powerpoint presentation july 2016... · jin et al int j hem 2015 37 iron chelation • deferasirox...
TRANSCRIPT
7/12/2016
1
1
New Directions in Aplastic Anemia:
What's on the Horizon?
Amy E. DeZern, MD; MHS
Assistant Professor
Hematologic Malignancies
Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
Baltimore, MD
Objectives
• To provide information on new concepts
emerging in AA in somatic molecular
testing
• To review updates on markers of
response to therapy in AA
• To review newer data on emerging
therapies in aplastic anemia (AA)
TESTING
July 12, 2016 3
Better way to evaluate clonal
evolution?
• As survival is improving, we may see
more late development of MDS/AML in
≥15% of patients clonal evolution
• Extrapolation from MDS field somatic
mutational testing
• Goal: to use this testing to ID group of
AA pts more likely to get MDS
(treatment would be modified)
Kulasekararaj et al. Blood 2014
Yoshizato et al. NEJM 2015
4
The Dawn of the Molecular Era of
the Myelodysplastic Syndromes• 51% of patients ≥1 mutation (including ~50% with
normal karyotype)
• FIVE genes (in ~30% of pts) independent
prognostic significance and predicted poor overall
survival
– EZH2 ETV6 RUNX1 ASXL1 P53
Bejar et al NEJM
2011
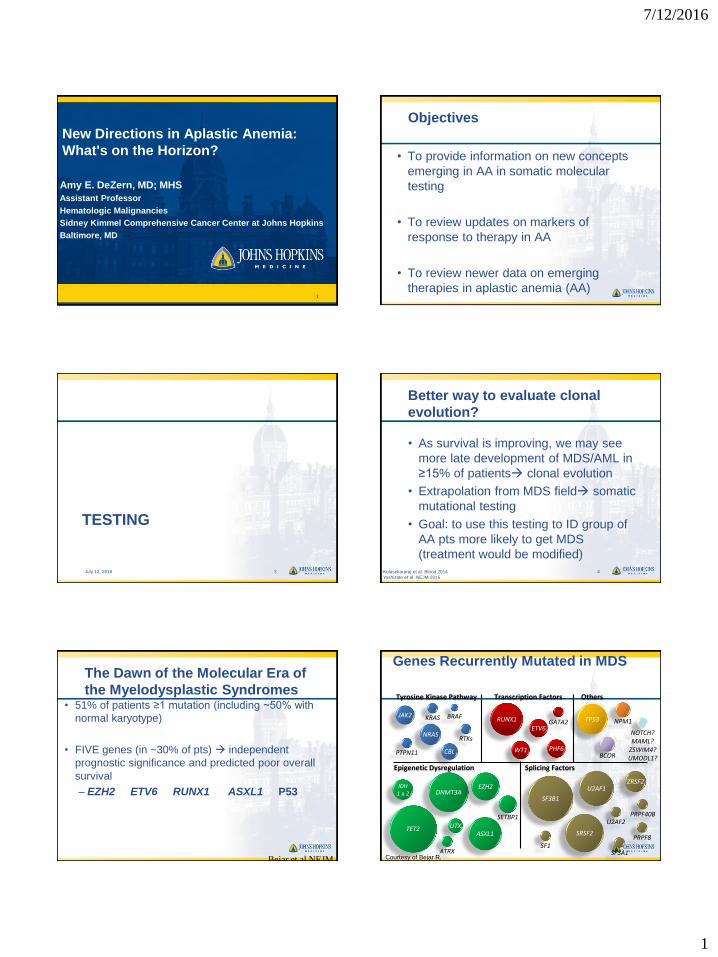
RUNX1
ETV6
WT1 PHF6
GATA2
DNMT3AEZH2
ASXL1
IDH1 & 2
UTX
TP53
Transcription FactorsTyrosine Kinase Pathway
Epigenetic Dysregulation
SF3B1
Splicing Factors
JAK2
NRAS
BRAFKRAS
RTKs
PTPN11
NOTCH?MAML?
ZSWIM4?UMODL1?
CBL
NPM1
ATRX
Others
SRSF2
U2AF1ZRSF2
SETBP1
SF1SF3A1
PRPF40BU2AF2
PRPF8
BCOR
TET2
Genes Recurrently Mutated in MDS
Courtesy of Bejar R.
7/12/2016
2
Retrospective from the UK
• From UK: looked at 150 pts with no
evidence (by microscope) of MDS
• Screen for mutations
– ASXL1, DNMT3A, BCOR, TET2, MPL at least
– 19% AA pts had mutations
– Pts with mutations had a longer disease
duration (37 vs. 8 months, p<0.04)
– AA patients with disease duration of > 6 mos
AND mutation40% risk of transformation to
MDS (p <0.0002) 7
Kulasekararaj et al. Blood 2014
Candidate gene mutations in acquired
aplastic anemia - correlation with survival
and clonal evolution to myelodysplastic
syndrome-courtesy of Dr. Dumitriu
Yoshizato et al. NEJM 2015
NIH SAA cohort
Time
De novo
MDS/AML
“Stable AA” – responders or
non-responders to
immunosuppressive therapySAA
6 months after IST
≈ 15% clonal evolution to MDS/AML
Clonal evolution
N = 256 patients (3 institutions)Yoshizato et al. NEJM 2015
ACQUIRED MUTATIONS IN SAA – NIH COHORT (n=256)
0 1 2 >2
Number mutations
per SAA patient
65%
23%
7%
5%
0%
25%
50%
75%
100%
Epigenesis Transcription
factor Signal
transduction Others
DNA
repair Receptor
Ribosomal
protein
AEBP2 ATM BRAF CDAN1 FANCA FLT3 RPL11 ASXL1 BCOR CSMD1 CDH23 FANCC KIT RPL35a ATRX BCORL1 GNAS DIS3 FANCD1 GCSFR RPL5 DNMT3A CEBPA GPRC5A DKC1 FANCD2 MPL RPS10 EED CTCF JAK1 ELANE FANCE RPS19 EZH1 CUX1 JAK2 ETNK1 FANCG RPS26 EZH2 DAXX JAK3 LAMB4 IDH1 Dido1 KRAS LUC7L2 Telomere Splicing Cohesin IDH2 ETV6 LNK PEG3 NHP2 DDX41 RAD21 JARID2 GATA1 MAP3K4 PIGA NOP10 PRPF8 SMC1A KDM6A GATA2 NF1 PRF1 POT1 SF3B1 SMC3 RBBP4 IRF1 NRAS SBDS RAP1 SRSF2 STAG2 RBBP7 NCOR2 PTPN11 SETBP1 RTEL1 U2AF1 SUZ12 NPM1 RIT1 UMODL1 TERC U2AF2 Ubiquitin TET2 PHF6 SRP72 ZSWIM4 TERF1 ZRSR2 BRCC3
Rb STAT3 TERF2 CBL RUNX1 TERT FBXW7 TP53 TINF2 WT1 TPP1
Targeted gene panel
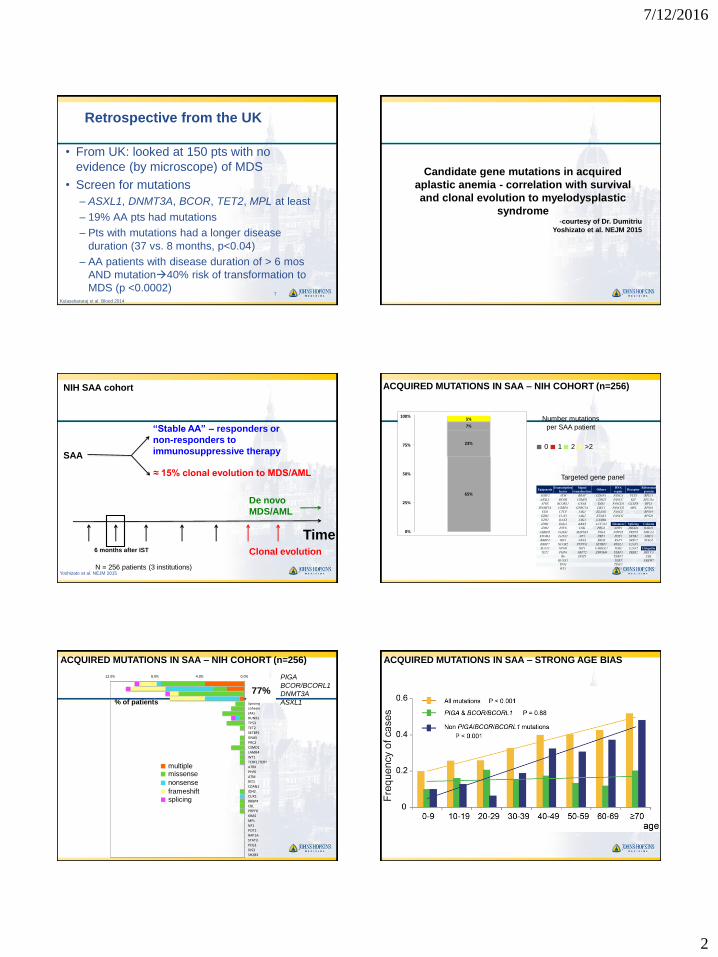
ACQUIRED MUTATIONS IN SAA – NIH COHORT (n=256)
0.0%4.0%8.0%12.0%
PIGA
BCOR/BCORL1
DNMT3A
ASXL1
Splicing
cohesin
JAKs
RUNX1
TP53
TET2
SETBP1
GNAS
PRC2
CSMD1
LAMB4
WT1
TERF1/TERT
ATRX
PHF6
ATM
RIT1
CDAN1
IDH2
CUX1
RBBP4
CBL
PRPF8
KRAS
MPL
NF1
POT1
RAP1A
STAT3
PEG3
DIS3
SH2B3
77%% of patients
multiplemissense
nonsense
frameshiftsplicing
PIGA
BCOR/BCORL1
DNMT3A
ASXL1
ACQUIRED MUTATIONS IN SAA – STRONG AGE BIAS
7/12/2016
3
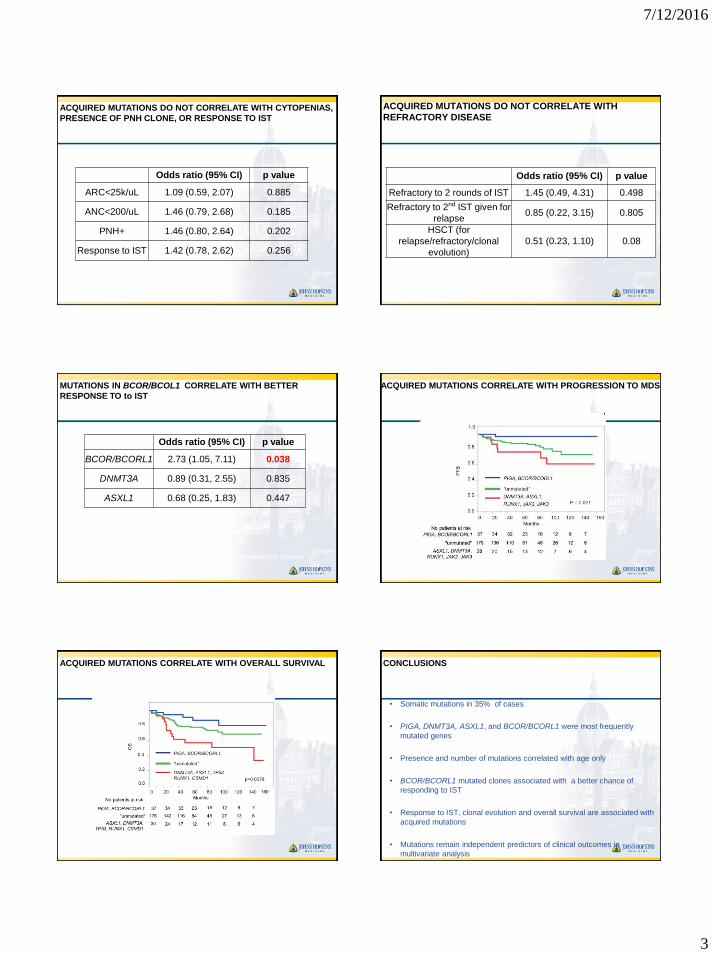
Odds ratio (95% CI) p value
ARC<25k/uL 1.09 (0.59, 2.07) 0.885
ANC<200/uL 1.46 (0.79, 2.68) 0.185
PNH+ 1.46 (0.80, 2.64) 0.202
Response to IST 1.42 (0.78, 2.62) 0.256
ACQUIRED MUTATIONS DO NOT CORRELATE WITH CYTOPENIAS,
PRESENCE OF PNH CLONE, OR RESPONSE TO IST
Odds ratio (95% CI) p value
Refractory to 2 rounds of IST 1.45 (0.49, 4.31) 0.498
Refractory to 2nd IST given for
relapse0.85 (0.22, 3.15) 0.805
HSCT (for
relapse/refractory/clonal
evolution)
0.51 (0.23, 1.10) 0.08
ACQUIRED MUTATIONS DO NOT CORRELATE WITH
REFRACTORY DISEASE
Odds ratio (95% CI) p value
BCOR/BCORL1 2.73 (1.05, 7.11) 0.038
DNMT3A 0.89 (0.31, 2.55) 0.835
ASXL1 0.68 (0.25, 1.83) 0.447
MUTATIONS IN BCOR/BCOL1 CORRELATE WITH BETTER
RESPONSE TO to IST
None of these mutations correlate with clonal evolution/refractory disease
OS
0.0
0.4
0.2
1.0
0.6
0.8
ACQUIRED MUTATIONS CORRELATE WITH PROGRESSION TO MDS
OS
0.0
0.4
0.2
1.0
0.6
0.8
ACQUIRED MUTATIONS CORRELATE WITH OVERALL SURVIVAL CONCLUSIONS
• Somatic mutations in 35% of cases
• PIGA, DNMT3A, ASXL1, and BCOR/BCORL1 were most frequently
mutated genes
• Presence and number of mutations correlated with age only
• BCOR/BCORL1 mutated clones associated with a better chance of
responding to IST
• Response to IST, clonal evolution and overall survival are associated with
acquired mutations
• Mutations remain independent predictors of clinical outcomes in
multivariate analysis
7/12/2016
4
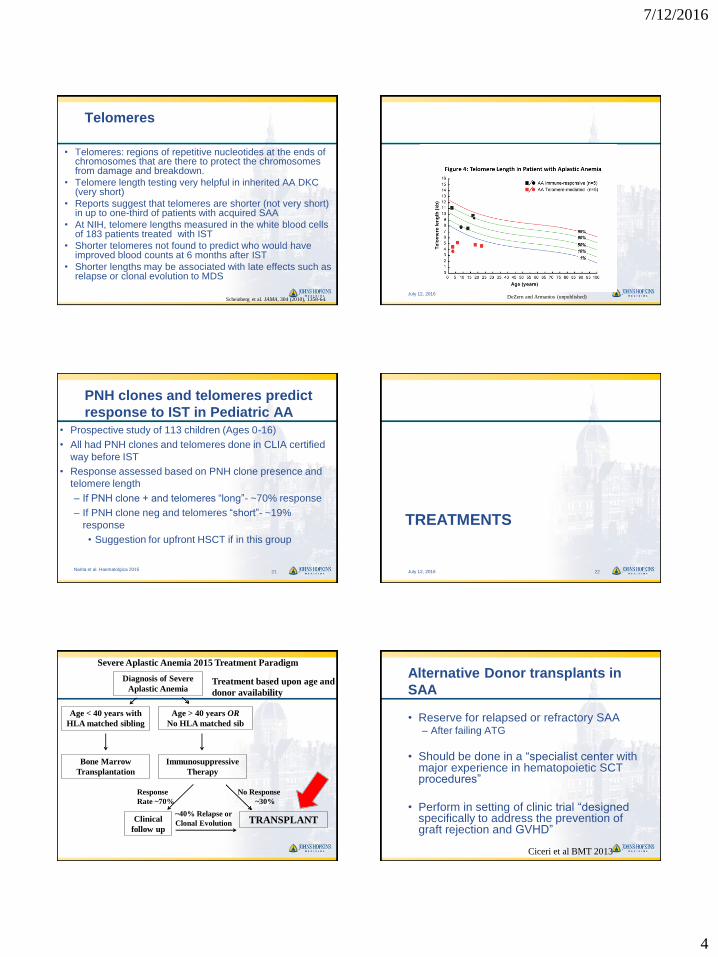
Telomeres
• Telomeres: regions of repetitive nucleotides at the ends of chromosomes that are there to protect the chromosomes from damage and breakdown.
• Telomere length testing very helpful in inherited AA DKC (very short)
• Reports suggest that telomeres are shorter (not very short) in up to one-third of patients with acquired SAA
• At NIH, telomere lengths measured in the white blood cells of 183 patients treated with IST
• Shorter telomeres not found to predict who would have improved blood counts at 6 months after IST
• Shorter lengths may be associated with late effects such as relapse or clonal evolution to MDS
Scheinberg et al. JAMA, 304 (2010), 1358-64.July 12, 2016
DeZern and Armanios (unpublished)
PNH clones and telomeres predict
response to IST in Pediatric AA
• Prospective study of 113 children (Ages 0-16)
• All had PNH clones and telomeres done in CLIA certified
way before IST
• Response assessed based on PNH clone presence and
telomere length
– If PNH clone + and telomeres “long”- ~70% response
– If PNH clone neg and telomeres “short”- ~19%
response
• Suggestion for upfront HSCT if in this group
Narita et al. Haematolgica 201521
TREATMENTS
July 12, 2016 22
Severe Aplastic Anemia 2015 Treatment Paradigm
Bone Marrow
Transplantation
Immunosuppressive
Therapy
No Response
~30%
~40% Relapse or
Clonal Evolution TRANSPLANTClinical
follow up
Response
Rate ~70%
Age < 40 years with
HLA matched sibling
Age > 40 years OR
No HLA matched sib
Diagnosis of Severe
Aplastic AnemiaTreatment based upon age and
donor availability
Alternative Donor transplants in
SAA
• Reserve for relapsed or refractory SAA– After failing ATG
• Should be done in a “specialist center with major experience in hematopoietic SCT procedures”
• Perform in setting of clinic trial “designed specifically to address the prevention of graft rejection and GVHD”
Ciceri et al BMT 2013
7/12/2016
5
Unrelated Donor or Alternative donor
BMT
• The sooner, the better after relapse/ refractoriness noted
• Bone marrow still the best source
• Similar conditioning regimens
• Often in setting of clinical trial
• Unrelated donor (NMDP- “MUDs”)
• Haplo-identical donor (half match)
• Umbilical cord donor
New Trial
July 12, 2016 26
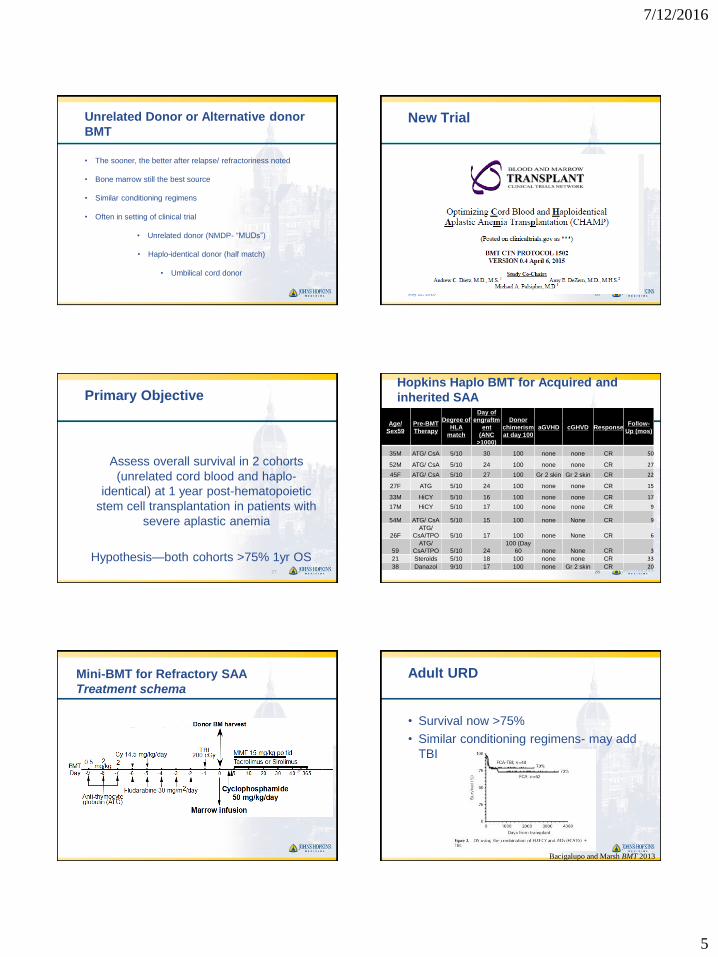
Primary Objective
Assess overall survival in 2 cohorts
(unrelated cord blood and haplo-
identical) at 1 year post-hematopoietic
stem cell transplantation in patients with
severe aplastic anemia
Hypothesis—both cohorts >75% 1yr OS27
Hopkins Haplo BMT for Acquired and
inherited SAA
28
Age/
Sex59
Pre-BMT
Therapy
Degree of
HLA
match
Day of
engraftm
ent
(ANC
>1000)
Donor
chimerism
at day 100
aGVHD cGHVD ResponseFollow-
Up (mos)
35M ATG/ CsA 5/10 30 100 none none CR 50
52M ATG/ CsA 5/10 24 100 none none CR 27
45F ATG/ CsA 5/10 27 100 Gr 2 skin Gr 2 skin CR 22
27F ATG 5/10 24 100 none none CR 15
33M HiCY 5/10 16 100 none none CR 17
17M HiCY 5/10 17 100 none none CR 9
54M ATG/ CsA 5/10 15 100 none None CR 9
26F
ATG/
CsA/TPO 5/10 17 100 none None CR 6
59
ATG/
CsA/TPO 5/10 24
100 (Day
60 none None CR 3
21 Steroids 5/10 18 100 none none CR 33
38 Danazol 9/10 17 100 none Gr 2 skin CR 20
Mini-BMT for Refractory SAA
Treatment schema
Adult URD
• Survival now >75%
• Similar conditioning regimens- may add
TBI
Bacigalupo and Marsh BMT 2013
7/12/2016
6
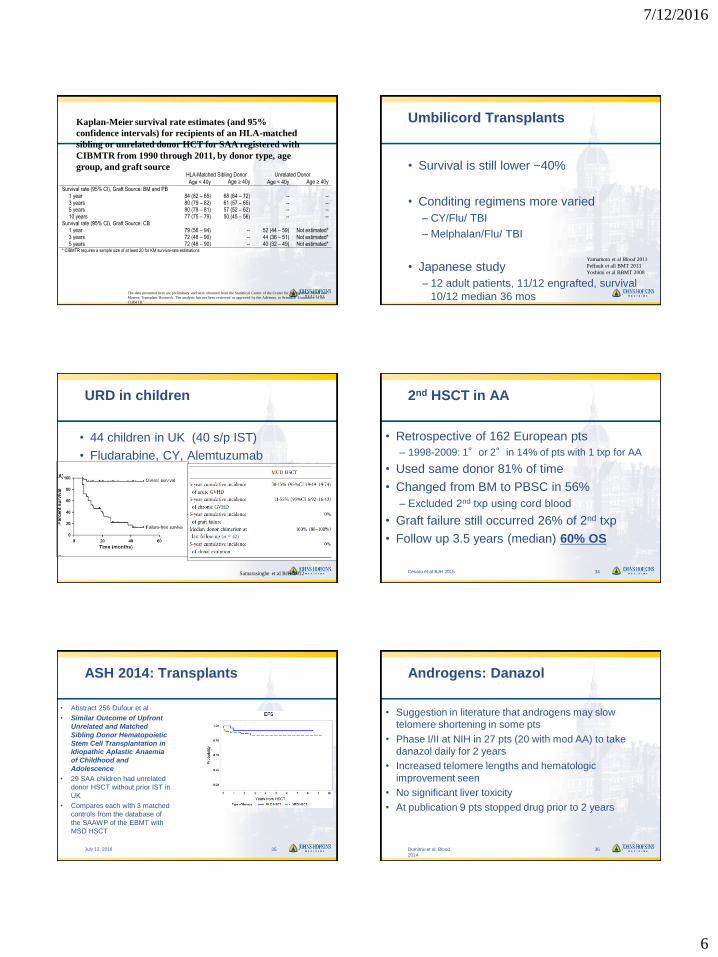
Kaplan-Meier survival rate estimates (and 95%
confidence intervals) for recipients of an HLA-matched
sibling or unrelated donor HCT for SAA registered with
CIBMTR from 1990 through 2011, by donor type, age
group, and graft source HLA-Matched Sibling Donor Unrelated Donor
Age < 40y Age ≥ 40y Age < 40y Age ≥ 40y
Survival rate (95% CI), Graft Source: BM and PB 1 year 84 (82 – 85) 68 (64 – 72) -- -- 3 years 80 (79 – 82) 61 (57 – 65) -- -- 5 years 80 (78 – 81) 57 (52 – 62) -- -- 10 years 77 (75 – 79) 50 (45 – 56) -- -- Survival rate (95% CI), Graft Source: CB 1 year 79 (56 – 94) -- 52 (44 – 59) Not estimated* 3 years 72 (48 – 90) -- 44 (36 – 51) Not estimated* 5 years 72 (48 – 90) -- 40 (32 – 49) Not estimated* * CIBMTR requires a sample size of at least 20 for KM survival-rate estimations
The data presented here are preliminary and were obtained from the Statistical Center of the Center for International Blood and
Marrow Transplant Research. The analysis has not been reviewed or approved by the Advisory or Scientific Committee of the
CIBMTR.’
Umbilicord Transplants
• Survival is still lower ~40%
• Conditing regimens more varied
– CY/Flu/ TBI
– Melphalan/Flu/ TBI
• Japanese study
– 12 adult patients, 11/12 engrafted, survival
10/12 median 36 mos
Yamamoto et al Blood 2011
Peffault et all BMT 2013
Yoshimi et al BBMT 2008
URD in children
• 44 children in UK (40 s/p IST)
• Fludarabine, CY, Alemtuzumab
conditioning
• Overall survival and failure free survival
was 95%
Samarasinghe et al BJH 2012
2nd HSCT in AA
• Retrospective of 162 European pts
– 1998-2009: 1°or 2°in 14% of pts with 1 txp for AA
• Used same donor 81% of time
• Changed from BM to PBSC in 56%
– Excluded 2nd txp using cord blood
• Graft failure still occurred 26% of 2nd txp
• Follow up 3.5 years (median) 60% OS
Cesaro et al BJH 2015 34
ASH 2014: Transplants
• Abstract 256 Dufour et al
• Similar Outcome of Upfront
Unrelated and Matched
Sibling Donor Hematopoietic
Stem Cell Transplantation in
Idiopathic Aplastic Anaemia
of Childhood and
Adolescence
• 29 SAA children had unrelated
donor HSCT without prior IST in
UK
• Compares each with 3 matched
controls from the database of
the SAAWP of the EBMT with
MSD HSCT
July 12, 2016 35
Androgens: Danazol
• Suggestion in literature that androgens may slow
telomere shortening in some pts
• Phase I/II at NIH in 27 pts (20 with mod AA) to take
danazol daily for 2 years
• Increased telomere lengths and hematologic
improvement seen
• No significant liver toxicity
• At publication 9 pts stopped drug prior to 2 years
Dumitriu et al. Blood
2014
36
7/12/2016
7
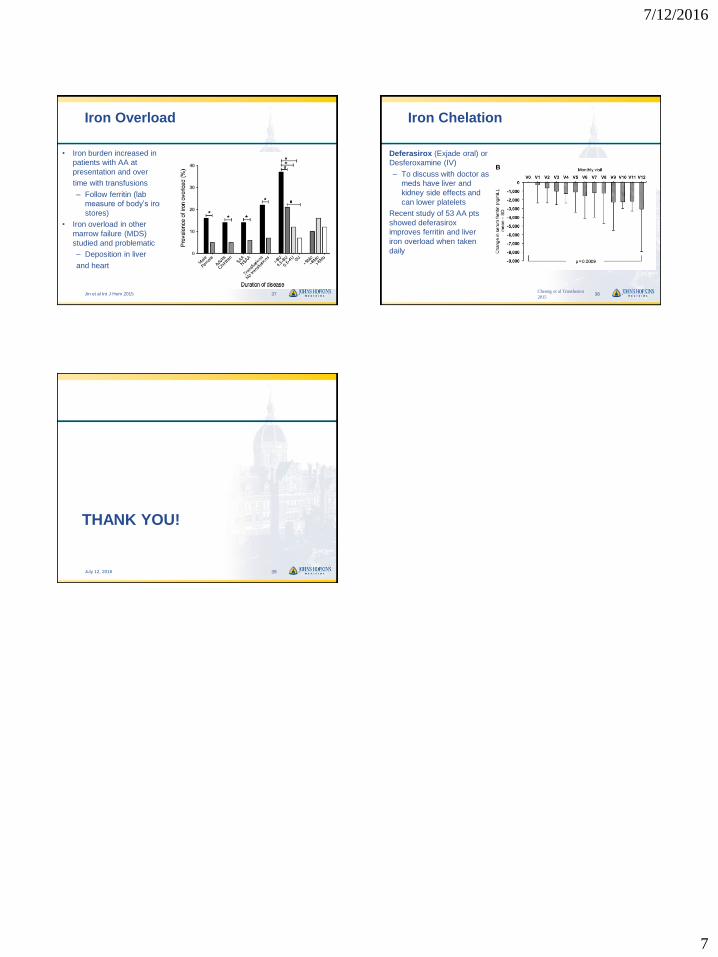
Iron Overload
• Iron burden increased in
patients with AA at
presentation and over
time with transfusions
– Follow ferritin (lab
measure of body’s iron
stores)
• Iron overload in other
marrow failure (MDS)
studied and problematic
– Deposition in liver
and heart
Jin et al Int J Hem 2015 37
Iron Chelation
• Deferasirox (Exjade oral) or
Desferoxamine (IV)
– To discuss with doctor as
meds have liver and
kidney side effects and
can lower platelets
• Recent study of 53 AA pts
showed deferasirox
improves ferritin and liver
iron overload when taken
daily
Cheong et al Transfusion
201538
THANK YOU!
July 12, 2016 39