seeing the forest through the wheeze: laryngeal involvement in
TRANSCRIPT
Seeing the Forest Through
the Wheeze:
Laryngeal Involvement in
Episodes of Dyspnea
Marc Haxer, M.A., CCC-Sp
Departments of Speech-Language Pathology and Otolaryngology/Head and Neck Surgery
University of Michigan Health System
Introduction
• Goals/Objectives – Become familiar with upper versus lower
airway etiologies for dyspnea
– Become able to differentially diagnose upper airway involvement in dyspnea
– Become familiar with chronic cough, involuntary vocal fold closure, laryngospasm, adductory laryngeal breathing dystonia and irritable larynx syndrome as they relate to compromised respiration
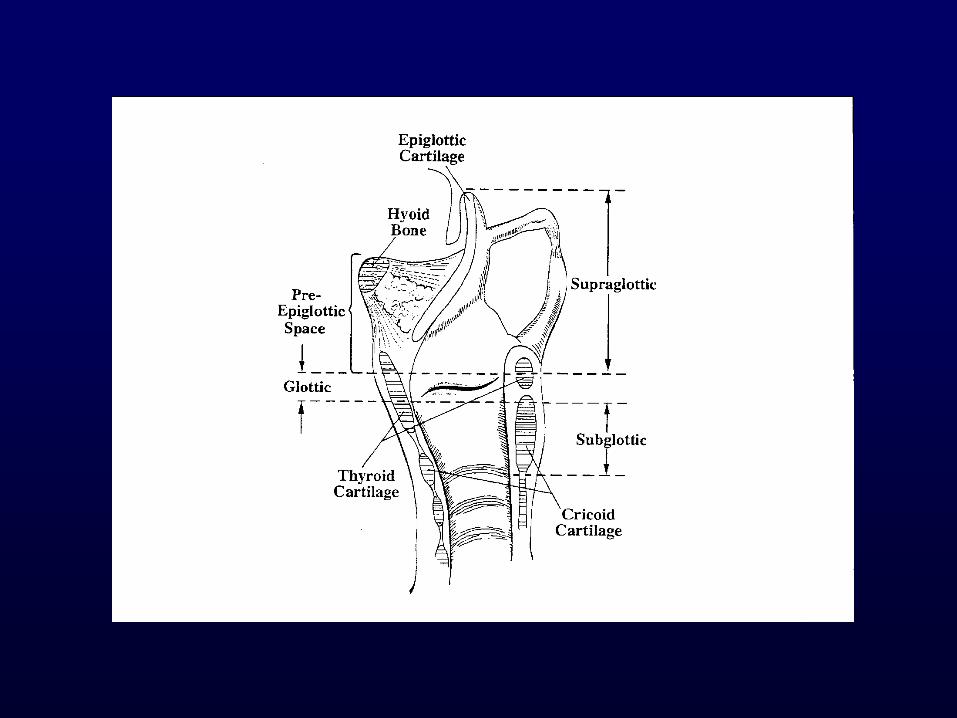
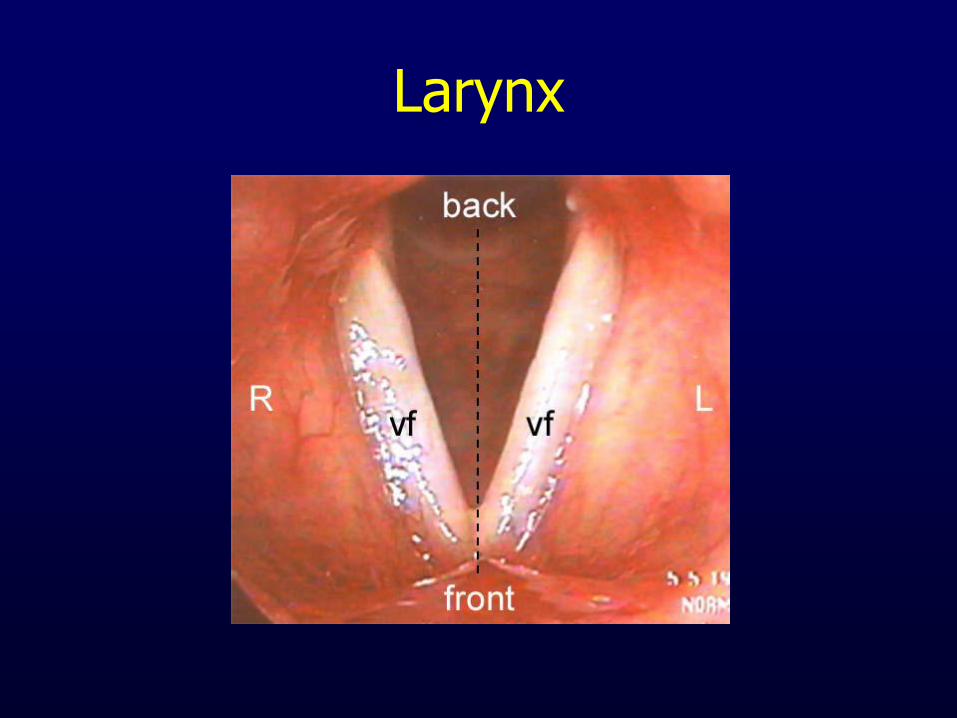
Larynx
• Cartilaginous tube – Connects inferiorly to respiratory system
• Trachea, lungs
– Connects superiorly to vocal tract • Pharynx, oropharynx, nasopharynx
• Anatomic orientation important – Highlights interactive relationship between vocal
subsystems • Pulmonary mechanism
• Laryngeal valve
• Supraglottic vocal tract resonator
Larynx
• Complex arrangement of muscles, mucus membranes, and other connective tissue – Soft tissues responsible for airway preservation
– Cartilage housing serves as columnar protective shield for laryngeal valve
• Muscles and cartilages provide three levels of “folds” – Serve as sphincters which provide communicative and
vegetative functions
– Angles of closure multidimensional (valve in horizontal and vertical planes)
Larynx
• Upper rim of larynx formed by aryepiglottic folds
– Fibrous membrane extending from epiglottis to arytenoid towers
– Thus serves as lateral boundary of larynx
– Epiglottic inversion posteriorly/inferiorly over laryngeal vestibule results in separation of larynx from pharynx and serves as most superior level of airway protection
Larynx
• Second sphincter formed by ventricular folds – Not normally active during phonation – Can become hyperfunctional during episodes of
increased vocal effort/extreme vegetative closure – Directly superior to ventricle/true vocal folds – Form double layer of medial closure w/TVFs if needed – Principle function is to increase intrathoracic pressure
by blocking exhalatory airflow from lungs – Compress tightly during sneezing/coughing, lifting,
emesis, childbirth, defecation – Also provide medial level of airway protection during
swallows
Larynx
• Most inferiorly are true vocal folds
– Provide vibrating source for phonation
– Also close tightly for nonspeech and vegetative tasks
• Thus, larynx and vocal folds function as variable valve
– Modulate airflow through VFs during phonation
– Close off trachea/lungs to prevent soiling of airway during swallows
– Provide resistance to increased abdominal pressure during effortful activities
Neurologic Supply
• Cranial nerve X innervates larynx peripherally
– Vagus = “wanderer”
– Innervates sites from skull to abdomen
• Innervates larynx through two important branches
– Superior laryngeal nerve (SLN)
– Recurrent laryngeal nerve (RLN)
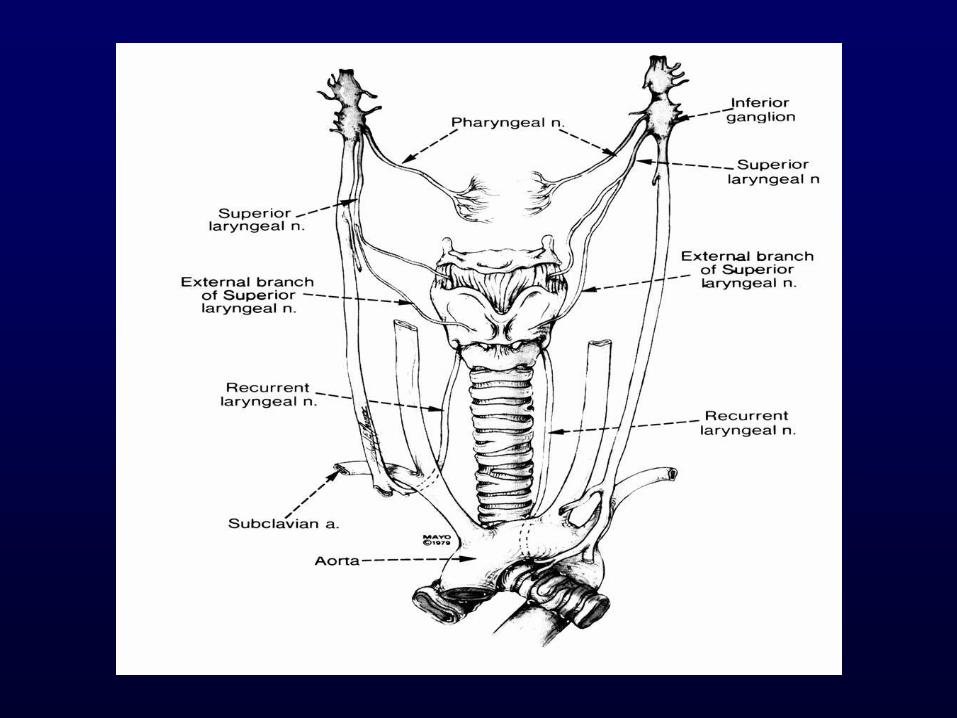
Neurologic Supply
• Superior laryngeal nerve
– Branches off vagus near nodose ganglia in neck
– Course alongside carotid artery
– Forms internal/external branches
• Internal branch inserts through thyrohyoid membrane superior to VFs and provides all sensory information to larynx
• External branch is motor nerve to cricothyroid (CT) muscle
Neurologic Supply
• Recurrent laryngeal nerve – Extends to thorax
– Forms long loop under heart before coursing superiorly under thyroid gland and into larynx
– Different on right/left sides of body • L RLN courses under aorta
• R RLN course under subclavian artery
– Nerves (especially left) susceptible to injury
– Supplies all sensory information to area below VFs and all motor innervation to PCA, TA, LCA, and IA muscles
Larynx
Where/What’s the Problem?
• Upper airway issue?
• Lower airway issue?
• Problem w/inhalation?
• Problem w/exhalation?
• Problem w/both?
• Acute versus chronic issue?
• Episodes same/different w/regard to presentation?
• Episodes same/different w/regard to severity?
Upper Airway Issues that can Compromise Respiration
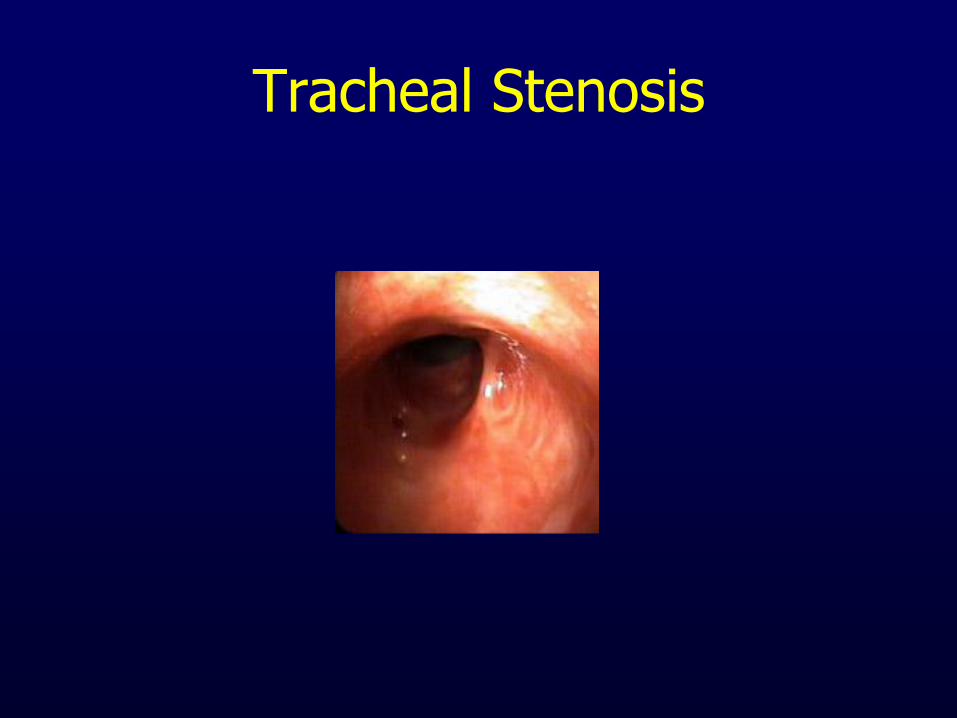
• Unilateral vocal fold motion impairment (abductory) • Bilateral vocal fold motion impairment (abductory) • Reinke’s edema • Laryngeal papilloma • Laryngeal carcinoma • Vocal Fold Granuloma • Laryngospasm • Involuntary vocal fold closure • Cough • Adductory Laryngeal Breathing Dystonia • Acute infection (eg croup, laryngitis, epiglottitis) • Allergies • Laryngomalacia • Tracheomalacia/Stenosis • Foreign body in airway • Extrinsic/intrinsic airway compression by tumor inferior to glottis
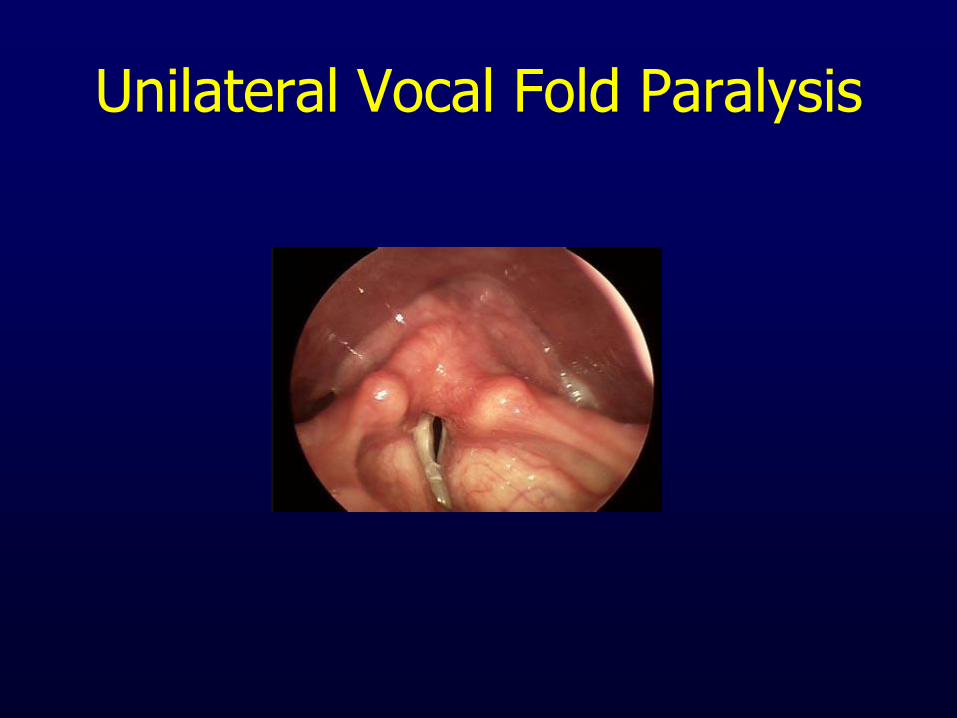
Unilateral Vocal Fold Paralysis
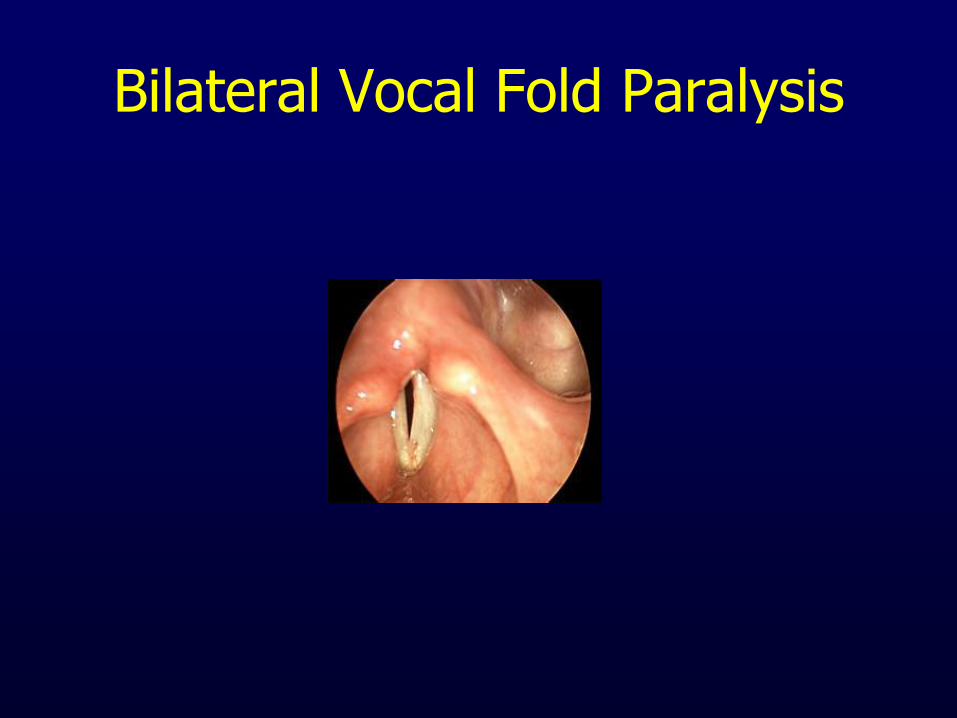
Bilateral Vocal Fold Paralysis
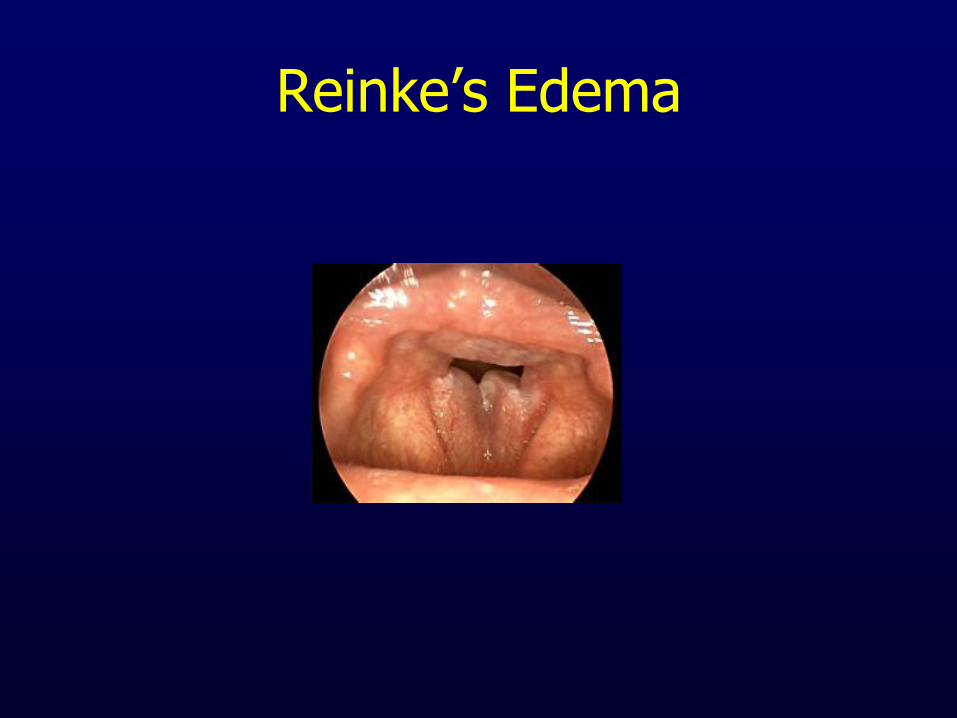
Reinke’s Edema
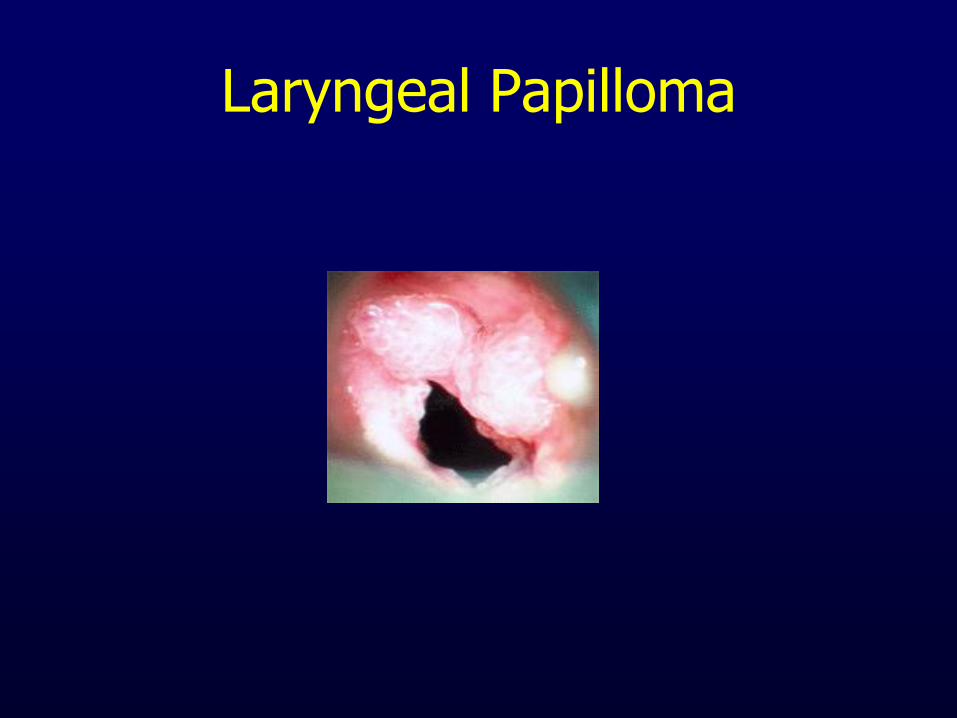
Laryngeal Papilloma
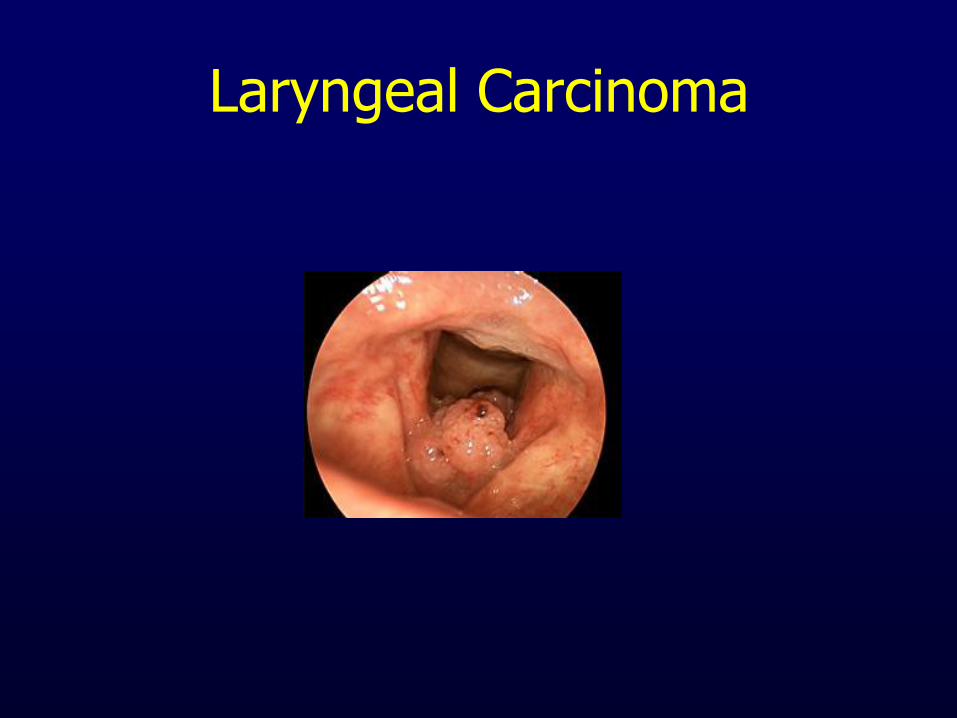
Laryngeal Carcinoma
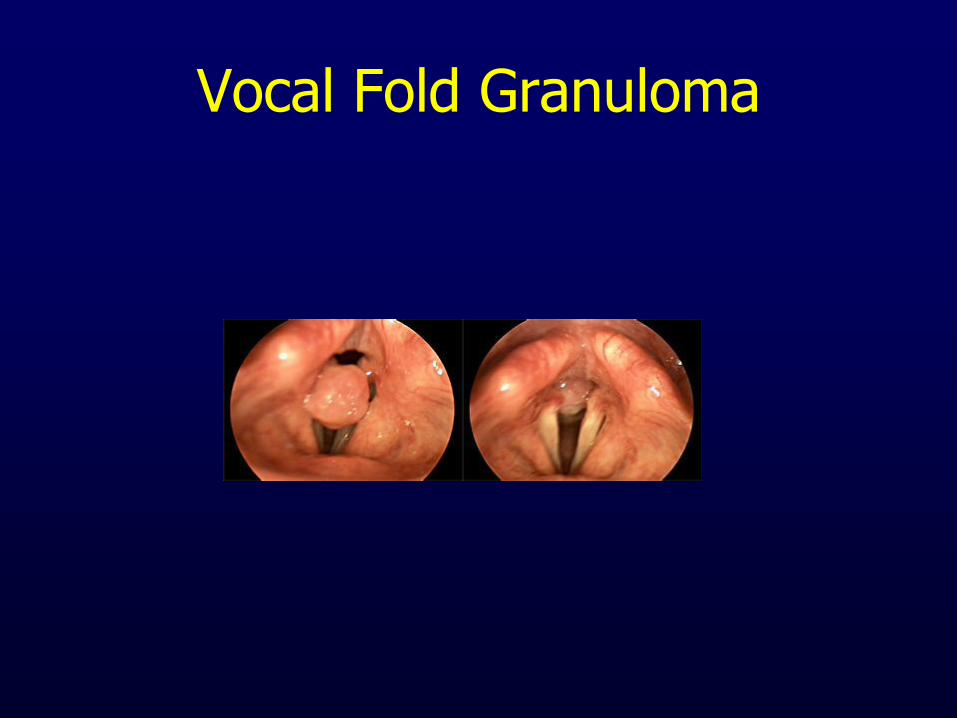
Vocal Fold Granuloma
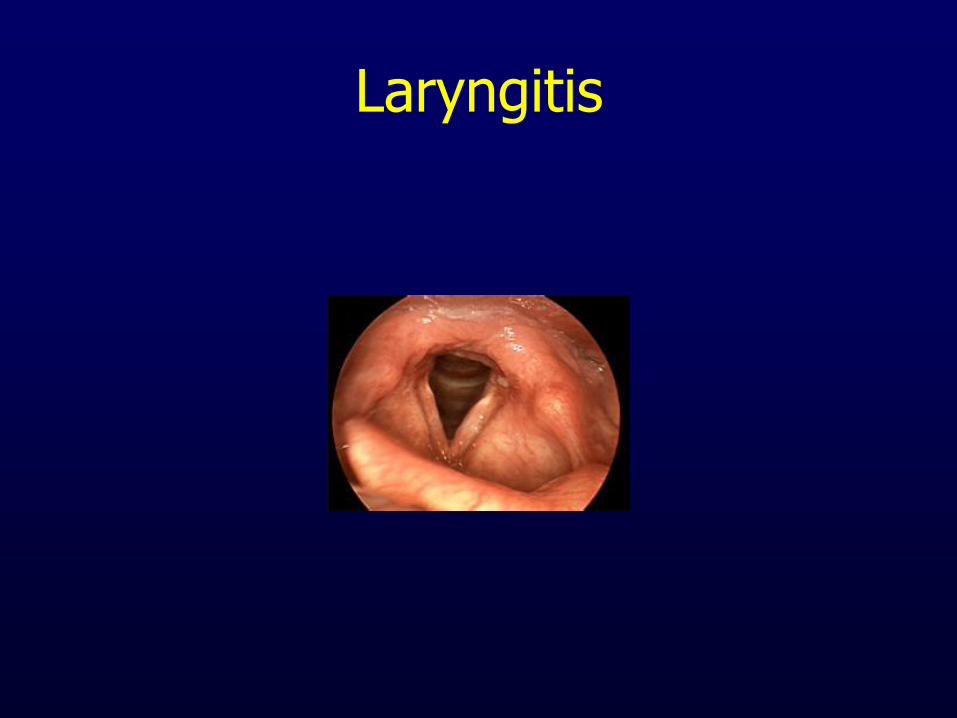
Laryngitis
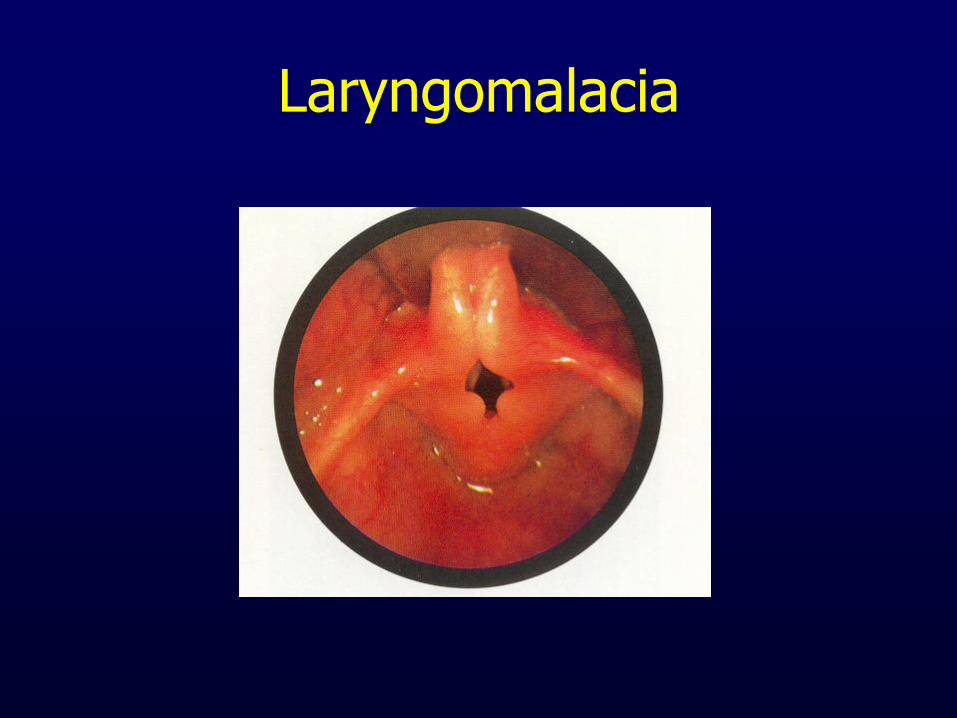
Laryngomalacia
Lower Airway Issues that can Compromise Respiration
• Asthma
• COPD
• Emphysema
• Restrictive Airway Disease
• Lung Cancer
• Interstitial lung disease
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Chronic sinusitis/URI
– Cough/throat clear
• Can cause trauma to laryngeal tissues
– Antihistamines
• Dry secretions
• Resultant dehydration of VFs
– Anti-cough medications
• Drying agents
• Contribute to VF dehydration
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Asthma
• Chronic obstructive pulmonary disease
• Emphysema
• Lung CA – Above can be direct/indirect cause of laryngeal
problems • Vocal fold tissue abuse
• Poor breath support
• Vocal fold dryness secondary to medication use
• VF paresis/paralysis
• Cough
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Allergies
– Congestion/edema of VFs
– VF dehydration
– VF tissue trauma
• cough/throat clear
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Laryngopharyngeal reflux disease – Is GERD that affects pharynx/larynx
– Occult chronic reflux is etiologic factor in high percentage of patients w/laryngologic complaints
– Reflux involves multiple anatomic sites • LES
• Entire esophagus
• UES
• Larynx/pharynx/oral cavity
• Trachea
• Lungs
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Laryngopharyngeal reflux disease – Symptoms
• Chronic hoarseness • Voice fatigue • Cough • Chronic throat clearing • Globus sensation • Sensation of choking • Edema • Ulceration/granulation of laryngeal mucosa • Hyperkeratosis • Carcinoma of larynx
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Laryngopharyngeal reflux disease – LPRD best managed via multidisciplinary team
• Otolaryngologist
• Internist/PCP
• Gastroenterologist
• Allergist
• Pulmonologist
• Speech Pathologist
• Nutritionist
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Laryngopharyngeal reflux disease
– Almost always associated w/some degree of aspiration
• Amount of aspiration may be clinically insignificant
• Or, may be clinically significant enough to cause:
– Chronic cough
– Involuntary vocal fold closure
– Reactive airway disease
– Difficult to control asthma
– Pneumonia
– Bronchiectasis
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Laryngopharyngeal reflux disease
– Evaluation
• Esophagram
• Dual 24-hour pH probe
• Bravo capsule study
• Flexible fiberoptic endoscopy
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Laryngopharyngeal reflux disease
– Treatment
• Behavioral
• Chewable antacids
• Viscous antacids
• H2-receptor antagonists
• Proton pump inhibitors
• Nissen fundoplication/Stretta procedure
Chronic Illnesses/Disorders That Can Affect Laryngeal Function
• Smoking/alcohol abuse/illicit drug use
– Erythema/edema
– Generalized inflammation
– Drying of mucous membranes
– Incoordination/dysarthria/impaired judgment
– LPRD
– Chronic cough
Primary Disorder Etiologies That Can Affect Laryngeal Function
• Environmental stress – Loss of employment – Death of spouse/significant other – Family conflict
• Conversion behaviors – Avoidance behavior(s) developed to counteract stressful
situation(s) – Whispering, muteness, unusual dysphonias
• Identity conflict – Establishment of own personality
• High-pitched falsetto in post-pubescent adolescent • Weak, juvenile, thin-sounding voice of adult female • Raised pitch in male-to-female transsexual

Case Study #1
• 41 year-old female • Presenting Dx of “difficult to control asthma” • Trialed on multiple courses of different asthma
medications over a # of months w/no appreciable improvement in respiratory function
• No hx of smoking/excessive alcohol use • Presenting symptoms
– Chronic sense of chest tightness – Chronic restriction of inhalation/exhalation – Sense of “elephant sitting on chest” – Chronic hoarseness X12 months w/no Otolaryngologic
examination – Denied sense of throat constriction
Case Study #1
• Presenting symptoms not consistent with upper airway involvement
• Extended duration of hoarseness concerning
• Referral to Otolaryngology
• Fiberoptic endoscopic exam results – Marked endolaryngeal erythema/edema
– Laryngeal candidiasis
– No concerning lesions
Case Study #1
• Treatment
– Speech Pathology not involved in Tx
– Aggressive pharmacologic management of LPRD/candidiasis for six months
• Oral anti-fungal medication (swish/swallow)
• Anti-reflux management
– Rigid behavioral strategies
– 40mg PPI b.i.d. 30 minutes prior to oral intake
Case Study #1
• Results of treatment
– 40 lb. weight loss
– Return of baseline vocal functioning
– Return of baseline respiratory functioning
– Secondary to tx, QOL markedly improved
Irritable Larynx Syndrome
Laryngospasm
IVFC
Chronic Cough
Chronic Throat Clearing
Irritable Larynx Syndrome
• Postulated by Morrison, Rammage, and Emami in 1999
• Suggests that various laryngeal behaviors can be categorized within the context of “hyperkinetic laryngeal dysfunction”
These Behaviors Include:
• Muscle Tension Dysphonia
• Episodic laryngospasm
• Globus sensation
• Cough
Muscle Tension Dysphonia
• Incoordination between respiration and phonation
• Above results in elevated levels of laryngeal/throat muscle tension
• In turn, contributes to general laryngeal hyperfunction – Laryngeal pain/discomfort
– Increased vocal effort
– Vocal fatigue
Muscle Tension Dysphonia
• In addition to elevated levels of tension in larynx/throat, can also contribute to increased tension in neck, shoulder, and upper chest musculature
– Can then masquerade as sensation of limited movement of air through the neck/throat area during inhalation
Episodic Laryngospasm
• Adduction of VFs during inhalatory phase of respiration • In differential Dx
– Involuntary Vocal Fold Closure – Adductory Laryngeal Breathing Dystonia – Closure of VFs as protective mechanism during reflux episode
• Somatoform/anxiety disorder? – Intrinsic/extrinsic stress vs. psychological issue – Larynx “Achilles heel” for stress/anxiety?
• Variations on a theme? – Asthma variant
• Functional? – Implies normal structure/function of larynx but inappropriate behavior
of the same
Globus
• “Lump in throat” sensation
• Secondary to increased levels of muscle tension in larynx? – Inappropriate resting or holding position of
laryngeal musculature
• Secondary to laryngopharyngeal reflux disease? – Laryngeal erythema/edema masquerading as
sensation of mucous
Cough
• Secondary to respiratory disease?
– Acute vs. chronic
– Productive vs. non-productive
• Secondary to laryngopharyngeal reflux disease?
• Increase in stress/anxiety?
– Stress vs. psychogenic
– Functional?
• Secondary to allergies?
• Neuropathic?

For All of These Behaviors
• Larynx appears structurally normal on visualization
• Abnormal laryngeal muscle posture present – Anteroposterior “squeeze” of laryngeal
complex
• Palpable laryngeal muscle tension present – Massage of thyroid cartilage/hyoid bone
results in pain, discomfort
Irritable Larynx Syndrome
• Defined as:
– “hyperkinetic laryngeal dysfunction resulting from an assorted collection of causes in response to a definitive triggering stimulus”
ILS – Inclusion Criteria
• Symptoms attributable to laryngeal tension – Dysphonia and/or laryngospasm
• With or without chronic cough • Visible and palpable evidence of tension
– Lateral and A/P compression of larynx during laryngoscopic examination
– Discomfort during laryngeal palpation
• Presence of sensory trigger(s) – Airborne substance – Esophageal irritant – Odors
ILS – Exclusion Criteria
• Apparent organic laryngeal pathology
• Identifiable neurologic disease
• Identifiable psychiatric diagnosis
Patients with Dx of ILS
• Tend to have complex combination of signs, symptoms, and background factors
• Laryngospasm and dysphonia are two major ILS symptoms – Laryngospasm most distressing to patient
• More minor symptoms – Globus
– Cough
– Perilaryngeal pain
• Above will vary from patient to patient
ILS Symptom Complex Grouping
• Laryngospasm alone
• Laryngospasm with dysphonia, globus, or cough
• Dysphonia alone
• Dysphonia with laryngospasm, globus, or cough
• Other
– Globus and/or cough
Triggering Stimuli
• Airborne irritants
• Reflux
• Perfumes/colognes
• Foods
• Emotions
• Voice use
• Exertion
Possible Etiologic Factors
• Reflux
• Viral
• Stress/Psychogenic
• Asthma
• Environmental allergy(ies)
• Torsion injury to neck/throat/larynx
Hypothesis for ILS
• Develops as reaction to some sort of CNS change that leaves sensorimotor pathways in state of hypersensitivity
• # of possible causative factors
• Several can be active in any one patient
• Most prevalent – Emotional distress
• Stress component vs. psychogenic cause
– Habitual inappropriate resting posture of laryngeal musculature
– LPRD
– Post-viral illness • Viral neuropathy
Treatment
• Reflux management – Behavioral/pharmacologic
• Exercises
• Stress management
• Massage/manipulation
• Non-reflux pharmacologic management – Botulinum Toxin A
– Nebulized topical anesthetic
– Amitriptyline/Gabepentin
Cough
• Important respiratory defense mechanism
• Responsible for clearance of excessive secretions, fluids, or foreign materials from the airway
• Despite this protective role, excessive coughing can result in multisystem issues
– Anxiety, dysphonia, fatigue, urinary incontinence, emesis, rib fracture(s), etc.
Cough – Differential Diagnosis
• Upper Respiratory Tract
• Allergic or vasomotor rhinitis, postnasal drip syndrome, infectious/post-infectious cough, sinusitis
Cough – Differential Diagnosis
• Lower Respiratory Tract • Abscess, allergic inflammation, aspiration, asthma, bronchiectasis, bronchitis, COPD, cystic fibrosis, drugs, eosinophilic bronchitis, interstitial lung disease, pertussis, primary or metastatic lung tumors, sarcoidosis, tuberculosis
Cough – Differential Diagnosis
• Cardiovascular system
• Gastrointestinal system
• Left ventricular failure, mitral stenosis, medications (ACE inhibitors)
• Reflux disease (laryngopharyngeal)
Cough – Differential Diagnosis
• Central Nervous System (psychological response)
• D’Urzo and Jugovic (2002)
• Habit cough, chronic cough, psychogenic cough, neuropathic cough
Cough – Clinical Presentation
• School age children to older adults
• Average length of cough months to years
• Most pts have attempted multiple interventions w/o resolving of cough
• Most have associated fatigue
• Most do not have accompanying hoarseness
• Most have been treated for reflux for a short period of time w/o success
Cough
• Habit/chronic cough – Larynx engaged in disordered loop of behavior
• Psychogenic cough – Cough occurs secondary to emotional/psychological issues
• Laryngeal hypersensitivity/hyper-reactivity – Larynx over-reacts to triggering stimuli secondary to irritation of
the larynx by refluxed stomach contents
• Neuropathic cough – Cough occurs secondary to viral neuropathy
• Cough Hypersensitivity Syndrome (Morice, 2009) – Th2-type immune response vs. reflux symptoms
Behavioral/Environmental History
• Nature of cough – Light dry coughs throughout the day – Severe/overwhelming cough “attacks”
• Pattern of cough – Occurs at specific time(s) of day? – Follow meals or specific activity(ies)? – Getting worse/remaining stable?
• Work/home/social environment – New building materials? – Ventilation relative to work space? – Dusty and/or dry environment?
Cough - Tx
• Habit/chronic cough – Behaviorally reposture larynx into appropriate pattern of functioning – Improve laryngeal environment – Improve awareness of sensations/behaviors that precipitate cough – Implement behavior to delay/eliminate the cough before it
“recalibrates” laryngeal sensitivity threshold
• Psychogenic cough – Behavioral/psychological treatment
• Laryngeal hypersensitivity/hyper-reactivity – Behavioral/aggressive reflux tx
• Neuropathic cough – Amitriptyline, Gabepentin
• Cough Hypersensitivity Syndrome – Treat causal phenotype appropriately
Involuntary Vocal Fold Closure
• Confusing disorder that is frequently mistaken for asthma or organic obstructive upper airway conditions
• Fully 78 different names for disorder in the literature
• Encompasses inappropriate vocal fold adduction during inhalation
IVFC - Symptoms
• Sudden onset
• Compromised inhalation
• Sensation of throat closure/tightness
• Inhalatory stridor
IVFC Mimicking Asthma
• IVFC
– Throat tightness, dysphonia during episodes – esp inhalation
– Little/no improvement w/use of bronchodilators during episodes
– No night awakening or cough unless associated with reflux-induced laryngospasm
• Asthma
– Chest tightness – esp exhalation
– Improvement w/use of bronchodilators
– Nighttime symptoms frequent
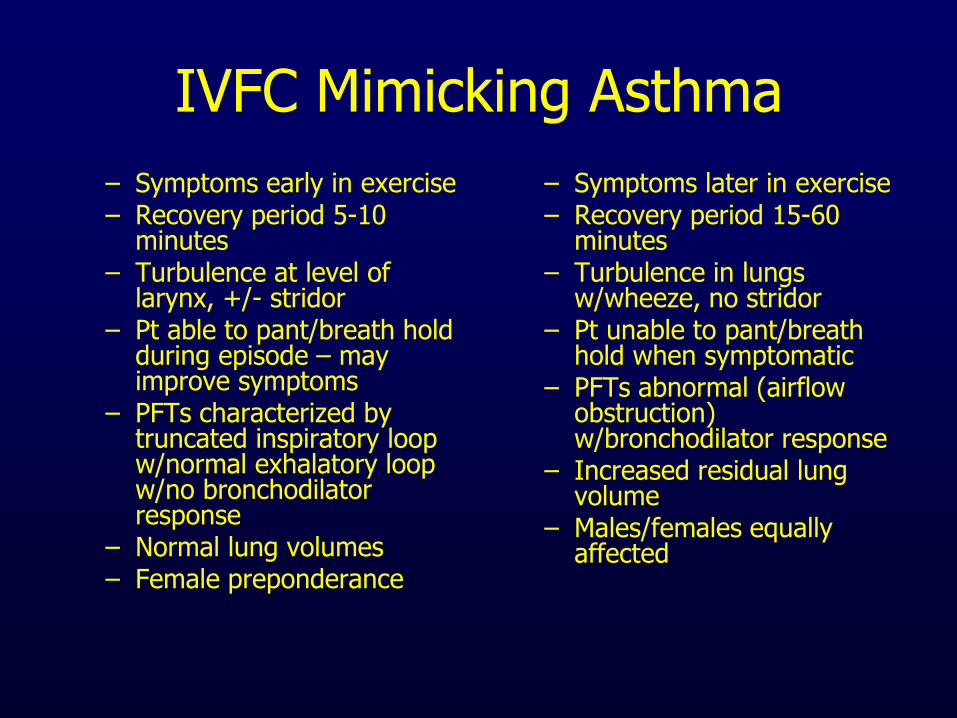
IVFC Mimicking Asthma
– Symptoms early in exercise – Recovery period 5-10
minutes – Turbulence at level of
larynx, +/- stridor – Pt able to pant/breath hold
during episode – may improve symptoms
– PFTs characterized by truncated inspiratory loop w/normal exhalatory loop w/no bronchodilator response
– Normal lung volumes – Female preponderance
– Symptoms later in exercise – Recovery period 15-60
minutes – Turbulence in lungs
w/wheeze, no stridor – Pt unable to pant/breath
hold when symptomatic – PFTs abnormal (airflow
obstruction) w/bronchodilator response
– Increased residual lung volume
– Males/females equally affected
IVFC
• Causal factors
– Functional or psychogenic issue?
– Laryngeal hypersensitivity/hyper-reactivity?
– Laryngospasm?
– Adductor laryngeal breathing dystonia (Blitzer and Brin, 1991; Grillone, et.al., 1994)
• Rare disorder whose symptoms are similar to IVFC
• Neurological issue
• Behavioral intervention not efficacious in management
IVFC - Evaluation
• History – Acute versus chronic issue?
– Episodes same/different w/regard to presentation?
– Episodes same/different w/regard to severity?
– Triggers
• Flexible endoscopy during/subsequent to challenge
• Spirometry
IVFC - Treatment
• Functional issue – Behavioral intervention
• Psychogenic issue – Behavioral/psychological treatment
• Laryngeal hypersensitivity/hyper-reactivity – Aggressive reflux management
• Laryngospasm – Aggressive reflux management, behavioral management, use of
Heliox if severe, tracheotomy if life-threatening
• Adductory laryngeal breathing disorder – Botulinum Toxin A injections
Case Study #2
• 13 year-old female
• Placed into foster care/living w/supportive foster mother
• Reason for placement – ongoing sexual/psychological abuse at hands of one parent w/other parent/family members unable/unwilling to intervene
• Patient actively pursuing legal severance of parental rights/involvement w/family
Case Study #2
• Parents/other family members under court order not to contact patient
• When court order violated, patient experienced episodes of dyspnea: sudden onset, sensation of throat constriction, compromised inhalation, and inhalatory stridor
Case Study #2
• During flexible endoscopy, sudden onset of VF adduction occurred
• Use of behavioral intervention efficacious in alleviating episode
• Episodes continued to occur but were effectively managed w/behavioral strategies
• Episodes ceased subsequent to legal severance of parental/family rights, adoption of patient by foster mother, and 18 months of psychotherapy
Thank you!
Bibliography
• Christopher, K.L., Wood II, R.P., Eckert, R.C., Blager, F.L., Raney, R.A., Souhrada, J.F.: Vocal Cord Dysfunction Presenting as Asthma. New England Journal of Medicine, 308: 1566-1570 (1983)
• Martin, R.J., Blager, F.L., Gay, M.L., Wood II, R.P.: Paradoxic Vocal Cord Motion in Presumed Asthmatics. Seminars in Respiratory Medicine, 8: 332-337 (1987)
• Grillone, G.A., Blitzer, A., Brin, M.F., Annino, D.J., Saint-Hilaire, M.H.: Treatment of Adductor Laryngeal Breathing Dystonia with Botulinum Toxin Type A. Laryngoscope, 104: 30-32 (1994)
• Bless, D.M., Swift, E.: Vocal Fold Dysfunction: Diagnosis and Management. Paper presented at the 4th Biennial Phonosurgery Symposium: Madison, WI (1996)
• Irwin, R.S., Boulet, L.P., Cloutier, M.M., Fuller, R., Gold, P.M., Hoffstein, V., Ing, A.J., McCool, D., O’Byrne, P., Poe, R.H., Prakash, U.B.S., Pratter, M.R., Rubin, B.K.: Managing Cough as a Defense Mechanism and as a Symptom: A Consensus Report of the American College of Chest Physicians. Chest, 133-207 (1998)
Bibliography
• Abaza, W.: Vocal Cord Dysfunction: Diagnosis and Treatment. Grand Rounds presentation to Faculty and Staff of the Department of Pediatric Pulmonary Medicine, University of Michigan Health System (1999)
• Morrison, M., Rammage, L., Emami, A.J.: The Irritable Larynx Syndrome. Journal of Voice, 13: 447-455 (1999)
• Sandage, M., Swift, E.: A New Look at Assessment and Treatment of Paradoxical Vocal Cord Dysfunction. Short Course presented at the Annual Convention of the American Speech-Language-Hearing Association. San Francisco, CA (1999)
• Altman, K.W., Mirza, M., Ruiz, C., Sataloff, R.T.: Paradoxical Vocal Fold Motion: Presentation and Treatment Options. Journal of Voice, 14: 99-103 (2000)
• Andrianopoulos, M.V., Gallivan, G.J., Gallivan, K.H.: PVCM, PVCD, EPL, and Irritable Larynx Syndrome: What are we Talking About and How do we Treat it? Journal of Voice, 14: 607-618 (2000)
Bibliography
• Altman, K.W., Simpson, C.B., Amin, M.R., Balkissoon, R., Casiano, R.R.: Cough and Paradoxical Vocal Fold Motion. Otolaryngology-Head and Neck Surgery, 127: 501-511 (2002)
• D’Urzo, A., Jugovic, P.: Chronic Cough. Canadian Family Physician, 48: 1311-1316 (2002)
• Newsham, K.R., Klaben B.K., Miller, V.J.: Paradoxical Vocal-Cord Dysfunction: Management in Athletes. Journal of Athletic Training, 37: 325-328 (2002)
• Sandage, M., Zelazny, S.K.: Paradoxical Vocal Fold Motion in Children and Athletics. Language, Speech, and Hearing Services in Schools, 35: 353-362 (2004)
• Sataloff, R.T., Castell, D.O., Katz, P.O., Sataloff, D.M.: Reflux Laryngitis and Related Disorders. San Diego; Plural Publishing (2006)
• Simpson, C.B., Amin, M.R.: Chronic Cough: State of the Art Review. Otolaryngology-Head and Neck Surgery, 134: 693-700 (2006)
Bibliography
• Johnston, N., Dettmar, P.W., Bishwokarma, B., Lively, M.O., Koufman, J.A.: Activity/Stability of Human Pepsin: Implications for Reflux Attributed Laryngeal Disease. Laryngoscope, 117: 1036-1039 (2007)
• Rank, M.A., Kelkar, P., Oppenheimer, J.J.: Taming Chronic Cough. Annals of Allergy, Asthma, and Immunology, 98: 305-313 (2007)
• Bastian, R.W.: Neurogenic Cough and Other Sensory/Pain disorders of the Head and Neck – 20 Year’s Experience. Paper presented at the Annual Convention of the American Speech-Language-Hearing Association, Chicago, IL (2008)
• Birchall, M.A., Bailey, M., Gutowska-Owsiak, D., Johnston, N., Inman, C.F., Stokes, C.R., Postma, G., Pazmany, L., Koufman, J.A., Phillips, A., Rees, L.E.: Immunologic Response of the Laryngeal Mucosa to Extraesophageal Reflux. Annals of Otology, Rhinology, and Laryngology, 117: 891-895 (2008)
• Blager, F.B.: Symptoms and Treatment of Vocal Cord Dysfunction/Paradoxical Vocal Fold Motion. Short Course presented at the Annual Convention of the American Speech-Language-Hearing Association, Chicago, IL (2008)

Bibliography
• Brugman, S.M.: What’s This Thing Called Vocal Cord Dysfunction? Retrieved 6/24/2008 at http://chestnet.org/education/online/pccu/vol20/lessons25_27/print26.php
• Cukier-Blaj, S., Bewley, A., Aviv, J.E., Murry, T.: Paradoxical Vocal Fold Motion: A Sensory-Motor Laryngeal Disorder. Laryngoscope, 118: 367-370 (2008)
• Koufman, J.A., Block, C.: Differential Diagnosis of Paradoxical Vocal Fold Movement. American Journal of Speech-Language Pathology, 17: 327-334 (2008)
• Ramanuja, S., Kelkar, P.: Habit Cough. Annals of Allergy, Asthma, and Immunology, 102: 91-95 (2009)
• Morice, A.H.: The Cough Hypersensitivity Syndrome: A Novel Paradigm for Understanding Cough. Lung, published online on October 7, 2009
• Sandage, M.: Sniffs, Gasps and Cough: Treatment of Irritable Larynx Syndrome Across the Lifespan. Paper presented at the Concepts in Voice Therapy Conference, New Orleans, LA (2009).