recent trends
DESCRIPTION
recent trendsTRANSCRIPT

UNIT VRECENT TRENDS AND ELECTRICAL SAFETY
Principles of thermography, detecting circuits, it’s application in medicine, principles of cryogenic techniques, it’s application in medicine, principles of fibre optic cable, endoscopy, laproscopy, opthalmic equipments, macro and micro shock, sources of shock, monitoring and interrupting circuit from leakage current, earthing scheme.
Principles of thermography
Infrared thermography (IRT), thermal imaging, and thermal video are examples of infrared imaging science. Thermal imaging cameras detect radiation in the infrared range of the electromagnetic spectrum (roughly 9,000–14,000 nanometers or 9–14 µm) and produce images of that radiation, called thermograms. Since infrared radiation is emitted by all objects above absolute zero according to the black body radiation law, thermography makes it possible to see one's environment with or without visible illumination. The amount of radiation emitted by an object increases with temperature; therefore, thermography allows one to see variations in temperature. When viewed through a thermal imaging camera, warm objects stand out well against cooler backgrounds; humans and other warm-blooded animals become easily visible against the environment, day or night. As a result, thermography is particularly useful to military and other users of surveillance cameras.Thermography has a long history, although its use has increased dramatically with the commercial and industrial applications of the past fifty years. Government and airport personnel used thermography to detect suspected swine flu cases during the 2009 pandemic. Firefighters use thermography to see through smoke, to find persons, and to localize the base of a fire. Maintenance technicians use thermography to locate overheating joints and sections of power lines, which are a sign of impending failure. Building construction technicians can see thermal signatures that indicate heat leaks in faulty thermal insulation and can use the results to improve the efficiency of heating and air-conditioning units. Some physiological changes in human beings and other warm-blooded animals can also be monitored with thermal imaging during clinical diagnostics.
Thermogram of a cat

The appearance and operation of a modern thermographic camera is often similar to a camcorder. Often the live thermogram reveals temperature variations so clearly that a photograph is not necessary for analysis. A recording module is therefore not always built-in.Non-specialized CCD and CMOS sensors have most of their spectral sensitivity in the visible light wavelength range. However by utilizing the "trailing" area of their spectral sensitivity, namely the part of the infrared spectrum called near-infrared (NIR), and by using off-the-shelf CCTV camera it is possible under certain circumstances to obtain true thermal images of objects with temperatures at about 280°C and higher. Specialized thermal imaging cameras use focal plane arrays (FPAs) that respond to longer wavelengths (mid- and long-wavelength infrared). The most common types are InSb, InGaAs, HgCdTe and QWIP FPA. The newest technologies use low-cost, uncooled microbolometers as FPA sensors. Their resolution is considerably lower than that of optical cameras, mostly 160x120 or 320x240 pixels, up to 640x512 for the most expensive models. Thermal imaging cameras are much more expensive than their visible-spectrum counterparts, and higher-end models are often export-restricted due to the military uses for this technology. Older bolometers or more sensitive models such as InSb require cryogenic cooling, usually by a miniature Stirling cycle refrigerator or liquid nitrogen.
Thermal EnergyThermal images, or thermograms, are actually visual displays of the amount of infrared energy emitted, transmitted, and reflected by an object. Because there are multiple sources of the infrared energy, it is difficult to get an accurate temperature of an object using this method. A thermal imaging camera is capable of performing algorithms to interpret that data and build an image. Although the image shows the viewer an approximation of the temperature at which the object is operating, the camera is actually using multiple sources of data based on the areas surrounding the object to determine that value rather than detecting the actual temperature. This phenomenon may become clearer upon consideration of the formula Incident Energy = Emitted Energy + Transmitted Energy + Reflected
EnergyWhere Incident Energy is the energy profile when viewed through a thermal imaging camera. Emitted Energy is generally what is intended to be measured. Transmitted Energy is the energy that passes through the subject from a remote thermal source. Reflected Energy is the amount of energy that reflects off the surface of the object from a remote thermal source.If the object is radiating at a higher temperature than its surroundings, then power transfer will be taking place and power will be radiating from warm to cold following the principle stated in the Second Law of Thermodynamics. So if there is a cool area in the thermogram, that object will be absorbing the radiation emitted by the warm object. The ability of both objects to emit or
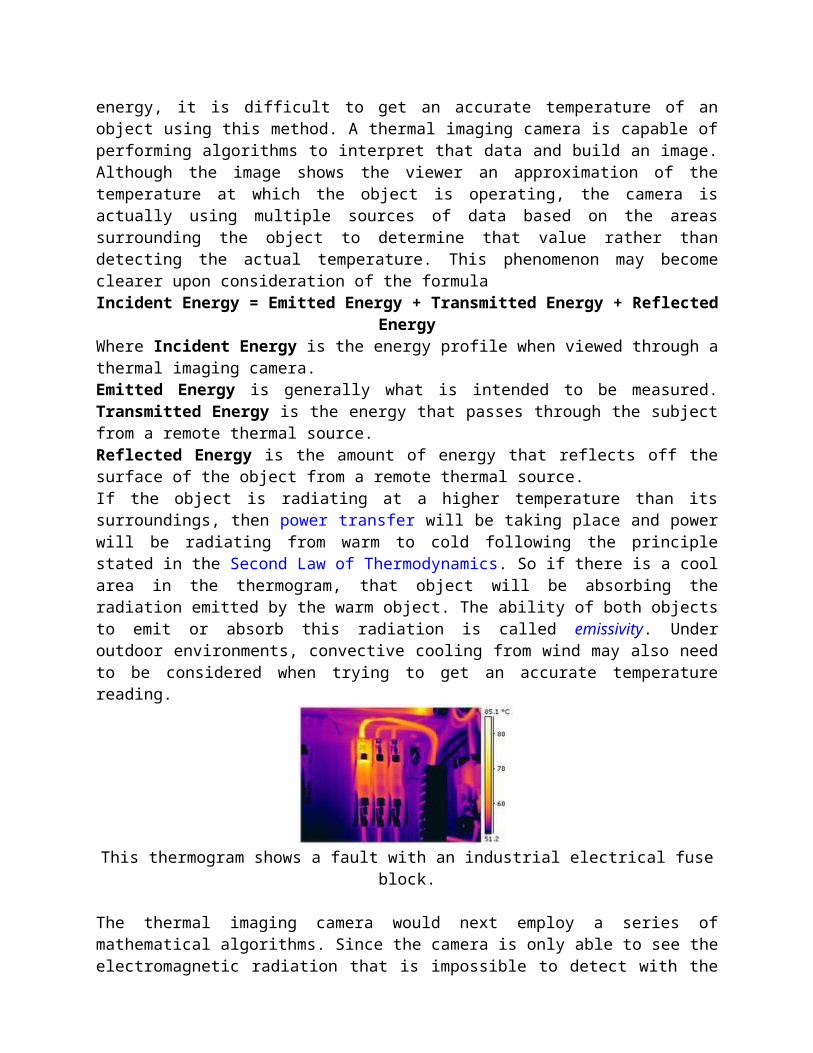
absorb this radiation is called emissivity. Under outdoor environments, convective cooling from wind may also need to be considered when trying to get an accurate temperature reading.
This thermogram shows a fault with an industrial electrical fuse block.
The thermal imaging camera would next employ a series of mathematical algorithms. Since the camera is only able to see the electromagnetic radiation that is impossible to detect with the human eye, it will build a picture in the viewer and record a visible picture, usually in a JPG format.In order to perform the role of noncontact temperature recorder, the camera will change the temperature of the object being viewed with its emissivity setting. Other algorithms can be used to affect the measurement, including the transmission ability of the transmitting medium (usually air) and the temperature of that transmitting medium. All these settings will affect the ultimate output for the temperature of the object being viewed. This functionality makes the thermal imaging camera an excellent tool for the maintenance of electrical and mechanical systems in industry and commerce. By using the proper camera settings and by being careful when capturing the image, electrical systems can be scanned and problems can be found. Faults with steam traps in steam heating systems are easy to locate.In the energy savings area, the thermal imaging camera can do more. Because it can see the radiating temperature of an object as well as what that object is radiating at, the product of the radiation can be calculated using the Stefan–Boltzmann constant.
EmissivityEmissivity is a term representing a material's ability to emit thermal radiation. Each material has a different emissivity, and it can be difficult to determine the appropriate emissivity for a subject. A material's emissivity can range from a theoretical 0.00 (completely not-emitting) to an equally-theoretical 1.00 (completely emitting); the emissivity often varies with temperature. An example of a substance with low emissivity would be silver, with an emissivity coefficient of .02. An example of a substance with high emissivity would be asphalt, with an emissivity coefficient of .98.A black body is a theoretical object which will radiate infrared radiation at its contact temperature. If a thermocouple on a black body radiator reads 50 °C, the radiation the black body will give up will also be 50 °C. Therefore a true black body will have an emissivity of 1.

Thermogram of a snake held by a humanSince there is no such thing as a perfect black body, the infrared radiation of normal objects will appear to be less than the contact temperature. The rate (percentage) of emission of infrared radiation will thus be a fraction of the true contact temperature. This fraction is called emissivity.Some objects have different emissivities in long wave as compared to mid wave emissions. Emissivities may also change as a function of temperature in some materials. To make a temperature measurement of an object, the thermographer will refer to the emissivity table to choose the emissivity value of the object, which is then entered into the camera. The camera's algorithm will correct the temperature by using the emissivity to calculate a temperature that more closely matches the actual contact temperature of the object.If possible, the thermographer would try to test the emissivity of the object in question. This would be more accurate than attempting to determine the emissivity of the object via a table. The usual method of testing the emissivity is to place a material of known high emissivity in contact with the surface of the object. The material of known emissivity can be as complex as industrial emissivity spray which is produced specifically for this purpose, or it can be as simple as standard black insulation tape, emissivity 0.97. A temperature reading can then be taken of the object with the emissivity level on the imager set to the value of the test material. This will give an accurate value of the temperature of the object. The temperature can then be read on a part of the object not covered with the test material. If the temperature reading is different, the emissivity level on the imager can be adjusted until the object reads the same temperature. This will give the thermographer a much more accurate emissivity reading. There are times, however, when an emissivity test is not possible due to dangerous or inaccessible conditions. In these situations the thermographer must rely on tables.
Difference between infrared film and thermographyIR film is sensitive to infrared (IR) radiation in the 250°C to 500°C range, while the range of thermography is approximately -50°C to over 2,000°C. So, for an IR film to work thermographically, it must be over 250°C or be reflecting infrared radiation from something that is at least that hot. (Usually, infrared photographic film is used in conjunction with an IR illuminator, which is a filtered incandescent source or IR diode illuminator, or else with an IR flash (usually a xenon flash that is IR filtered). These correspond with "active" near-IR modes as discussed in the next section.

Night vision infrared devices image in the near-infrared, just beyond the visual spectrum, and can see emitted or reflected near-infrared in complete visual darkness. However, again, these are not usually used for thermography due to the high temperature requirements, but are instead used with active near-IR sources.Starlight-type night vision devices generally only magnify ambient light.
Passive vs. active thermographyAll objects above the absolute zero temperature (0 K) emit infrared radiation. Hence, an excellent way to measure thermal variations is to use an infrared vision device, usually a focal plane array (FPA) infrared camera capable of detecting radiation in the mid (3 to 5 μm) and long (7 to 14 μm) wave infrared bands, denoted as MWIR and LWIR, corresponding to two of the high transmittance infrared windows. Abnormal temperature profiles at the surface of an object are an indication of a potential problem.
Thermal imaging camera & screen.Thermal imaging can detect elevated body temperature, one of the signs of the virus H1N1 (Swine influenza).In passive thermography, the features of interest are naturally at a higher or lower temperature than the background. Passive thermography has many applications such as surveillance of people on a scene and medical diagnosis (specifically thermology).In active thermography, an energy source is required to produce a thermal contrast between the feature of interest and the background. The active approach is necessary in many cases given that the inspected parts are usually in equilibrium with the surroundings.
Advantages of thermography It shows a visual picture so temperatures over a large area can be
compared It is capable of catching moving targets in real time It is able to find deteriorating, i.e., higher temperature components
prior to their failure It can be used to measure or observe in areas inaccessible or
hazardous for other methods It is a non-destructive test method

It can be used to find defects in shafts, pipes, and other metal or plastic parts
It can be used to detect objects in dark areas It has some medical application, essentially in kinesiotherapy
Limitations and disadvantages of thermography Quality cameras often have a high price range (often US$ 3,000 or
more), cheaper are only 40x40 up to 120x120 pixels Images can be difficult to interpret accurately when based upon certain
objects, specifically objects with erratic temperatures, although this problem is reduced in active thermal imaging
Accurate temperature measurements are hindered by differing emissivities and reflections from other surfaces
Most cameras have ±2% accuracy or worse in measurement of temperature and are not as accurate as contact methods
Only able to directly detect surface temperatures Condition of work, depending of the case, can be drastic: 10°C of
difference between internal/external, 10km/h of wind maximum, no direct sun, no recent rain,
Applications
Kite aerial thermogram of the site of Ogilface Castle, Scotland. Condition monitoring Digital infrared thermal imaging in health care Medical imaging Infrared mammography Archaeological Kite Aerial Thermography: Kite_aerial_photography Thermology Veterinary Thermal Imaging Night vision UAV Surveillance Stereo vision Research Process control Nondestructive testing Surveillance in security, law enforcement and defence Chemical imaging Volcanology Building

Thermal imaging cameras convert the energy in the infrared wavelength into a visible light display. All objects above absolute zero emit thermal infrared energy, so thermal cameras can passively see all objects, regardless of ambient light. However, most thermal cameras only see objects warmer than -50°C.The spectrum and amount of thermal radiation depend strongly on an object's surface temperature. This makes it possible for a thermal imaging camera to display an object's temperature. However, other factors also influence the radiation, which limits the accuracy of this technique. For example, the radiation depends not only on the temperature of the object, but is also a function of the emissivity of the object. Also, radiation originates from the surroundings and is reflected in the object, and the radiation from the object and the reflected radiation will also be influenced by the absorption of the atmosphere.
StandardsInternational Organization for Standardization (ISO)
ISO 6781, Thermal insulation - Qualitative detection of thermal irregularities in building envelopes - Infrared method
ISO 18434-1, Condition monitoring and diagnostics of machines - Thermography - Part 1: General procedures
ISO 18436-7, Condition monitoring and diagnostics of machines - Requirements for qualification and assessment of personnel - Part 7: Thermography
Biological counterpartThermography by definition is by means of an instrument (artifact), but some living creatures have natural organs that function as counterparts to bolometers, and thus possess a crude type of thermal imaging capability (thermoception). One of the best known examples is infrared sensing in snakes.
Principles of cryogenic techniques and its application in medicine
In physics, cryogenics is the study of the production of very low temperature (below −150 °C, −238 °F or 123 K) and the behavior of materials at those temperatures. A person who studies elements that have been subjected to extremely cold temperatures is called a cryogenicist. Rather than the relative temperature scales of Celsius and Fahrenheit, cryogenicists use the absolute temperature scales. These are Kelvin (SI units) or Rankine scale (Imperial & US units).Cryogenics is the study and use of materials at extremely low temperatures. Such low temperatures cause changes in the physical properties of materials that allow them to be used in unusual engineering, industrial, and medical applications. For example, in the cryogenic temperature range, air becomes a liquid—or even a solid—and living tissue freezes instantly. Matter behaves strangely at the lowest temperatures of the cryogenic range. Electric

currents never stop flowing, liquids run uphill, and rubber becomes as brittle as glass. In medicine, cryogenic cooling is used in some diagnostic techniques, such as magnetic resonance imaging (MRI). Cryosurgery uses liquid nitrogen to kill unhealthy tissue by freezing it. Cryogenics is expected to play an important role in the development of better procedures for preserving human organs for transplant.
Definitions and distinctionsCryogenicsThe branches of physics and engineering that involve the study of very low temperatures, how to produce them, and how materials behave at those temperatures.CryobiologyThe branch of biology involving the study of the effects of low temperatures on organisms (most often for the purpose of achieving cryopreservation).CryosurgeryThe branch of surgery applying very low temperatures (down to -196 °C) to destroy malignant tissue, e.g. cancer cells.CryonicsThe emerging medical technology of cryopreserving humans and animals with the intention of future revival. Researchers in the field seek to apply the results of many sciences, including cryobiology, cryogenics, rheology, emergency medicine, etc.CryoelectronicsThe field of research regarding superconductivity at low temperatures.CryotronicsThe practical application of cryoelectronics.
EtymologyThe word cryogenics stems from Greek and means "the production of freezing cold"; however, the term is used today as a synonym for the low-temperature state. It is not well-defined at what point on the temperature scale refrigeration ends and cryogenics begins, but most scientists assume it starts at or below -150 °C or 123 K (about -240 °F). The National Institute of Standards and Technology at Boulder, Colorado has chosen to consider the field of cryogenics as that involving temperatures below −180 °C (-292 °F or 93.15 K). This is a logical dividing line, since the normal boiling points of the so-called permanent gases (such as helium, hydrogen, neon, nitrogen, oxygen, and normal air) lie below −180 °C while the Freon refrigerants, hydrogen sulfide, and other common refrigerants have boiling points above −180 °C.
Industrial application

Cryogenic valveLiquefied gases, such as liquid nitrogen and liquid helium, are used in many cryogenic applications. Liquid nitrogen is the most commonly used element in cryogenics and is legally purchasable around the world. Liquid helium is also commonly used and allows for the lowest attainable temperatures to be reached.These liquids are held in either special containers known as Dewar flasks, which are generally about six feet tall (1.8 m) and three feet (91.5 cm) in diameter, or giant tanks in larger commercial operations. Dewar flasks are named after their inventor, James Dewar, the man who first liquefied hydrogen. Museums typically display smaller vacuum flasks fitted in a protective casing.Cryogenic transfer pumps are the pumps used on LNG piers to transfer liquefied natural gas from LNG carriers to LNG storage tanks, as are cryogenic valves.
Cryogenic processingThe field of cryogenics advanced during World War II when scientists found that metals frozen to low temperatures showed more resistance to wear. Based on this theory of cryogenic hardening, the commercial cryogenic processing industry was founded in 1966 by Ed Busch. With a background in the heat treating industry, Busch founded a company in Detroit called CryoTech in 1966. They originally experimented with the possibility of increasing the life of metal tools to anywhere between 200%-400% of the original life expectancy using cryogenic tempering instead of heat treating. This evolved in the late 1990s into the treatment of other parts (that did more than just increase the life of a product) such as amplifier valves (improved sound quality), baseball bats (greater sweet spot), golf clubs (greater sweet spot), racing engines (greater performance under stress), firearms (less warping after continuous shooting), knives, razor blades, brake rotors and even pantyhose. The theory was based on how heat-treating metal works (the temperatures are lowered to room temperature from a high degree causing certain strength increases in the molecular structure to occur) and supposed that continuing the descent would allow for further strength increases. Using liquid nitrogen, CryoTech formulated the first early version of the cryogenic processor. Unfortunately for the newly born industry, the results were unstable, as components sometimes experienced thermal shock when they were cooled too quickly. Some components in early tests even shattered because of the ultra-low temperatures. In the late

twentieth century, the field improved significantly with the rise of applied research, which coupled microprocessor based industrial controls to the cryogenic processor in order to create more stable results.Cryogens, like liquid nitrogen, are further used for specialty chilling and freezing applications. Some chemical reactions, like those used to produce the active ingredients for the popular statin drugs, must occur at low temperatures of approximately −100°C (about -148°F). Special cryogenic chemical reactors are used to remove reaction heat and provide a low temperature environment. The freezing of foods and biotechnology products, like vaccines, requires nitrogen in blast freezing or immersion freezing systems. Certain soft or elastic materials become hard and brittle at very low temperatures, which makes cryogenic milling (cryomilling) an option for some materials that cannot easily be milled at higher temperatures.Cryogenic processing is not a substitute for heat treatment, but rather an extension of the heating - quenching - tempering cycle. Normally, when an item is quenched, the final temperature is ambient. The only reason for this is that most heat treaters do not have cooling equipment. There is nothing metallurgically significant about ambient temperature. The cryogenic process continues this action from ambient temperature down to −320 °F (140 °R; 78 K; −196 °C). In most instances the cryogenic cycle is followed by a heat tempering procedure. As all alloys do not have the same chemical constituents, the tempering procedure varies according to the material's chemical composition, thermal history and/or a tool's particular service application.The entire process takes 3–4 days.
FuelsAnother use of cryogenics is cryogenic fuels. Cryogenic fuels, mainly liquid hydrogen, have been used as rocket fuels. Liquid oxygen is used as an oxidizer of hydrogen, but oxygen is not, strictly speaking, a fuel. For example, NASA's workhorse space shuttle used cryogenic hydrogen/oxygen propellant as its primary means of getting into orbit, and all of the rockets built for the Soviet space program by Sergei Korolev used liquid oxygen as their oxidizer.Russian aircraft manufacturer Tupolev developed a version of its popular design Tu-154 with a cryogenic fuel system, known as the Tu-155. The plane uses a fuel referred to as liquefied natural gas or LNG, and made its first flight in 1989.
ApplicationsSome applications of cryogenics: Magnetic resonance imaging (MRI)MRI is a method of imaging objects that uses a strong magnetic field to detect the relaxation of protons that have been perturbed by a radio-frequency pulse. This magnetic field is generated by electromagnets, and high field strengths can be achieved by using superconducting magnets. Traditionally, liquid helium is used to cool the coils because it has a boiling

point of around 4 K at ambient pressure, and cheap metallic superconductors can be used for the coil wiring. So-called high-temperature superconducting compounds can be made to superconduct with the use of liquid nitrogen which boils at around 77 K. Electric power transmission In big cities It is difficult to transmit power by overhead cables in big cities, so underground cables are used. But underground cables get heated and the resistance of the wire increases leading to waste of power. Superconductors could be used to increase power throughput, although they would require cryogenic liquids such as nitrogen or helium to cool special alloy-containing cables to increase power transmission. Several feasibility studies have been performed and the field is the subject of an agreement within the International Energy Agency.
Cryogenic gases delivery truck at a supermarket Frozen food
Cryogenic gases are used in transportation of large masses of frozen food. When very large quantities of food must be transported to regions like war zones, earthquake hit regions, etc., they must be stored for a long time, so cryogenic food freezing is used. Cryogenic food freezing is also helpful for large scale food processing industries. Forward looking infrared (FLIR)
Many infra-red cameras require their detectors to be cryogenically cooled. Blood banking Certain rare blood groups are stored at low temperatures, such as -165 °C.
ProductionCryogenic cooling of devices and material is usually achieved via the use of liquid nitrogen, liquid helium, or a cryocompressor (which uses high pressure helium lines). Newer devices such as pulse cryocoolers and Stirling cryocoolers have been devised. The most recent development in cryogenics is the use of magnets as regenerators as well as refrigerators. These devices work on the principle known as the magnetocaloric effect.
DetectorsCryogenic temperatures, usually well below 77 K (−196 °C) are required to operate cryogenic detectors.
Cryosurgery In 1961 American surgeon Irving S. Cooper introduced a freezing technique called cryosurgery. Cryosurgery is relatively bloodless because the low temperatures used constrict the blood vessels, stemming the flow. Special instruments are used that have freezing tips to kill the damaged tissue and

shields to protect surrounding tissue. Cooper used cryosurgery to freeze and destroy damaged tissue in the brains of patients with Parkinson's disease (a degenerative illness). Since then, cryosurgery has found many applications. It is used to repair detached retinas and to remove cataracts. It is also used to treat liver cancer and prostate cancer. Cryosurgery is also widely used in the fields of dermatology, gynecology, plastic surgery, orthopedics, and podiatry. Cryosurgery has also been used successfully for more than 30 years in veterinary medicine.
Endoscopy, Laproscopy, Opthalmic Equipments
Endoscopy means looking inside and typically refers to looking inside the body for medical reasons using an endoscope, an instrument used to examine the interior of a hollow organ or cavity of the body. Unlike most other medical imaging devices, endoscopes are inserted directly into the organ. Endoscopy can also refer to using a borescope in technical situations where direct line of-sight observation is not feasible.
ComponentsAn endoscope can consist of
a rigid or flexible tube a light delivery system to illuminate the organ or object under
inspection. The light source is normally outside the body and the light is typically directed via an optical fiber system
a lens system transmitting the image from the objective lens to the viewer, typically a relay lens system in the case of rigid endoscopes or a bundle of fiberoptics in the case of a fiberscope
an eyepiece an additional channel to allow entry of medical instruments or
manipulators.
IndicationsA health care provider may use endoscopy for any of the following:
investigation of symptoms, such as symptoms in the digestive system including nausea, vomiting, abdominal pain, difficulty swallowing and gastrointestinal bleeding
confirmation of a diagnosis, most commonly by performing a biopsy to check for conditions such as anemia, bleeding, inflammation, cancers of the digestive system.
giving treatment, such as cauterization of a bleeding vessel, widening a narrow esophagus, clipping off a polyp or removing a foreign object
Specialty professional organizations which specialize in digestive problems advise that many patients with Barrett's esophagus are too frequently receiving endoscopies. Such societies recommend that patients with Barrett's esophagus and no cancer symptoms after two biopsies receive biopsies as indicated and no more often than the recommended rate.

Applications
An anoscope, a proctoscope, and a rectoscope with approximate lengths.
Endoscopy SurgeryHealth care providers can use endoscopy to review any of the following body parts:
The gastrointestinal tract (GI tract): o oesophagus , stomach and duodenum
(esophagogastroduodenoscopy)o small intestine (enteroscopy)o large intestine /colon (colonoscopy, sigmoidoscopy)o Magnification endoscopy o bile duct
endoscopic retrograde cholangiopancreatography (ERCP), duodenoscope-assisted cholangiopancreatoscopy, intraoperative cholangioscopy
o rectum (rectoscopy) and anus (anoscopy), both also referred to as (proctoscopy)
The respiratory tract o The nose (rhinoscopy)o The lower respiratory tract (bronchoscopy)
The ear (otoscope) The urinary tract (cystoscopy) The female reproductive system (gynoscopy)
o The cervix (colposcopy)o The uterus (hysteroscopy)o The fallopian tubes (falloposcopy)
Normally closed body cavities (through a small incision): o The abdominal or pelvic cavity (laparoscopy)o The interior of a joint (arthroscopy)o Organs of the chest (thoracoscopy and mediastinoscopy)
During pregnancy o The amnion (amnioscopy)o The fetus (fetoscopy)
Plastic Surgery Panendoscopy (or triple endoscopy)
o Combines laryngoscopy, esophagoscopy, and bronchoscopy

Orthopedic surgery o Hand Surgery , such as endoscopic carpal tunnel releaseo Epidural space (Epiduroscopy)o Bursae (Bursectomy)
Endodontic surgery o Maxillary sinus surgeryo Apicoectomy
Non-medical uses for endoscopy o The planning and architectural community have found the
endoscope useful for pre-visualization of scale models of proposed buildings and cities (architectural endoscopy)
o Internal inspection of complex technical systems (borescope)o Endoscopes are also a tool helpful in the examination of
improvised explosive devices by bomb disposal personnel.o The FBI uses endoscopes for conducting surveillance via tight
spaces.An Endoscopy is a simple procedure which allows a doctor to look inside human bodies using an instrument called an endoscope. A cutting tool can be attached to the end of the endoscope, and the apparatus can then be used to perform surgery. This type of surgery is called Key hole surgery, and usually leaves only a tiny scar externally.
HistoryThe first endoscope was developed in 1806 by Philipp Bozzini in Mainz with his introduction of a "Lichtleiter" (light conductor) "for the examinations of the canals and cavities of the human body". However, the Vienna Medical Society disapproved of such curiosity.. The use of electric light was a major step in the improvement of endoscopy. The first such lights were external. Later, smaller bulbs became available making internal light possible, for instance in a hysteroscope by Charles David in 1908. Hans Christian Jacobaeus has been given credit for early endoscopic explorations of the abdomen and the thorax with laparoscopy (1912) and thoracoscopy (1910). Laparoscopy was used in the diagnosis of liver and gallbladder disease by Heinz Kalk in the 1930s. Hope reported in 1937 on the use of laparoscopy to diagnose ectopic pregnancy. In 1944, Raoul Palmer placed his patients in the Trendelenburg position after gaseous distention of the abdomen and thus was able to reliably perform gynecologic laparoscopy.
Wolf and StorzGeorg Wolf (1873–1938) a Berlin manufacturer of rigid endoscopes, established in 1906, produced the Sussmann flexible gastroscope in 1911(Modlin,Farhadi-Journal of Clinical Gastroenterology, 2000). Karl Storz began producing instruments for ENT specialists in 1945. His intention was to develop instruments which would enable the practitioner to look inside the human body. The technology available at the end of the Second World War was still very modest: The area under examination in the interior of the human body was illuminated with miniature electric lamps; alternatively,

attempts were made to reflect light from an external source into the body through the endoscopic tube. Karl Storz pursued a plan: He set out to introduce very bright, but cold light into the body cavities through the instrument, thus providing excellent visibility while at the same time allowing objective documentation by means of image transmission. With more than 400 patents and operative samples to his name, which were to play a major role in showing the way ahead, Karl Storz played a crucial role in the development of endoscopy. It was however, the combination of his engineering skills and vision, coupled with the work of optical designer Harold Hopkins that ultimately would revolutionize the field of medical optics.
Use of fiber opticsFernando Alves Martins of Portugal invented the first fiber optic endoscope in 1963-64. Earlier in the 1950s Harold Hopkins had designed a “fibroscope” consisting of a bundle of flexible glass fibres able to coherently transmit an image. This proved useful both medically and industrially, and subsequent research led to further improvements in image quality. Further innovations included using additional fibres to channel light to the objective end from a powerful external source, thereby achieving the high level of full spectrum illumination that was needed for detailed viewing, and colour photography. The previous practice of a small filament lamp on the tip of the endoscope had left the choice of either viewing in a dim red light or increasing the light output - which carried the risk of burning the inside of the patient. Alongside the advances to the optical side, the ability to 'steer' the tip was developed, as well as innovations in remotely operated surgical instruments contained within the body of the endoscope itself. This was the beginning of "key-hole surgery" as we know it today.
Rod-lens endoscopesThere were physical limits to the image quality of a fibroscope. A bundle of say 50,000 fibers gives effectively only a 50,000-pixel image, and continued flexing from use breaks fibers and so progressively loses pixels. Eventually so many are lost that the whole bundle must be replaced (at considerable expense). Hopkins realised that any further optical improvement would require a different approach. Previous rigid endoscopes suffered from low light transmittance and poor image quality. The surgical requirement of passing surgical tools as well as the illumination system within the endoscope's tube - which itself is limited in dimensions by the human body - left very little room for the imaging optics. The tiny lenses of a conventional system required supporting rings that would obscure the bulk of the lens area; they were difficult to manufacture and assemble and optically nearly useless.The elegant solution that Hopkins produced (in the late 1960s) was to fill the air-spaces between the 'little lenses' with rods of glass. These fitted exactly the endoscope's tube, making them self-aligning, and required no other

support. This allowed the little lenses to be dispensed with altogether. The rod-lenses were much easier to handle and used the maximum possible diameter available. With the appropriate curvature and coatings to the rod ends and optimal choices of glass-types, all calculated and specified by Hopkins, the image quality was transformed - even with tubes of only 1mm in diameter. With a high quality 'telescope' of such small diameter the tools and illumination system could be comfortably housed within an outer tube. Once again it was Karl Storz who produced the first of these new endoscopes as part of a long and productive partnership between the two men.Whilst there are regions of the body that will always require flexible endoscopes (principally the gastrointestinal tract), the rigid rod-lens endoscopes have such exceptional performance that they are still the preferred instrument and have enabled modern key-hole surgery. (Harold Hopkins was recognized and honoured for his advancement of medical-optic by the medical community worldwide. It formed a major part of the citation when he was awarded the Rumford Medal by the Royal Society in 1984.)
ApplicationBy measuring absorption of light by the blood (by passing the light through one fibre and collecting the light through another fibre) we can estimate the proportion of haemoglobin in the blood and diagnose ulceration in the stomach.
DisinfectionDisinfection is essential for all types of endoscopes. The first disinfection device was constructed by S.E.Miederer in 1976 at the University of Bonn in Germany.
RisksInfection and over-sedationThe main risks are perforation, or a tear, of the stomach or oesophagus lining and bleeding. Although perforation generally requires surgery, certain cases may be treated with antibiotics and intravenous fluids. Bleeding may occur at the site of a biopsy or polyp removal. Such typically minor bleeding may simply stop on its own or be controlled by cauterisation. Seldom does surgery become necessary.Perforation and bleeding are rare during gastroscopy.Other minor risks include drug reactions and complications related to other diseases the patient may have. Consequently, patients should inform their doctor of all allergic tendencies and medical problems.Occasionally, the site of the sedative injection may become inflamed and tender for a short time. This is usually not serious and warm compresses for a few days are usually helpful.While any of these complications may possibly occur, it is good to remember that each of them occurs quite infrequently.A doctor can further discuss risks with the patient with regard to the particular need for gastroscopy.

After the endoscopyAfter the procedure the patient will be observed and monitored by a qualified individual in the endoscopy room or a recovery area until a significant portion of the medication has worn off. Occasionally the patient is left with a mild sore throat, which may respond to saline gargles, or chamomile tea. It may last for weeks or not happen at all. The patient may have a feeling of distention from the insufflated air that was used during the procedure. Both problems are mild and fleeting. When fully recovered, the patient will be instructed when to resume their usual diet (probably within a few hours) and will be allowed to be taken home. Because of the use of sedation, most facilities mandate that the patient be taken home by another person and that he or she not drive or handle machinery for the remainder of the day.
Recent developmentsWith the application of robotic systems, telesurgery was introduced as the surgeon could be at a site far removed from the patient. The first transatlantic surgery has been called the Lindbergh Operation.
Disposable endoscopyDisposable endoscopy is an emerging category of endoscopic instruments. Recent developments have allowed the manufacture of endoscopes cheap enough to be used on a single patient only. It is meeting a growing demand to lessen the risk of cross contamination and hospital acquired diseases. A European consortium of SME are working on the DUET project to build a disposable endoscope.
Capsule endoscopyMain article: Capsule endoscopyA new endoscopy technology uses a Magnetically Guided Capsule Endoscope (MGCE) for wireless control, monitor and imaging.
3D endoscopyAfter successful 12 years supply of 3D endoscopes for Robotic DaVinci system, recently Schoelly Fiberoptic GmbH launched 3D-HD Laparoscopy system.
Augmented RealityThe endoscopic image can be combined with other image sources to provide the surgeon with additional information. For instance the position of an anatomical structure or tumor might be shown in the endoscopic video.
Measuring endoscopyCurrent research works on the endoscopic collection of dimensional 3D-data, for instance using laser triangulation or the approach of structured light projection. Depending on the used optics technical inner geometries can be measured with accuracies in the low µm-area.

Laparoscopy (from Ancient Greek λαπάρα (lapara), meaning "flank, side", and σκοπέω (skopeó), meaning "to see") is an operation performed in the abdomen or pelvis through small incisions (usually 0.5–1.5 cm) with the aid of a camera. It can either be used to inspect and diagnose a condition or to perform surgery.
TypesThere are two types of laparoscope: (1) a telescopic rod lens system, that is usually connected to a video camera (single chip or three chip), or (2) a digital laparoscope where a miniature digital video camera is placed at the end of the laparoscope, eliminating the rod lens system.
SurgeryMain article: Laparoscopic surgeryThe laparoscope allows doctors to perform both minor and complex surgeries with a few small cuts in the abdomen. There are a number of advantages to the patient with laparoscopic surgery versus an open procedure. These include reduced pain due to smaller incisions and hemorrhaging, and shorter recovery time.
Gynecological diagnosisFurther information: FertiloscopeIn gynecology, diagnostic laparoscopy may be used to inspect the outside of the uterus, ovaries and fallopian tubes, for example in the diagnosis of female infertility. Usually, there is one incision near the navel and a second near to the pubic hairline.For gynecological diagnosis a special type of laparoscope can be used, called a fertiloscope. A fertiloscope is modified to make it suitable for trans-vaginal application.A dye test may be performed to detect any blockage in the reproductive tract, wherein a dark blue dye is passed up through the cervix and is followed with the laparoscope through its passage out into the fallopian tubes to the ovaries.
Pediatric laparoscopyAlthough laparoscopy in adult age group is widely accepted, its advantages in pediatric age group is questionable. The efficacy of laparoscopy is inferior to open surgery in situations such as pyloromyotomy for infantile hypertrophic pyloric stenosis. Although laparoscopic appendectomy results in less wounds than open surgery, the former is also associated with more intra-abdominal abscesses.
Laparoscopic surgery, also called minimally invasive surgery (MIS), bandaid surgery, or keyhole surgery, is a modern surgical technique in which

operations in the abdomen are performed through small incisions (usually 0.5–1.5 cm) as opposed to the larger incisions needed in laparotomy.Keyhole surgery makes use of images displayed on TV monitors to magnify the surgical elements.Laparoscopic surgery includes operations within the abdominal or pelvic cavities, whereas keyhole surgery performed on the thoracic or chest cavity is called thoracoscopic surgery. Laparoscopic and thoracoscopic surgery belong to the broader field of endoscopy.There are a number of advantages to the patient with laparoscopic surgery versus an open procedure. These include reduced pain due to smaller incisions and hemorrhaging, and shorter recovery time.The key element in laparoscopic surgery is the use of a laparoscope. There are two types: (1) a telescopic rod lens system, that is usually connected to a video camera (single chip or three chip), or (2) a digital laparoscope where the charge-coupled device is placed at the end of the laparoscope, eliminating the rod lens system. Also attached is a fiber optic cable system connected to a 'cold' light source (halogen or xenon), to illuminate the operative field, inserted through a 5 mm or 10 mm cannula or trocar to view the operative field. The abdomen is usually insufflated, or essentially blown up like a balloon, with carbon dioxide gas. This elevates the abdominal wall above the internal organs like a dome to create a working and viewing space. CO2 is used because it is common to the human body and can be absorbed by tissue and removed by the respiratory system. It is also non-flammable, which is important because electrosurgical devices are commonly used in laparoscopic procedures. Contents
1 History 2 Procedures 3 Advantages 4 Disadvantages 5 Risks 6 Robotics and technology 7 Non-robotic hand guided assistance systems 8 See also 9 References 10 External links
History

Hans Christian JacobaeusIt is difficult to credit one individual with the pioneering of the laparoscopic approach. In 1902, Georg Kelling, of Dresden, Germany, performed the first laparoscopic procedure in dogs and in 1910, Hans Christian Jacobaeus, of Sweden, reported the first laparoscopic operation in humans. In the ensuing several decades, numerous individuals refined and popularized the approach further for laparoscopy. The start of computer chip television camera was a seminal event in the field of laparoscopy. This technological innovation provided the means to project a magnified view of the operative field onto a monitor and, at the same time, freed both the operating surgeon's hands, thereby facilitating performance of complex laparoscopic procedures. Prior to its conception, laparoscopy was a surgical approach with very few applications, mainly for purposes of diagnosis and performance of simple procedures in gynecologic applications.The first publication on diagnostic laparoscopy by Raoul Palmer appeared in the early 1950s, followed by the publication of Frangenheim and Semm. Hans Lindermann and Kurt Semm practised CO2 hysteroscopy during the mid-1970s.In 1972, Clarke invented, published, patented, presented, and recorded on film laparoscopic surgery, with instruments marketed by the Ven Instrument Company of Buffalo, New York, USA. In 1975, Tarasconi, from the Department of Ob-Gyn of the University of Passo Fundo Medical School (Passo Fundo, RS, Brazil), started his experience with organ resection by laparoscopy (Salpingectomy), first reported in the Third AAGL Meeting, Hyatt Regency Atlanta, November 1976 and later published in The Journal of Reproductive Medicine in 1981. This laparoscopic surgical procedure was the first laparoscopic organ resection reported in medical literature.In 1981, Semm, from the Universitats Frauenklinik, Kiel, Germany, performed the first laparoscopic appendectomy. Following his lecture on laparoscopic appendectomy, the president of the German Surgical Society wrote to the Board of Directors of the German Gynecological Society suggesting suspension of Semm from medical practice. Subsequently, Semm submitted a paper on laparoscopic appendectomy to the American Journal of Obstetrics and Gynecology, at first rejected as unacceptable for publication on the grounds that the technique reported on was 'unethical,' but finally published in the journal Endoscopy. The abstract of his paper on endoscopic appendectomy can be found at here. Semm established several standard procedures that were regularly performed, such as ovarian cyst enucleation, myomectomy, treatment of ectopic pregnancy and finally laparoscopic-assisted vaginal hysterectomy (nowadays termed as cervical intra-fascial Semm hysterectomy). He also developed a medical instrument company Wisap in Munich, Germany, which still produces various endoscopic instruments of high quality. In 1985, he constructed the pelvi-trainer = laparo-trainer, a practical surgical model whereby colleagues could practice laparoscopic techniques. Semm published over 1000 papers in various journals.He also produced over 30 endoscopic films and more than 20,000

colored slides to teach and inform interested colleagues about his technique. His first atlas, More Details on Pelviscopy and Hysteroscopy was published in 1976, a slide atlas on pelviscopy, hysteroscopy, and fetoscopy in 1979, and his books on gynecological endoscopic surgery in German, English, and many other languages in 1984, 1987, and 2002.Prior to 1990, the only specialty performing laparoscopy on a widespread basis was gynecology, mostly for relatively short, simple procedures such as a diagnostic laparoscopy or tubal ligation. The introduction in 1990 of a laparoscopic clip applier with twenty automatically advancing clips (rather than a single load clip applier that would have to be taken out, reloaded and reintroduced for each clip application) made general surgeons more comfortable with making the leap to laparoscopic cholecystectomies (gall bladder removal). On the other hand, some surgeons continue to use the single clip appliers as they save as much as $200 per case for the patient, detract nothing from the quality of the clip ligation, and add only seconds to case lengths.
Procedures
Surgeons perform laparoscopic stomach surgery.Laparoscopic cholecystectomy is the most common laparoscopic procedure performed. In this procedure, 5-10mm diameter instruments (graspers, scissors, clip applier) can be introduced by the surgeon into the abdomen through trocars (hollow tubes with a seal to keep the CO2 from leaking). Over one million cholecystectomies are performed in the U.S. annually, with over 96% of those being performed laparoscopically.There are two different formats for laparoscopic surgery. Multiple incisions are required for technology such as the "Da Vinci" system, which uses a console located away from the patient, with the surgeon controlling a camera, vacuum pump, saline cleansing solution, cutting tools, etc. each located within its own incision site, but oriented toward the surgical objective. The surgeon uses two PlayStation-type controls to manipulate the devices.In contrast, requiring only a single small incision, the "Bonati system" (invented by Dr. Alfred Bonati), uses a single 5-function control, so that a saline solution and the vacuum pump operate together when the laser cutter is activated. A camera and light provide feedback to the surgeon, who sees the enlarged surgical elements on a TV monitor. The Bonati system was designed for spinal surgery and has been promoted only for that purpose.

Rather than a minimum 20 cm incision as in traditional (open) cholecystectomy, four incisions of 0.5–1.0 cm will be sufficient to perform a laparoscopic removal of a gallbladder. Since the gall bladder is similar to a small balloon that stores and releases bile, it can usually be removed from the abdomen by suctioning out the bile and then removing the deflated gallbladder through the 1 cm incision at the patient's navel. The length of postoperative stay in the hospital is minimal, and same-day discharges are possible in cases of early morning procedures.In certain advanced laparoscopic procedures where the size of the specimen being removed would be too large to pull out through a trocar site (as would be done with a gallbladder) an incision larger than 10mm must be made. The most common of these procedures are removal of all or part of the colon (colectomy), or removal of the kidney (nephrectomy). Some surgeons perform these procedures completely laparoscopically, making the larger incision toward the end of the procedure for specimen removal, or, in the case of a colectomy, to also prepare the remaining healthy bowel to be reconnected (create an anastomosis). Many other surgeons feel that since they will have to make a larger incision for specimen removal anyway, they might as well use this incision to have their hand in the operative field during the procedure to aid as a retractor, dissector, and to be able to feel differing tissue densities (palpate), as they would in open surgery. This technique is called hand-assist laparoscopy. Since they will still be working with scopes and other laparoscopic instruments, CO2 will have to be maintained in the patient's abdomen, so a device known as a hand access port (a sleeve with a seal that allows passage of the hand) must be used. Surgeons that choose this hand-assist technique feel it reduces operative time significantly versus the straight laparoscopic approach. It also gives them more options in dealing with unexpected adverse events (i.e. uncontrolled bleeding) that may otherwise require creating a much larger incision and converting to a fully open surgical procedure.Conceptually, the laparoscopic approach is intended to minimise post-operative pain and speed up recovery times, while maintaining an enhanced visual field for surgeons. Due to improved patient outcomes, in the last two decades, laparoscopic surgery has been adopted by various surgical sub-specialties including gastrointestinal surgery (including bariatric procedures for morbid obesity), gynecologic surgery and urology. Based on numerous prospective randomized controlled trials, the approach has proven to be beneficial in reducing post-operative morbidities such as wound infections and incisional hernias (especially in morbidly obese patients), and is now deemed safe when applied to surgery for cancers such as cancer of colon.

Laparoscopic instruments.The restricted vision, the difficulty in handling of the instruments (new hand-eye coordination skills are needed), the lack of tactile perception and the limited working area are factors which add to the technical complexity of this surgical approach. For these reasons, minimally invasive surgery has emerged as a highly competitive new sub-specialty within various fields of surgery. Surgical residents who wish to focus on this area of surgery gain additional laparoscopic surgery training during one or two years of fellowship after completing their basic surgical residency. In OBGYN residency programs, the average laparoscopy-to-laparotomy quotient (LPQ) is 0.55.The first transatlantic surgery (Lindbergh Operation) ever performed was a laparoscopic gallbladder removal.Laparoscopic techniques have also been developed in the field of veterinary medicine. Due to the relative high cost of the equipment required, however, it has not become commonplace in most traditional practices today but rather limited to specialty-type practices. Many of the same surgeries performed in humans can be applied to animal cases - everything from an egg-bound tortoise to a German Shepherd can benefit from MIS. A paper published in JAVMA (Journal of the American Veterinary Medical Association) in 2005 showed that dogs spayed laparoscopically experienced significantly less pain (65%)than those that were spayed with traditional 'open' methods. Arthroscopy, thoracoscopy, cystoscopy are all performed in veterinary medicine today. The University of Georgia School of Veterinary Medicine and Colorado State University's School of Veterinary Medicine are two of the main centers where veterinary laparoscopy got started and have excellent training programs for veterinarians interested in getting started in MIS.
AdvantagesThere are a number of advantages to the patient with laparoscopic surgery versus an open procedure. These include:
Reduced hemorrhaging, which reduces the chance of needing a blood transfusion.
Smaller incision, which reduces pain and shortens recovery time, as well as resulting in less post-operative scarring.
Less pain, leading to less pain medication needed. Although procedure times are usually slightly longer, hospital stay is
less, and often with a same day discharge which leads to a faster return to everyday living.
Reduced exposure of internal organs to possible external contaminants thereby reduced risk of acquiring infections.
Although laparoscopy in adult age group is widely accepted, its advantages in pediatric age group is questioned. Benefits of laparoscopy appears to recede with younger age. Efficacy of laparoscopy is inferior to open surgery in certain conditions such as pyloromyotomy for Infantile hypertrophic pyloric stenosis. Although laparoscopic appendectomy has lesser wound problems

than open surgery, the former is associated with more intra-abdominal abscesses.
DisadvantagesWhile laparoscopic surgery is clearly advantageous in terms of patient outcomes, the procedure is more difficult from the surgeon's perspective when compared to traditional, open surgery:
The surgeon has limited range of motion at the surgical site resulting in a loss of dexterity
Poor depth perception Surgeons must use tools to interact with tissue rather than manipulate
it directly with their hands. This results in an inability to accurately judge how much force is being applied to tissue as well as a risk of damaging tissue by applying more force than necessary. This limitation also reduces tactile sensation, making it more difficult for the surgeon to feel tissue (sometimes an important diagnostic tool, such as when palpating for tumors) and making delicate operations such as tying sutures more difficult.
The tool endpoints move in the opposite direction to the surgeon's hands due to the pivot point, making laparoscopic surgery a non-intuitive motor skill that is difficult to learn.
RisksSome of the risks are briefly described below:
The most significant risks are from trocar injuries to either blood vessels or small or large bowel. The risk of such injuries is increased in patients who have below average body mass index or have a history of prior abdominal surgery. The initial trocar is typically inserted blindly. While these injuries are rare, significant complications can occur. Vascular injuries can result in hemorrhage that may be life threatening. Injuries to the bowel can cause a delayed peritonitis. It is very important that these injuries be recognized as early as possible.
Some patients have sustained electrical burns unseen by surgeons who are working with electrodes that leak current into surrounding tissue. The resulting injuries can result in perforated organs and can also lead to peritonitis. This risk is eliminated by utilizing active electrode monitoring.
There may be an increased risk of hypothermia and peritoneal trauma due to increased exposure to cold, dry gases during insufflation. The use of heated and humidified CO2 may reduce this risk.
Many patients with existing pulmonary disorders may not tolerate pneumoperitoneum (gas in the abdominal cavity), resulting in a need for conversion to open surgery after the initial attempt at laparoscopic approach.
Not all of the CO2 introduced into the abdominal cavity is removed through the incisions during surgery. Gas tends to rise, and when a pocket of CO2 rises in the abdomen, it pushes against the diaphragm

(the muscle that separates the abdominal from the thoracic cavities and facilitates breathing), and can exert pressure on the phrenic nerve. This produces a sensation of pain that may extend to the patient's shoulders. For an appendectomy, the right shoulder can be particularly painful. In some cases this can also cause considerable pain when breathing. In all cases, however, the pain is transient, as the body tissues will absorb the CO2 and eliminate it through respiration.
Coagulation disorders and dense adhesions (scar tissue) from previous abdominal surgery may pose added risk for laparoscopic surgery and are considered relative contra-indications for this approach.
Robotics and technology
A laparoscopic robotic surgery machine.The process of minimally invasive surgery has been augmented by specialized tools for decades. For example, TransEnterix of Durham, North Carolina received U.S. Food and Drug Administration approval in October 2009 for its SPIDER Surgical System using flexible instruments and one incision in the navel area instead of several, allowing quicker healing for patients. Dr. Richard Stac of Duke University developed the process. In recent years, electronic tools have been developed to aid surgeons. Some of the features include:
Visual magnification — use of a large viewing screen improves visibility Stabilization — Electromechanical damping of vibrations, due to
machinery or shaky human hands

Simulators — use of specialized virtual reality training tools to improve physicians' proficiency in surgery
Reduced number of incisionsThere has been a distinct lack of disclosure regarding nano-scale developments in keyhole surgery and remote medicine, a "disparity of disclosure" which does not correlate with the rapid advancements in both the medical and nanotechnology fields over the last two-decades.Robotic surgery has been touted as a solution to underdeveloped nations, whereby a single central hospital can operate several remote machines at distant locations. The potential for robotic surgery has had strong military interest as well, with the intention of providing mobile medical care while keeping trained doctors safe from battle.
Non-robotic hand guided assistance systemsThere are also user-friendly non robotic assistance systems that are single hand guided devices with a high potential to save time and money. These assistance devices are not bound by the restrictions of common medical robotic systems. The systems enhance the manual possibilities of the surgeon and his team, regarding the need of replacing static holding force during the intervention.Some of the features are:
The stabilisation of the camera picture because the whole static workload is conveyed by the assistance system.
Some systems enable a fast repositioning and very short time for fixation of less than 0.02 seconds at the desired position. Some systems are lightweight constructions (18 kg) and can withstand a force of 20 N in any position and direction.
The benefit – a physically relaxed intervention team can work concentrated on the main goals during the intervention.
The potentials of these systems enhance the possibilities of the mobile medical care with those lightweight assistance systems. These assistance systems meet the demands of true solo surgery assistance systems and are robust, versatile, and easy to use.
Instrument listA complete list of ophthalmic instruments can be found below:Instrument Uses
Toric Markerto mark 0 to 180 degree reference mark for Toric IOL implant
Pre-chopperto chop lens into pieces before implantation new lens and reduce phaco time
Spectacles (glasses) to correct refractive errors of the eye; not invasive
Contact lensesto correct refractive errors of the eye; a little invasive
Phoropter used in refraction testingTonometers used to determine the intraoccular pressure (IOP) -

useful in glaucoma; vide link for various types of tonometers.
Speculum: to keep the eyes open during any operation
Universal eye speculum-do-; heavy instrument and can not keep eyelashes out of the operating field
•Guarded eye speculum (left and right)
-do-; heavy instrument but can keep eyelashes out of the operating field with its "guard" and hence left or right ones are required
•Wire Speculumto keep the eyes open during any operation; light wire instrument
Needle holders: holding the needle in position while applying sutures
•Silcock's needle holder-do-; has a catch and is used for heavier gauge needles; used mainly for skin, muscle and corneal incisions
•Arruga's needle holder-do-; has a catch (lock) and is used for heavier gauge needles (thicker than 6-0); used mainly for skin, muscle and corneal incisions
•Barraquer's needle holder
-do-; small instrument with a spring action with or without a catch used for finer gauge needles (5-0 or finer); used mainly for intraoccular incisions
Forceps: to hold anything
•Artery forceps (haemostat)
medium sized, with a serrated tip and a catch; used to hold bleeding vessels and compress them in order to make them stop bleeding and also to hold or crush structures.
•Fixation forcepshas a few teeth at the tip; for holding structures and restricting their movement or to hold small swabs
•Plain dissecting forcepsblunt untoothed with a serrated tip; for holding structures and restricting their movement or to hold small swabs
•Iris forcepsfine tipped (straight or otherwise) with small teeth; to hold the iris tissue during procedures
•Elschnig's intracapsular forceps
fine untoothed forceps for holding tissue, swabs, sutures, etc.; removing things like clots, capsule fragments, lens, etc.; used in cataract surgery
•Arruga's intracapsular forceps
fine untoothed forceps holding tissue, swabs, sutures, etc.; removing things like clots, capsule fragments, lens, etc.; used in cataract surgery
•Colibri forcepsfine toothed forceps for holding flaps of cornea or sclera and rarely the iris
•Saint Martin's forceps holding flaps of cornea or sclera and rarely the iris
•Superior rectus holding forceps
specially curved (to fit into the orbit of the eye) forceps for catching hold of the muscle bellies of the intraorbital muscles and sutures
•Suture tier forceps fine limbed untoothed forceps to hold fine sutures or

hairs
•Capsulotomy forcepsto tear the anterior capsule of the lens during cataract surgery
•Disc holding forceps used in glaucoma surgery (obsolete)
•Capsulorhexis forceps
fine sharp-tipped untoothed forceps for doing a continuous curvilinear incision and removal of the anterior capsule of the lens ("continuous curvilinear capsulorhexis - ccc")
•MacPherson's forcepsfine sharp-tipped untoothed forceps with an angulation for holding parts of the lens, the intraocular lens, 10-0 (very fine) sutures, etc.
•Chalazion forceps (clamp)
self-retaining with discoid ends; used to hold and prevent a chalazion from bleeding during its surgery
•Epilation forceps (Cilia forceps)
stout flat-ended blunt forceps with a thickened end to remove eyelashes
•Entropion forcepsself-retaining with big discoid ends used to hold and prevent an entropion from bleeding during its surgery
Chalazion scoopto remove the granulation tissue from a chalazion during surgery
Entropion clamp
right and left varieties exist; large clamp with two limbs; self-retaining with big discoid ends used to hold and prevent an entropion from bleeding during its surgery
Nettleship's punctum dilator
to dilate the lacrimal punctum of the lacrimal apparatus of the eye for syringing or operations
Cystitomea 26 gauge needle bent twice used for incising the anterior capsule of the lens in lens extraction
Wire vectisa loop of wire attached to a stack used to extract cataract affected lenses
Irrigating vectisa small hollow instrument with a used to introduce fluid into the anterior chamber to raise its pressure to aid cataract extraction
Canula used to carry fluid
•Irrigation-aspiration two-way canula
effectively two small canulae fitted together, one to introduce fluid and the other to extract the cortical materials, blood, etc. in eye operations
•Lacrimal canula
small curved canula the size of a syringe needle used to introduce fluids or drugs into the nasolacrimal passage to test its patency or during surgery (dacrocystography, dacrocystectomy, dacryocystorhinostomy(DCR), etc.
Lang's lacrimal dissector with scoop
for blunt dissections and cleaning during operations like dacryocystorhinostomy
Rougine dissection of lacrimal sac

Retractorto pull and hold overlying tissue out of the operating field
•Muller's self retaining adjustable haemostatic retractor
-do-; self retaining haemostatic
•Cat's paw retractor -do-•Desmarre's lid retractor
-do-; specially for noncooperative patients and to see the fornices (see human eye)
Bone punchto fracture pieces from a thin bone in facial surgery and during operations like dacryocystorhinostomy
Evisceration spoon or scoop
removing all the contents of the eyeball during evisceration (complete removal of all structures within the eye in diseases like endophthalmitis
Lid plateflat large instrument that has a groove and is placed between the lid and globe of the eye to provide a solid support for eyelid surgery
Hammer, chisel and bone gouge
bone cutting and shaping
Bowmen's discission needle
microsurgery of the lens capsule
Knives to cut structures•Surgical scalpel with small blades
general purpose instrument
•von Graefe's cataract knife
cutting out of the anterior chamber from the inside through the limbus
•Tookes' knife (Sclero-corneal splitter)
making sclerocorneal tunnels in "small incision cataract surgery (SICS)" and keratoplasty
•Crescent knife (Sclero-corneal splitter)
making sclerocorneal tunnels in "small incision cataract surgery"
•Angular keratomemaking sclerocorneal tunnels in "small incision cataract surgery"; larger one used to increase the size of the incision
•Side-port blademaking sclerocorneal "side port" (a secondary tunnel) tunnels in "small incision cataract surgery"
•Beer's knife incise the conjunctiva or the eyelid skin
•Keratotomesmall triangular blade with two sharp edges used to incise the limbus (sclerocorneal junction)
•Zeigler's knifevery tiny knife for intaoccular maneuvers specially when space is less
Scissors -•Conjunctival sac scissors
flat small curved scissors to cut the conjunctive
•Corneal spring scissorsmedium spring-open used to cut the external side of the cornea, fine sutures; iris, etc.

•de' Wecker's iris scissors
small slender spring-open scissors for intraoccular maneuvers (iris and deeper and more delicate structures); has two wings to operate it and one sharp and one blunt blade.
•Vannas' scissors
small slender spring-open scissors for intraoccular maneuvers (iris and deeper and more delicate structures); has two wings to operate it and one sharp and one blunt blade.
•Enucleation scissorsthick scissors used to cut the optic nerve in enucleation operation
Bowman's lacrimal probe
probing the nasolacrimal duct
Lens expressorused to force out the lens in extracapsular or intracapsular cataract extraction
McNamar's spoonused to force out the lens in intracapsular cataract extraction
Iris repositortwo limbed instrument used to remove the iris during posterior chamber maneuvers
Sinsky's hook intraocular lens dialler
angulated round hook with a handle used in insertion of an intraocular lens
Strabismus hookmuscle hook or squint hook; sharp tip or knobbed tip; used in squint surgery
Foreign body spud and needle
Spud to remove superficial and needle for the deep foreign bodies in the eye
Elliot's trephine with handle
used in corneal donation (eye donation) to cut out the cornea in a circular fashion
Castroveijo's calipers various measurements are takenCastroveijo's corneal trephine
used in corneal donation (eye donation) to cut out the cornea in a circular fashion
Pin-hole testing visual acuity
Red green goggles(red - right side & green - left side) used in Worth 4 dot test, diplopia testing
Prismsto measure the degree of squints; in other instruments; refractive correction; etc.
Placido's disc to assess the condition of the corneal surface
Retinoscopeobjective determination of refractive error and for looking inside the eye
Loupeused ot search for magnified examination of the anterior segment of the eye (uniocular or binocular)
Jackson's cross cylinderused to check the power and axis of a cylindrical lens
Maddox rod used to test for latent squint and retinal functionRefraction box has lenses of different powers for refraction testingSlit lamp bio microscope used for examining the anteriorly placed structures

the eye; vide linkCharts for vision -•Distant vision to determine visual acuity of distant vision••Snellen's distant vision chart
-do-; for those who can read in English
••Regional language charts
-do-; for those who can read in their local language
••E Chart -do-; for those who can not read••Landolt's broken ring chart
-do-; for those who can not read
••Toys pr picture chart -do-; for children•Near vision -do-; to determine visual acuity of near vision••Jager's chart -do-••Printer's types of N series
-do-
••Snellen's near chart (1/17th reduction of distant chart)
-do-; standard chart of alphabets; vide link
•Colour vision: to test colour vision••Ishihara's chart to determine the type of colour blondness
Stenopaeic slitdetection of axis of the cylindrical (astigmatism) power of the eye; glaucoma testing
Implants -
•Intraocular lensprosthetic lenses implanted after lens (anatomy) removal
•Artificial eyesas non-functional cosmetic implants into the eye socket
Blade breaker to break disposable blade after use to prevent reuse
Thermo-cauteryto coagulate blood vessels and prevent haemorrhage
Cryoprobe to freeze and extract the lens
Yttrium aluminium garnet laser (YAG laser)
to correct posterior capsular opacification (specially after removal of a cataract, if required), peripheral iridotomy, retinal surgery, laser-assisted sub-epithelial keratectomy (LASEK) etc.
Electrolysis used for permanent hair removalElectrocautery for electrosurgery
Phacoemulsificationused for extraction of a cataract affected lens after emulsifying it using a high frequency (energy) ultrasound probe
Image gallery