renal transplant: anaesthetic implications & considerations
TRANSCRIPT
RENAL TRANSPLANT
Dr. Sandeep B. More
Essential functions of kidney :
1) regulate ionic composition of plasma
2) maintain fluid volume
3) elimination of nitrogenous wastes and drugs
4) Erythropoetin production
5) maintenance of pH
First kidney transplant in 1950
Indications of renal transplant:
Patients with Chronic kidney disease or End Stage Renal Disease (ESRD) caused by 1) DM 31% 2) CGN 28% 3)polycystic kidney 12% 4)hypertension 9% 5) SLE 3% 6)interstitial nephritis 7) smoking 8) tuberculosis 9) HIV, HEP B & C 10) lead, cadmium, mercury
Renal graft failure is a new indication for renal transplant .
What is ESRD: it is final progression of chronic kidney disease when renal function is irreversibly impaired and can be fatal without RRT(GFR < 25%)
Uremic syndrome : Extreme form of CRF with GFR < 10% regulation of ECF volume & composition and excretion of waste products hampered that cause1) Water homeostasis alterations causing : ECF expansion2) Electrolyte & acid base disturbances cause : Hyponatremia, hyperkalemia, hyper/hypo calcemia, hyperphosphatemia, hypermagnesemia, metabolic acidosis3) Endocrine changes cause : renal osteodystrophy, decreased glucose intolerance, hypertriglyceridemia, atherosclerosis
ESRD Pathophysiology:
Indications for Dialysis
1) GFR <10 without DM
2) GFR<15 with DM,
3) Uremic syndrome (nausea, vomiting, wt loss, pericarditis, pleuritis),
4) Potassium >6 mEq/L with ECG changes
5) CCF
6) metabolic acidosis
ESRD and CVS: Cardiovascular disease is the most common cause of
morbidity and mortality in patients with ESRD
35-40% of deaths in pts on HD
Even after renal transplant cardio vascular disease remains the most common cause of death in the form of:
1) MI 2) CCF 3) atrial fibrillation
ESRD causes increased atherosclerosis leading toischemic vascular disease coronary, cerebral or peripheral vascular diseases
And the incidence is more in pts with DM and HTN
HTN causes ESRD in 30% pts
ESRD leads to hyper-reninemia, hypervolemia, renal vascular changes finally leading to HTN
2DECHO: concentric LVH and diastolic dysfunction(early and common changes)
Heart failure due to dilated cardiomyopathy is also common
Cardio-renal syndromes 5 types: renal and cardiac interconnection
Correction of renal function by transplant improves systolic function and reverse LV dilatation and hypertrophy
Arrhythmias: because of cardiac disease, MI, electrolyte imbalance
Atrial fibrillation most common (13 to 27%) stroke risk
Normochromic, normocytic anemia due to 1) EPO deficiency,2) nutritional (iron & folate), 3)chronic inflammatory state, 4)bone marrow fibrosis
Hb can be as low as 5-7mg/dl with Hct 15-25% Compensation by increased cardiac output & RBC 2,3 DPG shift
of O2 dissociation curve to right Hb target should be 10 mg/dl with drugs Avoid blood transfusion as far as possible to prevent
sensitization Platelet dysfunction (abnormal adhesion, aggregation),
decreased vWF & factor 8 coagulation disorders Increased coagulation & endothelial activation
hypercoagulable state
HEMATOLOGIC CHANGES OF HYPERCOAGULABILITY ARE RESOLVED AFTER SUCCESSFUL KIDNEY TRANSPLANT
Hematological
Gastrointestinal: nausea, vomiting, abdominal pain, decreased gastric motility(gastroparesis)
Delayed gastric emptying because of ESRD or presence of diabetes and obesity
These patients are considered always full stomach because of theses factors with increased risk of aspiration so they are the candidates for Rapid sequence induction for GA CNS: due to accumulation of nitrogenous products Memory loss, attention deficit, irritability Asterixis, seizures Uremia disrupts BBB
Muscle weakness, uremic osteodystrophy (osteomalacia, osteosclerosis, osteitis fibrosa cystica)Hypertriglyceridemia, carbohydrate intolerance, secondary hyperPTH, vit D deficiency
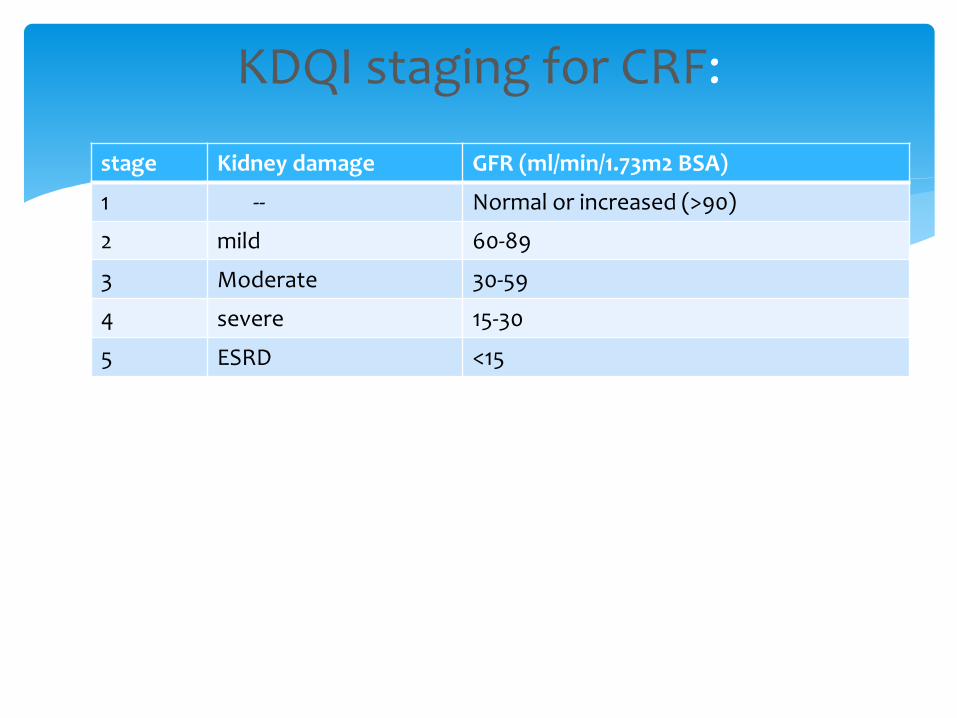
stage Kidney damage GFR (ml/min/1.73m2 BSA)
1 -- Normal or increased (>90)
2 mild 60-89
3 Moderate 30-59
4 severe 15-30
5 ESRD <15
KDQI staging for CRF:
It is an intermediate risk procedure in the AHA guidelines. Recipient undergoes a multidisciplinary assessment to determine the candidacy
Two types:
Cadaveric : urgent procedure as harvested kidney can tolerate cold ischemia only for less than 24 hrs
Living donor transplant: the ischemia time of harvested kidney can be less than one hour
So thorough preop assessmernt of the recipient and the donor can be done so as to minimize intraop and postop complications in both donor and recipient and to decrease incidence of graft rejection improving postop survival of the recipient
Nephrology, Medicine, cardiology, psychiatry, dental, gastromed(and OBGY for females)
Preop work up for renal transplant
HIV positive not absolute contraindication if stable on HAART, RNA negative, CD4> 200 cmm however if pt is diagnosed with AIDS then it is a contraindication for transplant
Other recommendations for prospective recipient:
Stop smoking
Weight reduction
BP control
Dental care
Exercise
Pre-op
Blood cross matching (recipient blood with donor blood cells)
Human leukocyte antigen (HLA) profile of recipient determined & compared with donor HLA
Blood Transfusion, prior transplantation and pregnancy lead to preformed antibodies positive cross matches against living donor tissue antigens PREOP PLASMAPHERESIS to remove these Abs & immunoglobulins living donor transplant is conducted when the cross match turns negative additional plasmapheresis and immunoglobulins to be given postop: hence blood transfusion is avoided as far as possible with anemia treated with hematinics and erythropoetin
Organ matching and allocation :
Ideal cadaveric donor : with prior family consent and registration
1. Age 5 to 49yrs
2. Nonhypertensive
3. Cause of death other than cerebrovascular accident
4. Creat <1.5
Expanded criteria : age 50 to 59 yrs with 2 additional risk factors i.e. hypertensive, CVA death or creat >1.5 to increase pool of donors
Donor criteria:
Living Donor:
surgeries scheduled simultaneously advantage is minimal ischemia time (<1 hour) immediate graft function, high UO, creat clearance
Exchange donor or kidney swap
Chain of paired kidney donations
Continue dialysis as per schedule
Dialysis before surgery : to be done in pts with increased intravascular volume, hyperkalemia, acidosis
CBC (platelet)
LFTs with enzymes
RFTs with electrolytes
PT/INR, aPTT
CXR
ECG
2D ECHO
Pre-requisites:
Pt typically undergoes dialysis within 48 hrs of surgery
Intravascular volume maybe assessed using their current weight and dry weight
Pt maybe hypovolemic and prone to hypotension if loss during dialysis is more than 2 kg
Preloading with non potassium containing saline or colloid maybe required if hypotension present
In case pt is hypervolemic then preloading can precipitate CCF
Monitors:
ECG
pulse oximeter
NIBP
IABP
CVP monitoring with central line
Urine output
Temperature monitoring
(AV fistula to be palpated and protected)
Preoperative:
Goals: adequate depth, hemodynamic stability, appropriate relaxationPreanesthetic medication:Diazepam : protein bound increased durationMidaz: water soluble can be usedAntacid (Na citrate 30 ml) and H2 blocker as pre anesthetic medicationsRapid sequence induction with cricoid pressure is recommended i/v/o incresedrisk of aspiration because of associated DM and obesity and delayed gastric emptying
Induction agent : Symp responses is blunted because of anti HTN t/t and diabetic autonomic neuropathy causing impaired vasoconstriction resulting in hypotension. Also because of preop dialysis pt can be hypovolemic and there is increased CNS sensitivity. All this make pt susceptible for hypotensive effects of induction agents. So induction agent should be given slowly and in lower dose to avoid hypotension.Pento : increased Vd & reduced protein binding reduce dosePropofol : use in low dose, advantage is reduced ischemia/reperfusion injuryKetamine : causes hypertension. To be used with cautionEtomidate : well tolerated, stable hemodynamics
Intra op management
Neuromuscular blocker:
1) Scoline can be used safely if potassium less than 5.5 mEq/l (hyperkalemia by 0.5 to 1.0 mEq/L for 10-15 mins)
2) Rocuronium 0.8-1.2 mg/kg IV is the best choice if sugammadex is available
To counteract DL scopy response : Opioids Fentanyl (2-5 mics/kg) Esmolol (0.5-1 mg/kg) Lignocaine 1-1.5 mg/kg Nitroglycerin
Blood sugar level monitoring perioperatively. And consider shift from OHA to Insulin if required and follow sliding scale intraop
Intra-op:
IV fluid: NS & NS based solutions to prevent hyperkalemia due to RL
NS can cause acidosis
Intraop targets
1) Systolic BP 130 – 160 mm Hg
2) CVP 12 to 14 mm Hg
3) Pulmponary artery pressure 18-20 mm Hg
Adequate IV fluid intra-op (30 ml/hr plus previous hour’s urine output): leads to earliest onset of graft function, low postop creat, higher postop creatclearance, improved graft survival
IV methylprednisolone after induction
Intra-op
Inhalational: Desflurane and Isoflurane not associated with nephrotoxicity
Sevoflurane : potentially nephrotoxic due to compound A and fluoride but no human data available
Analgesia: fentanyl 2-5 mic/kg
Relaxant : Atracurium 0.5 mg/kg , Cis-atracurium is best choice if available
Vec /Roc : prolonged action because hepatic and renal metabolism
Pancuronium: avoid because primary renal excretion
Forced air warmer or fluid warmer : to avoid hypothermia (temp <35 can l/t delayed recovery)
Maintenance of anesthesia:
Vertical curvilinear incision from pubic symphysis to ASIS 20-25 cm
External iliac vein and artery mobilized vein clamped first artery clamped anastomosis performed
Left kidney preferred as left renal vein is longer
Renal allograft is placed in Right extrarenal fossa
Furosemide and Mannitol before reperfusion
Mannitol and fluid avoid ATN
Adequate fluid increase blood flow improve immediate graft rejection
Surgical Procedure:
Vascular clamp removal acute bleeding/ release of inflammatory products accumulated cytokines, histamine vasodilatation hypotension hypotension f/b reperfusion hypoperfusion of graft vascular thrombosis of graft
T/t hypotension with fluid
Adrenergic vasopressors can cause renal vasoconstriction
Dopa : tachycardia, arrhythmias and MI
After vascular anastomoses donor graft ureter implanted in bladder (bladder filled with NS)
If recipient’s weight < 20 kg kidney placed intra-abdominally posterior to the right colon
In cadaveric donor transplant : aftere vascular anastomosis, intra-arterial papaverine/ verapamil is given to prevent arterial spasm then release arterial clamp
Donors younger than 2 yrs , both kidneys transplanted en bloc with donor’s aorta, which is then anastomosed to external iliac artery
Kidney cocktail : infused during vascular anastomosis in the recipient for cadaveric kidney: it consists of 600 ml of 0.45% dextrose in 0.45 % NS, 37.5 gm Albumin, 80 mg Frusemide, 37.5 gm Mannitol
Ischemia time : it starts with clamping of the renal vessels in the donor and ends with vascular anastomosis in the recipient
Shorter ischemia time better organ preservation
Warm ischemia time begins with clamping of renal vessels in the donor, it is interrupted by cold preservation solution and resumes again when the kidney is placed in the recipient and ends with the vascular anastomosis
Cold ischemia: kidney is preserved by storing at 4 degree celsius for less than 24 hrs
EXTUBATION:
Avoid extubation response to avoid coughing on tube
Extubation only after adequate reversal of neuromuscular blockade and presence of normal reflexes as they are prone for aspirations
Monitor : BP, UO, GCS, reflexes
Adequate fluid : CVP may decline 1-2 hrs after revascularization (25-50%) due to redistribution of fluids, changes of vascular permeability, increased nitric oxide levels
Postop complications : vascular thrombosis(1-2%), wound hematomas(1-2%), infection
Cardiac monitoring Pain: opioids preferred (avoid NSAIDs as may exacerbate HTN,
precipitate edema, increased CVS complications) Epidural : better analgesia but better avoided because of
presence of coagulopathy and increased incidence of hypotension
Preop TAP block Graft rejection : Interleukin 2 mediated activation of
lymphocytes is a critical factor in the cellular immune response of rejection
Post op management:
Post transplant: Pt is considered as stage 2 or 3 CKD as GFR >30 ml/min (GFR decrease by 1.4 – 2.4 ml/min/year)
Assess renal function
Rule out rejection
Cause of death : CVS
Survival : IHD, cerebrovascular and peripheral vascular disease
Immunosuppression: hyperlipidemia, HTN, diabetes
Obesity and metabolic syndromes
Post transplant malignancies, anemia, osteodystrophy
Post transplant pt for other surgery:
Infection: CMV (CMV negative blood if BT required)
Immunosuppressants : prevent acute and chronic T cell allo immune rejection. They may not present with typical signs & symptoms of intra abdominal sepsis such as fever, increased TLC, peritonitis signs
4 classes:
1. Corticosteroids
2. Calcineurine inhibitors (cyclosporine, tacrolimus)
3. Antimetabolites (mycophenolate mofetil, mycophenolate sodium, azathioprine)
4. Sirolimus (rapamycin inhibitor)
started in immediate preop period
Infections and immunosuppression:
Corticosteroids: In the early 1960s, Goodwin and Mims reported
that they had used corticosteroids to reverse acute rejection in a living-donor kidney transplant recipient. Starzl and Marchioro, in 1963, confirmed the efficacy with corticosteroids and the “almost miracle” effect. But over the years with recognition of severe irreversible side effects of corticosteroids and availability of newer and relatively safer drugs corticosteroids are not advocated now.
1]Calcineurin inhibitor : main stay
1)Cyclosporine : HTN, hyperlipidemia, hyperkalemia, hypomagnesemia, gum hypertrophy, nephrotoxicity with renal fibrosis. Lower seizure threshold (avoid hyperventilation), hirsutism
Potentiate NMB & post op respiratory failure
2)Tacrolimus : inhibits the formation of cytotoxic lymphocytes which are regarded as being primarily responsible for graft rejection.
Adv : less HTN & hyperlipidemia. Nephrotoxic but improves long term post-transplant renal function
S/E : DM, tremors, diarrhoea, neurotoxic
Both can cause chronic allograft nephropathy. In case of Acute rejection on cyclosporine switch over to tacrolimus can be considered
2] Antimetabolites : Mycophenolate mofetil : inhibits de novo purine synthesis in lymphocytes. No nephrotoxicity. Oral bioavailability 94%Side effects : diarrhoea,constipation, nausea, indigestion, fluid retentionAzathioprine : Used in combination with cyclosporin or tacrolimusor sirolimusSide effects; skin rash , myalgias, fever, headache, vomitingbone marrow suppression & pancytopenia
3) Sirolimus: inhibits T cell activation induced by most stimuli by blocking calcium dependent and calcium independent intracellular signal transduction. its effects are mediated by a mechanism that is different from that of cyclosporin, tacrolimus and other immunosuppressive agents.

THANK YOU