relation between cardiac hypertrophy and forearm vascular structural changes before and during...
TRANSCRIPT

Relation between Cardiac Hypertrophy and Forearm Vascular Structural Changes before and during Long-Term Antihypertensive Treatment
ENRICO AGABITI-ROSEI, M.D. MARIA LORENZA MUIESAN, M.D. ALESSANDRO GERI, M.D. GIUSEPPE ROMANELLI, M.D. GIOVANNI MONTANI, M.D. GIULIO MUIESAN, M.D.
Brescia, k/y
In patients with hypertension, structural changes develop in the heart and in the systemic arteries that have a significant role in the maintenance and gradual worsening of the hypertensive disease. Blood pressure, basal and post-ischemic “maximal” forearm blood flow (strain-gauge venous occlusive plethysmography), and echo- cardiographic left ventricular mass index were measured in 28 hy- pertensive patients (WHO class I or II, 23 men and five women, aged 26 to 59 years). Minimal vascular resistance (mean arterial pressure/ peak blood flow) was taken as an index of vascular structural changes. The same measurements were made in a group of 14 pa- tients before and after long-term antihypertensive treatment: in eight patients after six and 12 months of treatment with captopril (50 mg twice a day, plus 25 mg of hydrochlorothiazide per day if necessary) and in six patients after six months of treatment with nitrendipine (20 mg per day, plus 50 mg of atenolol per day if neces- sary). A significant but weak direct correlation was found between the degree of left ventricular hypertrophy and mean arterial pres- sure (r = 0.41) or minimal vascular resistance (r = 0.31). Thus, pa- tients were categorized according to whether they had left ventricu- lar hypertrophy or impaired blood flow; the results suggested that left ventricular hypertrophy may be detected earlier than increased minimal vascular resistance. After six months of treatment, both captopril and nitrendipine significantly reduced left ventricular mass index and minimal vascular resistance. Left ventricular mass index was normalized in 50 percent of the patients, whereas minimal vascular resistance was normalized in one patient only. After 12 months of treatment, left ventricular mass index was normalized in all patients; minimal vascular resistance was on the average further reduced but normalized in only one additional patient. Thus, regres- sion of cardiovascular structure also seems to occur earlier in the heart.
From the Clinica Medica Generale e Terapia Med- ica, University of Brescia, Brescia, Italy. Requests for reprints should be addressed to Dr. Enrico Agabiti-Rosei, Clinica Medica, University of Bre- scia, c/o 1 Divisione Medicina Generale, Spedali Civili, 25100 Brescia, Italy.
It has been demonstrated that the development of structural changes in the heart as well as in the systemic arteries and arterioles significantly contributes to the maintenance and progressive worsening of arterial hypertension [1,2]. The assessment of cardiovascular structural changes in human beings may be reliably obtained with the use of noninvasive techniques, such as echocardiography and venous occlusion plethys- mography. In fact, echocardiography permits the direct evaluation of left ventricular wall thickness, dimension, and mass [3]. In contrast, evalua- tion of structural vascular changes is performed indirectly, by determina- tion of minimal vascular resistance from measurements of arterial pres-
March 11, 1988 The American Journal of Medicine Volume 84 (suppl 3A) 125

SYMPOSIUM ON THE RENIN-ANGIOTENSIN SYSTEM-AGABITI-ROSEI ET AL
sure and maximal blood flow [4,5]. In previous studies, we suggested that left ventricular hypertrophic changes seem to precede arterial structural changes in the calves [6]. The purpose of the described herein study was to extend these observations to the forearm circulation, and also to evaluate the effects of long-term antihypertensive treat- ment.
PATIENTS AND METHODS
In 28 untreated patients (23 men and five women) aged 26 to 59 years (mean, 43) with essential hypertension at stage I or II of the WHO classification, simultaneous assessment of left ventricular mass and forearm vascular structural changes was performed. Secondary causes of hypertension were ex- cluded by the usual clinical and laboratory investigations. The patients were hospitalized and received a diet with a fixed normal sodium and potassium content. For the assessment of structural changes in the vasculature and in the heart, ve- nous occlusion plethysmography and echocardiography were used. Blood flow was measured in the forearm, using an electrocardiographically triggered strain-gauge plethysmo- graph (Periflow, Janssen Instruments; Beerse, Belgium). Structural vascular changes in the limb arteries were evalu- ated indirectly on the basis of the minimal vascular resistance (normal, less than 2.5 units) calculated from maximal blood flow and mean arterial pressure. Maximal blood flow was measured during peak reactive hyperemia after six to seven minutes of arterial occlusion and muscle work, until exhaus- tion [5]. Arterial blood pressure was measured by the auscul- tatory method (Korotkoff phase V for diastolic arterial pres- sure); mean arterial pressure was calculated by adding one third of the pulse pressure to the diastolic pressure. Left ven- tricular mass index (normal, less than 120 g/m’) was meas- ured from M-mode echocardiographic tracings obtained with two-dimensional image control, using an SKI-5000, ATL MK- 300, or HP-77020A instrument; calculations were made ac- cording to the “Penn convention” [3].
In a group of 14 patients (12 men and two women) aged 26 to 59 years (mean, 46), the effect of antihypertensive medical treatment on cardiovascular structural changes was evalu- ated. Eight patients were given 100 mg of captopril per day (plus 25 mg of hydrochlorothiazide per day in five), and six patients were given 20 mg of nitrendipine per day (plus 50 mg of atenolol in four); simultaneous measurements of arterial pressure, left ventricular mass, and forearm flow and resist- ance were obtained before treatment and after six months of treatment in all 14 patients and after 12 months of treatment in seven patients. Statistical evaluation included simple linear regression analysis and the Student t test for paired and un- paired observations.
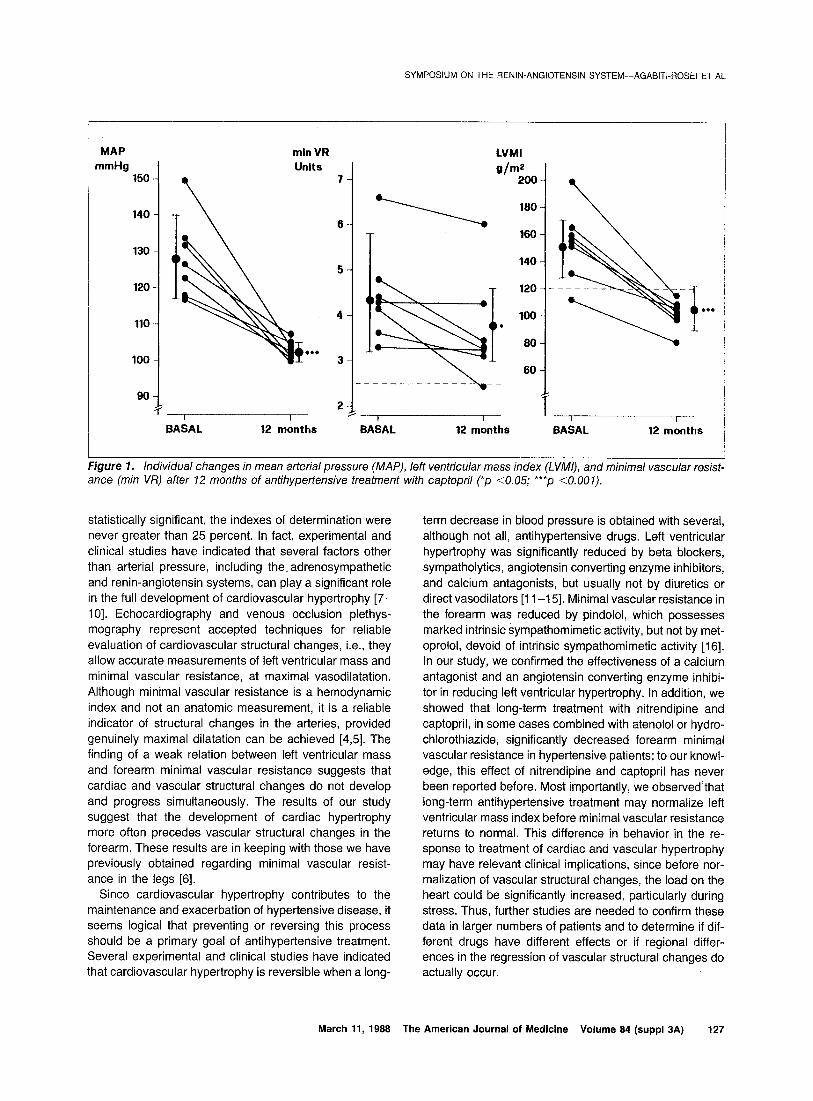
was directly related to minimal vascular resistance (r = 0.37). For further investigation of the relation between car- diac and arterial structural changes, the patients were subdivided according to the values of left ventricular mass index and values of minimal vascular resistance. In the group with minimal vascular resistance in the normal range-hence, presumably without structural changes in the arteries of the forearm-left ventricular hypertrophy was found in IO of 16 patients, or 62 percent. In contrast, in the group of patients with minimal vascular resistance of more than 2.5 units-therefore, presumably with struc- tural changes in the forearm vasculature-absence of left ventricular hypertrophy was found only in three of 12 pa- tients, or 25 percent. Effect of Long-Term Medical Treatment on Left Ven- tricular Hypertrophy and Vascular Structural Changes. Captopril was given to eight patients for six months and to seven patients for 12 months. Nitrendipine was given to six patients for six months only. Arterial blood pressure was significantly reduced after six months (ni- trendipine, n = 6, from 124 2 9 to 104 + 6 mm Hg, p <O.OOl ; captopril, n = 8, from 127 i 11 to 107 ? 5 mm Hg, p <O.OOl); and after 12 months (captopril, n = 7, from 128 -C 12 to 103 2 3 mm Hg, p <O.OOl). On average, both left ventricular mass index and minimal vascular re- sistance were significantly reduced after six months (left ventricular mass index, from 141 t 41 to 111 r 24 g/m’, p <O.OOi ; minimal vascular resistance, from 4.7 * 1.3 to 4 ? 1.2 units, p ~0.02) and after 12 months (left ventricu- lar mass index, from 151 ? 26 to 104 -c 11 g/m’, p <O.OOl ; minimal vascular resistance from 4.4 1. 1 .l to 3.8 +- 1 .I units, p cO.03). Considered individually, 12 pa- tients had increased minimal vascular resistance in basal conditions, and in one of them (given nitrendipine), it was normal after six months; in another patient (given capto- pril), the minimal vascular resistance was normalized after 12 months of treatment. Ten patients (seven who received captopril and three who received nitrendipine) had left ventricular hypertrophy before treatment, and in five of them, the left ventricular mass index was normal after six months of antihypertensive therapy; the left ventricular mass index was normalized after 12 months in every one of the seven patients treated for one year. Individual changes in mean arterial pressure, left ventricular mass index, and minimal vascular resistance after 12 months of treatment with captopril are shown in Figure 1.
COMMENTS RESULTS
Relation between Left Ventricular Mass and Minimal Vascular Resistance in the Forearm. In this group of 28 untreated patients with essential hypertension, mean arterial pressure was significantly related to minimal vas- cular resistance in the forearm (r = 0.32) and to left ven- tricular mass index (r = 0.54). Left ventricular mass index
In this study, we observed that cardiovascular structural changes are detectable in a consistent proportion of unse- lected patients with mild to moderate essential hyperten- sion (WHO class I or II). In addition, both left ventricular hypertrophy and forearm vascular structural changes are proportional to the severity of hypertension. However, al- though the correlations among the several variables were
126 March 11, 1988 The American Journal of Medicine Volume 84 (suppl 3A)
SYMPOSIUM ON THE RENIN-ANGIOTENSIN SYSTEM-AGABITI-ROSEI ET AL
MAP mmHg
150
140
130
120
110
100
90
min VR Units
7
I BASAL
2 I
I2 months
LVMI
g/m2 200
\ 180
T 160
100 .
80
---- --- ----- -\--
I I
BASAL I2 months BAAAL I2 mbnths
Figure 1. Individual changes in mean arterial pressure (MAP), left ventricular mass index (LVMI), and minimal vascular resist- ance (min VR) after 12 months of antihypertensive treatment with captopril (*p CO.05; ***p <O.OOl).
statistically significant, the indexes of determination were never greater than 25 percent. In fact, experimental and clinical studies have indicated that several factors other than arterial pressure, including the. adrenosympathetic and renin-angiotensin systems, can play a significant role in the full development of cardiovascular hypertrophy [7- lo]. Echocardiography and venous occlusion plethys- mography represent accepted techniques for reliable evaluation of cardiovascular structural changes, i.e., they allow accurate measurements of left ventricular mass and minimal vascular resistance, at maximal vasodilatation. Although minimal vascular resistance is a hemodynamic index and not an anatomic measurement, it is a reliable indicator of structural changes in the arteries, provided genuinely maximal dilatation can be achieved [4,5]. The finding of a weak relation between left ventricular mass and forearm minimal vascular resistance suggests that cardiac and vascular structural changes do not develop and progress simultaneously. The results of our study suggest that the development of cardiac hypertrophy more often precedes vascular structural changes in the forearm. These results are in keeping with those we have previously obtained regarding minimal vascular resist- ance in the legs [6].
Since cardiovascular hypet-trophy contributes to the maintenance and exacerbation of hypertensive disease, it seems logical that preventing or reversing this process should be a primary goal of antihypertensive treatment. Several experimental and clinical studies have indicated that cardiovascular hypertrophy is reversible when a long-
March 11, 1988 The American Journal of Medicine Volume 84 (suppl 3A) 127
term decrease in blood pressure is obtained with several, although not all, antihypertensive drugs. Left ventricular hypertrophy was significantly reduced by beta blockers, sympatholytics, angiotensin converting enzyme inhibitors, and calcium antagonists, but usually not by diuretics or direct vasodilators [l l-l 51. Minimal vascular resistance in the forearm was reduced by pindolol, which possesses marked intrinsic sympathomimetic activity, but not by met- oprolol, devoid of intrinsic sympathomimetic activity [16]. In our study, we confirmed the effectiveness of a calcium antagonist and an angiotensin converting enzyme inhibi- tor in reducing left ventricular hypertrophy. In addition, we showed that long-term treatment with nitrendipine and captopril, in some cases combined with atenolol or hydro- chlorothiazide, significantly decreased forearm minimal vascular resistance in hypertensive patients; to our knowl- edge, this effect of nitrendipine and captopril has never been reported before. Most importantly, we observed’that long-term antihypertensive treatment may normalize left ventricular mass index before minimal vascular resistance returns to normal. This difference in behavior in the re- sponse to treatment of cardiac and vascular hypertrophy may have relevant clinical implications, since before nor- malization of vascular structural changes, the load on the heart could be significantly increased, particularly during stress. Thus, further studies are needed to confirm these data in larger numbers of patients and to determine if dif- ferent drugs have different effects or if regional differ- ences in the regression of vascular structural changes do actually occur.

SYMPOSIUM ON THE RENIN-ANGIOTENSIN SYSTEM-AGABITI-ROSEI ET AL
4.
5.
6.
7.
a.
9.
REFERENCES
Bohr DF: What makes the pressure go up? Hypertension 1961; 3 (suppl 2): 11-160-11-165.
Folkow B: Cardiovascular structural adaptation; its role in the initiation and maintenance of primary hypertension. Clin Sci Mol Med 1976; 55: 3s-22s.
Devereux RB, Reichek N: Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation 1977; 55: 613-616.
Sivertsson R: The hemodynamic importance of structural vas- cular changes in essential hypertension. Acta Physiol Stand [Suppl] 1970; 343: l-56.
Conway J: A vascular abnormality in hypertension. A study of blood flow in the forearm. Circulation 1963; 27: 520-529.
Geri A, Agabiti-Rosei E, Muiesan ML, Romanelli G, Platto L, Muiesan G: Interrelations of cardiac and arterial vascular wall hypertrophy in essential hypertension. J Hypertens 1965; 3: 335s-337s.
Frohlich ED, Tarazi RC: Is arterial pressure the sole factor re- sponsible for hypertensive cardiac hypertrophy? Am J Cardiol 1979; 44: 959-963.
Yamori Y, lgawa T, Tagami M, et al: Humoral trophic influence on cardiovascular structural changes in hypertension. Hyper- tension 1964; (suppl Ill): 27-32.
Tarazi RC, Sen S, Saragoca M, Khairallah PA: The multifactorial role of catecholamines in hypertensive cardiac hypertrophy.
Eur Heart J 1982; 3: 103-l lo. 10. Muiesan G, Agabiti-Rosei E, Muiesan ML: Adrenergic activity
and myocardial anatomy and function in essential hyperten- sion J Hypertens 1965; 3 (suppl 4): S45-S50.
11. Tarazi RC, Fouad FM: Reversal of cardiac hypertrophy in man. Hypertension 1964; 6 (suppl II): S140-S146.
12.. Rowlands DB, Glover DR, Stallard TJ, Littler WA: Control of blood pressure and reduction of echocardiographically as- sessed left ventricular mass with once-daily timolol. Br J Clin Pharmacol 1982; 14: 89-95.
13. Fouad FM, Nakashima Y, Tarazi RC, Salcedo EE: Reversal of left ventricular hypertrophy in hypertensive patients treated with methyldopa. Lack of association with blood pressure control. Am J Cardiol 1962; 49: 759-601.
14. Mujais SK, Fouad FM, Tarazi RC: Reversal of left ventricular hypertrophy with captopril: heterogeneity of response among hypertensive patients. Clin Cardiol 1963; 6: 595-602.
15. Muiesan G. Aaabiti-Rosei E. Romanelli G. Muiesan ML. Castel- lano M, Be&hi M: Adrenergic activity and left ventricular func- tion during treatment of essential hypertension with calcium antagonists. Am J Cardiol 1964; 53 (suppl D): 44D-49D.
16. Svensson A, Gudbrandsson T, Sivertsson R, Hansson L: Hemo- dynamic effects of metoprolol and pindolol: a comparison in hypertensive patients. Br J Clin Pharmacol 1962; 13 (suppl2): 2598-2678.
128 March 11, 1988 The American Journal of Medicine Volume 84 (suppl 3A)