renal failure and renal replacement therapy
TRANSCRIPT
Renal failure and renal replacement therapy
Norma J. Maxvold, MDa, Timothy E. Bunchman, MDb,*aDepartment of Pediatric Critical Care, Children’s Hospital of Alabama,
University of Alabama at Birmingham, 1600 7th Avenue, Birmingham, AL 35233, USAbDepartment of Pediatric Nephrology and Transplantation, Children’s Hospital of Alabama,
University of Alabama at Birmingham, 1600 7th Avenue, Birmingham, AL 35233, USA
This article provides an overview of current knowledge, opinion, and evidence
to the extent that is currently available for approaching a child with acute renal
failure (ARF). Over the last 2 decades the treatment of ARF has changed
remarkably [1,2] because of generally improved care of children, a shift toward
continuous treatment modalities, research and advances in vascular access, and
the understanding that children with ARF usually have a high chance of recovery.
Acute renal failure often occurs in the face of multiorgan system failure (MOSF)
as a consequence of sepsis, solid or bone marrow transplantation, or acute
respiratory disease syndrome [2–4].
The authors present the shared perspective of a pediatric intensivist and a
pediatric nephrologist who have worked together for more than 10 years caring
for children with ARF and MOSF. They have reviewed current literature and
address what is known, what is bias, and what is open for research.
Pathophysiology
The causes of ARF can be divided into prerenal causes, intrarenal causes, and
postrenal causes [5]. In a child with MSOF, the cause is often multifactorial. In
the evaluation of a child with ARF, the obvious issue is to make certain that there
is adequate perfusion pressure and intravascular volume integrity with no
evidence of obstruction. In an examination report, this finding is often identified
as ‘‘warm, well-perfused with good blood pressure, good pulses, no evidence of
tense ascites, with a Foley catheter in place.’’ Laboratory results should provide
0749-0704/03/$ – see front matter D 2003 Elsevier Inc. All rights reserved.
doi:10.1016/S0749-0704(03)00010-1
* Corresponding author. Department of Pediatric Nephrology and Transplantation, Children’s
Hospital of Alabama, University of Alabama at Birmingham, CHT 735, 1600 7th Avenue,
Birmingham, AL 35233.
E-mail address: [email protected] (T.E. Bunchman).
Crit Care Clin 19 (2003) 563–575

evidence that a fractional excretion of sodium (FeNa) is not compatible with a
prerenal state (ie, low), with adequate osmolality and oncotic pressure and
without confounding variables that would result in an ongoing insult (ie, tumor
lysis syndrome or rhabdomyolysis), and with adequate volume resuscitation.
Etiology
There is no consensus regarding the definition of ARF. Many programs
consider a child as having ARF when there is a change from baseline levels of
more than 50% of serum creatinine or a blood nitrogen urea level above 40 mg/dL
or when urine output is insufficient to make accommodate medications, vaso-
pressor agents, or adequate nutrition. Because these definitions vary considerably
from program to program and from clinician to clinician, the decision concerning
the need for renal replacement therapy (RRT), as well as the overall care of the
child, varies considerably. During the past decade, many authors have addressed
the causes of ARF at admission to a pediatric ICU (PICU) or developing during
the stay in a PICU [2–4,6,7]. The population with ARF varies depending on the
author, the type of population served by the hospital, and the presence or absence
of programs in cardiac surgery program, extracorporeal membrane oxygenation
(ECMO), bone marrow transplantation, or solid-organ transplantation. The single
most common cause of ARF in children throughout the world continues to be
related to the hemolytic uremic syndrome (HUS) or volume depletion from
diarrhea-induced ARF with or without evidence of HUS [7]. Often these children
have been ill for a period of time before clinical identification of ARF, and poor
nutrition potentially affects their treatment and outcome.
Work by Menster et al [8] and Parekh et al [9] identified the typical causes of
ARF seen in economically developed societies as (1) previously unrecognized
congenital renal disease presenting as ARF and (2) toxic insults related to other
disease processes. In contrast, Goldstein et al [4] noted sepsis or shock as the
causes in their cohort of children who underwent hemofiltration for treatment of
ARF/MOSF. Therefore, the population surveyed influences the definition of ARF
as well as the decision concerning the need for RRT.
Options for renal replacement therapy
Before the late 1980s the options for RRT modality were limited to either
peritoneal dialysis or hemodialysis [1,10–12]. Since the initial paper by Ronco
et al [13] looking at continuous arterial venous hemofiltration (CAVH) in an
infant, the use of hemofiltration has become more common. This practice has
been further influenced by the newest generation of more user-friendly machines
that employ thermic controllers and more accurate ultrafiltration controllers.
Local experience and the clinical circumstances of the child mostly influence the
choice of peritoneal dialysis, hemodialysis, or hemofiltration. For example,
peritoneal dialysis is avoided in children with intra-abdominal catastrophes,
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575564
whereas hemodialysis or hemofiltration is precluded when vascular access is
unobtainable. Surveys within the pediatric nephrology literature over the past
6 years have confirmed clinicians’ experience of a trend away from peritoneal
dialysis toward hemofiltration when a continuous renal replacement therapy
(CRRT) is needed. Hemodialysis still remains the mainstay for the less sick child
with ARF and the therapy for the child with intoxication [1,14–17]. Because of
this trend, and because this article addresses the treatment of ARF in the PICU,
this discussion focuses on hemofiltration.
Hemofiltration for acute renal failure
The treatment of ARF with hemofiltration can be continuous arterial venous
hemofiltration with or without dialysis (CAVH[D]) or continuous veno-venous
hemofiltration with or without dialysis (CVVH[D]) [18,19]. Pediatric studies to
date have demonstrated the ease and simplicity of CAVH but have also demon-
strated the lack of obtainable prescription for CRRT when using CAVH [20].
Blood flow for CAVH depends on adequate cardiac output and is negatively
influenced by a high hematocrit, making CAVH mostly of historical interest.
Pump-assisted CVVH[D] is consider the standard for CRRT in children and
adults. This form of CRRT can be convective (CVVH), diffusive (CVVHD), or a
combination of both continuous veno-venous diahemofiltration (CVVHDF). The
choice between CVVH and CVVHD is often based on local standard, on the desire
for larger molecule clearance (improved with CVVH but dependent on the sieving
coefficient of the solute), and on the availability of replacement or dialysis
solutions. Data to date in both adults and children have shown when the
prescription is similar with the single variable of replacement or dialysate fluid,
urea clearance is similar [21]. Because the goal of most CRRT is to maintain
adequate volume status of the child, room for nutrition, and solute clearance, the
final decision of convective or diffusive treatment is often related to availability of
solutions for these therapies.
Access for continual renal replacement therapy
Access for CRRT depends on the size of the child, the necessary blood flow
rates, and, more recently, the choice of anticoagulation (Table 1). Access is needed
to maintain blood flow rates in the range of 10 to 70 mL/min in children weighing
less than 15 kg, 50 to 100 mL/min in children weighing 15 to 30 kg, and 100 too
250 mL/min in children weighing more than 30 kg. Dialysate or replacement fluid
becomes saturated with solute at commonly used rates of 2 L/hour (in contrast, the
dialysate flow rate in hemodialysis is 30–40 L/hour); therefore higher blood flow
rates have little effect on solute clearance and only tend to cause more alarms from
flow resistance. Triple-lumen access is helpful in the setting of inadequate
vascular access for the patient as well as in the setting of citrate anticoagulation
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575 565
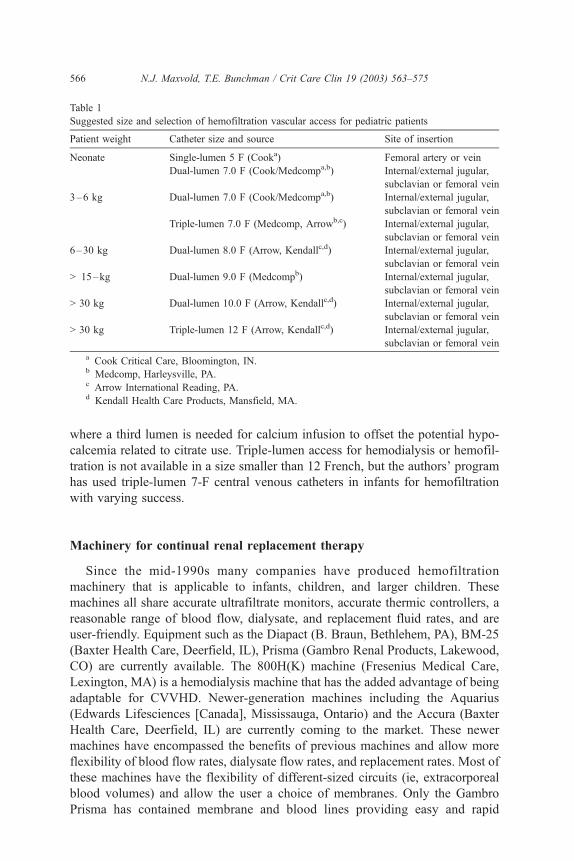
where a third lumen is needed for calcium infusion to offset the potential hypo-
calcemia related to citrate use. Triple-lumen access for hemodialysis or hemofil-
tration is not available in a size smaller than 12 French, but the authors’ program
has used triple-lumen 7-F central venous catheters in infants for hemofiltration
with varying success.
Machinery for continual renal replacement therapy
Since the mid-1990s many companies have produced hemofiltration
machinery that is applicable to infants, children, and larger children. These
machines all share accurate ultrafiltrate monitors, accurate thermic controllers, a
reasonable range of blood flow, dialysate, and replacement fluid rates, and are
user-friendly. Equipment such as the Diapact (B. Braun, Bethlehem, PA), BM-25
(Baxter Health Care, Deerfield, IL), Prisma (Gambro Renal Products, Lakewood,
CO) are currently available. The 800H(K) machine (Fresenius Medical Care,
Lexington, MA) is a hemodialysis machine that has the added advantage of being
adaptable for CVVHD. Newer-generation machines including the Aquarius
(Edwards Lifesciences [Canada], Mississauga, Ontario) and the Accura (Baxter
Health Care, Deerfield, IL) are currently coming to the market. These newer
machines have encompassed the benefits of previous machines and allow more
flexibility of blood flow rates, dialysate flow rates, and replacement rates. Most of
these machines have the flexibility of different-sized circuits (ie, extracorporeal
blood volumes) and allow the user a choice of membranes. Only the Gambro
Prisma has contained membrane and blood lines providing easy and rapid
Table 1
Suggested size and selection of hemofiltration vascular access for pediatric patients
Patient weight Catheter size and source Site of insertion
Neonate Single-lumen 5 F (Cooka) Femoral artery or vein
Dual-lumen 7.0 F (Cook/Medcompa,b) Internal/external jugular,
subclavian or femoral vein
3–6 kg Dual-lumen 7.0 F (Cook/Medcompa,b) Internal/external jugular,
subclavian or femoral vein
Triple-lumen 7.0 F (Medcomp, Arrowb,c) Internal/external jugular,
subclavian or femoral vein
6–30 kg Dual-lumen 8.0 F (Arrow, Kendallc,d) Internal/external jugular,
subclavian or femoral vein
> 15–kg Dual-lumen 9.0 F (Medcompb) Internal/external jugular,
subclavian or femoral vein
> 30 kg Dual-lumen 10.0 F (Arrow, Kendallc,d) Internal/external jugular,
subclavian or femoral vein
> 30 kg Triple-lumen 12 F (Arrow, Kendallc,d) Internal/external jugular,
subclavian or femoral vein
a Cook Critical Care, Bloomington, IN.b Medcomp, Harleysville, PA.c Arrow International Reading, PA.d Kendall Health Care Products, Mansfield, MA.
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575566

implementation of CRRTwith a single cassette system. The choice of machines is
usually influenced by hospital and service contracts and somewhat by experiential
advice from other programs.
Membranes
The choice of membrane for CRRT depends on the machine, the need for
convective or diffusive clearance, and the size of the child. The Gambro Prisma
has a membrane (AN-69) that is part of the cassette that comes with the machine.
This membrane has been shown to be biocompatible and can be used for either
convective or diffusive clearance. Alternately, polysulfone membranes are also
biocompatible and offer a variety of sizes with the same convective and diffusive
flexibility. Use of these biocompatible membranes has positively affected
recovery of renal function, with less oliguria and with overall improved survival
rates in studies of hemodialysis in adults with ARF [22]. A similar comparison of
membranes has not occurred to date in either pediatric or adult CRRT, but all
membranes used in CRRT are considered biocompatible. One unique problem
that occurs with the AN-69 membrane is that of a bradykinin reaction when the
membrane interacts with acidotic plasma. Work by Brophy et al [23] has shown
that when a blood prime occurs with the use of the AN-69 membrane, the pH of
blood-banked blood (pH of 6.2–6.4) begins a series of events that results in
production of bradykinin within the circuit, resulting in a clinical event of
anaphylaxis. Adult programs have also reported this event when acidotic patients
are treated using a machine with an AN-69 membrane. Brophy’s work demon-
strated that the use of a buffering system or a bypass maneuver could easily avoid
the risk of this reaction.
Solutions for continual renal replacement therapy
Until the fall of 2000, the only solution approved by the Food and Drug Ad-
ministration (FDA) for dialysis was Hemofiltration Solution (Baxter Health Care,
Deerfield, IL), which has lactate as a buffer. Alternatively, peritoneal dialysis
solutions (also lactate-based and containing high glucose concentrations) have
been used. Programs have reported that detectable plasma levels of lactate are
demonstrated when lactate-based solutions are used for CRRT. This observation
raised the question of whether the lactate was from the solution or from the
development of lactic acidosis from the patient [24]. As with hemodialysis in
1980s, when the buffer was changed from acetate to bicarbonate, many programs
have begun to employ pharmacy-made solutions with bicarbonate as the buffer.
Barenbrock et al [24] recently demonstrated detectable plasma lactate levels and
hemodynamic compromise in patients when lactate-based hemofiltration solutions
rather than bicarbonate-based were used [24]. In the fall of 2000, the first FDA
bicarbonate-based solution became available for CVVHD (Normocarb1, Dialysis
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575 567
Solution, Richmond Hills, Ontario, Canada) with other companies to follow [25].
This development has allowed many programs to maintain a bicarbonate-based
dialysis solution with less expense and less risk of pharmacy error than with a
customized pharmacy-made solution. An additional advantage of Normocarb1 is
that it is the only calcium-free solution currently available, allowing ease of use
with citrate anticoagulation; if heparin is preferred, the calcium chloride can be
added to physiologic doses. At the time of this writing, there is not an FDA-
approved bicarbonate solution for replacement fluid, but submissions for 510K
approval are in process and are expected to be available in the first quarter of 2003.
Anticoagulation treatment
Anticoagulation treatment is needed to maintain the patency of an extracorpo-
real circuit. Studies have demonstrated that in coagulopathic patients the use of
normal saline flushes or no anticoagulation will result in a shorter circuit lifespan
than when anticoagulation is used. Historically heparin has been the mainstay of
anticoagulation for CRRT [3,18,26–28]. A standard protocol includes an initial
bolus of 10 to 30 units/kg of heparin (assuming that the initial activated clotting
time [ACT], or partial thromboplastin time [PTT] is normal) and maintaining a
continuous infusion at a rate between 10 and 30 units/kg/hour to target a ACT of
170 to 220 seconds or a PTT of two times normal. The use of heparin has the
advantage of being familiar to many clinicians and easily controlled with bedside
ACT monitoring. The risk of heparin use is excessive anticoagulation resulting in
an increased incidence of clinically significant bleeding. Furthermore, with the
recent availability of activated protein C in the therapy of sepsis, heparin may
further increase the risk of serious bleeding.
An alternative to heparin anticoagulation is citrate. In the early 1990s, Mehta
et al [29] championed the use of citrate as a form of anticoagulation for CRRT. In
this model, citrate is infused postpatient but prefilter to bind the calcium that is in
the hemofiltration circuit. When calcium is bound with citrate, the blood looses its
ability to coagulate, so the patency of the hemofiltration circuit is maintained. The
usual target for the ionized calcium (ICa) of the circuit is 0.25 to 0.4 mmols/L. To
prevent citrate toxicity in the patient, calcium then is infused independent of the
hemofiltration circuit back to the patient, targeting the patient’s ICa to a phys-
iologic level of 1.1 to 1.3 mmol/L. Protocols vary as to the source of the citrate
from a 4% sodium citrate solution with total sodium of 440 mEq/L to the 2%
citrate solution (220 mEq/L of sodium) of ACD-A (Baxter Health Care, Deerfield,
IL) [25,29,30]. Depending on the source of the citrate, one may need to prescribe a
normal sodium dialysis/replacement solution or a hyponatremic dialysis/replace-
ment solution. The only way to obtain a hyponatremic dialysis/replacement
solution is to have pharmacy custom-make the solutions, increasing both the risk
of error at the time of production and the cost. As a result, many programs prefer
ACD-A solution that can be combined with an industry-produced dialysis solution
that is calcium free (ie, Normocarb1).
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575568
The use of citrate anticoagulation has two primary side effects, metabolic
alkalosis and citrate loc (a term meaning excessive citrate) or citrate toxicity.
Metabolic alkalosis is a predicable side effect of citrate, because 1 mmol of citrate
converts to 3 mmol of bicarbonate in the presence of normal hepatic function. The
metabolic alkalosis may be further potentiated by bicarbonate in the Normocarb1,
along with acetate from the total parenteral nutrition (TPN) and acid and chloride
loss from nasogastric suction. This alkalosis can be easily remedied by reducing
the rate of the Normocarb1 and replacing the difference with normal saline. The
pH of normal saline is 5 to 5.4, and this acid load will offset the side effect of
metabolic alkalosis. Citrate LOC is a situation in which the citrate delivery
exceeds the citrate clearance. Citrate is cleared by the liver and by the hemofiltra-
tion membrane. Citrate LOC is observed clinically as rising total calcium and
decreasing Ica levels. This gap is caused by the citrate’s being bound to the
calcium. This situation is easily remedied by withholding the citrate dose for 30
minutes and then restarting it at a reduced rate. The findings of citrate LOC in a
previously stable patient may be a sign of worsening hepatic function and may
warrant further investigation of hepatic function. Although no prospective adult or
pediatric study has shown one anticoagulant to be superior to another, many
programs have reported less work at bedside and longer circuit life with the use of
citrate anticoagulation.
When to commence continual renal replacement therapy
A debate that will continue for decades is when to begin CRRT [31–36].
Advocates of early intervention argue it is better to initiate CRRT early because
(1) access is easier, (2) the staff has more opportunity at bedside to become more
comfortable with CRRT, (3) data by Ronco et al [37] in escalating the CVVH
dose indicate that survivors had a lower serum urea nitrogen than nonsurvivors,
and (4) data by Goldstein et al [4] show that survivors had less fluid accumulation
than nonsurvivors. Opponents of early use argue that (1) no prospective data
show that early intervention affects outcome, (2) placing the access adds risk to
the patient, (3) fluid removal adds risk to the patient, and (4) CRRT adds con-
fusion to bedside.
Both these positions will continue to find adherents, because the large,
randomized study by Mehta et al [36] to evaluate CRRT versus intermittent
hemodialysis began with more than 800 adults but ended with only approx-
imately 160 patients over a 5-year period [36]. Styles of practice and practice
bias will influence decision-making. Both positions have some validity,
because the limited prospective studies have not shown benefit, but the
authors know of no prospective study for ventilator use in children with
respiratory failure. The argument of excessive ultrafiltration is not valid with
the new hemofiltration systems that have accurate ultrafiltration controllers,
and one can provide solute clearance without ultrafiltration. Both Ronco’s
work [34] that was designed to examine escalating doses of replacement fluid
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575 569
and showed that the beginning serum urea nitrogen level predicted outcome
and Goldstein’s work [4] were retrospective. Nevertheless, proponents of a
prospective study understand that styles of practice and patient populations
vary from program to program and thus appreciate the real difficulties in
designing such a trial. One final factor to consider is that, like many therapies
and procedures, infrequent use increases anxiety when a modality is employed
and carries an increased risk of complications. This anxiety may be offset with
more frequent use of CRRT that allows for more familiarity and experience
with the modality.
Nutrition in acute renal failure
Children with ARF often have inadequate nutrition. Often these patients have
a pre-existing illness before the onset of ARF (eg, postoperative ARF in infants
following repair of congenital heart disease) or have a disease that affects ab-
sorption (eg, HUS). This situation can be further exacerbated by the tendency to
restrict fluid intake in a child with ARF, often compromising overall nutrition.
Work by Bartlett in the 1980s demonstrated that inadequate nutrition had a
negative effect on patient survival in an adult surgical population [38]. Similar
studies have not been performed in a pediatric population, but common wisdom
would suggest that findings would be similar. Many programs use CRRT as a
way to deliver at least 100% recommended dietary allowance (RDA) of
nutrition either by TPN or, preferably, by enteral nutrition. The continuous
aspect of CRRT lends itself well to a continuous delivery of nutrition. A
question that arises is whether the loss of nutrition on CRRT exceeds the
delivery of nutrition and the patient’s needs. In separate studies, Davies [39],
Davenport [40], and Mokrzycki [41] have demonstrated that the rate at which
CRRT (either CVVH or CVVHD) is prescribed affects amino acid losses with
the potential risk of a negative protein balance. In a prospective study by these
authors [21], children were randomly assigned to receive either CVVH or
CVVHD for the first 24 hours with subsequent crossover to the opposite therapy
for the next 24 hours. During that time, the hemofiltration prescription of the
membrane, the blood flow rate, and the net ultrafiltration were fixed. The only
variable was that for 1 24-hour period dialysate was delivered at 2000 mL/hour/
1.73m2 and for the alternative 24 hours prefilter replacement fluid was delivered
at 2000 mL/hour/1.73m2. All children received TPN with 1.5 g/kg/day of amino
acid proteins; daily energy expenditure was measured by indirect calorimetry.
Both prescriptions resulted in a negative nitrogen balance and an average loss
of amino acids of approximately 10 g/1.73m2 (�10% of protein intake). A
recent paper by Bellomo et al [42] looked at a prospective analysis of delivery
of 2.5 g/kg/day with CVVHDF and again noted that nitrogen balance was
improved but the overall nitrogen balance remained negative [42]. Both these
prospective articles demonstrated that there was no risk from this high level of
protein delivery. Work by Maxvold [21] also demonstrated a further potential
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575570
complication of CRRT caused by a predominant loss of glutamine. Glutamine is
needed for protein production and is the major intracellular amino acid–
regulating signal trafficking of proteins. This predominant loss coupled with
the fact that many amino acid TPN preparations are deficient in glutamine
places the patient at risk for glutamine deficiency. This preferential clearance of
glutamine places these highly catabolic patients further at risk for negative
balances and worsening glutamine total body deficits. Ongoing work in
glutamine supplementation in hypermetabolic patients (eg, those with sepsis
or ARF or recipients of bone marrow transplants) continues to evaluate the role
of the nonessential but increasingly obvious key nutrient for cellular recovery
[43–46].
Many of the replacement or dialysis solutions have no glucose. Glucose,
because of its small size, has a sieving coefficient of 1. Therefore in a patient with
a serum glucose level of 100 mg/dL receiving replacement or dialysate at a rate of
2 L/hour, 48 L containing 48 g of glucose may be lost in a single day. This loss
represents approximately 200 calories as the result of glucose clearance becoming
negligible in a patient with multiple intravenous pumps all containing dextrose-
containing fluids.
Vasopressor and continual renal replacement therapy
Much of the early experience with CRRT was in the care of critically ill
patients requiring cardiovascular support. The ability of CRRT to provide a
controllable, steady titration of excess body volume brought CRRT to the ICU.
Whenever dialysis is implemented, adjustments of drugs are necessary because of
altered kinetics, potential drug/hemofiltration membrane interactions and alter-
ations of the volume of distribution (Vd) as the body edema lessens with ongoing
ultrafiltration. Data are available for clearance of drugs with CRRT [47–49].
Schetz et al [50] in a review of extracorporeal drug removal nicely demonstrated
the lack of effect on many of the cardiovascular drugs (eg, dopamine, dobu-
tamine, norepinephrine, and epinephrine) by CRRT [50]. Although these drugs
are not protein-bound and their molecular weights are below that of similar
molecules normally cleared by CRRT, the investigators observed that the rapid,
endogenous metabolism of these drugs by nonrenal mechanisms made elimina-
tion by CRRT minimal. Exceptions to these findings were milrinone, digoxin,
atenolol, and clonidine, which require dose adjustments when used with CRRT
[51,52].
Recent work by Ronco et al [53] found an actual improvement in the mean
arterial pressure (MAP) when patients with sepsis and MOSF were placed on
CRRT. This improvement was further augmented when CRRT was coupled with
plasma absorption. They postulated improvement in leukocyte responsiveness to
lipopolysaccharide as a potential explanation for this occurrence. The application
of coupled plasma absorption with filtration is just beginning to develop. The
hope of reestablishing a balanced state of pro- and anti-inflammatory mediators
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575 571

in the systemic vascular bed continues to challenge those who care for critically
ill patients.
Outcome in acute renal failure
The outcome of children with ARF is as varied as the causes for developing
ARF/MOSF. Single-center studies have identified outcome by disease and
modality [2–4,7]. Work by Fleming et al [54] showed that the use of CRRT is
superior to peritoneal dialysis in the postoperative cardiac population, allowing
improved clearance and increased provision of nutritional support, but survival
could not be addressed because of small numbers. Goldstein’s work [4] with
CRRT in sepsis showed that accumulated fluid overload at the time of commenc-
ing CRRT had a negative impact on outcome, in that average fluid accumulation in
survivors (16%) was significantly less that in nonsurvivors (34%). The use of the
pediatric risk of mortality (PRISM) score did not correlate with outcome in this
population. A presentation at the Second International Conference on Pediatric
Renal Replacement Therapy (June 2002) expanded on Goldstein’s work. Data
were presented on 50 children from five separate centers with an overall survival
rate of 60% (S. Goldstein, personal communication). Using Goldstein’s model of
fluid overload at the time of commencing CRRT, investigators observed that
survivors had an average fluid overload of 8%, whereas nonsurvivors had a fluid
overload of 16%. These authors analyzed a large series of children with ARF
treated by peritoneal dialysis, hemodialysis, or CRRT and identified the under-
lying disease and the use of vasopressor agents as factors predicting outcome [3].
Concerns about use of CRRT in smaller children have been well addressed by
Zobel et al [55] who showed that CVVH[D] in infants has a more effective
clearance then CAVH[D]. These authors noted that CVVH[D] requires less anti-
coagulation and requires less-frequent changes to another form of RRT than
CAVH[D] [20]. In a study of 86 infants weighing less than 10 kg who required
CVVH[D], Symons et al [56] showed that, except in infants weighing less than
3 kg, there was no difference in survival when compared with older children [56].
Recently, Clermont et al looked at four groups of adult ICU patients in which
the overall incidence of ARF was 17% in 1530 admissions [33]. They compared
survival rates of patients without ARF, of those with ARF who did not require
dialysis, of those with ARF who required dialysis, and of those with end-stage
renal disease already undergoing (and continuing with) dialysis. The ICU mor-
tality rates were 5% in those without renal disease, 11% in those with end-stage
renal disease, 23% in the nondialyzed ARF population, and 57% in those with
ARF on acute dialysis. The investigators pointed out that the Acute Physiology
and Chronic Health Evaluation (APACHE III) score predicted outcome only in
those without ARF but overall was less predicative of mortality.
Clearly the outcome of children or adults with ARF is related to the overall
severity of illness. Current scoring systems (APACHE, PRISM) do not adequately
capture or predict the confounding variables that occur in this population.
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575572
Summary
Continuous renal replacement therapy is an effective means for fluid and solute
management in ARF/MOSF. Prospective studies have examined issues of anti-
coagulation, the impact of replacement/dialysis, the effects of bicarbonate- versus
lactate-based solutions, and nutritional and medication clearance. Speculation and
bias exists concerning when and for what indications CRRT should be initiated.
Many clinicians, supported by data from Ronco and Goldstein [4,37], would
contest that early institution is better if the risks (eg, access, anticoagulation) are
minimal and the possible benefits are maximal. The authors, examining the issues
as an intensivist and as a nephrologist, believe that early institution, aggressive
replacement/dialysis, and use of citrate-based replacement fluids provide sub-
stantive advantages. With the advent of Ronco’s recent data on sepsis managed
with filtration and plasma absorption, the indication for use of CRRT in MOSF
may become more evident regardless of the presence or absence of ARF [53].
References
[1] Warady B, Bunchman T. Dialysis therapy for children with acute renal failure: survey results.
Pediatr Nephrol 2000;15:11–3.
[2] Lowrie L. Renal replacement therapies in pediatric multiorgan dysfunction syndrome. Pediatr
Nephrol 2000;14:6–12.
[3] Bunchman T, McBryde K, Mottes T, et al. Pediatric acute renal failure: outcome by modality and
disease. Pediatr Nephrol 2001;16:1067–71.
[4] Goldstein S, Currier H, Graf J, et al. Outcome in children receiving continuous venovenous
hemofiltration. Pediatrics 2001;107(6):1309–12.
[5] Andreoli SP. Acute renal failure. Curr Opin Pediatr 2002;14(2):183–8.
[6] Wong W, McCall E, Anderson B, et al. Acute renal failure in the paediatric intensive care unit.
N Z Med J 1996;109:450–61.
[7] Mogal NE, Brocklebank JT, Meadow SR. A review of acute renal failure in children: incidence,
etiology and outcome. Clin Nephrol 1998;49:91–5, 1998.
[8] Menster M, Bunchman TE. Nephrology in the pediatric intensive care unit. Semin Nephrol 1998;
18(3):330–40.
[9] Parekh RS, Bunchman TE. Dialysis support in the pediatric intensive care unit. Adv Ren Replace
Ther 1996;3(4):326–36.
[10] Flynn J. Choice of dialysis modality for management of pediatric acute renal failure. Pediatr
Nephrol 2002;17:63–9.
[11] Bunchman TE. Acute peritoneal dialysis in infant renal failure. Perit Dial Int 1996;16(Suppl 1):
S509–11.
[12] Maxvold NJ, Smoyer WE, Gardner JJ, et al. Management of acute renal failure in the pediatric
patient: hemofiltration versus hemodialysis. Am J Kidney Dis 1997;30(5 Suppl 4):S84–8.
[13] Ronco C, Brendolan A, Bragantini L, et al. Treatment of acute renal failure in the newborn by
continuous arteriovenous hemofiltration. Trans Am Soc Artif Intern Organs 1985;31:634–8.
[14] Schuerer DH, Brophy PD, Maxvold NJ, et al. High-efficiency dialysis for Carbamazepine over-
dose. J Toxicol Clin Toxicol 2000;38(3):321–3.
[15] Bunchman TE, Valentini RP, Gardner J, et al. Treatment of vancomycin overdose using high-
efficiency dialysis membranes. Pediatr Nephrol 1999;13:773–4.
[16] Brophy PD, Tenebein M, Gardner J, et al. Childhood diethylene glycol poisoning treated with
alcohol dehydrogenase inhibitor Fomepizole and hemodialysis. Am J Kidney Dis 2000;35(5):
958–62.
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575 573
[17] Meyer RJ, Flynn JT, Brophy PD, et al. Hemodialysis followed by continuous hemofiltration for
treatment of lithium intoxication in children. Am J Kidney Dis 2001;37(5):1044–7.
[18] Bunchman TE, Donckerwolcke RA. Continuous arterial-venous diahemofiltration and continu-
ous veno-venous diahemofiltration in infants and children. Pediatr Nephrol 1994;8(1):96–102.
[19] Ronco C, Bellomo R, Ricci Z. Continuous renal replacement therapy in critically ill patients.
Nephrol Dial Transplant 2001;(Suppl 5):16:67–72.
[20] Bunchman TE, Maxvold NJ, Kershaw DB, et al. Continuous venovenous hemodiafiltration in
infants and children. Am J Kidney Dis 1995;25(1):17–21.
[21] Maxvold NJ, Smoyer WE, Custer JR, et al. Amino acid loss and nitrogen balance in critically ill
children with acute renal failure: a prospective comparison between classic hemofiltration and
hemofiltration with dialysis. Crit Care Med 2000;28(4):1161–5.
[22] Hakim RM, Wingard RL, Parker RA. Effect of the dialysis membrane in the treatment of patients
with acute renal failure. N Eng J Med 1994;331:1338–42.
[23] Brophy PD, Mottes TA, Kudelka TL, et al. AN-69 membrane reactions are pH-dependent and
preventable. Am J Kid Dis 2001;38(1):173–8.
[24] Barenbrock M, Hausberg M, Matzkies F, et al. Effects of bicarbonate and lactate buffered
replacement fluids on cardiovascular outcome n CVVH patients. Kidney Int 2000;4:1751–7.
[25] Bunchman TE, Maxvold NJ, Barnett J, et al. Pediatric hemofiltration: Normocarb1 dialysate
solution with citrate anticoagulation. Pediatr Nephrol 2002;17:150–4.
[26] Clark WR, Mueller BA, Kraus MA, et al. Extracorporeal therapy requirements for patients with
acute renal failure. J Am Soc Nephrol 1997;8:804–12.
[27] Briglia A, Paganini E. Acute renal failure in the intensive care unit: therapy overview, patient risk
stratification, complications of renal replacement, and special circumstances. Intensive Care Com-
plications 1999;20(2):347–66.
[28] Swartz R, Messana J, Orzol S, et al. Comparing continuous hemofiltration with hemodialysis in
patients with severe acute renal failure. Am J Kidney Dis 1999;34(3):424–32.
[29] Mehta RL, McDonald BR, Aguilar MM, et al. Regional citrate anticoagulation for continuous
arteriovenous hemodialysis in critically ill patients. Kidney Int 1990;38:976–81.
[30] Tolwani A, Campbell R, Schenk M, et al. Simplified citrate anticoagulation for continuous renal
replacement therapy. Kidney Int 2001;60:370–4.
[31] Silvester W, Bellomo R, Cole L. Epidemiology, management, and outcome of severe acute renal
failure of critical illness in Australia. Crit Care Med 2001;29:1910–5.
[32] Kellum J, Angus D, Johnson J, et al. Continuous versus intermittent renal replacement therapy:
a meta-analysis. Intensive Care Med 2002;28:29–37.
[33] Clermont G, Acker CG, Angus DC, et al. Renal failure in the ICU: comparison of the impact
of acute renal failure and end-stage renal disease on ICU outcomes. Kidney Int 2002;62(3):
986–96.
[34] Clermont G, Angus DC, Linde-Zwirble WT, et al. Does acute organ dysfunction predict patient-
centered outcomes? Chest 2002;121:1963–71.
[35] Tremblay R, Ethier J, Querin S, et al. Veno-venous continuous renal replacement therapy for
burned patients with acute renal failure. Burns 2000;26(7):638–43.
[36] Mehta R, McDonald B, Gabbal F, et al. A randomized clinical trial of continuous versus
intermittent dialysis for acute renal failure. Kidney Int 2001;60:1154–63.
[37] Ronco C, Bellomo R, Homel P, et al. Effects of different doses in continuous veno-venous haemo-
filtration on outcomes of acute renal failure: a prospective randomized trial. Lancet 2000;356:
26–30.
[38] Bartlett RH, Mault HR, Dechert RE, et al. Continuous arteriovenous hemofiltration: improved
survival in surgical acute renal failure? Surgery 1986;100:400–8.
[39] Davies SP, Reaveley DA, Brown EA, et al. Amino acid clearance and daily losses in patients
with acute renal failure treated by continuous arteriovenous hemofiltration. In: Kramer P, editor.
Arteriovenous hemofiltration. Berlin: Springer-Verlag; 1985. p. 139–51.
[40] Davenport A, Roberts NB. Amino acid losses during continuous high-flux hemofiltration in the
critically ill patient. Crit Care Med 1989;17:1010–4.
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575574
[41] Mokrzycki MH, Kaplan AA. Protein losses in continuous renal replacement therapies. J Am Soc
Nephrol 1996;7:2259–63.
[42] Bellomo R, Tan HK, Bhonagiri S, et al. High protein intake during continuous hemodiafiltration:
impact on amino acids and nitrogen balance. Int J Artif Organs 2002;25(4):263–8.
[43] Payne-Jams JJ, Grimble GK. Present status of glutamine. Curr Opin Gastroenterol 1995;11:
161–7.
[44] Wilmore DW. Alterations in protein, carbohydrate and fat metabolism in injured and septic
patients. J Am Coll Nutr 1983;2:3–13.
[45] Georgieff M, Tvgtekin IF. Positive role of immune nutrition on metabolism in sepsis and multi-
orgam failure. Kidney Int 1998;53(Suppl):S80–3.
[46] Pastores SM, Kvetan V, Katz DP. Immunomodulatory effects and therapeutic potential of glu-
tamine in the critically ill surgical patient. Nutrition 1994;10:365–91.
[47] Golper TA. Drug removal during continuous renal replacement therapies. Dial Transplant 1993;
22:185–212.
[48] Reetze-Bonorden P, Bohler J, Keller E. Drug dosing in patients during continuous renal replace-
ment therapy. Clin Pharmacokinit 1993;24:362–79.
[49] Bressolli F, Kinowski JM, de la Coussaye JE, et al. Clinical pharmacokinetics during continuous
hemofiltration. Clin Pharmacokinet 1994;26:457–71.
[50] Schetz M, Ferdinade P, Van den Berghe G, et al. Pharmacokinetics of continuous renal replace-
ment therapy. Intensive Care Med 1995;21:612–20.
[51] Singlas E, Fillastre P. Pharmacokinetics of newer drugs in patients with renal impairment II. Clin
Pharmoackinet 1991;20:389–419.
[52] Kong K, Haynes S, Bion J, et al. Newer drugs in intensive care. Clin Anaesthesia 1990;4:305–31.
[53] Ronco C, Brendolan A, Lonnemann G, et al. A pilot study of coupled plasma filtration and
absorption in septic shock. Crit Care Med 2002;30:1250–5.
[54] Fleming F, Bohn D, Edwards H, et al. Renal replacement therapy after repair of congenital heart
disease in children. A comparison of hemofiltration and peritoneal dialysis. J Thorac Cardiovasc
Surg 1995;109:322–31.
[55] Zobel G, Ring E, Zobel V. Continuous arteriovenous renal replacement systems for critically ill
children. Pediatr Nephrol 1989;3:140–3.
[56] Symons JM, Brophy PD, Gregory MJ, et al. Continuous renal replacement therapy in pediatric
patients weighing 10 kg or less [abstract]. Blood Purif 2002;20:306.
N.J. Maxvold, T.E. Bunchman / Crit Care Clin 19 (2003) 563–575 575