rehospitalization rates of patients with bipolar disorder discharged on a mood stabilizer versus a...
TRANSCRIPT

Rehospitalization Rates of Patients With Bipolar Disorder Discharged on a Mood Stabilizer Versus a Mood Stabilizer Plus an Atypical or Typical Antipsychotic
Nick C. Patel, PharmD, PhD M. Lynn Crismon, PharmD Michael Pondrom, PharmD
Abstract One-year rehospitalization rates of patients with bipolar disorder discharged on a mood stabi-
lizer alone, a mood stabilizer plus a typical antipsychotic, or a mood stabilizer plus an atypical antipsychotic were examined. Time to rehospitalization was measured by using the product-limit (Kaplan-Meier) formula. Twenty-three percent of patients on a mood stabilizer alone, 27% of pa- tients on a mood stabilizer plus a typical antipsychotic, and 25% of patients on a mood stabilizer plus an atypical antipsychotic were rehospitalized within 1 year of discharge. There were no sig- nificant differences in rehospitalization rate or time to rehospitalization between groups. One-year rehospitalization rates for patients on a mood stabilizer plus olanzapine or risperidone were 25%. The number of previous psychiatric hospitalizations contributed to the risk of readmission. Risk factors and medication costs should be considered when designing the optimal treatment plan for an individual patient. Long-term prospective studies are needed to better delineate the effectiveness of different pharmacotherapeutic regimens on the long-term treatment outcomes in patients with bipolar disorder.
Introduction In clinical practice, patients with bipolar disorder are commonly treated with combination therapy
of a mood stabilizer and an antipsychotic.1 Acute manic episodes, particularly with severe agitation or psychotic symptoms, provide clinical rationale for the use of antipsychotics in patients with bipolar disorder. Newer atypical antipsychotics have demonstrated efficacy in treating acute mania in patients with bipolar disorder. Olanzapine is indicated for the short-term treatment of acute mania, either as monotherapy or in combination with lithium or valproate, as recent, double-blind, placebo- controlled trials have demonstrated its efficacy in reducing manic symptoms. 2-4 Similar reductions in symptoms have been demonstrated in patients with acute mania with the use of risperidone (alone
Address correspondence to Nick C. Patel, PharmD, PhD, Assistant Professor of Pharmacy Practice and Psychiatry, The University of Cincinnati, 3225 Eden Avenue, PO Box 670004, Cincinnati, OH 45267. E-mail: [email protected].
M. Lynn Crismon, PharmD, is Behrens Inc Centennial Professor in Pharmacy and Associate Dean of Clinical Programs, College of Pharmacy, The University of Texas at Austin.
Michael Pondrom, PharmD, is clinical psychiatric pharmacist, 39 Chepachet Rd, Avon, Conn.
Journal of Behavioral Health Services & Research, 2005, 32(4), 438-445. (~ 2005 National Council for Community Behavioral Healthcare.
438 The Journal of Behavioral Health Services & Research 32:4 October~December 2005

and in combination with mood stabilizers), quetiapine, ziprasidone, and aripiprazole. 5-1~ Quetiapine also has an indication for acute mania, but did not at the time of this study.
With regard to maintenance treatment of bipolar disorder, olanzapine is the only atypical an- tipsychotic studied in randomized double-blind trials and was recently approved as maintenance treatment for patients with bipolar disorder. Studies have demonstrated significantly higher remis- sion rates and lower rates of relapse over 43 to 49 weeks with olanzapine alone or in combination with mood stabilizers. 2'11,12 Six- and 12-month open-label t_rials of risperidone plus a mood stabilizer have shown significant reduction in manic symptoms, ls'14 To date, no head-to-head comparisons of atypical antipsychotics for the maintenance treatment of bipolar disorder have been conducted.
Despite several pharmacological options for maintenance phase treatment, many patients with bipolar disorder continue to experience unfavorable outcomes. Twenty-five percent of patients with bipolar disorder are rehospitalized within 11 months of their first episode, and 50% within 4 years. 15 It is important to know from naturalistic evaluations as well as randomized controlled trials how different medication regimens, including use of mood stabilizers and specific atypical antipsychotics in combination, affect rehospitalization rates in patients with bipolar disorder, as hospitalization is one indicator of poor patient outcomes. The purpose of the current study was to examine 1-year rehospitalization rates of patients with bipolar disorder discharged from Austin State Hospital on a mood stabilizer alone versus a mood stabilizer plus an atypical or typical antipsychotic.
Methods
Approvals for human subjects research from the institutional review boards at The University of Texas at Austin and the Texas Department of Mental Health and Mental Retardation were received prior to the initiation of this study.
All patients between 18 and 65 years of age and discharged from the Austin State Hospital between August 1, 1997, and June 30, 2000, with a diagnosis of bipolar affective disorder were considered eligible for the study. To examine the effects of specific medication regimens on rehospitalization rates, patients were required to be discharged on lithium or divalproex, with or without adjunctive typical or atypical antipsychotic therapy. Evidence-based practice guidelines recommend lithium and divalproex as first-line treatment in bipolar disorder. L6 These two have the largest combination of research evidence and clinical experience, 16 and are the most commonly used mood stabilizers at the Austin State Hospital. Thus, a large number of potential participants were identified. Limiting subject inclusion to patients discharged on lithium or divalproex also decreased sample variability. With regard to the inclusion of selected atypical antipsychotics, olanzapine was the only atypical antipsychotic with a Food and Drug Administration-approved indication for the treatment of acute mania at the time of the study. Risperidone was chosen on the basis of the large clinical off-label use of the drug in treating bipolar disorder, thus allowing evaluation of rehospitalization rates of individuals with bipolar disorder discharged on the most commonly used pharmacological interven- tions. Concurrent discharge psychotropic medications (antidepressants and benzodiazepines) and anticholinergic medications were allowed.
Patients with other primary Axis I diagnoses, excluding substance abuse, were not considered for this study. Patients not discharged on either lithium or divalproex, patients discharged on both lithium and divalproex, or patients discharged on other anticonvulsants (eg, carbamazepine, gabapentin, lamotrigene, or topiramate) were not eligible.
One-year rehospitalization status was examined from August 1, 1997, to June 30, 2001 for patients discharged from the Austin State Hospital on 1 of the following 3 medication regimens: a mood stabilizer alone, a mood stabilizer plus a typical antipsychotic, or a mood stabilizer plus an atypical antipsychotic. Readmission was defined as rehospitalization to the Austin State Hospital. Risk factors for readmission that were examined included number of previous psychiatric rehospitalizations
Rehospitalization Rates of Patients With Bipolar Disorder PATEL et al. 439

(5-year period), duration of index hospitalization, time on mood stabilizer prior to discharge, time on antipsychotic prior to discharge, co-occurring substance abuse, and concomitant antidepressant u s e .
Time to rehospitalization analyses were conducted in 2 separate stages: (1) a mood stabilizer alone versus a mood stabilizer plus a typical or an atypical antipsychotic and (2) a mood stabilizer plus olanzapine versus a mood stabilizer plus risperidone. Survival curves were estimated by using the product-limit (Kaplan-Meier) formula and compared by the log-rank testJ 7 Rehospitalization rates were compared using the Mantel-Cox chi-square test. 17 The Cox proportional hazards regression model was used to analyze covariates thought to affect time to rehospitalization, such as age, gender, ethnicity, bipolar diagnostic subtype, presence of psychotic symptoms, comorbid substance abuse disorder, and concomitant antidepressant use. Standard chi-square tests, unpaired t tests, and non- parametric tests were used to compare demographic variables. All statistical tests used were 2-tailed, and significance was defined as ot < .05.
An a priori power analysis was conducted to determine the sample size necessary to achieve adequate power given a medium effect size and standard c~ level. For the comparison of a mood stabilizer alone versus a mood stabilizer plus a typical or an atypical antipsychotic, 107 patients per medication group were necessary to achieve an effect size of 0.30 at a power of 0.80 for an a of .05. For the comparison of a mood stabilizer plus olanzapine versus a mood stabilizer plus risperidone, 87 patients per group were necessary for the same statistical parameters.
Results
A total of 479 patients met inclusion criteria for the study: 157 (32.8%) patients receiving mood stabilizer monotherapy, 84 (17.5%) receiving a mood stabilizer plus a typical antipsychotic, and 238 (49.7%) receiving a mood stabilizer plus an atypical antipsychotic. No significant differences in age, percent of comorbid substance abuse, or average daily lithium dose were evident between the 3 groups. No significant difference was found for time on antipsychotic before discharge between the 2 groups receiving antipsychotic therapy.
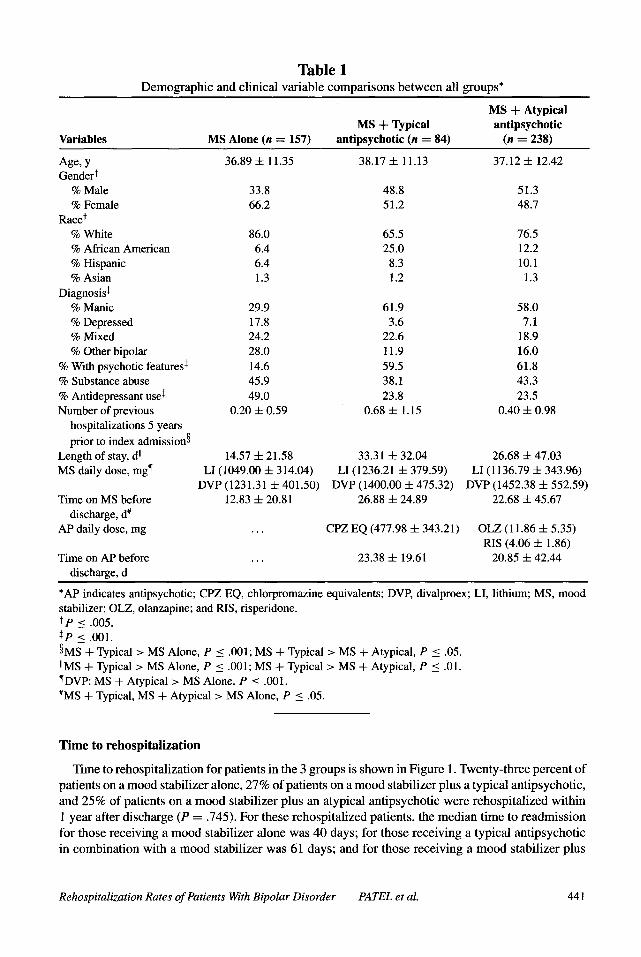
Significant differences in gender (X z = 12.272, d f = 2, P = .002), ethnicity (X 2 = 19.793, d f = 6, P = .003), and percent concomitant antidepressant use (X 2 = 31.428, d f = 2, P < .001) were found between all the 3 groups. Additional differences in bipolar disorder diagnostic subtype (X 2 = 44.558, d f = 6, P < .001 ) and percentage of patients with psychotic features (X 2 = 92.137, d f = 2, P < .001) were seen, as the group receiving a mood stabilizer plus an atypical antipsychotic was predominantly of the manic subtype and had psychotic symptoms. The groups significantly differed in the number of previous psychiatric hospitalizations (F = 7.769, P < .001), duration of hospitalization (F = 8.013, P < .001), and time on mood stabilizer (F = 5.395, P = .005). Post hoc analysis showed that patients receiving a mood stabilizer plus a typical antipsychotic had more psychiatric hospitalizations in a 5-year period prior to admission compared with those receiving a mood stabilizer alone (P < .001) or a mood stabilizer plus an atypical antipsychotic (P = .041). Patients treated with a mood stabilizer alone had shorter durations of hospitalization compared with patients treated with a mood stabilizer plus a typical (P = .001) or an atypical (P = .006) antipsychotic. Patients taking a mood stabilizer alone had shorter times on mood stabilizer before discharge compared with patients taking a mood stabilizer plus a typical (P = .011) or an atypical (P = .02) antipsychotic. A significant difference in the average daily dose of divalproex was found between groups (F = 6.612, P ---- .002), as patients on divalproex alone had lower daily doses compared with those on divalproex plus an atypical antipsychotic (P = .001). Table 1 shows further details of demographic and clinical variables.
Within the mood stabilizer plus an atypical antipsychotic group, 136 patients received olanzapine and 102 patients received risperidone. There were no significant differences on any demographic or clinical variables between the olanzapine and risperidone groups.
440 The Journal of Behavioral Health Services & Research 32:4 October~December 2005
T a b l e 1 Demographic and clinical variable comparisons between all groups*
Variables MS Alone (n = 157) MS h- Typical
antipsychotic (n = 84)
MS + Atypical antipsychotic
(n = 238)
Age, y Gender t
% Male % Female
Race t % White % African American % Hispanic % Asian
Diagnosis~ % Manic % Depressed % Mixed % Other bipolar
% With psychotic features ~ % Substance abuse % Antidepressant use~ Number of previous
hospitalizations 5 years prior to index admissionw
Length of stay, d II MS daily dose, mg �82
Time on MS before discharge, d #
AP daily dose, mg
36.89 • 11.35
33.8 66.2
86.0 6.4 6.4 1.3
29.9 17.8 24.2 28.0 14.6 45.9 49.0
0.20 • 0.59
14.57 -4- 21.58 LI (1049.00 • 314.04)
DVP (1231.31 5: 401.50) 12.83 -4- 20.81
38.17 • 11.13
48.8 51.2
65.5 25.0
8.3 1.2
61.9 3.6
22.6 11.9 59.5 38.1 23.8
0.68 • 1.15
33.31 • 32.04 LI (1236.21 q- 379.59)
DVP (1400.00 • 475.32) 26.88 • 24.89
CPZ EQ (477.98 • 343.21)
Time on AP before ... 23.38 -4- 19.61 discharge, d
37.12 q- 12.42
51.3 48.7
76.5 12.2 10.1
1.3
58.0 7.1
18.9 16.0 61.8 43.3 23.5
0.40 • 0.98
26.68 4- 47.03 LI (1136.79 + 343.96)
DVP (1452.38 4- 552.59) 22.68 -I- 45.67
OLZ (11.86 -t- 5.35) RIS (4.06 + 1.86)
20.85 + 42.44
*AP indicates ant• CPZ EQ, chlorpromazine equivalents; DVP, divalproex; LI, lithium; MS, mood stabilizer; OLZ, olanzapine; and RIS, risperidone. t p < .005. ~P < .001. w + Typical > MS Alone, P < .001; MS + Typical > MS + Atypical, P < .05. IIMS 4- Typical > MS Alone, P < .001; MS + Typical > MS + Atypical, P < .01. �82 MS + Atypical > MS Alone, P < .001. #MS + Typical, MS + Atypical > MS Alone, P < .05.
Time to rehospital izat ion
Time to rehospitalization for patients in the 3 groups is shown in Figure 1. Twenty-three percent of patients on a mood stabilizer alone, 27% of patients on a mood stabilizer plus a typical ant• and 25% of patients on a mood stabilizer plus an atypical ant• were rehospitalized within 1 year after discharge (P = .745). For these rehospitalized patients, the median time to readmission for those receiving a mood stabilizer alone was 40 days; for those receiving a typical ant• in combination with a mood stabilizer was 61 days; and for those receiving a mood stabilizer plus
Rehospitalization Rates of Patients With Bipolar Disorder PATEL et al. 441

Figure 1 Time to rehospitalization. ATYP indicates atypical antipsychotic; MS, mood stabilizer; and TYP,
typical antipsychotic. Log-rank = 0.08, d f = 1, P = .78.
an atypical antipsychotic was 68 days. Differences in median time to rehospitalization (P = .489) and time course to rehospitalization (P = .78) were not significant.
One-year rehospitalization rate for patients on a mood stabilizer plus olanzapine or risperidone was 25% (P = .931). For those rehospitalized, the median time to readmission for those receiving a mood stabilizer plus olanzapine or risperidone was 58 and 83 days, respectively (P = .701). No difference in time to rehospitalization existed between these 2 groups (P = .91).
Analysis using the Cox proportional hazards regression model demonstrated that the number of previous psychiatric hospitalizations 5 years prior to the study period index admission was associated with time to rehospitalization (~ = .384, Wald = 43.070, P < .001). After controlling for previous hospitalizations (covariate mean = 0.382) using the Cox model, it was found that patients discharged on a mood stabilizer and a typical antipsychotic had a rehospitalization rate of 24.7%, those discharged on a mood stabilizer alone had a rehospitalization rate of 24.2%, and those discharged on a mood stabilizer plus an atypical antipsychotic had a rehospitalization rate of 23.2%. The differences in rehospitalization rates and time to rehospitalization between the groups were not significant.
Discussion
The 1-year rehospitalization rates in this study (23%-27%) are lower than those in previous published reports, which range from 41% to 60%. 18-20 In all 3 groups, the mean number of previous hospitalizations 5 years prior to the index admission was less than 1, which may suggest that these patients were at relatively low risk for rehospitalization during the study period. 21 Other factors may have influenced a lower rehospitalization rate in the current study, including managed care and increased pressure to keep patients out of the hospital. While it is difficult to compare rehospitalization
442 The Journal of Behavioral Health Services & Research 32:4 October~December 2005
rates from different studies, these findings reflect that pharmacotherapy had positive effects on patient outcomes.
In bipolar patients without a psychotic component, mood stabilizer monotherapy appears to be associated with reduced rehospitalization. The results suggest that physicians are more likely to use an antipsychotic in combination with a mood stabilizer for bipolar patients with mania and psychosis, and that physicians view combination treatment to be warranted in this patient population so as to achieve symptom reduction and patient stabilization. Comparable rehospitalization rates between patients receiving a mood stabilizer plus olanzapine or risperidone suggest the possibility of similar mood-stabilizing properties for these 2 agents when used in combination with a mood stabilizer.
Several possible explanations exist as to why no significant differences in rehospitalization rates or time to rehospitalization were found for patients receiving monotherapy versus combination therapy. On the basis of bipolar diagnostic subtypes, patients receiving a mood stabilizer plus an antipsychotic were more likely to be manic and have psychotic symptoms than were patients receiving a mood stabilizer alone. Patients on combination treatment also had a longer length of stay of the index hospitalization. All of these differences suggest that the combination therapy patients may have had a greater severity of illness. As typical and atypical antipsychotics have been shown to have mood-stabilizing properties, similar rehospitalization rates between the 2 groups suggest that patients receiving a mood stabilizer plus an antipsychotic may have experienced fewer exacerbations of illness. 2,11-14,22 Analyses based upon bipolar diagnostic subtypes and the presence of psychotic symptoms were not conducted because the study was not adequately powered to examine these parameters. Unmeasured factors (eg, family support, social stressors, adequacy of community-based services, medication adherence) are other important variables affecting rehospitalization that were not evaluated in this study. 21,23 Lastly, it is possible that no significant difference exists among these treatment regimens in their ability to prevent rehospitalization.
When drawing conclusions from this study, one must remember that individuals may experience moderate exacerbations of psychiatric symptoms and still not require hospitalization. On the other hand, readmission to a psychiatric hospital does not necessarily mean that a patient has experienced an acute exacerbation of the psychiatric illness. It has been suggested that individuals with severe mental disorders may seek readmission to state hospitals because of social stressors, such as financial or housing problems. 24,25 Individuals with mental disorders admitted to Texas state hospitals must be a danger to themselves or others or have experienced a significant deterioration in symptoms, and economic pressures have decreased the likelihood that hospitalizations are for social reasons. Thus, it is unlikely that rehospitalizations in this study were largely for social reasons.
The limitations of this study are similar to those of previous studies that examined rehospitalization rates for certain psychiatric disorders. 26-28 Patients were not randomly assigned to drug treatment groups, and this introduces the possibility that differences between groups affected the results. Al- though differences in previous hospitalizations were adjusted, the possibility exists that other factors that were unavailable, such as type and duration of outpatient mental health services and treatments, may have affected time to rehospitalization. The possibility also exists that patients could have had psychiatric hospitalization at other hospitals. Medication adherence rates postdischarge could not be determined and thus, differing rates of medication adherence may have influenced the results. Additionally, continuation of the medication regimen on which the patient was discharged could not be confirmed. It is possible that medications were switched or additional adjunctive medications were initiated. From this perspective, the analyses should be viewed as intent-to-treat analyses. This is significant in that at the time data were collected for this study, lithium and divalproex were consid- ered first-line treatment options in most accepted guidelines for the treatment of bipolar disorder. 16,29 In fact, these agents are used in up to 90% of patients with bipolar disorder. 3~ Augmentation with antipsychotics, usually in more severely symptomatic patients, is also viewed as an appropriate in- tervention. Thus, the results of this study provide a snapshot of the rehospitalization rate outcomes that were associated with a decision to use different first-line pharmacotherapy options during an
Rehospitalization Rates of Patients With Bipolar Disorder PATEL et al. 443

index hospitalization. It is recognized that patients discharged on other mood-stabilizer regimens may have different rehospitalization rates than those reported in this study. 30'31 Furthermore, pa- tients with comorbid Axis I or II diagnoses may also have different rehospitalization rates compared with rates in patients with only bipolar disorder. Despite these limitations, this study provides a "real-world" evaluation of rehospitalization rates associated with commonly used pharmacotherapy for the treatment of bipolar disorder.
Implications for Behavioral Health
Patients with bipolar disorder with psychotic features may require more assertive treatment, and past hospitalizations are a predictor of future increased risk of hospitalization. These baseline dif- ferences indicate that patients treated with combination treatment may have been more severely ill, and this provides a possible explanation for no difference in rehospitalization rates being seen between the 2 treatment groups. It is therefore feasible that combination treatment allowed more severely ill patients to achieve outcomes that were similar to those observed with mood stabilizer monotherapy in individuals without these risk factors. These types of patient population risk factors are important for clinicians to consider in making drug treatment choices for individual patients in an attempt to improve adaptive functioning and decrease the risk of relapse and rehospitalization. Long-term prospective studies are needed to better delineate the effectiveness of different phar- macotherapeutic regimens on the long-term treatment outcomes of patients with bipolar disorder. Additionally, future research should examine how outpatient services and treatments, in conjunction with pharmacological interventions, impact rehospitalization rates in bipolar disorder.
Acknowledgments
This research was supported in part by grants from Eli Lilly and Company (UTA02-9135) and the Texas Department of Mental Health and Mental Retardation, and a Ruth L. Kirschstein National Research Service Awards Postdoctoral Training Fellowship sponsored by the National Institute of Mental Health (N. Patel). The authors thank Karen Rascati, PhD (College of Pharmacy, The University of Texas at Austin), for her support and Mark Mason, MA (Texas Department of Mental Health and Mental Retardation), for his assistance with data collection.
References
1. SemyakMJ, Griffin RA, Johnson RM, et al. Neuroleptic exposure following inpatient treatmentofacute mania with lithium and neuroleptic. American Journal of Psychiatry. 1994;151:133-135.
2. Tohen M, Sanger TM, McElroy SL, et al. Olanzapine versus placebo in the treatment of acute mania. American Journal of Psychiatry. 1999;156:702-709.
3. Tohen M, Jacobs TG, Grundy SL, et al. Efficacy of olanzapine in acute bipolar mania: a double-blind, placebo-controlled study. Archives of General Psychiatry. 2000;57:841-849.
4. Tohen M, Chengappa KN, Suppes TR, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Archives of General Psychiatry. 2002;59:62-69.
5. Segal J, Berk M, Brook S. Risperidone compared with both lithium and haloperidol in mania: a double-blind randomized controlled trial. Clinical Neuropharmacology. 1998;21:176-180.
6. Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania. International, double-blind, randomised controlled trial. British Journal of Psychiatry. 2003; 182:141-147.
7. Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. American Journal of Psychiatry. 2002; 159:1146-1154.
8. Jones MW, Huizar K. Quetiapine monotherapy for acute mania associated with bipolar disorder (STAMP 1 and STAMP 2). Poster presented at: Annual Meeting of the American Psychiatric Association; May 17-22, 2003; San Francisco, Calif.
9. Keck PE Jr, Versiani M, Potkin S, et al. Ziprasidone in the treatment of acute bipolar mania: a three-week, placebo-controlled, double-blind, randomized trial. American Journal of Psychiatry. 2003;160:741-748.
10. Keck PE, Marcus R, Tourkodimitris S, et al. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. American Journal of Psychiatry. 2003;160:1651-1658.
444 The Journal of Behavioral Health Services & Research 32:4 October~December 2005

11. Tohen M, Ketter TA, Zarate CA, et al. Olanzapine versus divalproex sodium for the treatment of acute mania and maintenance of remission: a 47-week study. American Journal of Psychiatry. 2003; 160:1263-1271.
12, Vieta E, Reinares M, Corbella B, et al. Olanzapine as long-term adjunctive therapy in treatment-resistant bipolar disorder. Journal of Clinical Psychopharmacology. 2001 ;21:469-473.
13, Vieta E, Goikolea JM, Olivares JM, et al. 1 -year follow-up of patients treated with risperidone and topiramate for a manic episode. Journal of Clinical Psychiatry. 2003;64:834-839.
14. Vieta E, Goikolea JM, Corbella B, et al. Risperidone safety and efficacy in the treatment of bipolar and schizoaffective disorders: results from a 6-month, multicenter, open study. Journal of Clinical Psychiatry. 2001 ;62:818-825.
15. Kessing LV, Andersen PK, Mortensen PB, et al. Recurrence in affective disorder, I: case registry study. British Journal of Psychiatry. 1998;172:23-28.
16. Suppes T, Dennehy EB, Swann AC, et al. Report of the Texas Consensus Conference Panel on medication treatment of bipolar disorder 2000. Journal of Clinical Psychiatry. 2002;63:288-299.
17. Friedman LM, Furberg CD, DeMets DL. Fundamentals of Clinical Trials. 2nd ed. Littleton, Mass: PSG Publishing Co Inc; 1985. 18. Strober M, Morrell W, Lampert C, et al. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar
illness: a naturalistic study. American Journal of Psychiatry. 1990;147:457-461. 19. Goldberg JF, Harrow M, Grnssman LS. Course and outcome in bipolar affective disorder: a longitudinal follow-up study. American Journal
of Psychiatry. 1995;152:379-384. 20. Perlick DA, Rosenheck RA, Clarkin JF, et al. Symptoms predicting inpatient service use among patients with bipolar affective disorder.
Psychiatric Services. 1999;50:806-812. 21. Keck PE Jr, McElroy SL, Strakowski SM, et al. 12-month outcome of patients with bipolar disorder following hospitalization for a manic
or mixed episode. American Journal of Psychiatry. 1998;155:646-652. 22. Miller DS, Yathanl LN, Lain RW. Comparative efficacy of typical and atypical antipsychotics as add-on therapy to mood stabilizers in the
treatment of acute mania. Journal of Clinical Psychiatry. 2001;62:975-980. 23. Haywood TW, Kravitz HM, Grossman LS, et al. Predicting the "revolving door" phenomenon among patients with schizophrenic, schizoaf-
fective, and affective disorders. American Journal of Psychiatry. 1995;152:856-861. 24. Surber RW, Winkler EL, Monteleone M, et al. Characteristics of high users of psychiatric inpatient services. Hospital and Community
Psychiatry. 1987;38:1112-1114. 25. Harris M, Bergman HC, Bachrach LL. Psychiatric and nonpsychiatric indicators for rehospitalization in a chronic patient population.
Hospital and Community Psychiatry. 1986;37:630-631. 26. Conley RR, Love RC, Kelly DL, et al. Rehospitalization rates of patients recently discharged on a regimen of risperidone or clozapine.
American Journal of Psychiatry. 1999;156:863-868. 27. Rabinowitz J, Lichtenberg P, Kaplan Z, et al. Rehospitalization rates of chronically ill schizophrenic patients discharged on a regimen of
risperidone, olanzapine, or conventional antipsychotics. American Journal of Psychiatry. 2001;158:266-269. 28. Patel NC, Dorson PG, Edwards NJ, et al. One-year rehospitalization rates using the atypical antipsychotics versus the conventional
antipsychoties. Psychiatric Services. 2002;53:891-893. 29. Sachs GS, Printz D J, Kahn DA, et al. The Expert Consensus Guideline Series: Medication Treatment of Bipolar Disorder 2000. Postgraduate
Medicine. 2000:1-104. Special number. 30. Lim PZ, Tunis SL, Edell WS, et al. Medication prescribing patterns for patients with bipolar I disorder in hospital settings: adherence to
published practice guidelines. Bipolar Disorders. 2001 ;3:165-173. 31. Levine J, Chengappa KNR, Brar JS, et al. Psychotropic drug prescription patterns among patients with bipolar I disorder. Bipolar Disorders.
2000;2:120-130.
Rehospitalization Rates of Patients With Bipolar Disorder PATEL et al. 445