reimbursement review: pama danielle scelfo, mhsa senior …€¦ · reimbursement review: pama...
TRANSCRIPT
Reimbursement Review: PAMA
Danielle Scelfo, MHSA
Senior Director, Health Policy andReimbursement
Agenda
• Session Objective:o Better current reimbursement methods used by CMS
o Understand PAMA and how the industry is responding
o Introduce tools on how to accomplish greater understanding and value to yourcustomers
• PAMA: The Protecting Access to Medicare Acto What is it?
o How will Medicare set rates in the future?
o Why do we care and what is the impact to the laboratories?
How Reimbursement is Established by CMS
Two Approaches:1. Crosswalk
2. Gapfill
Crosswalk• Approach used when one test is
believed to be similar to another,in resource, technology, etc
• The same rate is applied
• Very common
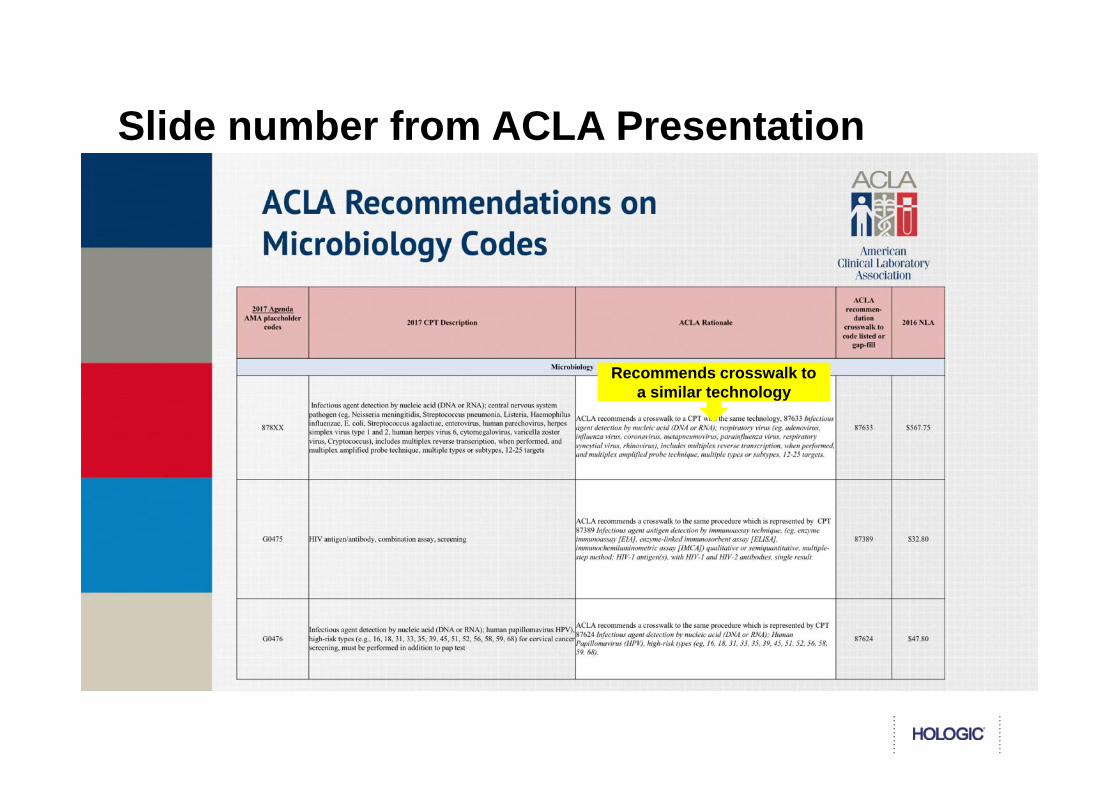
Slide number from ACLA Presentation
Recommends crosswalk toa similar technology
How Reimbursement is Established by CMS
Gapfill• Approach used when one test is believed to be
unique or dissimilar to another, in resource,technology, etc
• CMS instructs local Medicare contractors tosuggest a rate over a the next year
• Often used with new technology
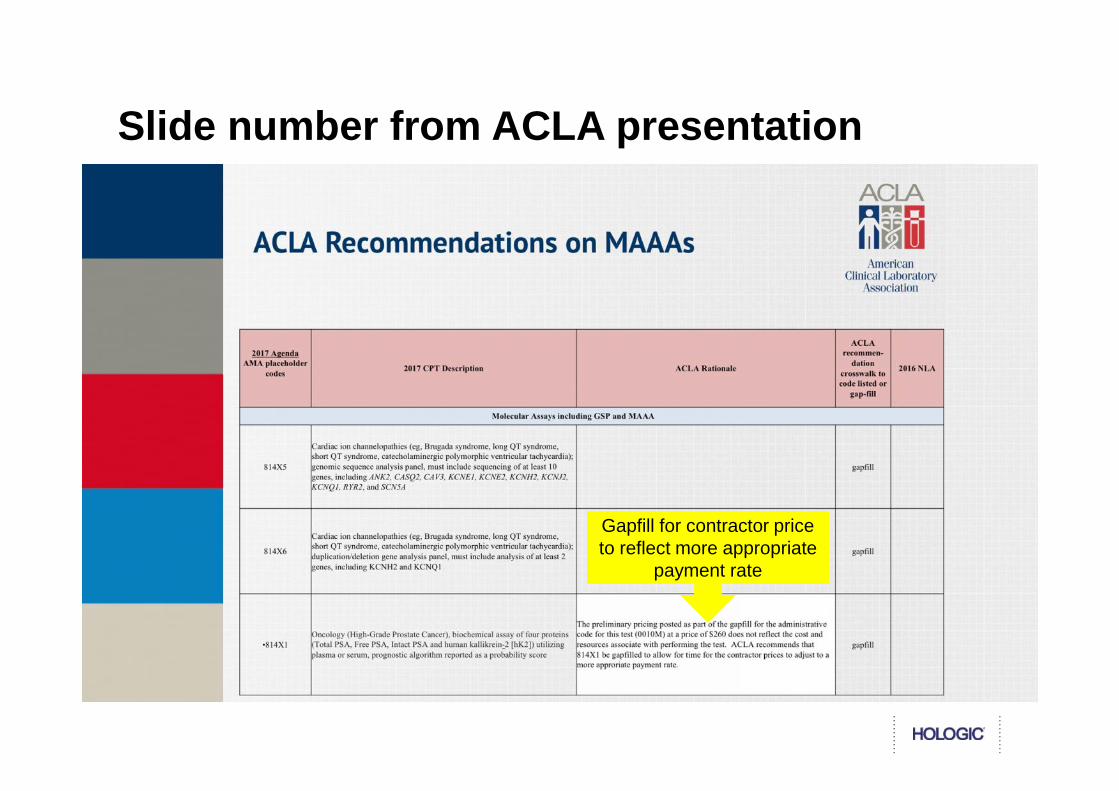
Slide number from ACLA presentation
Gapfill for contractor priceto reflect more appropriate
payment rate
PAMA Overview
PAMA reforms how Medicare pays forClinical Diagnostic Laboratory Tests(CDLTs)
• Became law April 1, 2014
• Most disruptive change to the payment system forlaboratory tests since inception of payment ratesin 1984
• Shifts Medicare payment for laboratory servicesaway from CMS administered pricing to market-based payments, reflecting private payor rates forlaboratory services
• In the CMS rule, payment reform excluded mosthospitals without unique NPI numbers fromreporting – impact of exclusion will carry theweight of the reduction.
PAMA In a nutshell:
CLFS Payment rates Starting January 1, 2018
Applicable labs report data(on applicable information)on Private Payor Rates
CMS calculates weightedmedian private payor ratefor each test
Below Average Above Average
Average/Median
# of
Req
uest
sResponse Time
Median determines new ratefor tests paid on MedicareCLFS
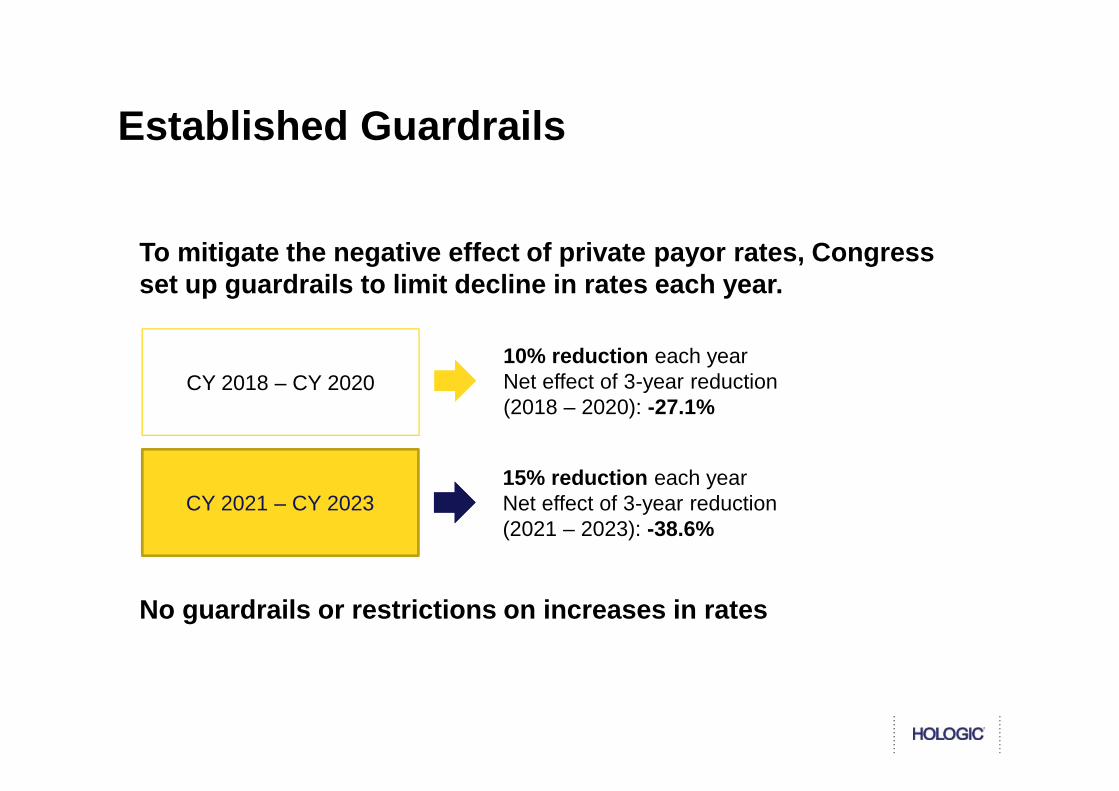
Established Guardrails
To mitigate the negative effect of private payor rates, Congressset up guardrails to limit decline in rates each year.
CY 2018 – CY 2020CY 2018 – CY 2020
CY 2021 – CY 2023
10% reduction each yearNet effect of 3-year reduction(2018 – 2020): -27.1%
15% reduction each yearNet effect of 3-year reduction(2021 – 2023): -38.6%
No guardrails or restrictions on increases in rates
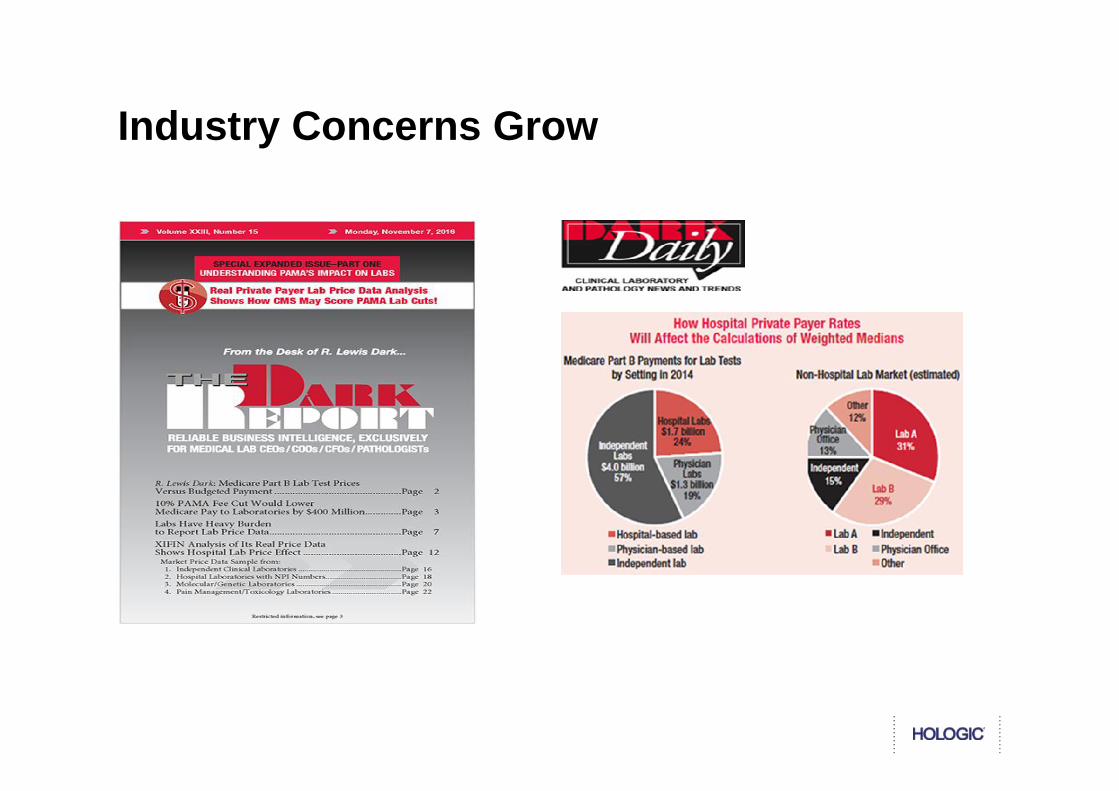
Industry Concerns Grow

Eric Zimmerman
Paul W. Radensky,M.D., J.D. John Warren
Efforts to Educate
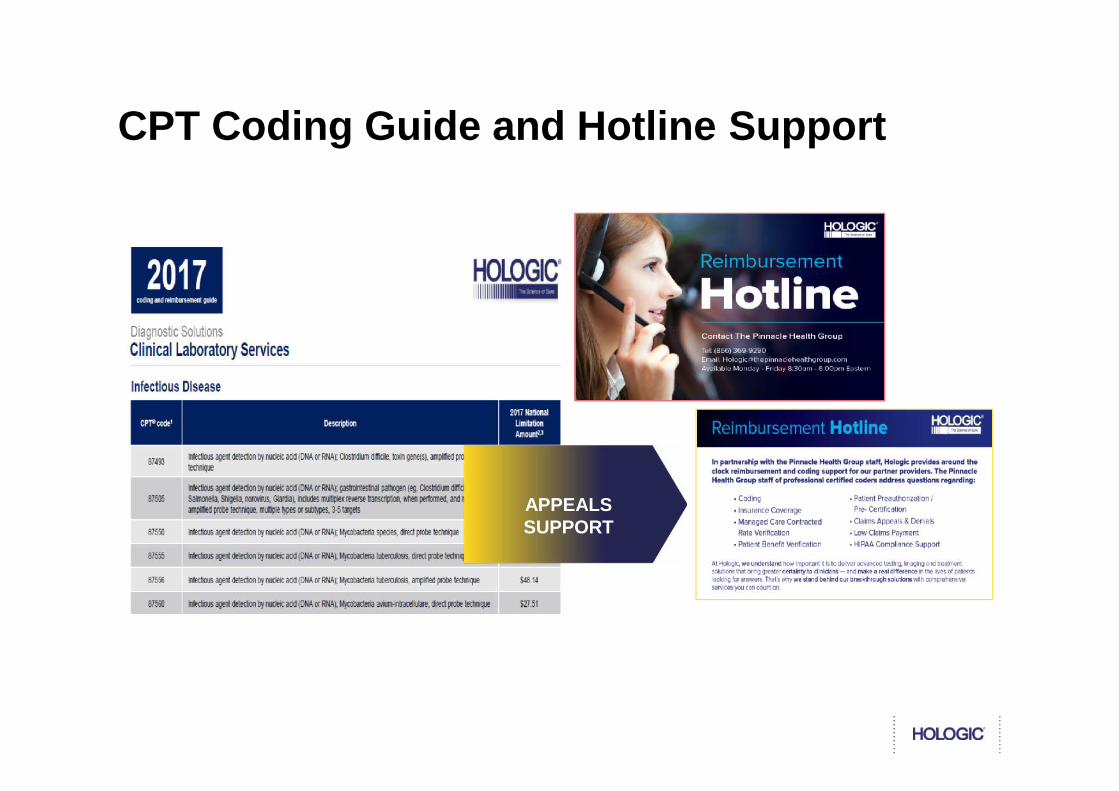
CPT Coding Guide and Hotline Support
APPEALSSUPPORT
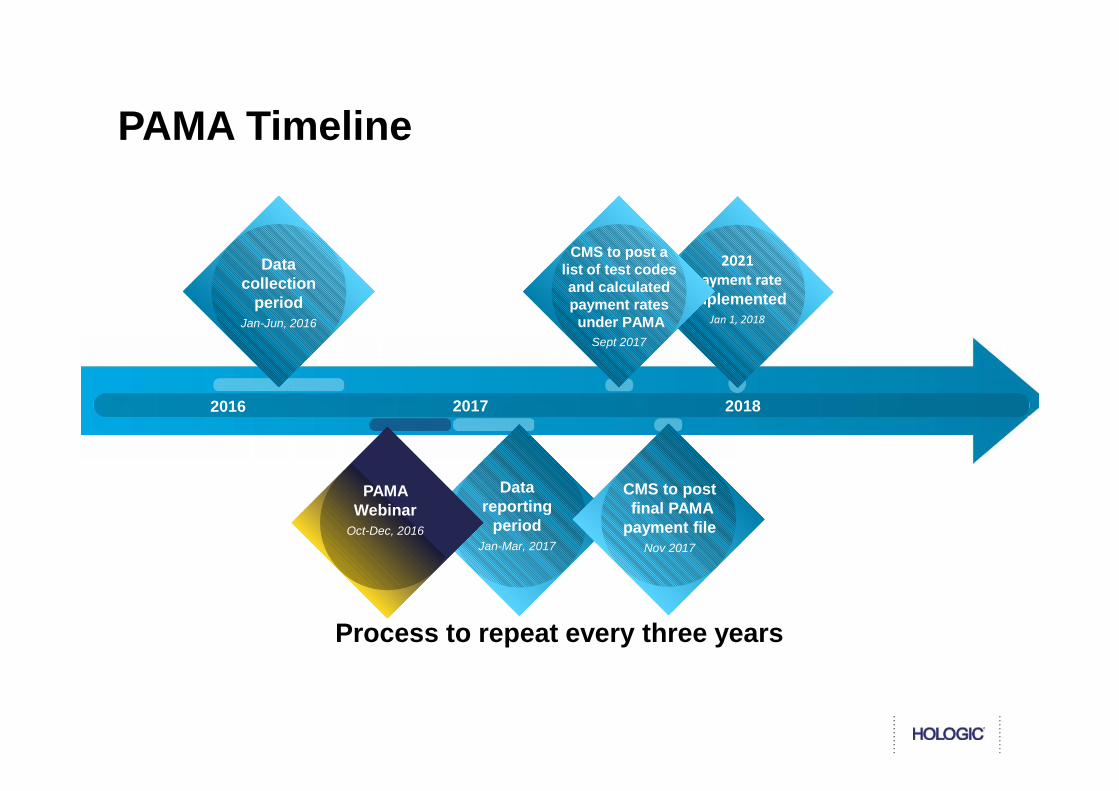
PAMA Timeline
Process to repeat every three years
Datareporting
periodJan-Mar, 2017
Datacollection
periodJan-Jun, 2016
2021payment rate
implementedJan 1, 2018
CMS to postfinal PAMA
payment fileNov 2017
2016 2017 2018
CMS to post alist of test codesand calculatedpayment ratesunder PAMA
Sept 2017
PAMAWebinar
Oct-Dec, 2016
Who Reported:“Applicable Laboratory”
• Not all labs were required to report data• Reporting was mandatory if the lab was an applicable lab
(subject to stiff penalties for failure to report)
“Applicable Information”• Private payor rates and volumes for CLFS tests using
specific• HCPCS codes
Timing•Reporting in 2017 of applicable information from first half of2016•New rates apply January 1, 2018•Three-year cycle
Special provisions for “Advanced DiagnosticLaboratory Tests”
Permit hospitals to report if they have significant outreach business
Was the Correct Information Reported?
Report • Tests furnished on a non-contracted basis(e.g. out-of-network, private pay)
ShouldNot
Report• Any test for which payment is made on a
capitated or other similar payment basisduring the data collection period
• Tests subject to an unresolved appeal
• Tests with final payment of zero dollars(e.g., because payor refusedto pay)
Customer Data Submission
Certified by the Lab Leadership
• Executive (President, CEO, or CFO, or an individual who has beendelegated authority to sign for and who reports directly to such anofficial) of the Reporting Entity must attest that data are accurate,complete, and truthful, and meet all the reporting parameters
• Individual with delegated authority added in response to comments
PAMA Participation Results
45 Percent of independent labs will report
5 Percent of physician office labs (POLs) will reportIn fact: Less than 1 percent (1,100) POLs reported
17 tests will not have data reported In fact: 57 tests had zero data reported
Hospital outreach labs will be represented in data set
In fact: 21 hospital labs reported data
Annual savings of $390 million in Year 1 alone In fact: Anticipated savings nearly doubled to $670
Million in CY 2018
CMS Cited Overall Impact to the CLFS:
• For approximately 10 percent of the HCPCS codes on the CLFS,the weighted median of the private payor rates is an increase overthe CY 2017 CLFS NLA.
• For approximately 75 percent of the HCPCS codes on the CLFS,the weighted median of the private payor rates is a decrease fromthe CY 2017 CLFS NLA.
• About 58 percent of HCPCS codes will receive a phased-inpayment reduction in CYs 2018, 2019, and 2020 rather than the fullprivate payor rate-based payment amount in CY 2018 because thetotal payment decrease would be greater than the 10 percent floor.
• The Top 25 HCPCS codes, by 2016 CLFS spending, account for 63percent of total CLFS spending.
The new payment system is scheduled to go into effect January 1,2018
The new payment system is scheduled to go into effect January 1,2018
The Diagnostic Industry Responds
Quest Diagnostics Responds to ProposedPAMA 2018 Medicare Payment Rates forClinical Laboratory Tests
LabCorp (LH) Objects To Proposed PAMA2018 Medicare Payment Rates For ClinicalLaboratory Tests; Calls For Delay InImplementation To Avoid Significant HarmTo Medicare Beneficiaries
CMS 2018 PAMA Pricing Cut for Lab Tests Deeper ThanPrior Estimate; Advanced Dx Lab Tests Fare WellSep 22, 2017 | Turna Ray This article was updated onSept. 25.
NEW YORK (GenomeWeb) – The Centers for Medicare &Medicaid Services' initial prices for clinical lab tests issuedunder the Protecting Access to Medicare Act (PAMA) wouldsave the government payor around $670 million, shavingnearly 10 percent off the $7 billion that it pays annually for labtests.
CMS previously estimated that using a market-based systemstipulated under PAMA would save $390 million in the firstyear of 2018, and $3.93 billion over a decade. The deeperproposed cuts, slated to go into effect in January, didn't sitwell with the American Clinical Laboratory Association.Industry players have a month to comment on the draft pricesand make their case to CMS for any changes before finalprices are released in November.
Draft 2018 CLFS Reveals Fundamental Flaws inPAMA Reporting Exercise; Time to Take Action
Four Key Issues to Challenge• The CMS definition of "applicable lab" resulted in the exclusion of the majority of hospital labs which
perform half of all lab testing. The narrow definition of size also excludes many POLS, comprising 7% ofthe lab market, leaving the exercise to just 34% of the lab market, where the two major labs represent 80%of the volume.
• The prior administration's decision to impose a retrospective data collection period through rulemaking did notallow labs to make arrangements to collect data accurately or in totality.
• The current regulation does not provide a clear and transparent mechanism for aggregation of eachclinical test's payment data and a means for stakeholders to validate the accuracy of the final paymentamount.
• The legislation indicates calculation of a "weighted median" vs. a "weighted average." Because the "applicablelab" definition has skewed the submitting labs to be primarily the two major labs, a weighted median resulted inhigh volume tests skewing to private payor pricing to only those two labs without the benefit of weighting paymentsmade to the greater majority of the lab industry.
Monday, September 25, 2017; published by Xifin;https://www.xifin.com/resources/blog/201709/draft-2018-clfs-reveals-fundamental-
flaws
Industry Advocacy Efforts
October 6 consensus letter to CMS from 22industry stakeholder groups including ACLA,NILA, AHA, AMA and others
Calling for CMS to:Modify the PAMA regulation to address data integrityconcerns and market exclusion through a statistically validprocess that is least burdensome on providers;Ensure that the private payer data CMS collects accuratelyrepresents all segments of the clinical laboratory market(national independent, community and rural independent,hospital outreach, and physician office laboratories); andProvide a transparent process to allow for the validation ofthe data collected by CMS
Biomarker and DiagnosticWorkshop
Danielle Scelfo, MHSA
Senior Director, Health Policy andReimbursement
10210 Genetic Center Drive, San DiegoCA 92121
1.858.410.7891