reliability and validity of the exercise self-regulatory ... · reliability and validity of the...
TRANSCRIPT
RSw
Aa
Rdde
FvizU
Fs
*ssi
RCA
0Cd
ISSUES IN PULMONARY NURSING
H
eliability and validity of the Exerciseelf-Regulatory Efficacy Scale* for individualsith chronic obstructive pulmonary disease
my H. T. Davis, RN, PhD,a Aurelio José Figueredo, PhD,b Bonnie F. Fahy, RN, MN,c
nd Tassanee Rawiworrakul, RN, PhDd
oi:
E
BACKGROUND: Exercise has important benefits for individuals with chronic obstructive pulmonarydisease (COPD). However, to sustain long-term benefits of exercise, adherence is needed. Adherencerequires self-regulation. No scale is available to measure exercise self-regulation in individuals withCOPD.
OBJECTIVES: We developed and tested the reliability and validity of an “Exercise Self-RegulatoryEfficacy Scale (Ex-SRES)” for individuals with COPD.
METHODS: A convenience sample of 109 subjects with COPD was recruited. Cronbach’s alpha wasused to assess the internal consistency reliability of the Ex-SRES. Subjects’ exercise behaviors and healthstatus were used to assess the validity of the Ex-SRES.
RESULTS: The Ex-SRES demonstrated evidence of reliability (Cronbach’s alpha .917) and validity (corre-lation with minutes of exercise per week [r � .41; P � .0001] and health status [r � .37; P � .0001]).
CONCLUSION: The Ex-SRES is a short (16-items) and easy to use questionnaire that may be valuablefor assessing patients in clinical settings, as well as for future research studies in behaviors related toexercise. (Heart Lung® 2007;36:205–216.)
lecewediavoaia8efa
egular exercise operates at every level ofhealth promotion, preventing the develop-ment of diseases and reducing the damage
one by diseases.1,2 Although there is still muchebate as to the best type, frequency, and length ofxercise individuals need to do on a regular basis,
rom the aCollege of Nursing, bDepartment of Psychology, Uni-ersity of Arizona, Tucson, Arizona; cCardiac/Pulmonary Rehabil-tation, St Joseph’s Hospital and Medical Center, Phoenix, Ari-ona; and dDepartment of Public Health Nursing, Mahidolniversity, Bangkok, Thailand.
unding sources: NIH/NINR 1 R15 NR008103-03 and The Univer-ity of Arizona, College of Nursing.
To request a copy of the Ex-SRES instrument, a one-pageummary of its psychometrics and scoring syntax, please send aelf-addressed envelope with return postage to the correspond-ng author.
eprint requests: Amy H. T. Davis, RN, PhD, Assistant Professor,ollege of Nursing, University of Arizona, 1305 N. Martin, Tucson,Z 85721-0203.
147-9563/$ – see front matteropyright © 2007 by Mosby, Inc.
i10.1016/j.hrtlng.2006.08.007
ART & LUNG VOL. 36, NO. 3
ittle doubt remains about the significant beneficialffects of regular exercise for an individual’s physi-al and mental well-being. The majority of availablevidence supports the overall tenet that the moree, as health providers, can inspire our patients toxercise regularly, the more benefit they will likelyerive from exercising.3 Despite efforts to educate
ndividuals about the benefits of regular exercisend to devise a myriad of exercise routines usingarious methods and equipment, approximatelyne third of individuals 18 years and older do notdhere to a regular exercise program. For thosendividuals who are socially and economically dis-dvantaged, the rate of nonadherence is closer to0%.4 It is clear that knowledge about the benefits ofxercise does not always lead to action, but theactors that influence exercise adherence at largere unclear.
Findings from a number of well-controlled stud-
es provide strong evidence that exercise is also anwww.heartandlung.org 205

eootcwdtwhtnsnscCtattbPtlifwv
opbtadcCbnmaslpbCsafifde
methtwilce
S
istltmioscreesictcsccfcccret
ekeechlewm
Reliability and validity of the Ex-SRES Davis et al
2
ffective intervention for individuals with chronicbstructive pulmonary disease (COPD).5,6 Becausef increasing health care costs and a movementoward active patient participation in their healthare, individuals who have COPD, similar to othersho have other chronic illnesses, bear a tremen-ous burden managing their illness and symp-oms.7,8 COPD is a chronic and progressive illnessithout a medical cure. However, regular exerciseas been shown to reduce the most disabling symp-om experienced by individuals with COPD: short-ess of breath.5,6 These findings supported thehort-term benefits of exercise interventions but didot address how these important benefits may beustained long term.5,6 Symptom management is aentral concept in the care of individuals withOPD. Because a key benefit of exercise interven-
ions is reduction of shortness of breath, exercisedherence may be viewed as a component of symp-om management.8 Adherence to exercise interven-ions serves as the bridge that facilitates sustainedenefits derived from exercise interventions.8
lainly, the long-term effectiveness of exercise in-erventions requires exercise adherence. Nonethe-ess, as in other populations, adherence to exercises poor in individuals with COPD.4,9 To investigateactors related to exercise adherence in individualsith COPD, it is therefore necessary to further de-elop the concept of exercise adherence.8
Adherence to a regular exercise program dependsn one’s ability to self-regulate and persist despiteotential difficulties or impediments.8,10 Individualeliefs in one’s ability to self-regulate (self-regula-ory efficacy) may vary across health conditionsnd be dependent on the nature of the potentialifficulties. Persisting despite difficulties may behallenging for many individuals. For those withOPD, they may experience severe shortness ofreath simply while doing their daily activities. It isot difficult to envision that individuals with COPDay face additional challenges as they attempt to
dhere to a regular exercise program. Although priortudies have examined other types of efficacy be-iefs in individuals with COPD, such as efficacy toerform physical tasks11,12 or manage shortness ofreath,13 self-regulatory efficacy in individuals withOPD is not well understood. Unlike efficacy beliefsuch as in weight lifting, in which an increase in themount of weight will predictably increase the dif-iculty of the task, the amount of difficulty eachmpediment poses on a person’s self-regulatory ef-icacy for exercise is more likely to be individuallyetermined.11 For example, bad weather or experi-
ncing shortness of breath with exercise may pose s06 www.heartandlung.org
ore difficulty for some individuals’ self-regulatoryfficacy for exercise. This will differentially affectheir ability to overcome these challenges and ad-ere to their exercise program. Unfortunately, fac-ors that influence exercise adherence in individualsith COPD are not well defined. Therefore, it is
mportant to understand issues that may pose chal-enges for individuals with COPD to adhere to exer-ise, especially their ability to self-regulate andxercise regularly despite these challenges.
ELF-REGULATORY EFFICACYThe ability to self-regulate is a prominent concept
n social cognitive theory.14 The social cognitive per-pective emphasizes that, as human beings, we havehe capability to interact with the environment, toearn, to regulate our thoughts and behaviors, ando adjust our performance and alter our environ-ent to meet certain standards.14 To further explain
ndividual behaviors, Bandura11 focused on the rolef personal cognitive factors (self-beliefs) within theocial cognitive theory and developed the self-effi-acy theory. The self-efficacy theory describes theole of individuals’ belief in their own capabilities toxercise control over their actions by organizing andxecuting courses of action necessary to obtain de-irable results.11,15 Self-efficacy beliefs have beenmportant predictors of behaviors related to physi-al and mental health.16,17 Individuals’ belief inheir ability to exercise regularly when faced withhallenges may be conceptualized as their exerciseelf-regulatory efficacy. Exercise self-regulatory effi-acy describes the ability for one to persist despitehallenges, in part, by setting up and managingavorable environments, thinking positive and en-ouraging thoughts, and identifying and applyingonsequences for their own actions related to exer-ising regularly.11,15 Improving exercise adherenceequires that individuals believe in their ability toxercise regularly even when there are disincentiveso exercise, such as bad weather or fatigue.11,15
Past findings have showed that self-regulatoryfficacy (belief in one’s ability to self-regulate) is aey variable that may influence exercise adher-nce.14,18,19 Accordingly, enhancing self-regulatoryfficacy may increase exercise behaviors and exer-ise adherence, and improvements in exercise ad-erence may serve to further enhance efficacy be-
iefs, creating a cycle of positive reinforcements. Forxample, in an early study of young adults, thoseho believed that they could resist relapse andake time for exercise, exercised more.20 In another
tudy, adults who adhered to a regular exercise
MAY/JUNE 2007 HEART & LUNG

pefscoaia
tshepeosCncpAetev
EE
cathrsbaeCtM
tebadtpap
tSow
adwwreCafacdTnjbbiwaifpcaTptt
nftwewicm
P
tserw
Davis et al Reliability and validity of the Ex-SRES
H
rogram believed there were fewer obstacles to ex-rcise than those who did not adhere.18 Findingsrom more recent studies also demonstrated thatelf-regulatory efficacy may be important for exer-ise adherence. This effect was seen in a study oflder adults, in which higher self-regulatory efficacyccounted for 30% of the variance in exercise activ-ty and was significantly related to their physicalnd mental health status.21
In summary, these findings support the conten-ion that it is important to continue to investigateelf-regulatory efficacy’s relationship to exercise ad-erence. In the past, several studies have examinedfficacy beliefs to perform various exercise-relatedhysical activities in patients with COPD, such asfficacy beliefs to physically walk a certain distancer for a certain length of time.13,22,23 None havetudied self-regulatory efficacy in individuals withOPD. Other researchers have developed question-aires that address self-regulatory efficacy to over-ome barriers or impediments to exercise in otheropulations, such as sedentary or older adults.21,24,25
validated measure of self-regulatory efficacy for ex-rcise in subjects with COPD is not available. To fur-her our understanding of exercise self-regulatoryfficacy in individuals with COPD, a reliable andalid measure is needed.
XERCISE SELF-REGULATORYFFICACY SCALEConceptually, the Exercise Self-Regulatory Effi-
acy Scale (Ex-SRES) is based on social cognitivend self-efficacy theories, and its roots are in symp-om management.7,8 Individuals with COPD mayave particular challenges related to exercise self-egulatory efficacy that are unique to their illness,uch as experiencing the symptom of shortness ofreath with exertion, which may cause additionalnxiety or distress. Therefore, to accurately measurexercise self-regulatory efficacy of individuals withOPD, it is important to elicit input from those with
he illness for instrument development (A. Bandura,D, personal communication, 1999; 2001).Individuals with COPD may share some charac-
eristics with sedentary adults because of a lowxercise rate; they may also resemble older adultsecause the average age of subjects with COPD ispproximately 65 years and would be similar inevelopmental stage and other preferences. Al-hough individuals with COPD may share some im-ediments to exercise with other populations suchs sedentary and older adults, they are likely to have
articular concerns and perspectives specific to fEART & LUNG VOL. 36, NO. 3
heir illness. Therefore, items included on the Ex-RES were based on prior studies in sedentary andlder adults,21,24 as well as input from individualsith COPD.
In part of a study that continued prior conceptu-lizations of exercise adherence, we conducted in-epth one-on-one interviews with 14 individualsith COPD. Subjects were asked to identify whatould impede them or keep them from exercising
egularly, as well as other questions related to theirxercise behaviors. In addition, 45 subjects withOPD participating in a separate study were alsosked to identify impediments that may keep themrom exercising regularly. Our findings indicated, asnticipated, that individuals with COPD had uniqueoncerns that were different from what has beenescribed in other populations (Fig 1 and 2).21,24,25
hese unique concerns included experiencing short-ess of breath, using oxygen, having bad days and
ust not feeling like exercising, being ill, and noteing able to pay for continuing in monitored reha-ilitation programs. In addition, different from stud-
es of sedentary and older adults,21,24 individualsith COPD in our samples did not differentiatemong being bored, having no interest in the activ-ties, or not liking the activities versus simply notinding exercising fun or enjoyable (Fig 2). It isossible that individuals with COPD perceive exer-ise as an important intervention rather than recre-tion or a casual option for health maintenance.hese findings suggest that individuals with COPDerceive challenges related to exercise self-regula-ory efficacy that are different from other popula-ions.
The Ex-SRES is a user-friendly, 16-item question-aire that measures the exercise self-regulatory ef-
icacy of individuals with COPD (Fig 1). The ques-ions ask participants to indicate the degree tohich they are confident they could continue toxercise regularly (3 times per week for 20 minutes)hen faced with various impediments. Participants
ndicated their confidence level from 0% (not at allonfident) to 100% (highly confident) as recom-ended by Bandura11 for efficacy measures.
URPOSEThe Ex-SRES was developed with the hypothesis
hat this scale has a one-factor structure and repre-ents one latent variable: exercise self-regulatoryfficacy. The purpose of this article is to examine theeliability and validity of the Ex-SRES in individualsith COPD. In theory, if exercise self-regulatory ef-
icacy is important in individuals with COPD, it will
www.heartandlung.org 207

Reliability and validity of the Ex-SRES Davis et al
2
Fig 1 Exercise Self-Regulatory Efficacy Scale (Ex-SRES).
08 www.heartandlung.org MAY/JUNE 2007 HEART & LUNG

Davis et al Reliability and validity of the Ex-SRES
H
Fig 2 Comparison of items between studies. Ex-SRES, Exercise Self-Regulatory Efficacy Scale;
COPD, chronic obstructive pulmonary disease.EART & LUNG VOL. 36, NO. 3 www.heartandlung.org 209

bwicwwa
S
urSrgwTrstrmpshmdtaetncSonett
M
essmdbwettv
clat
OM
wspCopsmbscwatstesju03M
Mh
wtiw3httsiwcptg(h
Reliability and validity of the Ex-SRES Davis et al
2
e related to their exercise behaviors. Further, thoseith better health status will be more apt to believe
n their ability to overcome impediments to exer-ise.21 Therefore, to test the validity of the Ex-SRES,e hypothesize that exercise self-regulatory efficacyill be positively correlated to exercise behaviorsnd health status in individuals with COPD.
AMPLE AND SETTINGA cross-sectional, correlational study design was
sed to achieve the purpose of this study. Aftereceiving approval from the University’s Humanubjects Committee and appropriate institutionaleview boards of pulmonary rehabilitation pro-rams, a convenience sample of men and womenith mild to severe COPD, based on the Americanhoracic Society’s26 disease severity criteria, wereecruited continuously over 36 months for thistudy. Subjects were recruited from various sites inwo major metropolitan cities and one suburbanetirement community 50 miles from one of theetropolitan cities. With permission flyers were
laced with physician offices, senior centers, COPDupport groups, and four outpatient pulmonary re-abilitation programs to recruit volunteers with per-ission. Volunteers 21 years of age or older with a
iagnosis of COPD were invited to participate. Par-icipants also had to be able to walk unassisted on
flat surface and had no contraindications for ex-rcise. After individuals gave consent to participate inhe study, they completed a short cognitive question-aire (Mini-Mental State Examination [MMSE])27 toonfirm their ability to comprehend study materials.pirometry testing was performed to confirm airwaybstruction.26 Participants were excluded if they didot score more than 16 on the MMSE, they had novidence of airway obstruction, or it was apparent thathey could not walk unassisted or had contraindica-ions for exercise.
ETHODSThose individuals who met inclusion criteria were
nrolled in the study after providing informed con-ent. Subjects’ mental status, English comprehen-ion, and degree of airflow obstruction were deter-ined. To minimize potential limitations related to
ata collection, all research personnel were trainedy the principle investigator, who is experiencedith this population and with study instruments, tonsure consistency of data collection. To be certainhat research assistants were able to answer ques-ions appropriately as they arose, the principle in-
estigator was initially available on site during data h10 www.heartandlung.org
ollection and thereafter by phone. During data col-ection, research assistants were present, clarifiedny questions participants had, and reviewed ques-ionnaires for completeness and accuracy.
THER STUDY INSTRUMENTSini-Mental State ExaminationThe MMSE27 was used to exclude participants
ith mental status changes or English comprehen-ion difficulties that may impact their ability torovide accurate responses to study questionnaires.ognitive impairment may be prevalent but not obvi-us in certain medical conditions and may impactarticipants’ ability to provide accurate information ontudy questionnaires; consequently, participants’ental status was screened by the MMSE.27 Also,
ecause an interviewer administered the MMSE, iterved as a means to assess participants’ Englishomprehension in this study to ensure participantsere able to understand study questionnaires. MMSEssesses several areas such as orientation, atten-ion, recall, language, calculation, and visual con-truction. The MMSE is a longstanding instrumenthat has been tested in various populations withvidence of reliability and validity in populations,uch as geriatric, psychiatric, and neurologic sub-ects. The MMSE takes approximately 5 to 10 min-tes to administer. The total scores may range fromto 30 with normal cutoffs from a score of 25 to
0.27 All participants in this sample passed theMSE.
edical outcome study’s short-formealth survey [36 items]Participants’ exercise self-regulatory efficacy
as hypothesized to be positively correlated toheir health status. To assess the construct valid-ty of the Ex-SRES, health status was assessedith the short-form health survey [36 items] (SF-6), which includes both a physical and a mentalealth status component.28 The SF-36 is one ofhe most frequently used self-administered ques-ionnaires to assess individuals’ general healthtatus, and it has been extensively administeredn a variety of populations including individualsith COPD (Cronbach’s alpha .92). The SF-36 hasonsistently demonstrated good psychometricroperties with evidence of reliability and validi-y.28 The two components of the SF-36 is furtherrouped into eight subscales of functioningphysical, role-physical, bodily pain, generalealth, vitality, social, role-emotional, and mental
ealth). Scores for all eight dimensions and twoMAY/JUNE 2007 HEART & LUNG

dww
E
heEmmeowhtuwb
S
isoideeittcftsepfwat
RS
fl5mtp
tojc
R
aulecd.ncrmeatiiiw
V
Davis et al Reliability and validity of the Ex-SRES
H
omains are expressed on a scale of 0 to 100, inhich higher scores indicate better health andell-being.28
xercise behaviorsParticipants’ exercise self-regulatory efficacy was
ypothesized to be positively correlated to theirxercise behaviors. To assess criterion validity of thex-SRES, participants’ exercise behavior (number ofinutes participants exercised per week) was deter-ined from participants’ detailed descriptions of
xercises they are currently doing. For the purposef this study, participants were asked to indicatehat type of exercises they are currently doing,ow often, and how much time they spent doinghese exercises at each exercise session. The min-tes performed for each of these exercises per weekere summed and represents their total exerciseehavior.
TATISTICAL ANALYSISThe reliability of the Ex-SRES was determined by
ndividual item analyses and analyses of the entirecale. Item analyses included assessment for floorr ceiling effects, item to total correlations, inter-
tem correlations, and changes in alpha with itemeleted. Cronbach’s alpha was used to estimate thentire scale’s internal consistency reliability, whichstimates the uniformity and cohesiveness of all thetems in the scale.29,30 Several methods were usedo test the validity of the Ex-SRES. Because we arehe first to validate this new scale specifically fo-used on individuals with COPD, we performed aactor analysis to determine whether our hypothesishat this scale has a one-factor structure and repre-ents one latent variable, exercise self-regulatoryfficacy, was supportable. Also, the factor procedureermitted us to explore the possibility of multiple
actors within this scale. In addition, the Ex-SRESas correlated to a measure of health status (SF-36)nd measure of participants’ exercise behavior toest its construct validity.
ESULTSample characteristicsA total of 109 subjects with COPD were included
or this analysis (mean age 70.8 � 8.5 years; FEV1 initers 1.6 � .6; FEV1 % predicted 47 � 19; FEV1/FVC0.4 � 18; pack/years smoked 43 � 33). The sampleostly consisted of whites (90%). Gender composi-
ion was 59 women (54%) and 50 men (46%). Most
articipants had some college education (70%). Of lEART & LUNG VOL. 36, NO. 3
hese, 18% had graduate education. As for the restf the participants, 28% had high school and 2% had
unior high school education. Additional sampleharacteristics are provided in Table I.
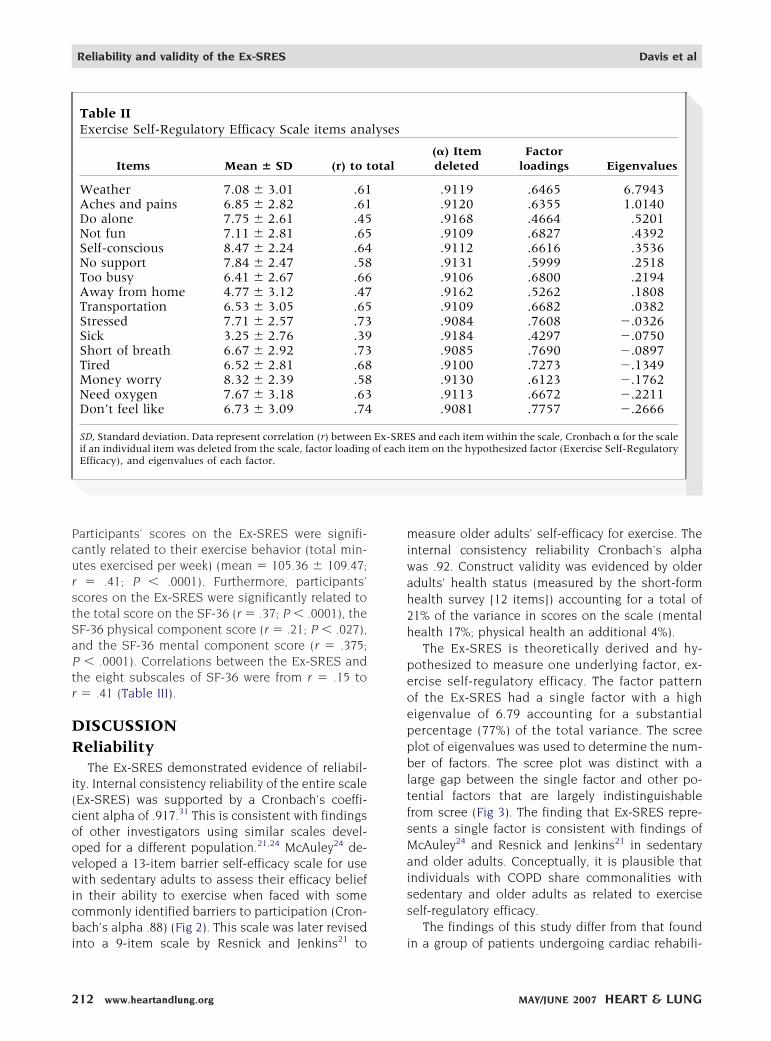
eliability testingFor the Ex-SRES as whole, Cronbach’s coefficient
lpha for internal consistency reliability was .917. Bysing the principle factor method, a one-factor so-
ution was sought and obtained, which had an eig-nvalue of 6.79 and accounted for 77.1% of theumulative variance in the Ex-SRES. Factor patternsemonstrated that factor loading of items were from
43 (item 11, if I feel sick or ill) to .76 (item 16, if I doot feel like exercising) (Table II). Squared multipleorrelations (R2) using ordinary least squaresanged from .19 to .60 (Table II). All items had ainimum value of 0 and maximum value of 10
xcept item 7 (too busy), which had a minimum of 1nd maximum of 10. Item to total correlations forhe 16 items ranged from .394 to .738. For any onetem deleted, the Cronbach coefficient alpha did notncrease by more than .05 (Table II). The greatestncrease seen was with item 11 (if I feel sick or ill),here Cronbach’s alpha increased slightly by .001.
alidity testingParticipants’ scores on the Ex-SRES were corre-
Table IAdditional characteristics of the sample
n � 109 Frequency Percent
Use oxygen 67 61.5Current smoker 2 2Shortness of breath,
constantly20 18
Shortness of breath,exercise only
53 49
Employed 10 9.2Unemployed 4 3.7Retired 91 83.5On disability 4 3.7Lives alone 36 33Lives with spouse/
partner60 55
Lives with other 13 12Married 53 49Have health insurance 109 100Income �$20,000/y 20 18Income �$40,000/y 44 40
ated to their exercise behaviors and health status.
www.heartandlung.org 211
PcurstSaPtr
DR
i(coovwicbi
miwah2h
peoeppbltfsMaiss
Reliability and validity of the Ex-SRES Davis et al
2
articipants’ scores on the Ex-SRES were signifi-antly related to their exercise behavior (total min-tes exercised per week) (mean � 105.36 � 109.47;� .41; P � .0001). Furthermore, participants’
cores on the Ex-SRES were significantly related tohe total score on the SF-36 (r � .37; P � .0001), theF-36 physical component score (r � .21; P � .027),nd the SF-36 mental component score (r � .375;� .0001). Correlations between the Ex-SRES and
he eight subscales of SF-36 were from r � .15 to� .41 (Table III).
ISCUSSIONeliabilityThe Ex-SRES demonstrated evidence of reliabil-
ty. Internal consistency reliability of the entire scaleEx-SRES) was supported by a Cronbach’s coeffi-ient alpha of .917.31 This is consistent with findingsf other investigators using similar scales devel-ped for a different population.21,24 McAuley24 de-eloped a 13-item barrier self-efficacy scale for useith sedentary adults to assess their efficacy belief
n their ability to exercise when faced with someommonly identified barriers to participation (Cron-ach’s alpha .88) (Fig 2). This scale was later revised
Table IIExercise Self-Regulatory Efficacy Scale items ana
Items Mean � SD (r) to t
Weather 7.08 � 3.01 .61Aches and pains 6.85 � 2.82 .61Do alone 7.75 � 2.61 .45Not fun 7.11 � 2.81 .65Self-conscious 8.47 � 2.24 .64No support 7.84 � 2.47 .58Too busy 6.41 � 2.67 .66Away from home 4.77 � 3.12 .47Transportation 6.53 � 3.05 .65Stressed 7.71 � 2.57 .73Sick 3.25 � 2.76 .39Short of breath 6.67 � 2.92 .73Tired 6.52 � 2.81 .68Money worry 8.32 � 2.39 .58Need oxygen 7.67 � 3.18 .63Don’t feel like 6.73 � 3.09 .74
SD, Standard deviation. Data represent correlation (r) betweenif an individual item was deleted from the scale, factor loadingEfficacy), and eigenvalues of each factor.
nto a 9-item scale by Resnick and Jenkins21 to i
12 www.heartandlung.org
easure older adults’ self-efficacy for exercise. Thenternal consistency reliability Cronbach’s alphaas .92. Construct validity was evidenced by olderdults’ health status (measured by the short-formealth survey [12 items]) accounting for a total of1% of the variance in scores on the scale (mentalealth 17%; physical health an additional 4%).
The Ex-SRES is theoretically derived and hy-othesized to measure one underlying factor, ex-rcise self-regulatory efficacy. The factor patternf the Ex-SRES had a single factor with a highigenvalue of 6.79 accounting for a substantialercentage (77%) of the total variance. The screelot of eigenvalues was used to determine the num-er of factors. The scree plot was distinct with a
arge gap between the single factor and other po-ential factors that are largely indistinguishablerom scree (Fig 3). The finding that Ex-SRES repre-ents a single factor is consistent with findings ofcAuley24 and Resnick and Jenkins21 in sedentary
nd older adults. Conceptually, it is plausible thatndividuals with COPD share commonalities withedentary and older adults as related to exerciseelf-regulatory efficacy.
The findings of this study differ from that found
(�) Itemdeleted
Factorloadings Eigenvalues
.9119 .6465 6.7943
.9120 .6355 1.0140
.9168 .4664 .5201
.9109 .6827 .4392
.9112 .6616 .3536
.9131 .5999 .2518
.9106 .6800 .2194
.9162 .5262 .1808
.9109 .6682 .0382
.9084 .7608 �.0326
.9184 .4297 �.0750
.9085 .7690 �.0897
.9100 .7273 �.1349
.9130 .6123 �.1762
.9113 .6672 �.2211
.9081 .7757 �.2666
S and each item within the scale, Cronbach � for the scaleitem on the hypothesized factor (Exercise Self-Regulatory
lyses
otal
Ex-SREof each
n a group of patients undergoing cardiac rehabili-
MAY/JUNE 2007 HEART & LUNG

tHatsrmdotntFsmupt
EbummtS
mitb(TtJoaHmwttaSsroqucat
Davis et al Reliability and validity of the Ex-SRES
H
ation, in whom three factors were identified.25
owever, in that study, the measure was broadlypplied to health behavior changes and not specifico the domain of exercise. Also, because the mea-ure was administered by mail, the initial responseate was 48% and decreased to 26% from the secondeasurement period. Further, the researcher used a
ifferent theoretic basis of wellness motivation the-ry.25 Although it is not uncommon for researcherso use a cutoff eigenvalue of 1.0 to identify theumber of factors, a cutoff score is inherently arbi-rary and needs to be supported by the scree plot.30
urther, to ensure that scree is not interpreted as aeparate factor in a purely exploratory analysis, aore conservative approach with higher eigenval-
es of 2.0 to 3.0 may be considered, but mostreferential is the identification of factors by a prioriheory.32
Findings from item analyses suggested that thex-SRES does not suffer from floor or ceiling effectsecause all items except item 7 (too busy or sched-le conflicts) had a minimum value of 0 and maxi-um value of 10. Item 7 had a minimum of 1 andaximum of 10, which still represents a wide dis-
ribution of scores among the participants. The Ex-
Table IIIRelationships between the Exercise Self-Regulato[36 items]
Ex
Mean �
SF-36 total score 46.38 � 1Physical health 37.72 � 1Physical functioning 45.63 � 2Role-physical .96 � .7Bodily pain 70.81 � 2General health 47.45 � 2Mental health 54.70 � 1Vitality 54.89 � 1Social Functioning 80.34 � 2Role emotional 1.40 � .7Mental health 54.7 � 1
SD, Standard deviation; Ex-SRES, Exercise Self-Regulatory Erepresent correlation (r) between Ex-SRES and SF-36’s totSignificance values were set at alpha less than .05, which wouare due to chance.
*P � .05.
†P � .01.
RES also demonstrated evidence of adequate ho- m
EART & LUNG VOL. 36, NO. 3
ogeneity of the items. Correlations betweenndividual items and the total scale were all abovehe traditionally recommended .20,33 and the Cron-ach coefficient alpha did not increase significantlyby more than .05) when any item was deleted.hese results indicate that each item contributed tohe reliability of the Ex-SRES scale. Resnick andenkins21 used a structural equations approach tobtain values of squared multiple correlations as anlternative to the above for estimating reliability.34
owever, the advantages of this alternative and aore complex approach for assessing reliabilityere unclear. All of these findings support the re-
ention of all items as each item seems relevant tohe total score, and none of the items negativelyffected the internal consistency of the entire Ex-RES. The rationale is that the reliability of a mea-ure is based on the whole and a test of theoryather than individual items. The elimination of the-retically and clinically important items, such asuestions related to oxygen use or illness that areniquely relevant to individuals with COPD, mayompromise the scale’s theoretic underpinningsnd its replicability in a different sample. In addi-ion, a scale with very few items is less stable and
cacy Scale and the short-form healthy survey
r P
.37 �.0001†
.21 �.05*
.23 �.05*
.18 .07
.15 .13
.19 �.05*
.38 �.0001†
.41 �.0001†
.35 �.001†
.27 �.01†
.33 �.001†
Scale; SF-36, short-form health survey [36 items]. Dataphysical and mental components, and eight subscales.
ate that there is less than 5% probability that the findings
ry Effi
-SRES
SD
2.026.083.1794.781.293.628.972.2893.6
fficacyal score,ld indic
ay also be less robust with a greater probability of
www.heartandlung.org 213

ers
V
vscafhrS
oblsprfsttlst
plot of e
Reliability and validity of the Ex-SRES Davis et al
2
rror in measurement. Therefore, caution is war-anted when considering item reduction based onuggested cutoff points.31-33
alidityThe Ex-SRES demonstrated evidence of construct
alidity. As hypothesized, participants’ Ex-SREScores were significantly correlated with theoreti-ally relevant criterion measures of health statusnd their exercise behaviors. Consistent with theindings of Resnick and Jenkins,21 participants’ealth status was associated with their exercise self-egulatory efficacy. Participants’ scores on the Ex-
Fig 3 Scree
RES were significantly related to their total scores i
14 www.heartandlung.org
n the SF-36 and indicated that individuals withetter health status have higher exercise self-regu-
atory efficacy. Those with better health statuscored higher on both the physical and mental com-onents of the SF-36, also consistent with previouseports in another population.21 These findings con-irm our hypothesis that those with better healthtatus would be more apt to believe in their abilityo overcome impediments to exercise, and thereforeheir self-regulatory efficacy will be positively corre-ated to their health status. Participants’ exerciseelf-regulatory efficacy was significantly related tohe SF-36’s physical health component but not to all
igenvalues.
ts subscales within this component (role-physical
MAY/JUNE 2007 HEART & LUNG

allsadamowinssnetcitpwh
L
lqTiaadsttiaf1wuaaooenasas
hobvubteAvtitbttfsfi
C
feilttefnicuavvtcitesollboSa
Davis et al Reliability and validity of the Ex-SRES
H
nd bodily pain). Role-physical questions related toimitations in work and accomplishments within theast 4 weeks may have not been as applicable to thisample because most of the participants are retired,nd none were having an exacerbation at the time ofata collection. Similarly, bodily pain may not be aspplicable to individuals with COPD because theirost prominent symptom is not pain but shortness
f breath. These findings support that individualsith COPD may have unique concerns and suggest
t may be useful to incorporate measures of short-ess of breath and COPD specific physical healthtatus measures for future studies.35,36 As hypothe-ized, participants’ scores on the Ex-SRES were sig-ificantly related to their exercise behavior (minutesxercised per week) (r � .41; P � .0001), suggestinghat greater exercise self-regulatory efficacy is asso-iated with increased exercise behaviors. This find-ng provides further support of construct validity forhe Ex-SRES. This finding is also consistent withrevious findings in a sample of older adults inhom efficacy beliefs were related to exercise be-aviors.21
IMITATIONSGeneralizability beyond non-Hispanic whites is a
imitation of this study because the sample ac-uired had a minimum number of minority subjects.herefore, although the sample size is adequate fornitial testing of an instrument using the sample as
whole, the sample size was too small to conductnalyses divided by subgroups, such as race, gen-er, or age, to gain additional insight into exerciseelf-regulatory efficacy and exercise adherence inhese subgroups of individuals with COPD. Never-heless, because the recruitment of subjects for clin-cal studies is challenging, particularly in individu-ls with COPD, this study represents one of only aew studies that has a sample size of greater than00 in this population. Obtaining a larger sampleith enough power for subgroup analyses would beseful in future studies. Five subjects did not given answer for their efficacy beliefs related to theirbility to continue to exercise if they had to usexygen. All five subjects were not currently usingxygen and did not think they could answer. Theirfficacy beliefs for other items in the Ex-SRES wereot different from those of the rest of the sample. Inddition, overall exercise self-regulatory efficacycores were not different between those who are orre not using oxygen. It is possible that these five
ubjects, who are not using oxygen, cannot imagine eEART & LUNG VOL. 36, NO. 3
ow they might respond if they had to use oxygen,r they may think that if they need oxygen, they maye too ill to exercise. Some individuals may becomeery ill with an exacerbation that they are physicallynable to exercise. Also, individuals with COPD maye advised not to exercise or to exercise less whenhey are ill; therefore, their response may be influ-nced by recommendation of health care providers.s a result, it may be more informative to ask indi-iduals with COPD to indicate their efficacy belief inheir ability to resume exercising regularly after anllness or worsening of symptoms. Another limita-ion of the study is the use of self-reported exerciseehaviors. Although participants were asked aboutheir current exercise and their report had to detailhe type, frequency, and length of exercise per-ormed to minimize recall bias,37 additional mea-ures from logs or accelerometers would provideurther validation of participants’ exercise behav-ors.
ONCLUSIONExercise self-regulatory efficacy seems important
or understanding determinants of exercise adher-nce in individuals with COPD. Further understand-ng of exercise self-regulatory efficacy in this popu-ation may provide information that could informhe development and implement individualized andargeted interventions to improve exercise adher-nce in individuals with COPD. In addition, thisinding suggests a potential area that may be ame-able to the development and implementation of
nterventions to enhance exercise. Interventionsould target and seek to improve exercise self-reg-latory efficacy, which may in turn improve exercisedherence in this population. The Ex-SRES could beital in evaluating success of these types of inter-entions. An essential step in the further identifica-ion of essential components of exercise self-effi-acy beliefs is the development of reliable and validnstruments that measure concepts related to iden-ified components of exercise self-efficacy andxercise adherence. The Ex-SRES was developedpecifically for individuals with COPD and has dem-nstrated preliminary evidence of reliability and va-
idity. Further testing of the Ex-SRES in this popu-ation is warranted. Accordingly, the Ex-SRES maye a simple and useful tool to assess efficacy beliefsf individuals with COPD. With refinement, the Ex-RES could provide a basis for tailoring and evalu-ting clinical interventions designed to enhance ex-
rcise adherence in individuals with COPD.www.heartandlung.org 215

v
t
F
W
U
m
f
s
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
Reliability and validity of the Ex-SRES Davis et al
2
We are grateful to the study participants for their
aluable contributions and the pulmonary community for
heir support of this research study, particularly Bonnie
ahy, Rosemary Weese, Charlotte Werpy, and Elaine Allin.
e thank the UCSF Center of Symptom Management,
niversity of Arizona Dean’s Scholar, and Writer’s Group
embers. A special thank you goes to Ki Moore, PhD, RN,
or her ongoing support and mentorship, and Janet Lar-
on, PhD, RN, for her consultation on this project.
EFERENCES
1. Booth FW, Chakravarthy MV, Gordon SE, Spangenburg EE.Waging war against physical inactivity: cellular/molecularmechanisms as weaponry. J Appl Phys 2002;93:3-30.
2. National Center for Chronic Disease Health Promotion andPrevention, Physical Activity and Health: A Report of theSurgeon General. Available at: http://www.cdc.gov/needphp/sgr/sgr.htm
3. Lethbridge-Cejku M, Schiller JS, Bernadel L. Summary healthstatistics for U.S. adults: National Health Interview Survey,2002. Vital Health Stat 10. 2006 Aug; (229):1-104.
4. Centers for Disease Control and Prevention, National Centerfor Health Statistics, National Health Interview Survey.Health, United States, 2005. Available at: www.cdc.gov/nchs/hus.htm.
5. Celli BR, MacNee W; ATS/ERS Task Force. Standards for thediagnosis and treatment of patients with COPD: a summaryof the ATS/ERS position paper. Eur Respir J 2004;23:932-46.
6. Lacasse Y, Maltais F, Goldstein RS. Pulmonary rehabilitation:an integral part of the long-term management of COPD.Swiss Med Wkly 2004;134:41-2, 601-5.
7. Larson PJ, Carrieri-Kohlman V, Dodd MJ, Douglas M, FaucettJ, Froelicher E, et al. A model for symptom management.Image J Nurs Sch 1994;26:272-6.
8. Dodd M, Janson S, Facione N, Faucett J, Froelicher ES, Hum-phreys J, et al. Advancing the science of symptom manage-ment. J Adv Nurs 2001;33:668-76.
9. Garcia-Aymerich J, Farrero E, Felez MA, Izquierdo J, MarradesRM, Anto JM. Risk factors of readmission to hospital for aCOPD exacerbation: a prospective study. Thorax 2003;58:2:100-5.
0. Chao D, Foy CG, Farmer D. Exercise adherence among olderadults: challenges and strategies. Control Clin Trials 2000;21:(5 Suppl):212S-7S.
1. Bandura A. Self-efficacy: the exercise of control. New York:WH Freeman and Company; 1997.
2. Kaplan RM, Atkins CJ. Specific efficacy expectations mediateexercise compliance in patients with COPD. Health Psychol1984;3:3:223-42.
3. Davis AHT, Carrieri-Kohlman V, Janson SL, Gold WM, Stul-barg MS. Effects of treatment on two types of self-efficacy inpeople with chronic obstructive pulmonary disease. J PainSymptom Manage 2006;32:60-70.
4. Bandura A. Social foundations of thought and action: a socialcognitive theory. NJ: Prentice Hall; 1986.
5. Bandura A. Social cognitive theory: an agentic perspective.
Ann Rev Psychol 2001;52:1-26.16 www.heartandlung.org
6. Tsay SL, Chao YF. Effects of perceived self-efficacy and func-tional status on depression in patients with chronic heartfailure. J Nurs Res 2002;10:271-8.
7. McAuley E, Blissmer B, Katula J, and Duncan TE. Exerciseenvironment: self-efficacy, and affective responses to acuteexercise in older adults. Psychol Health 2000;15:341-57.
8. Steinhardt MA. Reliability and validity of expected outcomeand barriers for habitual physical activity. J Occup Med 1989;31:6:536-46.
9. Stock J, Cervone D. Proximal goal-setting and self-regulatoryprocesses. Cognit Ther Res 1990;14:483-98.
0. Sallis JF, Haskell WL, Fortmann SP, Vranizan KM, Taylor CB,Solomon DS. Predictors of adoption and maintenance ofphysical activity in a community sample. Prev Med 1986;5:331-41.
1. Resnick B, Jenkins LS. Testing the reliability and validity ofthe self-efficacy for exercise scale. Nurs Res 2000;49:3:154-9.
2. Toshima MT, Kaplan RM, and Ries AL. Self-efficacy expect-ancies in chronic obstructive pulmonary disease rehabilita-tion. Self-efficacy: thought control of action. Washington:Hemisphere; 1992:325-54.
3. Gormley J, Carrieri-Kohlman V, Douglas M. Treadmill self-efficacy and walking performance in patients with COPD.J Cardiopulm Rehabil 1993:6:424-31.
4. McAuley E. The role of efficacy cognitions in the prediction ofexercise behavior in middle-aged adults. J Behav Med 1992;15:65-88.
5. Fleury J. The index of self-regulation: development and psy-chometric analysis. J Nurs Meas 1998;6:1:3-17.
6. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R,Coates A, et al. Standardisation of spirometry. Eur Respir J2005;26:319-38.
7. Folstein M. Mini-mental and son. Int J Geriatr Psychiatry1998;13:5.
8. Ware JE Jr, Sherbourne CD. The MOS 36-item short-formhealth survey (SF-36): conceptual framework and item selec-tion. Med Care 1992;30:6:473-83.
9. Nunnally JC, Bernstein IH. Psychometric theory. 3rd ed. NewYork: McGraw-Hill; 1994.
0. Munro BH. Statistical methods for health care research. 4thed. Philadelphia: Lippincott; 2001.
1. Cohen J, Cohen P, West SG, Alken LS. Applied multipleregression/correlation analysis for the behavioral sciences.3rd ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 2003.
2. Gorsuch RL. Factor analysis. 2nd ed. Hillsdale, NJ: LawrenceErlbaum Associates; 1983.
3. Streiner DL, Norman GR. Health measurement scales: a prac-tical guide to their development and use. 2nd ed. New York:Oxford University Press; 1994.
4. Bollen K. Structural equations with latent variables. NewYork: Wiley; 1989.
5. Larson JL, Kapella MC, Wirtz S, Covey MK, Berry J. Reliabilityand validity of the functional performance inventory in pa-tients with moderate to severe chronic obstructive pulmo-nary disease. J Nurs Meas 1998;6:1:55-73.
6. Lareau S, Meek P, Roos P. Development and testing of themodified version of the Pulmonary Functional Status and Dys-pnea Questionnaire (PFSDQ-M). Heart Lung 1998;27:159-68.
7. Stulbarg MS, Carrieri-Kohlman V, Gormley J, Tsang AH, PaulS. Accuracy of recall of dyspnea after exercise training ses-
sions. J Cardiopulm Rehabil 1999;19:4:242-8.MAY/JUNE 2007 HEART & LUNG