final version falls report 0405 - stockport nhs foundation ... · pdf filegreater manchester...
TRANSCRIPT

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
1
CONTENTS
Page1 Executive Summary 22 Project Board 43 Background 54 Aims and Objectives 75 Developing the Audit and Data Collection Strategy 86 Standards 97 Data Collection and Methodology 148 Results 199 Summary/Conclusions 4110 References 4611 Contact Details 4812 Acknowledgements 49
APPENDICESAppendix 1 List of Charts and Tables 50Appendix 2 Hospital wards – type and number of beds 51Appendix 3 Hospital Falls Services 53Appendix 4 Feedback Seminar Attendees 56Appendix 5 Proforma 57

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
2
1. EXECUTIVE SUMMARY
The purpose of this report is to inform Trust Management/Executive Teams, PCTs,
Strategic Health Authorities and the Greater Manchester Clinical Audit Group of the
outcome of the recent Greater Manchester and Wirral Falls Risk Assessment Audit.
The principal aim is to audit current Falls Management and Prevention in a group of
Hospitals across Greater Manchester within the context of the National Service
Framework for Older People.
The main results of the audit concentrate on assessments and documentation, risk
factors, mobility assessments, interventions and prevention measures, and the
possible impact of falls risk assessment tools (FRA) in preventing falls in hospital.
• Patients in the sample were predominantly the very elderly, those aged 80 years or
more comprised almost 58% of the sample. This proportion varied by Trust from,
45% in MRI to 73% at the Wirral.
• Approximately 30% of patients in the sample were admitted with a fall.
• Between 85 - 95% of patients in 4 of the hospitals were assessed. The other 6
hospitals all fell below the mean value, which was less than 53%.
• Overall 34% of patients who had a risk assessment were reviewed.
• Some form of action to prevent falls was taken in 61% of patients who had a risk
assessment form in the 5 hospitals that used Falls Risk Assessment forms.
• Patients were more likely to have mobility and/or transfer assessments done than
other assessments such as Lying & Standing BP and Medication reviews.
• The most likely interventions included referral to a physiotherapist and/or an OT,
the patient was placed under close observation, and a call bell was at hand.
• Patients having a FRA completed were significantly more likely to have certain
prevention measures.
• Fewer patients fell in the group that had a FRA completed.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
3
The main conclusions from the audit are: using a FRA may have a protective effect;
the patients are more likely to have prevention measures targeted at them; in-patient
falls were less likely in hospitals using a FRA and patients with risk factors are not
necessarily being documented as being at risk of falling.
Following the feedback seminar a Falls Working Group will be set up to look at
multidisciplinary core skills in relation to an inpatient falls action plan and to explore
standardising falls risk assessment and intervention across Greater Manchester.
Funding for the audit was provided by the Greater Manchester Clinical Audit Leads
Group.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
4
2. PROJECT BOARD
Members Title Organisation
Mrs J Barnes Physiotherapist Tameside & Glossop AcuteServices NHS Trust
Dr D BourneConsultant in GeneralMedicine and ElderlyCare
Central Manchester & ManchesterChildren’s University HospitalsNHS Trust *
Dr G Cook ConsultantEpidemiologist Stockport NHS Foundation Trust
Mrs J Gray Falls Co-ordinator South Manchester UniversityHospitals NHS Trust
Mrs S Gunnion Lead Falls NurseCentral Manchester & ManchesterChildren’s University HospitalsNHS Trust **
Dr M Hanley Consultant in ElderlyMedicine Stockport NHS Foundation Trust
Mrs J Powell Falls Prevention Officer Pennine Acute Hospitals NHSTrust
Dr M Pritchard-Howarth
ConsultantOrthogeriatrician Wirral Hospital NHS Trust
Ms J Rodgers Audit Co-ordinator Stockport NHS Foundation Trust
Jacquie Ruddick Clinical Governance Co-ordinator Wirral Hospital NHS Trust
Mrs G Wakefield Clinical GovernanceFacilitator Trafford Healthcare NHS Trust
* Now employed by South Manchester University Hospitals NHS Trust** Now employed by Stockport PCT

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
5
3. BACKGROUND
Injury is a leading contribution to the burden of disease in the world. In 1998 injury
from falls was the 14th leading contributor for all age groups (Myers, 2003). Falls are a
major cause of disability and the leading cause of mortality due to injury in people
aged over 75 in the UK. Up to 14,000 people a year die in the UK as a result of an
osteoporotic hip fracture (DoH, 2001). Falls prevention is a priority area for research
and interventions. Identification of high risk patients is an important component of falls
prevention measures (Myers, 2003).
NSF for Older People
The National Service Framework (NSF) for Older People, recognises the importance
of prevention (DoH, 2001). The NSF sets out the aims in standard six, to reduce the
number of falls which result in serious injury and to ensure effective treatment and
rehabilitation for those who have fallen. The NSF promotes the establishment of
specialist falls services within specialist multidisciplinary and multi-agency services for
older people including health and social care staff that target, especially, older people
who are at high risk of falling.
As part of the Service Model, the NSF states that staff in hospitals should be trained to
recognise when older people are at risk of falling and be able to refer them to the falls
service for assessment. Assessments should identify the risk factors for falls and
osteoporosis and offer appropriate interventions. Current practice should be examined.
New procedures should be agreed by a range of professionals involved in the falls
service. Finally, prior to discharge, the needs of the patient and their carers for care
and support at home should be identified. This includes making sure that patients are
advised about how they can reduce their risk of falling and therefore prevent further
falls or fractures. (DoH, 2001)
This audit aimed to assess whether or not such services were established in the
hospitals involved. Preventing falls in older people depends on identifying those most
at risk of falling and co-ordinating appropriate preventative action. The audit would

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
6
examine how hospitals identify those at risk and whether this is routinely done and
what preventative measures are then put into place. The audit would examine current
practice and whether the standards developed within and through the NSF had been
met.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
7
4. AIMS & OBJECTIVES
AIM
To audit current falls management and prevention in a group of hospitals across
Greater Manchester in support of the National Service Framework for Older People.
OBJECTIVES
I. To conduct a multidisciplinary audit of the use of risk assessment tools for falls
prevention on Care of the Elderly and Trauma and Orthopaedics wards
II. To develop further the multidisciplinary clinical network between Care of the
Elderly, Trauma and Orthopaedics and Anaesthetics
III. To develop further links with the local collaborative initiatives around
orthopaedics and care of the elderly
IV. To establish a baseline of current services within each hospital setting

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
8
5. DEVELOPING THE AUDIT AND DATA COLLECTIONSTRATEGY
5.1 Trusts participating in the audit
Six trusts from Greater Manchester and one from Wirral were recruited to the audit.
The trusts were Central Manchester & Manchester Children’s University Hospitals
NHS Trust, Pennine Acute Hospitals NHS Trust (across 4 hospital sites), South
Manchester University Hospitals NHS Trust, Stockport NHS Foundation Trust,
Tameside & Glossop Acute Services NHS Trust, Trafford Healthcare NHS Trust and
Wirral Hospital NHS Trust. In total 10 hospitals participated.
5.2 Progression and Development
A multidisciplinary project group comprising Care of the Elderly Physicians,
Physiotherapists, Nursing staff and Clinical Audit staff met on four occasions to agree
the audit questions, audit criteria and standards and methodology.
From discussions in the group it appeared that there are 2 main risk assessment tools
for falls currently in use in the hospitals involved, these are:
FRASE (Cannard, 1996): An adaptation of this un-validated tool is currently in use in
Stockport and Tameside.
STRATIFY (Oliver et al, 1997): A tool developed in an NHS setting with a good
evidence base, in use at South Manchester, Wirral and Pennine.
The audit criteria were derived largely from the NSF and the above tools. A few
additional criteria were decided upon by the project group using a variety of resources
(see section 6).
5.3 Other Information
Information was collected concerning resources about each individual hospital site to
enable a comparison of the structure of the hospitals’ falls service. Information
includes for example: whether or not there was a falls co-ordinator and what their role
was, was a falls risk assessment tool being used and the number of falls in a year.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
9
6. STANDARDS
6.1 The National Service Framework for Older People was published in 2001. It set
new national standards and service models of care across health and social services
for all older people. It addresses those conditions which are particularly significant for
older people - stroke, falls and mental health problems associated with older age. (For
further background information please refer to the NSF for Older People document
which be found on the Department of Health website).
The NSF focuses on:
• rooting out age discrimination
• providing person-centred care
• promoting older people’s health and independence
• fitting services around people’s needs.
This audit focuses on Standard Six: Falls. The aim of standard six is: to reduce the
number of falls which result in serious injury and ensure effective treatment and
rehabilitation for those who have fallen. (DoH, 2001)
The standard set by the NSF was as follows: the NHS, working in partnership with
councils, takes action to prevent falls and reduce resultant fractures or other injuries in
their populations of older people. Older people who have fallen receive effective
treatment and, with their carers, receive advice on prevention through a specialised
falls service. (DoH, 2001)
Prevention
Preventing falls in older people depends on identifying those most at risk of falling and
co-ordinating appropriate preventative action. Older people may be identified as being
at risk through the presence of certain risk factors. Interventions which target both
multiple risk factors for individuals (intrinsic risk factors) and environmental hazards
are most successful.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
10
Specialist assessment should be carried out by the falls service in collaboration with
primary and social care professionals. This should build on the single assessment
process. It should identify risk factors associated with an older person’s health. (DoH,
2001)
Two particular criteria addressed by the audit are:
• An operational falls service has been set up in each local health economy with
appropriate complement of staff. (DoH, 2001)
• The falls service has access to dieticians, optometrists, orthotists,
ophthalmologists, audiologists, bi-linguists, and to bone densomitry. Older
people who fall should, with their consent, be referred to a specialist falls
service. (DoH, 2001)
Interventions
Interventions should be agreed with the individual concerned. These may include:
• diagnosis and treatment of underlying medical problems such as eye
examinations, correction of postural hypotension or cardiac rhythm abnormality,
changes in medication etc.
• rehabilitation, including physiotherapy to improve confidence in mobility,
occupational therapy to identify home and environmental hazards
• equipment to improve the safety of the older person at home
• repairs or improvements to the home and an assessment for home adaptations
if warranted
• social care support.
Falls prevention programmes for individuals should contain more than one intervention
and focus on the individual’s particular risk factors. These interventions are focused
upon in the audit and are identified on the audit form in sections F, G and H (see
appendix 5 for a copy of the proforma).
Falls in hospitals should be recorded on registers. Although we did not look at this
specifically in the audit it is an important part of falls prevention. Critical incident

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
11
analysis, following a fall will develop an awareness and learning culture amongst staff
and will ensure that action taken will minimise future incidents.
6.2 Other documents used:
Scottish Intercollegiate Guidelines Network (SIGN)
The SIGN guidelines number 56 Prevention and Management of Hip Fracture in
Older People suggest older people should be assessed for risk of falling by using
identified risk indicators (patient and environment) and any interventions should be
based on this risk assessment.
The guidelines also suggest that those at increased risk should be offered multiple
interventions, e.g. exercise programme, balance training, modification of identified
hazards etc, aimed at reducing the identified individual and environmental risks.
The British Orthopaedic Association’s document The Care of Fragility Fracture
Patients has a small section on falls prevention. It suggests that a full clinical history
should identify possible factors predisposing to falls such as postural hypotension,
diabetes and alcohol excess. They also suggest that if a risk remains then hip
protectors should be considered.
The Best Practice document Falls in Hospital also suggested a number of risk
factors, which were looked at by the project group and incorporated into the proforma.
It also suggests that education should be part of the falls program, targeting staff,
patients and relatives to increase their awareness of the risk of falling during
hospitalisation and to try and minimise this risk.
The British Geriatrics Society’s Guideline for the Prevention of Falls in Older
Persons aims to assist health care professionals in their assessment of falls risk and
in their management of older patients who are at risk of falling and those who have
fallen. The guideline listed certain interventions and analysed how effective they were,
for example exercise, review of medications, environmental modifications, footwear
etc.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
12
6.3 Standards set by the Project Group
Risk Factors
The project group identified specific risk factors that were incorporated into the
proforma, these include for example:
• taking four or more medications, especially sedative hypnotics
• visual impairment
• impaired cognition, confusion, depression
• history of falls
• Particular medical conditions, e.g. Diabetes, Parkinson’s, Stroke
The extent to which these clinical risk factors are documented through the risk
assessment tool will be audited.
Intervention Measures
The group also identified a number of intervention measures that can be used to
prevent falls. Sources included the Action Plan used by Stockport NHS Foundation
Trust. See section 7.1 for further details regarding interventions. Examples of
interventions include:
• Using a coloured wristband to identify those at risk
• Frequent toileting
• Educating the patient and relatives
• Bed Rails
• Home visit to assess the patient’s home for risk factors
The standard ideal for both of these factors was that in all patients’ records there was
documented evidence of checking for the risk factors and including or excluding
interventions.
The full list risk factors and interventions can be found on the proforma in appendix 5.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
13
Other standards:
• A falls risk assessment tool is in use on the appropriate wards in each hospital.
• An environmental audit tool and action plan is in place
• All patients are assessed and a completed form is in each patient’s set of notes.
• Each form is fully completed.
• In appropriate cases patients will have been re-assessed after one week, and their
care plan reviewed.
• All patients who are classified at high risk have an appropriate care plan and
preventive steps outlined and acted upon.
Other issues that would be looked for:
• All ward staff have been formally trained on how to use the tool
• The use of health promotion material
• The provision of Falls clinics, patient sitter programmes and response systems
• The issue of patient information, for example Falls Prevention: Your safety
checklist and guide.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
14
7. DATA COLLECTION & METHODOLOGY
7.1 Developing the Proforma
Section A asks for demographic information such as the date of birth and gender.
Section B was designed to capture details about the episode such as date of
admission, reason for admission and whether the admission was due to a fall.
Section C was designed using the various risk assessment tools; it is to assess how
thoroughly the risk assessment form has been completed for each patient. It should
cover all aspects of all the different tools.
Section D was designed for hospitals that didn’t use a tool and for patients who had
not had a formal assessment using a falls risk assessment tool. The questions were
designed to see if any other assessment for falls risk had been carried out or to see if
any staff had noted that the patient was at risk of falling.
Section E the list of risk factors was identified as detailed in Section 6 Standards. It
was noted on the proforma if the patient had had any of these risk factors recorded or
excluded anywhere in the patient’s notes.
Section F is used to record whether or not assessments for certain indicators of falls
risk have been carried out. Again the project group decided upon these indicators after
looking through the guidelines.
Section G was included to determine whether or not certain assessments usually
done by Physiotherapists and Occupational Therapists had been carried out as
appropriate. The project group devised the list, members advised the group as to what
assessments their particular hospital used so that the section would cover all possible
assessments

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
15
Section H was mainly taken from the action plan used at Stockport NHS Foundation
Trust. Additional interventions came from the various guidelines and papers reviewed
by members of the group. Project group members added other interventions to the
proforma, in accordance to what is in place specifically at their particular hospitals.
The purpose of this section was to ascertain whether or not any interventions, which
are believed to help reduce the risk of falls, were implemented and whether or not the
decision had been recorded in the casenotes. Some of the interventions are only
appropriate for a patient with specific risks e.g. dementia, the need to ‘special’ the
patient, trial without catheter etc. Some were only appropriate if the patient had been
assessed as being at risk or at high risk of falling.
The following interventions from the list were taken from the Action Plan used at
Stockport
• Close observation of patients in an appropriate area.
• Assess for the use of alarms on bed/chair.
• Assess the need for hip protectors
• Assess the need to “special” the patient if they are a frequent faller.
• Undertake in-depth assessment of patients’ dementia.
• Frequent toileting of high-risk patients.
• Coloured wristband to alert staff of risk of patient falling.
• Inform physiotherapist of patients at high risk.
• Call bell is at hand
• If appropriate explain to the patient the importance of asking for help whenwalking
• Leave bed in low position when patient is unattended
• Use a chair, of appropriate height for the individual (Hips should be flexed at90° and feet should be flat on the floor)
• Footwear assessment documented
• Discuss patients’ risk of falling with relatives, if appropriate.
Section I included other related information such as whether or not the patient fell
during the time they were in hospital and specific details regarding the fall. This would

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
16
be used to determine whether or not using a risk assessment tool was effective in
preventing falls in hospital.
The proforma for collecting audit data was piloted twice, in February and March 2004,
with help from members of the project board, before a final version was agreed.
A copy of the proforma can be found in appendix 5.
7.2 Sample
The project board members decided upon the sample size and inclusion criteria. It was
decided to take 52 patients from each trust aged 65 and over. These 52 patients would
be spread over Care of the Elderly and/or General Medical wards and Orthopaedic
wards, with 40 from Care of the Elderly/Medical and 12 from Orthopaedics. It was
agreed that the patients in the sample must have been in hospital for at least 3 days.
For a list of wards and number of beds please see appendix 2.
Inclusion Criteria:
• Patients aged 65 and over
• In-patient for 3 or more days
• On General/Adult Medical, Care of the Elderly and Orthopaedic wards
Exclusion Criteria:
• Patients under 65 years of age
• In patient for less than 3 days
• On any other ward not stated above
• Elective patients
• On rehab wards
7.3 Data Collection
The project co-ordinator visited staff at each hospital before data collection started to
discuss how and when the data collection would be conducted in each hospital.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
17
Data collection began in the first hospital in May 2004, each hospital was allocated a
certain week when data collection would take place, data collection was complete by
the end of the first week of August 2004. See table 1.
Table 1. Data Collection dates at each hospital
HOSPITAL DATA COLLECTION START DATESouth Manchester Tuesday 4 May 2004
Oldham Wednesday 2 June 2004Wirral Tuesday 8 June 2004
Stockport Monday 14 June 2004Trafford Tuesday 22 June 2004
MRI Monday 28 June 2004Rochdale Thursday 15 July 2004Tameside Tuesday 20 July 2004
North Manchester Monday 26 July 2004Bury Tuesday 3 August 2004
Up to 5 Medical/Care of Elderly wards were selected, as can be seen in the table 2.
Some hospitals used all Care of the Elderly wards, some did not have specific Elderly
wards and so used 5 General/Adult Medical wards, those that had both types of wards
used a mix of the two types.
Table 2. Number of Wards at each hospital by specialty
HOSPITAL CARE OFELDERLY
GENERAL/ADULTMEDICAL T&O
South Manchester 0 5 1Oldham 0 5 1Wirral 5 0 1
Stockport 2 3 2Trafford 2 3 1
MRI 0 5 1Rochdale 0 5 1Tameside 0 5 2
North Manchester 0 5 1Bury 0 5 2
Lists of all patients on the appropriate wards were generated from the Information
departments or PAS systems. All inappropriate patients, i.e. those with exclusion
criteria, were removed from the lists. Using Microsoft EXCEL each ward list was
randomised and the first 8 patients on each of the lists were selected from each of the
5 wards, making 40 in total. If a patient’s notes were unavailable on arrival on the
wards the next patient on the randomised list was selected and so on.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
18
Most of the hospitals had one main trauma ward but a few had more than one ward.
Where there was more than one trauma ward all the patients from both wards were
added together and the sample of 12 patients was randomly selected from the list.
Lists were randomised in the same way as the Medical wards. The first 12 patients
were randomly selected from the orthopaedic wards.
The Audit co-ordinator worked with staff from various departments including Clinicians,
Clinical Audit staff, Physiotherapists and Occupational Therapists at each hospital to
complete the proformas for the data collection.
Data from completed proformas was entered onto an Access database by the Audit
Co-ordinator. Data was then analysed using Excel spreadsheets and pivot tables.
Some hospitals were not using a falls risk assessment tool or were only just
implementing a tool. For part of the analysis the hospitals were split into 2 groups. The
first group included those hospitals where the tool was established and should have
been in use throughout the hospital. The second group consisted of those hospitals
not using the tool or only just introducing it.
Information regarding falls services, incident reporting of falls and the use of falls risk
assessments was also collected from each hospital. Information gathered can be
found in appendix 3.
The project board met again in September 2004. The purpose of the meeting was to
agree a format for feeding back the results, to discuss the preliminary results of the
audit and to discuss any specific issues raised by the results and clarify what should
be presented at the main feedback seminar.
The main feedback seminar was held on 1st November 2004 at Stepping Hill Hospital,
Stockport and was well attended by representatives from various NHS Trusts and
other NHS organisations. The results of the audit were presented to the audience.
Trusts will also be able to present their results to staff at their own meetings.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
19
8. RESULTS
8.1 General Demographics
Table 3. General Demographics7 Trusts/10 Hospital Sites 518 Patients52 patients from 9 hospitals, 50 from 1 hospitalMean Age = 81.5 Age Range = 65 – 100Male:Female = 2:3 (3 gender unknown)Average time in hospital = 22 days Range = 3 days – 179 days
Chart 1. Age Group by Hospital
N = 518Comment
Patients included were predominantly the very elderly, those aged 80 years or more
comprised almost 58% of the sample. This proportion varied by Trust from, 45% in
MRI to 73% at the Wirral.
This degree of variation may be explained by the different types of wards used in each
hospital and the predominance of younger or older patients accordingly. Some
hospitals did not have specific Care of the Elderly wards and so General/Adult Medical
wards were used were there is a greater mix of ages, some had a mix of different
types of wards and one of the hospitals used all Care of the Elderly wards. See
appendix 2.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
BuryM
RI
NMGH
Oldham
Rochdale
Stockport
Tamesid
e
Traffo
rd
Wirr
al
Wyth
enshawe All
65-79
80+

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
20
Chart 2. Proportion of Patients admitted due to a fall
N = 518
Comment
The mean percentage of patients admitted with a fall is just over 30%. 6 hospitals fell
below this average, 3 were just above the average, and 1 hospital had nearly 20%
more patients admitted with a fall than the average.
0%
10%
20%
30%
40%
50%
60%
Bury
MRI
NMGH
Oldham
Rochdale
Stock
port
Tamesid
e
Traffo
rd
Wirr
al
Wyth
ensha
we
% FALL
MEAN
GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
21
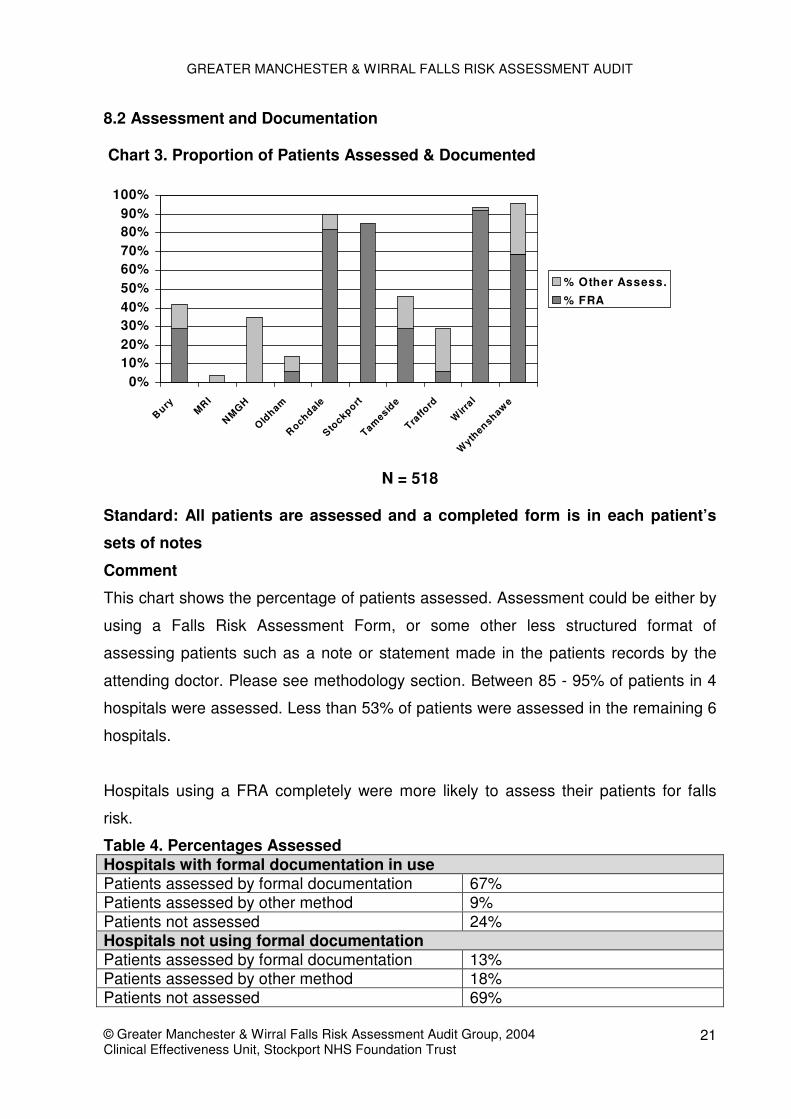
8.2 Assessment and Documentation
Chart 3. Proportion of Patients Assessed & Documented
N = 518
Standard: All patients are assessed and a completed form is in each patient’s
sets of notes
Comment
This chart shows the percentage of patients assessed. Assessment could be either by
using a Falls Risk Assessment Form, or some other less structured format of
assessing patients such as a note or statement made in the patients records by the
attending doctor. Please see methodology section. Between 85 - 95% of patients in 4
hospitals were assessed. Less than 53% of patients were assessed in the remaining 6
hospitals.
Hospitals using a FRA completely were more likely to assess their patients for falls
risk.
Table 4. Percentages AssessedHospitals with formal documentation in usePatients assessed by formal documentation 67%Patients assessed by other method 9%Patients not assessed 24%Hospitals not using formal documentationPatients assessed by formal documentation 13%Patients assessed by other method 18%Patients not assessed 69%
0%10%20%30%40%50%60%70%80%90%
100%
BuryM
RI
NMGH
Oldham
Rochdale
Stockport
Tamesid
e
Traffo
rd
Wirr
al
Wyth
enshawe
% Other Assess.
% FRA

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
22
Chart 4. If a form was filled in was it fully completed?
(5 hospitals using a FRA)
N = 258
Standard: Each form is completed fully
Comment
This chart just uses the 5 hospitals that were supposed to be using a FRA all the time
(Oldham, Rochdale, Stockport, Wirral and Wythenshawe).
Where forms were filled in the majority of them were done so completely.
2% 8%
90%
No
Partially
Yes

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
23
Chart 5. If FRA was completed was the patient reviewed during their admission?
(5 hospitals using a FRA)
N = 172
Standard: In appropriate cases patients will have been re-assessed after one
week, and their care plan reviewed.
Comment
Among the 5 hospitals using a FRA, 1 reviewed over 60% of the patients with a
completed FRA, 2 other hospitals reviewed just over 30%. The lower re-assessment
rates may reflect the length of time patients were in hospital. Overall 34% of patients
who had a risk assessment were reviewed.
The criteria stated that if appropriate all patients should be reassessed after one week,
so some of the patients not reviewed might have been in less than one week. Table 5
shows the percentage of patients reviewed by the length of time they were in hospital,
this is also shown for each hospital.
0%
20%
40%
60%
80%
100%
Oldham Rochdale Stockport Wirral Wythenshawe
No/NR
Yes

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
24
Table 5. Percentages reviewed by Length of stay
Stay Number Number (%)with FRA
Number (%)reviewed
<7 days 54 37 (69%) 4 (11%)> 7 days 204 135 (66%) 54 (40%)By hospital number staying >7 daysOldham 47 3 (6%) 0 (0%)Rochdale 42 36 (86%) 25 (69%)Stockport 33 28 (85%) 12 (43%)Wirral 43 41 (95%) 16 (39%)Wythenshawe 39 27 (69%) 1 (4%)
The longer the patients have been in the more likely they are to have been reviewed.
Chart 6. Was the patient reviewed? By Length of stay (in weeks)
N = 172
Average Length of time in hospital
Oldham = 23 days
Rochdale = 25 days
Stockport = 13 days
Wirral = 25 days
Wythenshawe = 19 days
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
<1 week 2 weeks 3 w eeks 4 w eeks >4 weeks
No
Yes

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
25
Chart 7. The proportion of patients with completed FRA for whom action was
taken and documented
(5 hospitals using a FRA)
N = 172
Comment
The proforma was used to assess how well the FRA was used and this included the
question was any action taken to prevent falls. 61% did take some type of preventative
action, but 37% didn’t.
Of the patients included in this analysis, 117 were either said to be at risk or were in a
category of medium or high risk. Of these patients 68% were documented on the
proforma as having action taken to prevent falls.
Of the patients classified as being not at risk, in the low risk category or where level of
risk was not recorded 45% were documented on the proforma as having action taken
to prevent falls. See chart 12 for proportion of patients at risk.
Table 6. Number of risk factors by action recommendedNumber of Risk Factors % Action recommended (FRA completed)
0-2 43%3-5 60%6+ 77%
61%
37%
2%
YesNoNR

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
26
8.3 Risk Factors, assessments and interventions
Chart 8. Number of Risk Factors for whole population
N = 518
Standard: The standard ideal was that in all patients’ records there was
documented evidence of checking for the risk factors.
Comment
This chart shows the distribution of patients according to the number of risk factors
recorded. The graph has a normal distribution. The majority of patients 57% had
between 3 -5 risk factors, 15 patients had 8 or more risk factors, 1 of these had 11 (the
maximum on the list).
9
24
63
101 10291
76
37
15
0
20
40
60
80
100
120
0 1 2 3 4 5 6 7 8+
No of Risk Factors

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
27
Chart 9. Have any of the following Key Risk Factors been assessed?(whole population)
N = 518Comment
This chart shows if certain key risk factors identified by the working group had been
assessed.
Specific assessments such as lying & standing BP and medication review were not
commonly done.
Medication review and mental test score were the most likely to have been completed.
It was also discovered that a patient was no more likely to have these assessments
completed whether they had had a FRA or not.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Lying andstanding BP
Eye Test Mental TestScore
Medications
NA
NO
NR
YES

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
28
Chart 10. Number of patients having any documented mobility assessments
N = 518
Comment
This chart shows the numbers of patients having Physiotherapy or Occupational
Therapy assessments completed. Patients were more likely to have a mobility and/or
transfer assessment done than other assessments such as Lying/Standing BP and
Medication reviews. It is worth noting that the high level of assessments reflects that
these are routine assessments done by PAMs, whereas other assessments are more
specific to a patient’s particular needs.
0
50
100
150
200
250
300
350
400
Bartell
Mobilit
y
T ransfe
rsGait
T innetti
EMS
GU&G
180 tu
rn
Func Reac
hDG
I
Berg B
Stairs

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
29
Table 7. Is there any evidence in the notes that any of the following
interventions/prevention measures have been started?
N = 518
Intervention % YesPhysiotherapist 72%OT 42%Call Bell at hand 34%Close Observation 25%Bed rails 23%Asking for help 17%Alarms 13%Educate 12%Frequent toileting 12%Discussed with relatives 11%Bed left in low position 10%Home visit 8%Dementia assessment 7%Chair 7%Intermediate Care 6%Trial without catheter 4%Special if frequent faller 4%Coloured wristband 3%Footwear Assessment 3%Hip Protectors 1%Balance Class 1%Falls Clinic 0%
Standard: The standard ideal was that in all patients’ records there was
documented evidence of including or excluding interventions
A list of intervention or prevention measures was devised (please see methodology
section for list and sources) using other lists that other groups had compiled such as
the action list from Stockport, and used on the proforma. Data collectors looked to see
whether or not these had been documented in a patient’s notes. It is important to note
that not all hospitals have the same intervention measures, for example very few
hospitals use coloured wristbands to identify patients at risk and some do not have
falls clinics.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
30
Comment
The most likely interventions were the patient was referred to a physiotherapist and/or
an OT, the patient was under close observation, and a call bell was at hand.
Some of these interventions may have been carried out but not recorded in the notes
which could explain the low percentages.
Unfortunately it is impossible to deduce from the data which patients should have had
certain interventions. Each hospital uses different care plans or action plans so what
one hospital deems as an appropriate action for a patient at risk another may not.
Chart 11. Intervention measures/FRA completed
N = 518Comments
Chart 11 compares those patients who had a FRA completed (regardless of hospital
group) with those that didn’t. It was noteworthy that a higher percentage of patients
who had a FRA completed had certain interventions (e.g. Close Observation, Bed
Rails, Asking for help, Alarms on bed/chair). The difference in use of these specific
interventions is statistically significant.
0%
5%
10%
15%
20%
25%
30%
35%
Close o
bs
Bed ra
ils
Asking
for h
elp
Alarms
Educa
te
Discus
sed w
ith re
lative
s
Bed in
low po
sition
Wris
tband
Specia
l
Footw
ear
Hip Pro
tector
s
Toileti
ng
Chair h
eight
Balanc
e clas
s
Falls c
linic
FRA completed (all hosp) %No FRA %

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
31
Chi-Squared tests
Close observation = P = 0.04
Bed Rails = P = 0.01
Asking for help = P = 0.01
Alarms = P = <0.01
Educate = P = 0.01
Wristband = P = <0.01
Therefore if a patient has a FRA completed they are more likely to have these certain
prevention measures.
� A patient who had a FRA completed had an average of 4 Interventions whereas
a patient who didn’t had an average of 3 interventions.
� Patients who fell in hospital had an average of 5 interventions and those that
didn’t had an average of 3 interventions.
� Also those at risk of falling had an average of 4 interventions whereas those
that weren’t at risk had an average of 3.
� The average number of interventions for the whole population was 3.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
32
8.4 Patients At Risk of Falling
Chart 12. Proportion of patients considered at risk of falling by trust
N = 518Comment
This shows the proportion of patients assessed as ‘at risk’ either by falls risk
assessment or otherwise noted in the patients’ documentation.
There is a non-standard approach to classifying patients at risk. Some falls risk
assessment forms classify patients in one of 3 categories either low, medium or high
risk. Others simply classify patients either at risk of falling or low risk/no risk.
For the purpose of this analysis At Risk included patients assessed as medium or high
risk, patients assessed as being ‘at risk’ of falling and those for whom it was noted
elsewhere in the notes (not as part of a formal risk assessment form) that they were at
risk.
There may be some variation between hospitals, as to how a patient comes to be
assessed as being at risk of falling, due to the different forms, some take into account
more or different factors than others
0%
10%
20%
30%
40%
50%
60%
70%
80%B
ury
MR
I
NM
GH
Old
ham
Ro
chd
ale
Sto
ckp
ort
Tam
esid
e
Tra
ffo
rd
Wir
ral
Wyt
hen
shaw
e
% at Risk

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
33
Certain hospitals had more patients classified as at risk than others - this coincides
with the proportion of patients who were actually assessed. See chart 13 below which
combines the data from charts 12 and 3 and highlights the risk status of those patients
who were assessed (assessment includes both the formal method and informal).
Chart 13. Proportion of population assessed, by risk status by hospital
N = 518
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Bury
MRI
North
Manch
ester
Oldham
Rochd
ale
Stockp
ort
Tames
ide
Traffo
rdW
irral
Wyth
ensh
awe All
% Not at Risk% At Risk

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
34
Chart 14. Patients At Risk/Risk Factors
N = 518Comment
This chart shows the number of risk factors per patient for those diagnosed as being at
risk of falling, compared with those who had no diagnosis or were deemed not to be at
risk. The question needs to be asked why were some patients not diagnosed at risk
yet they had high numbers of risk factors?
There are differences in the way each hospital is identifying patients at risk of falling
due in part to the use of different FRA forms. However there are also differences
between those hospitals that are using a variation of the same form. The explanation
may lie in differences in the number of risk factors assessed. This varies on each form.
Nonetheless all assess History of falls, sensory deficits and mobility. Other risk factors
assessed include age, sex, medication, mental state, toileting requirements, medical
history etc. The patients are then categorised depending on the score. Some falls risk
assessment forms classify patients in one of 3 categories either low, medium or high
risk. Others simply classify patients either at risk of falling or low risk/no risk.
The audit proforma looked for a more comprehensive list of risk factors (11 in total)
than the falls risk assessment forms at each trust. The project group identified the list
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6 7+
No of R isk Factors
Not diagnosed
At Risk

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
35
of risk factors from various sources including the FRAs. Therefore it is possible that
the proforma would have picked up a number of other risk factors mentioned in the
casenotes that the FRA did not prompt the person assessing the patient to pick up.
Therefore a patient might have had 7+ risk factors according to the audit proforma, but
not all were picked up on the FRA and the patient might not been classified ‘at risk’.
Table 8 shows which risk factors from the audit were actually on the local risk
assessment forms:
Table 8. Risk Factors assessed by each hospital
Risk Factor Bury Oldham Rochdale Stockport Tameside Trafford Wythen
shawe Wirral
Falls 4 4 4 4 4 4 4 4
Meds 4 X X 4 4 4 X XIncontinence X 4 X 4 4 4 4 4
Mental state 4 4 4 4 4 4 4 4
Mobility 4 4 4 4 4 4 4 4
Vision 4 4 4 4 4 4 4 4
Hearing 4 X 4 4 4 X X XAlcohol 4 X X X X X X XPosturalHypotension X X X X X X X X
Medicalcondition X X X 4 4 X X X
Seizures X X X 4 4 X X X
Chart 15. Patients’ risk status by number of risk factors
N = 205
832
45
4513
923
24
6
0
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 1 2 3 4
Not at Risk
At Risk

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
36
Chart 15 includes only those patients who had a formal falls risk assessment. It
incorporates the four risk factors included by all the hospitals on their falls risk
assessment forms. There is an increasing proportion of patients assessed as at risk
with an increasing number of risk factors the patient was noted to have. It is gratifying
that 100% of those patients with all four risk factors were deemed to be at risk of
falling. However almost 50% of those with ‘no risk factors’ in this analysis were also
deemed as at risk. These patients only numbered 8, of these 8 6 had 2 other risk
factors, 1 patient had 1 other risk factor and 1 patient had 0 risk factors whatsoever.
(The risk assessment form for this patient with no risk factors had not been completed
fully and only stated that the patient was at risk without reasoning why). This
observation reflects the inclusion of other risk factor assessments in some trusts.
There is a need to develop a standardised approach to this part of the assessment
process.
Two examples of Risk Assessment Forms are given here:
Example of a Falls Risk Assessment tool
Taken from Falls Risk Assessment, The Pennine Acute Hospitals NHS Trust (Rochdale)
IF NO * SCORED, ASSESS AS LEVEL 1IF ONE OR MORE * SCORED, ASSESS AS LEVEL 2
HISTORY OF RECENT FALLS*YES NO
COGNITIVE STATEALERT* CONFUSED* UNABLE TO IDENTIFY DANGERS
SENSORY DEFICITSNONE* VISUAL IMPAIRMENTS (NOT CORRECTED BY GLASSES)* HEARING IMPAIRMENTS (NOT CORRECTED BY HEARING AID)* LIMBS; AMPUTATION
NEUROPATHY
GAITSTABLE AND SAFE* STABLE WITH WALKING AIDS* UNSTABLE OR UNSAFE WITH WALKING AIDS* UNABLE TO WALK SAFELY
ASSESSED AS LEVEL …

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
37
Example of a Falls Risk Assessment tool
Falls Risk AssessmentTO BE COMPLETED ON ADMISSION TO WARD FOR ALL PATIENTS
(Refer to full guidelines)
Score on admission ………….
Date/time Score Action Initial Review Time
Sex Sensory Deficit AgeFemale 2 2 2 Sight 1 1 1 <60 0 0 0Male 1 1 1 Hearing 1 1 1 60-70 1 1 1
Balance 2 2 2 71-80 2 2 281+ 3 3 3
Fall History Mobility Medical History
None 0 0 0 Full 1 1 1 Alcohol/unconscious 3 3 3At home 2 2 2 Uses aid 2 2 2 Overdose 2 2 2In ward 1 1 1 Restricted 3 3 3 Assault/head injury 1 1 1Both/frequentfalls 3 3 3 Bed bound 1 1 1 Organic brain
disease/confusion 1 1 1
Purgative 1 1 1 Incontinence/frequency 1 1 1laxatives Seizures 1 1 1
Diabetes 1 1 1Gait Medication
Steady 0 0 0 Hypnotic 1 1 1 3-8………….... LOW RISKHesitant 1 1 1 Tranquillisers 1 1 1 9-12………….. MEDIUM RISKPoor transfer 3 3 3 Hypotensives 1 1 1 13+……….….. HIGH RISKUnsteady 3 3 3 Diuretics 1 1 1
Taken from Falls Risk Assessment, Stockport NHS Foundation Trust

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
38
8.5 Falls in hospital
Chart 16. Has the patient fallen whilst in hospital?
N = 518
Comment
This shows the percentage of patients who fell during the hospital episodes under
scrutiny.
Stockport and Wythenshawe had no falls at all. This observation may be genuine or
the result of under-recording of falls in the notes.
In Oldham 15% of the sample fell, and just slightly less so in Bury and Rochdale.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
BuryM
RI
NMGH
Oldham
Rochdale
Stockport
Tamesid
e
Traffo
rd
Wirr
al
Wyth
enshawe All
Yes
No

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
39
Chart 17. Did the patient fall in hospital?
Comparing trusts that use a FRA and those that don’t.
N = 518
P=0.051 (chi-squared test)
Comment
This graphs looks at the two hospital groups and the incidence of falls.
Interestingly only 14 patients fell out of the group using FRAs whereas 26 fell in the
other group. A chi-squared test just failed to reach statistical significance.
See chart 18 on the following page.
234244
14 26
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
FRA No FRA
Yes
No
GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
40
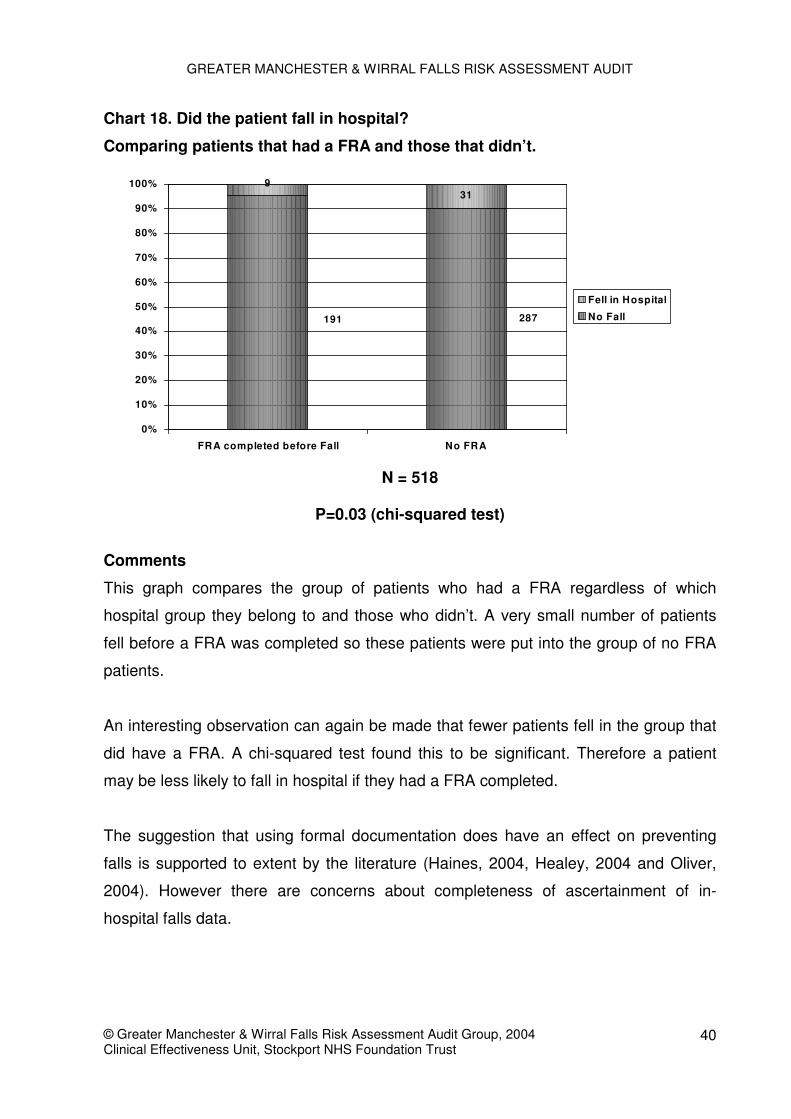
Chart 18. Did the patient fall in hospital?
Comparing patients that had a FRA and those that didn’t.
N = 518
P=0.03 (chi-squared test)
Comments
This graph compares the group of patients who had a FRA regardless of which
hospital group they belong to and those who didn’t. A very small number of patients
fell before a FRA was completed so these patients were put into the group of no FRA
patients.
An interesting observation can again be made that fewer patients fell in the group that
did have a FRA. A chi-squared test found this to be significant. Therefore a patient
may be less likely to fall in hospital if they had a FRA completed.
The suggestion that using formal documentation does have an effect on preventing
falls is supported to extent by the literature (Haines, 2004, Healey, 2004 and Oliver,
2004). However there are concerns about completeness of ascertainment of in-
hospital falls data.
931
287191
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
FRA completed before Fall No FRA
Fell in Hospital
No Fall

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
41
9. SUMMARY/CONCLUSIONS
9.1 Key Results
• Patients in the sample were predominantly the very elderly, those aged 80 years or
more comprised almost 58% of the sample. This proportion varied by Trust from,
45% in MRI to 73% at the Wirral.
• The mean percentage of patients admitted with a fall is just over 30%. 6 hospitals
fell below this average, 3 were just above the average, and 1 hospital had nearly
20% more patients admitted with a fall than the average.
• Between 85 - 95% of patients in 4 of the hospitals were assessed. The other 6
hospitals all fell below the mean, which was just below 53%.
• Overall 34% of patients who had a risk assessment were reviewed.
• The proforma was used to assess how well the FRA was used and this included
the question was any action taken to prevent falls. 61% did take some type of
preventative action, but 37% didn’t.
• Patients were more likely to have mobility and/or transfer assessments done than
other assessments such as Lying & Standing BP and Medication reviews.
• The most likely interventions were the patient was referred to a physiotherapist
and/or an OT, the patient was under close observation, and a call bell was at hand.
• With regards to interventions, Chi-squared tests were done on a number of the
results and found them to be significant. Therefore if a patient has a FRA
completed they are more likely to have these certain prevention measures.
• An interesting observation can be made that fewer patients fell in the group of
patients that did have a FRA. A chi-squared test found this to be significant.
Therefore a patient may be less likely to fall in hospital if they had a FRA
completed.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
42
9.2 Aims and Objectives
The project aimed to audit current Falls Management and Prevention in a group of
Hospitals across Greater Manchester in support of the National Service Framework for
the Elderly. The audit has been successfully completed and therefore the aim has
been met.
Another objective was to establish a baseline of current services within each hospital
setting. The results of this can be found in appendix 3.
9.3 Criteria and Standards
� A falls risk assessment tool is in use on the wards in each hospital.
8 out of 10 hospitals had a falls risk assessment form in use, however in some of the
hospitals it was only in a pilot stage or not in full use. 5 out of these 8 hospitals had a
tool in full use.
� An environmental audit tool and action plan is in place
The audit was unable to address this standard on this occasion.
� All patients are assessed and a completed form is in each patient’s set of notes.
Each form is fully completed.
53% of the whole population were assessed, 40% of the whole population were
assessed using a formal risk assessment form. 90% of all assessment forms were fully
completed.
� In appropriate cases patients will have been re-assessed after one week, and their
care plan reviewed.
Of the 5 hospitals where a risk assessment form was in full use 34% of those patients
who had a risk assessment completed were reassessed. Please note that due to the
data collected it has not been possible to distinguish how long it took before the patient
was reassessed.
GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
43
� All patients who are classified at high risk have an appropriate care plan and
preventive steps outlined and acted upon.
As each hospital uses a different assessment form some do not classify their patients
by risk categories such as Low/Medium/High and simply categorise them as ‘At risk’ or
‘Not at risk’. Also each hospital uses different care plans or action plans so what one
hospital deems as an appropriate action for a patient at High Risk another hospital
may not. Not all hospitals have the same intervention measures; for example very few
hospitals use coloured wristbands to identify patients at risk and some do not have
falls clinics. Therefore it has not been possible to assess this criteria using the data
collected. Analysis of the data has shown that for those patients who had a falls risk
assessment form completed they are more likely to have certain interventions than
those patients who did not. Please see chart 11 for more information.
� The standard ideal for both of these factors was that in all patients’ records there
was documented evidence of checking for the risk factors and including or
excluding interventions.
Please see chart 8 which shows the distribution of patients according to the number of
risk factors recorded, and table 7 which shows what percentage of the population had
an intervention.
� All ward staff have been formally trained on how to use the tool
Appendix 3 shows that 3 hospitals have an educational programme to train staff how
to identify those at risk of falling and how to prevent falls. One hospital’s education
programme is only in a developmental stage. Interestingly 4 of the 8 hospitals using a
tool had no educational programme for staff.
� The use of Health promotion material
� The issue of patient information concerning for example Falls prevention: Your
safety checklist and guide
6 out of the 10 hospitals had some sort of information regarding falls available for
patients.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
44
� An operational falls service has been set up in each local health economy with
appropriate complement of staff.
In light of the information provided it would appear that each hospital has some form of
falls service. 4 out of 10 had a falls co-ordinator. 5 out of 10 have falls clinics, but 2 of
these were still in a pilot stage and 2 began in October 2004 (after the audit took
place). 2 hospitals have neither a clinic nor a co-ordinator. 1 hospital had a falls co-
ordinator at the time of the audit but, at the time of this report, the post was vacant.
� The fall service has access to dieticians, optometrists, orthotists, ophthalmologists,
audiologists, access to bi-linguists, access to bone densomitry. Older people who
fall should, with their consent, be referred to a specialist falls service.
Most of the hospitals have a multi-disciplinary team working towards preventing falls
as part of the falls service provided at the hospital. The staff involved are
predominately nurses, physiotherapists, occupational therapists and clinicians,
although some hospitals had podiatrists, dieticians, pharmacists and Age Concern
involved in the service.
Information regarding hospitals falls services can be found in Appendix 3.
� The provision of Falls clinics, patient sitter programmes and response systems
5 out of 10 hospitals now have falls clinics, but 2 of these were still in a pilot stage and
2 began in October 2004 (after the audit took place). The audit was unable to assess
the implementation of patient sitter programmes and response systems, however
neither of these were recorded on the forms as part of the hospitals’ service so it could
be presumed that they aren’t used by the hospitals.
9.4 In summary
� Using a FRA may have a protective effect
� The patients are more likely to have prevention measures targeted at them if a
FRA has been completed
� In-patient falls appear less likely in hospitals using a FRA

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
45
� Patients with a high number of risk factors are not necessarily being documented
as being at risk of falling
9.5 Questions to be asked
� What other pertinent features should we be addressing with the data?
� Is the evidence strong enough to suggest we should implement risk assessment
forms or is there more that we could do to justify implementation?
� What recommendations & actions can be made?
� Can falls prevention be standardised across Greater Manchester? Including Falls
Risk Assessment and Action Plans.
� Should we do another falls risk assessment audit?
� What other pertinent measurable factors should be collected in future audits?
9.6 Future Plans
As a result of the feedback seminar a Falls Working Group will be set up to look at
multidisciplinary core skills in relation to an inpatient falls action plan and to look at
standardising falls risk assessment and intervention across Greater Manchester. A
variety of staff from the meeting volunteered to be part of the group and the first
meeting will be held in early 2005.
A Fracture Neck of Femur re-audit is planned for 2005 with 4 other trusts joining the 7
trusts from the original audit.
The Falls Risk Assessment Audit could be re-visited in 2006 to see if changes have
been successfully implemented.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
46
10. REFERENCES
American Geriatrics Society, British Geriatrics Society, and American Academy of
Orthopaedic Surgeons Panel on Falls Prevention. Guideline for the Prevention of Falls
in Older Persons. AGS Panel on Falls Prevention. Vol 49, No. 5. 2001.
Cannard G. Fall risk assessment scale for the elderly F.R.A.S.E. Nursing Development
Unit, General Hospital, Tullamore, 1996.
Department of Health. National Service Framework for Older People, 2001.
Doughty, K. Fall Prevention and Management Strategies Based on Intelligent
Detection, Monitoring and Assessment. Technology in Healthcare. 2000.
Dyer, C. A. Risk-factor assessment for falls: from a written checklist to the penless
clinic. Age and Ageing. 27(5), 569-72. 1998.
Haines, T et al. Effectiveness of targeted falls prevention programme in subacute
hospital setting: randomised controlled trial. BMJ, 328, 676. 2004.
Healey, F et al. Using targeted risk factor reduction to prevent falls in older in-patients:
a randomised controlled trial. Age and Ageing, 33, 390. 2004.
Huda, A and Wise, L.C. Evolution of compliance within a fall prevention program.
Journal of Nursing Care Quality. 12(3): 55-63, 1998.
Joanna Briggs Institute for Evidence Based Nursing and Midwifery. Falls in Hospital.
Best Practice. Evidence Based Practice Information Sheets for Health Professionals.
Adelaide: JBIEBNM, 1998.
Kinn, S. and Kood, K. A falls risk-assessment tool in an elderly care environment.
Myers, H. Hospital falls risk assessment tools: A critique of the literature. International
Journal of Nursing Practice. 9, 223. 2003.
Oliver, D. Risk factors and risk assessment tools for falls in hospital in-patients: a
systematic review. Age and Ageing, 33, 122. 2004.
Scottish Intercollegiate Guidelines Network. Prevention and Management of Hip
Fracture in Older People, 2002.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
47
The Royal College of Physicians of London. Fractured Neck of Femur Prevention and
Management, 1989.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
48
11. CONTACT DETAILS
If you have any comments/feedback or you require any further information please seecontact details below.
Ms Joanna RodgersAudit Co-ordinatorClinical Audit Department6th Floor, MaternityStepping Hill HospitalStockportSK2 7JE
Tel. No. 0161 419 4692Email: [email protected]
Dr Gary CookConsultant Epidemiologist/R&D LeadThe WillowsStepping Hill HospitalStockportSK2 7JE
Tel. No. 0161 419 5984Email: [email protected]

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
49
12. ACKNOWLEDGEMENTS
The following staff collected data at their respective hospitals:
South ManchesterJulia Gray
PennineSue Baxter (O, R)Margaret Carney (N)Emma Clarke (F)Julie Fraser (F)Reehana Khan (F)Mark Lammas (N, F)Trish Mitchell (O, R, N, F)Janet Powell (O)Aviva Richards (N)Michael Sullivan (R)
(Key: O = The Royal Oldham Hospital, R = Rochdale Infirmary, N = North ManchesterGeneral Hospital, F = Fairfield General Hospital
TamesideJanice BehrSheetal Sureen
WirralBev HawkesJane MarriottJacquie Ruddick
StockportDr Marie Hanley
TraffordGill CritchleyMaggie HughesGaynor Wakefield
Thank you to all of the above for all the hard work they put into the data collection.
Thank you to:
Sylvia Cooper, P&G Pharmaceuticals UK Ltd for sponsoring the Feedback Seminar
Dr David Bourne and Julia Gray for presenting at the Feedback Seminar

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
50
Appendix 1: List of Charts and Tables
Title PageTable 1 Data collection dates at each hospital 17Table 2 Number of wards at each hospital by specialty 17Table 3 General Demographics 19Chart 1 Age group by hospital 19Chart 2 Proportion of Patients admitted due to a fall 20
Chart 3 Proportion of Patients assessed and documented 21Table 4 Percentages Assessed 21Chart 4 If a form was filled in was it fully completed? 22
Chart 5 If FRA was completed was the patient reviewed during theiradmission 23
Table 5 Percentages reviewed by Length of Stay 24Chart 6 Was the patient reviewed? By Length of stay 24
Chart 7 The proportion of patients with completed FRA for whom actionwas taken and documented 25
Table 6 Number of risk factors by action recommended 25Chart 8 Number of risk factors for whole population 26Chart 9 Have any of the following Key Risk Factors been assessed? 27
Chart 10 Number of patients having any documented mobilityassessments 28
Table 7 Is there any evidence in the notes that any of the followinginterventions/prevention measures have been started? 29
Chart 11 Intervention measures/FRA completed 30Chart 12 Proportion of patients considered at risk of falling by trust 32Chart 13 Proportion of patients assessed according to risk status by trust 33Chart 14 Patients at Risk/Risk Factors 34Table 8 Risk Factors assessed by each hospital 35Chart 15 Patients’ risk status by number of risk factors 35
Example of a Falls Risk Assessment tool 36Example of a Falls Risk Assessment tool 37
Chart 16 Has the patient fallen whilst in hospital? 38
Chart 17 Did the patient fall in hospital? Comparing trusts that use a FRAand those that don’t. 39
Chart 18 Did the patient fall in hospital? Comparing patients that had aFRA and those that didn’t. 40

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
51
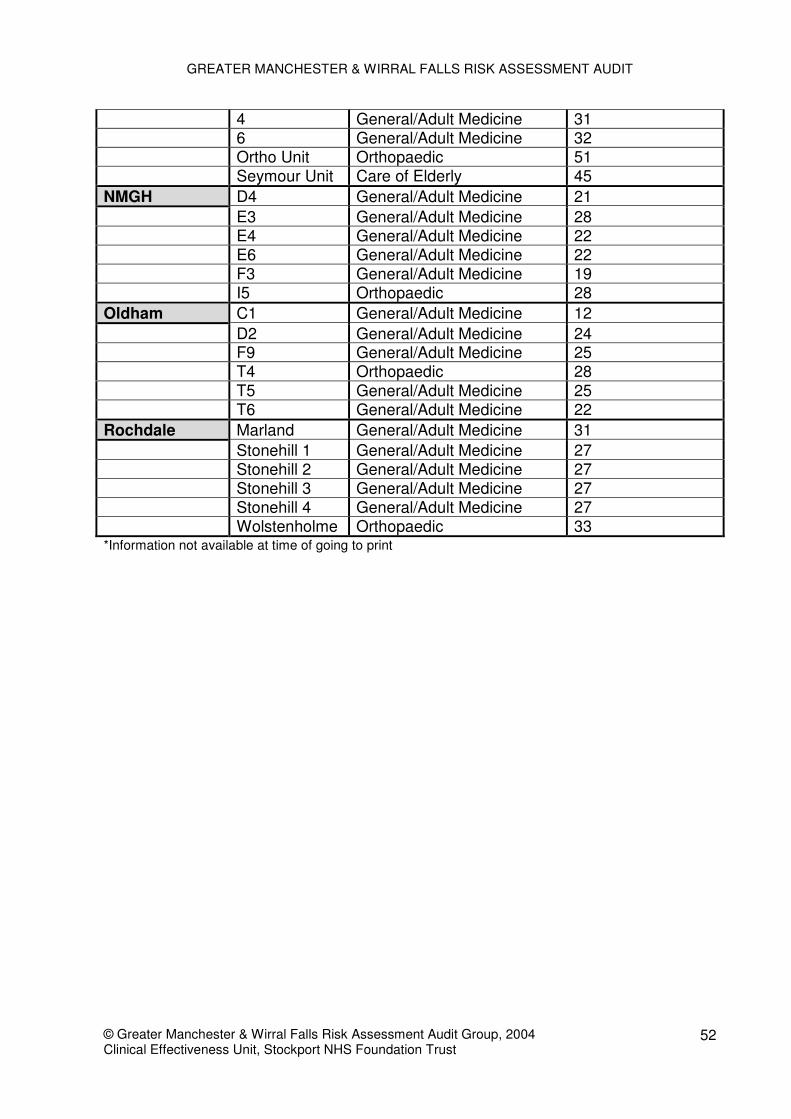
Appendix 2: Ward types and number of beds
Hospital Ward Ward Type Number of bedsWythenshawe A5 Orthopaedic 28
A7 General/Adult Medicine 28A8 General/Adult Medicine 28A9 General/Adult Medicine 28A10 General/Adult Medicine 28F11 General/Adult Medicine 32
Tameside 2 Orthopaedic 284 Orthopaedic 2840 General/Adult Medicine 3041 General/Adult Medicine 3042 General/Adult Medicine 3044 General/Adult Medicine 2446 General/Adult Medicine 24
Stockport A12 General/Adult Medicine 28A14 General/Adult Medicine 28A15 General/Adult Medicine 28D1 Orthopaedic 25D2 Orthopaedic 25E2 Care of Elderly 38E3 Care of Elderly 38
Wirral 20 Care of Elderly 3021 Care of Elderly 3022 Care of Elderly 3023 Care of Elderly 3024 Care of Elderly 2425 Orthopaedic 37
Bury 6 General/Adult Medicine 288 Orthopaedic 229 Orthopaedic 2818 General/Adult Medicine 3019 General/Adult Medicine 3229 General/Adult Medicine 2330 General/Adult Medicine 27
MRI 1 Orthopaedic *15 General/Adult Medicine *AM1 General/Adult Medicine *AM2 General/Adult Medicine *AM3 General/Adult Medicine *AM4 General/Adult Medicine *
Trafford 1 Care of Elderly 282 General/Adult Medicine 29
GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
52
4 General/Adult Medicine 316 General/Adult Medicine 32Ortho Unit Orthopaedic 51Seymour Unit Care of Elderly 45
NMGH D4 General/Adult Medicine 21E3 General/Adult Medicine 28E4 General/Adult Medicine 22E6 General/Adult Medicine 22F3 General/Adult Medicine 19I5 Orthopaedic 28
Oldham C1 General/Adult Medicine 12D2 General/Adult Medicine 24F9 General/Adult Medicine 25T4 Orthopaedic 28T5 General/Adult Medicine 25T6 General/Adult Medicine 22
Rochdale Marland General/Adult Medicine 31Stonehill 1 General/Adult Medicine 27Stonehill 2 General/Adult Medicine 27Stonehill 3 General/Adult Medicine 27Stonehill 4 General/Adult Medicine 27Wolstenholme Orthopaedic 33
*Information not available at time of going to print

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
53
Appendix 3: Hospital Falls Services
Hospital FRAin use Type Used on all
wardsPlan to
useCareplan
Info forpatients
Falls Co-ordinator
FallsClinic
Educationfor staff
No of falls2003/04
(aged 65+)
Medicalin-
patients65+
Ortho in-patients65+ (notelective)
MRI No NA NA ^ ^ ^ Yes # ^ ^ 1088 ^ ^
Bury Yes NK Noonly elderly Yes Yes Yes Yes † No NR 6770 897
NMGH No NA NA Yes No Yes No No NR 11715 1033
Oldham Yes STRATIFYNo(not
orthopaedic)- Yes Yes Yes
YesPilotstage
Yes 826 8665 1035
Rochdale Yes NK Yes NA Yes No Yes(Sept 04) - No 374 9447 1011
Stockport Yes FRASE Yes NA Yes Yes* No
YesOct 04
pilotstage
Yes 1393** 8316 1100
Tameside Yes Cannard NoPilot stage Yes Yes - No Yes
Oct 04
Develop-mentalstage
1161 4558 1039
Trafford Yes STRATIFYNo
Only Elderlyand Medical
- No No No Yes No 1308 3325 4512
SMUHT Yes STRATIFY
NoOnly Elderly,
Medical &Rehab
Yes Yes Yes Yes Yes Yes 852 5094 443
Wirral Yes STRATIFY Yes NA Yes Yes No - No 1939 14763 1219
^Information not available at time of going to print# Falls Co-ordinator in post at the time of the audit, position currently vacant† PCT based co-ordinator, doesn’t cover in-patients*Only in Day hospital and out-patients, not on wards**Cannot distinguish by age so number is all falls reported regardless of age

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
54
Hospital Falls Services (cont.)
Central Manchester & Manchester Children’s University Hospitals NHS TrustInformation not available at the time of going to print
Pennine Acute Hospitals NHS TrustFairfield General Hospital• The hospital has a falls co-ordinator, but they are employed by the PCT. The falls
co-ordinator is based in the hospital and in the community, she receives referralsfrom A&E, GPs, District Nurses and Health Visitors, but they do not cover in-patients.
North Manchester General HospitalNo other information
The Royal Oldham Hospital• The hospital has a falls co-ordinator. This is mainly a community role with a wide
remit to reduce falls incidence in Oldham• Hospital falls service – has input from Physiotherapists and Occupational
Therapists in A&E. There are falls exercises and education sessions for outpatients. There is a pilot falls clinic with the falls co-ordinator (physio) and aSpecialist Registrar.
• There is an educational programme for staff at the trust regarding falls riskassessment. This is offered on a regular basis, it is a half day including prevalence,risk factors, interventions, use of STRATIFY, use of falls action prompt,osteoporosis and fractures.
Rochdale Infirmary• The hospital has a falls co-ordinator who was newly appointed in September 2004
(after the audit). Their role is to develop and co-ordinate a falls care pathway, toprovide specialist advice and teaching and to develop an integrated falls serviceand community falls clinic.
• Hospital falls service – there is a pathway for fallers admitted to A&E. Patients arereferred to the intermediate care team for assessment. When patients are admittedto the ward a falls risk assessment form is completed by nursingstaff/physiotherapists. Patients are discharged home for follow-up by communityfalls service.
• The Falls Service involves Physiotherapists, Nurses and Occupational Therapists.
Stockport NHS Foundation Trust• The hospital is currently piloting a Falls Clinic from October 2004 to December
2004. The aim is to continue the clinic after the pilot. The clinic is divided into 2sessions, patients initially attend Tuesday pm for medical and nursing, then returnfollowing Tuesday am for physio and OT, this is followed by a MDT meeting. Thereis a business case for therapy input and falls co-ordinator.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
55
• The Falls Service involves Clinicians, Physiotherapists, Nurses, OccupationalTherapists, links for pharmacy advice and Accident Prevention officer from AgeConcern. It is hoped that there will be podiatry input in January 2005
• There is an educational programme for staff at the trust regarding falls riskassessment. This is given at the mandatory training sessions which all staff attendonce a year.
Tameside & Glossop Acute Services NHS Trust• Use a Falls Risk Assessment tool based on Cannard which is currently being
piloted on one ward in each specialty before it is introduced across all wards ineach hospital.
• Hospital falls service – a clinician led falls clinic will be commencing in October2004. There is also a falls group
• The Falls Service involves Physiotherapists, Nurses, Doctors (from Oct 04) andOccupational Therapists.
• There is no educational programme for staff at the trust regarding falls riskassessment; this is in a developmental stage at the moment.
Trafford Healthcare NHS Trust• Hospital falls service – 1 session a week in the Altrincham rehab unit where there
is podiatry, physiotherapist, occupational therapist, doctor, nurse and pharmacist.Follow up sessions run over 7 weeks for patients who will benefit from the exercisegroup, this involves OTs and Physios + Care and Repair, Age Concern andDietician.
South Manchester University Hospitals NHS Trust• The hospital has a falls co-ordinator whose role is to triage all falls clinic referrals,
organise waiting list and help to draw together integrated pathways for fallers. Theyalso have to map current situation for the trust, help areas where fallers passthrough evaluate their service in line with the NSF and adjust accordingly, providelinks with the PCT, develop pathway, update standards and protocols, audit inpatient fallers and develop links with other trusts.
• Hospital falls service – there is a MDT falls clinic, a falls consultant, links in A&E,falls medication group. Departmental falls groups.
• The Falls Service involves Consultant Geriatrician, Lead Nurse, Physiotherapists,Senior Podiatrist and Occupational Therapists and Dieticians as required.
• There is an educational programme for staff at the trust regarding falls riskassessment. There are quarterly sessions as part of the NSF lasting half a day,falls take up about 1/5 of the programme. Routine education for physios. Ad hoceducation.
Wirral Hospital NHS Trust• Hospital falls service is led by Physiotherapists. The Community Assessment and
Rehabilitation Team (CART) are also involved. Exercise classes are held atVictoria Central Hospital.
• The Falls Service involves Physiotherapists, Nurses and Occupational Therapists.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
56
Appendix 4. Feedback Seminar Attendees
Name Job Title OrganisationElsie Lynch Head of Physiotherapy Birkenhead and Wallasey PCTHelen Home Therapy Rehab Co-ordinator Birkenhead and Wallasey PCTDebbie Monaghan Supt II Physiotherapist Bolton Hospitals NHS TrustChristine Atkinson Clinical Governance Manager Bolton Primary Care TrustPaul Campbell Audit Co-ordinator Bury PCTDr David Bourne Consultant Physician Central ManchesterJoanne Makin Physiotherapist Central ManchesterNicola Brown Senior Physiotherapist Central ManchesterPam Leah Occupational Therapist Central ManchesterRomaine Short Physiotherapist Central ManchesterDr Sethi Consultant Physician Pennine Acute Hospitals NHS TrustJanet Powell Falls Prevention Officer Pennine Acute Hospitals NHS TrustMargaret Carney Senior Physiotherapist Pennine Acute Hospitals NHS TrustPatricia Mitchell Clinical Audit Facilitator Pennine Acute Hospitals NHS TrustShirley Naylor Clinical Audit Co-ordinator Pennine Acute Hospitals NHS TrustSue Plevey OT Manager Pennine Acute Hospitals NHS Trust
Dr Keith Harkins Consultant Geriatrician South Manchester University HospitalsNHS Trust
Janet Brennan Nurse Manager South Manchester University HospitalsNHS Trust
Jenny Rawcliffe Modern Matron South Manchester University HospitalsNHS Trust
Julia Gray Falls Co-ordinator South Manchester University HospitalsNHS Trust
Mrs Susan O'Flynn Senior I Physiotherapist South Manchester University HospitalsNHS Trust
Dr Gary Cook Consultant Epidemiologist Stockport NHS Foundation TrustDr M Hanley Consultant in Elderly Medicine Stockport NHS Foundation TrustJanine Lewis Senior Occupational Therapist Stockport NHS Foundation TrustLinda Woolley Ward Sister Stockport NHS Foundation TrustDr Marie McDevitt Public Health Specialist Stockport PCTSue Gunnion Case Management Lead Stockport PCTSarah Hince Stockport PCTDr Luciano Garcia-Allen Consultant Physician Tameside & Glossop Acute Services
NHS Trust
Heather Leyland Clinical Audit Officer Tameside & Glossop Acute ServicesNHS Trust
Jan Barnes Team Leader Orthopaedics Tameside & Glossop Acute ServicesNHS Trust
Maggie Tate Clinical Governance Info Manager Tameside & Glossop Acute ServicesNHS Trust
Deborah Maloney Trafford Healthcare NHS Trust

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
57
GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDITPROFORMA
Proforma completed by (name and designation): ………………………………………………
Date proforma completed: _ _ / _ _ / _ _ _ _
A. Patient Details: (please fill in details below)Hospital
Ward Name Specialty
Date of Birth _ _ / _ _ / _ _ _ _ Gender M F
B. Episode DetailsDate of Admission _ _ / _ _ / _ _ _ _Reason for Admission (presenting complaint / diagnosis)
Was the admission due to a fall? Yes NoPreadmission Walking Ability (e.g. walked unaided,one aid, two, frame, wheelchair etc):
C. Please complete this section if your trust uses a Risk Assessment Tool (Go tosection D if your trust doesn’t have a risk assessment tool)(please delete / fill in as appropriate)Has the patient had a falls assessment completed for this episode? Yes No(If no, please fill in Section D)What date was the form completed on? _ _ / _ _ / _ _ _ _Has it been fully completed? Yes No Partially
What was the patient’s falls assessment score?
Was the patients assessed as being ‘at risk’? Yes NoIf appropriate, what risk category did thepatient fall into? High Medium Low
What action has been recommended?
Was any action taken? Yes No
Was a review date set? Yes No
What was the date? _ _ / _ _ / _ _ _ _
If yes, has the patient been reviewed? Yes NoNow go to section E

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
58
D. Please complete this section if you do not have a risk assessment tool in use at yourtrust.Is there written evidence in the notes that the patient has beenassessed for falls risk? Yes No
If yes:
Date of assessment/diagnosis _ _ / _ _ / _ _ _ _Has it been noted anywhere in the patient’s notes that/is there adiagnosis of “At risk of falling”? Yes No
Has any action been recommended in the notes with regards torisk of falling? Yes No
Is there documented evidence to suggest that the patient hasbeen reassessed for falls risk? Yes No
Date of review/reassessment? _ _ / _ _ / _ _ _ _
E. Are any of the following risk factors noted in the patient’s records?(Please tick box – Y=Yes, N=No, NR=No record)Risk Factor Y N NR NAHistory of fallsMultiple medications (>4 per day, including hypnotics)Urinary incontinence/frequency/assisted toiletingImpaired mental status (confusion/disorientation/depression etc)Impaired mobility/balance/gait (unsteady on feet, requires frame/stickto walkVisual ImpairmentHearing impairmentAlcohol problems (>1 unit of alcohol per day)Postural HypotensionMedical Conditions (e.g. Diabetes, Stroke, Parkinson’s)Seizures*Yes = it has been noted that the patient has the risk factor, No = it has been noted that thepatient doesn’t have this risk factor, No record = there is no record in the notes either way,NA=Not applicable
F. Have any of the following Key Indicators been carried out?(Please tick box – Y=Yes, N=No, NR=No record)
Indicator Y N NR DateLying and standing BPEye TestMental Test ScoreMedications (4+ inc. psychotropic, plan/review,any recommendations/comments)Extra Info re medications – write here
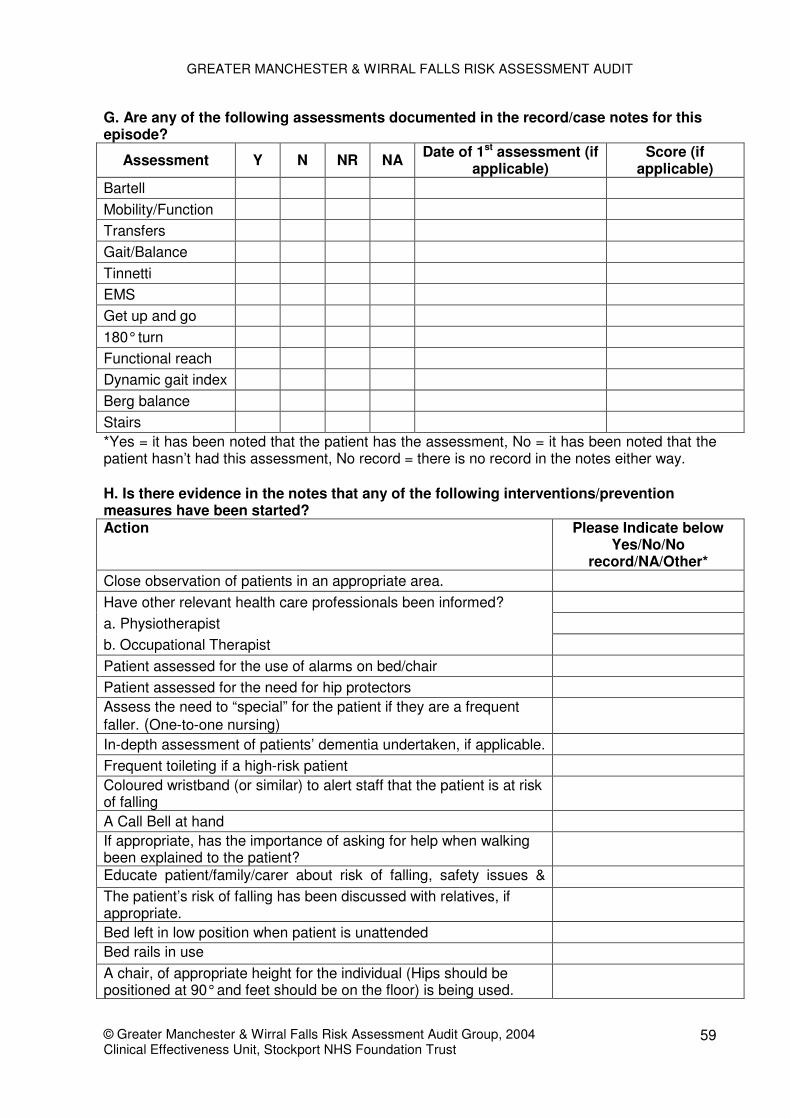
GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
59
G. Are any of the following assessments documented in the record/case notes for thisepisode?
Assessment Y N NR NA Date of 1st assessment (ifapplicable)
Score (ifapplicable)
BartellMobility/FunctionTransfersGait/BalanceTinnettiEMSGet up and go180° turnFunctional reachDynamic gait indexBerg balanceStairs*Yes = it has been noted that the patient has the assessment, No = it has been noted that thepatient hasn’t had this assessment, No record = there is no record in the notes either way.
H. Is there evidence in the notes that any of the following interventions/preventionmeasures have been started?Action Please Indicate below
Yes/No/Norecord/NA/Other*
Close observation of patients in an appropriate area.Have other relevant health care professionals been informed?a. Physiotherapistb. Occupational TherapistPatient assessed for the use of alarms on bed/chairPatient assessed for the need for hip protectorsAssess the need to “special” for the patient if they are a frequentfaller. (One-to-one nursing)In-depth assessment of patients’ dementia undertaken, if applicable.Frequent toileting if a high-risk patientColoured wristband (or similar) to alert staff that the patient is at riskof fallingA Call Bell at handIf appropriate, has the importance of asking for help when walkingbeen explained to the patient?Educate patient/family/carer about risk of falling, safety issues &The patient’s risk of falling has been discussed with relatives, ifappropriate.Bed left in low position when patient is unattendedBed rails in useA chair, of appropriate height for the individual (Hips should bepositioned at 90° and feet should be on the floor) is being used.

GREATER MANCHESTER & WIRRAL FALLS RISK ASSESSMENT AUDIT
© Greater Manchester & Wirral Falls Risk Assessment Audit Group, 2004Clinical Effectiveness Unit, Stockport NHS Foundation Trust
60
Has a home visit been arranged to assess home?Patient referred to Intermediate Care?Patient referred to Balance ClassHas the patient been referred to a falls clinic?Footwear assessment documentedHas there been a trial without catheter (if applicable)Any other actions noted not on this list (give details)
*Yes = it has been noted that the patient has had this intervention, No = it has been noted thatthe patient hasn’t had this intervention, No record = there is no record in the notes either way,NA = not applicable.
I. Other related informationHas the patient fallen whilst in hospital? Yes / No
If yes, Date patient fell: _ _ / _ _ / _ _ _ _Details of fall (where, was the incident reported, etc)
Comments (anything else mentioned in notes regarding falls)
Patient Id _ _ _/_ _ _(to be filled in by audit facilitator)