pulmonary vein isolation with complex fractionated atrial ... · from the pulmonary veins play a...
TRANSCRIPT

W
fA
Pulmonary vein isolation with complex fractionated atrialelectrogram ablation for paroxysmal and nonparoxysmal atrialfibrillation: A meta-analysisRobert M. Hayward, MD,* Gaurav A. Upadhyay, MD,* Theofanie Mela, MD,*Patrick T. Ellinor, MD, PhD,* Conor D. Barrett, MD,* E. Kevin Heist, MD, PhD, FHRS,*Atul Verma, MD,† Niteesh K. Choudhry, MD, PhD,‡ Jagmeet P. Singh, MD, DPhil*
From the *Department of Medicine and Cardiac Arrhythmia Service, Massachusetts General Hospital Heart Center,Boston, Massachusetts, †Southlake Regional Health Centre, Ontario, Canada, and ‡Department of Medicine, Brigham and
omen’s Hospital, Boston, Massachusetts.
BACKGROUND: Pulmonary vein isolation (PVI) is recognized as apotentially curative treatment for atrial fibrillation (AF). Ablationof complex fractionated atrial electrograms (CFAEs) in addition toPVI has been advocated as a means to improve procedural out-comes, but the benefit remains unclear.
OBJECTIVE: This study sought t synthesize the available datatesting the incremental benefit of adding CFAE ablation to PVI.
METHODS: We performed a meta-analysis of controlled studiescomparing the effect of PVI with CFAE ablation vs. PVI alone inpatients with paroxysmal and nonparoxysmal AF.
RESULTS: Of the 481 reports identified, 8 studies met our inclu-sion criteria. There was a statistically significant increase in free-dom from atrial tachyarrhythmia (AT) with the addition of CFAEablation (relative risk [RR] 1.15, P � .03). In the 5 reports ofnonparoxysmal AF (3 randomized controlled trials, 1 controlledclinical trial, and 1 trial using matched historical controls), addi-tion of CFAE ablation resulted in a statistically significant increase
aap
a consultant to Biosense Webster, Medtronic, Sanofi Aventis, Astra
1547-5271/$ -see front matter © 2011 Heart Rhythm Society. All rights reserved
84 of 179 [47%] for PVI alone; RR 1.32, P � .02). In trials ofparoxysmal AF (3 randomized controlled trials and 1 trial usingmatched historical controls), addition of CFAE ablation did notresult in a statistically significant increase in freedom from AT(n � 131 of 166 [79%] for PVI�CFAE vs. n � 122 of 164 [74%]for PVI alone; RR 1.04, P � .52).
CONCLUSION: In these studies of patients with nonparoxysmalAF, addition of CFAE ablation to PVI results in greater improve-ment in freedom from AF. No additional benefit of this combinedapproach was observed in patients with paroxysmal AF.
KEYWORDS: Atrial fibrillation; Catheter ablation; Complex frac-tionated atrial electrogram; Pulmonary vein isolation
ABBREVIATIONS: AF � atrial fibrillation; AT � atrial tachyar-rhythmia; CFAE � complex fractionated atrial electrogram;PVAI � pulmonary vein antrum isolation; PVI � pulmonary veinisolation.
(Heart Rhythm 2011;8:994–1000) © 2011 Heart Rhythm Society.
in freedom from AT (n � 112 of 181 [62%] for PVI�CFAE vs. n � All rights reserved.IntroductionAtrial fibrillation (AF) affects more than 2 million Americans1
and is associated with increased risk of stroke and death despiteoptimal medical therapy.2,3 The observation that ectopic beatsrom the pulmonary veins play a major role in the initiation ofF4 has led to the development of percutaneous isolation of
This work was conducted with support from Harvard Catalyst, TheHarvard Clinical and Translational Science Center (National Institutes ofHealth Award UL1 RR 025758 and financial contributions from HarvardUniversity and its affiliated academic health care centers). The content issolely the responsibility of the authors and does not necessarily representthe official views of Harvard Catalyst, Harvard University and its affiliatedacademic health care centers, the National Center for Research Resources,or the National Institutes of Health. Dr. Mela is a consultant to Biotronikand has lectured for Medtronic, St. Jude Medical, and Biotronik. Dr. Heistis a consultant to St. Jude Medical; has received research support fromBoston Scientific and St. Jude Medical; and has lectured for Biotronik,Boston Scientific, Medtronic, St. Jude Medical, and Sorin. Dr. Verma is
the pulmonary veins (PVI) as an accepted treatment for AF.PVI has resulted in high single procedural success rates forpatients with paroxysmal AF,5-8 but success rates for PVIlone in patients with nonparoxysmal AF are often lower, anddditional ablation has been advocated by some to increaserocedural success rates in this population.
Zeneca, and Servier; has lectured for Biosense Webster, Medtronic, andSt. Jude Medical; and has received research grants from BiosenseWebster, Medtronic, and St. Jude Medical. Dr. Singh is a consultantto Biotronik, Boston Scientific, Biosense Webster, CardioInsight,Medtronic, St. Jude Medical, CardioInsight, Thoratec, and the SorinGroup; has lectured for Biotronik, Boston Scientific, Medtronic, St.Jude Medical, and the Sorin Group; and has received research grantsfrom Biotronik, Boston Scientific, Medtronic, and St. Jude Medical.Address reprint requests and correspondence: Dr. Jagmeet P. Singh,Cardiac Arrhythmia Service, Cardiology Division, Gray Building 109,Massachusetts General Hospital Heart Center, 55 Fruit Street, Boston, MA02114. E-mail address: [email protected]. (Received January 23, 2011;
accepted February 22, 2011.). doi:10.1016/j.hrthm.2011.02.033
bdma
5coerMD
vBn
for repo
995Hayward et al Electrogram Ablation for AF
More recently, the targeting of specific sites within theatria that contain electrogram fractionation has been de-scribed as a technique for terminating AF.9 These sites,termed complex fractionated atrial electrograms (CFAEs),are areas where electrograms are rapid and multiphasic orcontinuous and are thought to be important drivers for themaintenance of AF. Ablation of CFAEs has been proposedas a way to improve the success of PVI,10-18 but the addedenefit remains unclear. We conducted a meta-analysis toetermine the effect of adding ablation of CFAEs to pul-onary vein isolation (PVI) for patients with paroxysmal
nd nonparoxysmal AF.
MethodsSearch strategyWe performed an electronic literature search of MEDLINE(1950 to March 27, 2010), MEDLINE In-Process and otherNon-Indexed Citations, EMBASE (all years, searchedMarch 28, 2010), the Cochrane Database of SystematicReviews (February 2010), and the Cochrane Central Reg-ister of Controlled Trials (first quarter 2010). Search strat-egies were developed with the help of a research librarianand are published as an Online Data Supplement. We alsomanually searched the bibliographies of the selected publi-cations, our personal archives, and review articles publishedin the last 5 years on catheter ablation for AF.
EligibilityRandomized trials or controlled clinical trials that comparedelectrical isolation of the pulmonary veins to the sameprocedure with additional ablation of CFAEs were included.To be included, studies were required to report on the endpoint of freedom from atrial tachyarrhythmia (AT) or AF atleast 3 months postprocedure. There were no language re-strictions, and incomplete information (abstracts, brief re-ports) could be included as long as it met all other inclusioncriteria. Ablation could be performed as a first-line therapyor after failure of antiarrhythmic drugs. Any method ofisolation of the pulmonary veins (including PVI or pulmo-nary vein antrum isolation [PVAI]) was accepted as long aselectrical isolation of the pulmonary veins was confirmed.Additional anatomical ablation lines performed after PVIwere allowed as long as these were performed for both
Figure 1 Search flow diagram
groups. CFAEs could be defined, identified, and ablated in a
any manner, and this could be performed before or afterPVI.
End pointsThe primary end point was freedom from atrial arrhythmiaoff antiarrhythmic drugs. If the end point was unclear, theauthors were contacted directly for clarification. Repeatprocedures were not allowed (and were considered fail-ure to reach the primary end point if they occurred).Secondary end points were procedure time, fluoroscopytime, all-cause mortality, pericardial tamponade, andthromboembolic events. For the purpose of this analysis,pericardial tamponade was defined as any pericardialeffusion requiring percutaneous or surgical drainage.
Data extractionData extraction was performed independently by 2 inves-tigators, and results were recorded on a standardized dataextraction form. Disagreements were resolved by consen-sus.
Data analysisDichotomous outcomes were analyzed using the DerSimo-nian and Laird random effects model. We explored hetero-geneity by visually inspecting the outcome plots and thencalculating the I2 statistic as well as the �2 statistic; I2�0% indicated significant heterogeneity. Statistical signifi-ance was set at � � 0.05. If significant heterogeneity wasbserved, we explored this by repeating the analysis whilexcluding studies with methodological differences from theest. All statistical analysis was performed using Review
anager 5.0.21 (The Cochrane Collaboration, Copenhagen,enmark).Procedure time and fluoroscopy time, both continuous
ariables, were also analyzed using a random-effects model.etween-study variance was estimated using the DerSimo-ian and Laird method.
ResultsSearch resultsOur electronic search identified 481 potentially eligible ref-erences; 8 of these met our inclusion criteria (Figure 1). Ofthese, 5 were randomized controlled trials,19-23 2 usedmatched historical controls,24,25 and 1 study performed PVI
rts included in the meta-analysis.
nd CFAE in 30 consecutive patients followed by PVI alone
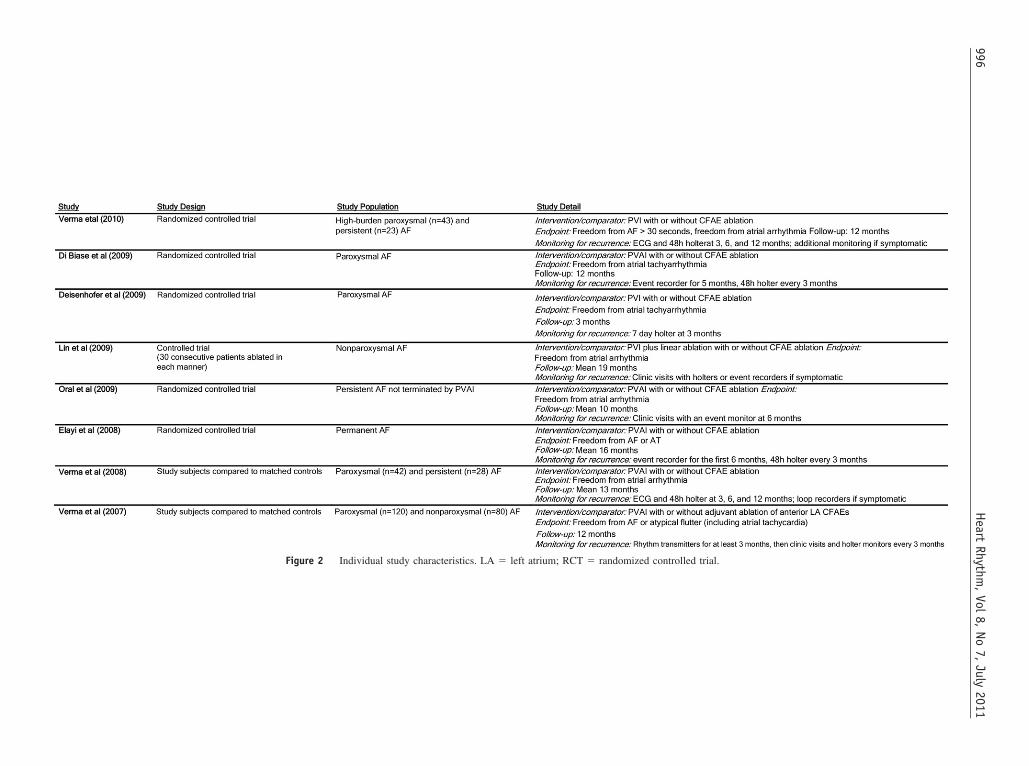
Figure 2 Individual study characteristics. LA � left atrium; RCT � randomized controlled trial.
996H
eartRhythm
,Vol
8,No
7,July
2011
(tada
cty
PFutOnson
h.rc
NFmctocP
ythmia
997Hayward et al Electrogram Ablation for AF
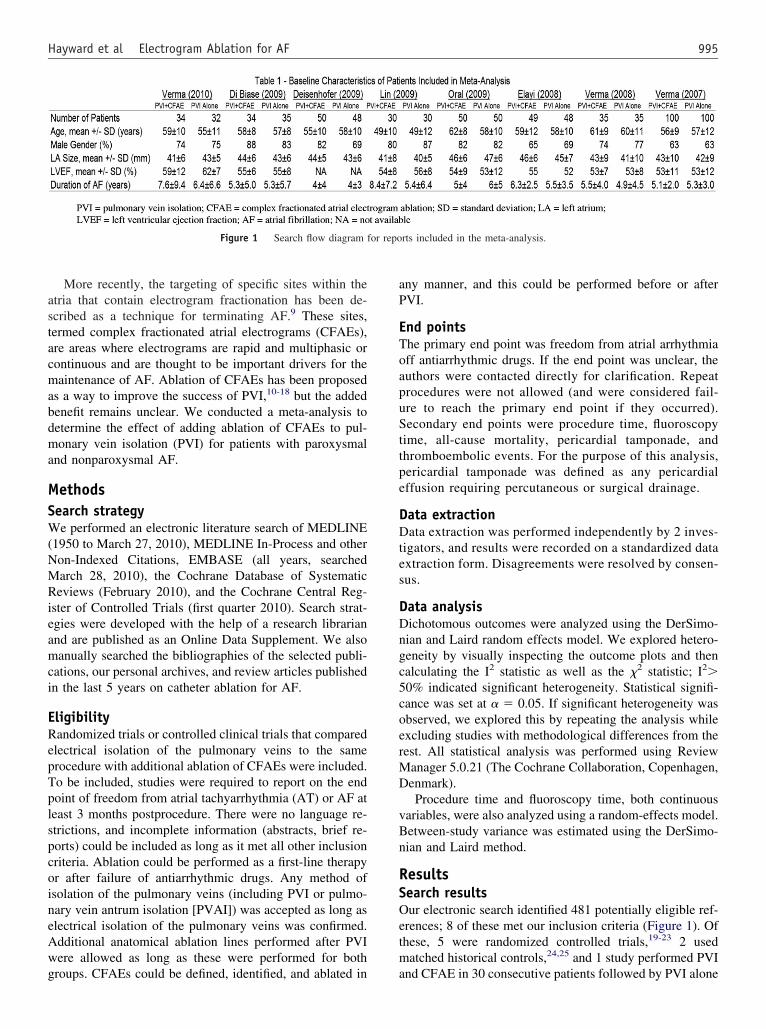
in 30 consecutive patients.26 There were 2 studies of patientswith paroxysmal AF, 3 studies of patients with nonparoxysmalAF, and 3 studies of patients with both paroxysmal andnonparoxysmal AF (Figure 2). Table 1 summarizes the base-line characteristics of the patients in the included studies. These8 studies represent a total of 760 patients; 372 had paroxysmalAF and 388 had nonparoxysmal AF. The mean age of thepatients was 57 years, and 74% were male. The mean left atrialdimension was 43 mm, and the average duration of AF was 5.6years; 378 patients underwent PVI alone, and 382 underwentPVI�CFAE.
Of note, a single investigator (A. Verma) was the leadauthor on 3 of the included trials. However, the subjects inthese trials did not overlap, and 2 of these trials weremulticenter studies.
Primary outcomes
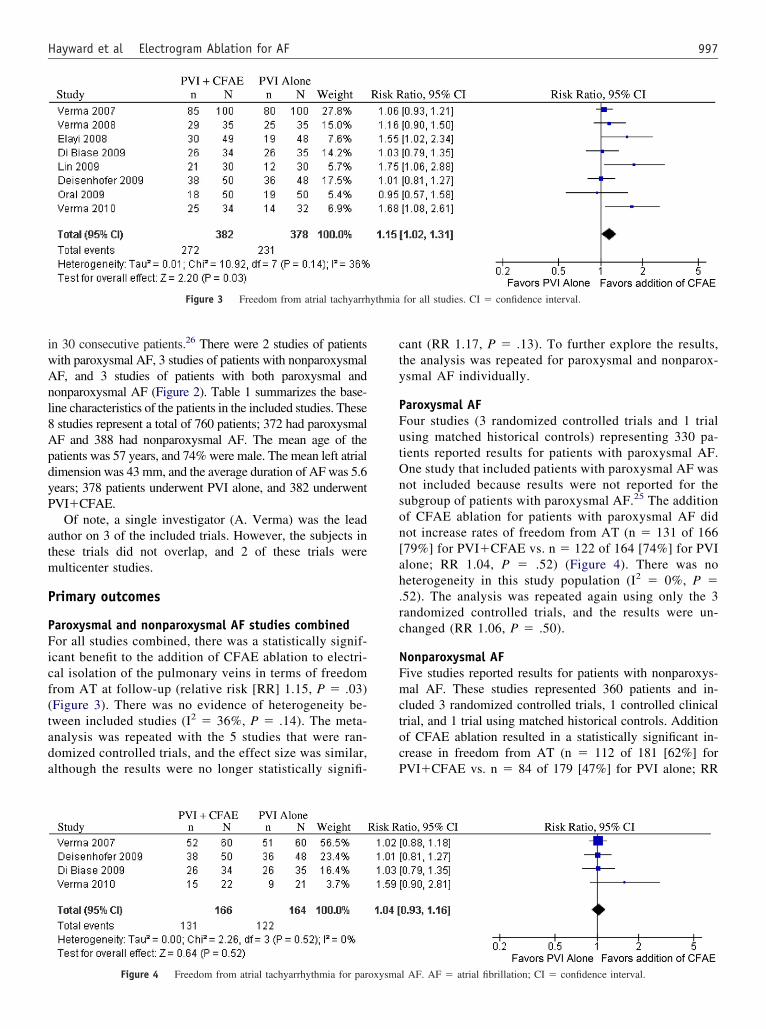
Paroxysmal and nonparoxysmal AF studies combinedFor all studies combined, there was a statistically signif-icant benefit to the addition of CFAE ablation to electri-cal isolation of the pulmonary veins in terms of freedomfrom AT at follow-up (relative risk [RR] 1.15, P � .03)Figure 3). There was no evidence of heterogeneity be-ween included studies (I2 � 36%, P � .14). The meta-nalysis was repeated with the 5 studies that were ran-omized controlled trials, and the effect size was similar,lthough the results were no longer statistically signifi-
Figure 3 Freedom from atrial tachyarrh
Figure 4 Freedom from atrial tachyarrhythmia for paroxysma
ant (RR 1.17, P � .13). To further explore the results,he analysis was repeated for paroxysmal and nonparox-smal AF individually.
aroxysmal AFour studies (3 randomized controlled trials and 1 trialsing matched historical controls) representing 330 pa-ients reported results for patients with paroxysmal AF.ne study that included patients with paroxysmal AF wasot included because results were not reported for theubgroup of patients with paroxysmal AF.25 The additionf CFAE ablation for patients with paroxysmal AF didot increase rates of freedom from AT (n � 131 of 166
[79%] for PVI�CFAE vs. n � 122 of 164 [74%] for PVIalone; RR 1.04, P � .52) (Figure 4). There was no
eterogeneity in this study population (I2 � 0%, P �52). The analysis was repeated again using only the 3andomized controlled trials, and the results were un-hanged (RR 1.06, P � .50).
onparoxysmal AFive studies reported results for patients with nonparoxys-al AF. These studies represented 360 patients and in-
luded 3 randomized controlled trials, 1 controlled clinicalrial, and 1 trial using matched historical controls. Additionf CFAE ablation resulted in a statistically significant in-rease in freedom from AT (n � 112 of 181 [62%] forVI�CFAE vs. n � 84 of 179 [47%] for PVI alone; RR
for all studies. CI � confidence interval.
l AF. AF � atrial fibrillation; CI � confidence interval.
.cl
aroxysm
998 Heart Rhythm, Vol 8, No 7, July 2011
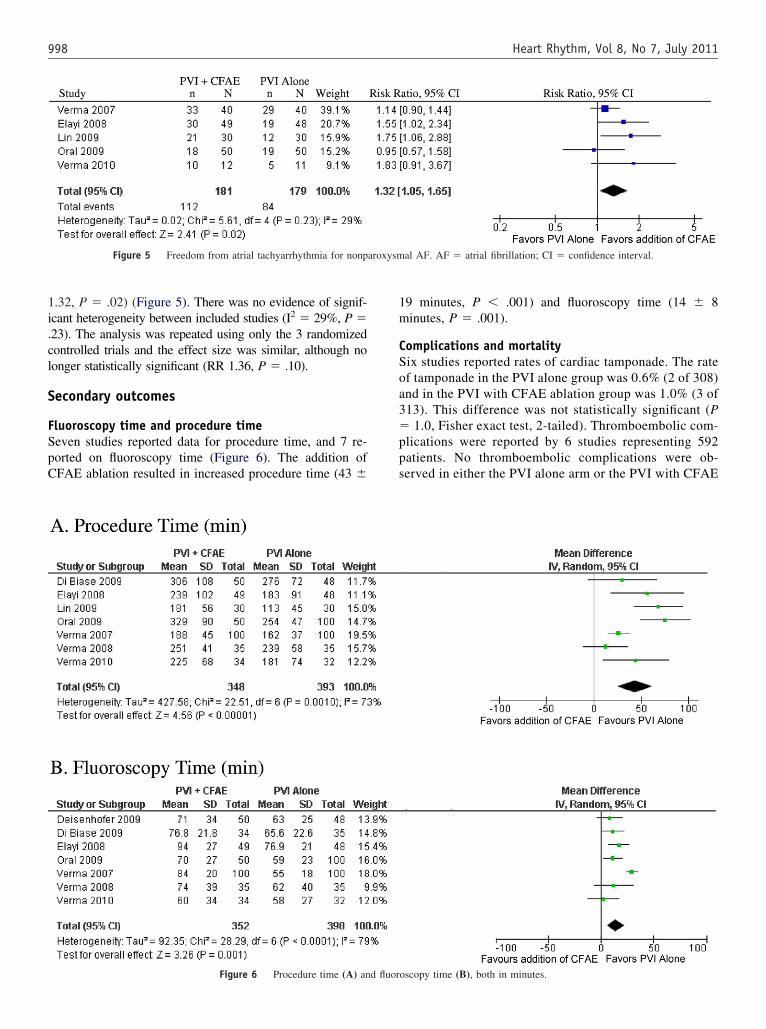
1.32, P � .02) (Figure 5). There was no evidence of signif-icant heterogeneity between included studies (I2 � 29%, P �23). The analysis was repeated using only the 3 randomizedontrolled trials and the effect size was similar, although noonger statistically significant (RR 1.36, P � .10).
Secondary outcomes
Fluoroscopy time and procedure timeSeven studies reported data for procedure time, and 7 re-ported on fluoroscopy time (Figure 6). The addition ofCFAE ablation resulted in increased procedure time (43 �
Figure 5 Freedom from atrial tachyarrhythmia for nonp
Figure 6 Procedure time (A) and fluor
19 minutes, P � .001) and fluoroscopy time (14 � 8minutes, P � .001).
Complications and mortalitySix studies reported rates of cardiac tamponade. The rateof tamponade in the PVI alone group was 0.6% (2 of 308)and in the PVI with CFAE ablation group was 1.0% (3 of313). This difference was not statistically significant (P� 1.0, Fisher exact test, 2-tailed). Thromboembolic com-plications were reported by 6 studies representing 592patients. No thromboembolic complications were ob-served in either the PVI alone arm or the PVI with CFAE
al AF. AF � atrial fibrillation; CI � confidence interval.
oscopy time (B), both in minutes.

tsCfaAtosceu
ti9ce
fsp
fsatts
tim
i
999Hayward et al Electrogram Ablation for AF
ablation arm. No deaths were reported by any of theincluded studies (although not all studies reported ondeaths at follow-up).
DiscussionMain findingsIn this meta-analysis of controlled trials comparing PVIalone vs. PVI with CFAE ablation for AF, we found thatthe addition of CFAE ablation to PVI results in a statis-tically significant increase in freedom from AT at fol-low-up for subjects with nonparoxysmal, but not parox-ysmal, AF. The added benefit of CFAE ablation comes atthe cost of increased procedure time and increased fluo-roscopy time. There was no statistically significant dif-ference in the rate of tamponade, and the rate of othercomplications was low enough to prohibit statistical anal-ysis. To our knowledge, this is the first meta-analysisaddressing these questions.
PVI aims to electrically isolate the pulmonary veinsand thus the triggers of AF. This procedure has resultedin high success rates for paroxysmal AF, but is inade-quate for many patients with nonparoxysmal AF. As AFmoves from the paroxysmal to the nonparoxysmal state,the atria undergo both structural and electrical remodel-ing, resulting in areas of fibrosis and slowed conduction.These structural changes facilitate anisotropy, and theassociated pivoting and colliding of wavelets, which re-sult in regions with fractionated electrograms. It was firstproposed by Konings et al27 that these areas are critical tohe persistence of AF. Nademanee et al9 were the first tohow that substrate modification through ablation ofFAEs could be used to terminate AF. As AF moves
rom the paroxysmal to the persistent state, abnormaltrial substrate plays a larger role in the persistence ofF. As a result, simply isolating the pulmonary vein
riggers of AF may not be sufficient to prevent recurrencef nonparoxysmal AF. In this meta-analysis, targetedubstrate ablation was shown to improve procedural out-omes for patients with nonparoxysmal AF, possibly byliminating the specific substrate responsible for perpet-ation of AF in these patients.
In the pooled analysis of studies of nonparoxysmal AF,he use of CFAE ablation as an adjunct to PVI resulted in anncrease in freedom from AT at follow-up (RR ratio 1.32,5% confidence interval 1.05 to 1.65). This analysis in-luded 5 studies, 4 of which showed improved long-termfficacy over anatomical ablation alone. Oral et al22 found
no improvement in outcome with the addition of CFAEablation. This study differed from the others in the group inseveral ways. First, the study population had larger leftatrial diameters (4.65 cm on average vs. 4.29 cm for theother studies), and the success rates of the procedures werelower. Given this, the patient population may have had moreadvanced AF that was less suitable for ablation in general,biasing against an effect. Finally, the investigators limitedCFAE ablation to 2 hours or stopped ablating CFAEs when
AF terminated.In the pooled analysis of studies of paroxysmal AF, theuse of CFAE ablation as an adjunct to PVI did not result inan increase in freedom from AT at follow-up (RR ratio 1.04,95% confidence interval 0.93 to 1.16). One of the 4 studies,Verma et al,19 showed a nonsignificant trend toward benefitrom the combined approach (P � .14). Interestingly, thistudy included patients with high-burden paroxysmal AF,ossibly accounting for this trend.
Study limitationsMeta-analysis was developed for application to randomizedtrials. However, there has been a recent trend in the use ofmeta-analysis for nonrandomized studies.28 To address theact that we included nonrandomized data, we performed aensitivity analysis by repeating each part of the meta-nalysis using only the data from randomized controlledrials. The effect sizes remained remarkably consistent, al-hough the statistically significant findings were no longerignificant with the smaller number of included studies.
The second limitation of this study was the variation inhe technique of ablation between centers. Different stud-es used different methods to electrically isolate the pul-onary veins (PVI or PVAI). One study, Lin et al26
performed linear ablation by an anatomic approach afterPVI. In addition, the definition of CFAEs, the method ofidentification of CFAEs (visual identification or auto-mated mapping), and the method of CFAE ablation dif-fered between studies. For example, the study by Vermaet al24 limited CFAE ablation for the anterior left atriumand the anterior septum, whereas the study by Deisen-hofer et al21 performed a more extensive CFAE ablationnvolving both the left and right atria. Oral et al22 limited
CFAE ablation to 2 hours. However, the average addi-tional procedure time for CFAE ablation was only 75minutes, which was similar to the other included studiesand comfortably below their 2-hour limit.
Another limitation of this study was the variation on thelength of follow-up. Deisenhofer et al21 had only 3 months offollow-up. In their study, 2 subjects who were classified asprocedural successes at 3 months later developed atrial tachy-cardias that required ablation. These patients would have beenconsidered treatment failures in any of the other studies thathad a longer period of follow-up. The study by Lin et al26 haddifferent follow-up durations for the intervention and controlgroups. By chance, this did not affect the analysis because bothcurves reached a plateau by 15 months.
A final limitation is that Verma et al19 had a smallpercentage of patients still on antiarrhythmic drugs atfollow-up. This was allowed in this analysis for 3 rea-sons: the study protocol specified that patients should betaken off antiarrhythmic drugs after 2 months, a highpercentage (96%) of subjects considered to have a suc-cessful postablation outcome were off antiarrhythmicdrugs, and the small number of subjects still on antiar-rhythmic drugs were evenly distributed between the
groups.
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
1000 Heart Rhythm, Vol 8, No 7, July 2011
ConclusionIn this meta-analysis of randomized controlled trials and con-trolled clinical trials, addition of CFAE ablation to PVI resultsin greater improvement in freedom from atrial arrhythmia forpatients with nonparoxysmal AF, but not for patients withparoxysmal AF. This improvement comes at the cost of longerfluoroscopy time and procedure time. This analysis providesanother piece of evidence that CFAE ablation may be a usefuladjunct to PVI for patients with nonparoxysmal but not par-oxysmal AF. The analysis was limited by the retrospectivenature of some of the studies in addition to variation in thetechnique of ablation between centers. More randomized trialsare needed to fully evaluate the benefits of CFAE ablation.
AcknowledgementsThe authors thank Eric A. Macklin, PhD, for his assistancein creating a random-effects model to analyze proceduretime and fluoroscopy time.
AppendixSupplementary dataSupplementary data associated with this article can befound, in the online version, at doi:10.1016/j.hrthm.2011.02.033.
References1. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation
in adults: national implications for rhythm management and stroke prevention:the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study.JAMA 2001;285:2370–2375.
2. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent riskfactor for stroke: the Framingham Study. Stroke 1991;22:983–988.
3. Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D.Impact of atrial fibrillation on the risk of death: the Framingham Heart Study.Circulation 1998;98:946–952.
4. Haissaguerre M, Jais P, Shah DC, et al. Spontaneous initiation of atrial fibril-lation by ectopic beats originating in the pulmonary veins. N Engl J Med1998;339:659–666.
5. Hocini M, Sanders P, Jais P, et al. Techniques for curative treatment of atrialfibrillation. J Cardiovasc Electrophysiol 2004;15:1467–1471.
6. Pappone C, Augello G, Sala S, et al. A randomized trial of circumferentialpulmonary vein ablation vs. antiarrhythmic drug therapy in paroxysmal atrialfibrillation: the APAF study. J Am Coll Cardiol 2006;48:2340–2347.
7. Jais P, Cauchemez B, Macle L, et al. Catheter ablation vs. antiarrhythmic drugsfor atrial fibrillation: the A4 study. Circulation 2008;118:2498–2505.
8. Wazni OM, Marrouche NF, Martin DO, et al. Radiofrequency ablation vsantiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: arandomized trial. JAMA 2005;293:2634–2640.
9. Nademanee K, McKenzie J, Kosar E, et al. A new approach for catheter ablationof atrial fibrillation: mapping of the electrophysiologic substrate. J Am CollCardiol 2004;43:2044–2053.
10. Estner HL, Hessling G, Ndrepepa G, et al. Acute effects and long-termoutcome of pulmonary vein isolation in combination with electrogram-
guided substrate ablation for persistent atrial fibrillation. Am J Cardiol2008;101:332–337.
1. Mansour M, Forleo GB, Pappalardo A, et al. Combined use of cryoballoon andfocal open-irrigation radiofrequency ablation for treatment of persistent atrialfibrillation: results from a pilot study. Heart Rhythm 2010;7:452–458.
2. Nair M, Nayyar S, Rajagopal S, Balachander J, Kumar M. Results of radiofre-quency ablation of permanent atrial fibrillation of �2 years duration and leftatrial size �5 cm using 2-mm irrigated tip ablation catheter and targeting areasof complex fractionated atrial electrograms. Am J Cardiol 2009;104:683–688.
3. Oral H, Chugh A, Good E, et al. A tailored approach to catheter ablation ofparoxysmal atrial fibrillation. Circulation 2006;113:1824–1831.
4. Porter M, Spear W, Akar JG, et al. Prospective study of atrial fibrillationtermination during ablation guided by automated detection of fractionated elec-trograms. J Cardiovasc Electrophysiol 2008;19:613–620.
5. Scharf C, Boersma L, Davies W, et al. Ablation of persistent atrial fibrillationusing multielectrode catheters and duty-cycled radiofrequency energy. J AmColl Cardiol 2009;54:1450–1456.
6. Takahashi Y, O’Neill MD, Hocini M, et al. Characterization of electrogramsassociated with termination of chronic atrial fibrillation by catheter ablation.J Am Coll Cardiol 2008;51:1003–1010.
7. Tondo C, Forleo GB, Pappalardo A, et al. A combined cryoenergy andradiofrequency approach to catheter ablation of persistent atrial fibrillation:preliminary results from a pilot study. J Cardiovasc Electrophysiol 2009;20:S27–S28.
8. Wang X, Liu X, Shi H, et al. Heart rhythm disorders and pacemakers: pulmonaryvein isolation combined with substrate modification for persistent atrial fibrillationtreatment in patients with valvular heart diseases. Heart 2009;95:1773–1783.
9. Verma A, Mantovan R, Macle L, et al. Substrate and Trigger Ablation forReduction of Atrial Fibrillation (STAR AF): a randomized, multicentre, inter-national trial. Eur Heart J 2010;31(11):1344–56.
0. Di Biase L, Elayi CS, Fahmy TS, et al. Atrial fibrillation ablation strategies forparoxysmal patients: randomized comparison between different techniques. CircArrhythm Electrophysiol 2009;2:113–119.
1. Deisenhofer I, Estner H, Reents T, et al. Does electrogram guided substrateablation add to the success of pulmonary vein isolation in patients with parox-ysmal atrial fibrillation? A prospective, randomized study. J Cardiovasc Elec-trophysiol 2009;20:514–521.
2. Oral H, Chugh A, Yoshida K, et al. A randomized assessment of the incrementalrole of ablation of complex fractionated atrial electrograms after antral pulmo-nary vein isolation for long-lasting persistent atrial fibrillation. J Am CollCardiol 2009;53:782–789.
3. Elayi CS, Verma A, Di Biase L, et al. Ablation for longstanding permanent atrialfibrillation: results from a randomized study comparing three different strategies.Heart Rhythm 2008;5:1658–1664.
4. Verma A, Patel D, Famy T, et al. Efficacy of adjuvant anterior left atrial ablationduring intracardiac echocardiography-guided pulmonary vein antrum isolationfor atrial fibrillation. J Cardiovasc Electrophysiol 2007;18:151–156.
5. Verma A, Novak P, Macle L, et al. A prospective, multicenter evaluation ofablating complex fractionated electrograms (CFEs) during atrial fibrillation (AF)identified by an automated mapping algorithm: acute effects on AF and efficacyas an adjuvant strategy. Heart Rhythm 2008;5:198–205.
6. Lin YJ, Tai CT, Chang SL, et al. Efficacy of additional ablation of complexfractionated atrial electrograms for catheter ablation of nonparoxysmal atrialfibrillation. J Cardiovasc Electrophysiol 2009;20:607–615.
7. Konings KT, Smeets JL, Penn OC, Wellens HJ, Allessie MA. Configuration ofunipolar atrial electrograms during electrically induced atrial fibrillation inhumans. Circulation 1997;95:1231–1241.
8. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observationalstudies in epidemiology: a proposal for reporting. Meta-analysis Of Obser-
vational Studies in Epidemiology (MOOSE) group. JAMA 2000;283:2008 –2012.