R de Azevedo ldquoThe Bristol stool formscale its translation to Portuguese cultural adaptation andvalidationrdquo Revista Latino-Americana de Enfermagem vol 20no 3 pp 583ndash589 2012
[43] J Blessmann H Buss P A T Nu et al ldquoReal-time PCRfor detection and differentiation of Entamoeba histolytica andEntamoeba dispar in fecal samplesrdquo Journal of Clinical Microbi-ology vol 40 no 12 pp 4413ndash4417 2002
[44] J A Platts-Mills J Gratz EMduma et al ldquoAssociation betweenstool enteropathogen quantity and disease in Tanzanian chil-dren using TaqMan Array Cards a nested case-control studyrdquoAmerican Journal of Tropical Medicine and Hygiene vol 90 no1 pp 133ndash138 2014
[45] B Lindsay J B Ochieng U N Ikumapayi et al ldquoQuantitativePCR for detection of Shigella improves ascertainment of Shigellaburden in children with moderate-to-severe diarrhea in low-income countriesrdquo Journal of Clinical Microbiology vol 51 no6 pp 1740ndash1746 2013
[46] M Yavzori N Uriel N Porat et al ldquoDevelopment of moleculartests for rapid detection of enteropathogensrdquoHarefuah vol 138no 9 pp 758ndash805 2000 (Hebrew)
[47] I Zollner-Schwetz and R Krause ldquoTherapy of acute gastroen-teritis role of antibioticsrdquo Clinical Microbiology and Infection2015
[48] P Connor and M J Farthing ldquoTravellersrsquo diarrhoea a militaryproblemrdquo Journal of the Royal ArmyMedical Corps vol 145 no2 pp 95ndash101 1999
[49] C D Ericsson ldquoTravellersrsquo diarrhoeardquo International Journal ofAntimicrobial Agents vol 21 no 2 pp 116ndash124 2003
[50] P Layer and V Andresen ldquoReview article rifaximin a mini-mally absorbed oral antibacterial for the treatment of travellersrsquodiarrhoeardquo Alimentary Pharmacology and Therapeutics vol 31no 11 pp 1155ndash1164 2010
[51] K L Hopkins S Mushtaq J F Richardson et al ldquoIn vitroactivity of rifaximin against clinical isolates of Escherichia coliand other enteropathogenic bacteria isolated from travellersreturning to the UKrdquo International Journal of AntimicrobialAgents vol 43 no 5 pp 431ndash437 2014
[52] R Steffen D R Hill and H L DuPont ldquoTravelerrsquos diarrheaa clinical reviewrdquo Journal of the American Medical Associationvol 313 no 1 pp 71ndash80 2015
[53] G Peirano K B Laupland D B Gregson and J D D PitoutldquoColonization of returning travelers with CTX-M-producingEscherichia colirdquo Journal of Travel Medicine vol 18 no 5 pp299ndash303 2011
[54] S Paltansing J A Vlot M E M Kraakman et al ldquoExtended-spectrum 120573-lactamase-producing enterobacteriaceae amongtravelers from the Netherlandsrdquo Emerging Infectious Diseasesvol 19 no 8 pp 1206ndash1213 2013
[55] C Lubbert L Straube C Stein et al ldquoColonization withextended-spectrum beta-lactamase-producing and carbapene-mase-producing Enterobacteriaceae in international travelers
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
BioMed Research International 15
returning to Germanyrdquo International Journal of Medical Micro-biology vol 305 no 1 pp 148ndash156 2015
[56] S M Belderok A van denHoek J A Kint M F Schim van derLoeff and G J B Sonder ldquoIncidence risk factors and treatmentof diarrhoea among Dutch travellers reasons not to routinelyprescribe antibioticsrdquo BMC Infectious Diseases vol 11 article295 2011
[57] A Kantele ldquoA call to restrict prescribing antibiotics for trav-ellersrsquo diarrheamdashtravel medicine practitioners can play anactive role in preventing the spread of antimicrobial resistancerdquoTravelMedicine and InfectiousDisease vol 13 no 3 pp 213ndash2142015
[58] S Vandersee M Hannemann F Herrmann and P BeckerldquoMultiresistente erreger bei patienten des deutschen Bundes-wehr-Einsatzlazaretts in Masar-e Scharifrdquo Hygiene amp Medizinvol 36 pp 384ndash392 2011 (German)
[59] M Li R D Specian R D Berg and E A Deitch ldquoEffects ofprotein malnutrition and endotoxin on the intestinal mucosalbarrier to the translocation of indigenous flora inmicerdquo Journalof Parenteral and Enteral Nutrition vol 13 no 6 pp 572ndash5781989
[60] C Vaishnavi ldquoTranslocation of gut flora and its role in sepsisrdquoIndian Journal of Medical Microbiology vol 31 no 4 pp 334ndash342 2013
[61] M Gatt B S Reddy and J MacFie ldquoReview article bacterialtranslocation in the critically illmdashevidence and methods ofpreventionrdquo Alimentary Pharmacology and Therapeutics vol25 no 7 pp 741ndash757 2007
[62] M J Matar A Safdar and K V I Rolston ldquoRelationship ofcolonization with vancomycin-resistant enterococci and risk ofsystemic infection in patients with cancerrdquo Clinical InfectiousDiseases vol 42 no 10 pp 1506ndash1507 2006
[63] D M Weinstock M Conlon C Iovino et al ldquoColonizationbloodstream infection and mortality caused by vancomycin-resistant enterococcus early after allogeneic hematopoietic stemcell transplantrdquo Biology of Blood and Marrow Transplantationvol 13 no 5 pp 615ndash621 2007
[64] J B Bossaer P D Hall and E Garrett-Mayer ldquoIncidence ofvancomycin-resistant enterococci (VRE) infection in high-riskfebrile neutropenic patients colonized with VRErdquo SupportiveCare in Cancer vol 19 no 2 pp 231ndash237 2010
[65] E J Haas T E Zaoutis P Prasad M Li and S E CoffinldquoRisk factors and outcomes for vancomycin-resistant Entero-coccus bloodstream infection in childrenrdquo Infection Control andHospital Epidemiology vol 31 no 10 pp 1038ndash1042 2010
[66] C Ubeda Y Taur R R Jenq et al ldquoVancomycin-resistantEnterococcus domination of intestinal microbiota is enabled byantibiotic treatment inmice and precedes bloodstream invasionin humansrdquoThe Journal of Clinical Investigation vol 120 no 12pp 4332ndash4341 2010
[67] K F Bodmann and B Grabein ldquoExpertenkommission derPaul-Ehrlich-Gesellschaft fur Chemotherapie eV Empfehlun-gen zur kalkulierten parenteralen Initialtherapie bakteriellerErkrankungen bei Erwachsenen Update 2010rdquo ChemotherapyJournal vol 19 pp 179ndash255 2010 (German)
[68] A F Sadeghabadi A Ajami R Fadaei et al ldquoWidespreadantibiotic resistance of diarrheagenic Escherichia coli andShigella speciesrdquo Journal of Research in Medical Sciences vol 19supplement 1 pp S51ndashS55 2014
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology