relationships of sleep duration with sleep disturbances, basic socio-demographic factors, and bmi in...
TRANSCRIPT

Sleep Medicine 10 (2009) 1085–1089
Contents lists available at ScienceDirect
Sleep Medicine
journal homepage: www.elsevier .com/locate /s leep
Original Article
Relationships of sleep duration with sleep disturbances, basic socio-demographicfactors, and BMI in Chinese people
Yu-Tao Xiang a,b,*, Xin Ma a, Jin-Yan Lu b, Zhuo-Ji Cai a, Shu-Ran Li c, Ying-Qiang Xiang a, Hong-Li Guo a,Ye-Zhi Hou a, Zhen-Bo Li a, Zhan-Jiang Li a, Yu-Fen Tao a, Wei-Min Dang c, Xiao-Mei Wu a, Jing Deng a,Kelly Y.C. Lai b, Gabor S. Ungvari b
a Beijing Anding Hospital, Capital Medical University, Beijing, Chinab Department of Psychiatry, Chinese University of Hong Kong, Hong Kong SAR, Chinac Institute of Mental Health, Peking University, Beijing, China
a r t i c l e i n f o a b s t r a c t
Article history:Received 7 January 2009Received in revised form 5 March 2009Accepted 9 March 2009Available online 12 May 2009
Keywords:Long sleep syndromeShort sleep syndromeChinaEpidemiologyCommunityInsomnia
1389-9457/$ - see front matter � 2009 Elsevier B.V. Adoi:10.1016/j.sleep.2009.03.002
* Corresponding authors. Address: Department ofShatin, N.T., Hong Kong SAR, China. Tel.: +852 2636 7
E-mail address: [email protected] (Y.-T. Xiang).
Objective: This study aimed at determining the mean total sleep time (TST) and the relationship betweensleep duration and basic socio-demographic factors and BMI sleep problems in Chinese subjects.Method: A total of 5926 subjects were randomly selected and interviewed using standardized assessmenttools.Results: The reported mean TST was 7.76 h. Short sleepers were significantly older than medium and longsleepers. There were more urban residents who were short sleepers than medium and long sleepers.Short sleepers reported more sleep problems than medium and long sleepers. Short and long sleepersreported more psychiatric disorders than medium sleepers in both sexes, and short sleepers also hadmore major medical conditions in women. Short sleepers had a lower BMI than medium and long sleep-ers after controlling for the effects of age and psychiatric disorders in women.Conclusions: Nationwide epidemiologic surveys in China are needed to further explore the relationshipbetween sleep duration and sleep problems.
� 2009 Elsevier B.V. All rights reserved.
1. Introduction
Previous studies have indicated that both short and long sleepincrease total mortality risk [1–5]. To date, the mechanism of thisassociation is unknown [2]. Buysse and Ganguli [6] suggested thatshort sleep was due to several medical conditions or voluntarysleep restriction; whereas long sleep was associated with othersleep disturbances and a number of chronic medical and psychiat-ric disorders. A similar U-shaped relationship between sleep dura-tion and sleep complaints and BMI was also found [2,7,8]. Theseassociations between sleep duration and other clinical variableshave been posited as a clue to understanding the pathomechanismof increased mortality [7].
Over the past decade, socioeconomic, cultural, and racial factorshave been found to have important impacts on sleep problems[7,12]. The above-mentioned findings from Western countriesmay not be applicable in other socio-cultural contexts, and there-fore, investigations in Chinese populations are warranted. This
ll rights reserved.
Psychiatry, Shatin Hospital,748; fax: +852 2647 5321.
study set out to determine (1) the mean total sleep time (TST)and (2) the rates of short, medium, and long sleepers in the Chinesegeneral population. The types of sleep duration defined accordingto Heslop et al.’s criteria [1] include: short sleep: <7 h/day;medium sleep: 7–8 h/day; long sleep: >8 h/day; and (3) therelationships of short, medium, and long sleep with basic socio-demographic factors, selected sleep problems, and BMI (kg/m2)in Chinese people.
2. Methods
The method of the study, which was part of a large-scale epide-miologic survey of the prevalence of psychiatric disorders in Bei-jing, China, has been discussed in detail elsewhere [9,10]. Briefly,the study was based on a stratified, multistage, systematic, andprobability sample of permanent residents in Beijing who were15 years or older, lived with their family members, and had theability to comprehend the contents of the interview. The munici-pality of Beijing was chosen because it comprises both urban andrural areas. The study protocol was approved by the HumanResearch and Ethics Committee of Beijing Anding Hospital. Writtenconsent was obtained from each subject.
1086 Y.-T. Xiang et al. / Sleep Medicine 10 (2009) 1085–1089
The recruitment of study subjects took place as follows. (1)Neighborhood communities and village communities (NCs andVCs) in urban and rural regions, respectively, are basic communityorganizations with several hundreds of households in China. Fol-lowing the method of a previous psychiatric epidemiologic surveyin Beijing [11], 2% of the total NCs and VCs in Beijing, i.e., 126 NCsand VCs, with a total population of 313,356 persons were selectedusing a random number table that took into account the popula-tion and ratio of urban to rural residents in each of Beijing’s 18 dis-tricts and counties. In Beijing, residents are categorized as eitherurban or rural dwellers on their household cards, which are keptby the local Public Security Bureau. (2) On the basis of the prede-termined sampling interval and random starting points, 6267households from the 126 NCs/VCs were selected from the house-hold registry of the local Public Security Bureau. (3) The personin each selected household aged above 15 years whose date ofbirth was closest to April 1 was invited to participate in the study.As planned, the subjects of the study accounted for approximately2% of all the residents living in the 126 NCs and VCs.
Face to face household interviews were conducted. Socio-demo-graphic data were collected with a questionnaire designed for thestudy that inquired about TST, sleep disturbances, and major med-ical conditions affecting the cardiovascular, respiratory, digestive,hematological, endocrine, urinary, connective tissue, and nervoussystems. To determine TST in the past 12 months, subjects wereasked the following question: ‘‘On average, how many hours doyou sleep each night?” Reported sleep duration less than 2 or morethan 16 h each night was considered invalid information [2]. ThreeDSM-IV-defined sleep problems were detected in this study, i.e.,subjects were requested to answer ‘‘yes” or ‘‘no” to whether theyhad experienced three basic forms of sleep disturbance lasting 2weeks or longer in the past 12 months: first, difficulties initiatingsleep (DIS; specified as ‘‘it took you two hours or longer nearly everynight before you could fall sleep”); second, difficulties maintainingsleep (DMS; specified as ‘‘you woke up nearly every night and took
Table 1Basic socio-demographic characteristics of the participants (n = 5874).
Short sleepers (n = 806) Medium sleepers (n = 3845)
Mean (SD) Mean (SD)
Men (n = 2709)Age (years) 50.7 (15.6) 46.4 (16.6)BMI 24.3 (4.0) 24.2 (3.9)
N (%) N (%)
Urban 240 (69.8) 1102 (60.0)DIS 64 (18.6) 77 (4.2)DMS 68 (19.8) 90 (4.9)EMA 52 (15.1) 45 (2.4)Psychiatric disordersb 131 (38.1) 416 (22.6)Major medical condition(s) 119 (34.6) 498 (27.1)
Mean (SD) Mean (SD)
Women (n = 3165)Age (years) 55.2 (15.9) 46.2 (15.7)BMI 23.7 (4.0) 24.1 (4.1)
N (%) N (%)
Urban 299 (64.7) 1159 (57.7)DIS 136 (29.4) 146 (7.3)DMS 153 (33.1) 174 (8.7)EMA 103 (22.3) 98 (4.9)Psychiatric disordersb 198 (42.9) 340 (16.9)Major medical condition(s) 226 (48.9) 701 (34.9)
a A, short vs. medium; B, short vs. long sleepers; C, medium vs. long sleepers.b Psychiatric disorders include alcohol dependence, schizophrenia, major depressive ec No significant difference at level of 0.01.
an hour or more to get back to sleep”); and third, early morningawakening (EMA; specified as ‘‘you woke up nearly every morningat least two hours earlier than you wanted to”). These definitionsof sleep duration and insomnia have been used in recent studies[7,12]. Participants’ heights and weights were measured by theinterviewers before the interviews and their BMIs were calculated.
The Chinese version of the Composite International DiagnosticInterview-Version 1.0 (CIDI 1.0) that generates DSM-III-R diagno-ses was used to identify major psychiatric disorders including alco-hol dependence, schizophrenia, major depressive episode (MDE),generalized anxiety disorder (GAD), and phobias. The Chinese ver-sion of the CIDI 1.0 has satisfactory psychometric properties [13].The interviews were conducted by 102 qualified psychiatrists se-lected from 18 mental health services in Beijing. The interviewersunderwent training in epidemiological field work at a 10-dayworkshop and were given a detailed manual on the study methods.
Data were analyzed using SPSS 13.0 for Windows. Comparisonsof the basic socio-demographic and clinical characteristics andsleep problems of the different sleepers were performed by one-way ANOVA or chi-square test as appropriate. If these tests weresignificant, post-hoc tests were carried out. The level of statisticalsignificance was set at p < 0.01 to reduce the risk of Type I errordue to multiple tests.
3. Results
A total of 6251 subjects were approached and screened, with5926 meeting the study criteria and being interviewed. Responseswere invalid for 17 rural residents (0.7%) and 35 urban residents(1%), yielding a final sample of 5874.
The mean TST of the whole sample was 7.76 ± 1.22 h (95% CI:7.73–7.79 h), and short and long sleepers accounted for 13.7%(n = 806) and 20.8% (n = 1223) of the sample, respectively. Therewere more men among medium sleepers (47.8%) than short(42.7%) and long sleepers (43.2%; v2 = 12.3, df = 2, p = 0.002). Table
Long sleepers (n = 1223) Statistics Post-hoc analysesa
A B C
Mean (SD) F df p value
46.5 (19.1) 9.7 2.2706 <0.001 <0.001 <0.001 NSc
23.8 (3.9) 3.3 2.2706 0.036 – – –
N (%) v2 df p value
285 (54.0) 21.7 2 <0.001 0.001 <0.001 NS26 (4.9) 105.8 2 <0.001 <0.001 <0.001 NS26 (4.9) 104.8 2 <0.001 <0.001 <0.001 NS16 (3.0) 110.2 2 <0.001 <0.001 <0.001 NS165 (31.3) 44.0 2 <0.001 <0.001 NS <0.001151 (28.6) 8.0 2 0.018 � � �
Mean (SD) F df p value
47.8 (17.5) 57.4 2.3162 <0.001 <0.001 <0.001 NS24.1 (4.4) 1.6 2.3162 0.20 � � �
N (%) v2 df p value
325 (46.8) 40.7 2 <0.001 0.006 <0.001 NS44 (6.3) 214.9 2 <0.001 <0.001 <0.001 NS58 (8.3) 222.3 2 <0.001 <0.001 <0.001 NS33 (4.7) 175.4 2 <0.001 <0.001 <0.001 NS190 (27.3) 152.0 2 <0.001 <0.001 <0.001 <0.001217 (31.2) 41.3 2 <0.001 <0.001 <0.001 NS
pisode, generalized anxiety disorder, and phobias.
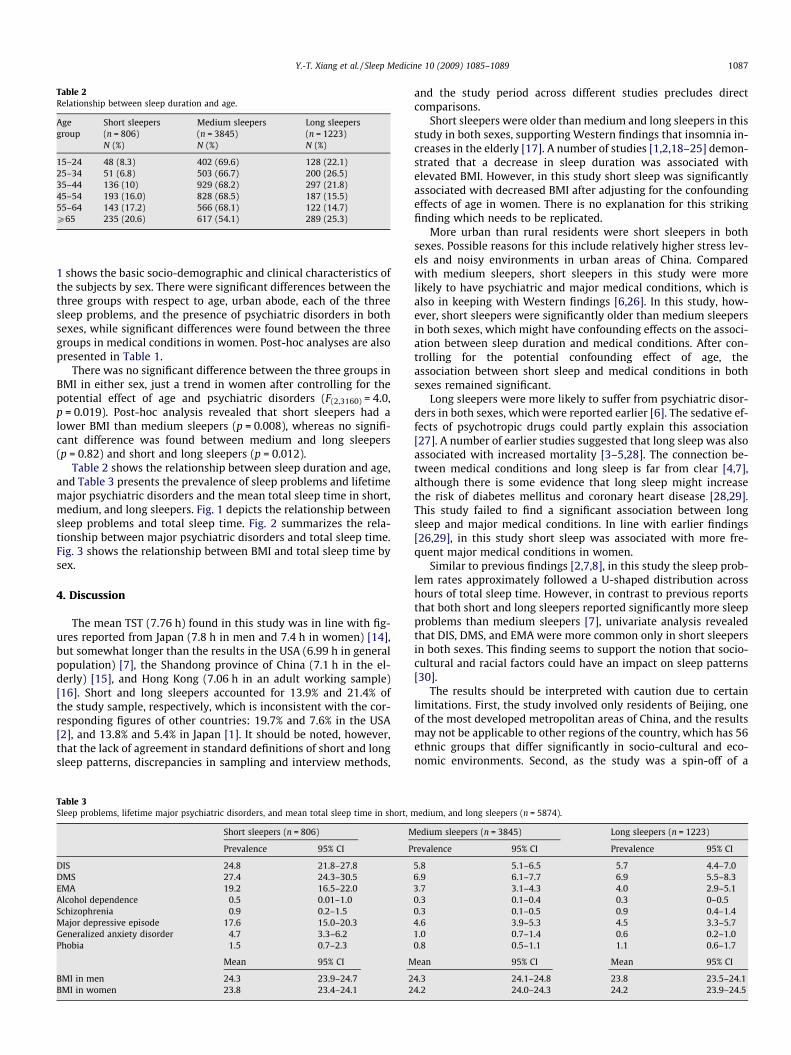
Table 2Relationship between sleep duration and age.
Agegroup
Short sleepers(n = 806)
Medium sleepers(n = 3845)
Long sleepers(n = 1223)
N (%) N (%) N (%)
15–24 48 (8.3) 402 (69.6) 128 (22.1)25–34 51 (6.8) 503 (66.7) 200 (26.5)35–44 136 (10) 929 (68.2) 297 (21.8)45–54 193 (16.0) 828 (68.5) 187 (15.5)55–64 143 (17.2) 566 (68.1) 122 (14.7)P65 235 (20.6) 617 (54.1) 289 (25.3)
Y.-T. Xiang et al. / Sleep Medicine 10 (2009) 1085–1089 1087
1 shows the basic socio-demographic and clinical characteristics ofthe subjects by sex. There were significant differences between thethree groups with respect to age, urban abode, each of the threesleep problems, and the presence of psychiatric disorders in bothsexes, while significant differences were found between the threegroups in medical conditions in women. Post-hoc analyses are alsopresented in Table 1.
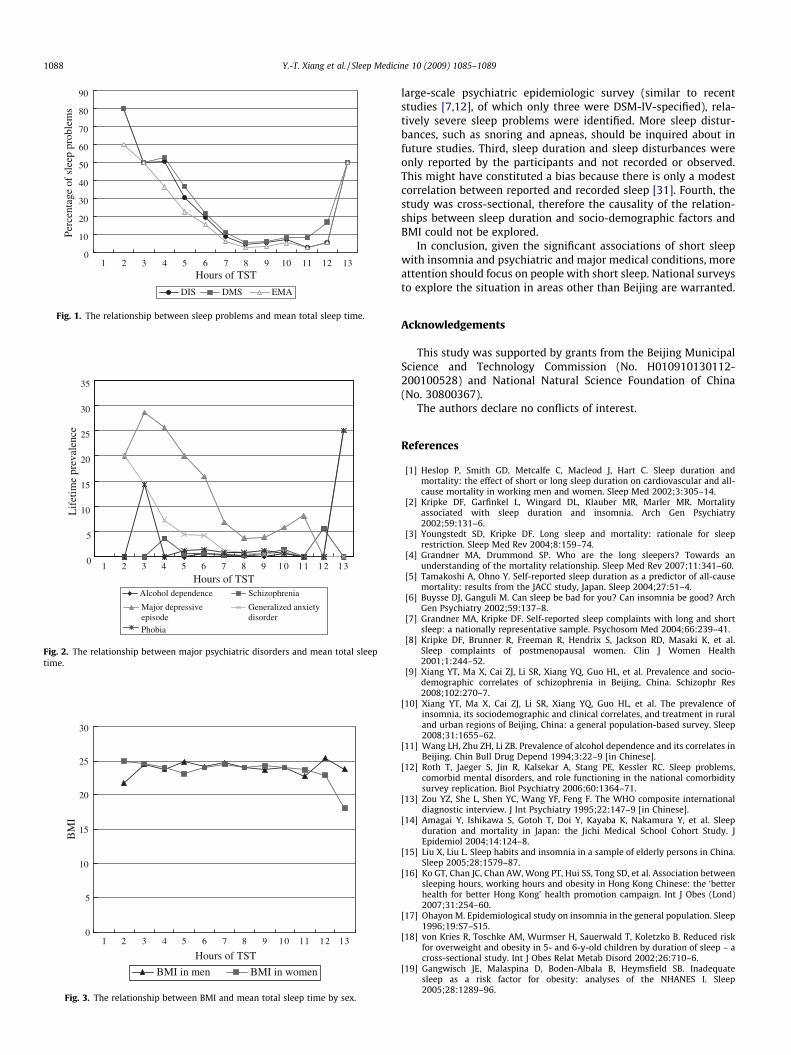
There was no significant difference between the three groups inBMI in either sex, just a trend in women after controlling for thepotential effect of age and psychiatric disorders (F(2,3160) = 4.0,p = 0.019). Post-hoc analysis revealed that short sleepers had alower BMI than medium sleepers (p = 0.008), whereas no signifi-cant difference was found between medium and long sleepers(p = 0.82) and short and long sleepers (p = 0.012).
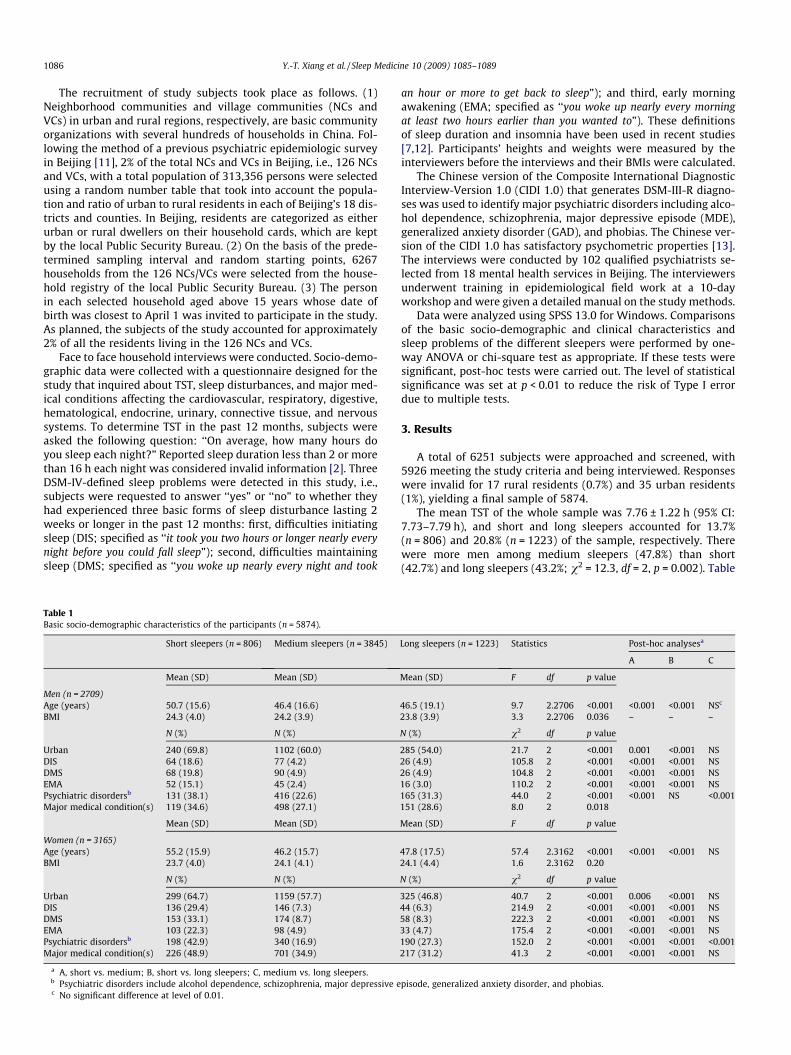
Table 2 shows the relationship between sleep duration and age,and Table 3 presents the prevalence of sleep problems and lifetimemajor psychiatric disorders and the mean total sleep time in short,medium, and long sleepers. Fig. 1 depicts the relationship betweensleep problems and total sleep time. Fig. 2 summarizes the rela-tionship between major psychiatric disorders and total sleep time.Fig. 3 shows the relationship between BMI and total sleep time bysex.
4. Discussion
The mean TST (7.76 h) found in this study was in line with fig-ures reported from Japan (7.8 h in men and 7.4 h in women) [14],but somewhat longer than the results in the USA (6.99 h in generalpopulation) [7], the Shandong province of China (7.1 h in the el-derly) [15], and Hong Kong (7.06 h in an adult working sample)[16]. Short and long sleepers accounted for 13.9% and 21.4% ofthe study sample, respectively, which is inconsistent with the cor-responding figures of other countries: 19.7% and 7.6% in the USA[2], and 13.8% and 5.4% in Japan [1]. It should be noted, however,that the lack of agreement in standard definitions of short and longsleep patterns, discrepancies in sampling and interview methods,
Table 3Sleep problems, lifetime major psychiatric disorders, and mean total sleep time in short, m
Short sleepers (n = 806) M
Prevalence 95% CI P
DIS 24.8 21.8–27.8DMS 27.4 24.3–30.5EMA 19.2 16.5–22.0Alcohol dependence 0.5 0.01–1.0Schizophrenia 0.9 0.2–1.5Major depressive episode 17.6 15.0–20.3Generalized anxiety disorder 4.7 3.3–6.2Phobia 1.5 0.7–2.3
Mean 95% CI M
BMI in men 24.3 23.9–24.7 2BMI in women 23.8 23.4–24.1 2
and the study period across different studies precludes directcomparisons.
Short sleepers were older than medium and long sleepers in thisstudy in both sexes, supporting Western findings that insomnia in-creases in the elderly [17]. A number of studies [1,2,18–25] demon-strated that a decrease in sleep duration was associated withelevated BMI. However, in this study short sleep was significantlyassociated with decreased BMI after adjusting for the confoundingeffects of age in women. There is no explanation for this strikingfinding which needs to be replicated.
More urban than rural residents were short sleepers in bothsexes. Possible reasons for this include relatively higher stress lev-els and noisy environments in urban areas of China. Comparedwith medium sleepers, short sleepers in this study were morelikely to have psychiatric and major medical conditions, which isalso in keeping with Western findings [6,26]. In this study, how-ever, short sleepers were significantly older than medium sleepersin both sexes, which might have confounding effects on the associ-ation between sleep duration and medical conditions. After con-trolling for the potential confounding effect of age, theassociation between short sleep and medical conditions in bothsexes remained significant.
Long sleepers were more likely to suffer from psychiatric disor-ders in both sexes, which were reported earlier [6]. The sedative ef-fects of psychotropic drugs could partly explain this association[27]. A number of earlier studies suggested that long sleep was alsoassociated with increased mortality [3–5,28]. The connection be-tween medical conditions and long sleep is far from clear [4,7],although there is some evidence that long sleep might increasethe risk of diabetes mellitus and coronary heart disease [28,29].This study failed to find a significant association between longsleep and major medical conditions. In line with earlier findings[26,29], in this study short sleep was associated with more fre-quent major medical conditions in women.
Similar to previous findings [2,7,8], in this study the sleep prob-lem rates approximately followed a U-shaped distribution acrosshours of total sleep time. However, in contrast to previous reportsthat both short and long sleepers reported significantly more sleepproblems than medium sleepers [7], univariate analysis revealedthat DIS, DMS, and EMA were more common only in short sleepersin both sexes. This finding seems to support the notion that socio-cultural and racial factors could have an impact on sleep patterns[30].
The results should be interpreted with caution due to certainlimitations. First, the study involved only residents of Beijing, oneof the most developed metropolitan areas of China, and the resultsmay not be applicable to other regions of the country, which has 56ethnic groups that differ significantly in socio-cultural and eco-nomic environments. Second, as the study was a spin-off of a
edium, and long sleepers (n = 5874).
edium sleepers (n = 3845) Long sleepers (n = 1223)
revalence 95% CI Prevalence 95% CI
5.8 5.1–6.5 5.7 4.4–7.06.9 6.1–7.7 6.9 5.5–8.33.7 3.1–4.3 4.0 2.9–5.10.3 0.1–0.4 0.3 0–0.50.3 0.1–0.5 0.9 0.4–1.44.6 3.9–5.3 4.5 3.3–5.71.0 0.7–1.4 0.6 0.2–1.00.8 0.5–1.1 1.1 0.6–1.7
ean 95% CI Mean 95% CI
4.3 24.1–24.8 23.8 23.5–24.14.2 24.0–24.3 24.2 23.9–24.5
0
5
10
15
20
25
30
35
1 2 3 4 5 6 7 8 9 10 11 12 13
Hours of TST
Lif
etim
e pr
eval
ence
Alcohol dependence Schizophrenia
Major depressiveepisode
Generalized anxietydisorder
Phobia
Fig. 2. The relationship between major psychiatric disorders and mean total sleeptime.
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10 11 12 13
Hours of TST
BM
I
BMI in men BMI in women
Fig. 3. The relationship between BMI and mean total sleep time by sex.
0
10
20
30
40
50
60
70
80
90
1 2 3 4 5 6 7 8 9 10 11 12 13Hours of TST
Perc
enta
ge o
f sl
eep
prob
lem
s
DIS DMS EMA
Fig. 1. The relationship between sleep problems and mean total sleep time.
1088 Y.-T. Xiang et al. / Sleep Medicine 10 (2009) 1085–1089
large-scale psychiatric epidemiologic survey (similar to recentstudies [7,12], of which only three were DSM-IV-specified), rela-tively severe sleep problems were identified. More sleep distur-bances, such as snoring and apneas, should be inquired about infuture studies. Third, sleep duration and sleep disturbances wereonly reported by the participants and not recorded or observed.This might have constituted a bias because there is only a modestcorrelation between reported and recorded sleep [31]. Fourth, thestudy was cross-sectional, therefore the causality of the relation-ships between sleep duration and socio-demographic factors andBMI could not be explored.
In conclusion, given the significant associations of short sleepwith insomnia and psychiatric and major medical conditions, moreattention should focus on people with short sleep. National surveysto explore the situation in areas other than Beijing are warranted.
Acknowledgements
This study was supported by grants from the Beijing MunicipalScience and Technology Commission (No. H010910130112-200100528) and National Natural Science Foundation of China(No. 30800367).
The authors declare no conflicts of interest.
References
[1] Heslop P, Smith GD, Metcalfe C, Macleod J, Hart C. Sleep duration andmortality: the effect of short or long sleep duration on cardiovascular and all-cause mortality in working men and women. Sleep Med 2002;3:305–14.
[2] Kripke DF, Garfinkel L, Wingard DL, Klauber MR, Marler MR. Mortalityassociated with sleep duration and insomnia. Arch Gen Psychiatry2002;59:131–6.
[3] Youngstedt SD, Kripke DF. Long sleep and mortality: rationale for sleeprestriction. Sleep Med Rev 2004;8:159–74.
[4] Grandner MA, Drummond SP. Who are the long sleepers? Towards anunderstanding of the mortality relationship. Sleep Med Rev 2007;11:341–60.
[5] Tamakoshi A, Ohno Y. Self-reported sleep duration as a predictor of all-causemortality: results from the JACC study, Japan. Sleep 2004;27:51–4.
[6] Buysse DJ, Ganguli M. Can sleep be bad for you? Can insomnia be good? ArchGen Psychiatry 2002;59:137–8.
[7] Grandner MA, Kripke DF. Self-reported sleep complaints with long and shortsleep: a nationally representative sample. Psychosom Med 2004;66:239–41.
[8] Kripke DF, Brunner R, Freeman R, Hendrix S, Jackson RD, Masaki K, et al.Sleep complaints of postmenopausal women. Clin J Women Health2001;1:244–52.
[9] Xiang YT, Ma X, Cai ZJ, Li SR, Xiang YQ, Guo HL, et al. Prevalence and socio-demographic correlates of schizophrenia in Beijing, China. Schizophr Res2008;102:270–7.
[10] Xiang YT, Ma X, Cai ZJ, Li SR, Xiang YQ, Guo HL, et al. The prevalence ofinsomnia, its sociodemographic and clinical correlates, and treatment in ruraland urban regions of Beijing, China: a general population-based survey. Sleep2008;31:1655–62.
[11] Wang LH, Zhu ZH, Li ZB. Prevalence of alcohol dependence and its correlates inBeijing. Chin Bull Drug Depend 1994;3:22–9 [in Chinese].
[12] Roth T, Jaeger S, Jin R, Kalsekar A, Stang PE, Kessler RC. Sleep problems,comorbid mental disorders, and role functioning in the national comorbiditysurvey replication. Biol Psychiatry 2006;60:1364–71.
[13] Zou YZ, She L, Shen YC, Wang YF, Feng F. The WHO composite internationaldiagnostic interview. J Int Psychiatry 1995;22:147–9 [in Chinese].
[14] Amagai Y, Ishikawa S, Gotoh T, Doi Y, Kayaba K, Nakamura Y, et al. Sleepduration and mortality in Japan: the Jichi Medical School Cohort Study. JEpidemiol 2004;14:124–8.
[15] Liu X, Liu L. Sleep habits and insomnia in a sample of elderly persons in China.Sleep 2005;28:1579–87.
[16] Ko GT, Chan JC, Chan AW, Wong PT, Hui SS, Tong SD, et al. Association betweensleeping hours, working hours and obesity in Hong Kong Chinese: the ‘betterhealth for better Hong Kong’ health promotion campaign. Int J Obes (Lond)2007;31:254–60.
[17] Ohayon M. Epidemiological study on insomnia in the general population. Sleep1996;19:S7–S15.
[18] von Kries R, Toschke AM, Wurmser H, Sauerwald T, Koletzko B. Reduced riskfor overweight and obesity in 5- and 6-y-old children by duration of sleep – across-sectional study. Int J Obes Relat Metab Disord 2002;26:710–6.
[19] Gangwisch JE, Malaspina D, Boden-Albala B, Heymsfield SB. Inadequatesleep as a risk factor for obesity: analyses of the NHANES I. Sleep2005;28:1289–96.

Y.-T. Xiang et al. / Sleep Medicine 10 (2009) 1085–1089 1089
[20] Gupta NK, Mueller WH, Chan W, Meininger JC. Is obesity associated with poorsleep quality in adolescents? Am J Hum Biol 2002;14:762–8.
[21] Hasler G, Buysse DJ, Klaghofer R, Gamma A, Ajdacic V, Eich D, et al. Theassociation between short sleep duration and obesity in young adults: a 13-year prospective study. Sleep 2004;27:661–6.
[22] Locard E, Mamelle N, Billette A, Miginiac M, Munoz F, Rey S. Risk factors ofobesity in a five year old population. Parental versus environmental factors. IntJ Obes Relat Metab Disord 1992;16:721–9.
[23] Singh M, Drake CL, Roehrs T, Hudgel DW, Roth T. The association betweenobesity and short sleep duration: a population-based study. J Clin Sleep Med2005;1:357–63.
[24] Vioque J, Torres A, Quiles J. Time spent watching television, sleep duration andobesity in adults living in Valencia, Spain. Int J Obes Relat Metab Disord2000;24:1683–8.
[25] Vorona RD, Winn MP, Babineau TW, Eng BP, Feldman HR, Ware JC. Overweightand obese patients in a primary care population report less sleep than patientswith a normal body mass index. Arch Intern Med 2005;165:25–30.
[26] Ayas NT, White DP, Manson JE, Stampfer MJ, Speizer FE, Malhotra A, et al. Aprospective study of sleep duration and coronary heart disease in women.Arch Intern Med 2003;163:205–9.
[27] Shen YC. Psychiatry. In: Sun BT, editor. Prophylaxis of accidents in psychiatricnursing. Beijing: People’s Medical Publishing House; 2002. p. 1–13.
[28] Patel SR, Ayas NT, Malhotra MR, White DP, Schernhammer ES, Speizer FE, et al.A prospective study of sleep duration and mortality risk in women. Sleep2004;27:440–4.
[29] Gottlieb DJ, Punjabi NM, Newman AB, Resnick HE, Redline S, Baldwin CM, et al.Association of sleep time with diabetes mellitus and impaired glucosetolerance. Arch Intern Med 2005;165:863–7.
[30] Gureje O, Makanjuola VA, Kola L. Insomnia and role impairment in thecommunity: results from the Nigerian survey of mental health and wellbeing.Soc Psychiatry Psychiatr Epidemiol 2007;42:495–501.
[31] Hoch CC, Reynolds CF, Kupfer DJ, Berman SR, Houck PR, Stack JA. Empiricalnote: self-report versus recorded sleep in healthy seniors. Psychophysiology1987;24:293–9.