research article detection of urinary tract...
TRANSCRIPT

Research ArticleDetection of Urinary Tract Pathology in Some Schistosomahaematobium Infected Nigerian Adults
O S Onile1 H O Awobode2 V S Oladele3 A M Agunloye4 and C I Anumudu3
1Department of Biological Sciences Elizade University PMB 002 Ilara-Mokin Ondo State Nigeria2Parasitology Unit Department of Zoology University of Ibadan Ibadan 20004 Nigeria3Cellular Parasitology Programme Department of Zoology University of Ibadan Ibadan 200004 Nigeria4Department of Radiology University Teaching Hospital University of Ibadan Ibadan 200004 Nigeria
Correspondence should be addressed to C I Anumudu cianumuduyahoocom
Received 19 May 2016 Revised 2 July 2016 Accepted 12 July 2016
Academic Editor Marcel Tanner
Copyright copy 2016 O S Onile et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Screening for Schistosoma haematobium infection and its possible morbidity was carried out in 257 adult participants in Egguacommunity Ogun State Nigeria Parasitological assessment for the presence of ova of S haematobium in urine and abdominopelvicultrasonographic examination for bladder and secondary kidney pathology were carried out S haematobium prevalence of 2568(66257) was recorded among the participants There was a significantly higher prevalence of 692 of urinary schistosomiasis inthe females than the prevalence of 318 inmales (119875 = 0902)The intensity of infections was mostly light (55) (218) compared toheavy (10) (39)with themean intensity of 167 eggs10mL urine Structural bladder pathology prevalence among participants was339The bladder and kidney pathologies observed by ultrasound in subjects with S haematobium infections included abnormalbladder wall thickness (59) abnormal bladder shape (152) bladder wall irregularities (152) bladder masses (15) bladdercalcification (15) and hydronephrosis (3) Infection with S haematobium was associated with bladder pathology Higherfrequencies of bladder abnormalities were observed more in the participants with light intensity of S haematobium infection thanin those with heavy infection More bladder pathology was also seen in women than in men although this was not statisticallysignificant In conclusion there is evidence that the development of bladder pathology may be associated with S haematobiuminfection
1 Introduction
An estimated 207 million cases of human schistosomiasishave been reported worldwide and about 90 of these live inSub-Saharan Africa with Nigeria having the highest preva-lence [1] Schistosoma infections cause significant morbidityandmortality with peak prevalence and intensity of infectionoccurring between the ages 10 and 20 years and subsequentdecline by age 65 years [2]
Chronic human circulatory system infection by Schisto-soma haematobium is reported to affect the urinary bladderand is a possible risk factor in the aetiology of cancers ofthe bladder and the urinary tract system [3] S haematobiuminfection has been linked with the development of squa-mous cell carcinoma of the bladder [4 5] S haematobiumassociated bladder damage has been closely linked to the
immune reaction elicited against the parasite egg deposited inthe bladder which eventually induces chronic inflammationrelated granulomatous injury [6]
Schistosomiasis and bladder cancer share common symp-toms such as haematuria dysuria and pain with micturitionThis may prevent early diagnosis of bladder cancer and theresultant severe bladder damage particularly in people livingin S haematobium endemic areas
In Nigeria most studies have focused on the epidemi-ology of S haematobium infection [3 7 8] particularly inschool-age children with limited information about themorbidity resulting from urinary schistosomiasis in adults
This study was therefore aimed at determining the preva-lence of schistosomiasis and associated bladder pathology inadults living in Eggua Yewa North Local Government AreaOgun State Nigeria
Hindawi Publishing CorporationJournal of Tropical MedicineVolume 2016 Article ID 5405207 5 pageshttpdxdoiorg10115520165405207
2 Journal of Tropical Medicine
2 Materials and Methods
The study was carried out in Eggua a rural agrarian commu-nity betweenAugust 2012 andMay 2013 It is one of the wardsthat make up Yewa North Local Government Area as previ-ously described [9] Eggua lies between latitude 7∘61015840481110158401015840Nand longitude 2∘5210158404377610158401015840E in a derived savanna zone Thearea is largely dominated by Yoruba speaking people Itconsists of settlements at Sagbon Imoto Tata Agbon-Ojoduand Igan Alade It shares boundaries with Igbogila IlaroIjoun and Benin Republic
Two major rivers (Yewa and Iju) flowing through thearea serve as the main water source resulting in high watercontact by the inhabitantsThese rivers are used for religiousdomestic and entertainment activities which enhance thetransmission of schistosomiasis
A cross-sectional study design was employed for thisstudy Participants aged 30 to more than 60 years old fromthe community were enrolled for the study Children wereexcluded from the study in line with the objective of the studyto determine the effect of chronic urinary schistosomiasis onadult members of the community
21 Ethical Considerations Informed consent was obtainedfrom each participant under a protocol approved by the LocalGovernment and local health officials Ethical approval forthe study was also obtained from the Ogun State Ministry ofHealth
22 Sample (Biofluid) Collection Blood (5mL) and urinespecimens were collected from each study participant Theurine samples were collected between 1000 and 1400 hoursto ensure maximum egg yield Packed cell volume (PCV) wasdetermined from the blood collected
23 Sample Analyses The urine samples (10mL) were pro-cessed for microscopic examination and egg count [3 10]The eggs were quantified by counting under the microscopeand classified as light infection if there were le50 (1ndash49)eggs10mL urine and heavy infection if there were gt50eggs10mL urine [3]
24 Ultrasound and Pathology A blind ultrasound exami-nation was carried out on each participant approximately1 h after drinking potable water (01ndash15 litre dependingon the age of the participant) to distend the bladder Theclassification of bladder pathology or damage was basedon the definition of the WHO [11 12] and Shiff et al[5] the abnormalities assessed included abnormal bladdershape bladder wall irregularities bladdermasses presence ofpolyps calcification and presence of hydronephrosis in thekidneys Bladder lesions were considered severely abnormalwhen four of the above conditions or three conditions as wellas hydronephrosis were present in a single individual Lesionswere considered moderate if fewer conditions were seen andnegative when no specific lesions were observed
25 Sociodemographic Data Collection A structured pre-tested questionnaire was used to obtain information about
Table 1 Prevalence and intensity of S haematobium by sex and agegroup in Eggua Nigeria
Light119873 le 50 ()
Heavy119873 gt 50 () Total
SexMale 18 (273) 3 (45) 21 (318)Female 38 (576) 7 (106) 45 (692)
Total 56 (218) 10 (39) 66 (2568)1205942
= 2514 119875 = 0113Age group30ndash34 2 (36) 1 (10)35ndash39 9 (161) 1 (10)40ndash44 8 (143) 1 (10)45ndash49 9 (161) 1 (10)50ndash54 6 (107) 2 (20)55ndash59 6 (107) 2 (20)60 and above 16 (286) 2 (20)
participantsrsquo habits regarding smoking and alcohol consump-tion which are determinants of bladder cancer Sociode-mographic information was also recorded for each of theparticipants
Statistical analysis of data obtained was done using SPSSversion 200 (119875 lt 005)
3 Results
A total of 257 (79 males and 178 females) participants aged30ndash90 years were screened for S haematobium infection andassociated bladder pathologies The mean age of participantswas 48plusmn122 yearsThe overall prevalence of S haematobiumin the sampled population was 2568 (66257) 21 (318)in males and 45 (682) in females The highest prevalenceof infection was observed in participants over 60 years old(Table 1) The majority (5666) (848) of those positive forS haematobium had a light intensity of infection with theegg mean intensity of 167 eggs10mL urine The Yewa riverwas the main source of water for most (4962) (790) of theparticipants infected with S haematobium (Table 4)
Bladder pathologies were observed in 339 (87257) ofthe sample population and included abnormal bladder wallthickness (3966) (59) abnormal bladder shape (1066)(152) bladder wall irregularities (152) bladder masses(15) and bladder calcification (15) (Table 2) Bladderwall thickness the most common abnormality was recordedin 4679 (582) males and 90178 (506) females (Table 3)Among the participants 56 (848) with bladder pathologiesalso had an existing schistosomiasis infection 48 (873) ofwhich were light intensity and 8 (727) of which were heavyintensity 1205942 = 2675 119875 = 0001 (Table 5) Thus there was anassociation between urinary tract pathology and the intensityof S haematobium infection (1205942 = 3754 119875 = 0001 Table 2)Among the participants with light and heavy intensity of Shaematobium infections bladder wall thickness was the mostcommon bladder structural pathology identified in 3356
Journal of Tropical Medicine 3
Table 2 Distribution of bladder pathology with intensity of Shaematobium infection
Pathology1205942
= 3754 119875 = 0001Intensity of infection Total
Light () Heavy ()Bladder wallthickness 33 (589) 6 (600) 59
Bladder shape 8 (143) 2 (200) 152Bladder wallirregularity 8 (143) 2 (200) 152
Bladder mass 0 (0) 1 (100) 15Calcification 0 (0) 1 (100) 15Polyps mdash mdash mdashHydronephrosis 6 (107) 0 (0) 9
Table 3 Distribution of bladder pathology among genders
Pathology GenderMale Female
Bladder wall thickness 46 (582) 90 (506)Bladder shape 7 (89) 6 (34)Bladder wall irregularity 7 (89) 6 (34)Bladder mass mdash 1 (06)Calcification mdash 1 (06)Polyps mdash mdashHydronephrosis mdash 6 (34)
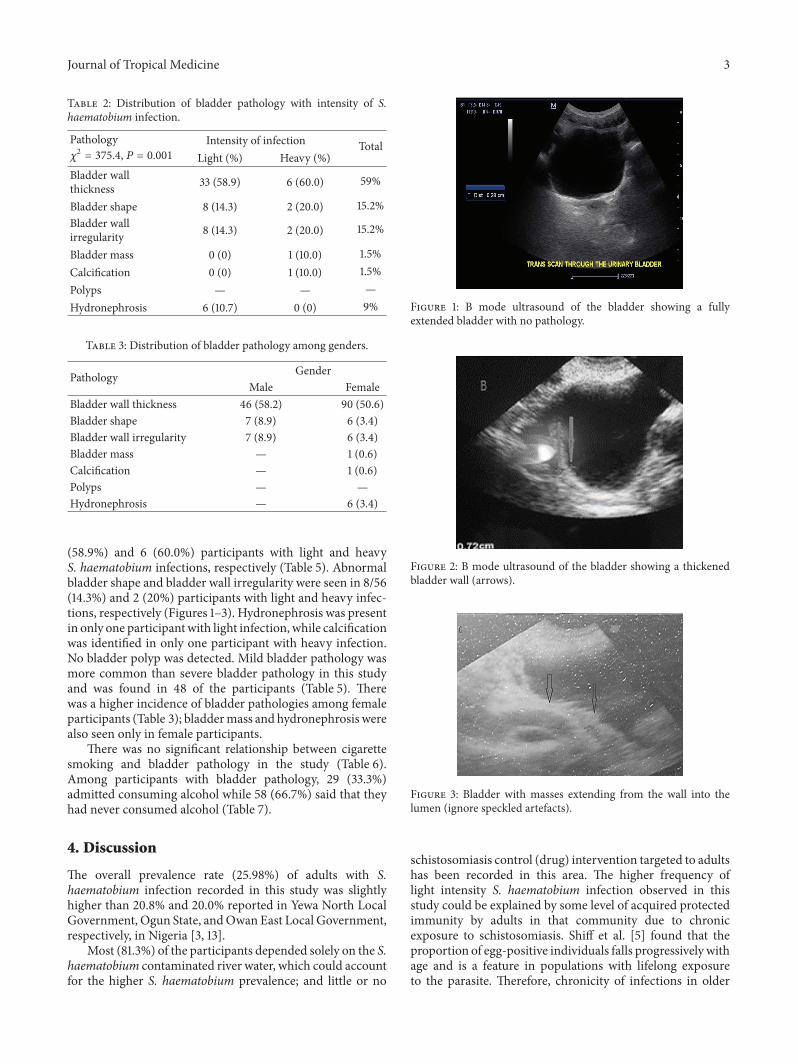
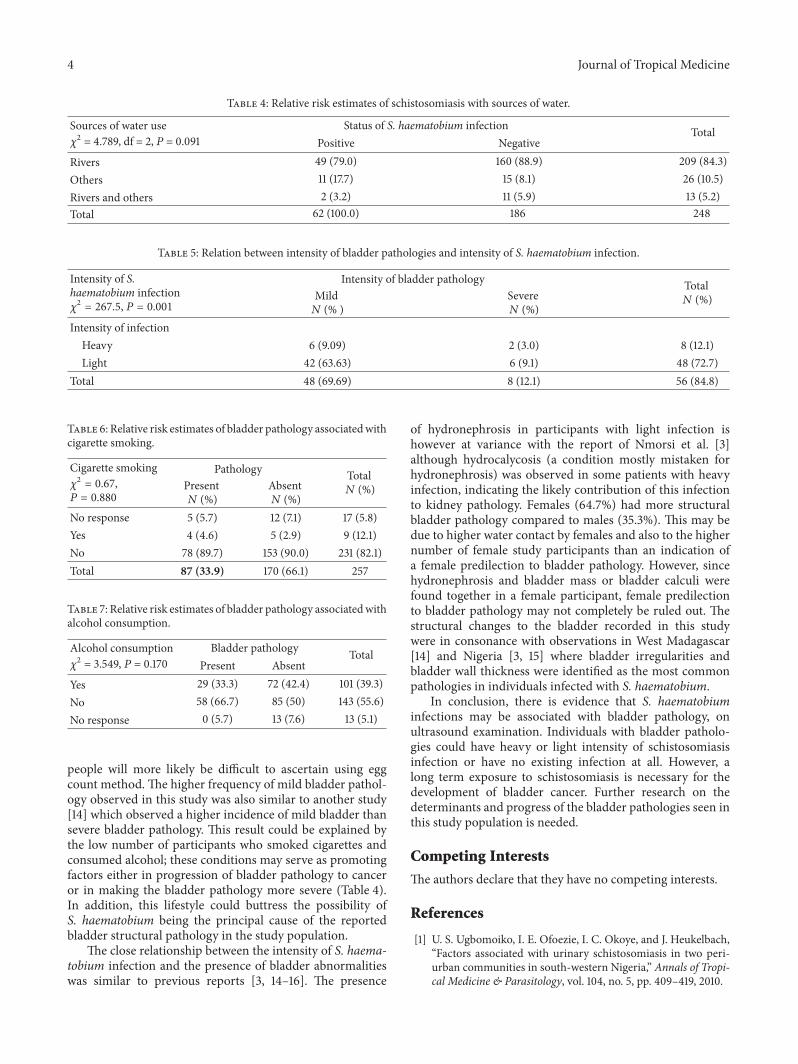
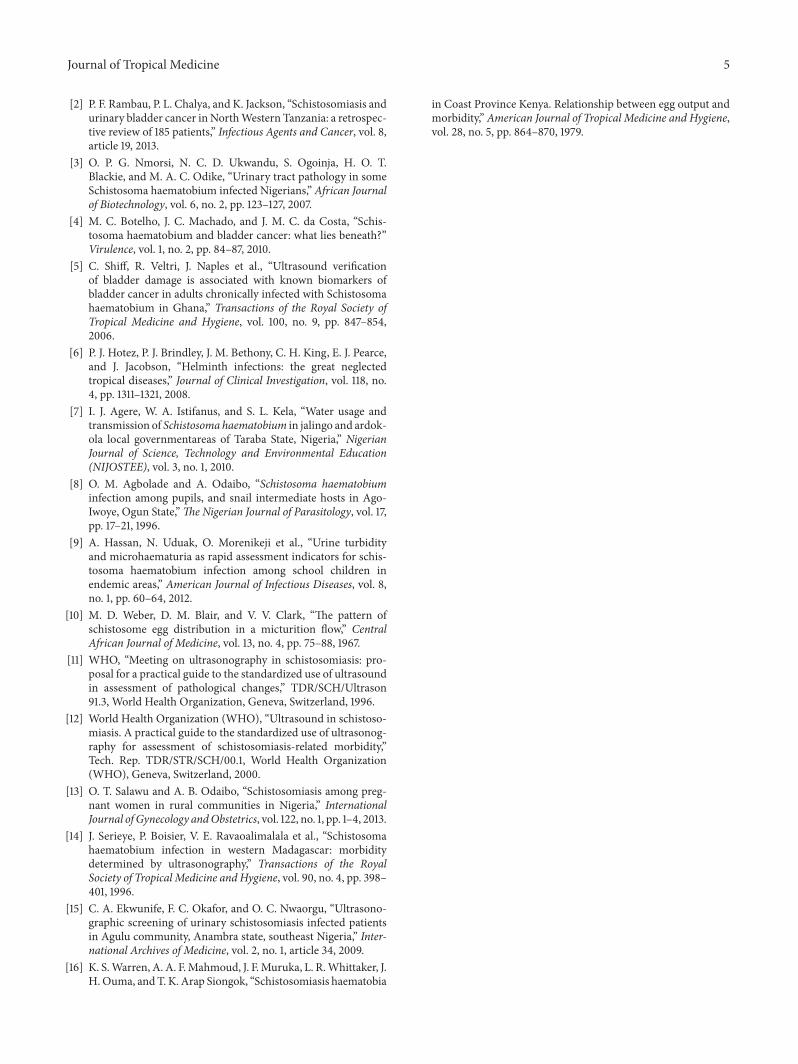
(589) and 6 (600) participants with light and heavyS haematobium infections respectively (Table 5) Abnormalbladder shape and bladder wall irregularity were seen in 856(143) and 2 (20) participants with light and heavy infec-tions respectively (Figures 1ndash3) Hydronephrosis was presentin only one participantwith light infection while calcificationwas identified in only one participant with heavy infectionNo bladder polyp was detected Mild bladder pathology wasmore common than severe bladder pathology in this studyand was found in 48 of the participants (Table 5) Therewas a higher incidence of bladder pathologies among femaleparticipants (Table 3) bladdermass and hydronephrosis werealso seen only in female participants
There was no significant relationship between cigarettesmoking and bladder pathology in the study (Table 6)Among participants with bladder pathology 29 (333)admitted consuming alcohol while 58 (667) said that theyhad never consumed alcohol (Table 7)
4 Discussion
The overall prevalence rate (2598) of adults with Shaematobium infection recorded in this study was slightlyhigher than 208 and 200 reported in Yewa North LocalGovernment Ogun State andOwan East Local Governmentrespectively in Nigeria [3 13]
Most (813) of the participants depended solely on the Shaematobium contaminated river water which could accountfor the higher S haematobium prevalence and little or no
Figure 1 B mode ultrasound of the bladder showing a fullyextended bladder with no pathology
Figure 2 B mode ultrasound of the bladder showing a thickenedbladder wall (arrows)
Figure 3 Bladder with masses extending from the wall into thelumen (ignore speckled artefacts)
schistosomiasis control (drug) intervention targeted to adultshas been recorded in this area The higher frequency oflight intensity S haematobium infection observed in thisstudy could be explained by some level of acquired protectedimmunity by adults in that community due to chronicexposure to schistosomiasis Shiff et al [5] found that theproportion of egg-positive individuals falls progressively withage and is a feature in populations with lifelong exposureto the parasite Therefore chronicity of infections in older
4 Journal of Tropical Medicine
Table 4 Relative risk estimates of schistosomiasis with sources of water
Sources of water use1205942 = 4789 df = 2 119875 = 0091
Status of S haematobium infection TotalPositive Negative
Rivers 49 (790) 160 (889) 209 (843)Others 11 (177) 15 (81) 26 (105)Rivers and others 2 (32) 11 (59) 13 (52)Total 62 (1000) 186 248
Table 5 Relation between intensity of bladder pathologies and intensity of S haematobium infection
Intensity of Shaematobium infection1205942
= 2675 119875 = 0001
Intensity of bladder pathology Total119873 ()Mild
119873 ( )Severe119873 ()
Intensity of infectionHeavy 6 (909) 2 (30) 8 (121)Light 42 (6363) 6 (91) 48 (727)
Total 48 (6969) 8 (121) 56 (848)
Table 6 Relative risk estimates of bladder pathology associatedwithcigarette smoking
Cigarette smoking1205942
= 067119875 = 0880
Pathology Total119873 ()Present
119873 ()Absent119873 ()
No response 5 (57) 12 (71) 17 (58)Yes 4 (46) 5 (29) 9 (121)No 78 (897) 153 (900) 231 (821)Total 87 (339) 170 (661) 257
Table 7 Relative risk estimates of bladder pathology associatedwithalcohol consumption
Alcohol consumption1205942 = 3549 119875 = 0170
Bladder pathology TotalPresent Absent
Yes 29 (333) 72 (424) 101 (393)No 58 (667) 85 (50) 143 (556)No response 0 (57) 13 (76) 13 (51)
people will more likely be difficult to ascertain using eggcount method The higher frequency of mild bladder pathol-ogy observed in this study was also similar to another study[14] which observed a higher incidence of mild bladder thansevere bladder pathology This result could be explained bythe low number of participants who smoked cigarettes andconsumed alcohol these conditions may serve as promotingfactors either in progression of bladder pathology to canceror in making the bladder pathology more severe (Table 4)In addition this lifestyle could buttress the possibility ofS haematobium being the principal cause of the reportedbladder structural pathology in the study population
The close relationship between the intensity of S haema-tobium infection and the presence of bladder abnormalitieswas similar to previous reports [3 14ndash16] The presence
of hydronephrosis in participants with light infection ishowever at variance with the report of Nmorsi et al [3]although hydrocalycosis (a condition mostly mistaken forhydronephrosis) was observed in some patients with heavyinfection indicating the likely contribution of this infectionto kidney pathology Females (647) had more structuralbladder pathology compared to males (353) This may bedue to higher water contact by females and also to the highernumber of female study participants than an indication ofa female predilection to bladder pathology However sincehydronephrosis and bladder mass or bladder calculi werefound together in a female participant female predilectionto bladder pathology may not completely be ruled out Thestructural changes to the bladder recorded in this studywere in consonance with observations in West Madagascar[14] and Nigeria [3 15] where bladder irregularities andbladder wall thickness were identified as the most commonpathologies in individuals infected with S haematobium
In conclusion there is evidence that S haematobiuminfections may be associated with bladder pathology onultrasound examination Individuals with bladder patholo-gies could have heavy or light intensity of schistosomiasisinfection or have no existing infection at all However along term exposure to schistosomiasis is necessary for thedevelopment of bladder cancer Further research on thedeterminants and progress of the bladder pathologies seen inthis study population is needed
Competing Interests
The authors declare that they have no competing interests
References
[1] U S Ugbomoiko I E Ofoezie I C Okoye and J HeukelbachldquoFactors associated with urinary schistosomiasis in two peri-urban communities in south-western Nigeriardquo Annals of Tropi-cal Medicine amp Parasitology vol 104 no 5 pp 409ndash419 2010
Journal of Tropical Medicine 5
[2] P F Rambau P L Chalya and K Jackson ldquoSchistosomiasis andurinary bladder cancer inNorthWestern Tanzania a retrospec-tive review of 185 patientsrdquo Infectious Agents and Cancer vol 8article 19 2013
[3] O P G Nmorsi N C D Ukwandu S Ogoinja H O TBlackie and M A C Odike ldquoUrinary tract pathology in someSchistosoma haematobium infected Nigeriansrdquo African Journalof Biotechnology vol 6 no 2 pp 123ndash127 2007
[4] M C Botelho J C Machado and J M C da Costa ldquoSchis-tosoma haematobium and bladder cancer what lies beneathrdquoVirulence vol 1 no 2 pp 84ndash87 2010
[5] C Shiff R Veltri J Naples et al ldquoUltrasound verificationof bladder damage is associated with known biomarkers ofbladder cancer in adults chronically infected with Schistosomahaematobium in Ghanardquo Transactions of the Royal Society ofTropical Medicine and Hygiene vol 100 no 9 pp 847ndash8542006
[6] P J Hotez P J Brindley J M Bethony C H King E J Pearceand J Jacobson ldquoHelminth infections the great neglectedtropical diseasesrdquo Journal of Clinical Investigation vol 118 no4 pp 1311ndash1321 2008
[7] I J Agere W A Istifanus and S L Kela ldquoWater usage andtransmission of Schistosoma haematobium in jalingo and ardok-ola local governmentareas of Taraba State Nigeriardquo NigerianJournal of Science Technology and Environmental Education(NIJOSTEE) vol 3 no 1 2010
[8] O M Agbolade and A Odaibo ldquoSchistosoma haematobiuminfection among pupils and snail intermediate hosts in Ago-Iwoye Ogun StaterdquoThe Nigerian Journal of Parasitology vol 17pp 17ndash21 1996
[9] A Hassan N Uduak O Morenikeji et al ldquoUrine turbidityand microhaematuria as rapid assessment indicators for schis-tosoma haematobium infection among school children inendemic areasrdquo American Journal of Infectious Diseases vol 8no 1 pp 60ndash64 2012
[10] M D Weber D M Blair and V V Clark ldquoThe pattern ofschistosome egg distribution in a micturition flowrdquo CentralAfrican Journal of Medicine vol 13 no 4 pp 75ndash88 1967
[11] WHO ldquoMeeting on ultrasonography in schistosomiasis pro-posal for a practical guide to the standardized use of ultrasoundin assessment of pathological changesrdquo TDRSCHUltrason913 World Health Organization Geneva Switzerland 1996
[12] World Health Organization (WHO) ldquoUltrasound in schistoso-miasis A practical guide to the standardized use of ultrasonog-raphy for assessment of schistosomiasis-related morbidityrdquoTech Rep TDRSTRSCH001 World Health Organization(WHO) Geneva Switzerland 2000
[13] O T Salawu and A B Odaibo ldquoSchistosomiasis among preg-nant women in rural communities in Nigeriardquo InternationalJournal of Gynecology andObstetrics vol 122 no 1 pp 1ndash4 2013
[14] J Serieye P Boisier V E Ravaoalimalala et al ldquoSchistosomahaematobium infection in western Madagascar morbiditydetermined by ultrasonographyrdquo Transactions of the RoyalSociety of Tropical Medicine and Hygiene vol 90 no 4 pp 398ndash401 1996
[15] C A Ekwunife F C Okafor and O C Nwaorgu ldquoUltrasono-graphic screening of urinary schistosomiasis infected patientsin Agulu community Anambra state southeast Nigeriardquo Inter-national Archives of Medicine vol 2 no 1 article 34 2009
[16] K SWarren A A FMahmoud J FMuruka L RWhittaker JH Ouma and T K Arap Siongok ldquoSchistosomiasis haematobia
in Coast Province Kenya Relationship between egg output andmorbidityrdquo American Journal of Tropical Medicine and Hygienevol 28 no 5 pp 864ndash870 1979
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Journal of Tropical Medicine
2 Materials and Methods
The study was carried out in Eggua a rural agrarian commu-nity betweenAugust 2012 andMay 2013 It is one of the wardsthat make up Yewa North Local Government Area as previ-ously described [9] Eggua lies between latitude 7∘61015840481110158401015840Nand longitude 2∘5210158404377610158401015840E in a derived savanna zone Thearea is largely dominated by Yoruba speaking people Itconsists of settlements at Sagbon Imoto Tata Agbon-Ojoduand Igan Alade It shares boundaries with Igbogila IlaroIjoun and Benin Republic
Two major rivers (Yewa and Iju) flowing through thearea serve as the main water source resulting in high watercontact by the inhabitantsThese rivers are used for religiousdomestic and entertainment activities which enhance thetransmission of schistosomiasis
A cross-sectional study design was employed for thisstudy Participants aged 30 to more than 60 years old fromthe community were enrolled for the study Children wereexcluded from the study in line with the objective of the studyto determine the effect of chronic urinary schistosomiasis onadult members of the community
21 Ethical Considerations Informed consent was obtainedfrom each participant under a protocol approved by the LocalGovernment and local health officials Ethical approval forthe study was also obtained from the Ogun State Ministry ofHealth
22 Sample (Biofluid) Collection Blood (5mL) and urinespecimens were collected from each study participant Theurine samples were collected between 1000 and 1400 hoursto ensure maximum egg yield Packed cell volume (PCV) wasdetermined from the blood collected
23 Sample Analyses The urine samples (10mL) were pro-cessed for microscopic examination and egg count [3 10]The eggs were quantified by counting under the microscopeand classified as light infection if there were le50 (1ndash49)eggs10mL urine and heavy infection if there were gt50eggs10mL urine [3]
24 Ultrasound and Pathology A blind ultrasound exami-nation was carried out on each participant approximately1 h after drinking potable water (01ndash15 litre dependingon the age of the participant) to distend the bladder Theclassification of bladder pathology or damage was basedon the definition of the WHO [11 12] and Shiff et al[5] the abnormalities assessed included abnormal bladdershape bladder wall irregularities bladdermasses presence ofpolyps calcification and presence of hydronephrosis in thekidneys Bladder lesions were considered severely abnormalwhen four of the above conditions or three conditions as wellas hydronephrosis were present in a single individual Lesionswere considered moderate if fewer conditions were seen andnegative when no specific lesions were observed
25 Sociodemographic Data Collection A structured pre-tested questionnaire was used to obtain information about
Table 1 Prevalence and intensity of S haematobium by sex and agegroup in Eggua Nigeria
Light119873 le 50 ()
Heavy119873 gt 50 () Total
SexMale 18 (273) 3 (45) 21 (318)Female 38 (576) 7 (106) 45 (692)
Total 56 (218) 10 (39) 66 (2568)1205942
= 2514 119875 = 0113Age group30ndash34 2 (36) 1 (10)35ndash39 9 (161) 1 (10)40ndash44 8 (143) 1 (10)45ndash49 9 (161) 1 (10)50ndash54 6 (107) 2 (20)55ndash59 6 (107) 2 (20)60 and above 16 (286) 2 (20)
participantsrsquo habits regarding smoking and alcohol consump-tion which are determinants of bladder cancer Sociode-mographic information was also recorded for each of theparticipants
Statistical analysis of data obtained was done using SPSSversion 200 (119875 lt 005)
3 Results
A total of 257 (79 males and 178 females) participants aged30ndash90 years were screened for S haematobium infection andassociated bladder pathologies The mean age of participantswas 48plusmn122 yearsThe overall prevalence of S haematobiumin the sampled population was 2568 (66257) 21 (318)in males and 45 (682) in females The highest prevalenceof infection was observed in participants over 60 years old(Table 1) The majority (5666) (848) of those positive forS haematobium had a light intensity of infection with theegg mean intensity of 167 eggs10mL urine The Yewa riverwas the main source of water for most (4962) (790) of theparticipants infected with S haematobium (Table 4)
Bladder pathologies were observed in 339 (87257) ofthe sample population and included abnormal bladder wallthickness (3966) (59) abnormal bladder shape (1066)(152) bladder wall irregularities (152) bladder masses(15) and bladder calcification (15) (Table 2) Bladderwall thickness the most common abnormality was recordedin 4679 (582) males and 90178 (506) females (Table 3)Among the participants 56 (848) with bladder pathologiesalso had an existing schistosomiasis infection 48 (873) ofwhich were light intensity and 8 (727) of which were heavyintensity 1205942 = 2675 119875 = 0001 (Table 5) Thus there was anassociation between urinary tract pathology and the intensityof S haematobium infection (1205942 = 3754 119875 = 0001 Table 2)Among the participants with light and heavy intensity of Shaematobium infections bladder wall thickness was the mostcommon bladder structural pathology identified in 3356
Journal of Tropical Medicine 3
Table 2 Distribution of bladder pathology with intensity of Shaematobium infection
Pathology1205942
= 3754 119875 = 0001Intensity of infection Total
Light () Heavy ()Bladder wallthickness 33 (589) 6 (600) 59
Bladder shape 8 (143) 2 (200) 152Bladder wallirregularity 8 (143) 2 (200) 152
Bladder mass 0 (0) 1 (100) 15Calcification 0 (0) 1 (100) 15Polyps mdash mdash mdashHydronephrosis 6 (107) 0 (0) 9
Table 3 Distribution of bladder pathology among genders
Pathology GenderMale Female
Bladder wall thickness 46 (582) 90 (506)Bladder shape 7 (89) 6 (34)Bladder wall irregularity 7 (89) 6 (34)Bladder mass mdash 1 (06)Calcification mdash 1 (06)Polyps mdash mdashHydronephrosis mdash 6 (34)
(589) and 6 (600) participants with light and heavyS haematobium infections respectively (Table 5) Abnormalbladder shape and bladder wall irregularity were seen in 856(143) and 2 (20) participants with light and heavy infec-tions respectively (Figures 1ndash3) Hydronephrosis was presentin only one participantwith light infection while calcificationwas identified in only one participant with heavy infectionNo bladder polyp was detected Mild bladder pathology wasmore common than severe bladder pathology in this studyand was found in 48 of the participants (Table 5) Therewas a higher incidence of bladder pathologies among femaleparticipants (Table 3) bladdermass and hydronephrosis werealso seen only in female participants
There was no significant relationship between cigarettesmoking and bladder pathology in the study (Table 6)Among participants with bladder pathology 29 (333)admitted consuming alcohol while 58 (667) said that theyhad never consumed alcohol (Table 7)
4 Discussion
The overall prevalence rate (2598) of adults with Shaematobium infection recorded in this study was slightlyhigher than 208 and 200 reported in Yewa North LocalGovernment Ogun State andOwan East Local Governmentrespectively in Nigeria [3 13]
Most (813) of the participants depended solely on the Shaematobium contaminated river water which could accountfor the higher S haematobium prevalence and little or no
Figure 1 B mode ultrasound of the bladder showing a fullyextended bladder with no pathology
Figure 2 B mode ultrasound of the bladder showing a thickenedbladder wall (arrows)
Figure 3 Bladder with masses extending from the wall into thelumen (ignore speckled artefacts)
schistosomiasis control (drug) intervention targeted to adultshas been recorded in this area The higher frequency oflight intensity S haematobium infection observed in thisstudy could be explained by some level of acquired protectedimmunity by adults in that community due to chronicexposure to schistosomiasis Shiff et al [5] found that theproportion of egg-positive individuals falls progressively withage and is a feature in populations with lifelong exposureto the parasite Therefore chronicity of infections in older
4 Journal of Tropical Medicine
Table 4 Relative risk estimates of schistosomiasis with sources of water
Sources of water use1205942 = 4789 df = 2 119875 = 0091
Status of S haematobium infection TotalPositive Negative
Rivers 49 (790) 160 (889) 209 (843)Others 11 (177) 15 (81) 26 (105)Rivers and others 2 (32) 11 (59) 13 (52)Total 62 (1000) 186 248
Table 5 Relation between intensity of bladder pathologies and intensity of S haematobium infection
Intensity of Shaematobium infection1205942
= 2675 119875 = 0001
Intensity of bladder pathology Total119873 ()Mild
119873 ( )Severe119873 ()
Intensity of infectionHeavy 6 (909) 2 (30) 8 (121)Light 42 (6363) 6 (91) 48 (727)
Total 48 (6969) 8 (121) 56 (848)
Table 6 Relative risk estimates of bladder pathology associatedwithcigarette smoking
Cigarette smoking1205942
= 067119875 = 0880
Pathology Total119873 ()Present
119873 ()Absent119873 ()
No response 5 (57) 12 (71) 17 (58)Yes 4 (46) 5 (29) 9 (121)No 78 (897) 153 (900) 231 (821)Total 87 (339) 170 (661) 257
Table 7 Relative risk estimates of bladder pathology associatedwithalcohol consumption
Alcohol consumption1205942 = 3549 119875 = 0170
Bladder pathology TotalPresent Absent
Yes 29 (333) 72 (424) 101 (393)No 58 (667) 85 (50) 143 (556)No response 0 (57) 13 (76) 13 (51)
people will more likely be difficult to ascertain using eggcount method The higher frequency of mild bladder pathol-ogy observed in this study was also similar to another study[14] which observed a higher incidence of mild bladder thansevere bladder pathology This result could be explained bythe low number of participants who smoked cigarettes andconsumed alcohol these conditions may serve as promotingfactors either in progression of bladder pathology to canceror in making the bladder pathology more severe (Table 4)In addition this lifestyle could buttress the possibility ofS haematobium being the principal cause of the reportedbladder structural pathology in the study population
The close relationship between the intensity of S haema-tobium infection and the presence of bladder abnormalitieswas similar to previous reports [3 14ndash16] The presence
of hydronephrosis in participants with light infection ishowever at variance with the report of Nmorsi et al [3]although hydrocalycosis (a condition mostly mistaken forhydronephrosis) was observed in some patients with heavyinfection indicating the likely contribution of this infectionto kidney pathology Females (647) had more structuralbladder pathology compared to males (353) This may bedue to higher water contact by females and also to the highernumber of female study participants than an indication ofa female predilection to bladder pathology However sincehydronephrosis and bladder mass or bladder calculi werefound together in a female participant female predilectionto bladder pathology may not completely be ruled out Thestructural changes to the bladder recorded in this studywere in consonance with observations in West Madagascar[14] and Nigeria [3 15] where bladder irregularities andbladder wall thickness were identified as the most commonpathologies in individuals infected with S haematobium
In conclusion there is evidence that S haematobiuminfections may be associated with bladder pathology onultrasound examination Individuals with bladder patholo-gies could have heavy or light intensity of schistosomiasisinfection or have no existing infection at all However along term exposure to schistosomiasis is necessary for thedevelopment of bladder cancer Further research on thedeterminants and progress of the bladder pathologies seen inthis study population is needed
Competing Interests
The authors declare that they have no competing interests
References
[1] U S Ugbomoiko I E Ofoezie I C Okoye and J HeukelbachldquoFactors associated with urinary schistosomiasis in two peri-urban communities in south-western Nigeriardquo Annals of Tropi-cal Medicine amp Parasitology vol 104 no 5 pp 409ndash419 2010
Journal of Tropical Medicine 5
[2] P F Rambau P L Chalya and K Jackson ldquoSchistosomiasis andurinary bladder cancer inNorthWestern Tanzania a retrospec-tive review of 185 patientsrdquo Infectious Agents and Cancer vol 8article 19 2013
[3] O P G Nmorsi N C D Ukwandu S Ogoinja H O TBlackie and M A C Odike ldquoUrinary tract pathology in someSchistosoma haematobium infected Nigeriansrdquo African Journalof Biotechnology vol 6 no 2 pp 123ndash127 2007
[4] M C Botelho J C Machado and J M C da Costa ldquoSchis-tosoma haematobium and bladder cancer what lies beneathrdquoVirulence vol 1 no 2 pp 84ndash87 2010
[5] C Shiff R Veltri J Naples et al ldquoUltrasound verificationof bladder damage is associated with known biomarkers ofbladder cancer in adults chronically infected with Schistosomahaematobium in Ghanardquo Transactions of the Royal Society ofTropical Medicine and Hygiene vol 100 no 9 pp 847ndash8542006
[6] P J Hotez P J Brindley J M Bethony C H King E J Pearceand J Jacobson ldquoHelminth infections the great neglectedtropical diseasesrdquo Journal of Clinical Investigation vol 118 no4 pp 1311ndash1321 2008
[7] I J Agere W A Istifanus and S L Kela ldquoWater usage andtransmission of Schistosoma haematobium in jalingo and ardok-ola local governmentareas of Taraba State Nigeriardquo NigerianJournal of Science Technology and Environmental Education(NIJOSTEE) vol 3 no 1 2010
[8] O M Agbolade and A Odaibo ldquoSchistosoma haematobiuminfection among pupils and snail intermediate hosts in Ago-Iwoye Ogun StaterdquoThe Nigerian Journal of Parasitology vol 17pp 17ndash21 1996
[9] A Hassan N Uduak O Morenikeji et al ldquoUrine turbidityand microhaematuria as rapid assessment indicators for schis-tosoma haematobium infection among school children inendemic areasrdquo American Journal of Infectious Diseases vol 8no 1 pp 60ndash64 2012
[10] M D Weber D M Blair and V V Clark ldquoThe pattern ofschistosome egg distribution in a micturition flowrdquo CentralAfrican Journal of Medicine vol 13 no 4 pp 75ndash88 1967
[11] WHO ldquoMeeting on ultrasonography in schistosomiasis pro-posal for a practical guide to the standardized use of ultrasoundin assessment of pathological changesrdquo TDRSCHUltrason913 World Health Organization Geneva Switzerland 1996
[12] World Health Organization (WHO) ldquoUltrasound in schistoso-miasis A practical guide to the standardized use of ultrasonog-raphy for assessment of schistosomiasis-related morbidityrdquoTech Rep TDRSTRSCH001 World Health Organization(WHO) Geneva Switzerland 2000
[13] O T Salawu and A B Odaibo ldquoSchistosomiasis among preg-nant women in rural communities in Nigeriardquo InternationalJournal of Gynecology andObstetrics vol 122 no 1 pp 1ndash4 2013
[14] J Serieye P Boisier V E Ravaoalimalala et al ldquoSchistosomahaematobium infection in western Madagascar morbiditydetermined by ultrasonographyrdquo Transactions of the RoyalSociety of Tropical Medicine and Hygiene vol 90 no 4 pp 398ndash401 1996
[15] C A Ekwunife F C Okafor and O C Nwaorgu ldquoUltrasono-graphic screening of urinary schistosomiasis infected patientsin Agulu community Anambra state southeast Nigeriardquo Inter-national Archives of Medicine vol 2 no 1 article 34 2009
[16] K SWarren A A FMahmoud J FMuruka L RWhittaker JH Ouma and T K Arap Siongok ldquoSchistosomiasis haematobia
in Coast Province Kenya Relationship between egg output andmorbidityrdquo American Journal of Tropical Medicine and Hygienevol 28 no 5 pp 864ndash870 1979
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Journal of Tropical Medicine 3
Table 2 Distribution of bladder pathology with intensity of Shaematobium infection
Pathology1205942
= 3754 119875 = 0001Intensity of infection Total
Light () Heavy ()Bladder wallthickness 33 (589) 6 (600) 59
Bladder shape 8 (143) 2 (200) 152Bladder wallirregularity 8 (143) 2 (200) 152
Bladder mass 0 (0) 1 (100) 15Calcification 0 (0) 1 (100) 15Polyps mdash mdash mdashHydronephrosis 6 (107) 0 (0) 9
Table 3 Distribution of bladder pathology among genders
Pathology GenderMale Female
Bladder wall thickness 46 (582) 90 (506)Bladder shape 7 (89) 6 (34)Bladder wall irregularity 7 (89) 6 (34)Bladder mass mdash 1 (06)Calcification mdash 1 (06)Polyps mdash mdashHydronephrosis mdash 6 (34)
(589) and 6 (600) participants with light and heavyS haematobium infections respectively (Table 5) Abnormalbladder shape and bladder wall irregularity were seen in 856(143) and 2 (20) participants with light and heavy infec-tions respectively (Figures 1ndash3) Hydronephrosis was presentin only one participantwith light infection while calcificationwas identified in only one participant with heavy infectionNo bladder polyp was detected Mild bladder pathology wasmore common than severe bladder pathology in this studyand was found in 48 of the participants (Table 5) Therewas a higher incidence of bladder pathologies among femaleparticipants (Table 3) bladdermass and hydronephrosis werealso seen only in female participants
There was no significant relationship between cigarettesmoking and bladder pathology in the study (Table 6)Among participants with bladder pathology 29 (333)admitted consuming alcohol while 58 (667) said that theyhad never consumed alcohol (Table 7)
4 Discussion
The overall prevalence rate (2598) of adults with Shaematobium infection recorded in this study was slightlyhigher than 208 and 200 reported in Yewa North LocalGovernment Ogun State andOwan East Local Governmentrespectively in Nigeria [3 13]
Most (813) of the participants depended solely on the Shaematobium contaminated river water which could accountfor the higher S haematobium prevalence and little or no
Figure 1 B mode ultrasound of the bladder showing a fullyextended bladder with no pathology
Figure 2 B mode ultrasound of the bladder showing a thickenedbladder wall (arrows)
Figure 3 Bladder with masses extending from the wall into thelumen (ignore speckled artefacts)
schistosomiasis control (drug) intervention targeted to adultshas been recorded in this area The higher frequency oflight intensity S haematobium infection observed in thisstudy could be explained by some level of acquired protectedimmunity by adults in that community due to chronicexposure to schistosomiasis Shiff et al [5] found that theproportion of egg-positive individuals falls progressively withage and is a feature in populations with lifelong exposureto the parasite Therefore chronicity of infections in older
4 Journal of Tropical Medicine
Table 4 Relative risk estimates of schistosomiasis with sources of water
Sources of water use1205942 = 4789 df = 2 119875 = 0091
Status of S haematobium infection TotalPositive Negative
Rivers 49 (790) 160 (889) 209 (843)Others 11 (177) 15 (81) 26 (105)Rivers and others 2 (32) 11 (59) 13 (52)Total 62 (1000) 186 248
Table 5 Relation between intensity of bladder pathologies and intensity of S haematobium infection
Intensity of Shaematobium infection1205942
= 2675 119875 = 0001
Intensity of bladder pathology Total119873 ()Mild
119873 ( )Severe119873 ()
Intensity of infectionHeavy 6 (909) 2 (30) 8 (121)Light 42 (6363) 6 (91) 48 (727)
Total 48 (6969) 8 (121) 56 (848)
Table 6 Relative risk estimates of bladder pathology associatedwithcigarette smoking
Cigarette smoking1205942
= 067119875 = 0880
Pathology Total119873 ()Present
119873 ()Absent119873 ()
No response 5 (57) 12 (71) 17 (58)Yes 4 (46) 5 (29) 9 (121)No 78 (897) 153 (900) 231 (821)Total 87 (339) 170 (661) 257
Table 7 Relative risk estimates of bladder pathology associatedwithalcohol consumption
Alcohol consumption1205942 = 3549 119875 = 0170
Bladder pathology TotalPresent Absent
Yes 29 (333) 72 (424) 101 (393)No 58 (667) 85 (50) 143 (556)No response 0 (57) 13 (76) 13 (51)
people will more likely be difficult to ascertain using eggcount method The higher frequency of mild bladder pathol-ogy observed in this study was also similar to another study[14] which observed a higher incidence of mild bladder thansevere bladder pathology This result could be explained bythe low number of participants who smoked cigarettes andconsumed alcohol these conditions may serve as promotingfactors either in progression of bladder pathology to canceror in making the bladder pathology more severe (Table 4)In addition this lifestyle could buttress the possibility ofS haematobium being the principal cause of the reportedbladder structural pathology in the study population
The close relationship between the intensity of S haema-tobium infection and the presence of bladder abnormalitieswas similar to previous reports [3 14ndash16] The presence
of hydronephrosis in participants with light infection ishowever at variance with the report of Nmorsi et al [3]although hydrocalycosis (a condition mostly mistaken forhydronephrosis) was observed in some patients with heavyinfection indicating the likely contribution of this infectionto kidney pathology Females (647) had more structuralbladder pathology compared to males (353) This may bedue to higher water contact by females and also to the highernumber of female study participants than an indication ofa female predilection to bladder pathology However sincehydronephrosis and bladder mass or bladder calculi werefound together in a female participant female predilectionto bladder pathology may not completely be ruled out Thestructural changes to the bladder recorded in this studywere in consonance with observations in West Madagascar[14] and Nigeria [3 15] where bladder irregularities andbladder wall thickness were identified as the most commonpathologies in individuals infected with S haematobium
In conclusion there is evidence that S haematobiuminfections may be associated with bladder pathology onultrasound examination Individuals with bladder patholo-gies could have heavy or light intensity of schistosomiasisinfection or have no existing infection at all However along term exposure to schistosomiasis is necessary for thedevelopment of bladder cancer Further research on thedeterminants and progress of the bladder pathologies seen inthis study population is needed
Competing Interests
The authors declare that they have no competing interests
References
[1] U S Ugbomoiko I E Ofoezie I C Okoye and J HeukelbachldquoFactors associated with urinary schistosomiasis in two peri-urban communities in south-western Nigeriardquo Annals of Tropi-cal Medicine amp Parasitology vol 104 no 5 pp 409ndash419 2010
Journal of Tropical Medicine 5
[2] P F Rambau P L Chalya and K Jackson ldquoSchistosomiasis andurinary bladder cancer inNorthWestern Tanzania a retrospec-tive review of 185 patientsrdquo Infectious Agents and Cancer vol 8article 19 2013
[3] O P G Nmorsi N C D Ukwandu S Ogoinja H O TBlackie and M A C Odike ldquoUrinary tract pathology in someSchistosoma haematobium infected Nigeriansrdquo African Journalof Biotechnology vol 6 no 2 pp 123ndash127 2007
[4] M C Botelho J C Machado and J M C da Costa ldquoSchis-tosoma haematobium and bladder cancer what lies beneathrdquoVirulence vol 1 no 2 pp 84ndash87 2010
[5] C Shiff R Veltri J Naples et al ldquoUltrasound verificationof bladder damage is associated with known biomarkers ofbladder cancer in adults chronically infected with Schistosomahaematobium in Ghanardquo Transactions of the Royal Society ofTropical Medicine and Hygiene vol 100 no 9 pp 847ndash8542006
[6] P J Hotez P J Brindley J M Bethony C H King E J Pearceand J Jacobson ldquoHelminth infections the great neglectedtropical diseasesrdquo Journal of Clinical Investigation vol 118 no4 pp 1311ndash1321 2008
[7] I J Agere W A Istifanus and S L Kela ldquoWater usage andtransmission of Schistosoma haematobium in jalingo and ardok-ola local governmentareas of Taraba State Nigeriardquo NigerianJournal of Science Technology and Environmental Education(NIJOSTEE) vol 3 no 1 2010
[8] O M Agbolade and A Odaibo ldquoSchistosoma haematobiuminfection among pupils and snail intermediate hosts in Ago-Iwoye Ogun StaterdquoThe Nigerian Journal of Parasitology vol 17pp 17ndash21 1996
[9] A Hassan N Uduak O Morenikeji et al ldquoUrine turbidityand microhaematuria as rapid assessment indicators for schis-tosoma haematobium infection among school children inendemic areasrdquo American Journal of Infectious Diseases vol 8no 1 pp 60ndash64 2012
[10] M D Weber D M Blair and V V Clark ldquoThe pattern ofschistosome egg distribution in a micturition flowrdquo CentralAfrican Journal of Medicine vol 13 no 4 pp 75ndash88 1967
[11] WHO ldquoMeeting on ultrasonography in schistosomiasis pro-posal for a practical guide to the standardized use of ultrasoundin assessment of pathological changesrdquo TDRSCHUltrason913 World Health Organization Geneva Switzerland 1996
[12] World Health Organization (WHO) ldquoUltrasound in schistoso-miasis A practical guide to the standardized use of ultrasonog-raphy for assessment of schistosomiasis-related morbidityrdquoTech Rep TDRSTRSCH001 World Health Organization(WHO) Geneva Switzerland 2000
[13] O T Salawu and A B Odaibo ldquoSchistosomiasis among preg-nant women in rural communities in Nigeriardquo InternationalJournal of Gynecology andObstetrics vol 122 no 1 pp 1ndash4 2013
[14] J Serieye P Boisier V E Ravaoalimalala et al ldquoSchistosomahaematobium infection in western Madagascar morbiditydetermined by ultrasonographyrdquo Transactions of the RoyalSociety of Tropical Medicine and Hygiene vol 90 no 4 pp 398ndash401 1996
[15] C A Ekwunife F C Okafor and O C Nwaorgu ldquoUltrasono-graphic screening of urinary schistosomiasis infected patientsin Agulu community Anambra state southeast Nigeriardquo Inter-national Archives of Medicine vol 2 no 1 article 34 2009
[16] K SWarren A A FMahmoud J FMuruka L RWhittaker JH Ouma and T K Arap Siongok ldquoSchistosomiasis haematobia
in Coast Province Kenya Relationship between egg output andmorbidityrdquo American Journal of Tropical Medicine and Hygienevol 28 no 5 pp 864ndash870 1979
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
4 Journal of Tropical Medicine
Table 4 Relative risk estimates of schistosomiasis with sources of water
Sources of water use1205942 = 4789 df = 2 119875 = 0091
Status of S haematobium infection TotalPositive Negative
Rivers 49 (790) 160 (889) 209 (843)Others 11 (177) 15 (81) 26 (105)Rivers and others 2 (32) 11 (59) 13 (52)Total 62 (1000) 186 248
Table 5 Relation between intensity of bladder pathologies and intensity of S haematobium infection
Intensity of Shaematobium infection1205942
= 2675 119875 = 0001
Intensity of bladder pathology Total119873 ()Mild
119873 ( )Severe119873 ()
Intensity of infectionHeavy 6 (909) 2 (30) 8 (121)Light 42 (6363) 6 (91) 48 (727)
Total 48 (6969) 8 (121) 56 (848)
Table 6 Relative risk estimates of bladder pathology associatedwithcigarette smoking
Cigarette smoking1205942
= 067119875 = 0880
Pathology Total119873 ()Present
119873 ()Absent119873 ()
No response 5 (57) 12 (71) 17 (58)Yes 4 (46) 5 (29) 9 (121)No 78 (897) 153 (900) 231 (821)Total 87 (339) 170 (661) 257
Table 7 Relative risk estimates of bladder pathology associatedwithalcohol consumption
Alcohol consumption1205942 = 3549 119875 = 0170
Bladder pathology TotalPresent Absent
Yes 29 (333) 72 (424) 101 (393)No 58 (667) 85 (50) 143 (556)No response 0 (57) 13 (76) 13 (51)
people will more likely be difficult to ascertain using eggcount method The higher frequency of mild bladder pathol-ogy observed in this study was also similar to another study[14] which observed a higher incidence of mild bladder thansevere bladder pathology This result could be explained bythe low number of participants who smoked cigarettes andconsumed alcohol these conditions may serve as promotingfactors either in progression of bladder pathology to canceror in making the bladder pathology more severe (Table 4)In addition this lifestyle could buttress the possibility ofS haematobium being the principal cause of the reportedbladder structural pathology in the study population
The close relationship between the intensity of S haema-tobium infection and the presence of bladder abnormalitieswas similar to previous reports [3 14ndash16] The presence
of hydronephrosis in participants with light infection ishowever at variance with the report of Nmorsi et al [3]although hydrocalycosis (a condition mostly mistaken forhydronephrosis) was observed in some patients with heavyinfection indicating the likely contribution of this infectionto kidney pathology Females (647) had more structuralbladder pathology compared to males (353) This may bedue to higher water contact by females and also to the highernumber of female study participants than an indication ofa female predilection to bladder pathology However sincehydronephrosis and bladder mass or bladder calculi werefound together in a female participant female predilectionto bladder pathology may not completely be ruled out Thestructural changes to the bladder recorded in this studywere in consonance with observations in West Madagascar[14] and Nigeria [3 15] where bladder irregularities andbladder wall thickness were identified as the most commonpathologies in individuals infected with S haematobium
In conclusion there is evidence that S haematobiuminfections may be associated with bladder pathology onultrasound examination Individuals with bladder patholo-gies could have heavy or light intensity of schistosomiasisinfection or have no existing infection at all However along term exposure to schistosomiasis is necessary for thedevelopment of bladder cancer Further research on thedeterminants and progress of the bladder pathologies seen inthis study population is needed
Competing Interests
The authors declare that they have no competing interests
References
[1] U S Ugbomoiko I E Ofoezie I C Okoye and J HeukelbachldquoFactors associated with urinary schistosomiasis in two peri-urban communities in south-western Nigeriardquo Annals of Tropi-cal Medicine amp Parasitology vol 104 no 5 pp 409ndash419 2010
Journal of Tropical Medicine 5
[2] P F Rambau P L Chalya and K Jackson ldquoSchistosomiasis andurinary bladder cancer inNorthWestern Tanzania a retrospec-tive review of 185 patientsrdquo Infectious Agents and Cancer vol 8article 19 2013
[3] O P G Nmorsi N C D Ukwandu S Ogoinja H O TBlackie and M A C Odike ldquoUrinary tract pathology in someSchistosoma haematobium infected Nigeriansrdquo African Journalof Biotechnology vol 6 no 2 pp 123ndash127 2007
[4] M C Botelho J C Machado and J M C da Costa ldquoSchis-tosoma haematobium and bladder cancer what lies beneathrdquoVirulence vol 1 no 2 pp 84ndash87 2010
[5] C Shiff R Veltri J Naples et al ldquoUltrasound verificationof bladder damage is associated with known biomarkers ofbladder cancer in adults chronically infected with Schistosomahaematobium in Ghanardquo Transactions of the Royal Society ofTropical Medicine and Hygiene vol 100 no 9 pp 847ndash8542006
[6] P J Hotez P J Brindley J M Bethony C H King E J Pearceand J Jacobson ldquoHelminth infections the great neglectedtropical diseasesrdquo Journal of Clinical Investigation vol 118 no4 pp 1311ndash1321 2008
[7] I J Agere W A Istifanus and S L Kela ldquoWater usage andtransmission of Schistosoma haematobium in jalingo and ardok-ola local governmentareas of Taraba State Nigeriardquo NigerianJournal of Science Technology and Environmental Education(NIJOSTEE) vol 3 no 1 2010
[8] O M Agbolade and A Odaibo ldquoSchistosoma haematobiuminfection among pupils and snail intermediate hosts in Ago-Iwoye Ogun StaterdquoThe Nigerian Journal of Parasitology vol 17pp 17ndash21 1996
[9] A Hassan N Uduak O Morenikeji et al ldquoUrine turbidityand microhaematuria as rapid assessment indicators for schis-tosoma haematobium infection among school children inendemic areasrdquo American Journal of Infectious Diseases vol 8no 1 pp 60ndash64 2012
[10] M D Weber D M Blair and V V Clark ldquoThe pattern ofschistosome egg distribution in a micturition flowrdquo CentralAfrican Journal of Medicine vol 13 no 4 pp 75ndash88 1967
[11] WHO ldquoMeeting on ultrasonography in schistosomiasis pro-posal for a practical guide to the standardized use of ultrasoundin assessment of pathological changesrdquo TDRSCHUltrason913 World Health Organization Geneva Switzerland 1996
[12] World Health Organization (WHO) ldquoUltrasound in schistoso-miasis A practical guide to the standardized use of ultrasonog-raphy for assessment of schistosomiasis-related morbidityrdquoTech Rep TDRSTRSCH001 World Health Organization(WHO) Geneva Switzerland 2000
[13] O T Salawu and A B Odaibo ldquoSchistosomiasis among preg-nant women in rural communities in Nigeriardquo InternationalJournal of Gynecology andObstetrics vol 122 no 1 pp 1ndash4 2013
[14] J Serieye P Boisier V E Ravaoalimalala et al ldquoSchistosomahaematobium infection in western Madagascar morbiditydetermined by ultrasonographyrdquo Transactions of the RoyalSociety of Tropical Medicine and Hygiene vol 90 no 4 pp 398ndash401 1996
[15] C A Ekwunife F C Okafor and O C Nwaorgu ldquoUltrasono-graphic screening of urinary schistosomiasis infected patientsin Agulu community Anambra state southeast Nigeriardquo Inter-national Archives of Medicine vol 2 no 1 article 34 2009
[16] K SWarren A A FMahmoud J FMuruka L RWhittaker JH Ouma and T K Arap Siongok ldquoSchistosomiasis haematobia
in Coast Province Kenya Relationship between egg output andmorbidityrdquo American Journal of Tropical Medicine and Hygienevol 28 no 5 pp 864ndash870 1979
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Journal of Tropical Medicine 5
[2] P F Rambau P L Chalya and K Jackson ldquoSchistosomiasis andurinary bladder cancer inNorthWestern Tanzania a retrospec-tive review of 185 patientsrdquo Infectious Agents and Cancer vol 8article 19 2013
[3] O P G Nmorsi N C D Ukwandu S Ogoinja H O TBlackie and M A C Odike ldquoUrinary tract pathology in someSchistosoma haematobium infected Nigeriansrdquo African Journalof Biotechnology vol 6 no 2 pp 123ndash127 2007
[4] M C Botelho J C Machado and J M C da Costa ldquoSchis-tosoma haematobium and bladder cancer what lies beneathrdquoVirulence vol 1 no 2 pp 84ndash87 2010
[5] C Shiff R Veltri J Naples et al ldquoUltrasound verificationof bladder damage is associated with known biomarkers ofbladder cancer in adults chronically infected with Schistosomahaematobium in Ghanardquo Transactions of the Royal Society ofTropical Medicine and Hygiene vol 100 no 9 pp 847ndash8542006
[6] P J Hotez P J Brindley J M Bethony C H King E J Pearceand J Jacobson ldquoHelminth infections the great neglectedtropical diseasesrdquo Journal of Clinical Investigation vol 118 no4 pp 1311ndash1321 2008
[7] I J Agere W A Istifanus and S L Kela ldquoWater usage andtransmission of Schistosoma haematobium in jalingo and ardok-ola local governmentareas of Taraba State Nigeriardquo NigerianJournal of Science Technology and Environmental Education(NIJOSTEE) vol 3 no 1 2010
[8] O M Agbolade and A Odaibo ldquoSchistosoma haematobiuminfection among pupils and snail intermediate hosts in Ago-Iwoye Ogun StaterdquoThe Nigerian Journal of Parasitology vol 17pp 17ndash21 1996
[9] A Hassan N Uduak O Morenikeji et al ldquoUrine turbidityand microhaematuria as rapid assessment indicators for schis-tosoma haematobium infection among school children inendemic areasrdquo American Journal of Infectious Diseases vol 8no 1 pp 60ndash64 2012
[10] M D Weber D M Blair and V V Clark ldquoThe pattern ofschistosome egg distribution in a micturition flowrdquo CentralAfrican Journal of Medicine vol 13 no 4 pp 75ndash88 1967
[11] WHO ldquoMeeting on ultrasonography in schistosomiasis pro-posal for a practical guide to the standardized use of ultrasoundin assessment of pathological changesrdquo TDRSCHUltrason913 World Health Organization Geneva Switzerland 1996
[12] World Health Organization (WHO) ldquoUltrasound in schistoso-miasis A practical guide to the standardized use of ultrasonog-raphy for assessment of schistosomiasis-related morbidityrdquoTech Rep TDRSTRSCH001 World Health Organization(WHO) Geneva Switzerland 2000
[13] O T Salawu and A B Odaibo ldquoSchistosomiasis among preg-nant women in rural communities in Nigeriardquo InternationalJournal of Gynecology andObstetrics vol 122 no 1 pp 1ndash4 2013
[14] J Serieye P Boisier V E Ravaoalimalala et al ldquoSchistosomahaematobium infection in western Madagascar morbiditydetermined by ultrasonographyrdquo Transactions of the RoyalSociety of Tropical Medicine and Hygiene vol 90 no 4 pp 398ndash401 1996
[15] C A Ekwunife F C Okafor and O C Nwaorgu ldquoUltrasono-graphic screening of urinary schistosomiasis infected patientsin Agulu community Anambra state southeast Nigeriardquo Inter-national Archives of Medicine vol 2 no 1 article 34 2009
[16] K SWarren A A FMahmoud J FMuruka L RWhittaker JH Ouma and T K Arap Siongok ldquoSchistosomiasis haematobia
in Coast Province Kenya Relationship between egg output andmorbidityrdquo American Journal of Tropical Medicine and Hygienevol 28 no 5 pp 864ndash870 1979
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom