repair of mandibular prognathism associated with macroglossia: case report
TRANSCRIPT
REPAIR OF MANDIBULAR PROGNATHISM ASSOCIATED WITH MACROGLOSSIA: CASE REPORT
By J. P. SZLAZAK, M.D.
Regina, Saskatchewan
A PATIENT, aged 26, female, was referred by her dentist with the request that surgery be performed to correct the mandibular prognathism so that dentures could be fitted. She had lost all teeth at the age of I5, and since that time had lived on a soft and fluid diet.
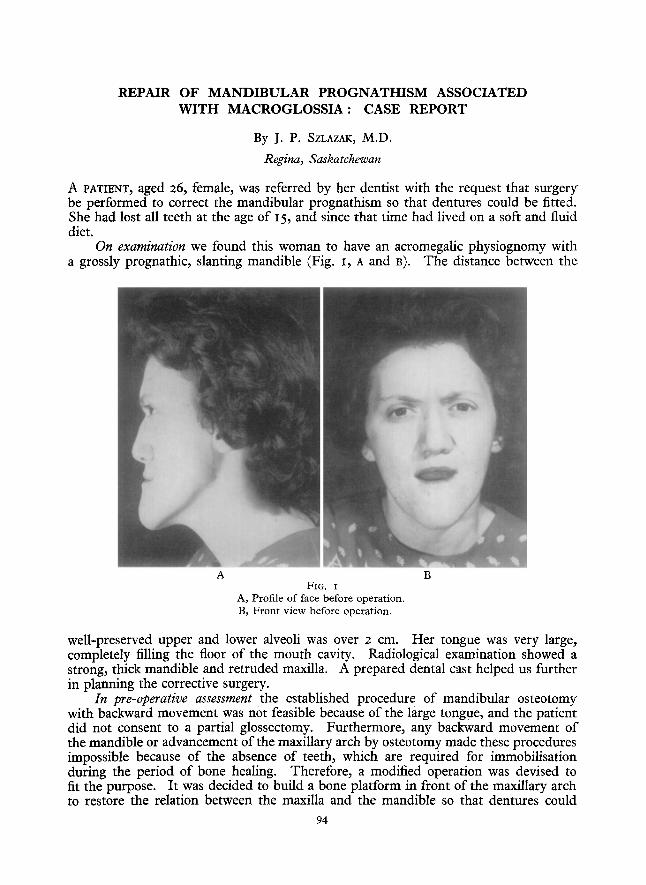
On examination we found this woman to have an acromegalic physiognomy with a grossly prognathic, slanting mandible (Fig. r, A and B). The distance between the
A B FIG. I
A, Profile of face before operation. B, Front view before operation.
well-preserved upper and lower alveoli was over 2 cm. Her tongue was very large, completely filling the floor of the mouth cavity. Radiological examination showed a strong, thick mandible and retruded maxilla. A prepared dental cast helped us further in planning the corrective surgery.
In pre-operative assessment the established procedure of mandibular osteotomy with backward movement was not feasible because of the large tongue, and the patient did not consent to a partial glossectomy. Furthermore, any backward movement of the mandible or advancement of the maxillary arch by osteotomy made these procedures impossible because of the absence of teeth, which are required for immobilisation during the period of bone healing. Therefore, a modified operation was devised to fit the purpose. It was decided to build a bone platform in front of the maxillary arch to restore the relation between the maxilla and the mandible so that dentures could
94
REPAIR OF MANDIBULAR PROGNATHISM 9~
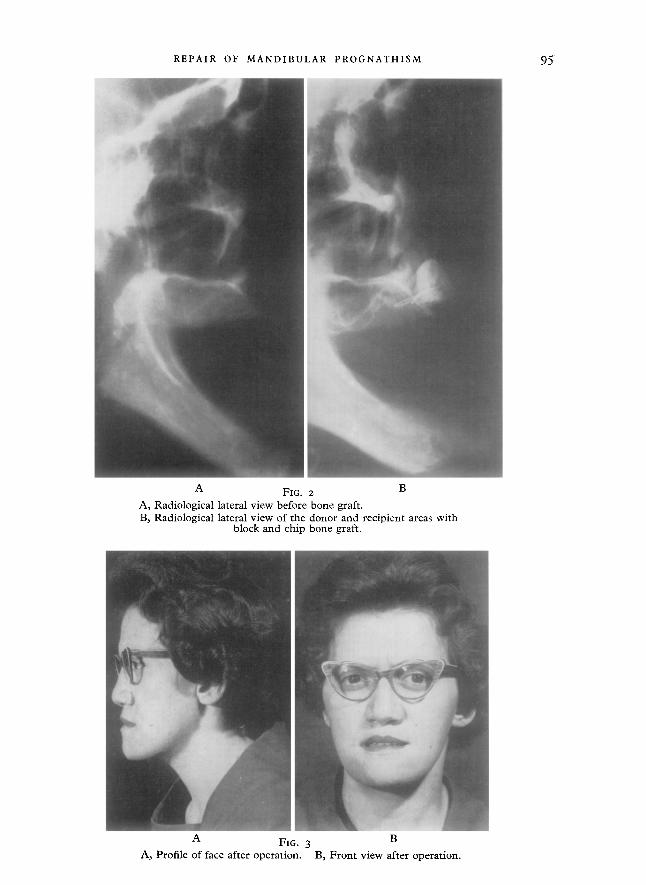
A FIG. 2 B A, Radiological lateral view before bone graft. B, Radiological lateral view of the donor and recipient areas with
block and chip bone graft.
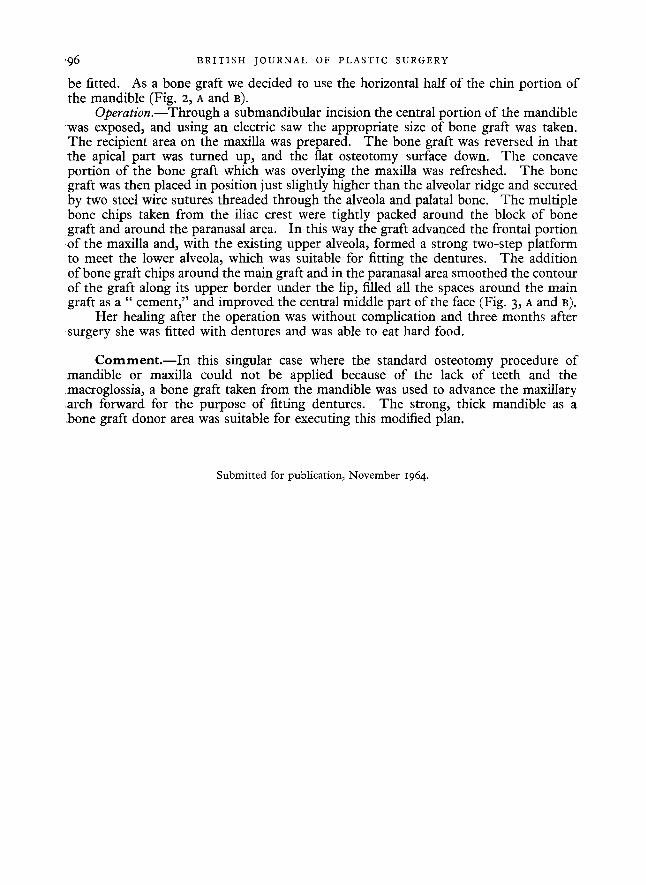
A FIG. 3 B A, Profile of face after operation. B, Front view after operation.
'96 B R I T I S H J O U R N A L OF P L A S T I C SURGERY
be fitted. As a bone graft we decided to use the horizontal half of the chin portion of the mandible (Fig. 2, A and B).
Operation.--Through a submandibular incision the central portion of the mandible was exposed, and using an electric saw the appropriate size of bone graft was taken. The recipient area on the maxilla was prepared. The bone graft was reversed in that the apical part was turned up, and the flat osteotomy surface down. The concave portion of the bone graft which was overlying the maxilla was refreshed. The bone graft was then placed in position just slightly higher than the alveolar ridge and secured by two steel wire sutures threaded through the alveola and palatal bone. The multiple bone chips taken from the iliac crest were tightly packed around the block of bone graft and around the paranasal area. In this way the graft advanced the frontal portion o f the maxilla and, with the existing upper alveola, formed a strong two-step platform to meet the lower alveola, which was suitable for fitting the dentures. The addition of bone graft chips around the main graft and in the paranasal area smoothed the contour of the graft along its upper border under the lip, filled all the spaces around the main graft as a " cement," and improved the central middle part of the face (Fig. 3, A and B).
Her healing after the operation was without complication and three months after surgery she was fitted with dentures and was able to eat hard food.
C o m m e n t . - - I n this singular case where the standard osteotomy procedure of mandible or maxilla could not be applied because of the lack of teeth and the macroglossia, a bone graft taken from the mandible was used to advance the maxillary arch forward for the purpose of fitting dentures. The strong, thick mandible as a bone graft donor area was suitable for executing this modified plan.
Submitted for publication, November 1964.