relationships between gastric emptying, postprandial...
TRANSCRIPT

Relationships Between GastricEmptying, Postprandial Glycemia, andIncretin HormonesCHINMAY S. MARATHE, MBBS
CHRISTOPHER K. RAYNER, MBBS, PHD, FRACP
KAREN L. JONES, DIP APP SCI (NUCLEAR
MEDICINE), PHD
MICHAEL HOROWITZ, MBBS, PHD, FRACP
The importance of achieving tightglycemic control, usually assessedby glycated hemoglobin (HbA1c),
for both the prevention and delay in theprogression of diabetes-relatedmicrovascu-lar complications, is established, and theAmerican Diabetes Association/EuropeanAssociation for the Study of Diabetes jointcommittee has recommended an HbA1c
,7% as the goal in patients with type 2diabetes (1). The relative contributions ofpre- and postprandial glycemia to HbA1c
have been clarified during the last decadefollowing the seminal report by Monnieret al. (2) indicating that in type 2 diabetes,postprandial glycemic excursions ac-count for about 70% of variability whenHbA1c is ,7.3%, while the contributionof “fasting” glycemia is greater in less well-controlled patients. Subsequent studieshave confirmed the predominance ofpostprandial glycemia in determiningoverall glycemic control in “well-controlled”type 2 diabetic patients managed by oralhypoglycemic agents or basal insulin (3).The importance of postprandial glycemiato overall glycemic control is not surpris-ing considering that 1) humans in mod-ern societies spend only about 3 or 4 hbefore breakfast in a truly fasting state be-cause in health, gastric emptying of mealsoccurs at an overall rate of 1–4 kcal/min(4), and 2) postprandial hyperglycemiaoccurs frequently in diabetes (1). The rel-evance of postprandial glycemia is fur-ther increased by the recognition that itmay represent an independent risk factorfor adverse cardiovascular outcomes in
both diabetic and nondiabetic popula-tions (5).
The determinants of postprandial gly-cemia include preprandial glycemic levels,meal composition, gastric emptying, insulinsecretion, small intestinal glucose absorp-tion, and hepatic and peripheral glucosemetabolism. Furthermore, the relative con-tribution of each of these factors may varyover time during the postprandial state.Nevertheless, both the rate of gastric emp-tying and the secretion and action of theincretin hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulino-tropic peptide (GIP), exert amajor influence(6). The latter limit postprandial glycemiathrough their insulinotropic and, in thecase of GLP-1, glucagonostatic actions.They account for the “incretin effect”danaugmentation of insulin secretion followingoral or enteral glucose exposure when com-pared with an isoglycemic intravenous glu-cose infusiondwhich is diminished intype 2 diabetes (7). GIP and GLP-1 are re-leased from entero-endocrine cells locatedmost densely in the proximal small intes-tine and distal small intestine/colon, re-spectively, following nutrient exposure.Each macronutrient has the capacity tostimulate GLP-1 and GIP release, althoughthe mechanisms underlying secretion dif-fer, and fat and carbohydrate may be morepotent stimuli than protein (8). Carbohy-drates, for example, stimulate incretin se-cretion through a number of interrelatedmechanisms that are likely to include thesodium-glucose cotransporter-1 (SGLT-1)and intestinal “sweet taste” receptors (8).
Following their release, the incretin hor-mones are rapidly degraded to inactiveme-tabolites by the ubiquitous enzyme,dipeptidyl peptidase-4 (DPP-IV). WhileGIP may be the most important incretinhormone in health, its capacity to stimulateinsulin is markedly diminished in type 2diabetes (8).
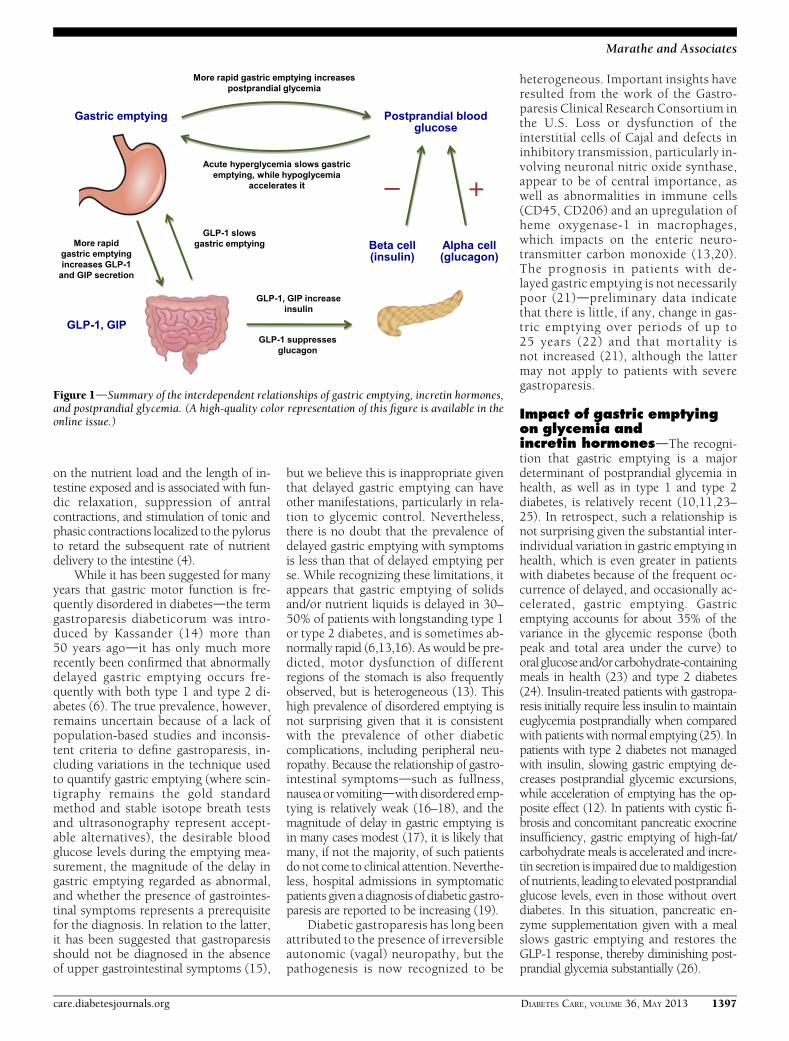
Even relatively minor variations ingastric emptying can have a major impacton the postprandial glycemic profile inhealth and type 2 diabetes (9–12). It isnow recognized that complex, interde-pendent relationships exist between gas-tric emptying, the incretin axis, andpostprandial glycemia, with the rate ofgastric emptying having a major impacton the magnitude of both the glycemicexcursion and incretin hormone secretionand, conversely, acute hyperglycemia andGLP-1 exerting negative feedback on gas-tric emptying (6). This review focuses onthese interrelationships, summarized inFig. 1, and the consequent implicationsfor dietary and pharmacological strategiesto manage postprandial glycemia in type2 diabetes.
Gastric emptying in healthand diabetesdIt is not well recog-nized that in both health and diabetes, therate of gastric emptying shows wide in-terindividualdwith much less intraindi-vidualdvariation (4). Gastric emptying isdetermined by the integration of motoractivity of the stomach and upper smallintestine, controlled by electrical slowwaves generated by the interstitial cellsof Cajal (4,13). The proximal stomach ini-tially relaxes to accommodate a meal andthe antrum then grinds solids to a smallparticle size (1–2 mm), before the chymeis pumped across the pylorus, predomi-nantly in a pulsatile manner (4). These pro-cesses are regulated primarily by inhibitoryfeedback arising from the interaction of nu-trients with the small intestine rather thanby “intragastric” mechanisms, and modu-lated by both stimulation of the vagus nerveand the secretion of gut hormones, includ-ing GLP-1, cholecystokinin (CCK), andpeptide YY (PYY). The magnitude of smallintestinal inhibitory feedback is dependent
c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c
From the Discipline of Medicine, University of Adelaide, Royal Adelaide Hospital, Adelaide, Australia, and theCentre of Clinical Research Excellence in Nutritional Physiology, Interventions and Outcomes, Universityof Adelaide, Adelaide, Australia.
Corresponding author: Michael Horowitz, [email protected] 10 August 2012 and accepted 15 November 2012.DOI: 10.2337/dc12-1609© 2013 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and thework is not altered. See http://creativecommons.org/licenses/by-nc-nd/3.0/ for details.
1396 DIABETES CARE, VOLUME 36, MAY 2013 care.diabetesjournals.org
R E V I E W A R T I C L E
on the nutrient load and the length of in-testine exposed and is associated with fun-dic relaxation, suppression of antralcontractions, and stimulation of tonic andphasic contractions localized to the pylorusto retard the subsequent rate of nutrientdelivery to the intestine (4).
While it has been suggested for manyyears that gastric motor function is fre-quently disordered in diabetesdthe termgastroparesis diabeticorum was intro-duced by Kassander (14) more than50 years agodit has only much morerecently been confirmed that abnormallydelayed gastric emptying occurs fre-quently with both type 1 and type 2 di-abetes (6). The true prevalence, however,remains uncertain because of a lack ofpopulation-based studies and inconsis-tent criteria to define gastroparesis, in-cluding variations in the technique usedto quantify gastric emptying (where scin-tigraphy remains the gold standardmethod and stable isotope breath testsand ultrasonography represent accept-able alternatives), the desirable bloodglucose levels during the emptying mea-surement, the magnitude of the delay ingastric emptying regarded as abnormal,and whether the presence of gastrointes-tinal symptoms represents a prerequisitefor the diagnosis. In relation to the latter,it has been suggested that gastroparesisshould not be diagnosed in the absenceof upper gastrointestinal symptoms (15),
but we believe this is inappropriate giventhat delayed gastric emptying can haveother manifestations, particularly in rela-tion to glycemic control. Nevertheless,there is no doubt that the prevalence ofdelayed gastric emptying with symptomsis less than that of delayed emptying perse. While recognizing these limitations, itappears that gastric emptying of solidsand/or nutrient liquids is delayed in 30–50% of patients with longstanding type 1or type 2 diabetes, and is sometimes ab-normally rapid (6,13,16). As would be pre-dicted, motor dysfunction of differentregions of the stomach is also frequentlyobserved, but is heterogeneous (13). Thishigh prevalence of disordered emptying isnot surprising given that it is consistentwith the prevalence of other diabeticcomplications, including peripheral neu-ropathy. Because the relationship of gastro-intestinal symptomsdsuch as fullness,nausea or vomitingdwith disordered emp-tying is relatively weak (16–18), and themagnitude of delay in gastric emptying isin many cases modest (17), it is likely thatmany, if not the majority, of such patientsdo not come to clinical attention.Neverthe-less, hospital admissions in symptomaticpatients given a diagnosis of diabetic gastro-paresis are reported to be increasing (19).
Diabetic gastroparesis has long beenattributed to the presence of irreversibleautonomic (vagal) neuropathy, but thepathogenesis is now recognized to be
heterogeneous. Important insights haveresulted from the work of the Gastro-paresis Clinical Research Consortium inthe U.S. Loss or dysfunction of theinterstitial cells of Cajal and defects ininhibitory transmission, particularly in-volving neuronal nitric oxide synthase,appear to be of central importance, aswell as abnormalities in immune cells(CD45, CD206) and an upregulation ofheme oxygenase-1 in macrophages,which impacts on the enteric neuro-transmitter carbon monoxide (13,20).The prognosis in patients with de-layed gastric emptying is not necessarilypoor (21)dpreliminary data indicatethat there is little, if any, change in gas-tric emptying over periods of up to25 years (22) and that mortality isnot increased (21), although the lattermay not apply to patients with severegastroparesis.
Impact of gastric emptyingon glycemia andincretin hormonesdThe recogni-tion that gastric emptying is a majordeterminant of postprandial glycemia inhealth, as well as in type 1 and type 2diabetes, is relatively recent (10,11,23–25). In retrospect, such a relationship isnot surprising given the substantial inter-individual variation in gastric emptying inhealth, which is even greater in patientswith diabetes because of the frequent oc-currence of delayed, and occasionally ac-celerated, gastric emptying. Gastricemptying accounts for about 35% of thevariance in the glycemic response (bothpeak and total area under the curve) tooral glucose and/or carbohydrate-containingmeals in health (23) and type 2 diabetes(24). Insulin-treated patients with gastropa-resis initially require less insulin to maintaineuglycemia postprandially when comparedwith patients with normal emptying (25). Inpatients with type 2 diabetes not managedwith insulin, slowing gastric emptying de-creases postprandial glycemic excursions,while acceleration of emptying has the op-posite effect (12). In patients with cystic fi-brosis and concomitant pancreatic exocrineinsufficiency, gastric emptying of high-fat/carbohydrate meals is accelerated and incre-tin secretion is impaired due tomaldigestionof nutrients, leading to elevatedpostprandialglucose levels, even in those without overtdiabetes. In this situation, pancreatic en-zyme supplementation given with a mealslows gastric emptying and restores theGLP-1 response, thereby diminishing post-prandial glycemia substantially (26).
Figure 1dSummary of the interdependent relationships of gastric emptying, incretin hormones,and postprandial glycemia. (A high-quality color representation of this figure is available in theonline issue.)
care.diabetesjournals.org DIABETES CARE, VOLUME 36, MAY 2013 1397
Marathe and Associates

The relationship of glycemiawith smallintestinal glucose delivery has recentlybeen shown to be nonlinear based on theoutcome of studies in which glucose wasinfused directly into the duodenum at ratesspanning the normal range of gastric emp-tying (i.e., 1–4 kcal/min) in healthy young(10) and older (27) subjects and patientswith type 2 diabetes managed by diet alone(11). In these groups, intraduodenal infu-sion of glucose at 1 kcal/minwas associatedwith only a modest rise in blood glucose,and while the glycemic responses to loadsof 2 kcal/min, 3 kcal/min, and 4 kcal/minwere substantially greater, there was littledifference between them (Fig. 2). The latterprobably reflects the much greater plasmainsulin response to the higher (i.e., 3 and 4kcal/min) intraduodenal glucose loads,which is, in turn, attributable to a muchgreaterGLP-1 response. PlasmaGIP, unlikeGLP-1, rises in an approximately linearfashion with increasing glucose loads(10,11,27). In other studies of healthy sub-jects and patients with type 2 diabetes, theeffects of initially more rapid intraduodenalglucose delivery, when compared with de-livery of the same amount of glucose at aconstant rate, were explored (9,28). Whilethe initial plasma insulin, GLP-1, and GIPresponses were predictably greater with theformer approach, therewas nodifference inthe overall glycemic response, implyingthat the initial increase in insulin was inad-equate to compensate for the greater load ofglucose absorbed. A fundamental implica-tion of these studies is that the magnitudeof the incretin effect in a given individualwill be dependent on their rate of gastricemptying, i.e., the incretin effect shouldbe greater in an individual, healthy orwith type 2 diabetes, whose stomachempties at 4 kcal/min when comparedwith another in whom emptying occursat 2 kcal/min, although the former situ-ation would also favor an initially greaterpostprandial glycemic excursion. Thisconcept is supported by recent evidencefrom our laboratory (29). Hence, studiesrelating to incretin hormone secretionshould take into account the rate of gas-tric emptying (which has hitherto fre-quently not been the case). The incretinhormone responses to a meal, parti-cularly that of GLP-1, appear to represent adynamic compensatory mechanism tominimize postprandial glycemia whenemptying is relatively more rapid. In ahealthy individual, the relative importanceof GIP and GLP-1 in determining the incre-tin effect is likely to be dependent on therate of gastric emptying. In an individual
Figure 2dData are mean 6 SEM. Blood glucose (A), plasma insulin (B), plasma GLP-1 (C),and plasma GIP (D) concentrations in response to a 120-min intraduodenal glucose infusion at1 kcal/min (G1), 2 kcal/min (G2), 4 kcal/min (G4), or (intraduodenal) saline control (S) in 10healthy subjects and eight type 2 diabetic patients. *P, 0.05 vs. control, #P, 0.05 vs. G1, xP,0.05 vs. G2. Reprinted with permission from Ma et al. (11).
1398 DIABETES CARE, VOLUME 36, MAY 2013 care.diabetesjournals.org
Gastric emptying and diabetes

with type 2 diabetes, the magnitude ofGLP-1 response is likely to be crucial giventhe reduced insulinotropic effect ofGIP (7).Wewould speculate that tominimize post-prandial glycemic excursions in individualswith type 2 diabetes, gastric emptying ofcarbohydrates should be slowed to about1 kcal/min in those whose emptying ismore rapid than this. As has been sug-gested, the prompt amelioration of type 2diabetes after Roux-en-Y gastric bypasssurgery is likely to reflect, at least inpart, an exaggerated incretin (particularlyGLP-1) response (30) consequent to dra-matically accelerated gastric emptying ofnutrient-containing liquids and “semi-solids” (31).
As well as being a determinant ofglycemia, gastric emptying is itself mod-ulated by acute changes in the bloodglucose concentration (6,32). Whilethere is a lack of consensus in relationto the magnitude of the effect of acutehyperglycemia and the potential influ-ence of chronic elevation of blood glu-cose, it is clear that marked acutehyperglycemia (i.e., blood glucose level;15 mmol/L) delays gastric emptyingsubstantially in both health and type 1diabetes when compared with euglyce-mia (;5 mmol/L). Emptying is slowedeven at physiological degrees of hy-perglycemia (;8 mmol/L) (32) and isaccelerated during insulin-induced hy-poglycemia (33); the latter response isevident even in patients with autonomicneuropathy and gastroparesis and likelyrepresents an important counterregula-tory mechanism to facilitate carbohydrateabsorption (33). Acute hyperglycemia at-tenuates the gastrokinetic effect of eryth-romycin (34), and this effect is likely alsoto apply to other prokinetic drugs. It re-mains to be determined whether the ef-fects of drugs that slow gastric emptyingare also modulated by acute changes inthe blood glucose concentration, but thisappears intuitively likely. The mecha-nisms by which acute hyperglycemiamodulates gastric emptying are poorlydefined, but nitrergic pathways appearimportant (35).
Effects of endogenousand exogenousincretin hormones ongastric emptyingdGIP and GLP-1differ in their effects on gastric emptying.Studies using the GLP-1 receptor antag-onist, exendin 9–39, indicate that endog-enous GLP-1 slows gastric emptyingmodestly (36) and affects intragastric
meal distribution (37) as a result of sup-pression of antro-duodenal motility andstimulation of pyloric contractions (38).That not all investigators have demon-strated effects on emptying probably re-flects methodological issues, includingthe composition of the test meal and theuse of suboptimal techniques to measuregastric emptying (37,39). The indirect as-sessment of gastric emptying using theabsorption kinetics of oral paracetamolis imprecise, but has been widely used.
Acute, intravenous infusion of GLP-1(in pharmacological doses) slows gastricemptying markedly in both healthy sub-jects and patients with type 2 diabetes in adose-dependent manner (40–42) bymechanisms that include relaxation ofthe proximal stomach, reduction of antraland duodenal motility, and an increase inpyloric tone (43), andwhich involve vagalpathways (44). With pharmacologicaldoses of GLP-1, nausea appears to occurrarely, unlike the situation with GLP-1agonists (as discussed below). By contrast,in healthy subjects, exogenousGIP in phar-macological doses does not slow gastricemptying (45) and may accelerate it mod-estly (46).
The magnitude of the retardation ofgastric emptying induced by exogenousGLP-1 is influenced by the baseline rate ofemptying, i.e., slowing is more marked inthose with more rapid gastric emptying.
For example, in the critically ill, GLP-1slows gastric emptying when the latter isnormal but not when it is delayed (47)(Fig. 3). Importantly, the reduction inpostprandial glycemia induced by exoge-nous GLP-1 is also closely related to themagnitude of the slowing of gastric emp-tying being greater when baseline empty-ing is relatively more rapid (42,47).Indeed, the effect of acute administrationof GLP-1 to slow gastric emptying out-weighs its insulinotropic effect, so thatwhile GLP-1 stimulates insulin duringhyperglycemia in the fasted state, post-prandial insulin concentrations are sup-pressed, rather than stimulated, in bothhealth and type 2 diabetes (40,42), andwhen the GLP-1-induced slowing of gas-tric emptying is reversed by administeringerythromycin, the insulinotropic actionof GLP-1 is unmasked (48). Accordingly,it is arguable whether GLP-1 should beregarded as a true incretin hormone ac-cording to Creutzfeldt’s definition (49).No studies have evaluated the effect ofexogenous GLP-1 on gastric emptying inpatients with gastroparesis, although it isknown that the relaxation of the proximalstomach induced by exogenous adminis-tration of GLP-1 is attenuated in diabeticpatients with autonomic neuropathy(50). Hence the magnitude of the slowingof gastric emptying induced by GLP-1will almost certainly be reduced in
Figure 3dRelationship between the effect of GLP-1 (1.2 pmol/kg/min intravenous) on gastricemptying and the rate of gastric emptying on placebo in critically ill patients (n = 25). Gastricemptying of a 100-mL nutrient liquid (Ensure) labeled with 13C octanoic acid was measured witha breath test and the gastric emptying coefficient (GEC) determined. A lower GEC is indicative ofmore rapid gastric emptying. R =20.48, P, 0.001. Reprinted with permission from Deane et al.(47).
care.diabetesjournals.org DIABETES CARE, VOLUME 36, MAY 2013 1399
Marathe and Associates

gastroparesis. It is also not knownwhetherthe GLP-1–induced slowing of gastricemptying can be “overridden” by hypogly-cemia, which, as discussed, is associatedwith prompt acceleration of emptying(33). This issue should be addressed, par-ticularly where GLP-1 agonists are used incombination with sulfonylureas or insulinwhen the propensity to hypoglycemia willbe increased.
A recent report suggests that theremay be rapid tachyphylaxis to the slowingof gastric emptying induced by exoge-nous GLP-1 (51). In that study, two liquidmeals, separated by 4 h, were given tohealthy volunteers during intravenous in-fusion of GLP-1 or placebo. GLP-1 wasshown to slow emptying of both mealsmarkedly, but the magnitude of the slow-ing of the second meal was less. It wassuggested that this tachyphylaxis occursat the level of the vagus nerve (51). Whilethe study hadmethodological limitations,the observations are of considerable inter-est and likely to be relevant to the ob-served effects of GLP-1 agonists ongastric emptying (as discussed below).
Modulation of gastricemptying to minimizepostprandial glycemicexcursions in type 2diabetesdA number of strategieshave been proposed to optimize post-prandial glycemic control based on mod-ulation of gastric emptying, stimulated byinsights relating to the impact of empty-ing on glycemia and incretin hormonesecretion. The focus of these strategies hasbeen type 2 diabetes, underpinned by therationale that a slower rate of nutrientdelivery to the small intestine would bedesirable to compensate for the delay ininsulin release and the resistance to itsactions, which are characteristic of thisdisease. The approaches include modify-ing the macronutrient content of meals,the use of fat and protein preloads, andpharmacological agents, particularlyGLP-1–based therapies and the amylinanalog, pramlintide (6).
In type 1 diabetes, gastric emptyingneeds to be predictable rather than specif-ically normal, delayed, or more rapid, toallow for accurate dosing of exogenous,short-acting insulin, although gastroparesisprobably increases the propensity for hy-poglycemia in the postprandial period(52), providing a rationale for measure-ment of emptying in patients with other-wise unexplained hypoglycemia. Studiesusing gastrokinetic drugs to improve
glycemic control in type 1 diabetic patientshave substantial methodological limita-tions and have yielded inconsistent obser-vations.
A number of studies have evaluatedthe effects of modifying the macronutri-ent and fiber content of meals based ontheir putative effects on gastric emptyingand/or incretin secretion. For example,increasing dietary fiber (53) or addingguar gum (54) slows emptying and re-duces postprandial glucose in type 2 di-abetes probably as a result of retardationof both gastric emptying and intestinalglucose absorption. Incorporating fatinto a carbohydrate-rich meal also slowsgastric emptying and improves the post-prandial glycemic profile, albeit at thecost of increasing the energy load (55).An increase in the protein content of thediet from 15 to 30% for 5 weeks reducespostprandial glycemia, as well as HbA1c,in patients with type 2 diabetes (56). Inthe latter study, the higher protein con-tent was at the cost of carbohydrates, andthe total energy intake remained stable.Longer-term studies are indicated todetermine whether these benefits aresustained.
Macronutrient preloadsAs discussed, fat, protein, and carbohy-drates stimulate incretin secretion byvarious mechanisms and retard gastricemptying. These effects underlie thenovel strategy of administering a smallamount of macronutrient (a preload) 30–60 min before a meal with the rationale oftriggering neurohormonal feedback viastimulation of GLP-1 and GIP, as well asPYY and CCK from the small intestine, toslow gastric emptying, stimulate insulin,and suppress glucagon in advance of themain meal and potentially to reduce sub-sequent energy intake (57). Fat is a potentinhibitor of gastric emptying because ofits high-caloric density, but while acuteadministration of a fat preload predictablyslows gastric emptying markedly, it re-sults in only a modest reduction in peakpostprandial glucose in type 2 diabeticpatients (58). On the other hand, a 55-gwhey protein preload, when given acutelyto type 2 diabetic patients, slows gastricemptying, stimulates GIP and GLP-1, andmarkedly reduces postprandial glycemicexcursions (59) (Fig. 4). The latter effect islikely to be attributable in part to the stim-ulation of insulin secretion by absorbedamino acids. In view of these promisingobservations, studies to evaluate the opti-mum dose and composition of protein
preloads and to determine whether thebeneficial effects on glycemia are sus-tained with chronic use are indicated.
A potential disadvantage of all mac-ronutrient preloads is that they involveadditional energy consumption. Two re-cent studies evaluating the effects of pre-loads entailing minimal additional energyare, accordingly, of interest (60,61).Sucralose, a noncalorific artificial sweet-ener, stimulates GLP-1 in vitro, but appar-ently has no effect on incretin secretion inhealthy humans when administered as apreload (61,62). A nonmetabolized SGLT-1 substrate, 3-O-methylglucose, does stim-ulate GLP-1, slow gastric emptying, anddiminish the glycemic response to a subse-quent oral glucose load (60). Further eval-uation of the effects of preloads that entailminimal added energy intake is warranted.A recent study indicates that bile acids canstimulate endogenous GLP-1 in type 2diabetic patients when administereddirectly to the distal large intestine (63).
Pharmacological agents: GLP-1agonists, DPP-IV inhibitors, andpramlintideWhile the beneficial effect of GLP-1 ago-nists and DPP-IV inhibitors on glycemia intype 2 diabetes has been attributed toglucose-dependent insulinotropic and glu-cagonostatic properties, GLP-1 agonistsalso slow gastric emptying and that is, atleast in some cases, an important mecha-nism by which they lower postprandialglucose excursions. The GLP-1 receptoragonistsdexenatide, liraglutide, and exe-natide LAR (long-acting release)darenow widely available, while a number ofother drugs including lixisenatide, albiglu-tide, dulaglutide, and semaglutide are inlate-phase development. Because of vari-able half-lives, there are major differencesbetween these drugs in the frequency ofdosing and the resulting plasma drug lev-els. It is also recognized that they vary in themagnitude of their effects on pre- versuspostprandial glycemia (7), although differ-ences in effects on HbA1c hitherto appearsubtle (1). All of these drugs cause gastro-intestinal adverse effects such as anorexia,nausea, and diarrhea and are associatedwith modest weight loss. Most patients re-spond to GLP-1 agonists, but there is sub-stantial interindividual variation in theresponse, and certainly not all achieve thetarget HbA1c of ,7%. With some rare ex-ceptions, no clear factors have hithertobeen established to indicate which patientswill respond best to these drugs, exceptthat the reduction in HbA1c is predictably
1400 DIABETES CARE, VOLUME 36, MAY 2013 care.diabetesjournals.org
Gastric emptying and diabetes

greater when baseline HbA1c is higher. Therelative effect of these drugs on gastric emp-tying as a determinant of their effect on gly-cemia has inappropriately received littleattention.
It is now clear that all GLP-1 agonistshave the capacity to slow gastric emptyingin a variable but often marked mannerwhen administered acutely, althoughemptying has often been quantified bythe suboptimal paracetamol absorptiontest. The effects on gastric emptying havebeenmost comprehensively examined forexenatide given twice daily, which slowsemptying in a dose-dependent manner intype 2 diabetic patients apparently irre-spective of the presence of cardiovascularautonomic neuropathy (64,65). Indeed,the slowing of emptying appears to bethe predominant mechanism by whichexenatide reduces postprandial glycemia(64) (Fig. 5), and the magnitude of thiseffect is dependent on the baseline rate ofemptying (64) as is the case with exoge-nous GLP-1 (47). Hence, like GLP-1,GLP-1 agonists would be anticipated tohave minimal, if any, effect on gastricemptying in gastroparesis. Moreover, thereduction in postprandial glycemia andthe impact on postprandial insulin in-duced by GLP-1 agonists are also relatedto the degree to which emptying isslowed, at least in the case of exenatidetwice daily and lixisenatide, i.e., whenthe slowing of gastric emptying is sub-stantial, improvement in postprandialglycemia is most marked, while postpran-dial insulin secretion is diminished ratherthan stimulated (64,66).
The different durations of action ofGLP-1 agonists appear to determine theirimpact on gastric emptying with repeateddosing. Evidence from animal and humanstudies indicates that the slowing of gas-tric emptying induced by a long-actingformulation of exenatide (exenatide LAR)(67) and liraglutide (68) and presumablyother long-acting GLP-1 agonistsdbutnot exenatide twice daily or lixisenatide(which are short-acting)ddiminisheswith time, presumably reflecting the ta-chyphylaxis phenomenon reported withGLP-1 by Nauck et al. (51). For example,in mice, the initial marked slowing of par-acetamol absorption induced by acute ad-ministration of liraglutide diminisheswithin 2 weeks of continuous dosing,whereas the initially comparable markedslowing of paracetamol absorption in-duced by exenatide is sustained (68).In a human study comparing exenatidetwicedailywith exenatideLAR (administered
once a week), the latter did not slow para-cetamol absorption significantly at 14weeks, while exenatide twice daily did(67). This is not to suggest that long-actingGLP-1 agonists such as liraglutide do nothave any sustained effect to slow gastricemptying, but rather that the magnitudeof this effect diminishes with time. In type2 diabetic patients, liraglutide slowedparacetamol absorption slightly after ad-ministration for 3 weeks (69) despite sig-nificant glucose lowering, which would
favor more rapid gastric emptying (32).Moreover, the reduction in paracetamolabsorption was related to the magnitudeof the decrease in postprandial glycemia,which is consistent with the concept thateven modest slowing of gastric emptyingcan affect postprandial glycemic excur-sions. As a short-acting GLP-1 agonist,lixisenatide appears likely to have a sus-tained, major effect to slow gastric emp-tying (66), so that after 4 weeks’administration it lowers postprandial
Figure 4dData are mean 6 SEM. Gastric emptying (A) and blood glucose (B), plasma insulin(C), plasma GLP-1 (D), plasma GIP (E), and plasma CCK (F) concentrations in response toa mashed potato meal in eight type 2 diabetic patients. On each study day, subjects ingested 350mL beef-flavored soup 30 min before a radiolabeled mashed potato meal; 55 g whey protein wasadded either to the soup (whey preload), to the potato (whey in meal), or no whey was given (nowhey). *P , 0.05, whey preload vs. whey in meal; #P , 0.05, whey in meal vs. no whey; xP ,0.05, whey preload vs. no whey. Reprinted with permission from Ma et al. (59).
care.diabetesjournals.org DIABETES CARE, VOLUME 36, MAY 2013 1401
Marathe and Associates

glucose much more than liraglutide andsuppresses rather than stimulates post-prandial insulin (70). Hence, it appearsthat in the longer term, the short-actingGLP-1 agonists may act predominantlyby lowering postprandial glycemia(through a sustained, substantial inhibi-tion of gastric emptying), while the long-acting GLP-1 agonists predominantlylower preprandial hyperglycemia throughinsulinotropic and glucagonostatic ef-fects. Accordingly, in the future the choiceof GLP-1 agonists may be dictated bywhether the dominant target is pre- orpostprandial glycemic control and bythe baseline rate of gastric emptying.A short-acting drug would intuitively bemost effective at lowering postprandial gly-cemia in those with normal or rapid emp-tying and relatively lower HbA1c, whilethose with already delayed emptying areless likely to require a focus onpostprandialglucose given that when duodenal carbo-hydrate delivery is #1 kcal/min, there ap-pears to be little rise in blood glucose(10,11). These hypotheses now warrantformal evaluation.
There is increasing interest incombining a GLP-1 agonist with exoge-nous basal insulin in type 2 diabetes (71)based on the rationale that the latter pri-marily targets preprandial glucose but isassociated with weight gain and an in-creased risk of hypoglycemia (1) and theaddition of a GLP-1 agonist that targetspostprandial blood glucose by slowinggastric emptying while inducing weightloss and without increasing the risk of
hypoglycemia would, therefore, providea complementary strategy to optimizeglycemic control. There is now clear evi-dence to support this strategy. For exam-ple, in a recent study by Buse et al. (71),exenatide twice daily improved glycemiccontrol (reduction in HbA1c of 0.7%) intype 2 diabetic patients managed with in-sulin glargine, associated with modestweight loss, and without an increased hy-poglycemia. While there is hitherto noevidence of an increased risk of hypogly-cemia with the addition of a GLP-1 ago-nist to basal insulin, this issue should beviewed circumspectly. While the majorityof these patients will have an intact gluca-gon response to hypoglycemia, it wouldalso be relevant to know whether hypo-glycemia overrides the deceleration ofgastric emptying induced by a GLP-1agonist.
The DPP-IV enzyme acts on bothGLP-1 and GIP, and DPP-IV inhibitorscan be given orally, unlike GLP-1 ago-nists. An important distinction fromGLP-1 agonists is that DPP-IV inhibitorshave minimal, if any, effect on gastricemptying. For example, 2 days’ dosingwith 100mg sitagliptin failed to affect gas-tric emptying (72). Vella et al. (73) simi-larly found no change in gastric emptyingfollowing 10 days’ administration of vil-dagliptin (50 mg) in type 2 diabetic pa-tients. In contrast, Woerle et al. (74)reported a modest slowing of gastric emp-tying following a single dose of vildaglip-tin (100 mg) in patients with type 2diabetes, raising the possibility that
tachyphylaxis may have been responsiblefor the negative outcome of repeated dos-ing. In healthy subjects, the magnitude ofthe initial rise in glucose after a carbohy-drate meal is related to the rate of gastricemptying on sitagliptin, although sita-gliptin itself had no effect on emptying(72). This indicates that gastric emptyingis, as would be predicted, also an impor-tant determinant of postprandial glyce-mia in the presence of DPP-IV inhibition.The lack of effect of DPP-IV inhibitors ongastric emptying is likely to contribute totheir apparently lesser effect on postpran-dial glycemia than GLP-1 agonists in clin-ical trials.
Amylin, a pancreatic hormone cose-creted with insulin by the b-cell, slowsgastric emptying in addition to suppress-ing glucagon. The synthetic amylin ana-log, pramlintide, which is available in theU.S. for the management of diabetes, alsoslows gastric emptying, which no doubtcontributes to its beneficial effect on post-prandial glycemia (75).
ConclusionsdGastric emptying ex-hibits a substantial interindividual varia-tion in health, is frequently abnormallydelayed in patients with long-standing di-abetes, and is a major determinant of post-prandial glycemia and the secretion of theincretin hormones GIP and GLP-1. Therelation of glycemia and GLP-1 secretionwith small intestinal glucose delivery isnonlinear in health and type 2 diabetes.Macronutrients, particularly protein pre-loads, show promise in the management oftype 2 diabetes by stimulating incretin andinsulin secretion and slowing gastric emp-tying. Acute, exogenous GLP-1 slows gas-tric emptying and thereby carbohydrateabsorption, but theremay be tachyphylaxisto this effect. GLP-1 agonists also slowgastric emptying and, when administeredacutely, this may represent their dominantmechanism of glucose lowering.With bothexogenous GLP-1 and GLP-1 agonists, themagnitude of slowing of gastric emptyingand the consequent reduction in postpran-dial glucose are greater when baselinegastric emptying is relatively more rapid.The slowing of gastric emptying inducedby long-acting GLP-1 agonists, such asexenatide LAR and liraglutide, appears todiminish with time in contrast to short-acting agonists, such as exenatide twicedaily and lixisenatide. Hence, in an indi-vidual type 2 diabetic patient, the impactof a GLP-1 agonist on postprandial glyce-mia is likely to be dependent on both thebaseline rate of emptying and the choice of
Figure 5dRelationship between the effect of exenatide subcutaneously twice a day for 5 days onpostprandial glycemia (plasma glucose area under the curve (AUC) [0–3 h]) and gastric emp-tying (50% emptying [t50]) of a radiolabeled solid meal in type 2 diabetic patients (n = 17).Placebo, white circles; 5 mg exenatide, black triangles; and 10 mg exenatide, black squares.R =20.49, P, 0.0001. A longer t50 is indicative of slower gastric emptying. Reprinted withpermission from Linnebjerg et al. (64).
1402 DIABETES CARE, VOLUME 36, MAY 2013 care.diabetesjournals.org
Gastric emptying and diabetes

GLP-1 agonist. If postprandial glycemia isto be targeted preferentially, short-actinganalogs are likely to be optimally combinedwith basal insulin.
AcknowledgmentsdM.H. has participatedin the advisory boards and/or symposia forNovo Nordisk, Sanofi, Novartis, Eli Lilly,Merck Sharp & Dohme, Boehringer In-gelheim, and AstraZeneca and has receivedhonoraria for this activity. No other potentialconflicts of interest relevant to this article werereported.C.S.M., C.K.R., K.L.J., and M.H. all con-
tributed to discussions relating to content ofthe manuscript and were involved in writingthe manuscript.
References1. Inzucchi SE, Bergenstal RM, Buse JB, et al.;
American Diabetes Association (ADA);European Association for the Study ofDiabetes (EASD). Management of hyper-glycemia in type 2 diabetes: a patient-centered approach: position statement ofthe American Diabetes Association (ADA)and the European Association for theStudy of Diabetes (EASD). Diabetes Care2012;35:1364–1379
2. Monnier L, Lapinski H, Colette C. Con-tributions of fasting and postprandialplasma glucose increments to the overalldiurnal hyperglycemia of type 2 diabeticpatients: variations with increasing levelsof HbA(1c). Diabetes Care 2003;26:881–885
3. Riddle M, Umpierrez G, DiGenio A, ZhouR, Rosenstock J. Contributions of basal andpostprandial hyperglycemia over a widerange of A1C levels before and after treat-ment intensification in type 2 diabetes. Di-abetes Care 2011;34:2508–2514
4. Horowitz M, Dent J. Disordered gastricemptying: mechanical basis, assessmentand treatment. Baillieres Clin Gastro-enterol 1991;5:371–407
5. Standl E, Schnell O, Ceriello A. Post-prandial hyperglycemia and glycemicvariability: should we care? Diabetes Care2011;34(Suppl. 2):S120–S127
6. Chang J, Rayner CK, Jones KL, HorowitzM. Diabetic gastroparesis and its impacton glycemia. Endocrinol Metab ClinNorth Am 2010;39:745–762
7. Drucker DJ, Nauck MA. The incretinsystem: glucagon-like peptide-1 receptoragonists and dipeptidyl peptidase-4 in-hibitors in type 2 diabetes. Lancet 2006;368:1696–1705
8. Baggio LL, Drucker DJ. Biology of in-cretins: GLP-1 and GIP. Gastroenterology2007;132:2131–2157
9. O’Donovan DG, Doran S, Feinle-Bisset C,et al. Effect of variations in small intestinalglucose delivery on plasma glucose,
insulin, and incretin hormones in healthysubjects and type 2 diabetes. J Clin En-docrinol Metab 2004;89:3431–3435
10. Pilichiewicz AN, Chaikomin R, BrennanIM, et al. Load-dependent effects of duo-denal glucose on glycemia, gastrointestinalhormones, antropyloroduodenal motility,and energy intake in healthy men. Am JPhysiol Endocrinol Metab 2007;293:E743–E753
11. Ma J, Pilichiewicz AN, Feinle-Bisset C,et al. Effects of variations in duodenalglucose load on glycaemic, insulin, andincretin responses in type 2 diabetes. Di-abet Med 2012;29:604–608
12. Gonlachanvit S, Hsu CW, Boden GH,et al. Effect of altering gastric emptying onpostprandial plasma glucose concen-trations following a physiologic meal intype-II diabetic patients. Dig Dis Sci 2003;48:488–497
13. Kashyap P, Farrugia G. Diabetic gastro-paresis: what we have learned and had tounlearn in the past 5 years. Gut 2010;59:1716–1726
14. Kassander P. Asymptomatic gastric re-tention in diabetics (gastroparesis dia-beticorum). Ann Intern Med 1958;48:797–812
15. Jung HK, Choung RS, Locke GR, 3rd,et al. The incidence, prevalence, andoutcomes of patients with gastroparesis inOlmsted County, Minnesota, from 1996to 2006. Gastroenterology 2009;136:1225–1233
16. Bharucha AE, Camilleri M, Forstrom LA,Zinsmeister AR. Relationship betweenclinical features and gastric emptyingdisturbances in diabetes mellitus. ClinEndocrinol (Oxf) 2009;70:415–420
17. Horowitz M, Maddox AF, Wishart JM,Harding PE, Chatterton BE, Shearman DJ.Relationships between oesophageal tran-sit and solid and liquid gastric emptying indiabetes mellitus. Eur J Nucl Med 1991;18:229–234
18. Jones KL, Russo A, Stevens JE, WishartJM, Berry MK, Horowitz M. Predictorsof delayed gastric emptying in diabetes.Diabetes Care 2001;24:1264–1269
19. Wang YR, Fisher RS, Parkman HP.Gastroparesis-related hospitalizations inthe United States: trends, characteristics,and outcomes, 1995-2004. Am J Gastro-enterol 2008;103:313–322
20. Grover M, Farrugia G, Lurken MS, et al.Cellular changes in diabetic and idio-pathic gastroparesis. Gastroenterology2011;140:1575–1585.e8
21. Kong MF, Horowitz M, Jones KL, WishartJM, Harding PE. Natural history of di-abetic gastroparesis. Diabetes Care 1999;22:503–507
22. Chang J, Russo A, Bound M, Rayner CK,Jones KL, Horowitz M. A 25-year longi-tudinal evaluation of gastric emptying indiabetes. Diabetes Care 2012;35:2594–2596
23. Horowitz M, Edelbroek MA, Wishart JM,Straathof JW. Relationship between oralglucose tolerance and gastric emptying innormal healthy subjects. Diabetologia1993;36:857–862
24. Jones KL, HorowitzM, Carney BI,WishartJM, Guha S, Green L. Gastric emptyingin early noninsulin-dependent diabetesmellitus. J Nucl Med 1996;37:1643–1648
25. Ishii M, Nakamura T, Kasai F, Onuma T,Baba T, Takebe K. Altered postprandialinsulin requirement in IDDM patientswith gastroparesis. Diabetes Care 1994;17:901–903
26. Kuo P, Stevens JE, Russo A, et al. Gastricemptying, incretin hormone secretion, andpostprandial glycemia in cystic fibrosisdeffects of pancreatic enzyme supplementa-tion. J Clin Endocrinol Metab 2011;96:E851–E855
27. Trahair LG, Horowitz M, Rayner CK, et al.Comparative effects of variations in duo-denal glucose load on glycemic, insulinemic,and incretin responses in healthy youngand older subjects. J Clin Endocrinol Metab2012;97:844–851
28. Chaikomin R, Doran S, Jones KL, et al.Initially more rapid small intestinal glu-cose delivery increases plasma insulin,GIP, and GLP-1 but does not improveoverall glycemia in healthy subjects. AmJ Physiol Endocrinol Metab 2005;289:E504–E507
29. Marathe CS, Rayner CK, Jones KL,Horowitz M. The size of incretin effect isdependent upon the small intestinal glu-cose load [Abstract]. Diabetes 2012;61(Suppl. 1):A94
30. Näslund E, Grybäck P, Hellström PM,et al. Gastrointestinal hormones andgastric emptying 20 years after jejunoi-leal bypass for massive obesity. Int JObes Relat Metab Disord 1997;21:387–392
31. Horowitz M, Cook DJ, Collins PJ, et al.Measurement of gastric emptying aftergastric bypass surgery using radio-nuclides. Br J Surg 1982;69:655–657
32. Rayner CK, Samsom M, Jones KL,Horowitz M. Relationships of upper gas-trointestinal motor and sensory functionwith glycemic control. Diabetes Care2001;24:371–381
33. Russo A, Stevens JE, Chen R, et al.Insulin-induced hypoglycemia acceler-ates gastric emptying of solids andliquids in long-standing type 1 diabetes.J Clin Endocrinol Metab 2005;90:4489–4495
34. Jones KL, Berry M, Kong M-F, KwiatekMA, Samsom M, Horowitz M. Hypergly-cemia attenuates the gastrokinetic effectof erythromycin and affects the percep-tion of postprandial hunger in normalsubjects. Diabetes Care 1999;22:339–344
35. Kuo P, Gentilcore D, Nair N, et al.The nitric oxide synthase inhibitor,
care.diabetesjournals.org DIABETES CARE, VOLUME 36, MAY 2013 1403
Marathe and Associates

Ng-nitro-L-arginine-methyl-ester, attenu-ates the delay in gastric emptying inducedby hyperglycaemia in healthy humans.Neurogastroenterol Motil 2009;21:1175,e103
36. Deane AM, Nguyen NQ, Stevens JE, et al.Endogenous glucagon-like peptide-1 slowsgastric emptying in healthy subjects, atten-uating postprandial glycemia. J Clin Endo-crinol Metab 2010;95:215–221
37. Witte AB, Grybäck P, Jacobsson H, et al.Involvement of endogenous glucagon-likepeptide-1 in regulation of gastric motilityand pancreatic endocrine secretion. ScandJ Gastroenterol 2011;46:428–435
38. Schirra J, Nicolaus M, Roggel R, et al. En-dogenous glucagon-like peptide 1 controlsendocrine pancreatic secretion and antro-pyloro-duodenal motility in humans. Gut2006;55:243–251
39. Salehi M, Vahl TP, D’Alessio DA. Regula-tion of islet hormone release and gastricemptying by endogenous glucagon-likepeptide 1 after glucose ingestion. J ClinEndocrinol Metab 2008;93:4909–4916
40. NauckMA,NiedereichholzU, Ettler R, et al.Glucagon-like peptide 1 inhibition of gas-tric emptying outweighs its insulinotropiceffects in healthy humans. Am J Physiol1997;273:E981–E988
41. Meier JJ, Gallwitz B, Salmen S, et al.Normalization of glucose concentrationsand deceleration of gastric emptying aftersolid meals during intravenous glucagon-like peptide 1 in patients with type 2 di-abetes. J Clin Endocrinol Metab 2003;88:2719–2725
42. Little TJ, Pilichiewicz AN, Russo A, et al.Effects of intravenous glucagon-likepeptide-1 on gastric emptying and in-tragastric distribution in healthy sub-jects: relationships with postprandialglycemic and insulinemic responses. JClin Endocrinol Metab 2006;91:1916–1923
43. Schirra J, Houck P, Wank U, Arnold R,Göke B, Katschinski M. Effects of glucagon-like peptide-1(7-36)amide on antro-pyloro-duodenal motility in the interdigestive stateand with duodenal lipid perfusion in hu-mans. Gut 2000;46:622–631
44. Wettergren A, Wøjdemann M, Holst JJ.Glucagon-like peptide-1 inhibits gastro-pancreatic function by inhibiting centralparasympathetic outflow. Am J Physiol1998;275:G984–G992
45. Meier JJ, Goetze O, Anstipp J, et al. Gas-tric inhibitory polypeptide does not in-hibit gastric emptying in humans. Am JPhysiol Endocrinol Metab 2004;286:E621–E625
46. Edholm T, Degerblad M, Gryback P,Hilsted L, Holst JJ, Jacobsson H, et al.Differential incretin effects of GIP andGLP-1 on gastric emptying, appetite,and insulin-glucose homeostasis. Neuro-gastroenterol Motil. 2010;22:1191–1200,e315
47. Deane AM, Chapman MJ, Fraser RJ, et al.Effects of exogenous glucagon-like peptide-1 on gastric emptying and glucose ab-sorption in the critically ill: relationshipto glycemia. Crit Care Med 2010;38:1261–1269
48. Meier JJ, KemmeriesG,Holst JJ,NauckMA.Erythromycin antagonizes the decelerationof gastric emptying by glucagon-like pep-tide 1 and unmasks its insulinotropic effectin healthy subjects. Diabetes 2005;54:2212–2218
49. Horowitz M, Nauck MA. To be or not tobedan incretin or enterogastrone? Gut2006;55:148–150
50. Delgado-Aros S, Vella A, Camilleri M,et al. Effects of glucagon-like peptide-1and feeding on gastric volumes in diabetesmellitus with cardio-vagal dysfunction.Neurogastroenterol Motil 2003;15:435–443
51. Nauck MA, Kemmeries G, Holst JJ, MeierJJ. Rapid tachyphylaxis of the glucagon-like peptide 1-induced deceleration ofgastric emptying in humans. Diabetes2011;60:1561–1565
52. Horowitz M, Jones KL, Rayner CK, ReadNW. ‘Gastric’ hypoglycaemiadan impor-tant concept in diabetes management.Neurogastroenterol Motil 2006;18:405–407
53. Chandalia M, Garg A, Lutjohann D, vonBergmann K, Grundy SM, Brinkley LJ.Beneficial effects of high dietary fiber in-take in patients with type 2 diabetesmellitus. N Engl J Med 2000;342:1392–1398
54. Russo A, Stevens JE, Wilson T, Wells F,Tonkin A, Horowitz M, Jones KL. Guargum attenuates fall in postprandial bloodpressure and slows gastric emptying oforal glucose in type 2 diabetes. Dig Dis Sci2003;48:1221–1229
55. Cunningham KM, Read NW. The effectof incorporating fat into different com-ponents of a meal on gastric emptyingand postprandial blood glucose andinsulin responses. Br J Nutr 1989;61:285–290
56. Gannon MC, Nuttall FQ, Saeed A, JordanK, Hoover H. An increase in dietary pro-tein improves the blood glucose responsein persons with type 2 diabetes. Am J ClinNutr 2003;78:734–741
57. Wu T, Rayner CK, Jones K, Horowitz M.Dietary effects on incretin hormonesecretion. Vitam Horm 2010;84:81–110
58. Gentilcore D, Chaikomin R, Jones KL,et al. Effects of fat on gastric emptying ofand the glycemic, insulin, and incretinresponses to a carbohydrate meal in type 2diabetes. J Clin Endocrinol Metab 2006;91:2062–2067
59. Ma J, Stevens JE, Cukier K, et al. Effectsof a protein preload on gastric emptying,glycemia, and gut hormones after a car-bohydrate meal in diet-controlled type 2
diabetes. Diabetes Care 2009;32:1600–1602
60. Wu T, Zhao BR, BoundMJ, et al. Effects ofdifferent sweet preloads on incretin hor-mone secretion, gastric emptying, andpostprandial glycemia in healthy humans.Am J Clin Nutr 2012;95:78–83
61. Ma J, Chang J, Checklin HL, et al. Effectof the artificial sweetener, sucralose, onsmall intestinal glucose absorption inhealthy human subjects. Br J Nutr 2010;104:803–806
62. Ma J, Bellon M, Wishart JM, et al. Effect ofthe artificial sweetener, sucralose, ongastric emptying and incretin hormonerelease in healthy subjects. Am J PhysiolGastrointest Liver Physiol 2009;296:G735–G739
63. Adrian TE, Gariballa S, Parekh KA, et al.Rectal taurocholate increases L cell andinsulin secretion, and decreases bloodglucose and food intake in obese type 2diabetic volunteers. Diabetologia 2012;55:2343–2347
64. Linnebjerg H, Park S, Kothare PA, et al.Effect of exenatide on gastric emptyingand relationship to postprandial glyce-mia in type 2 diabetes. Regul Pept 2008;151:123–129
65. Kolterman OG, Buse JB, FinemanMS, et al.Synthetic exendin-4 (exenatide) signifi-cantly reduces postprandial and fastingplasma glucose in subjects with type 2 di-abetes. J Clin Endocrinol Metab 2003;88:3082–3089
66. Lorenz M, Pfeiffer C, Steinstraber A, RuusP. Effects of lixisenatide once daily ongastric emptying and relationships topostprandial glycemia in type 2 diabetesmellitus [Abstract]. Diabetes 2012;61(Suppl. 1):A280
67. Drucker DJ, Buse JB, Taylor K, et al.;DURATION-1 Study Group. Exenatideonce weekly versus twice daily for thetreatment of type 2 diabetes: a rando-mised, open-label, non-inferiority study.Lancet 2008;372:1240–1250
68. Jelsing J, Vrang N, Hansen G, Raun K,Tang-Christensen M, Knudsen LB. Lir-aglutide: short-lived effect on gastric emp-tyingdlong lasting effects on body weight.Diabetes Obes Metab 2012;14:531–538
69. Flint A, Kapitza C, Hindsberger C,Zdravkovic M. The once-daily humanglucagon-like peptide-1 (GLP-1) analogliraglutide improves postprandial glucoselevels in type 2 diabetes patients. Adv Ther2011;28:213–226
70. Kapitza C, Coester H, Poitiers F, HeumannG, Ruus P, Hincelin-Mery A. Pharmacody-namic characteristics of lixisenatide QDvs liraglutide QD in patients with T2DMinadequately controlled with metformin[Abstract]. World Diabetes Congress 2011;D-0740
71. Buse JB, Bergenstal RM, Glass LC,et al. Use of twice-daily exenatide in basalinsulin-treated patients with type 2
1404 DIABETES CARE, VOLUME 36, MAY 2013 care.diabetesjournals.org
Gastric emptying and diabetes

diabetes: a randomized, controlled trial.Ann Intern Med 2011;154:103–112
72. Stevens JE, Horowitz M, Deacon CF,Nauck M, Rayner CK, Jones KL. The ef-fects of sitagliptin on gastric emptying inhealthy humansda randomised, con-trolled study. Aliment Pharmacol Ther2012;36:379–390
73. Vella A, BockG, Giesler PD, et al. Effects ofdipeptidyl peptidase-4 inhibition on gas-trointestinal function, meal appearance,and glucose metabolism in type 2 di-abetes. Diabetes 2007;56:1475–1480
74. Woerle HJ, Lindenberger T, Linke R, et al.A single dose of vildagliptin (VILDA) de-celerates gastric emptying in patients with
type 2 diabetes (T2DM) [Abstract]. Di-abetes 2007:56(Suppl. 1):A133
75. SamsomM, Szarka LA, CamilleriM, Vella A,Zinsmeister AR, Rizza RA. Pramlintide, anamylin analog, selectively delays gastricemptying: potential role of vagal inhibition.Am J Physiol Gastrointest Liver Physiol2000;278:G946–G951
care.diabetesjournals.org DIABETES CARE, VOLUME 36, MAY 2013 1405
Marathe and Associates