la terapia antibiotica,i fluidi, il sostegno emodinamico...
TRANSCRIPT

La terapia antibiotica,i fluidi, il sostegno emodinamico nella sepsi
severa
Roberto Fumagalli Ospedale Niguarda Ca’ Granda Universtà degli Studi Milano Bicocca
Financial disclosure: none
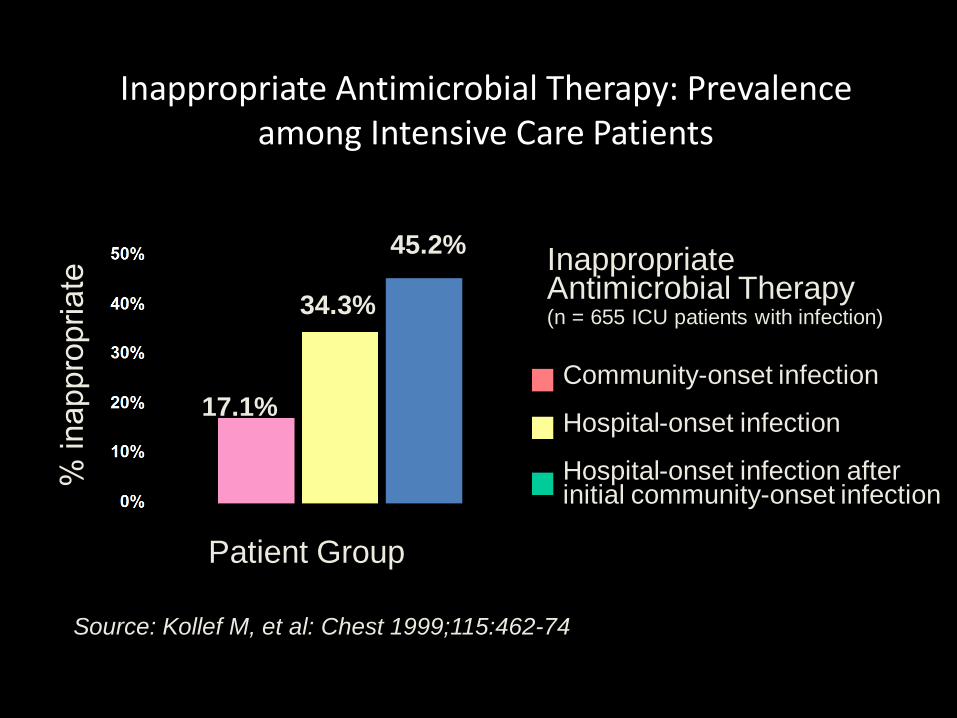
Inappropriate Antimicrobial Therapy: Prevalence among Intensive Care Patients
Source: Kollef M, et al: Chest 1999;115:462-74
Community-onset infection Hospital-onset infection Hospital-onset infection after initial community-onset infection
Inappropriate Antimicrobial Therapy (n = 655 ICU patients with infection)
Patient Group
17.1%
34.3%
45.2%
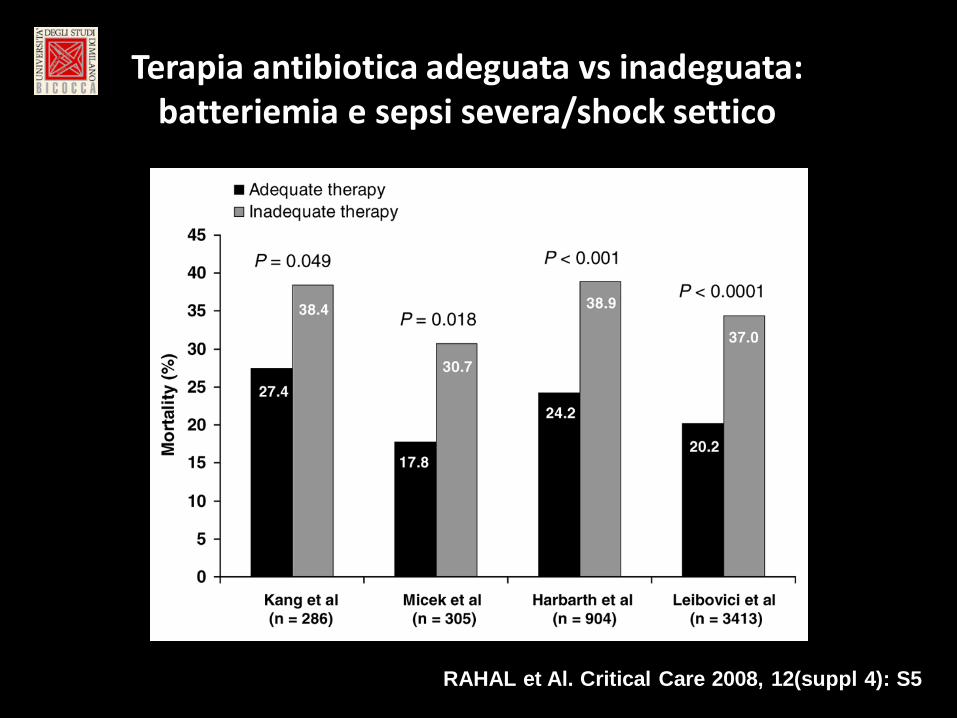
Terapia antibiotica adeguata vs inadeguata: batteriemia e sepsi severa/shock settico
RAHAL et Al. Critical Care 2008, 12(suppl 4): S5


Early antibiotics are good... Author n Setting Median time
(mins) Odds Ratio for death
Gaieski Crit Care Med 2010; 38:1045-53
261 ED, USA (Shock)
119 0.30 (first hour vs all times)
Daniels Emerg Med J 2010; doi:10.1136
567 Whole hospital, UK
121 0.62 (first hour vs all times)
Kumar Crit Care Med 2006; 34(6):1589-1596
2154 ED, Canada (Shock)
360 0.59 (first hour vs second hour)
Appelboam Critical Care 2010; 14(Suppl 1): 50
375 Whole hospital, UK
240 0.74 (first 3 hours vs delayed)
Levy Crit Care Med 2010; 38 (2): 1-8
15022 Multi-centre 0.86 (first 3 hours vs delayed)

ANTIBIOTICOTERAPIA • Somministrazione ev di ATB entro la prima
ora dal riconoscimento della sepsi grave o dello shock settico
• Utilizzare un ampio spettro ATB (uno o più) empirico contro il possibile patogeno, che penetri bene nel sito di infezione
RACCOMANDATO

ANTIBIOTICOTERAPIA
• La restrizione degli antibiotici per ridurre le resistenze e i costi non è la strategia iniziale appropriata per questi pz.
• Limitare la durata della terapia a 7-10 gg; – durata maggiore se risposta clinica lenta, immunodeficienza o se foci non
drenabili • Stop ATB se confermata causa non infettiva • Terapia di combinazione
– Se Pseudomonas – Pz neutropenico – Per < di 3-5 gg poi de-escalation dopo aver ottenuto l’antibiogramma
DE-ESCALATION THERAPY
Stage 1 • Administering the broadest-spectrum
antibiotic therapy to improve outcomes (decrease mortality, prevent organ dysfunction, and decrease length of stay)
Stage 2 • Focusing on de-escalating as a means to
minimize resistance and improve cost-effectiveness

Conclusions: De-escalation appears feasible in most cases without any obvious negative clinical impact in a medical ICU.



Esse sono, insieme, conseguenza e causa di eventi metabolici e danno tissutale
Le alterazioni circolatorie hanno un ruolo centrale nello SHOCK settico
L’evento emodinamico principale nello shock settico è la
MODS INSUFFICIENZA CARDIOCIRCOLATORIA
vasodilatazione arteriosa
COMPONENTI:
Vasodilatazione arteriosa
Ipovolemia - perdite verso l’esterno - aumentata permeabilità
“Depressione miocardica” - ridotta compliance - ridotta frazione d’eiezione
MODS INSUFFICIENZA CARDIOCIRCOLATORIA

COMPONENTI:
Vasodilatazione arteriosa
Ipovolemia - perdite verso l’esterno - aumentata permeabilità
“Depressione miocardica” - ridotta compliance - ridotta frazione d’eiezione
MODS INSUFFICIENZA CARDIOCIRCOLATORIA
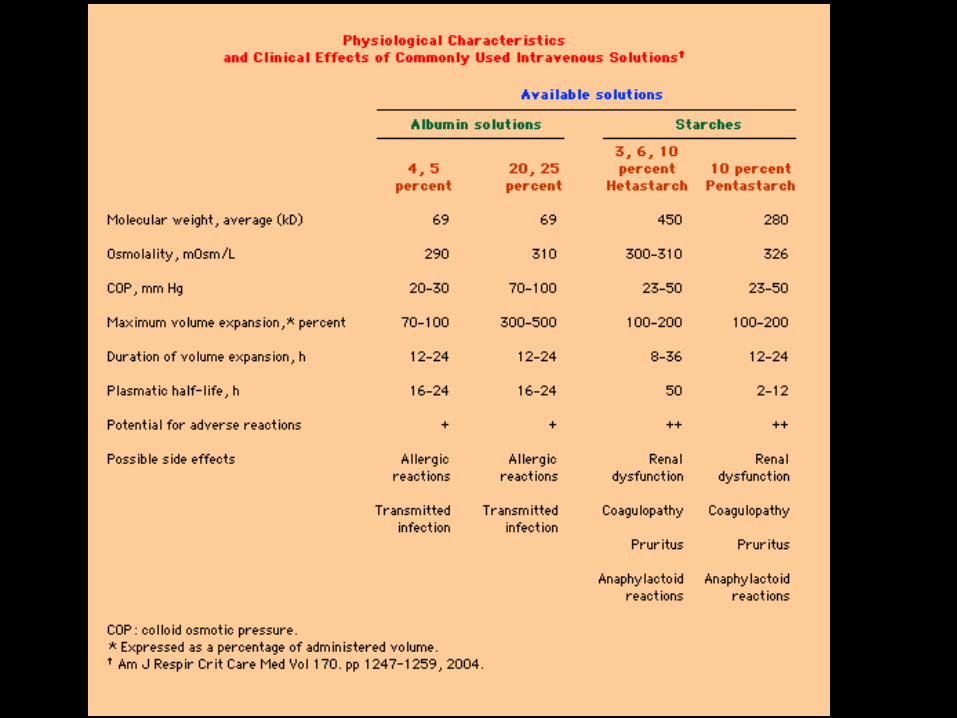
Types of Colloids

Types B

VISEP Study (Volume Substitution and Insulin Therapy in Severe Sepsis)

P=0.14 P=0.001
Normal Over
Low dose: ≤ 22 mL/kg BW/d; High dose: > 22 mL/kg BW/d Brunkhorst FM et al. NEJM 2008;358:125–39

Cumulative Effect of Volume Resuscitation on the Need for Renal-Replacement Therapy and the Rate of Death at 90 Days
Brunkhorst FM et al. N Engl J Med 2008;358:125-139

6S Study (Scandinavian Starch for Severe Sepsis/Septic Shock)

Investigation in haemodynamically mostly stabilized patients → no indication for HES!
Volumen replacement was not goal-directed. Criteria for renal replacement therapy
(a secondary outcome variable) were not defined! Use of potato-derived starch solution
Perner A et al. N Engl J Med 2012;367:124-34
6S Study – Main limitations –

CHEST Study (Crystalloid versus Hydroxyethyl Starch Trial)

HES Saline Relative Risk (95% CI) P Value
Myburgh JA et al. N Engl J Med 2012;367:1901-11

• Criteria for begin of renal replacement therapy (RRT) were not defined (”… such therapy was initiated at the discretion of the attending clinicians …“). • RRT was merely a secondary endpoint → adequate power only for primary endpoint → lack of statistical validity regarding RRT data
BUT!


Mortality and Hydroxyethyl Starch
Zarychanski R, et al. JAMA 2013;309:678–88

N Engl J Med. 2014 Apr 10;370(15):1412-21.

METHODS
● During the early phase of volume resuscitation, fluids were administered in both groups according to early goal-directed therapy
● In the a. g. 20% from day 1 until day 28 albumin was administered on a daily basis, to mantain a serum albumin level of 30 g/L or more (300 ml if <25, 200 ml if between 25 and 30g/L).
● In both groups crystalloids whenever clinically i di d
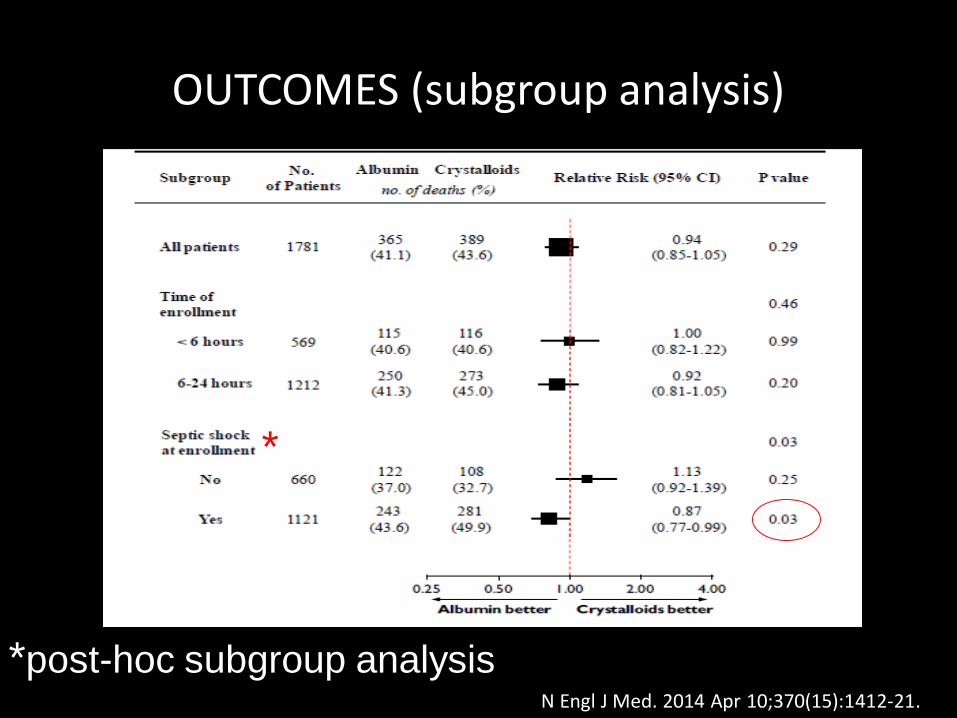
OUTCOMES (subgroup analysis)
*post-hoc subgroup analysis
*
N Engl J Med. 2014 Apr 10;370(15):1412-21.





COMPONENTI:
Vasodilatazione arteriosa
Ipovolemia - perdite verso l’esterno - aumentata permeabilità
“Depressione miocardica” - ridotta compliance - ridotta frazione d’eiezione
MODS INSUFFICIENZA CARDIOCIRCOLATORIA

Meccanismi fisiopatologici della vasodilatazione
Donald, N Eng J Med, 2001

Receptor Physiology
Receptor Location Effect
Alpha-1 Adrenergic Vascular wall Vasoconstriction
Heart Increase duration of contraction without
increased chronotropy
Beta Adrenergic Beta-1 Heart ↑Inotropy and chronotropy
Beta-2 Blood vessels Vasodilation
Dopamine Renal Vasodilation
Splanchnic (mesenteric)
Coronary Cerebral
Subtype Vasoconstriction

Drug Alpha-1 Beta-1 Beta-2 Dopaminergic Predominant Clinical Effects
(Neosynephrine) Phenylephrine *** 0 0 0 SVR ↑ ↑, CO ↔/↑
(Levophed) Norepinephrine *** ** 0 0 SVR ↑ ↑, CO ↔/↑
(Adrenalin) Epinephrine *** *** ** 0
CO ↑ ↑, SVR ↓ (low dose) SVR/↑ (higher dose)
(Intropin) Dopamine
(mcg/kg/min)
0.5 to 2 0 * 0 ** CO
5 to 10 * ** 0 ** CO ↑, SVR ↑
10 to 20 ** ** 0 ** SVR ↑ ↑
Dobutamine 0/* *** ** 0 CO ↑, SVR ↓
Isoproterenol 0 *** *** 0 CO ↑, SVR ↓
*** Very Strong Effect, ** Moderate effect, * Weak effect, 0 No effect.
Vasoactive Medication Receptor Activity and Clinical Effects


Original Article Vasopressin versus Norepinephrine Infusion
in Patients with Septic Shock James A. Russell, M.D., Keith R. Walley, M.D., Joel Singer, Ph.D., Anthony C. Gordon, M.B., B.S., M.D., Paul C. Hébert, M.D., D. James Cooper, B.M.,
B.S., M.D., Cheryl L. Holmes, M.D., Sangeeta Mehta, M.D., John T. Granton, M.D., Michelle M. Storms, B.Sc.N., Deborah J. Cook, M.D., Jeffrey J.
Presneill, M.B., B.S., Ph.D., Dieter Ayers, M.Sc., for the VASST Investigators
N Engl J Med Volume 358(9):877-887
February 28, 2008

Kaplan-Meier Survival Curves for Patients Who Underwent Randomization and Infusion
Russell JA et al. N Engl J Med 2008;358:877-887

INTERACTIONS BETWEEN FLUIDS AND VASOACTIVE AGENTS ON MORTALITY IN
SEPTIC SHOCK: A MULTICENTER OBSERVATIONAL STUDY
J Waecher et al: CCM Oct 2014, 42,10:2158-2168
Retrospective evaluation using a multivariate logistic regression to evaluate the association between
mortality, timing and amount of fluid resuscitation in septic shock

The focus during the first hour of resuscitation should be aggressive
fluid administration only thereafter starting vasoactive drugs
INTERACTIONS BETWEEN FLUIDS AND VASOACTIVE AGENTS ON MORTALITY IN SEPTIC SHOCK: A MULTICENTER OBSERVATIONAL STUDY
J Waecher et al: CCM Oct 2014, 42,10:2158-2168


Thank you [email protected]