renal cell carcinoma with renal artery aneurysm
TRANSCRIPT
International Urology and Nephrology 30 (4), pp. 385-390 (1998)
Renal Cell Carcinoma with Renal Artery Aneurysm
0 . ICHIYANAGI, M. ISHIGOOKA, Y. SUZUKI, I. SASAGAWA, T. NAKADA, K. INAZAWA,* T. NAKAMURA*
Department of Urology, Yamagata University School of Medicine; *Division of Surgery, Shinjo Prefectural Hospital, Yamagata, Japan
(Accepted February 22, 1998)
We describe a patient who was diagnosed as renal cell carcinoma with renal artery aneurysm in the contralateral kidney. Right aneurysmectomy followed by sim- ple arteriorrhaphy with termino-lateral anastomosis, and then left radical nephrecto- my were performed in one session. The patient did well postoperatively.
Generally, surgical indication of renal artery aneurysm itself has been yet a matter of debate. In such case like this, however, it seems better to resect any kind of aneurysm of the opposite side, taken into consideration the haemodynamic changes after nephrectomy. Surgical indications are commented on.
Introduction
Renal artery aneurysm (RAA) is a relatively uncommon vascular lesion. It has been estimated to occur in 0.01 and 1 per cent, based on previous autop- sy and angiographic studies [1-3]. However, RAA has been more frequently diagnosed chiefly because of the extensive use of angiography.
Complications of RAA include hypertension, peripheral dissection, thromboembolism, renal infarction, and rupture with bleeding [4]. Early reports claimed an extremely high risk for rupture [2, 5, 7], although recent investiga- tors have clarified its much lower incidence than generally thought. Rupture is, however, the most catastrophic episode with high mortality [2, 5, 7]. The oper- ation is usually urgent, complicated and dramatic once rupture takes place.
We report a rare case of a malignant renal tumour with an aneurysm of the renal artery on the opposite side.
Case report
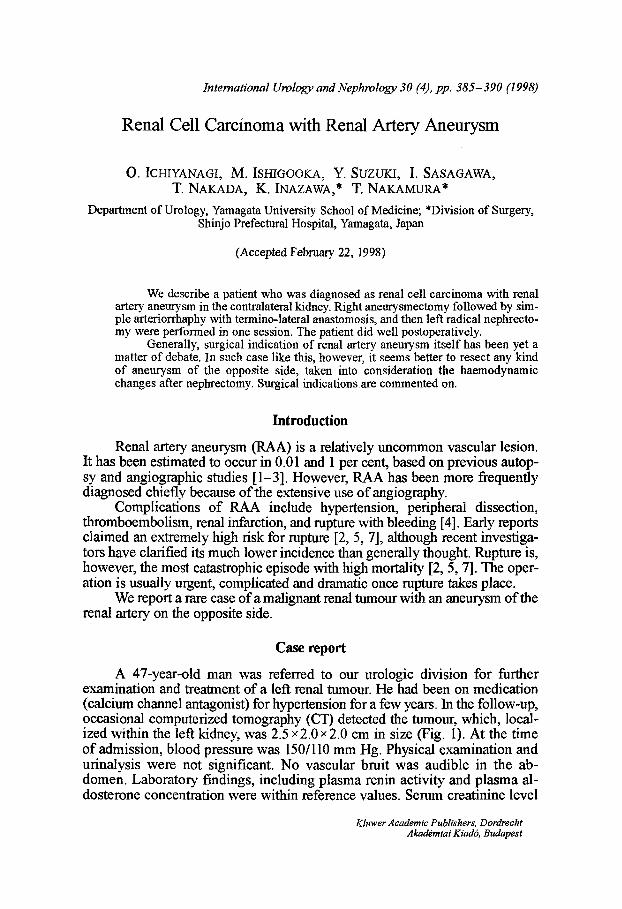
A 47-year-old man was referred to our urologic division for further examination and treatment of a left renal tumour. He had been on medication (calcium channel antagonist) for hypertension for a few years. In the follow-up, occasional computerized tomography (CT) detected the turnour, which, local- ized within the left kidney, was 2.5 •215 cm in size (Fig. 1). At the time of admission, blood pressure was 150/110 mm Hg. Physical examination and urinalysis were not significant. No vascular bruit was audible in the ab- domen. Laboratory findings, including plasma renin activity and plasma al- dosterone concentration were within reference values. Serum creatinine level
Kluwer Academic Publishers, Dordrecht Akad~raiai Kiadr, Budapest
386 Ichiyanagi et al.: Renal cell carcinoma with aneurysm
Fig. 1. CT showing a solid mass in the left kidney, without any swelling of regional lymph nodes. There is a simple cyst in the right kidney
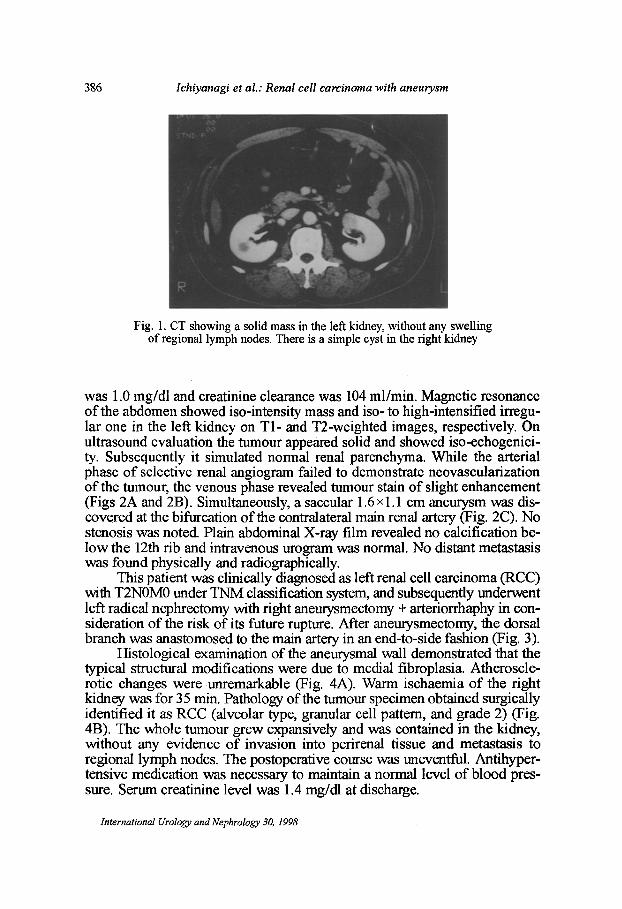
was 1.0 mg/dl and creatinine clearance was 104 ml/min. Magnetic resonance of the abdomen showed iso-intensity mass and iso- to high-intensified irregu- lar one in the left kidney on T1- and T2-weighted images, respectively. On ultrasound evaluation the tumour appeared solid and showed iso-echogenici- ty. Subsequently it simulated normal renal parenehyma. While the arterial phase of selective renal angiogram failed to demonstrate neovascularization of the tumour, the venous phase revealed tumour stain of slight enhancement (Figs 2A and 2B). Simultaneously, a saceular 1.6 • cm aneurysm was dis- covered at the bifurcation of the eontralateral main renal artery (Fig. 2C). No stenosis was noted. Plain abdominal X-ray film revealed no calcification be- low the 12th rib and intravenous urogram was normal. No distant metastasis was found physically and radiographically.
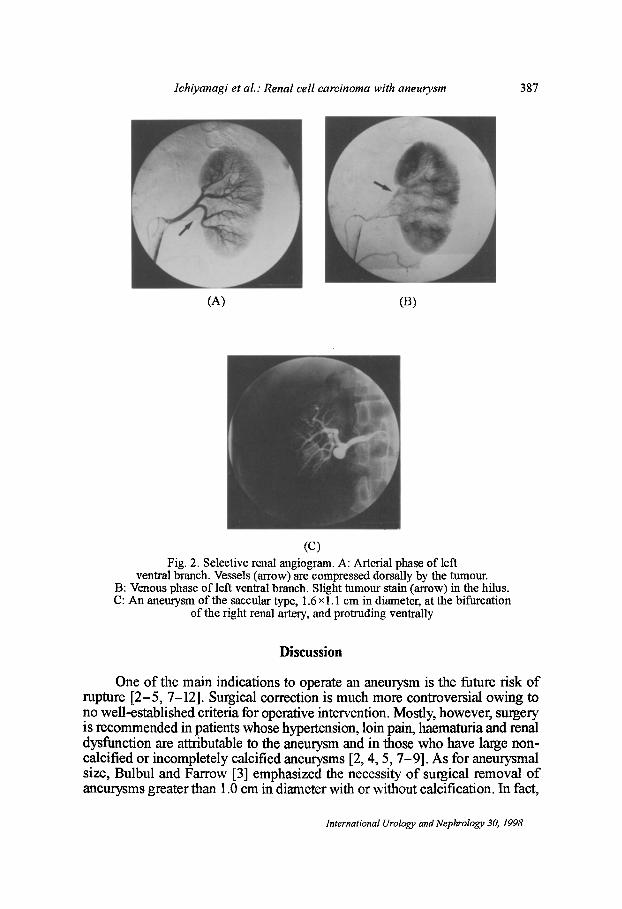
This patient was clinically diagnosed as left renal cell carcinoma (RCC) with T2NOM0 under TNM classification system, and subsequently underwent left radical nephrectomy with right aneurysmectomy + arteriorrhaphy in con- sideration of the risk of its future rupture. After aneurysmectomy, the dorsal branch was anastomosed to the main artery in an end-to-side fashion (Fig. 3).
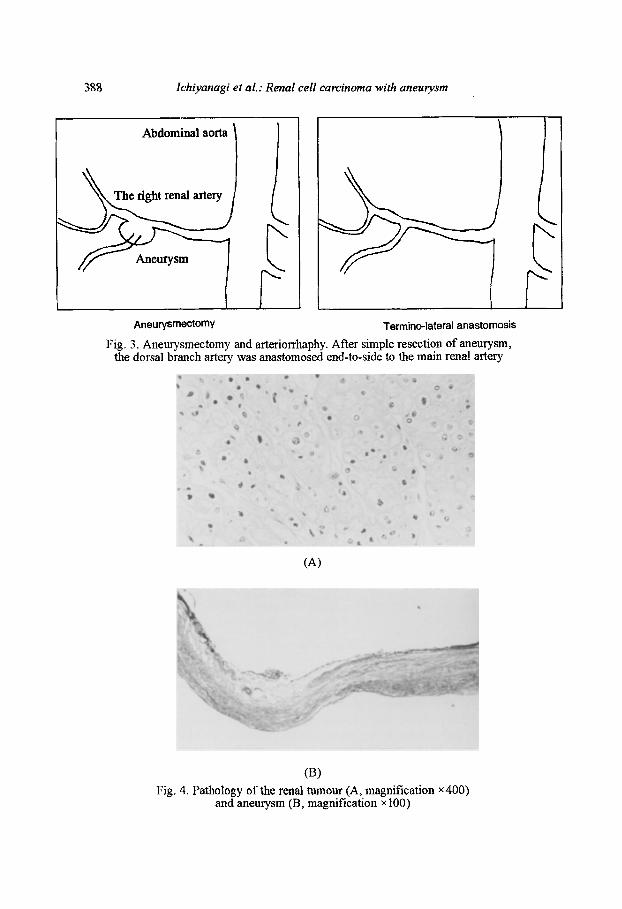
Histological examination of the aneurysmal wall demonstrated that the typical structural modifications were due to medial fibroplasia. Atheroscle- rotic changes were unremarkable (Fig. 4A). Warm ischaemia of the right kidney was for 35 min. Pathology of the tumour specimen obtained surgically identified it as RCC (alveolar type, granular cell pattem, and grade 2) (Fig. 4B). The whole tumour grew expansively and was contained in the kidney, without any evidence of invasion into perirenal tissue and metastasis to regional lymph nodes. The postoperative course was uneventful. Antihyper- tensive medication was necessary to maintain a normal level of blood pres- sure. Serum creatinine level was 1.4 mg/dl at discharge.
International Urology and Nephrology 30, 1998
lchiyanagi et aL : Renal cell carcinoma with aneurysm 387
(A) (B)
~ ) Fig. 2. Selective renal angiogram. A: Arterial phase of left
ventral branch. Vessels (arrow) are compressed dorsally by the tumour. B: Venous phase of left ventral branch. Slight tumour stain (arrow) in the hilus. C: An aneurysm of the saccular type, 1.6 xl.1 cm in diameter, at the bifurcation
of the right renal artery, and protruding ventrally
Discussion
One of the main indications to operate an aneurysm is the future risk of rupture [2-5, 7-12]. Surgical correction is much more controversial owing to no well-established criteria for operative intervention. Mostly, however, surgery is recommended in patients whose hypertension, loin pain, haematuria and renal dysfunction are attributable to the aneurysm and in those who have large non- calcified or incompletely calcified aneurysms [2, 4, 5, 7-9]. As for aneurysmal size, Bulbul and Farrow [3] emphasized the necessity of surgical removal of aneurysms greater than 1.0 cm in diameter with or without calcification. In fact,
International Urology and Nephrology 30, 1998
388 Ichiyanagi et al.: Renal cell carcinoma with aneurysm
Abdominal aorta
Aneurysmectomy
right renal artery
Termino-lateral anastomosis
Fig. 3. Aneurysmectomy and arteriorrhaphy, After simple resection of aneurysm, the dorsal branch artery was anastomosed end-to-side to the main renal artery
,I"
(a)
(t3) Fig, 4, Pathology of the renal tumour (A, magnification x400)
and aneurysm 03, magnification x 100)
Ichiyanagi et al.: Renal cell carcinoma with aneurysm 389
many researchers considered the cut-off point for surgical indication to be a diameter greater than 1.5 cm [3-5, 7-9, 11]. But there have been a few rup- tured cases of aneurysms smaller than 1.5 cm in diameter and vice versa [7]. Stanley and Whitehouse insisted on the limited value of size as an indicator of rupture potential [12]. In addition, RAA should be excised, regardless of its size, especially in females in whom there is potential for pregnancy. That is be- cause pregnancy hypothetically predisposes to rupture (80%) due to the haemo- dynamic changes, especially during late gestational period, such as increased cardiac output, hence increased renal blood flow and hormonal influence on the vascular bed [3, 7, 10].
Our patient was a rare case of RCC with a contralateral typical saccular non-calcified RAA. Only one such case has been reported before as far as we know [11]. It is quite natural that left radical nephrectomy was appropriate for therapy of RCC in our case, but what about the right aneurysmectomy? It has not been in the least discussed yet how such an aneurysm on the opposite side should be dealt with clinically when nephrectomy is required for some reason. In general, compensatory growth and hypertrophy after nephrectomy occur in the contralateral residual kidney, reactive to the reduced number of nephrons. This phenomenon may influence the vascular physiological or histological con- ditions of the remaining vasculature. That is, such a condition is accompanied by an increase in renal blood flow and thereby appears to strain the renal arte- rial wall much more than before. From the standpoint of haemodynamic changes, a certain analogy seems to exist between pregnancy and post-nephrec- tomized status. Theoretically, the aneurysm itself may also change the haemo- dynamics in the kidney and as a consequence cause hypertension without the presence of stenosis [6]. In the light of such consideration, it is easily speculat- ed that watchful waiting in RAA would carry a relatively high incidence of rup- ture after operative removal of the contralateral kidney. In conclusion, we be- lieve that surgical removal of aneurysm for prevention of a later rupture should be necessary in a patient who is supposed to undergo nephrectomy for some medical reason.
References
1. Fleshner, N. E., Johnston, K. W.: Repair of an autotransplant renal artery aneurysm: Case report and literature review. J. Urol., 148, 389 (1992).
2. Tham, G., Ekelund, L., Herrlin, K., Lindsredt, E. L., Olin, T., Bergentz, S.-E.: Renal artery aneurysms. Natural history and prognosis. Ann. Surg., 197, 348 (1982).
3. Bulbul, M. A., Farrow, G. A.: Renal artery aneurysms. Urology, 40, 124 (1992). 4. Ortenberg, J., Noviek, A. C., Stmffon, R. A., Stewart, B. H.: Surgical treatment of renal
artery aneurysms. Br J. Urol., 55, 341 (1983). 5. Henrikson, C., Bjorkerud, S., Nilson, A. E., Pettersson, S.: Natural history of renal
artery aneurysm elucidated by repeated angiography and pathoanatomical studies. Eur. Urol., 11, 244 (1985).
6. Dubemard, J. M., Gelet, M. A., Mongin, D.: Aneurysms of renal artery: Surgical man- agement with special reference to extracorporeal surgery and autotransplantation. Eur. Urol., 11, 26 (1985).
International Urology and Nephrology 30, 1998
390 Ichiyanagi et al.: Renal cell carcinoma with aneurysm
7. Hidai, H., Kinoshita, Y., Murayama, T., Miyai, K., Matsumoto, A., Ide, K., Sato, S.: Rupture of renal artery aneurysm. Eur. UroL, 11, 249 (1985).
8. Ma~.in, R. S., Meacham, P. W., Ditesheim, J. A, Mulherin, J. L. Jr., Edwards, W. H.: Renal artery anenrysm: Selective treatment for hypertension and prevention of rup- ture. J. Vasc. Surg., 9, 26 (1989).
9. Youkey, J. R., Collins, G. J. Jr., Orecchia, P. M., Brigham, R. A., Salander, J. M., Rich, N. M.: Saccular renal artery aneurysm as a cause of hypertension. Surgery, 97, 498 (1985).
10. Cohen, J. R., Shamash, F. S.: Ruptured renal artery aneurysms during pregnancy. J. Vasc. Surg., 6, 51 (1987).
11. Nakahara, M., Osi, M., Minowada, S., Aso, Y.: Renal cell carcinoma with renal artery aneurysm treated by extracorporeal surgery and autotransplantafion. A report of 2 cases. Jpn. J. Urol., 83, 546 (1992).
12. Stanley, J. C., Whitehouse, W. M. Jr.: Renal artery macro aneurysms. In: Bergan, Yao (eds): Anenrysms, Diagnosis and Treatment. Grune & Stratton, New York 1982, pp. 417-431.
International Urology and Nephrology 30, 1998