brachytherapy tg 56 59
TRANSCRIPT
SAMIR LAOUI, PH.D 08/15/2016

DEFINITION
Taken from the Greek word “brachys,” meaning
“near”, Brachytherapy (brak-e-THER-uh-pee) is
a procedure that involves placing radioactive
material inside your body
“……. there is no reason why
a tiny fragment of radium
sealed up in a glass tube
should not be inserted into
the very heart of the cancer;
thus acting directly upon the
diseased material.”
Alexander Graham Bell Letter to Science, 1903
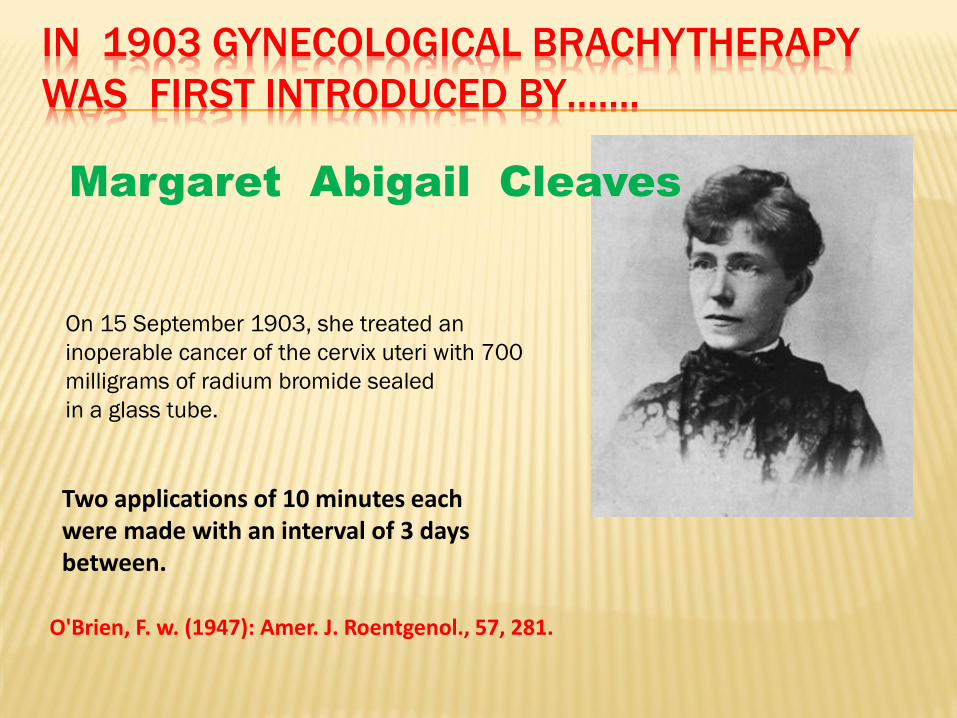
IN 1903 GYNECOLOGICAL BRACHYTHERAPY
WAS FIRST INTRODUCED BY…….
On 15 September 1903, she treated an
inoperable cancer of the cervix uteri with 700
milligrams of radium bromide sealed
in a glass tube.
Margaret Abigail Cleaves
Two applications of 10 minutes each were made with an interval of 3 days between.
O'Brien, F. w. (1947): Amer. J. Roentgenol., 57, 281.
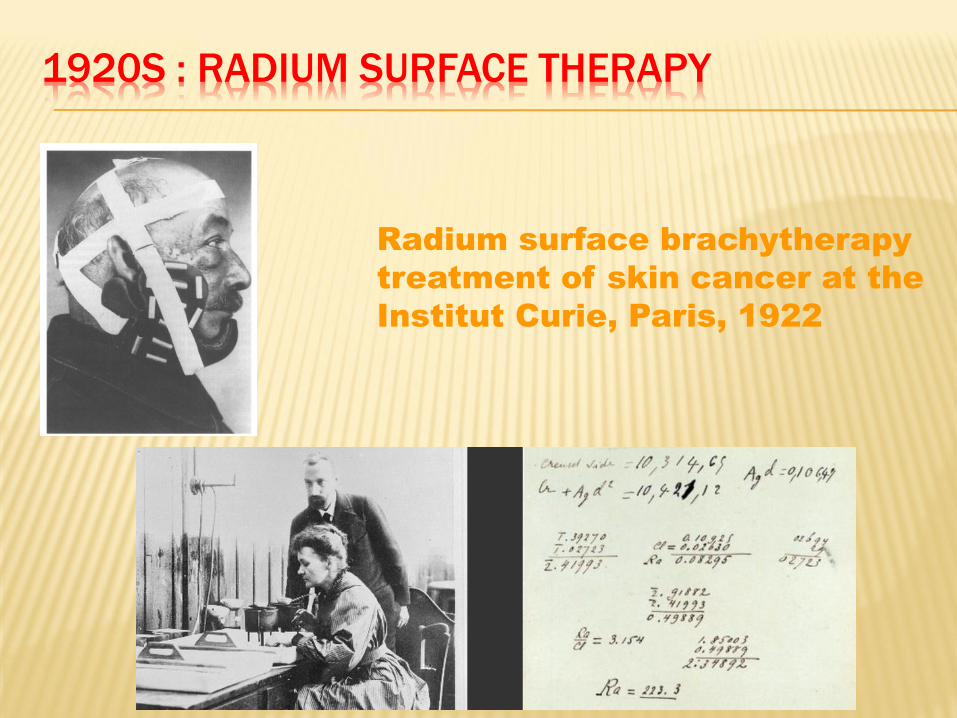
1920S : RADIUM SURFACE THERAPY
Radium surface brachytherapy
treatment of skin cancer at the
Institut Curie, Paris, 1922
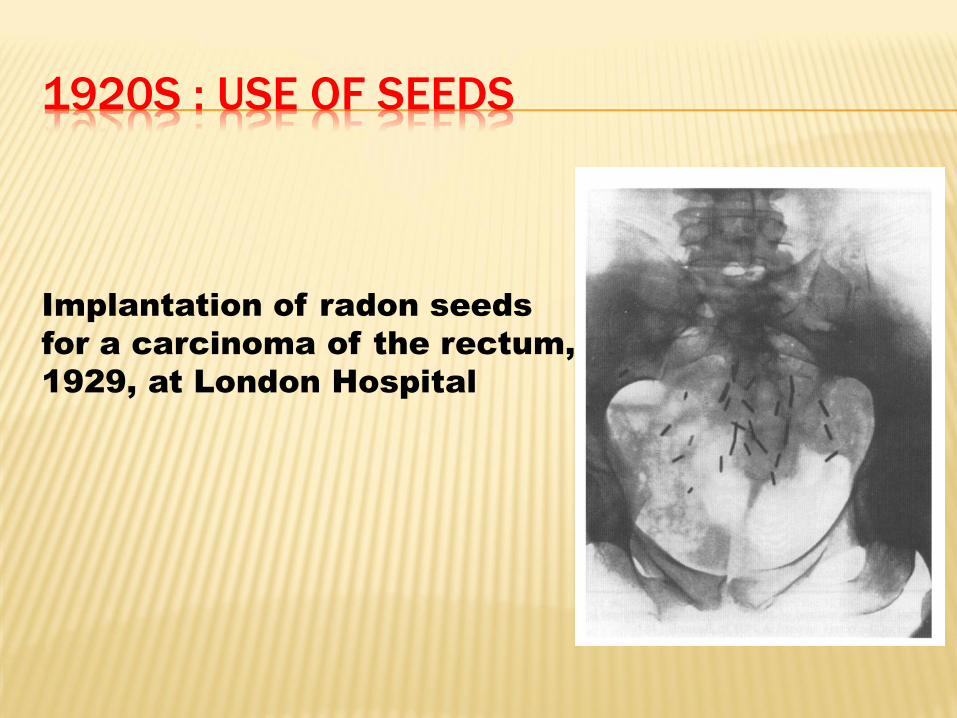
1920S : USE OF SEEDS
Implantation of radon seeds
for a carcinoma of the rectum,
1929, at London Hospital

INTRODUCTION
ICRU 38 classification
Low dose rate (LDR): 0.4 – 2 Gy/hr
Medium dose rate (MDR): 1-12 Gy/hr
High dose rate (HDR): > 12 Gy/hr
Intracavitary brachytherapy
Intraluminal brachytherapy
Interstitial brachytherapy
BRACHYTHERAPY SOURCE STRENGTH
Milligram radium equivalent
The air Kerma strength is defined as the air
kerma rate (µGy/hr) at a specified distance (1m)
Unit of uGym2/hr
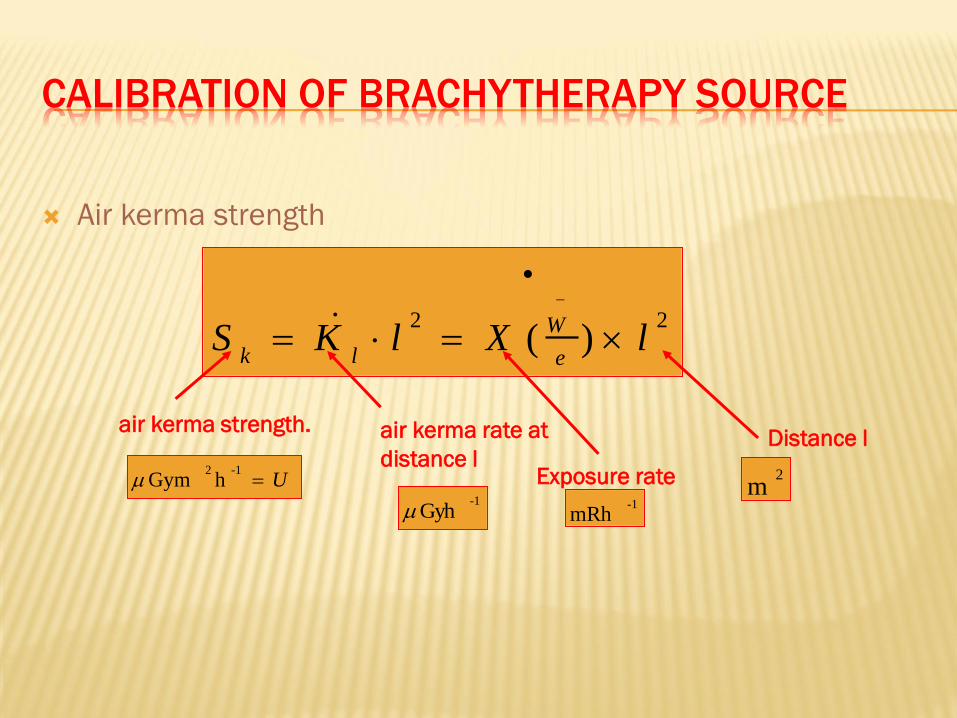
CALIBRATION OF BRACHYTHERAPY SOURCE
Air kerma strength
22)( lXlKS
e
W
lk
air kerma rate at
distance l U
-12hGym
-1Gyh
Distance l
2m
air kerma strength.
-1mRh
Exposure rate
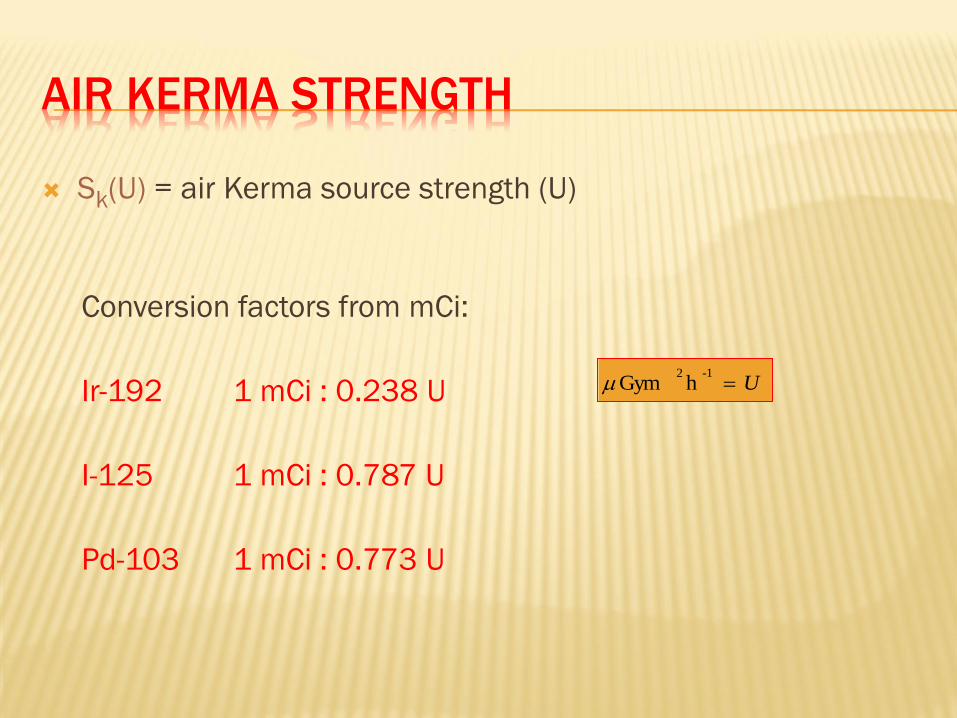
AIR KERMA STRENGTH
Sk(U) = air Kerma source strength (U)
Conversion factors from mCi:
Ir-192 1 mCi : 0.238 U
I-125 1 mCi : 0.787 U
Pd-103 1 mCi : 0.773 U
U-12
hGym
TRACEABILITY
The AAPM Task Group No. 40 had
recommended traceability of brachytherapy
sources in 1994
Direct traceability
Secondary traceability
Secondary traceability by statistical inference
TRACEABILITY
The NIST standard
ADCLs standards
A customer’s source is calibrated at an ADCL or
NIST by placing it in the well chamber
A customer’s well chamber is calibrated at an
ADCL or NIST against a national standard at an
ADCL or NIST.
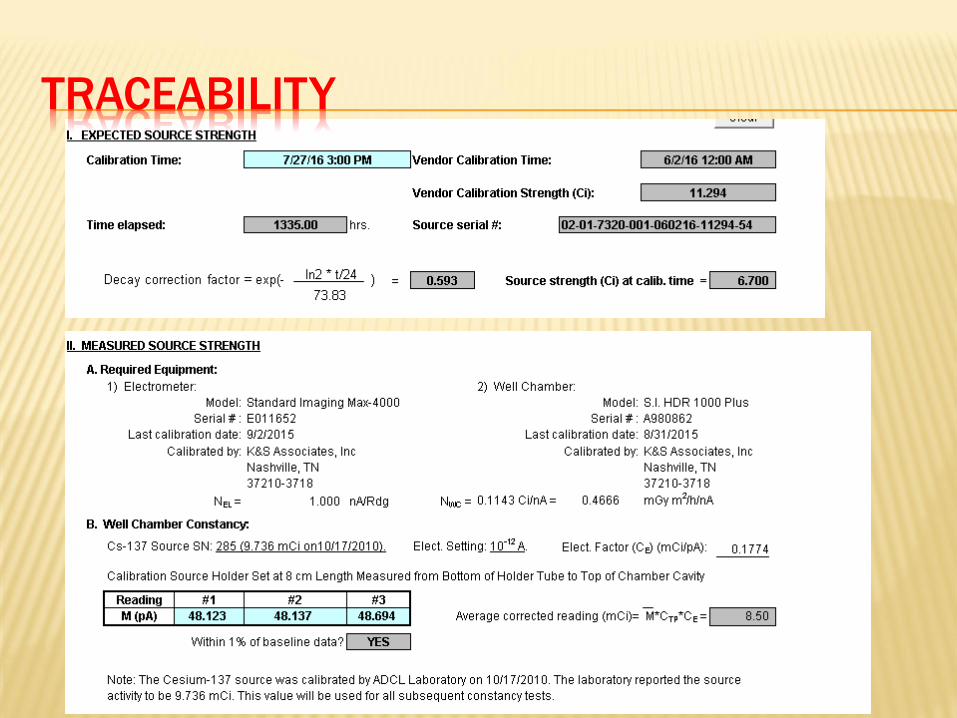
TRACEABILITY
SOURCE DOSIMETRY: ICWG
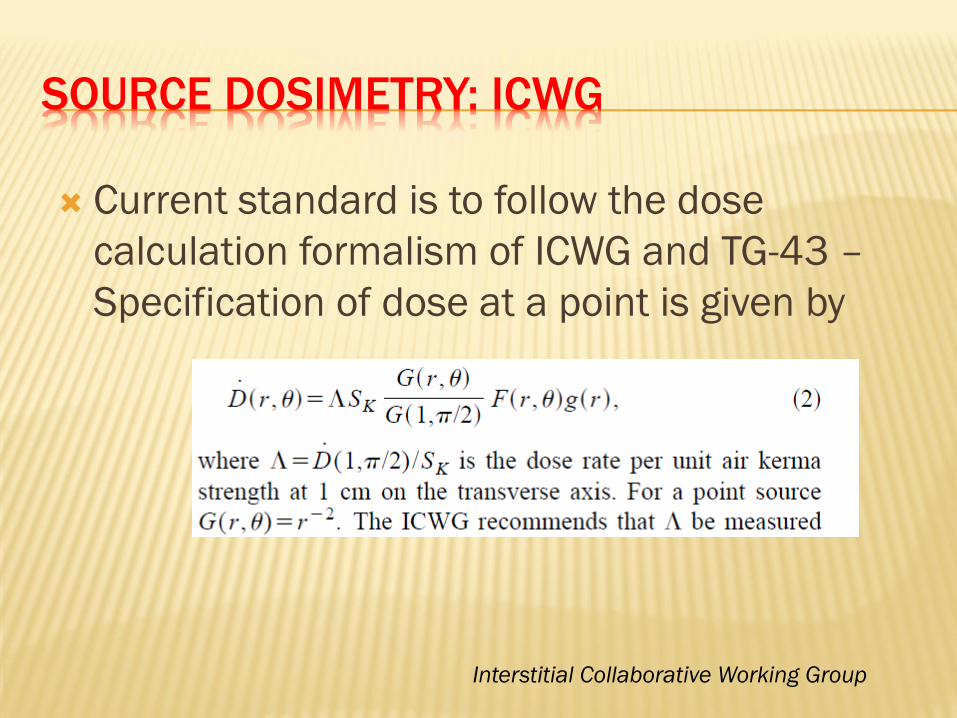
Current standard is to follow the dose
calculation formalism of ICWG and TG-43 –
Specification of dose at a point is given by
Interstitial Collaborative Working Group
GOAL OF QA PROGRAM
The QA program consists of a set of mandated
redundant performance checks, physical
measurements, documentation standards,
training and experience standards, and
guidelines
GOAL OF QA PROGRAM
QA program endpoints
Safety of the patient, the public, and the institution
Positional accuracy +/-2mm is reasonable (+/-
1mm, NRC)
Temporal accuracy 2%
Source calibration +/-3%, relative to existing air
kerma strength standards seems reasonable.
dose calculation +/-2%
PHYSICIST’S ROLE
Applicator insertion process
Implant design and evaluation process
Treatment delivery process
PERFORMANCE OF BRACHYTHERAPY
PROCEDURE
The physician–physicist interaction is a critical
link in promoting safe and accurate
Brachytherapy practices
Ordering sources (RML)
Receiving sources
Treatment planning goal, according to
prescription
TREATMENT QA
It is recommended that standard patterns of
dwell times for similar applications be used
whenever possible
Physicist should check the applicator position
and the connections between applicator and
afterloader head before treatment to be sure
that they agree with the treatment plan.
DOSE SPECIFICATION AND REPORTING
Lack of universal system for dose specification and reporting
Many quantities have been used to quantify, prescribe, and to constrain intracavitary therapy at gynecologic malignancies
Dose to point A
Vaginal surface dose
Treatment time
Curie seconds
DOSE SPECIFICATION AND REPORTING:
INTRACAVITARY BRACHYTHERAPY
ICRU attempted to address this issue in report N 38
In addition to reporting source strengths, treatment time, and standard isodose contours
the dimensions of the 60-Gy isodose (EBT + HDR)
the dose at a bladder point
Rectal dose
Doses at points representing lower para-aortic
Dose at points representing distal parametrium and lymph nodes
BACKGROUND
Prompted by:
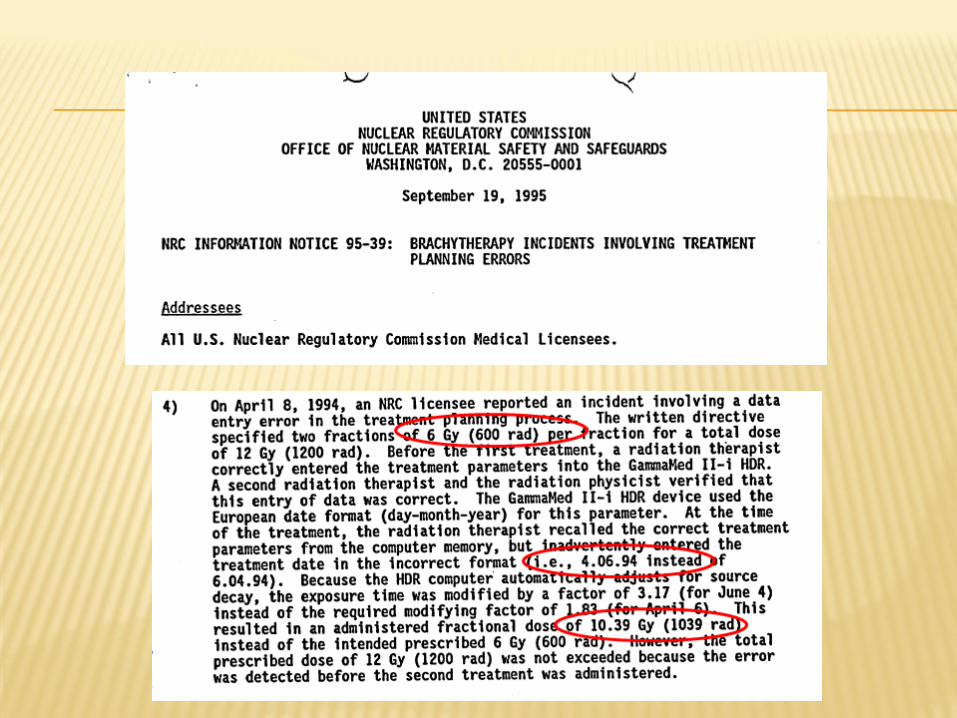
A death related to personnel errors in HDR
Greater use of HDR brachytherapy units
NRC proposal to rewrite 10 CFR 35
The need for education on comprehensive HDR
safe-treatment-delivery procedures
None of old reports addresses the details and
issues related to the safe delivery of HDR
treatments.
EGREGIOUS INCIDENT
Death related to personnel errors
Source left in the patient
Radiation alarm ignored
Survey meter was not used
OVERVIEW
To examine the current high dose-rate (HDR)
treatment delivery practices and to prepare a
document to assure safe delivery of HDR
treatments
The document provides an extensive quality
assurance (QA) check list
HDR PROS
Dose optimization capability
Outpatient treatment
More stable positioning
Smaller applicators
Sources do not need to be shipped
Better documentation
Reduced exposure to personnel
HDR CONS
More complex
Errors can lead to severe consequences
Radiobiological disadvantages (normal tissue
toxicity)
Need for accurate dosimetry
Potential of very high dose to patient and
personnel if source fails to retract
DESIGN OF AN HDR BRACHYTHERAPY
PROGRAM
HDR brachytherapy is prone to errors
The physicist’s role is to define the organization
and responsibilities of the treatment delivery
team members
PRINCIPLES OF GOOD HDR PROGRAM DESIGN
Use written documentation whenever possible
Develop a formal procedure for each type of expected case Roles, applicators, emergency situation, QA list
Exploit redundancy Independent verification
Exploit quality improvement techniques: Comprehensive QA program
DOCUMENTATION AND CHECKLIST
I. Written prescription and daily treatment
record
II. Treatment day remote afterloader QA protocol
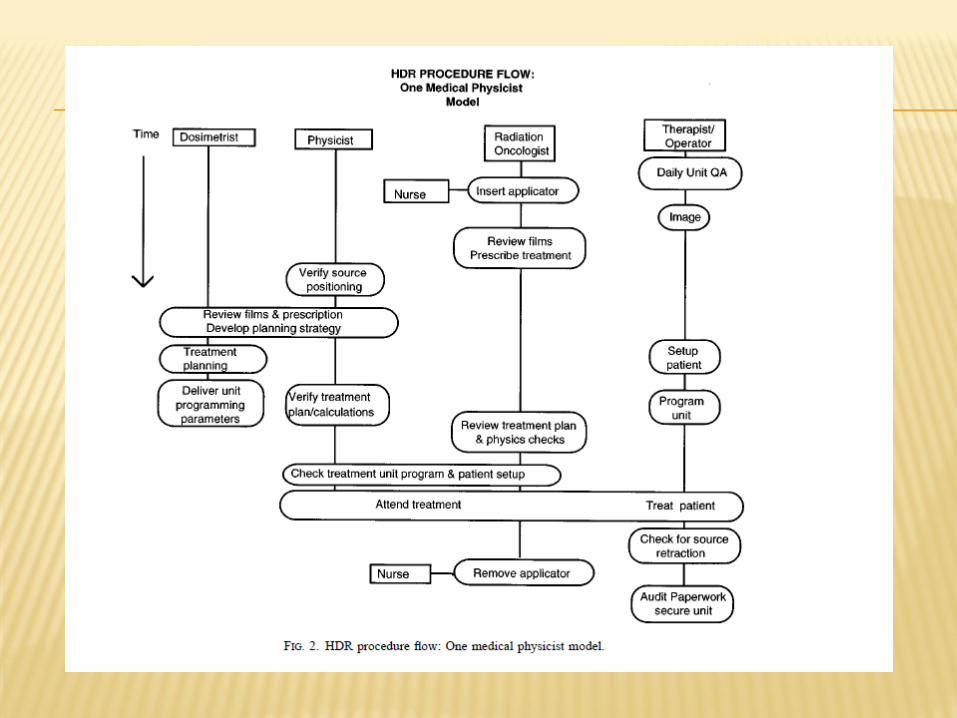
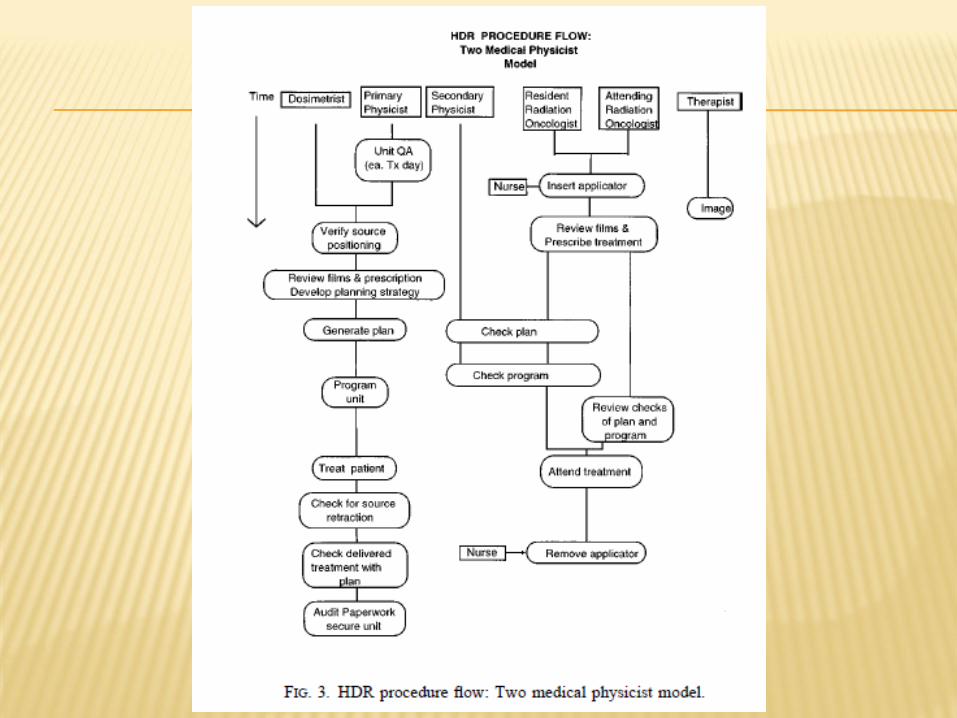
III. QA procedure flow checkoff list
IV. Physicist’s treatment plan/documentation
review
V. Implant geometry, Dwell time calculations
VI. Dose verification
STAFFING AND TRAINING
Physicians, department heads, and
administrators must realize that development and
maintenance of a safe and effective HDR program
requires a significant time commitment for all
staff involved, especially the medical physicist on
whom the burden of acceptance testing the
equipment, developing procedures, and training
other staff falls
STAFFING AND TRAINING
For an average load of 10 fractions per week,
including periodic QA, staff training and
treatment record audits, 1 FTE of a qualified
medical physicist should be allocated
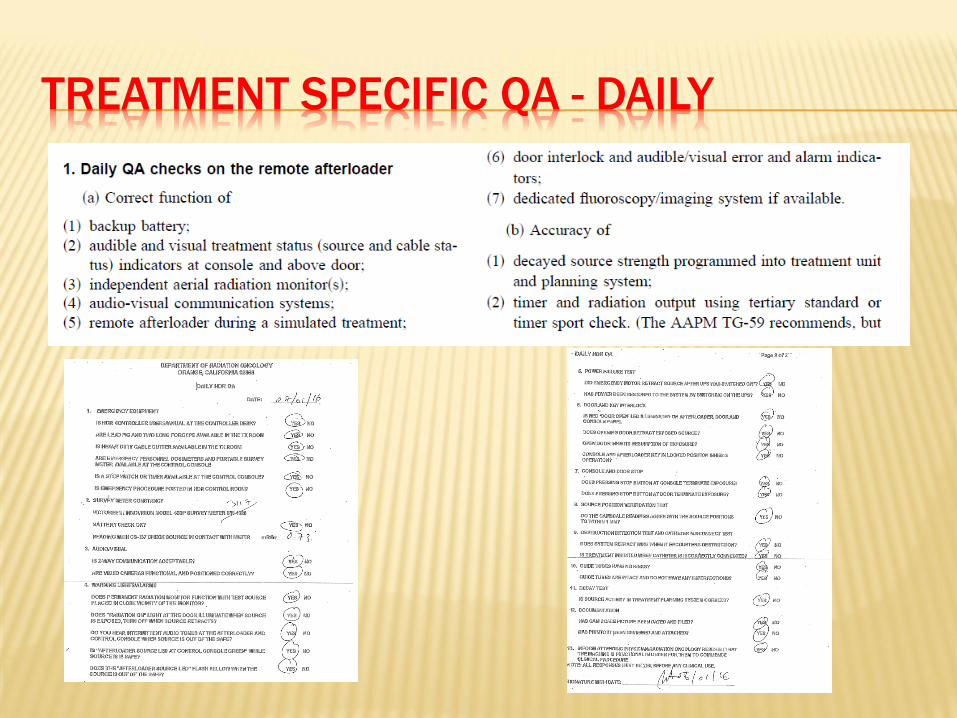
TREATMENT SPECIFIC QA - DAILY
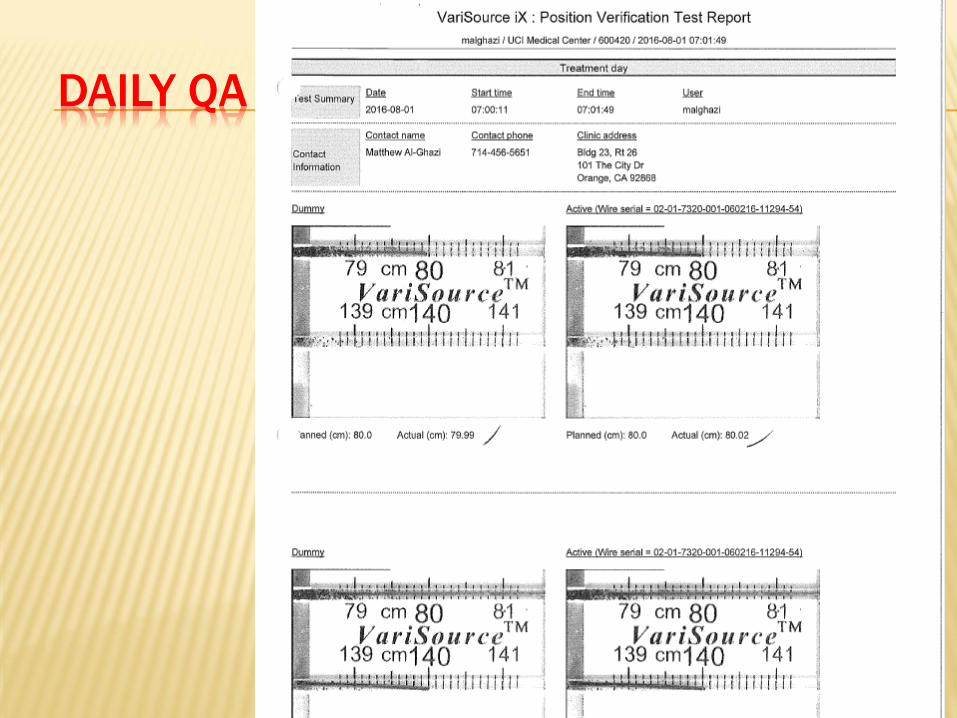
DAILY QA

PRESCRIPTION
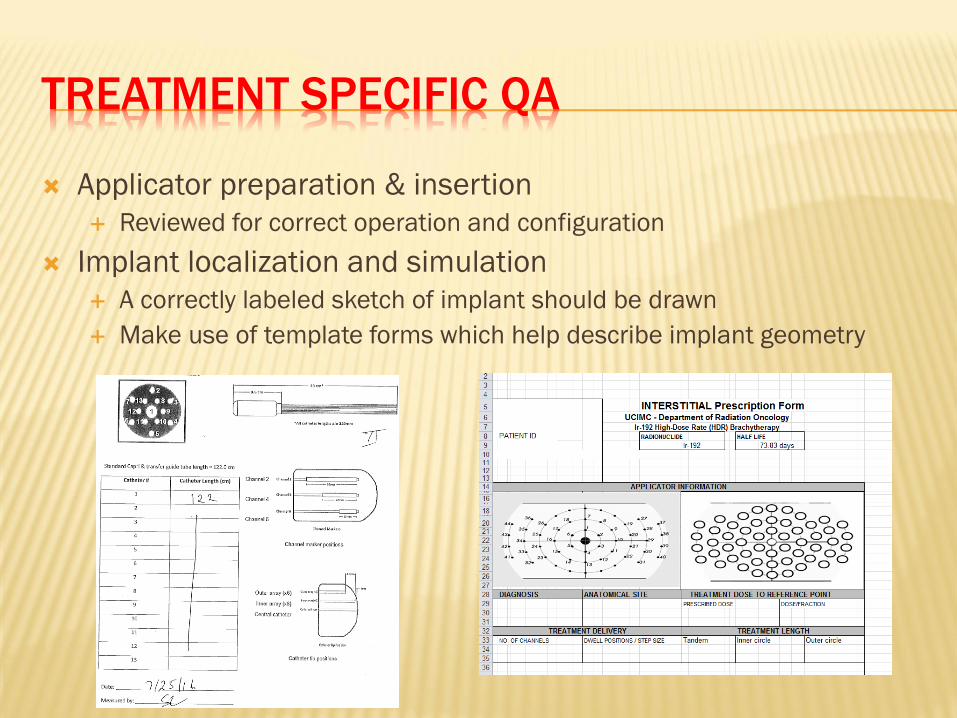
TREATMENT SPECIFIC QA
Applicator preparation & insertion
Reviewed for correct operation and configuration
Implant localization and simulation
A correctly labeled sketch of implant should be drawn
Make use of template forms which help describe implant geometry
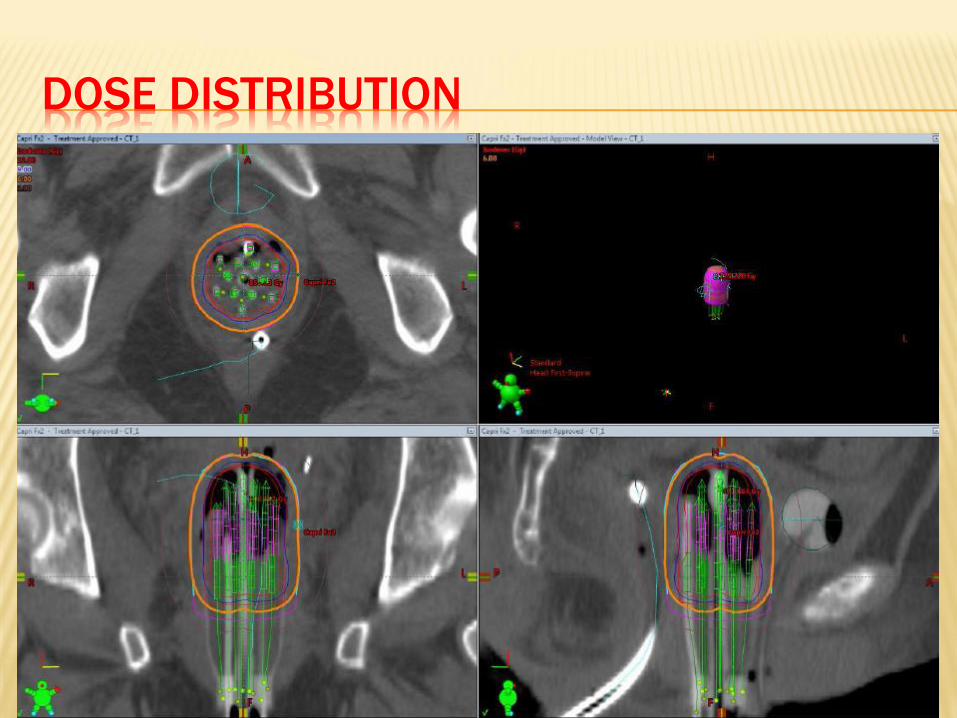
DOSE DISTRIBUTION
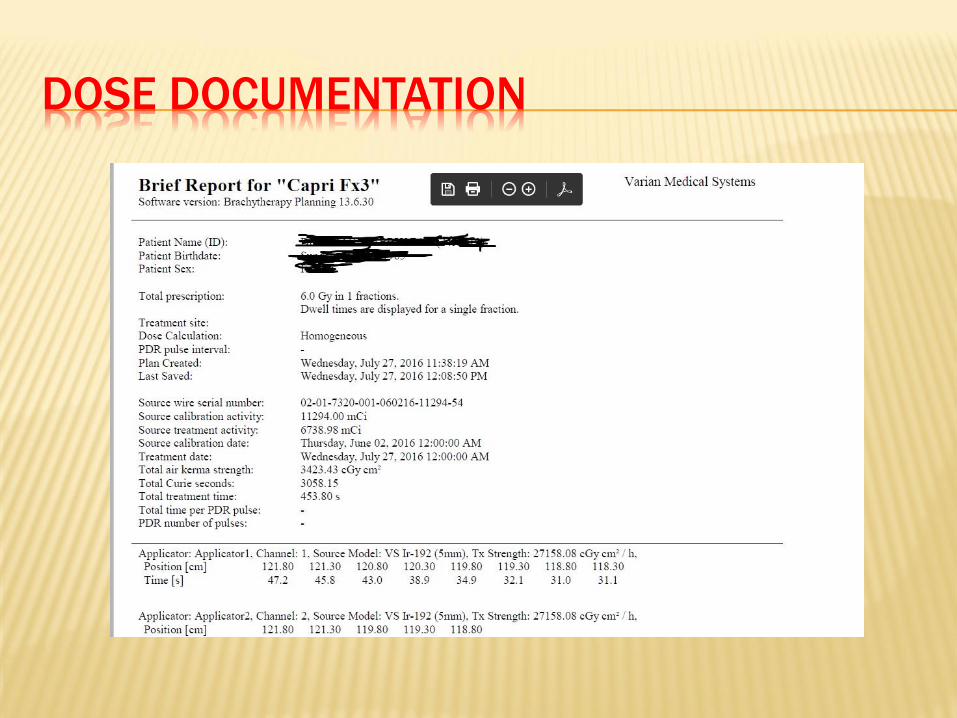
DOSE DOCUMENTATION
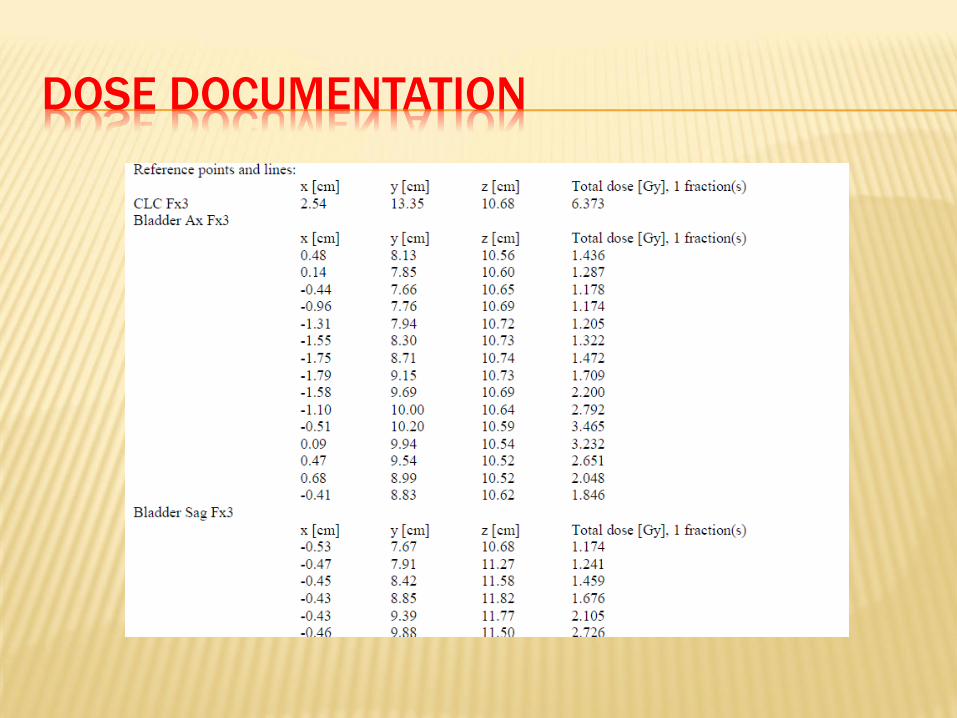
DOSE DOCUMENTATION
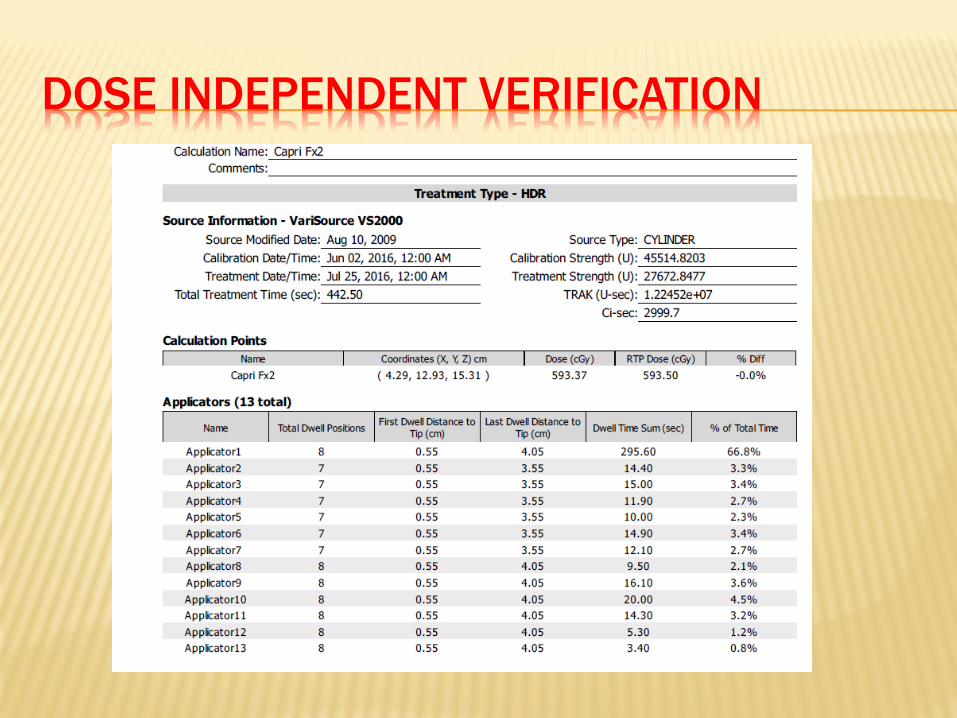
DOSE INDEPENDENT VERIFICATION
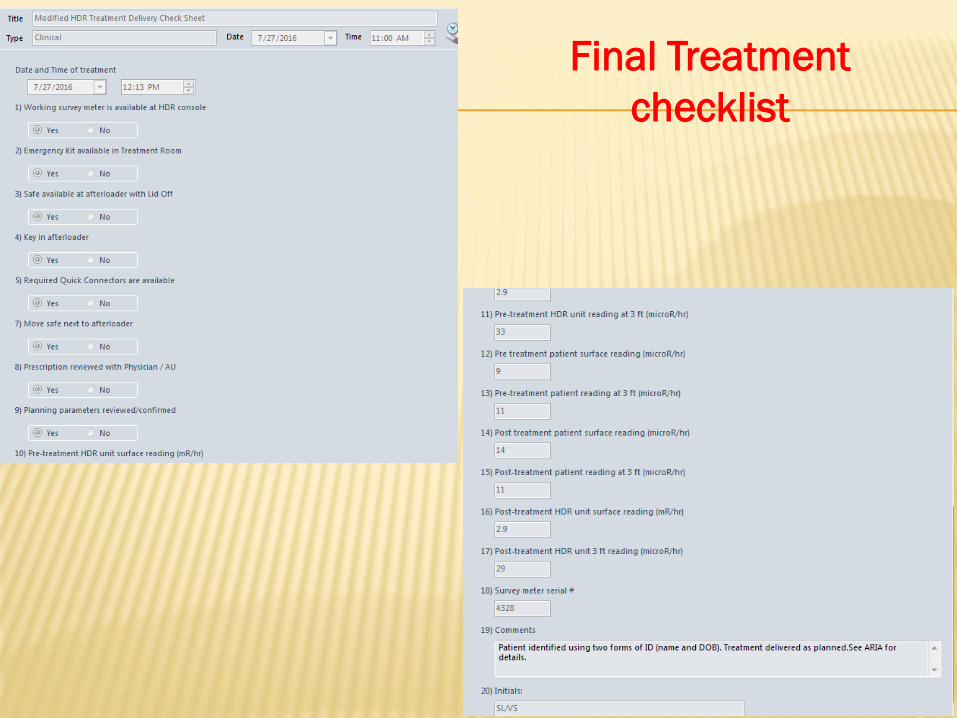
Final Treatment
checklist

TREATMENT SPECIFIC QA
Whenever treatment is interrupted, it is essential to
check the area monitor to confirm that the source has
been retracted
Again, after treatment is complete, it is again essential
check the area monitor to confirm that the source has
been retracted
EMERGENCY PROCEDURES
The best strategy is to be prepared for all scenarios by
developing emergency procedures for the following
categories:
Physical emergencies (fire, earthquake, floods, etc.)
Minor emergencies (loose source guide tube, vault
door not closing completely)
Major emergencies
Failure of source to retract, patient medical emergency,
computer failure etc.
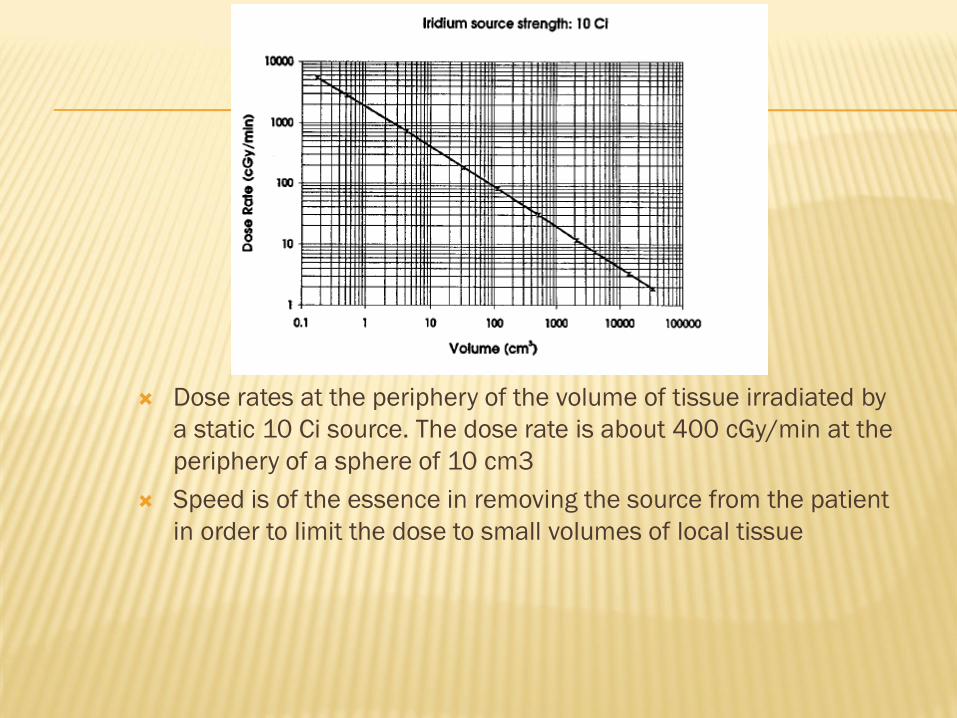
Dose rates at the periphery of the volume of tissue irradiated by
a static 10 Ci source. The dose rate is about 400 cGy/min at the
periphery of a sphere of 10 cm3
Speed is of the essence in removing the source from the patient
in order to limit the dose to small volumes of local tissue

THANKS AAPM 2016 annual meeting