le malattie cardiovascolari(cvd) · 1 le malattie cardiovascolari(cvd) • le malattie...
TRANSCRIPT

1
Le Malattie Cardiovascolari(CVD)
• Le malattie cardiovascolari sono la principale causa di mortalità e morbilità nei Paesi industrializzati. Più di tutte le forme di tumore. Acquistano sempre maggior peso anche nei Paesi emergenti. Possiamo distinguere:
• Cardiopatia ischemica(CHD):Infarto miocardico, Angina pectoris, morte cardiaca improvvisa.
• Ictus cerebrale, aneurismi aortici, malattia vascolare periferica.
www.cardiovascularprevention.com
2
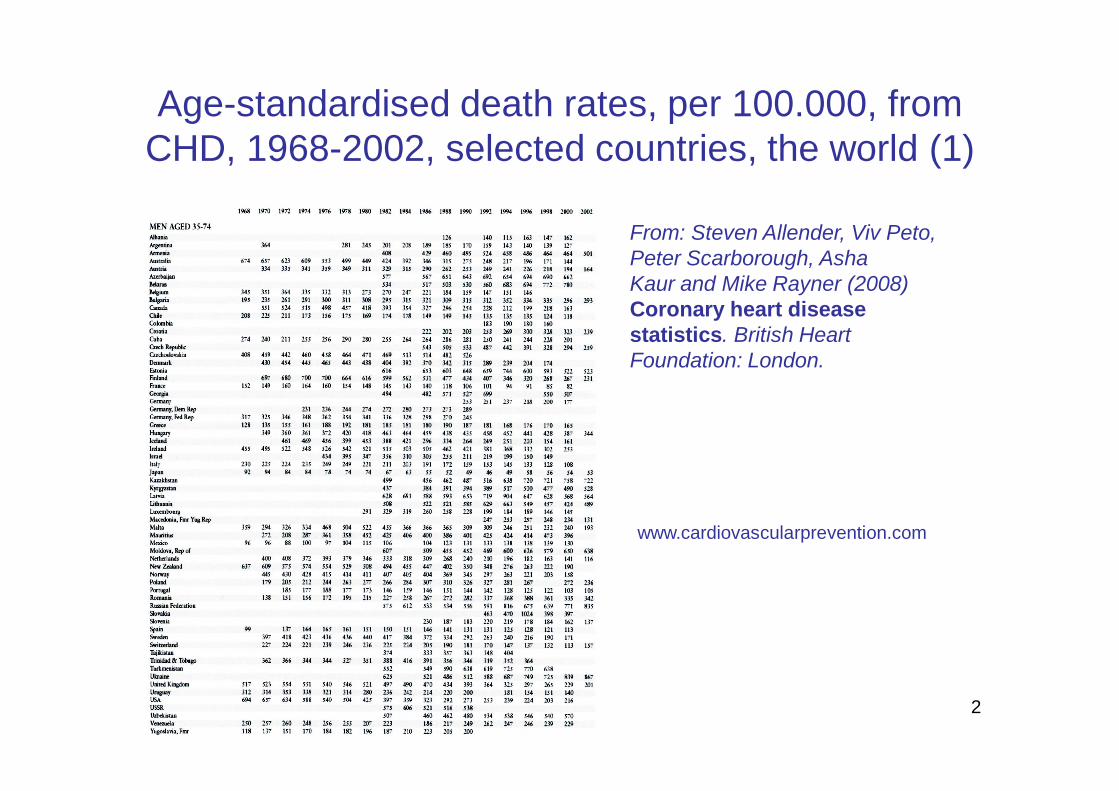
Age-standardised death rates, per 100.000, from CHD, 1968-2002, selected countries, the world (1)
www.cardiovascularprevention.com
From: Steven Allender, Viv Peto, Peter Scarborough, Asha Kaur and Mike Rayner (2008) Coronary heart disease statistics. British Heart Foundation: London.
3
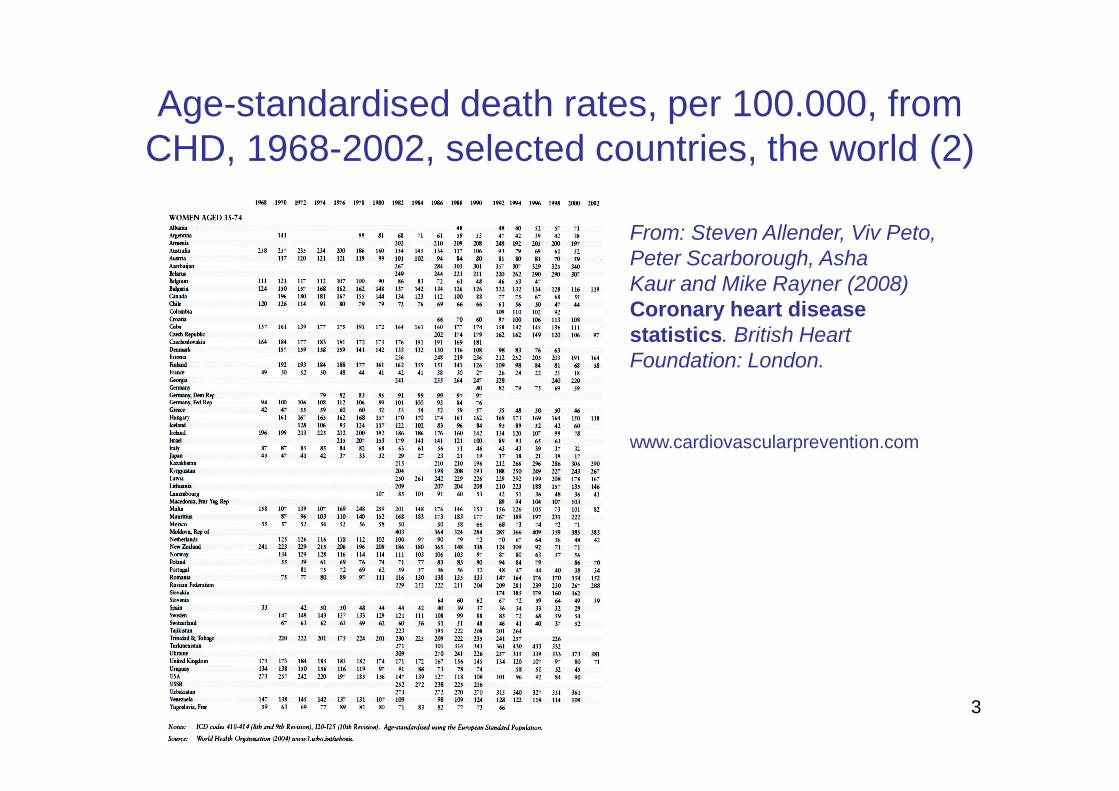
Age-standardised death rates, per 100.000, from CHD, 1968-2002, selected countries, the world (2)
www.cardiovascularprevention.com
From: Steven Allender, Viv Peto, Peter Scarborough, Asha Kaur and Mike Rayner (2008) Coronary heart disease statistics. British Heart Foundation: London.

4
La Malattia Cardiovascolare in Europa
• E’ la principale causa di morte contando per il 41% di tutti i decessi (Eurostat 2003)
• 1.2 milioni di decessi in Europa / anno
• 1/3 degli anni di vita perduti per morte precoce secondaria a CVD
www.cardiovascularprevention.com
5
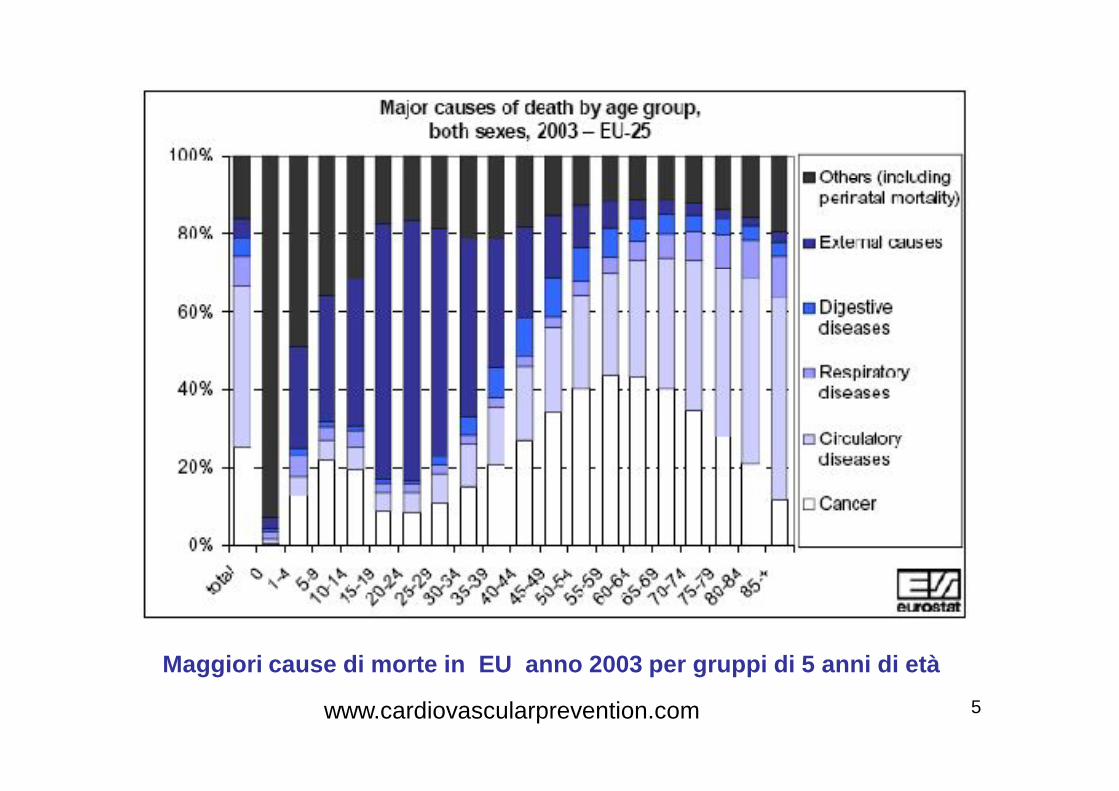
Maggiori cause di morte in EU anno 2003 per gruppi di 5 anni di età
www.cardiovascularprevention.com
6
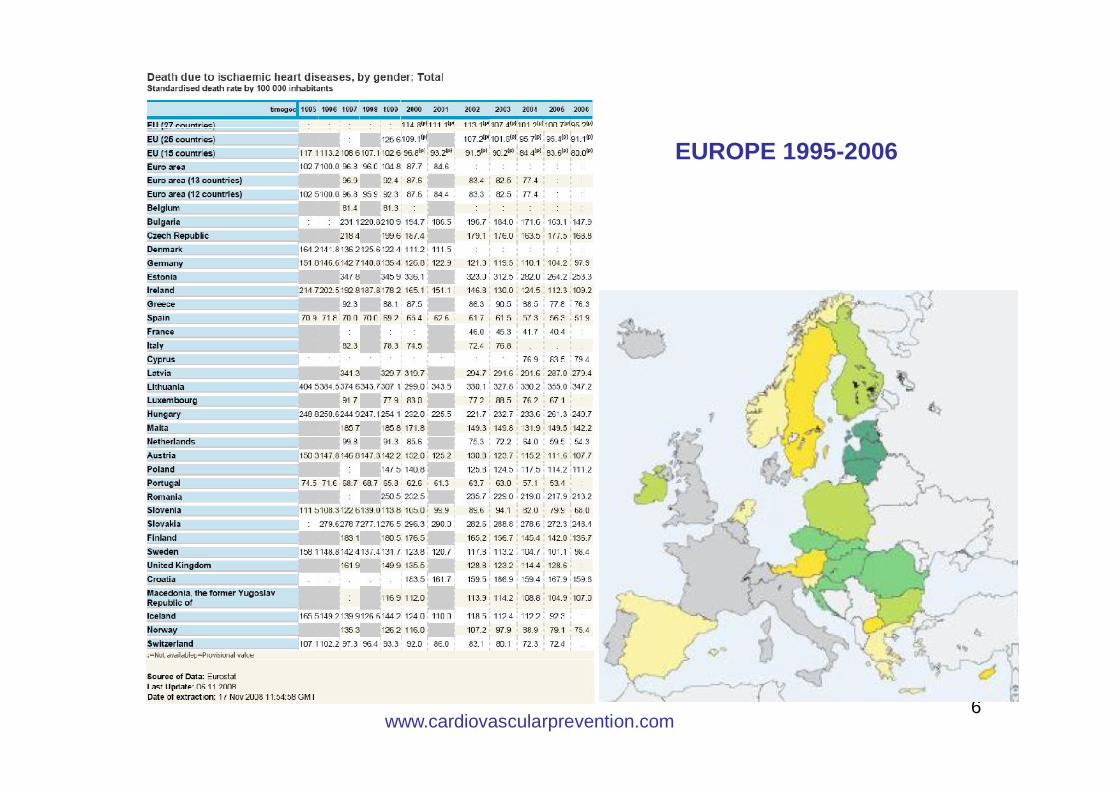
EUROPE 1995-2006
www.cardiovascularprevention.com
7
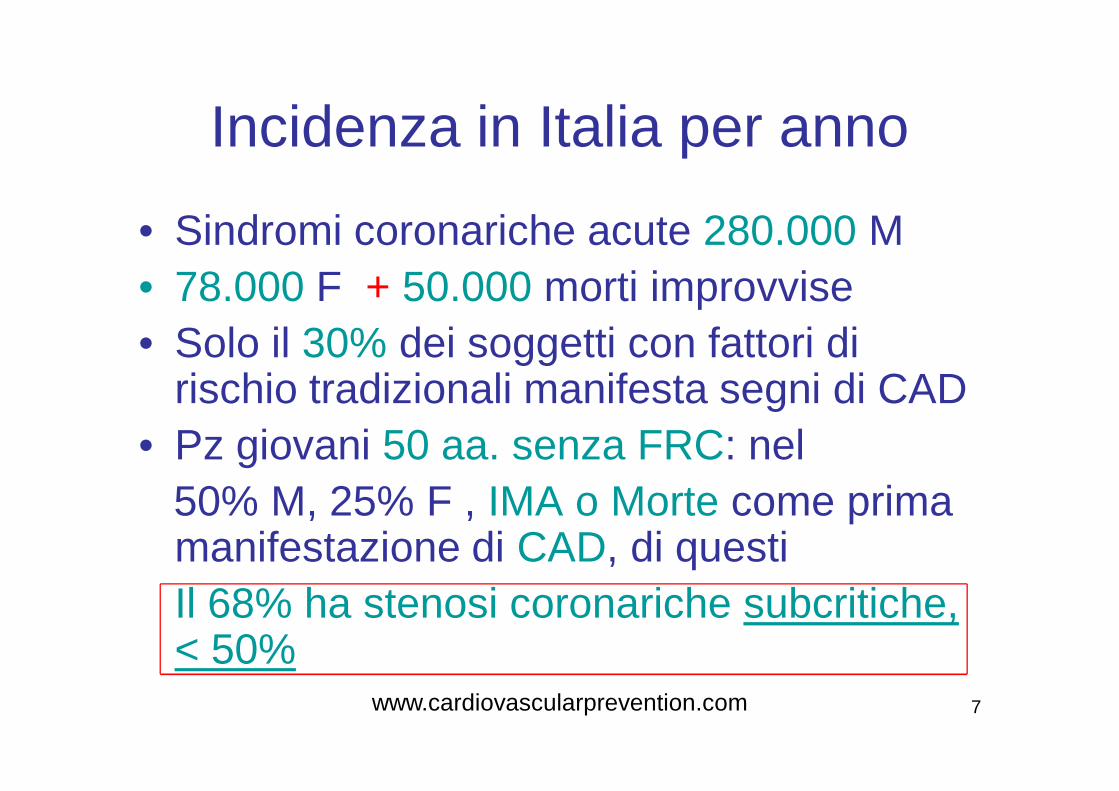
Incidenza in Italia per anno
• Sindromi coronariche acute 280.000 M• 78.000 F + 50.000 morti improvvise• Solo il 30% dei soggetti con fattori di
rischio tradizionali manifesta segni di CAD• Pz giovani 50 aa. senza FRC: nel
50% M, 25% F , IMA o Morte come prima manifestazione di CAD, di questiIl 68% ha stenosi coronariche subcritiche, < 50%
www.cardiovascularprevention.com

8
Mortalità Per Grandi Gruppianno 2002- ISTAT (Italy)
Malattie Cardiovascolari 237.198
Tumori 163.070
Morte improvvisa 54.000www.cardiovascularprevention.com

9
Numero dimessi 2004 - Ricoveri per acuti. ISTAT (Italy)
• Tumori 761.582
• Malattie cardiovascolari 1.413.082
www.cardiovascularprevention.com

10
Particolari condizioni patologiche associate ad elevata mortalità
cardiovascolare
• Diabete mellito• Scompenso cardiaco• Ictus ischemico/emorragico
www.cardiovascularprevention.com
11
Cardiovascular Disease in United Kingdom - 2006
• Diseases of the heart and circulatory system (cardiovascular disease or CVD) are the main cause of death in the UK and account for almost 198,000 deaths each year. More than one in three deaths (35%) are from CVD each year. The main forms of CVD are coronary heart disease (CHD: Acute myocardial infarction, Angina pectoris, sudden cardiac death) and stroke. About half (48%) of all deaths from CVD are from CHD and more than a quarter (28%) are from stroke.
• CHD by itself is the most common cause of death in the UK. Around one in five men and one in seven women die from the disease. CHD causes around 94,000 deaths in the UK each year.
• Other forms of heart disease cause over 31,000 deaths in the UK each year so in total there were just under 126,000 deaths from heart disease in the UK in 2006.
• Premature mortality(death before the age of 75).• CVD is one of the main causes of premature death in the UK 30% of premature deaths in men
and 22% of premature deaths in women were from CVD in 2006. CVD caused just over 53,000premature deaths in the UK in 2006.
• CHD, by itself, is the most common cause of premature death in the UK About one fifth (19%) of premature deaths in men and one in ten (10%) premature deaths in women were from CHD.
• CHD caused almost 31,000 premature deaths in the UK in 2006.• Other forms of heart disease cause more than 7,500 premature deaths in the UK each year. In
total there were over 38,000 premature deaths from heart disease in the UK in 2006 - around one fifth of all premature deaths.
From: Steven Allender, Viv Peto, Peter Scarborough, Asha Kaur and Mike Rayner (2008) Coronary heart disease statistics. British Heart Foundation: London.
www.cardiovascularprevention.com
12
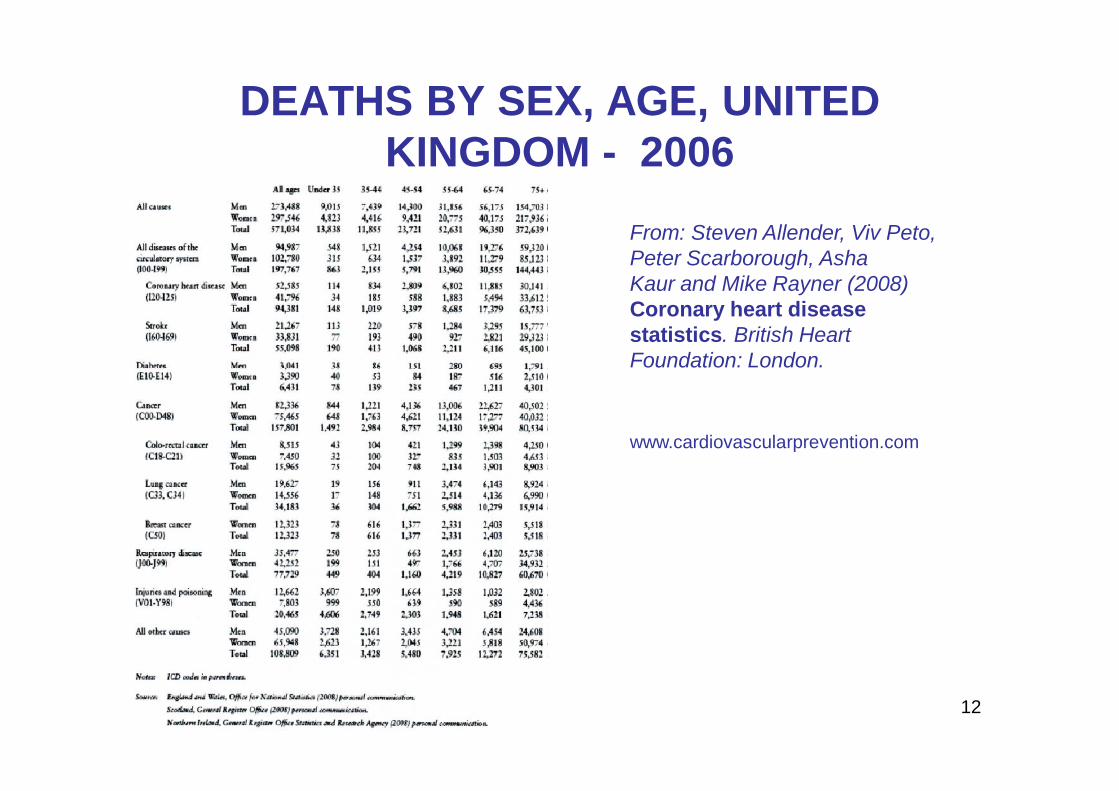
DEATHS BY SEX, AGE, UNITED KINGDOM - 2006
From: Steven Allender, Viv Peto, Peter Scarborough, Asha Kaur and Mike Rayner (2008) Coronary heart disease statistics. British Heart Foundation: London.
www.cardiovascularprevention.com
13
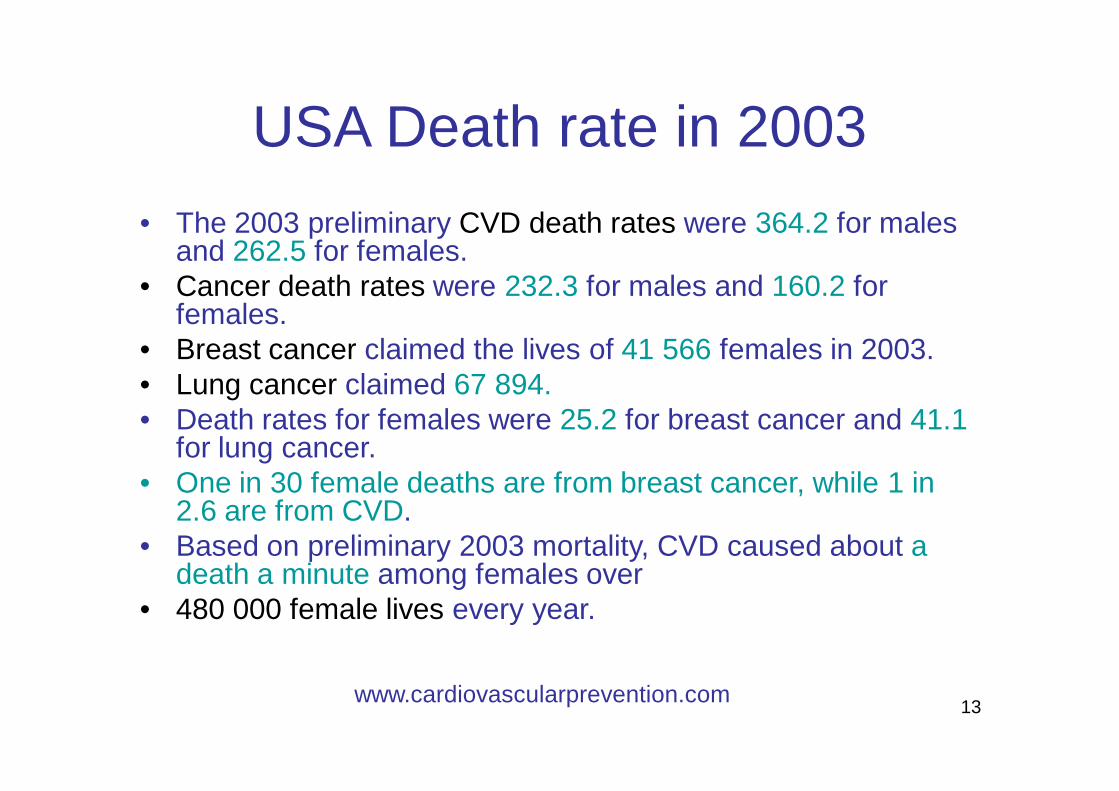
USA Death rate in 2003• The 2003 preliminary CVD death rates were 364.2 for males
and 262.5 for females. • Cancer death rates were 232.3 for males and 160.2 for
females.• Breast cancer claimed the lives of 41 566 females in 2003.• Lung cancer claimed 67 894.• Death rates for females were 25.2 for breast cancer and 41.1
for lung cancer. • One in 30 female deaths are from breast cancer, while 1 in
2.6 are from CVD. • Based on preliminary 2003 mortality, CVD caused about a
death a minute among females over • 480 000 female lives every year.
www.cardiovascularprevention.com
14
Other causes of death in 2003 in USA (preliminary data)
• Cancer 554 643• Accidents 105 695• Alzheimer’s disease 63 343 • HIV (AIDS) 13 544.
www.cardiovascularprevention.com
15
U.S.A. Data 1999-2002• Of the 71 300 000 American adults with 1 or more types
of cardiovascular disease (CVD), 27 400 000are estimated to be age 65 or older
• High blood pressure 65 000 000.• Coronary heart disease 13 200 000.
– Myocardial infarction (MI, or heart attack)7 200 000.
– Angina pectoris (AP, or chest pain) 6 500 000.• Heart failure 5 000 000.• Stroke 5 500 000.• Congenital cardiovascular defects 1 000 000.
www.cardiovascularprevention.com
16
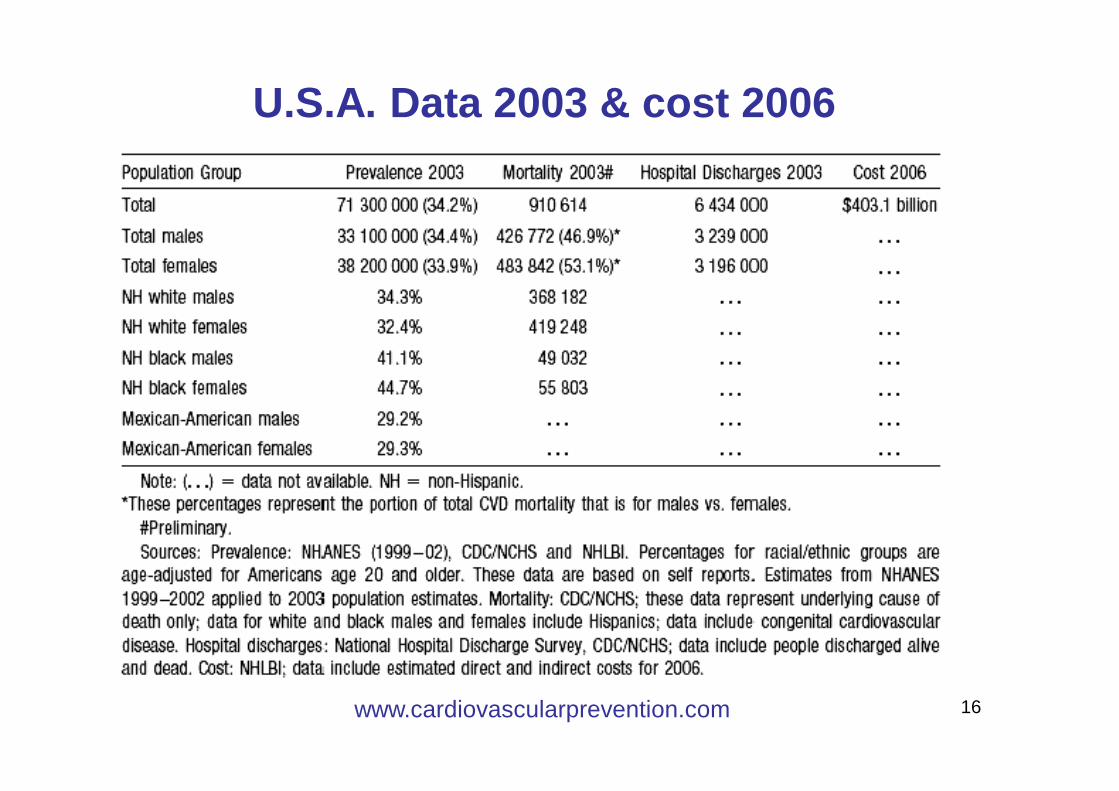
U.S.A. Data 2003 & cost 2006
www.cardiovascularprevention.com
17
CARDIOVASCULAR DISEASE IN CANADA (1)These statistics are based on 2004 data (from Statistics Canada)
Cardiovascular disease (heart disease, diseases of the blood vessels and stroke) accounts for the death of more Canadians than any other disease. Every 7 minutes in Canada, someone dies from heart disease or stroke.
Cardiovascular disease accounted for 72,338 deaths:32% of all deaths in Canada 31% of all male deaths 33% of all female deaths In 2004, of all cardiovascular deaths:54% were due to ischemic heart disease20% to stroke25% to heart attack
Cost of cardiovascular diseasesHeart disease and stroke costs the Canadian economy more than $18 billion every year in physician services, hospital costs, lost wages and
decreased productivity. www.cardiovascularprevention.com
18
CARDIOVASCULAR DISEASE IN CANADA (2)These statistics are based on 2004 data (from Statistics Canada)
Cardiac arrest
About 40,000 Canadians experience cardiac arrest every year.Less than 5% of those who have a cardiac arrest outside of a hospital
survive.
Congestive heart failure
It is estimated that there are 400,000 Canadians living with congestive heart failure (CHF).
Stroke
More than 50,000 strokes occur in Canada each year. That’s one stroke every 10 minutes.
Stroke is the third leading cause of death in Canada. Each year, more than 14,000 Canadians die from stroke.
Each year, more women than men die from stroke.
www.cardiovascularprevention.com
19
ACUTE CORONARY SINDROME IN INDIA• India has the largest percentage of heart disease in the world• Xavier et al's, examined the incidence of STEMI and non-STEMI among
almost 21 000 patients from 89 centers in 50 Indian cities. They found that more than 60% of these patients were diagnosed with STEMI, mean age was 57.5 years (although STEMI patients tended to be even younger), and the vast majority were from lower-middle-income or poor families.
• The Indians were, on average, 57,5 years of age compared with 70.7 yearsfor the European whites.
• Reinfarction, and stroke rates and 30-day death, were higher for STEMI patients than non-STEMI, and mortality, notably, was significantly higher in poor patients than in rich patients.
• They also had significantly increased prevalence of diabetes, hypertension, history of CAD compared with European whites.
• And triple-vessel disease was more common in the Indian Asians than in the whites.
• Almost all STEMI and non-STEMI patients were treated with antiplatelet drugs (primarily aspirin), but use of thrombolytics, ACE inhibitors or Angiotensin-Receptor Blockers, beta blockers, statins, omega 3 fatty-acids and PCI/CABG were all far lower than rates seen in the West.
www.cardiovascularprevention.com
20
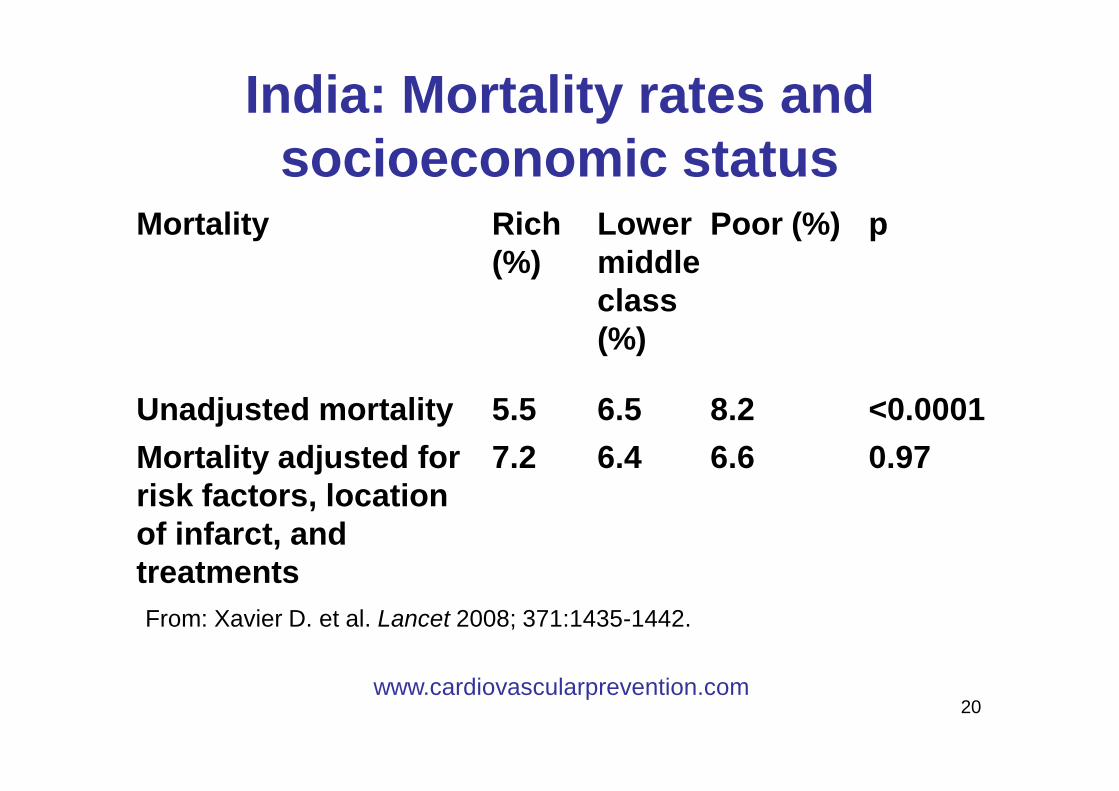
India: Mortality rates and socioeconomic status
Mortality Rich (%)
Lower middle class (%)
Poor (%) p
Unadjusted mortality 5.5 6.5 8.2 <0.0001Mortality adjusted for risk factors, location of infarct, and treatments
7.2 6.4 6.6 0.97
From: Xavier D. et al. Lancet 2008; 371:1435-1442.
www.cardiovascularprevention.com
21
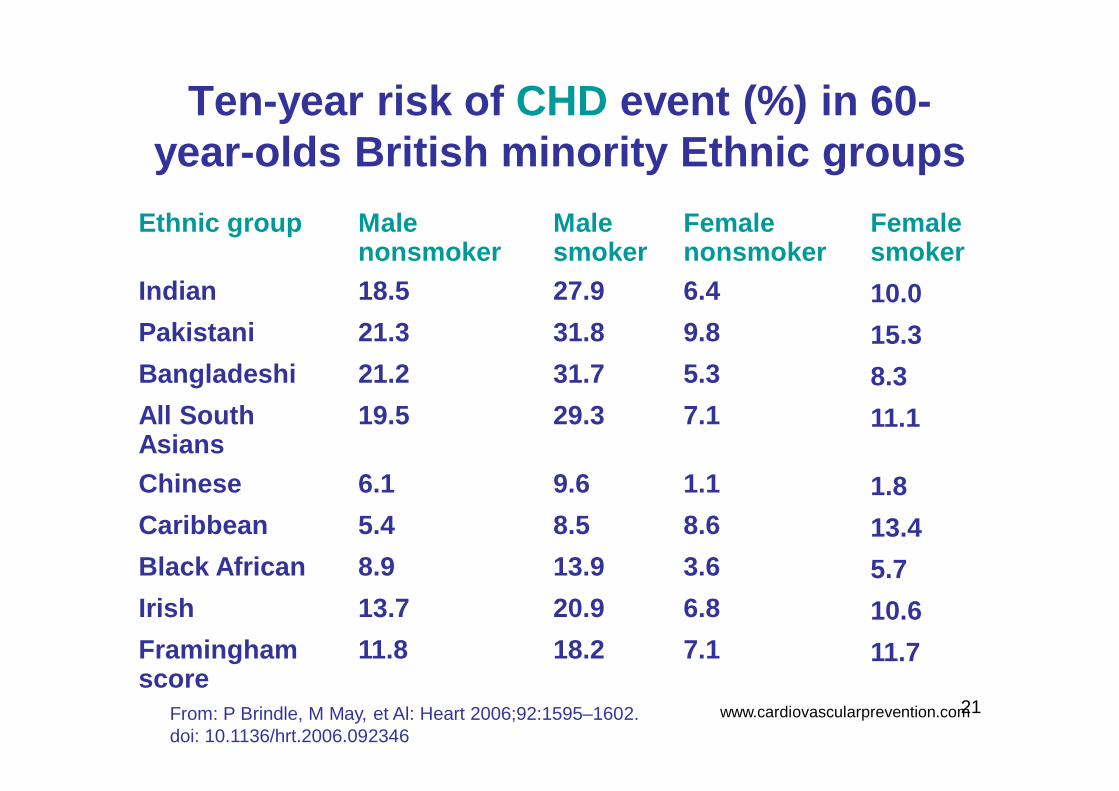
Ten-year risk of CHD event (%) in 60-year-olds British minority Ethnic groups
From: P Brindle, M May, et Al: Heart 2006;92:1595–1602. doi: 10.1136/hrt.2006.092346
Ethnic group Male nonsmoker
Male smoker
Female nonsmoker
Female smoker
Indian 18.5 27.9 6.4 10.0Pakistani 21.3 31.8 9.8 15.3Bangladeshi 21.2 31.7 5.3 8.3All South Asians
19.5 29.3 7.1 11.1
Chinese 6.1 9.6 1.1 1.8Caribbean 5.4 8.5 8.6 13.4Black African 8.9 13.9 3.6 5.7Irish 13.7 20.9 6.8 10.6Framingham score
11.8 18.2 7.1 11.7
www.cardiovascularprevention.com
22
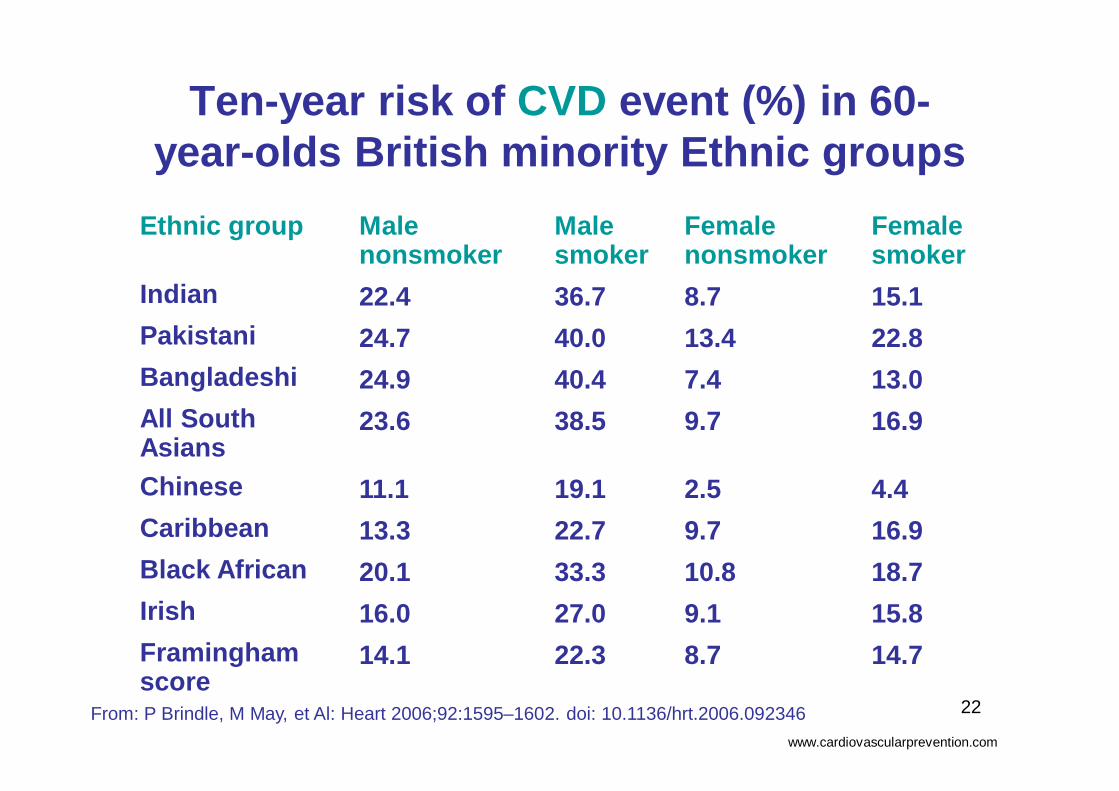
Ten-year risk of CVD event (%) in 60-year-olds British minority Ethnic groups
Ethnic group Male nonsmoker
Male smoker
Female nonsmoker
Female smoker
Indian 22.4 36.7 8.7 15.1Pakistani 24.7 40.0 13.4 22.8Bangladeshi 24.9 40.4 7.4 13.0All South Asians
23.6 38.5 9.7 16.9
Chinese 11.1 19.1 2.5 4.4Caribbean 13.3 22.7 9.7 16.9Black African 20.1 33.3 10.8 18.7Irish 16.0 27.0 9.1 15.8Framingham score
14.1 22.3 8.7 14.7
From: P Brindle, M May, et Al: Heart 2006;92:1595–1602. doi: 10.1136/hrt.2006.092346www.cardiovascularprevention.com

23
CVD: Costi in alcuni Paesianno 2006
• Costi Italiani• Euro 16,900 Miliardi
• 10% spesa sanitaria tot.
= Euro 235 pro capite
•Costi in USA•$393,500 Miliardi $•15.82% della spesa sanitaria totale
•$5621.42 pro capite
● Costi in U.K.Miliardi £ 14,4 miliardi Costo pro capite £ 250.
Costi Sociali Conseguenti
£ 8.2 milardi
www.cardiovascularprevention.com
● Costi EuropeiCosto pro capite € 250
10% Spesa sanitaria Totale
24
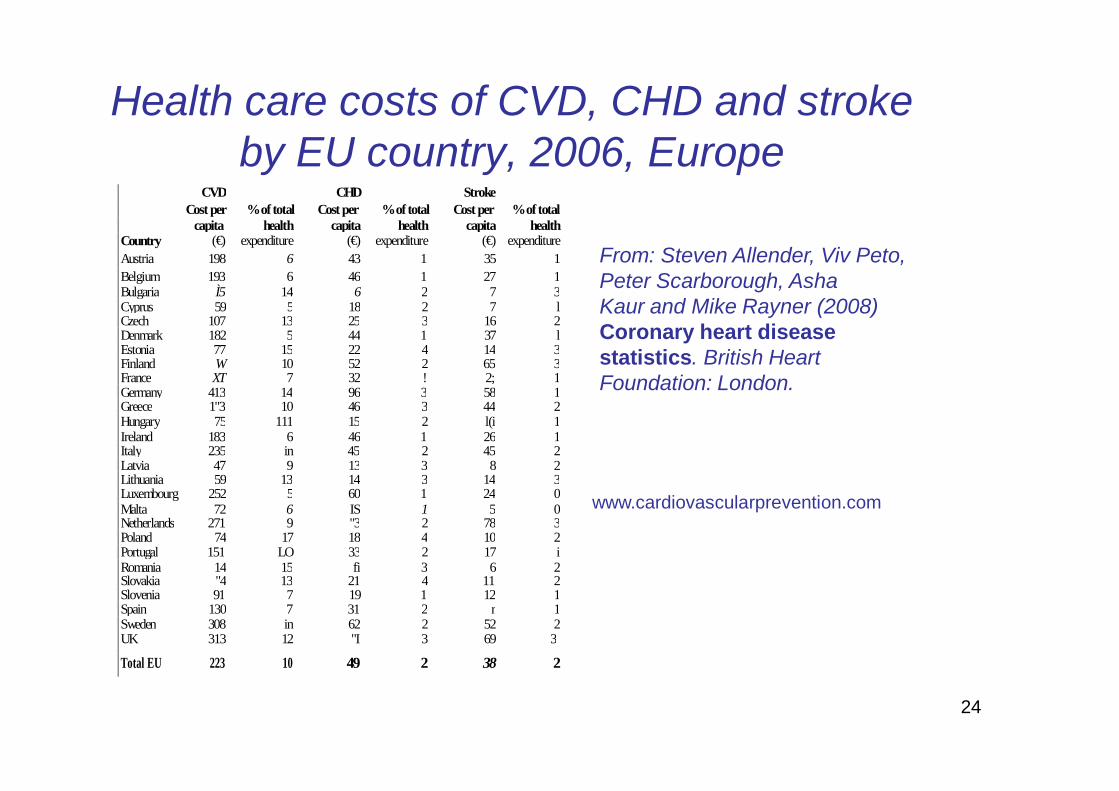
Health care costs of CVD, CHD and stroke by EU country, 2006, Europe
CVD CHD Stroke Cost per % of total Cost per % of total Cost per % of total capita health capita health capita health Country (€) expenditure (€) expenditure (€) expenditure Austria 198 6 43 1 35 1 Belgium 193 6 46 1 27 1 Bulgaria Ì5 14 6 2 7 3 Cyprus 59 5 18 2 7 l Czech 107 13 25 3 16 2 Denmark 182 5 44 1 37 l Estonia 77 15 22 4 14 3 Finland W 10 52 2 65 3 France XT 7 32 ! 2; 1 Germany 413 14 96 3 58 1 Greece 1"3 10 46 3 44 2 Hungary 75 111 15 2 l(i 1 Ireland 183 6 46 1 26 1 Italy 235 in 45 2 45 2 Latvia 47 9 13 3 8 2 Lithuania 59 13 14 3 14 3 Luxembourg 252 5 60 1 24 0 Malta 72 6 IS 1 5 0 Netherlands 271 9 "3 2 78 3 Poland 74 17 18 4 10 2 Portugal 151 LO 33 2 17 i Romania 14 15 fi 3 6 2 Slovakia "4 13 21 4 11 2 Slovenia 91 7 19 1 12 1 Spain 130 7 31 2 r 1 Sweden 308 in 62 2 52 2 UK 313 12 "I 3 69 3
Total EU 223 10 49 2 38 2
From: Steven Allender, Viv Peto, Peter Scarborough, Asha Kaur and Mike Rayner (2008) Coronary heart disease statistics. British Heart Foundation: London.
www.cardiovascularprevention.com

25
Consumo nazionale di farmaci a carico del Servizio Sanitario Nazionale per categorie terapeutiche (ATC al I° livello) - Anno 2005
CATEGORIA TERAPEUTICA DDD ogni 1.000 abitanti al giorno %Variazione
percentuale rispetto al 2004
CARDIOVASCOLARE 392,2 48,6 4,7GASTROINTESTINALE E METABOLISMO 92,9 11,5 5,3ANTIMICROBICI 24,2 3,0 4,8SISTEMA NERVOSO CENTRALE 46,3 5,7 7,1RESPIRATORIO 48,0 5,9 5,4ANTINEOPLASTICI 5,7 0,7 -3,0EMATOLOGICI 72,3 9,0 6,6GENITO-URINARI E ORMONI SESSUALI 40,2 5,0 -1,8MUSCOLO-SCHELETRICO 37,9 4,7 -7,9ORMONI SISTEMICI 27,7 3,4 7,9ORGANI DI SENSO 15,7 1,9 0,8DERMATOLOGICI 3,0 0,4 -1,5VARI 0,2 0,0 -2,0ANTIPARASSITARI 0,6 0,1 3,5
806,9 100,0 4,0
Fonte: AIFA - Rapporto nazionale OSMED sul consumo di farmaci 2005DDD - Daily Defined Dose (dose giornaliera di mantenimento in un adulto)
www.cardiovascularprevention.com
ITALY
CONSUMO DI FARMACI in Italia

26
• Sproporzione tra la domanda crescente di prestazioni e le risorse economiche scarse
• Ciò richiede fondamentali modifiche nella strategia diagnostica e terapeutica
Problemi cardiologici attuali e futuri
www.cardiovascularprevention.com
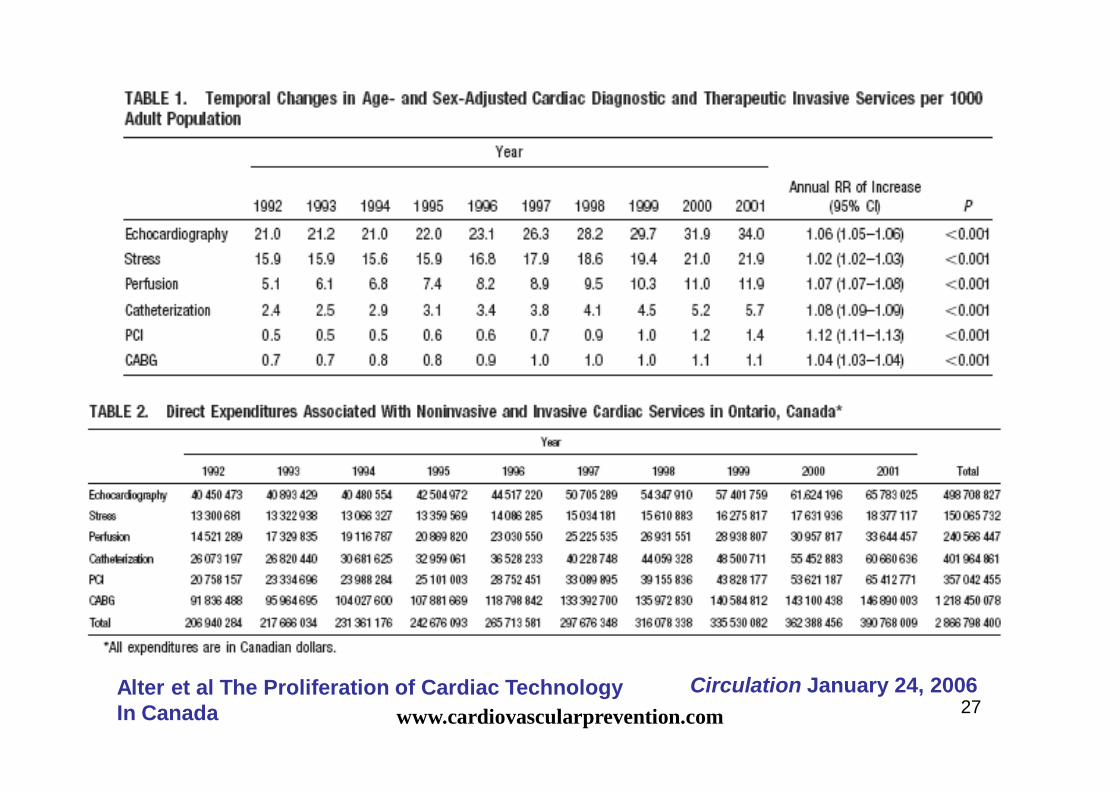
27Circulation January 24, 2006Alter et al The Proliferation of Cardiac Technology
In Canada www.cardiovascularprevention.com
28
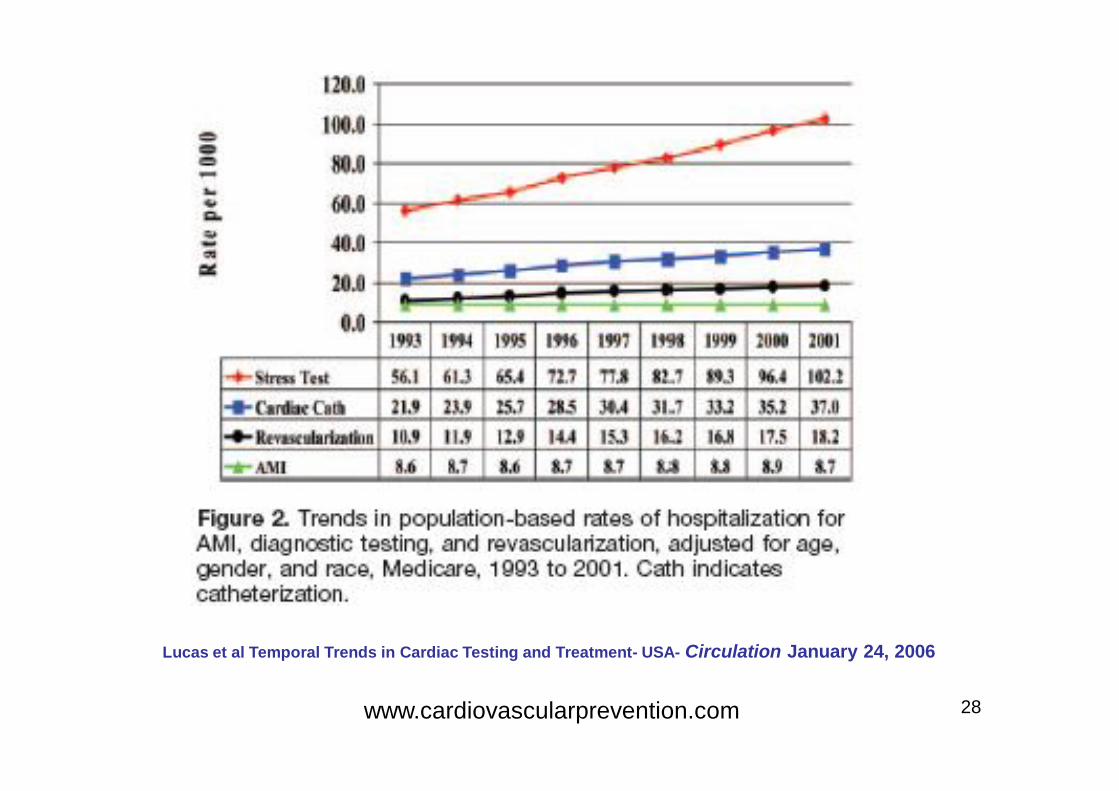
Lucas et al Temporal Trends in Cardiac Testing and Treatment- USA- Circulation January 24, 2006
www.cardiovascularprevention.com
29
• Numerosi trattamenti possono ridurre il rischio deimaggiori eventi cardiovascolari in grandi gruppi dipazienti
Prescrizione di tutti i farmaci benefici a tutti i pazienti
Medicina basata sull’Evidenza
Mentre il Beneficio è solo per una frazione dei pazienti trattati con elevati costi sociali
“ E’ come indossare LA STESSA TAGLIA PER TUTTI ”
www.cardiovascularprevention.com
30
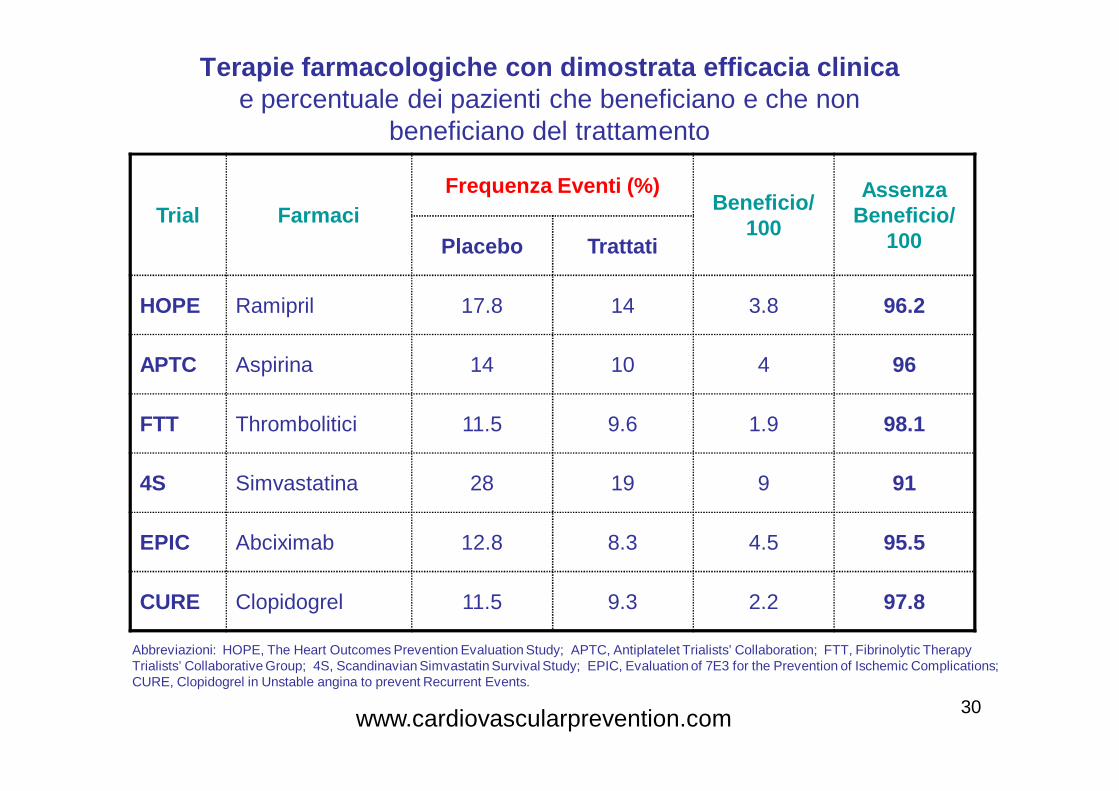
Terapie farmacologiche con dimostrata efficacia clinicae percentuale dei pazienti che beneficiano e che non
beneficiano del trattamento
Trial FarmaciFrequenza Eventi (%)
Beneficio/ 100
Assenza Beneficio/
100Placebo Trattati
HOPE Ramipril 17.8 14 3.8 96.2
APTC Aspirina 14 10 4 96
FTT Thrombolitici 11.5 9.6 1.9 98.1
4S Simvastatina 28 19 9 91
EPIC Abciximab 12.8 8.3 4.5 95.5
CURE Clopidogrel 11.5 9.3 2.2 97.8
Abbreviazioni: HOPE, The Heart Outcomes Prevention Evaluation Study; APTC, Antiplatelet Trialists’ Collaboration; FTT, Fibrinolytic TherapyTrialists’ Collaborative Group; 4S, Scandinavian Simvastatin Survival Study; EPIC, Evaluation of 7E3 for the Prevention of Ischemic Complications;CURE, Clopidogrel in Unstable angina to prevent Recurrent Events.
www.cardiovascularprevention.com
31
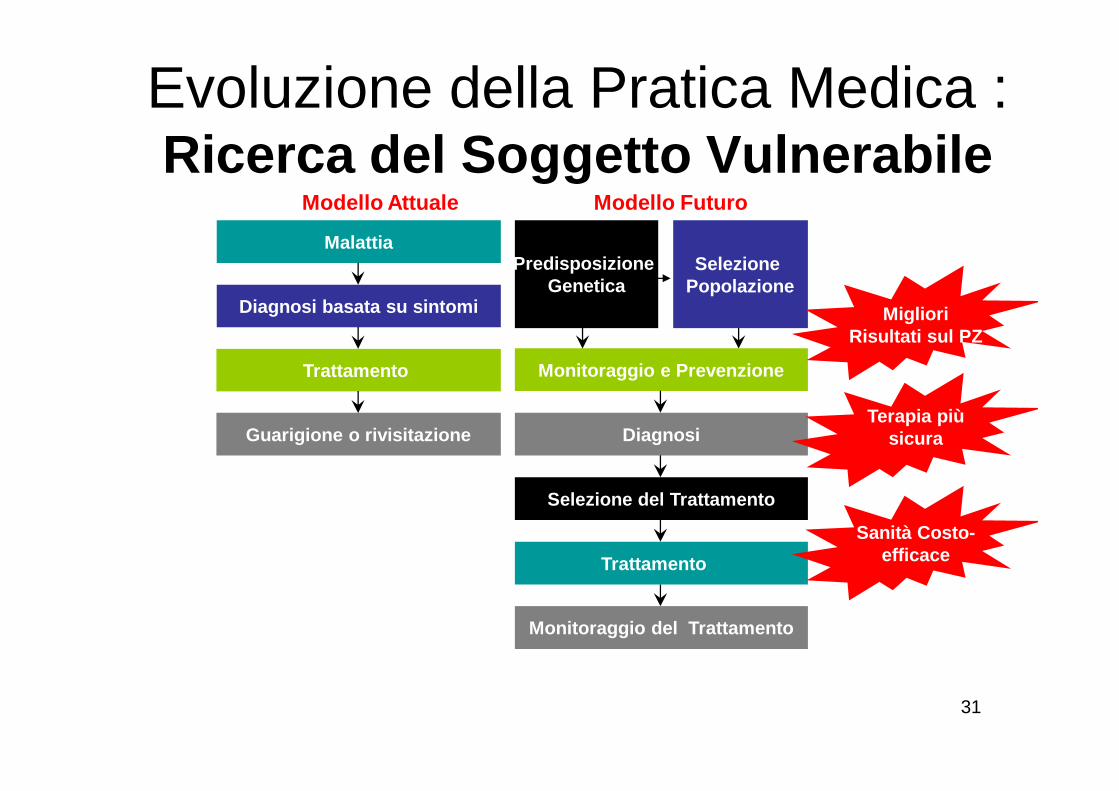
Evoluzione della Pratica Medica : Ricerca del Soggetto Vulnerabile
Modello Futuro
Malattia
Diagnosi basata su sintomi
Trattamento
Guarigione o rivisitazione
Modello Attuale
Selezione del Trattamento
Trattamento
Monitoraggio e Prevenzione
Diagnosi
Predisposizione Genetica
Selezione Popolazione
Monitoraggio del Trattamento
Migliori Risultati sul PZ
Sanità Costo-efficace
Terapia più sicura
32
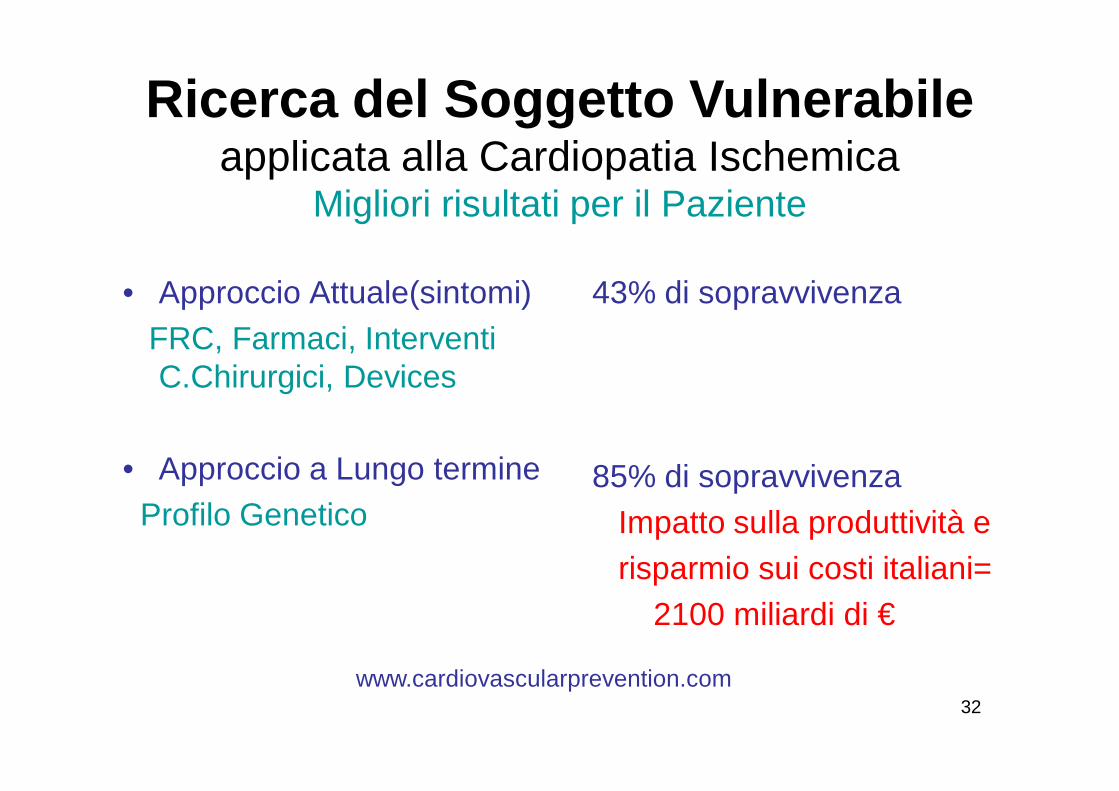
Ricerca del Soggetto Vulnerabileapplicata alla Cardiopatia Ischemica
Migliori risultati per il Paziente
• Approccio Attuale(sintomi)FRC, Farmaci, Interventi C.Chirurgici, Devices
• Approccio a Lungo termineProfilo Genetico
43% di sopravvivenza
85% di sopravvivenzaImpatto sulla produttività erisparmio sui costi italiani=
2100 miliardi di €
www.cardiovascularprevention.com

33
Cardiopatia Ischemica(CAD):Ricerca del Soggetto Vulnerabile
• Più di 1 miliardo di persone morirà di CAD nella prima metà del 21 secolo. Molte in età media.• Uccide più la CAD che tutte le forme di tumore• Le malattie cardiovascolari(CVD) oggi sono prevedibili• La diagnosi precoce migliora la sopravvivenza, la produttività e potenzialmente riduce i costi per la prevenzione secondaria
www.cardiovascularprevention.com
34
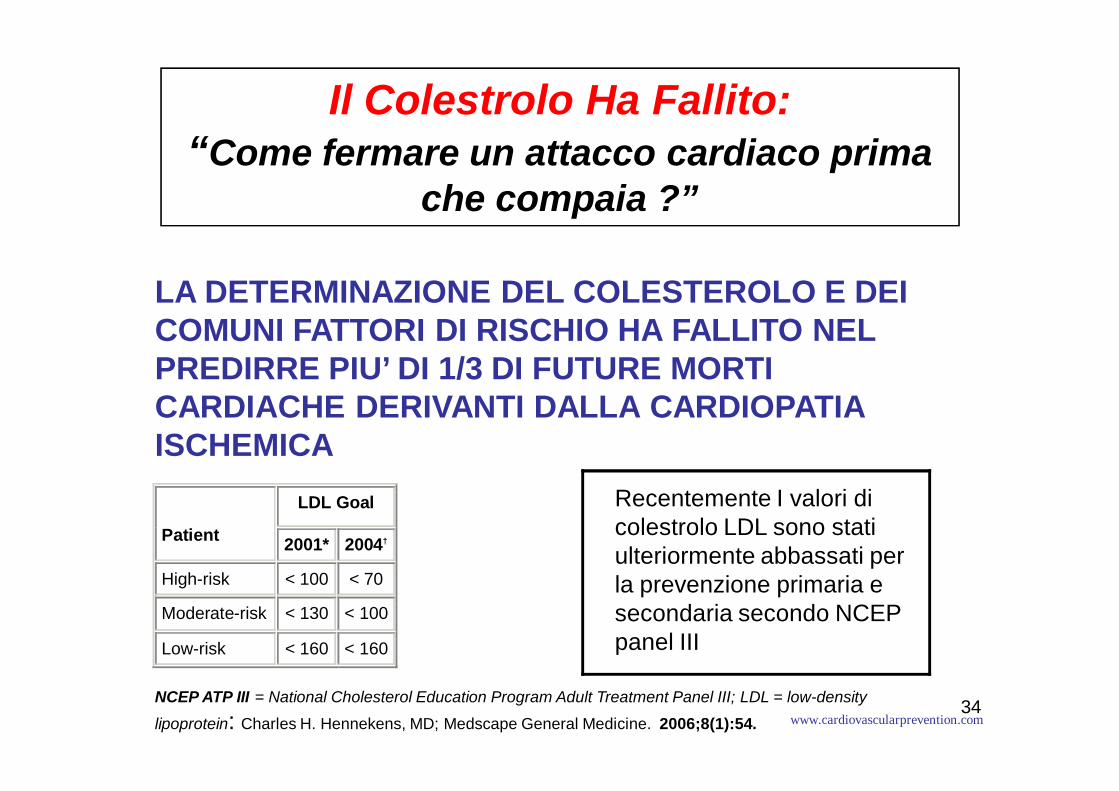
Il Colestrolo Ha Fallito:“Come fermare un attacco cardiaco prima
che compaia ?”
LA DETERMINAZIONE DEL COLESTEROLO E DEI COMUNI FATTORI DI RISCHIO HA FALLITO NEL PREDIRRE PIU’ DI 1/3 DI FUTURE MORTI CARDIACHE DERIVANTI DALLA CARDIOPATIA ISCHEMICA
LDL Goal
Patient 2001* 2004†
High-risk < 100 < 70
Moderate-risk < 130 < 100
Low-risk < 160 < 160
Recentemente I valori di colestrolo LDL sono stati ulteriormente abbassati per la prevenzione primaria e secondaria secondo NCEP panel III
NCEP ATP III = National Cholesterol Education Program Adult Treatment Panel III; LDL = low-density
lipoprotein: Charles H. Hennekens, MD; Medscape General Medicine. 2006;8(1):54. www.cardiovascularprevention.com

35
36
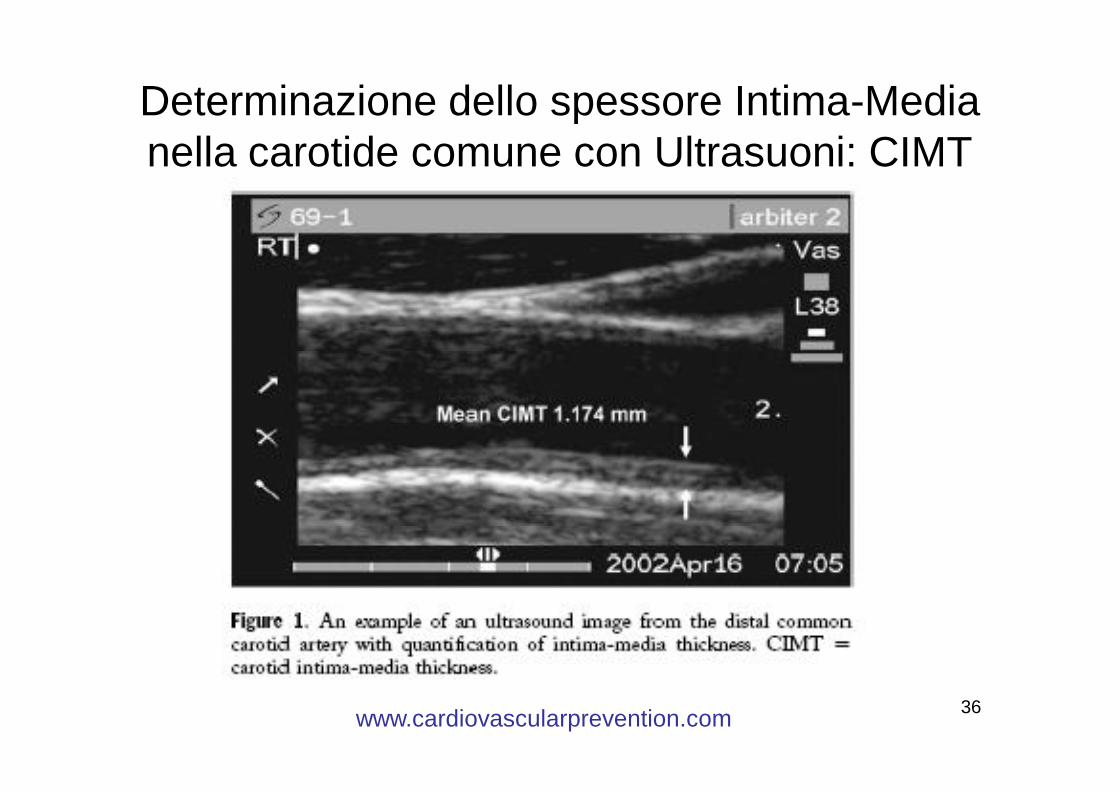
Determinazione dello spessore Intima-Media nella carotide comune con Ultrasuoni: CIMT
www.cardiovascularprevention.com
37
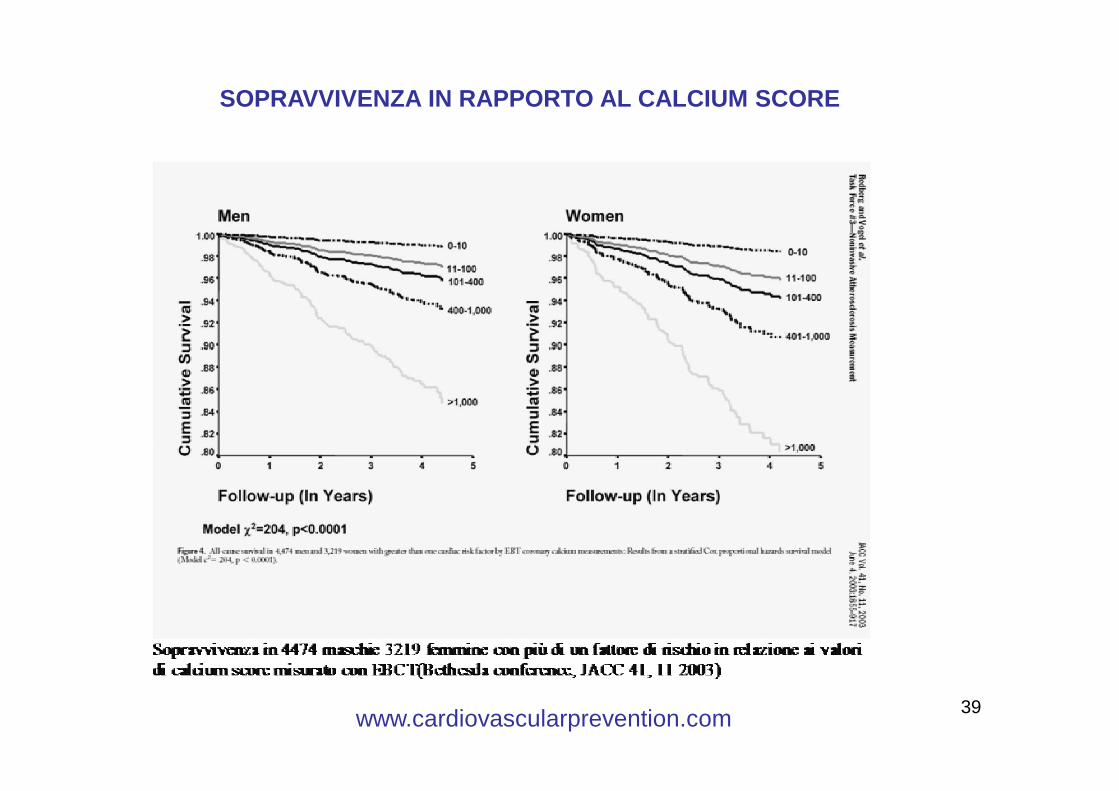
CALCIUM SCORE• Nelle arterie normali non sono presenti
calcificazioni. • La presenza di calcificazioni coronariche indica
la sussistenza di malattia coronarica.• L'entità delle calcificazioni si correla con l'entità
della placca e con il numero di stenosi coronariche.
• La ricerca del calcio coronarico è un metodo eccellente di screening dei pazienti asintomatici
• Il potere predittivo positivo varia dal 20 al 35% ed il potere predittivo negativo è vicino al 100%.
www.cardiovascularprevention.com
38
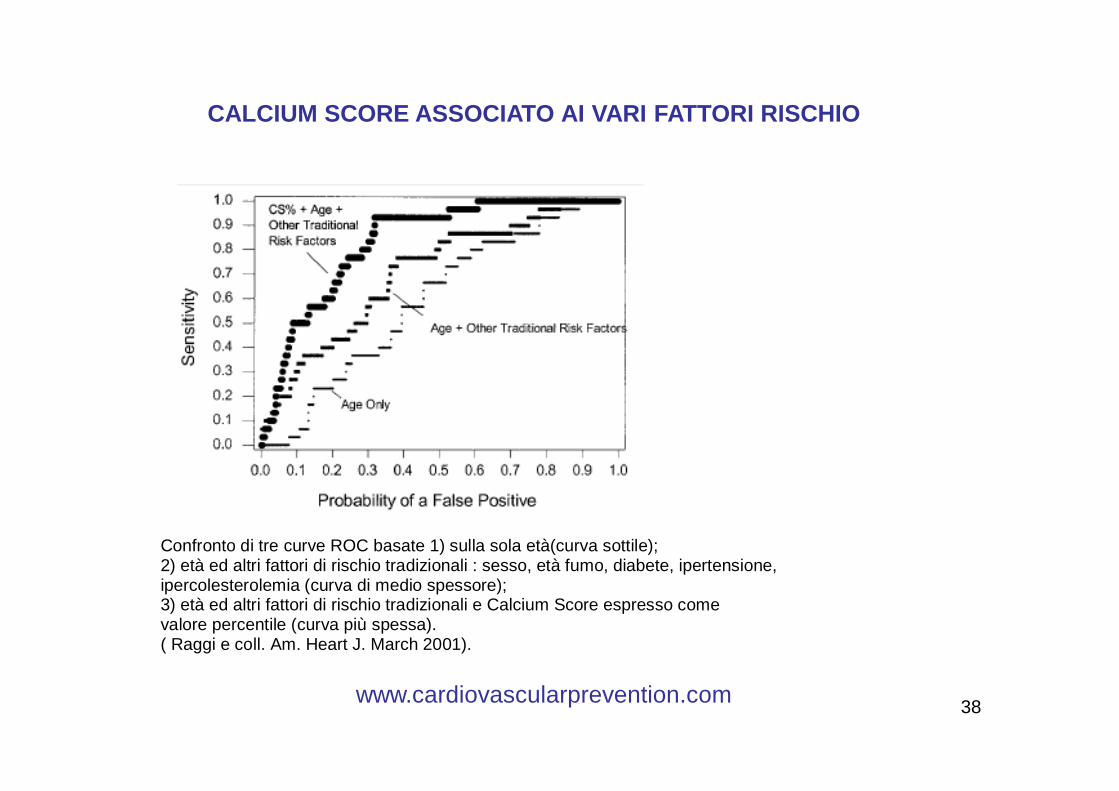
Confronto di tre curve ROC basate 1) sulla sola età(curva sottile); 2) età ed altri fattori di rischio tradizionali : sesso, età fumo, diabete, ipertensione, ipercolesterolemia (curva di medio spessore); 3) età ed altri fattori di rischio tradizionali e Calcium Score espresso come valore percentile (curva più spessa). ( Raggi e coll. Am. Heart J. March 2001).
CALCIUM SCORE ASSOCIATO AI VARI FATTORI RISCHIO
www.cardiovascularprevention.com
39
SOPRAVVIVENZA IN RAPPORTO AL CALCIUM SCORE
www.cardiovascularprevention.com
40
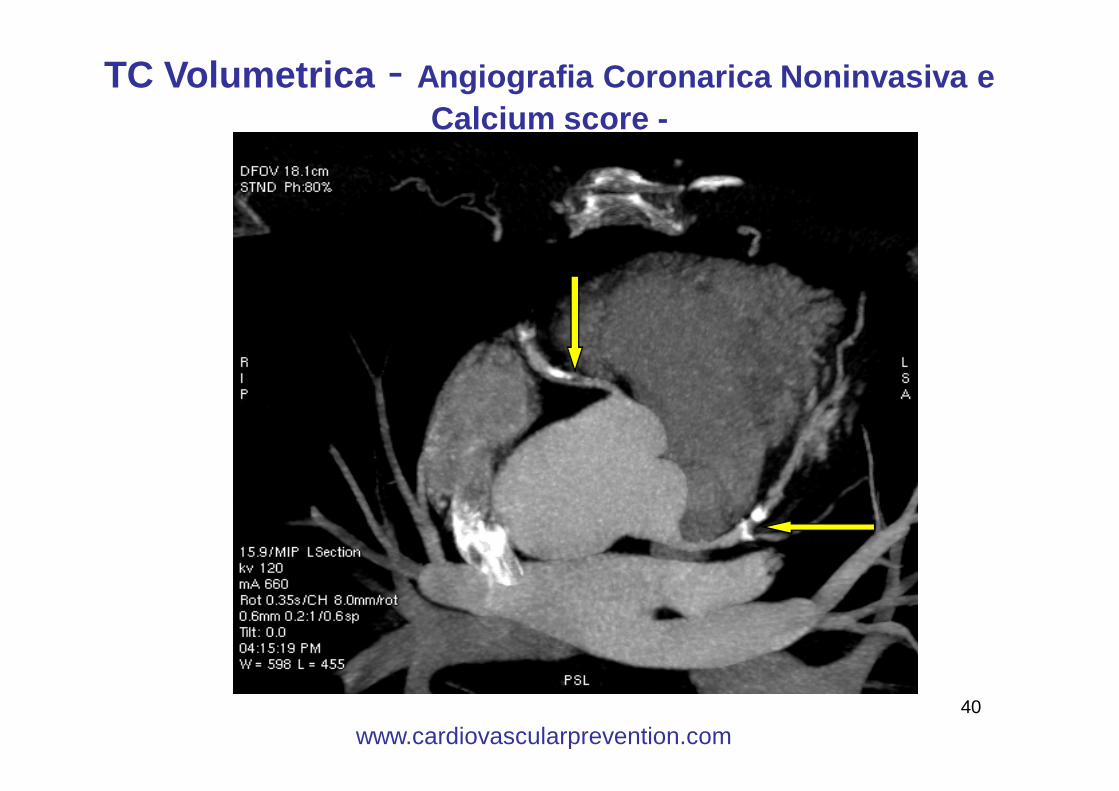
TC Volumetrica - Angiografia Coronarica Noninvasiva e Calcium score -
www.cardiovascularprevention.com
41
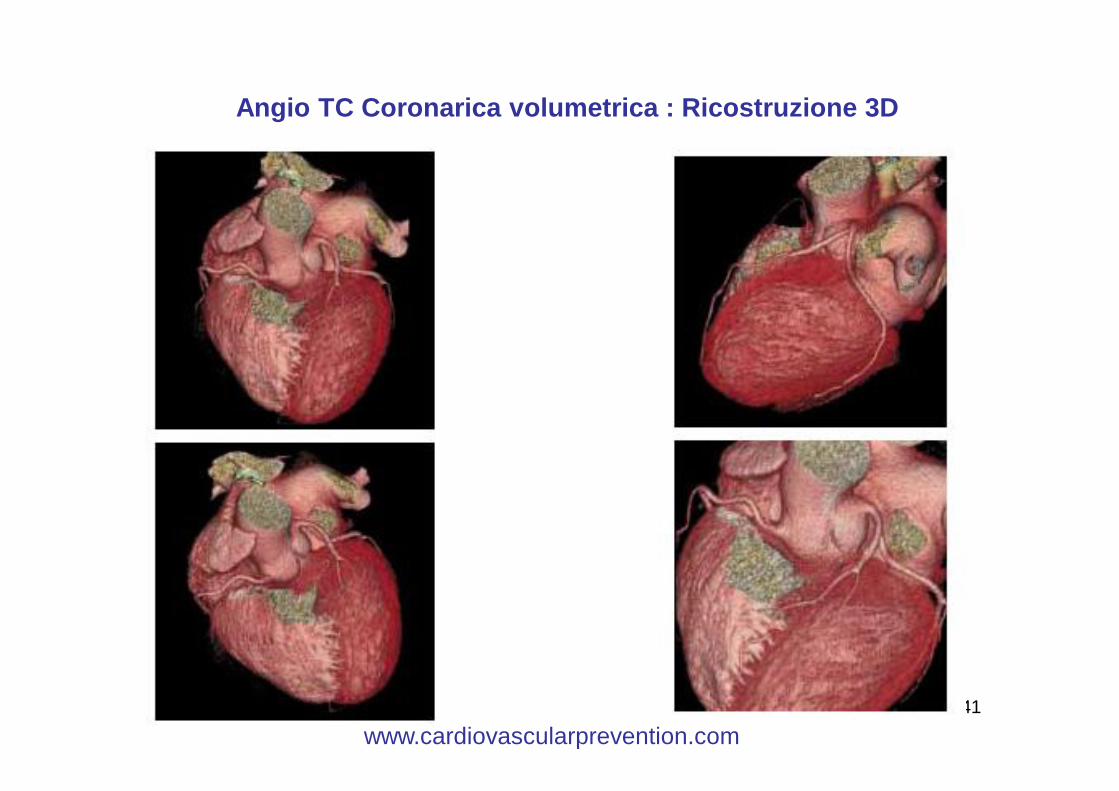
Angio TC Coronarica volumetrica : Ricostruzione 3D
www.cardiovascularprevention.com
42
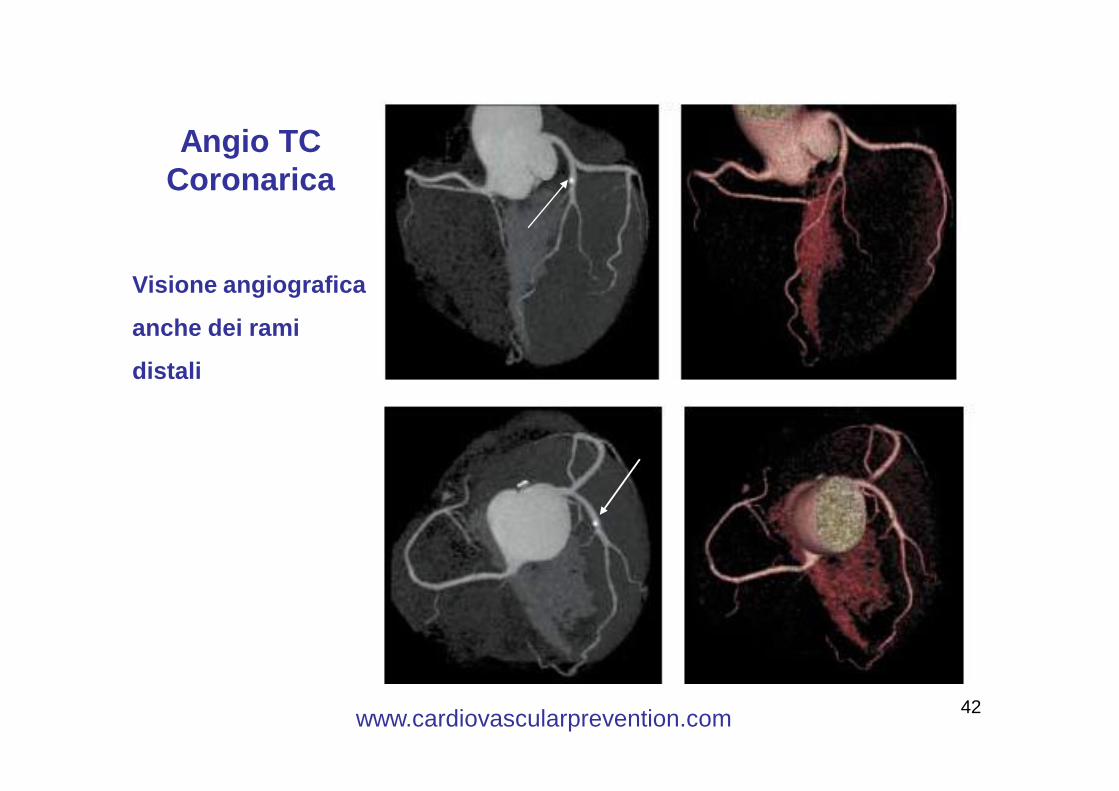
Angio TC Coronarica
Visione angiografica
anche dei rami
distali
www.cardiovascularprevention.com
43
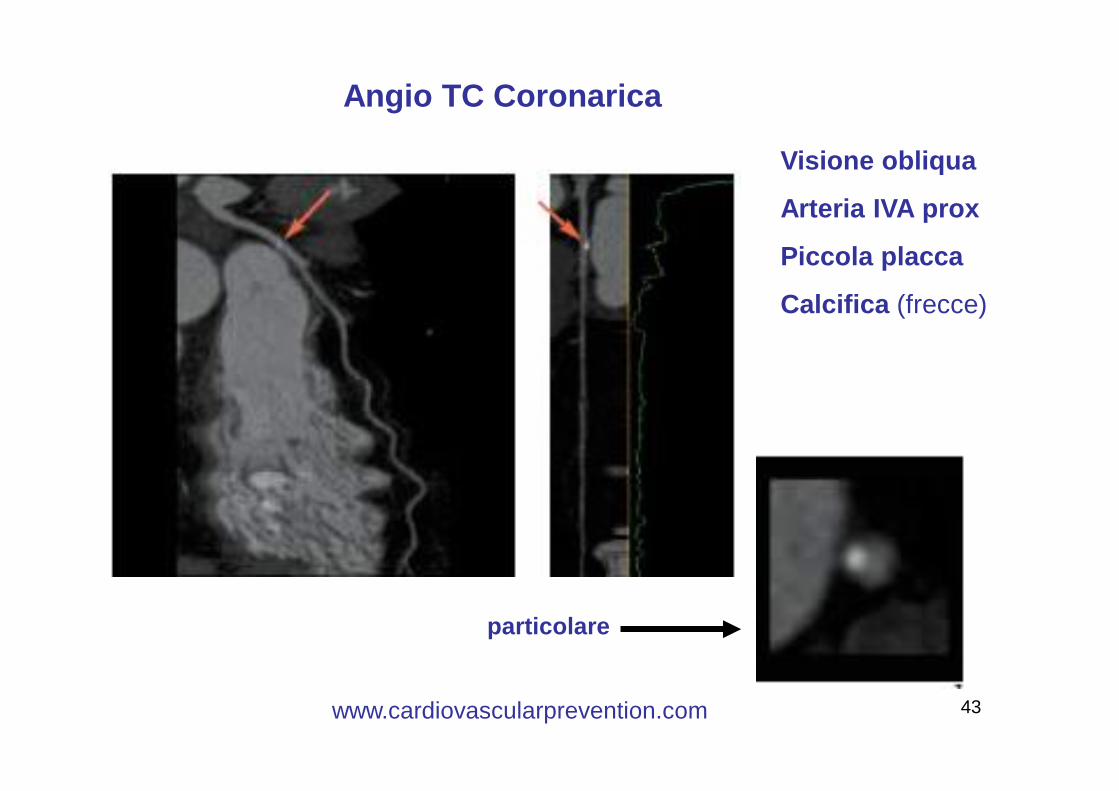
Angio TC Coronarica
Visione obliqua
Arteria IVA prox
Piccola placca
Calcifica (frecce)
particolare
www.cardiovascularprevention.com
44
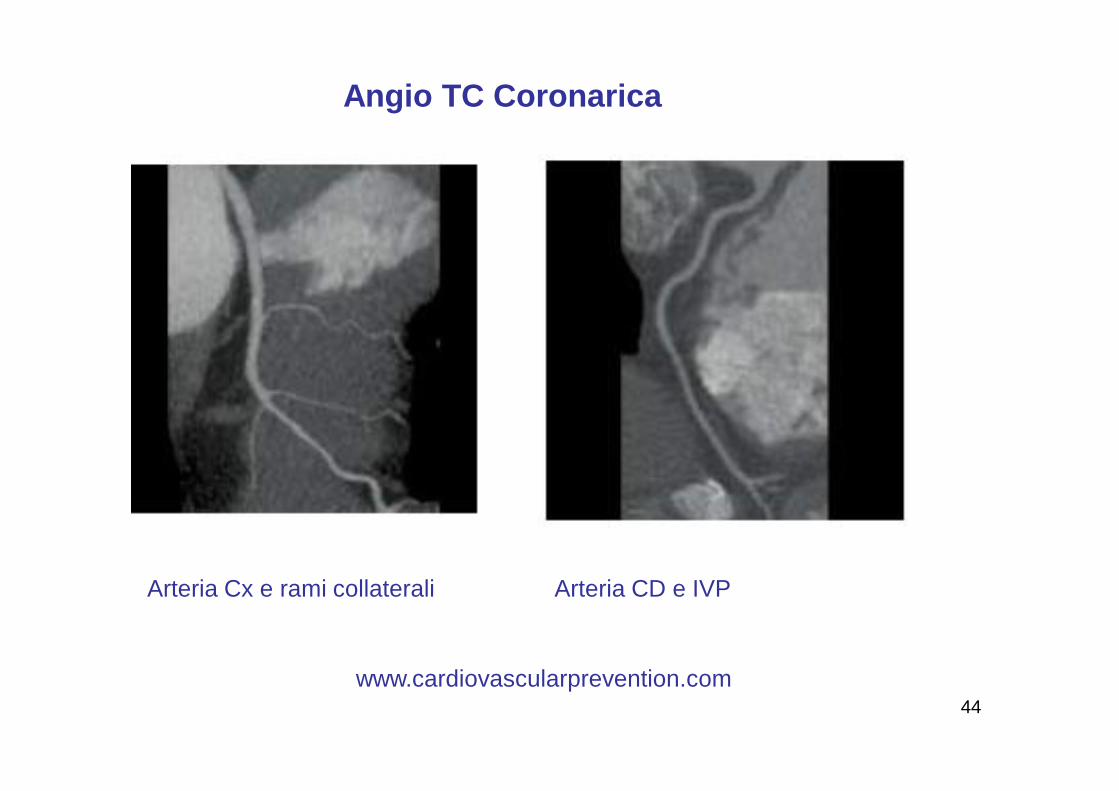
Arteria Cx e rami collaterali Arteria CD e IVP
Angio TC Coronarica
www.cardiovascularprevention.com
45
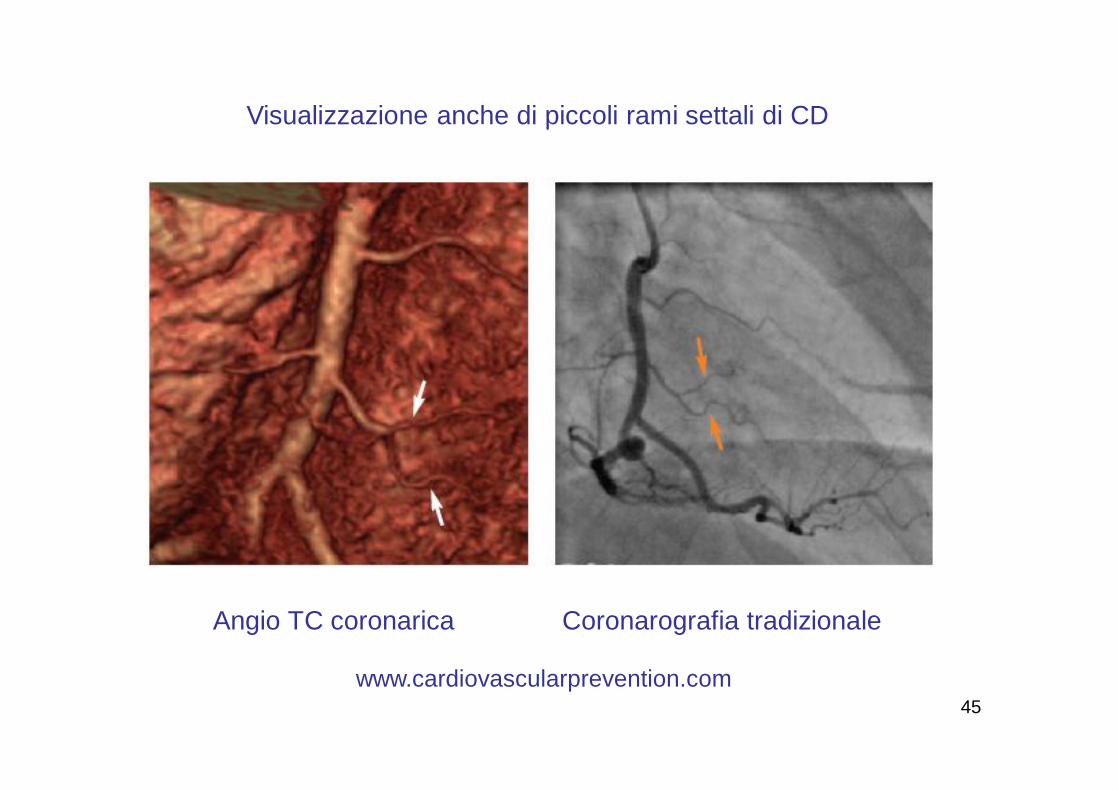
Visualizzazione anche di piccoli rami settali di CD
Angio TC coronarica Coronarografia tradizionale
www.cardiovascularprevention.com
46
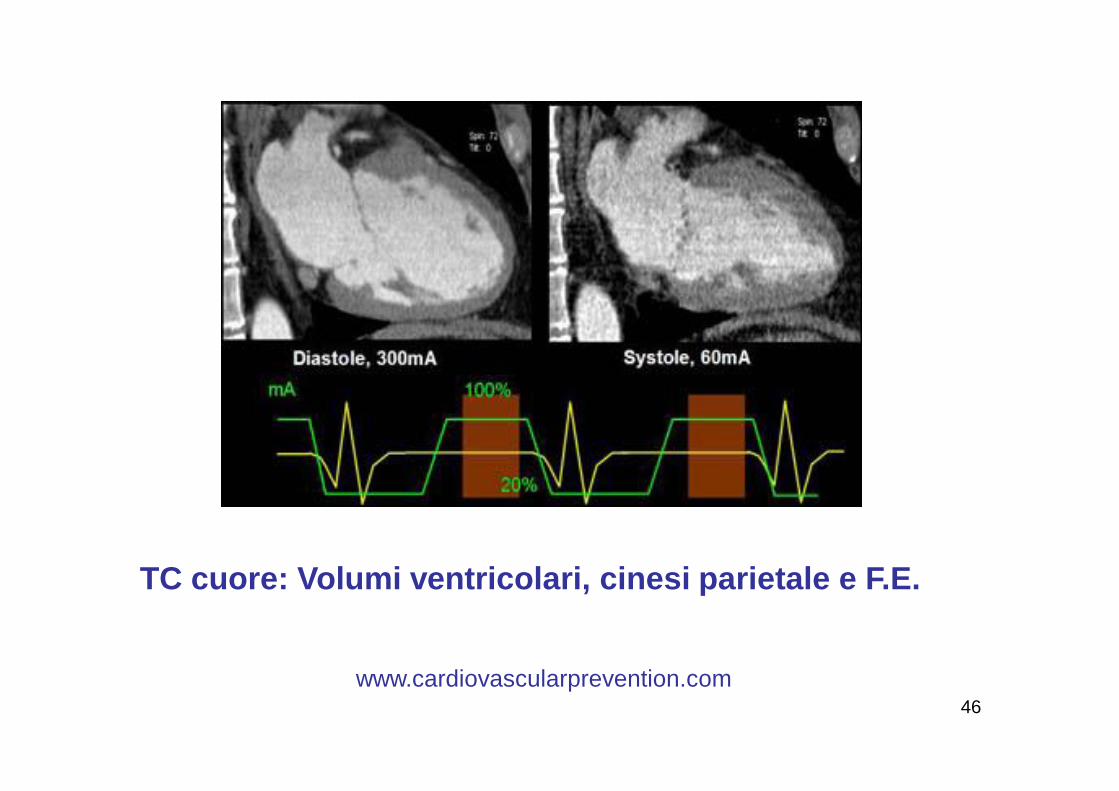
TC cuore: Volumi ventricolari, cinesi parietale e F.E.
www.cardiovascularprevention.com
47www.cardiovascularprevention.com
48
Noninvasive Screening for Coronary Artery Disease With Computed Tomography Is Useful
Melvin E. Clouse, MD
www.cardiovascularprevention.com

49
Il Nostro ProgrammaScoperta del Paziente Vulnerabile
• Prevenzione e diagnosi precoce:- della cardiopatia ischemica- dello scompenso cardiaco- Dell’ ictus cerebrale
CON ALTA TECNOLOGIA
www.cardiovascularprevention.com
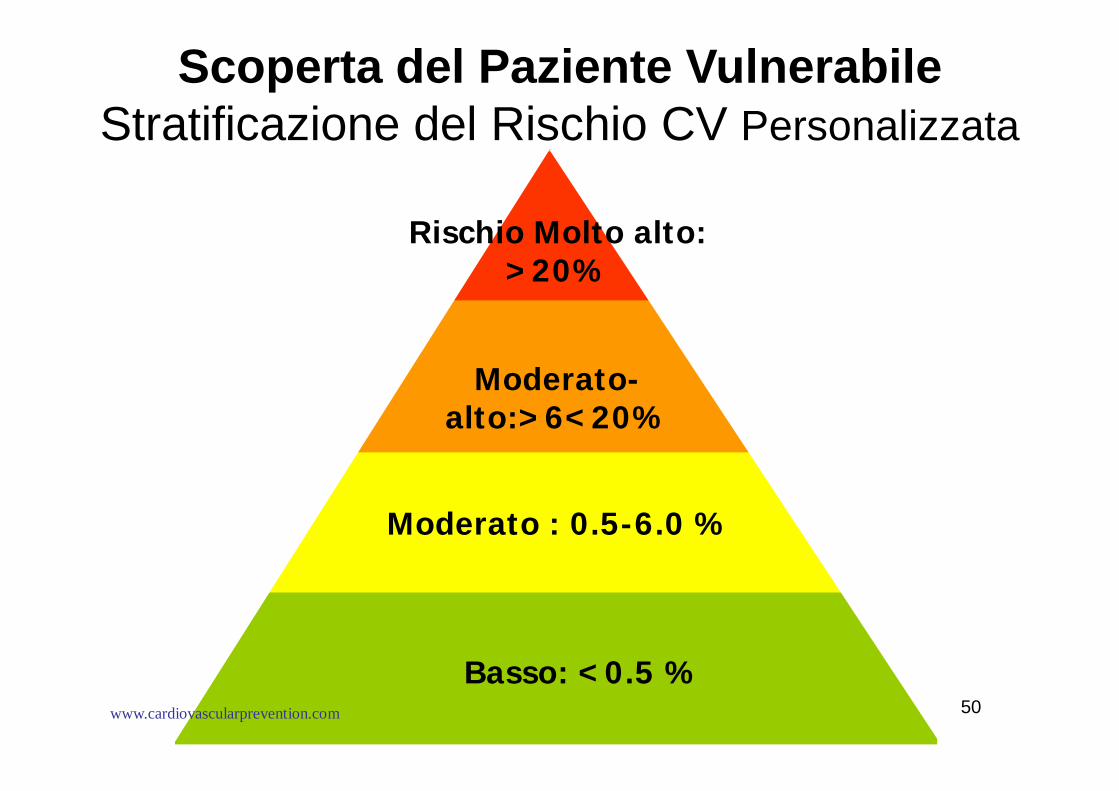
50Basso: <0.5 %
High: >2%
Moderato : 0.5-6.0 %
Moderato-alto:>6<20%
Rischio Molto alto: >20%
Scoperta del Paziente VulnerabileStratificazione del Rischio CV Personalizzata
www.cardiovascularprevention.com

51
Il Nostro Programma:Scoperta del Paziente Vulnerabile
Valutazione del rischio morte/IMA a 5-10 anni con algoritmo dedicato
§ Calcium score§ CIMT
§ Storia Clinica e FRC comuni e non comuni
§ Angio TC coronarica
Valutazione dei FRC secondo il modello Framingham e
NCEP Panel III =
Insufficiente 50%
Metodica AttualeNuova Metodica
www.cardiovascularprevention.com
52
Il Nostro Programma:Fattori di rischio noti e meno noti
-Età
-Colesterolo totale
-Colesterolo LDL
-Colesterolo HDL
-Apolipoproteina B /A1
-P.A. Sistolica
-Diabete
-Fumo di sigaretta
-Microalbuminuria
-ECG
-Pregresso IMA o Angjna P
-Hs PCR
-Fibrinogeno
-Omocisteinemia
-Vita sedentaria
-Obesità
-Fattori Psico-Sociali
-Familiarità
-Alimentazione
-Disfunzione erettile
www.cardiovascularprevention.com