recurrent embolic strokes associated with vertical atlantoaxial subluxation in a patient with...
TRANSCRIPT
Case
ReportRecurrent Embolic Strokes AssociatedwithVertical AtlantoaxialSubluxation in a Patient with Rheumatoid Arthritis: A Case
Report and Review of Literature
Takuma Kuroki, MD,* Yuji Ueno, MD, PhD,* Ikuko Takeda, MD,*
Taiki Kambe, MD, PhD,* Kenya Nishioka, MD, PhD,* Hideki Shimura, MD, PhD,*
Masanori Itoh, MD, PhD,† Nobutaka Hattori, MD, PhD,‡ and Takao Urabe, MD, PhD*
From the *Department
Hospital, Chiba; †Depart
Urayasu Hospital, Chiba
University School of Med
Received April 27, 201
July 5, 2013.
Funding: None.
Address corresponden
Neurology, Juntendo Un
Urayasu, Chiba 279-0021
1052-3057/$ - see front
� 2013 by National Str
http://dx.doi.org/10.1
e676
We report a 78-year-old woman with rheumatoid arthritis who developed recurrent
embolic cerebellar strokes associated with vertical atlantoaxial subluxation (AAS).
On contrast angiography, the bilateral vertebral arteries (VAs) were occluded be-
tween the C1 and C2 levels, and the distal parts of bilateral VA were supplied by
the collateral circulations. Dynamic cerebral angiography and carotid duplex ultra-
sonography showed that blood flow was substantially decreased in the left VA and
left posterior inferior cerebellar artery on cervical anteflexion. It is suggested that
vertical AAS reduced the blood flow of collateral circulation in the left VA with
cervical anteflexion and might be a cause of recurrent ischemic stroke. Key Words:
Atlantoaxial subluxation—recurrent embolic stroke—angiography—carotid duplex
ultrasonography.
� 2013 by National Stroke Association
Introduction
Atlantoaxial subluxation (AAS), which is because of
destruction of the transverse ligament, with subsequent
laxity, occurs in patients with rheumatoid arthritis
(RA).1 AAS may cause severe neurological morbidity, in-
cluding paresthesia, cervical myelopathy, vertebrobasilar
insufficiency, and even sudden death because of brain-
stem and spinal cord compression.1-3 Transverse
of Neurology, Juntendo University Urayasu
ment of Neurosurgery, Juntendo University
; and ‡Department of Neurology, Juntendo
icine, Tokyo, Japan.
3; revision received June 20, 2013; accepted
ce to Yuji Ueno, MD, PhD, Department of
iversity Urayasu Hospital, 2-1-1 Tomioka,
, Japan. E-mail: [email protected].
matter
oke Association
016/j.jstrokecerebrovasdis.2013.07.010
Journal of Stroke and Cerebrovasc
ligament destruction may cause anterior or vertical
subluxation, at 5% and 1.4%, respectively.1
Disorders of cervical spine including AAS and cervical
spondylosis can cause cerebrovascular accident. Ischemic
stroke and symptomatic vertebrobasilar insufficiency not
infrequently occur during horizontal head rotation in
patients with cervical spine diseases because several ex-
trinsic structural changes of the cervical spine could tran-
siently obstruct the vertebral artery (VA) with head
motion.4-8
We report a case of recurrent embolic strokes in the cer-
ebellar hemispheres in a patient with vertical AAS. Based
on the presence of vertical AAS, dynamic carotid duplex
ultrasonography and cerebral angiography were per-
formed to evaluate for positional alteration of the verte-
brobasilar system with head motion.
Case Report
A 78-year-old woman with a 10-year history of RA
had a head injury after falling, and she then developed
ular Diseases, Vol. 22, No. 8 (November), 2013: pp e676-e681

RECURRENT EMBOLIC STROKES AND ATLANTOAXIAL SUBLUXATION e677
headache and vertigo for 2 weeks before admission.
She also had a medical history of tuberculosis and os-
teoporosis. Her family history included no cerebrovas-
cular diseases. She did not drink alcohol and did not
smoke. She suddenly developed dysarthria and was re-
ferred to our hospital. On admission, her blood pres-
sure was 124/64 mm Hg, and no carotid bruit or
abnormal heart sounds were heard. She had defor-
mities of the proximal and distal interphalangeal joints
of her hands. On neurological examination, she was
alert, but she had bilateral, horizontal gaze-paretic nys-
tagmus and slight dysarthria. Her muscle strengths
were normal. Dysmetria was found in both upper
limbs. The National Institutes of Health Stroke Scale
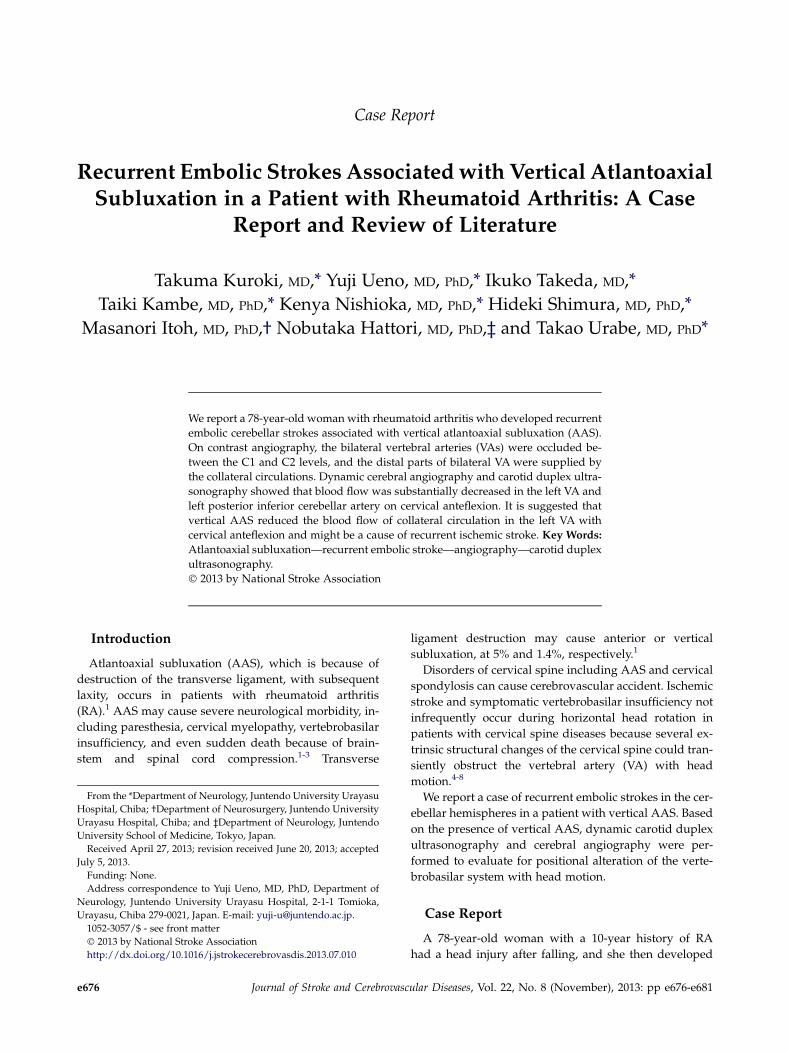
(NIHSS) score was 3 points. Diffusion-weighted imag-
ing showed multiple hyperintense lesions in the cere-
bellar hemispheres (Fig 1, A,B). MR angiography
showed reduced flow signals in vertebrobasilar arteries
(Fig 1, C). On 3-dimensional enhanced computed to-
mography, the left VA was occluded by dislodgment
between C1 and C2, and the right VA was occluded
at the same level and collaterally supplied by a branch
of the right thyrocervical trunk (Fig 1, D,E). There was
no evidence of arterial dissection, including intramural
hematoma, pearl and string signs, or barrel signs, in the
vertebrobasilar artery. We diagnosed her as having ver-
tical AAS based on cervical computed tomography and
magnetic resonance imaging (Fig 2, A-C). The patient
was treated with oral aspirin, intravenous edaravone
(a free radical scavenger), and glycerol soon after ad-
mission. On the third day of admission, she had a fever
of 39.0�C, and her blood pressure decreased to 60/
42 mm Hg. She became somnolent, and her dysarthria
and nystagmus worsened. She also showed left-sided
peripheral facial palsy, and dysmetria worsened in
left-sided limbs. Her NIHSS score was 10. Follow-up
diffusion-weighted imaging showed expansion of hy-
perintense lesions in the cerebellar hemispheres and
brainstem (Fig 2, B,C). Blood examinations revealed
a systemic inflammatory response: marked leukocytosis
with a left shift (white blood cells, 32,000/mL; neutro-
phils, 87%) and elevation of C-reactive protein
(17.6 mg/dL). The plasma D-dimer level was 2.88 mg/
mL. Escherichia coli was detected on blood cultures. Uri-
nalysis was normal. On transthoracic echocardiography,
left and right ventricular wall motions were normal, the
ejection fraction was 60%, and there was no evidence of
infectious endocarditis, including vegetations or de-
struction of valves. She was, therefore, diagnosed as
having early recurrent embolic stroke and septic shock.
Intravenous heparin was started, and an appropriate
antimicrobial agent and a vasopressor drug were given.
Moreover, she underwent cervical collar therapy ac-
cording to the previous case reports.8,9 On the
fifth day of admission, her temperature and blood
pressure were normalized. Her consciousness level
improved gradually, and her NIHSS score was 5.
Dynamic cervical spine X-ray and carotid duplex
ultrasonographic studies were performed (Fig 3A,B).
Doppler images showed an occluded flow pattern in
the left VA with cervical anteflexion, whereas the flow
pattern was normal in the mid-cervical position and
with cervical retroflexion (Fig 3, C,D). The flow pattern
was also normal on horizontal head rotation. Occluded
flow patterns in the right VA were found in any cervi-
cal positions. Cerebral angiography demonstrated that
the left VA was occluded between the C1 and C2 levels,
and the left vertebro-vertebral collateral circulation was
found in the mid-cervical position (Fig 3, E). On cervi-
cal anteflexion, blood flow was substantially decreased
in the left VA and posterior inferior cerebellar artery
(PICA) (Fig 3, F). The right VA could not be evaluated
because of anatomical problem. On the 18th day of ad-
mission, continuous heparin therapy was discontinued,
whereas oral aspirin therapy was continued. She has
had no further stroke recurrence.
Discussion
This case showed recurrent embolic strokes associated
with vertical AAS. She had chronic occlusion of the bilat-
eral VA, and the distal parts of bilateral VAwere supplied
by the collateral circulations.
On contrast angiography, the bilateral VAs were oc-
cluded between C1 and C2 levels. The distal part of
left VA was supplied by left proximal VA via vertebro-
vertebral anastomosis, and dynamic carotid duplex ul-
trasonography and cerebral angiography demonstrated
that blood flows of the left VA and PICA were substan-
tially reduced during cervical anteflexion. The distal
part of right VA was supplied by a branch of the right
thyrocervical trunk, and occluded flow patterns on dy-
namic carotid duplex ultrasonography in the right VA
were found in any cervical positions. In patients with
proximal vertebral artery occlusion, a variety of anasto-
motic flows including thyrocervical, deep cervical, occip-
ital, ascending pharyngeal, and anterior spinal arteries
compensate to the distal part of vertebral artery.10,11
Patients with RA for more than 20 years were reported
to have a high prevalence of VA stenosis or
occlusion.12 Although the present case had a 10-year his-
tory of RA, it is suggested that her bilateral VAs were
chronically occluded and collateral pathways were de-
veloped. There have been several case reports of symp-
tomatic vertebrobasilar insufficiency associated with
AAS in patients with RA.7,8,13 Intriguingly, those cases
showed transient positional occlusion of the VA during
horizontal head rotation.7,8 The present case had
chronic occlusion of the bilateral VA, and substantial
blood flow reduction in the left VA and PICA were
found during cervical anteflexion. Although the
association between reduction of vertebro-vertebral
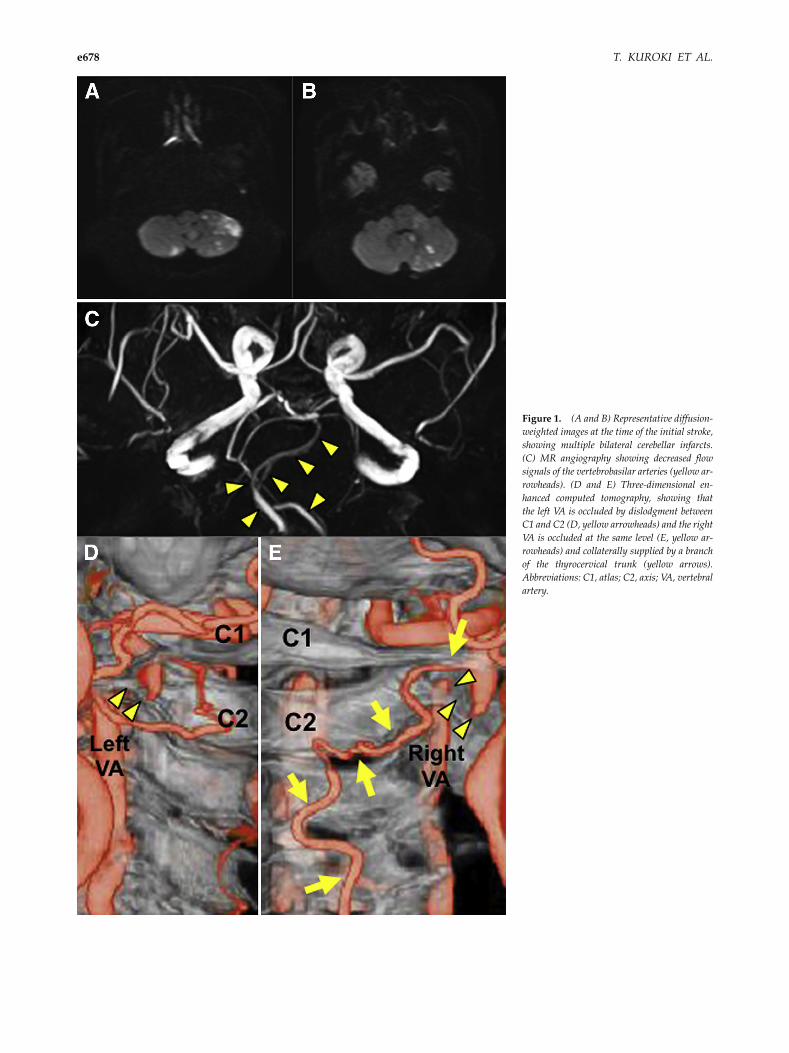
Figure 1. (A and B) Representative diffusion-
weighted images at the time of the initial stroke,
showing multiple bilateral cerebellar infarcts.
(C) MR angiography showing decreased flow
signals of the vertebrobasilar arteries (yellow ar-
rowheads). (D and E) Three-dimensional en-
hanced computed tomography, showing that
the left VA is occluded by dislodgment between
C1 and C2 (D, yellow arrowheads) and the right
VA is occluded at the same level (E, yellow ar-
rowheads) and collaterally supplied by a branch
of the thyrocervical trunk (yellow arrows).
Abbreviations: C1, atlas; C2, axis; VA, vertebral
artery.
T. KUROKI ET AL.e678
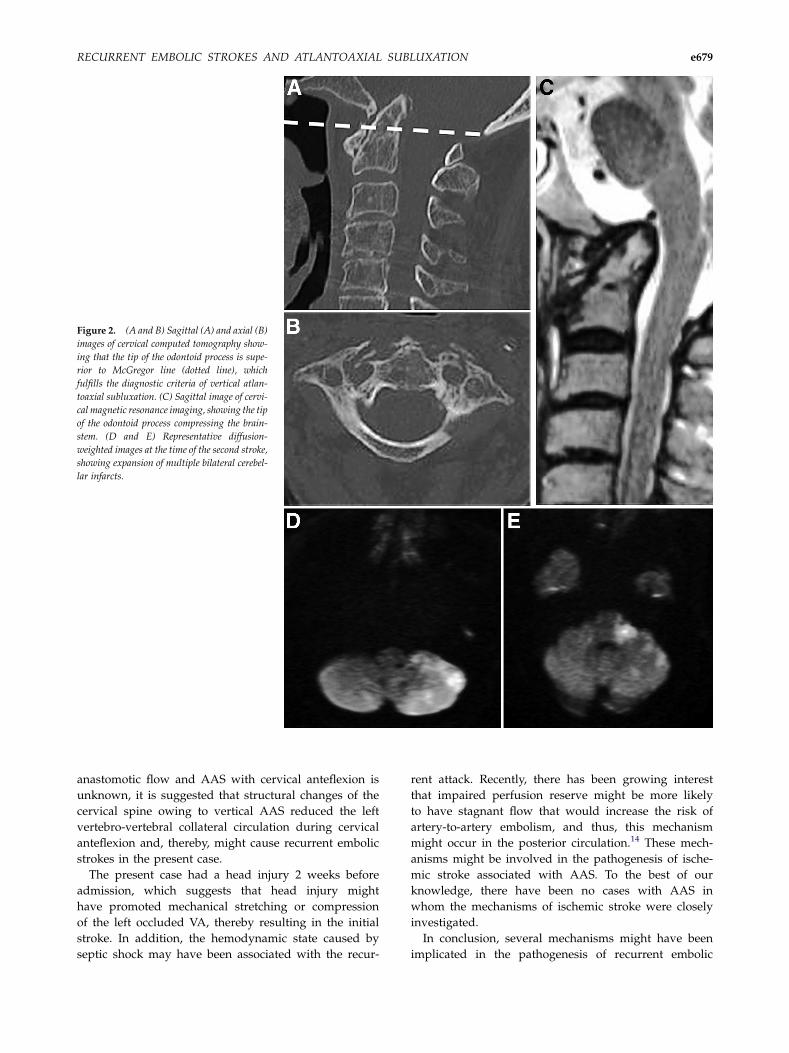
Figure 2. (A and B) Sagittal (A) and axial (B)
images of cervical computed tomography show-
ing that the tip of the odontoid process is supe-
rior to McGregor line (dotted line), which
fulfills the diagnostic criteria of vertical atlan-
toaxial subluxation. (C) Sagittal image of cervi-
cal magnetic resonance imaging, showing the tip
of the odontoid process compressing the brain-
stem. (D and E) Representative diffusion-
weighted images at the time of the second stroke,
showing expansion of multiple bilateral cerebel-
lar infarcts.
RECURRENT EMBOLIC STROKES AND ATLANTOAXIAL SUBLUXATION e679
anastomotic flow and AAS with cervical anteflexion is
unknown, it is suggested that structural changes of the
cervical spine owing to vertical AAS reduced the left
vertebro-vertebral collateral circulation during cervical
anteflexion and, thereby, might cause recurrent embolic
strokes in the present case.
The present case had a head injury 2 weeks before
admission, which suggests that head injury might
have promoted mechanical stretching or compression
of the left occluded VA, thereby resulting in the initial
stroke. In addition, the hemodynamic state caused by
septic shock may have been associated with the recur-
rent attack. Recently, there has been growing interest
that impaired perfusion reserve might be more likely
to have stagnant flow that would increase the risk of
artery-to-artery embolism, and thus, this mechanism
might occur in the posterior circulation.14 These mech-
anisms might be involved in the pathogenesis of ische-
mic stroke associated with AAS. To the best of our
knowledge, there have been no cases with AAS in
whom the mechanisms of ischemic stroke were closely
investigated.
In conclusion, several mechanisms might have been
implicated in the pathogenesis of recurrent embolic
Figure 3. (A and B) X-ray images of cervical
spine with retroflexion (A) and anteflexion (B).
(C and D) Representative Doppler images of
carotid duplex ultrasonography of the left VA,
showing a normal flow pattern in the
mid-cervical position (C) and an occluded flow
pattern with cervical anteflexion (D). (E and
F) Cerebral angiography shows occlusion of the
left VA at the C1-C2 level (arrow) and collateral
circulation bridges the distal part of the left VA
(arrowheads) (E). On cervical anteflexion, blood
flow of the left VA and PICA is significantly
reduced (arrows) (F).
T. KUROKI ET AL.e680
strokes in the present case. In patients with cerebrovascu-
lar accidents associated with AAS, physicians should be
aware of the presence of chronic occlusion of the vertebral
artery, and dynamic carotid duplex ultrasonography and
cerebral angiography with cervical anteflexion may be
helpful to assess vertebrobasilar artery hemodynamics
and to prevent further stroke recurrence.
References
1. Riise T, Jacobsen BK, Gran JT, et al. Total mortality is in-creased in rheumatoid arthritis. A 17-year prospectivestudy. Clin Rheumatol 2001;20:123-127.
2. Anderson ST. Mortality in rheumatoid arthritis: do ageand gender make a difference? Semin Arthritis Rheum1996;25:291-296.

RECURRENT EMBOLIC STROKES AND ATLANTOAXIAL SUBLUXATION e681
3. Halla JT, Hardin JG, Vitek J, et al. Involvement of the cer-vical spine in rheumatoid arthritis. Arthritis Rheum 1989;32:652-659.
4. Nakamura K, Saku Y, Torigoe R, et al. Sonographic detec-tion of haemodynamic changes in a case of vertebrobasi-lar insufficiency. Neuroradiology 1998;40:164-166.
5. Miele VJ, France JC, Rosen CL. Subaxial positional verte-bral artery occlusion corrected by decompression and fu-sion. Spine 2008;33:E366-E370.
6. Kuether TA, Nesbit GM, Clark WM, et al. Rotational ver-tebral artery occlusion: a mechanism of vertebrobasilarinsufficiency. Neurosurgery 1997;41:427-432.
7. Jones MW, Kaufmann JC. Vertebrobasilar artery insuffi-ciency in rheumatoid atlantoaxial subluxation. J NeurolNeurosurg Psychiatry 1976;39:122-128.
8. Robinson BP, Seeger JF, Zak SM. Rheumatoid arthritisand positional vertebrobasilar insufficiency. Case report.J Neurosurg 1986;65:111-114.
9. Toyota S, Wakayama A, Fujimoto Y, et al. Dissecting an-eurysm of the radiculomedullary artery originatingfrom extracranial vertebral artery dissection in a patientwith rheumatoid cervical spine disease: an unusual cause
of subarachnoid hemorrhage. Case report. J NeurosurgSpine 2007;7:660-663.
10. Macchi C, Catini C. The anatomy and clinical impor-tance of the collateral circles between the vertebral ar-teries and the cervical, costo-cervical, and occipitalbranches in 52 living subjects. Ital J Anat Embryol1993;98:153-163.
11. Kang HS, Han MH, Kim SH, et al. Anterior spinal arteryas a collateral channel in cases of bilateral vertebral arte-rial steno-occlusive diseases. Am J Neuroradiol 2007;28:222-225.
12. ZenmyoM, Ijiri K, Sasaki H, et al. Magnetic resonance an-giography for vertebral artery evaluation in rheumatoidarthritis patients. Neurosurgery 2010;66:1174-1180.
13. Howell SJ, Molyneux AJ. Vertebrobasilar insufficiency inrheumatoid atlanto-axial subluxation: a case report withangiographic demonstration of left vertebral artery occlu-sion. J Neurol 1988;235:189-190.
14. Caplan LR, Hennerici M. Impaired clearance of emboli(washout) is an important link between hypoperfusion,embolism, and ischemic stroke. Arch Neurol 1998;55:1475-1482.