radiation treatment of rectal and colon cancer :: july 2017 #crcwebinar
TRANSCRIPT

Radiation Treatment for CRC:
How it works and what to expect
Our webinar will begin shortly.
WELCOME!
#CRCWebinar

• Speaker: Michael Bassetti, MD, PhD
• Archived Webinars: FightCRC.org/webinars
• AFTER THE WEBINAR: Expect an email with links to the material & a survey. If you fill it out, we’ll send you an “I booty” bracelet
• Follow along via Twitter – use the hashtag #CRCWebinar be part of the dialog and tweet-up
Today’s Webinar:
@FightCRC | FightCRC.org
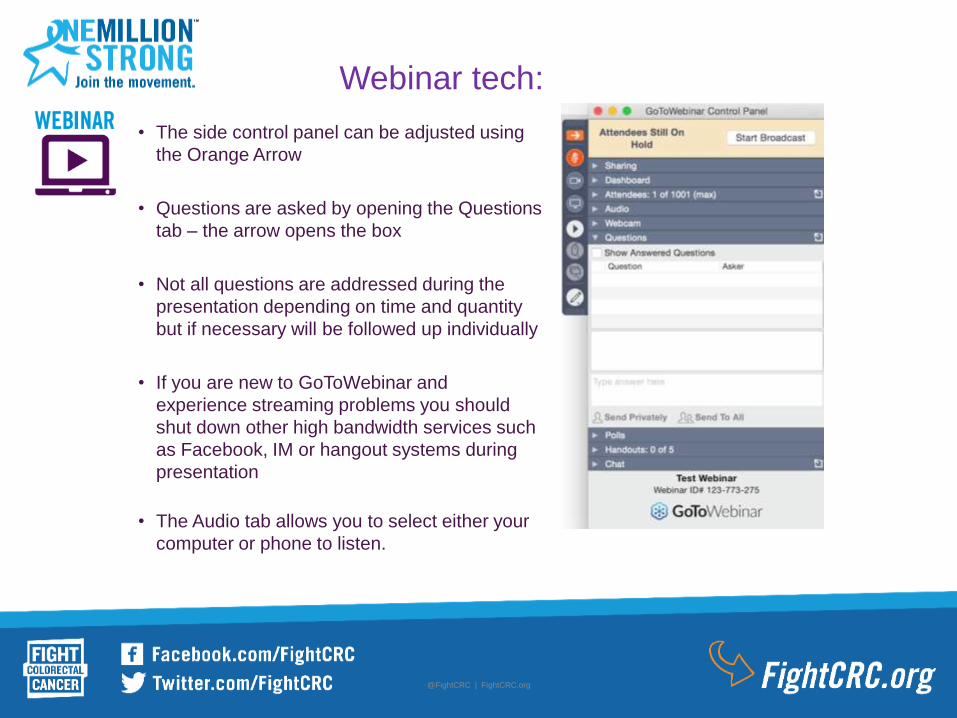
Webinar tech:
• The side control panel can be adjusted using
the Orange Arrow
• Questions are asked by opening the Questions
tab – the arrow opens the box
• Not all questions are addressed during the
presentation depending on time and quantity
but if necessary will be followed up individually
• If you are new to GoToWebinar and
experience streaming problems you should
shut down other high bandwidth services such
as Facebook, IM or hangout systems during
presentation
• The Audio tab allows you to select either your
computer or phone to listen.

Resources:
Disclaimer:
The information and services provided by Fight
Colorectal Cancer are for general informational
purposes only. The information and services are not
intended to be substitutes for professional medical
advice, diagnoses or treatment.
If you are ill, or suspect that you are ill, see a doctor
immediately. In an emergency, call 911 or go to the
nearest emergency room.
Fight Colorectal Cancer never recommends or
endorses any specific physicians, products or
treatments for any condition.
Speaker:
Dr. Bassetti is an Assistant Professor in
the Department of Human Oncology at
the UW School of Medicine and Public
Health and a member of the UW Carbone
Cancer Center. He sees patients at UW
Carbone Cancer Center.
Dr. Bassetti is a broadly trained radiation
oncologist with specialty focus on patents
with gastrointestinal (GI) cancers
(esophagus, stomach, colorectal region,
liver and pancreas). He brings expertise
in the use of 3D conformal radiation,
intensity modulated radiation and
stereotactic ablative radiation therapy. He
is committed to multidisciplinary cancer
care and the advancement of clinical
trials.
Radiation in the Treatment of
Rectal and Colon Cancer
Michael Bassetti MD PhD
University of Wisconsin
Assistant Professor of Radiation Oncology
• Radiation treatment basics
• Rectal cancer treatment
• Metastatic Colorectal Cancer
– Lungs, liver, brain
• Future Directions
– MRI guided treatment and response
– Immunotherapy in colorectal cancer
Overview
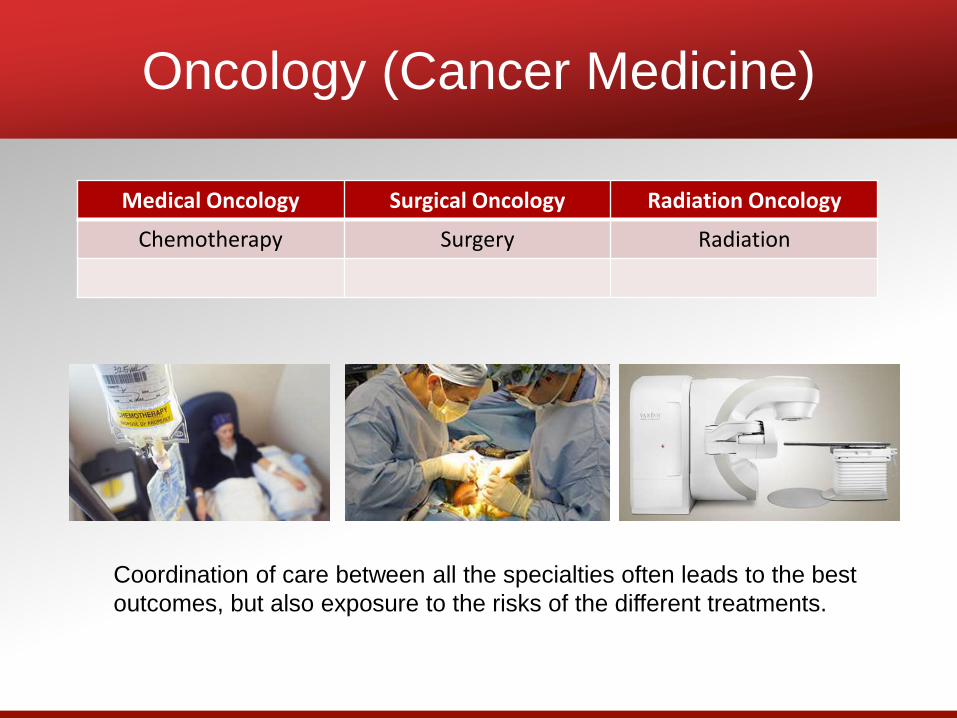
Oncology (Cancer Medicine)
Medical Oncology Surgical Oncology Radiation Oncology
Chemotherapy Surgery Radiation
Coordination of care between all the specialties often leads to the best
outcomes, but also exposure to the risks of the different treatments.
Radiation Therapy
• High energy “x-rays” aimed at the location
of the tumor.
• x-rays damage the cancer cells DNA
causing them to die.
Radiation in Colorectal Cancer Care
• Rectal cancer treatment
• Metastatic colorectal cancer treatment
– Stereotactic Radiation for spread of colorectal
cancer (metastasis) to the liver, lung, or other
organs
Radiation in Colorectal Cancer Care
• Rectal cancer treatment
• Metastatic colorectal cancer treatment
– Stereotactic Radiation for spread of colorectal
cancer (metastasis) to the liver, lung, or other
organs
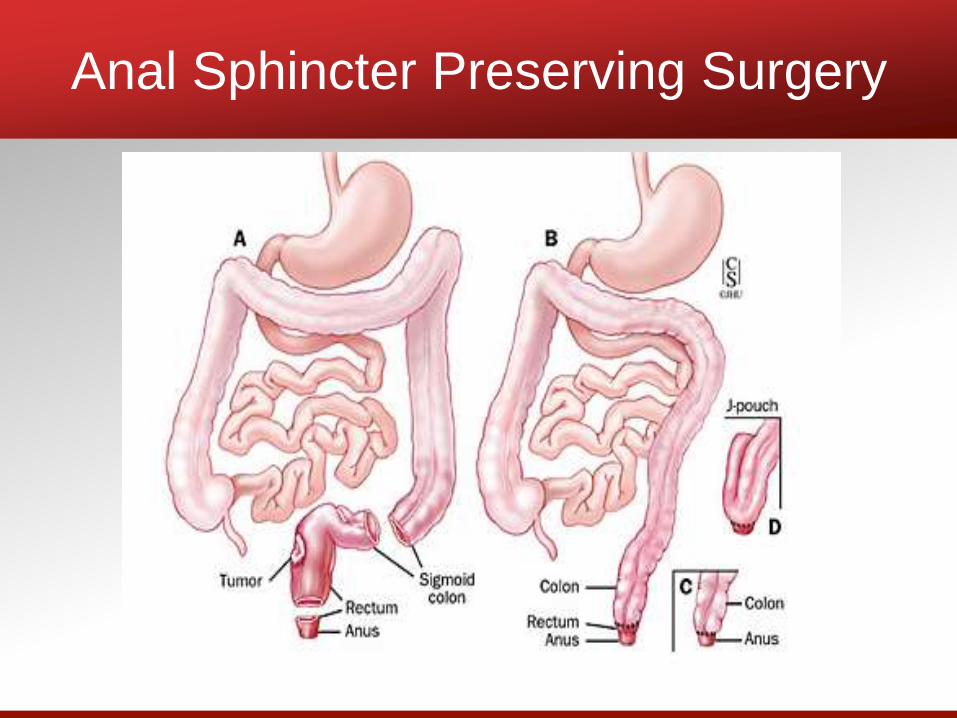
Anal Sphincter Preserving Surgery
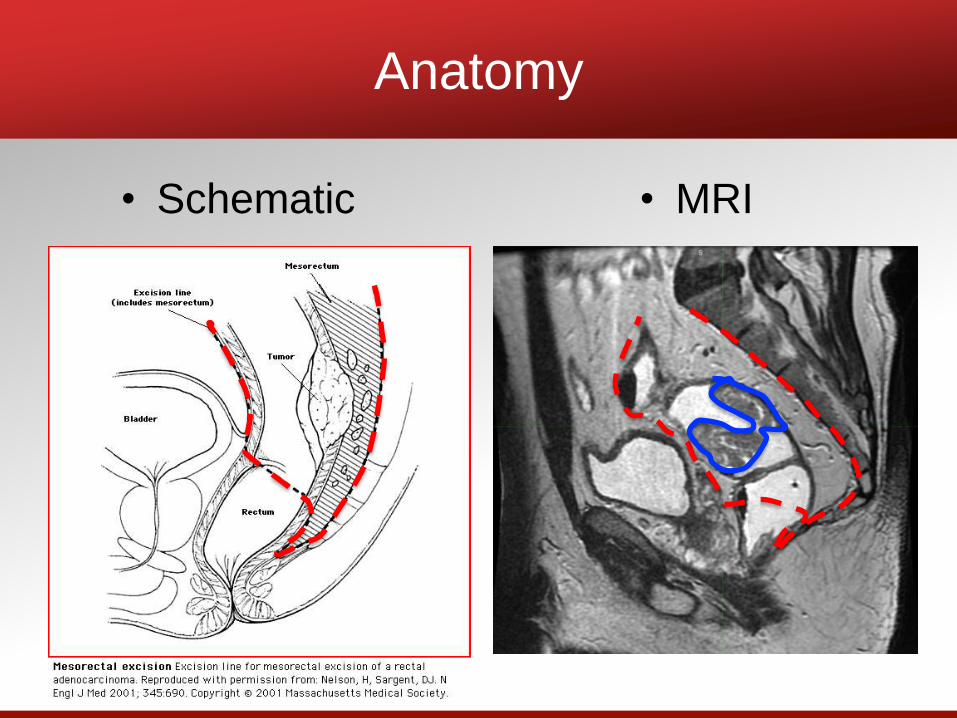
Anatomy
• Schematic • MRI
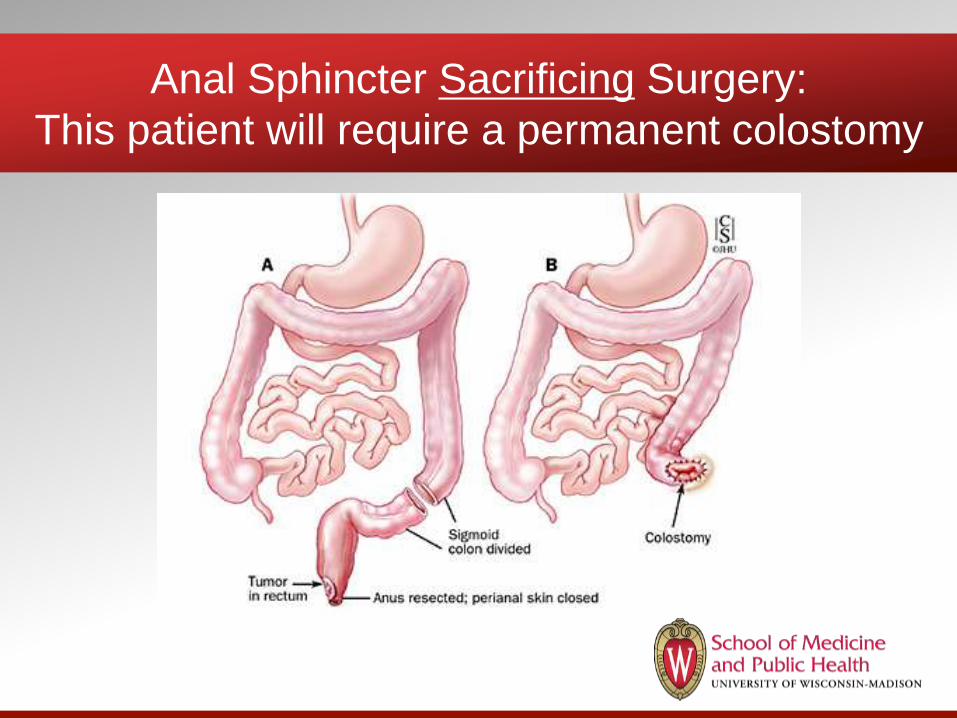
Anal Sphincter Sacrificing Surgery:
This patient will require a permanent colostomy
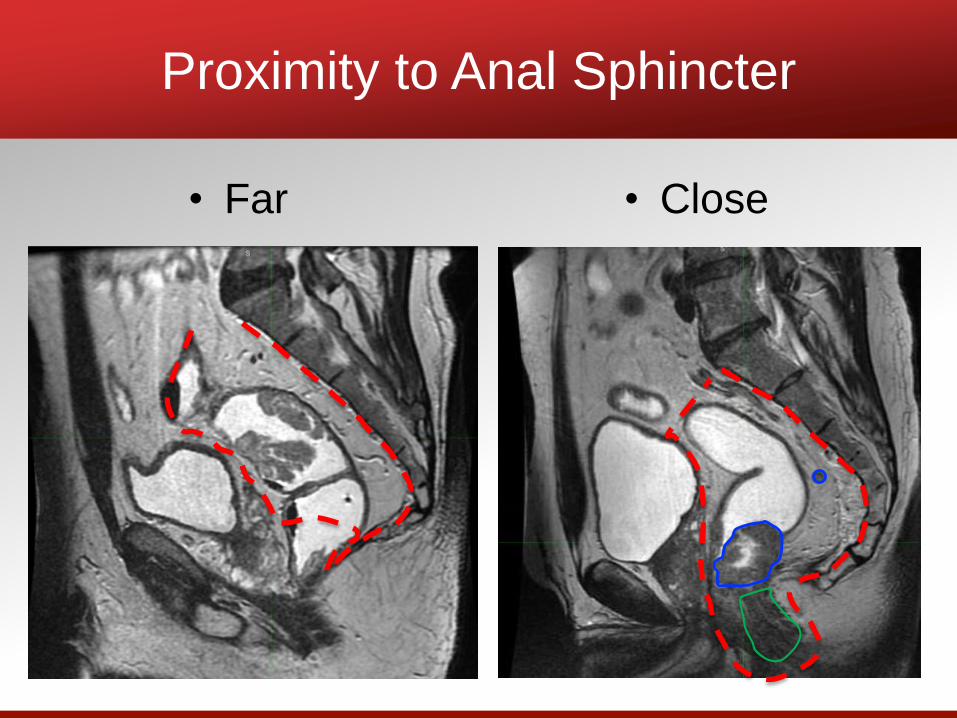
Proximity to Anal Sphincter
• Far • Close
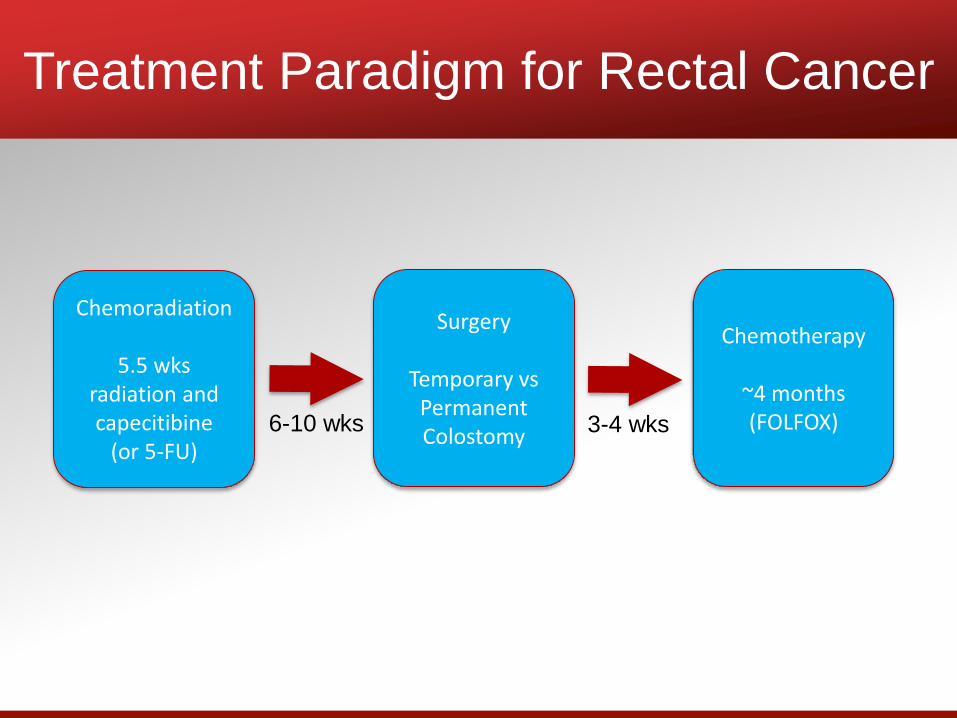
Treatment Paradigm for Rectal Cancer
Chemoradiation
5.5 wksradiation and capecitibine
(or 5-FU)
Surgery
Temporary vs Permanent Colostomy
Chemotherapy
~4 months(FOLFOX) 6-10 wks 3-4 wks
• Decrease the chance of a recurrence near
the rectum or in the adjacent lymph nodes
• Organ preservation: Decrease the chance
of an operation requiring a permanent
colostomy
• Less toxicity from chemoradiation if done
prior to surgery
Benefits of Chemoradiation
before Surgery
• Intensity Modulation lets us control the
shape of the radiation dose better than
ever before
• Improved quality of imaging both before
treatment and now during treatment with
Magnetic Resonance Image (MRI) guided
Radiation
Modern Radiation
Viewray inc
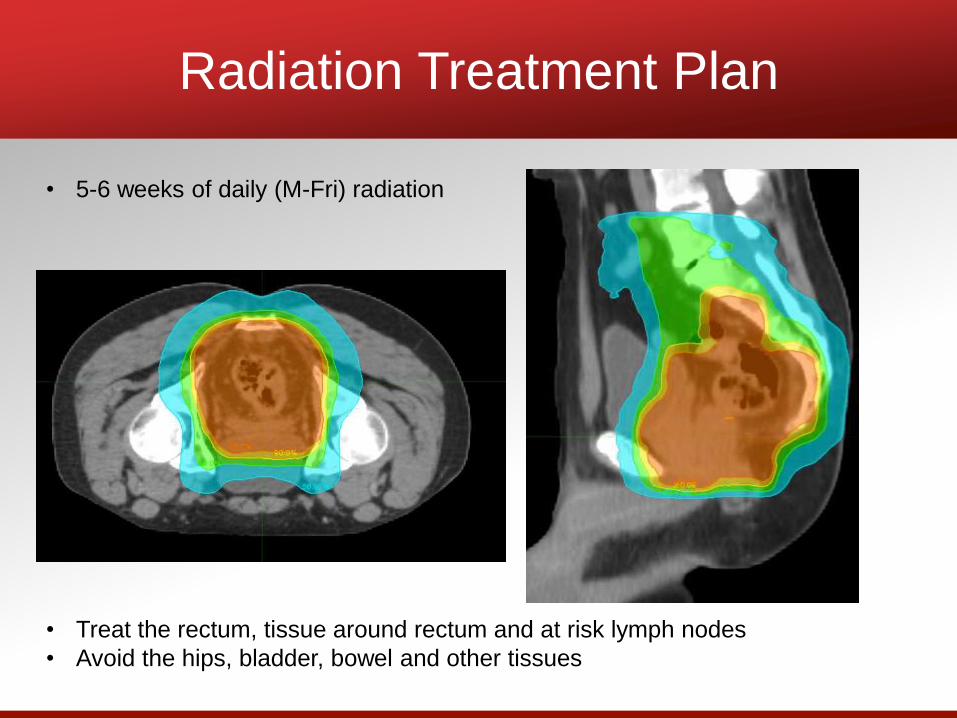
Radiation Treatment Plan
• Treat the rectum, tissue around rectum and at risk lymph nodes
• Avoid the hips, bladder, bowel and other tissues
• 5-6 weeks of daily (M-Fri) radiation
• Decreases chance of local recurrence
after surgery by half
• Organ preservation: avoid a permanent
colostomy
– One out of every five patients felt to need a
permanent colostomy was able to have avoid
it
• Less toxicity if radiation is done prior to
surgery
• Modern radiation may decrease toxicity in
some patients
Conclusions: Radiation before Surgery
• Are there situations where we could avoid
radiation?
• Do I really need to have a permanent
colostomy?
• These are questions being currently
investigated
Current Questions
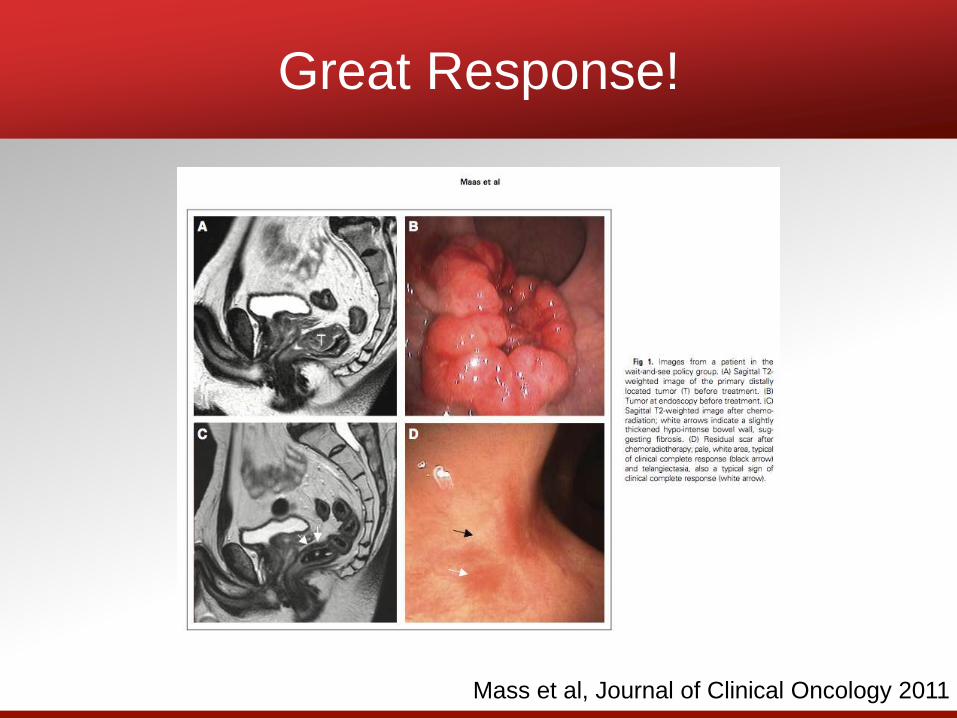
Great Response!
Mass et al, Journal of Clinical Oncology 2011
Non-Operative Management?
• Can some patients avoid surgery that
requires a permanent colostomy?
• Maybe? No Randomized Data. Long
term data from Brazil, MSKCC, and
prospective data from Netherlands support
this may be possible in highly selected
patientsHabr-Gama et al, journal of Gastrointestinal Surgery, 2006
Mass et al, Journal of Clinical Oncology 2011
Smith et al, Annals of Surgery, 2012
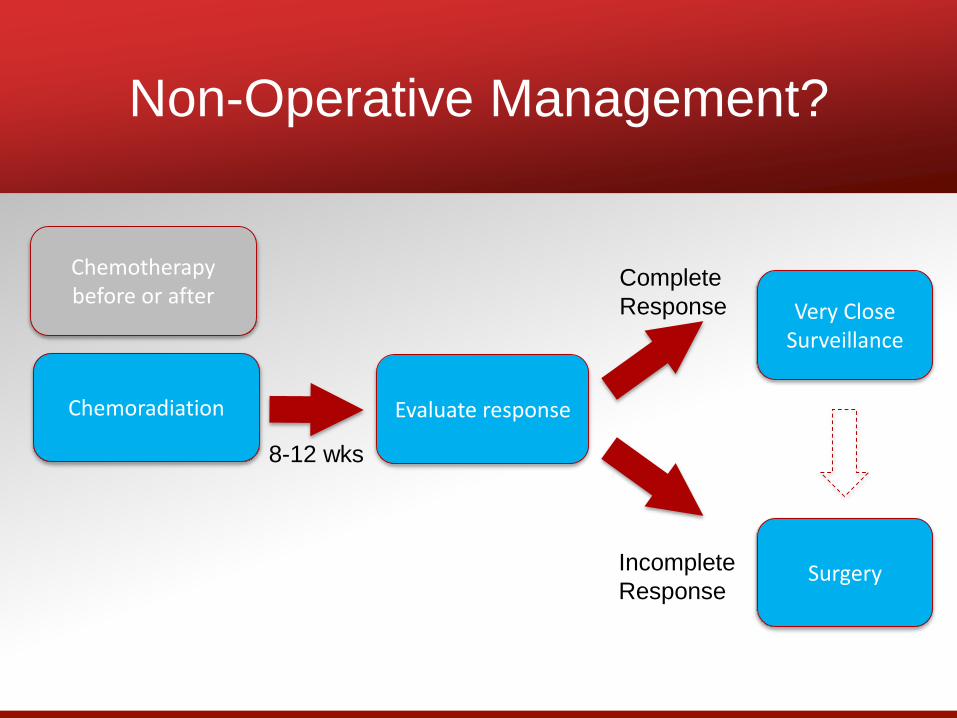
Non-Operative Management?
Chemoradiation
8-12 wks
Evaluate response
Complete
Response
Incomplete
ResponseSurgery
Very Close Surveillance
Chemotherapy before or after
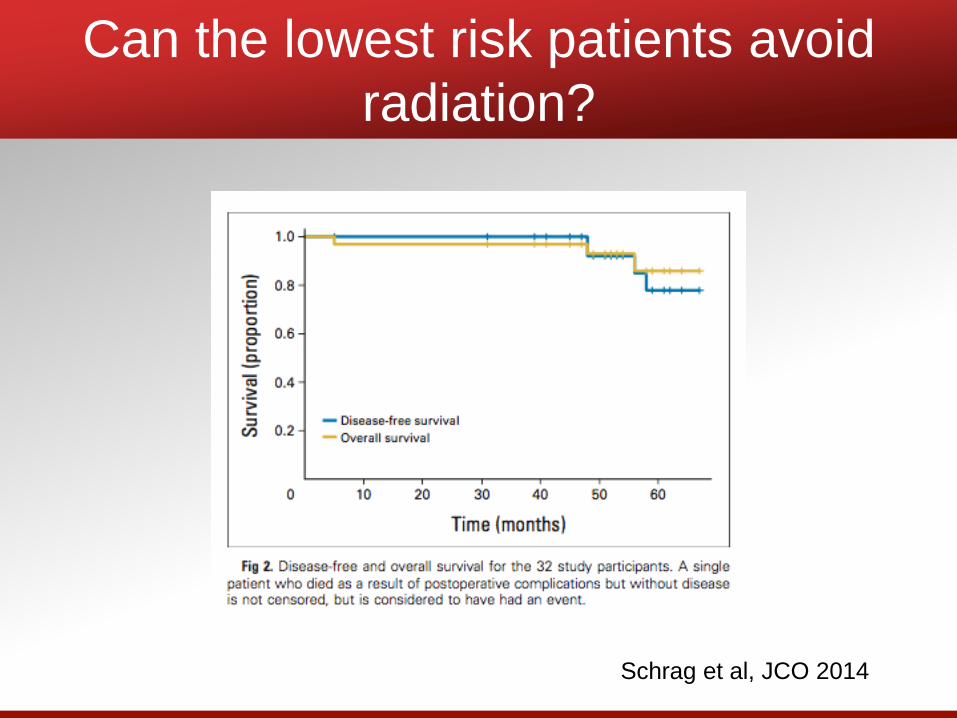
Can the lowest risk patients avoid
radiation?
Schrag et al, JCO 2014
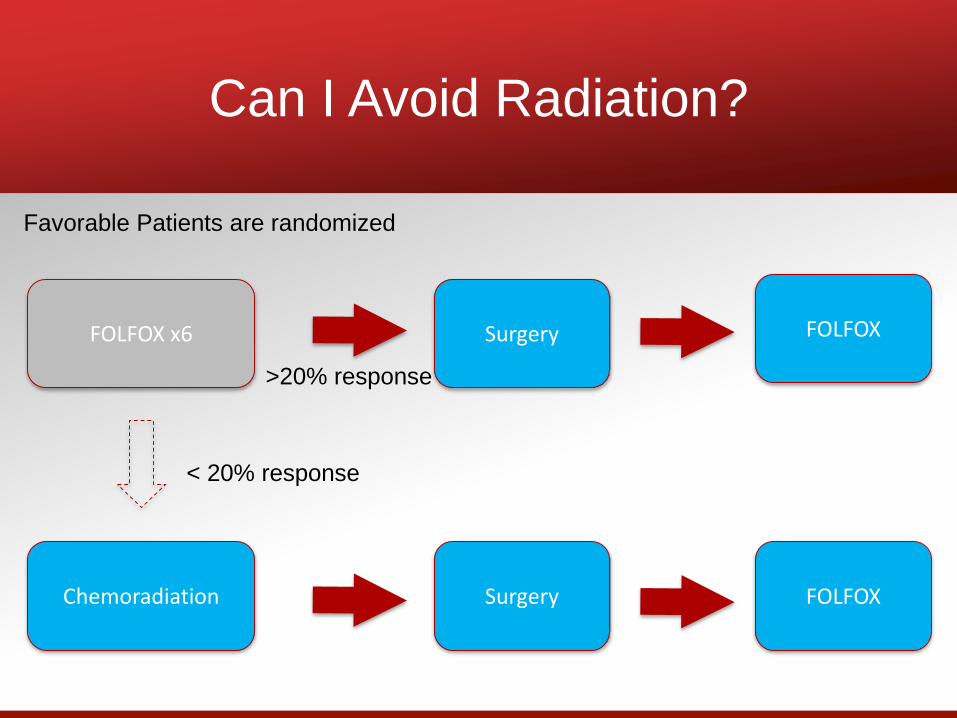
Can I Avoid Radiation?
Chemoradiation
>20% response
< 20% response
SurgeryFOLFOX x6
Surgery FOLFOX
FOLFOX
Favorable Patients are randomized
Conclusions
• Chemoradiation decreases pelvic
recurrences, optimizes chances of anal
sphincter preserving surgery.
• Omission of radiation and/or surgery are
both unanswered questions. These are
currently being investigated in randomized
clinical trials in appropriate risk patients
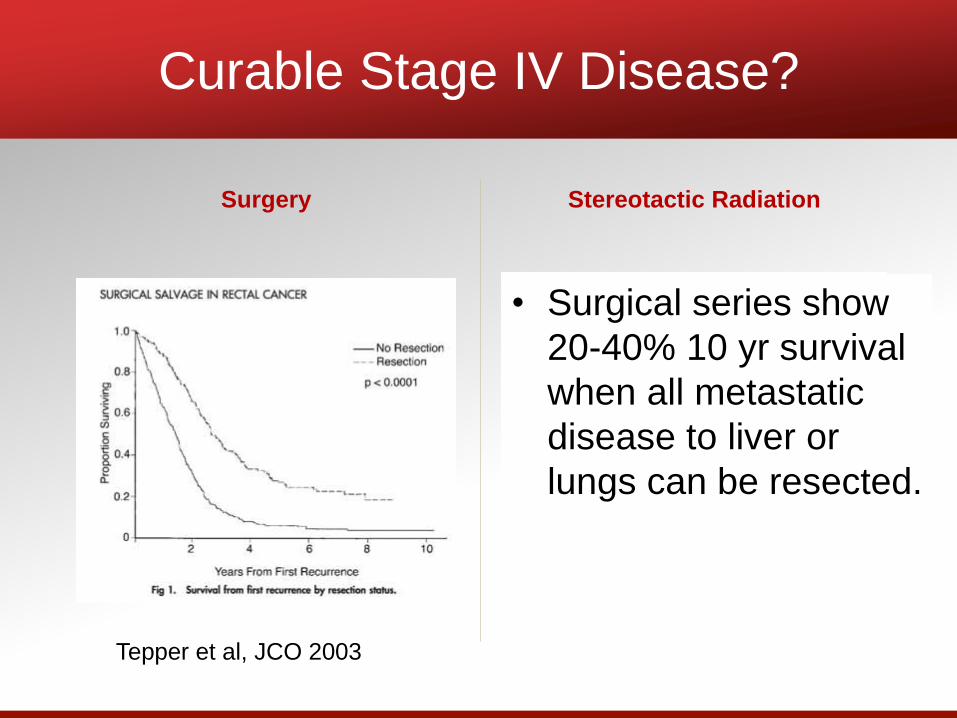
Curable Stage IV Disease?
Surgery Stereotactic Radiation
Bae et al, JSO 2010Tepper et al, JCO 2003
• Surgical series show
20-40% 10 yr survival
when all metastatic
disease to liver or
lungs can be resected.
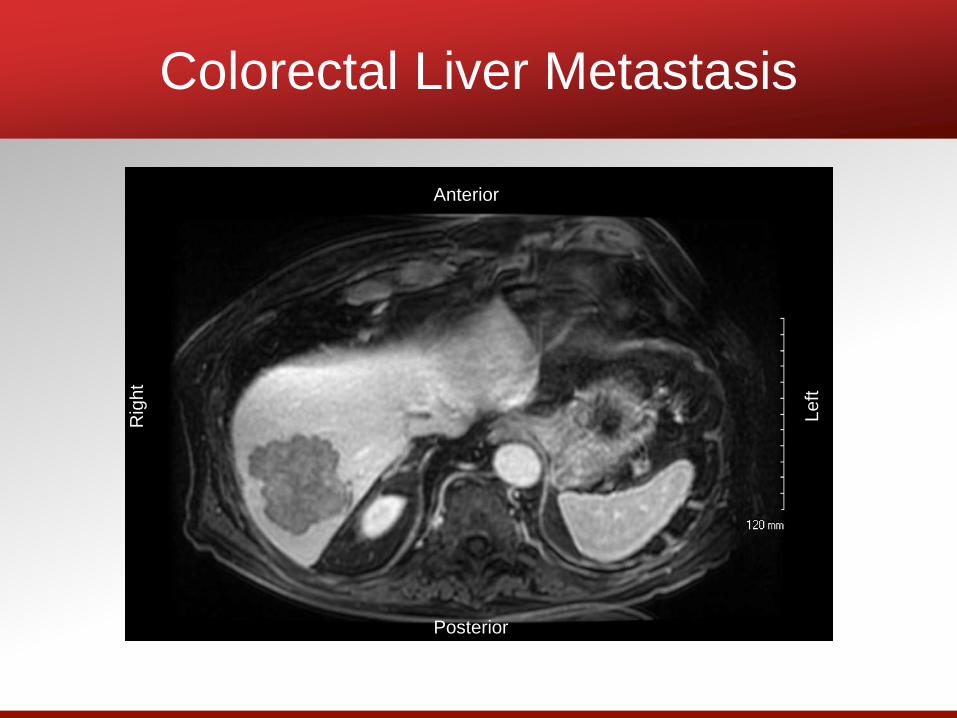
Colorectal Liver Metastasis
Anterior
Posterior
Rig
ht
Le
ft
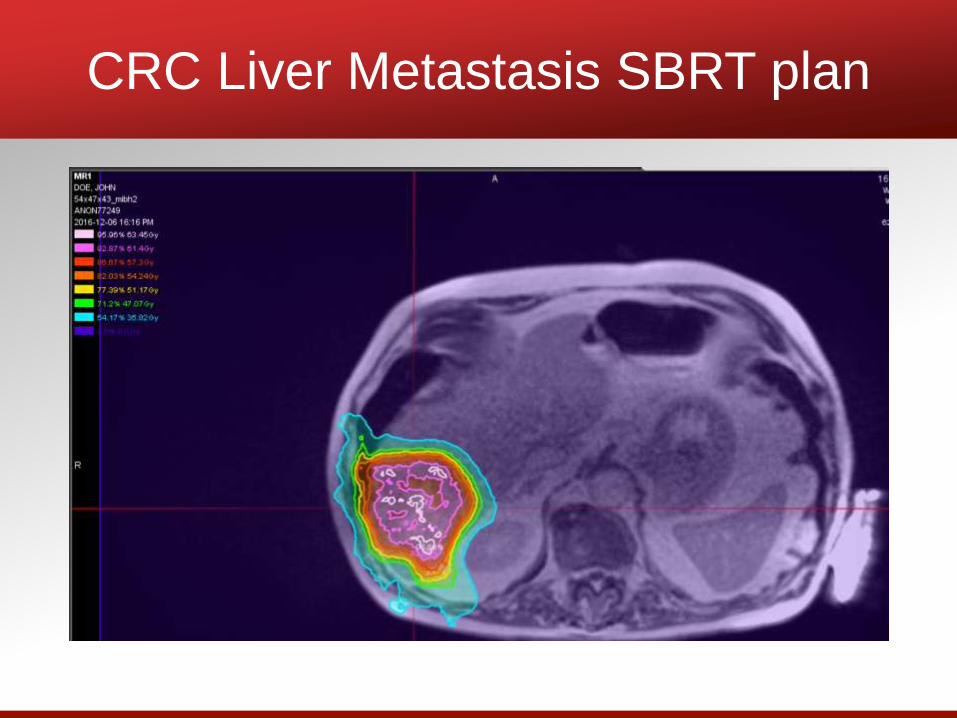
CRC Liver Metastasis SBRT plan
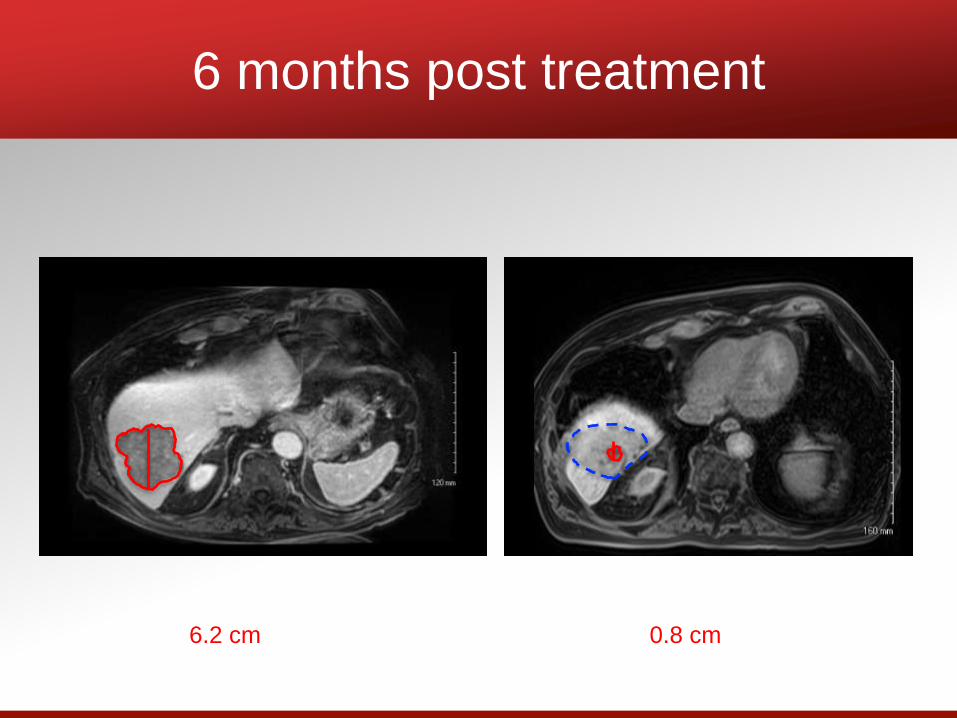
6 months post treatment
6.2 cm 0.8 cm
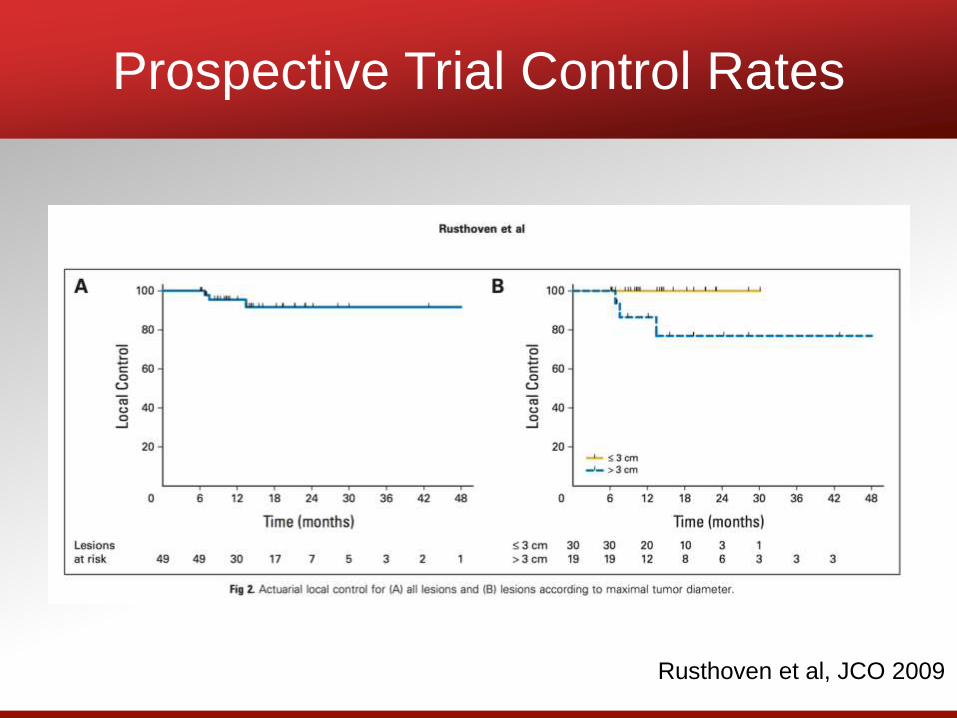
Prospective Trial Control Rates
Rusthoven et al, JCO 2009
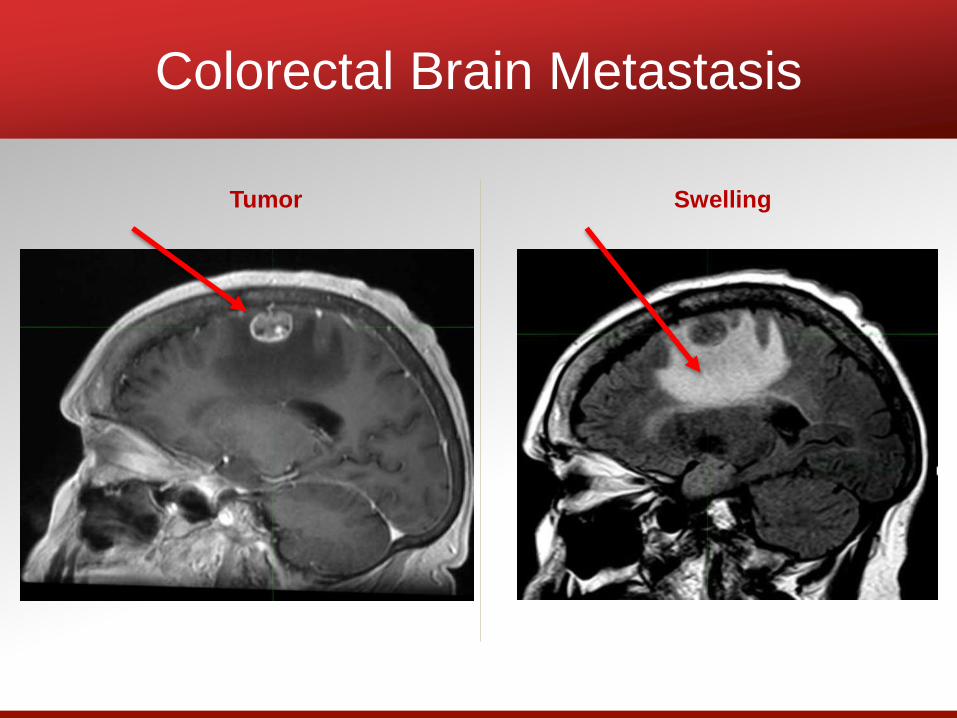
Colorectal Brain Metastasis
Tumor Swelling
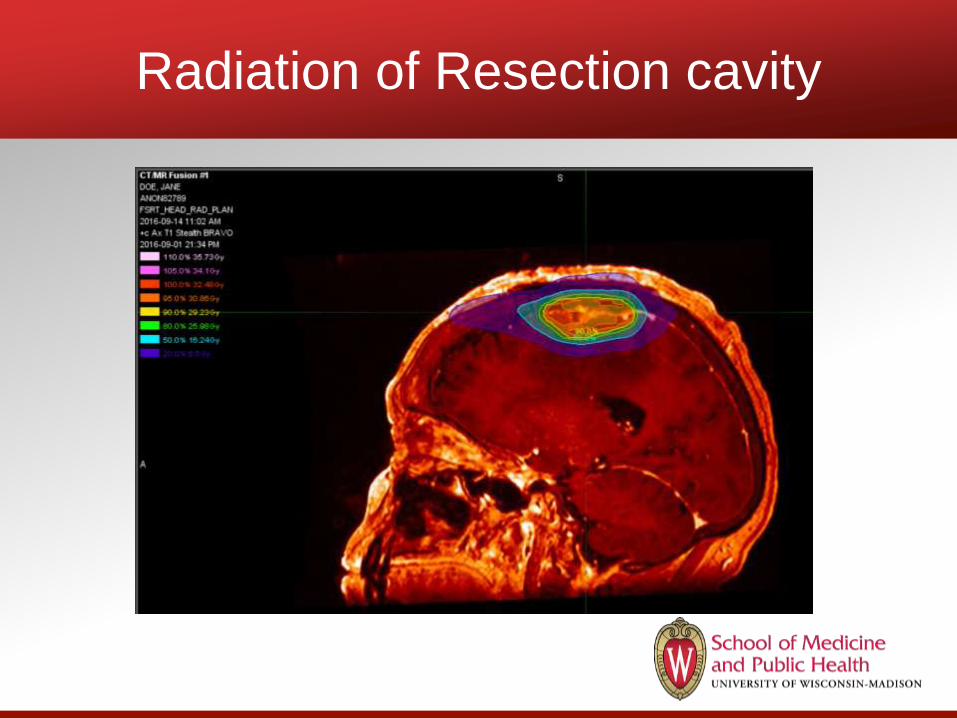
Radiation of Resection cavity
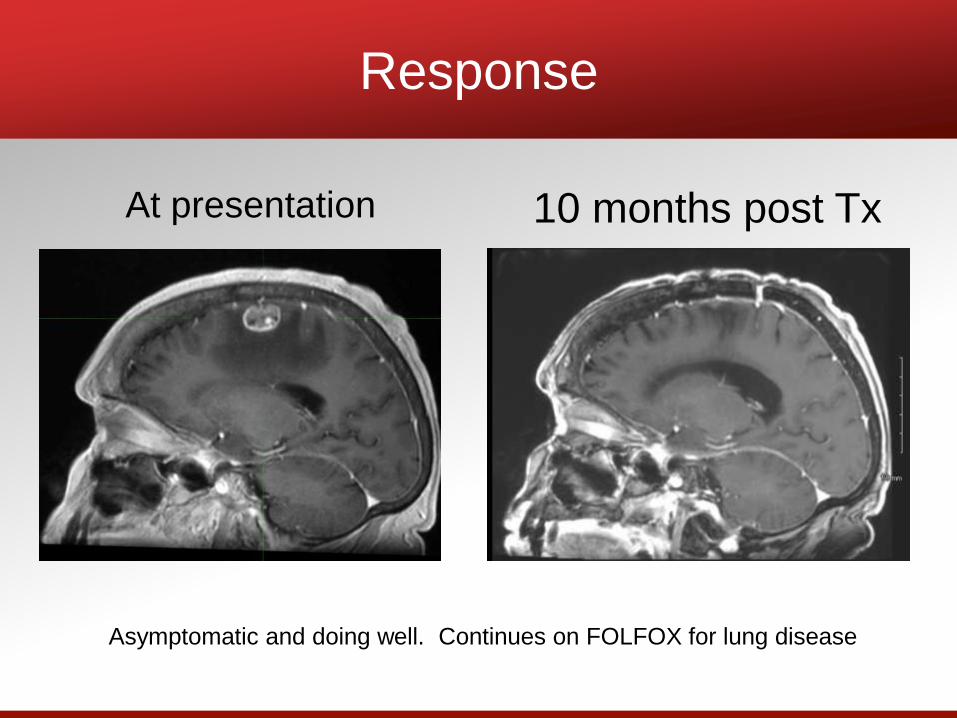
Response
At presentation 10 months post Tx
Asymptomatic and doing well. Continues on FOLFOX for lung disease
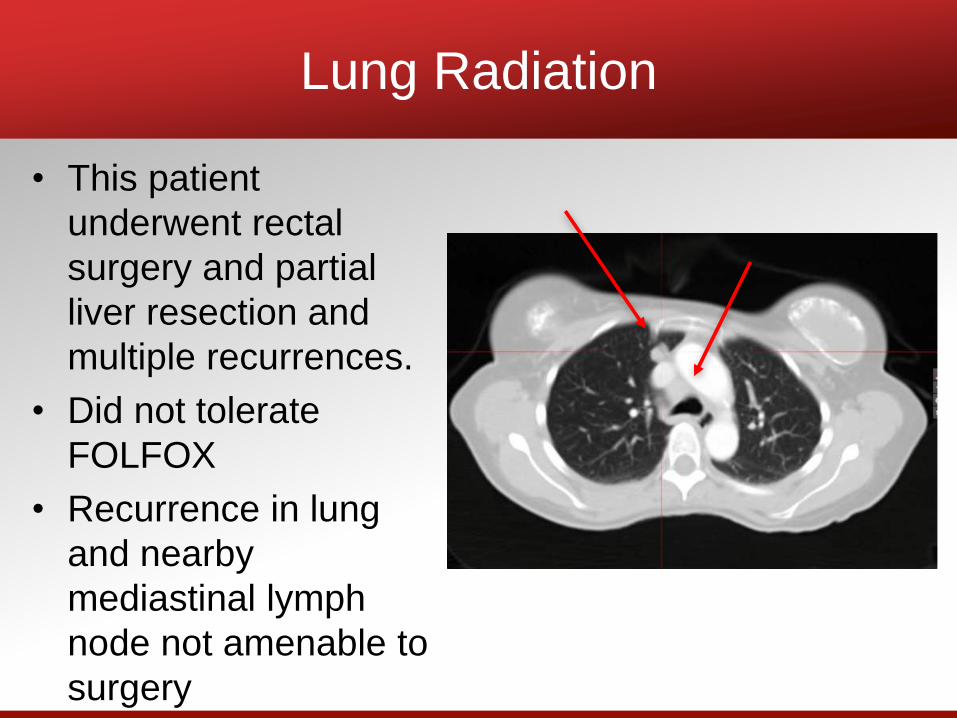
Lung Radiation
• This patient
underwent rectal
surgery and partial
liver resection and
multiple recurrences.
• Did not tolerate
FOLFOX
• Recurrence in lung
and nearby
mediastinal lymph
node not amenable to
surgery
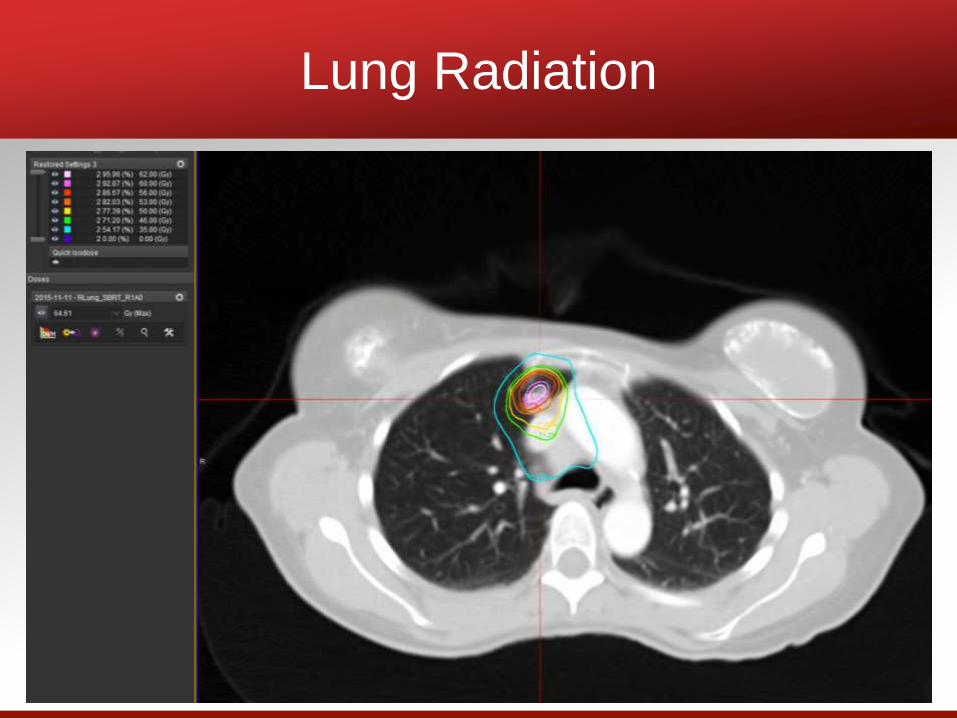
Lung Radiation

Lung Radiation
Before Treatment 1.5 years after treatment
• Stereotactic Radiation is an effective
treatment option for metastatic colorectal
patients to varying sites.
– Non-invasive
– Well tolerated
– Very effective
Conclusions
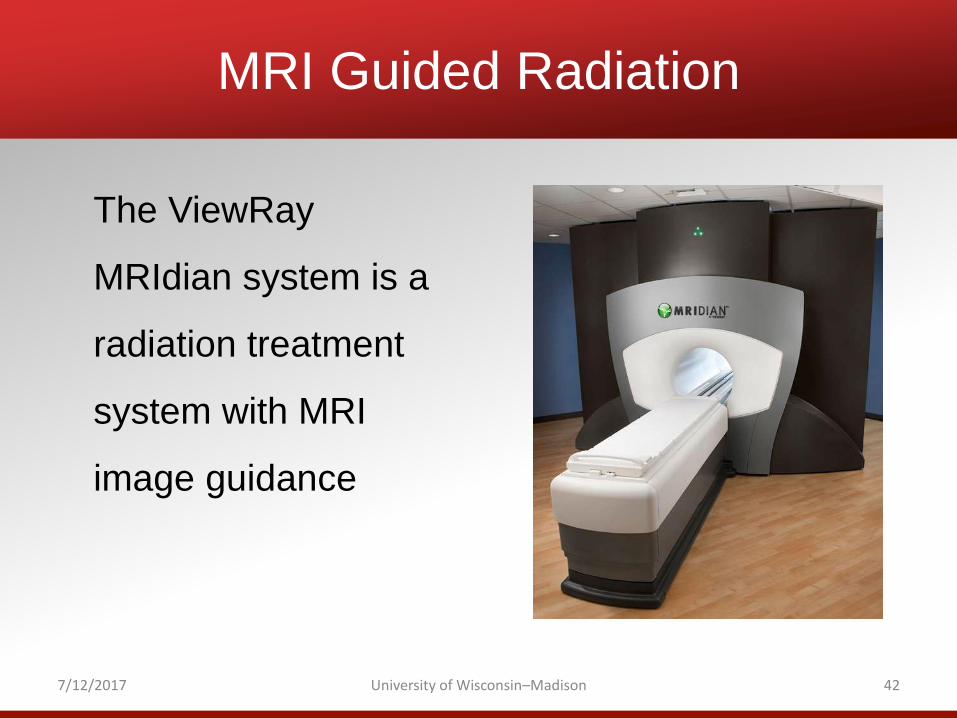
MRI Guided Radiation
The ViewRay
MRIdian system is a
radiation treatment
system with MRI
image guidance
7/12/2017 University of Wisconsin–Madison 42
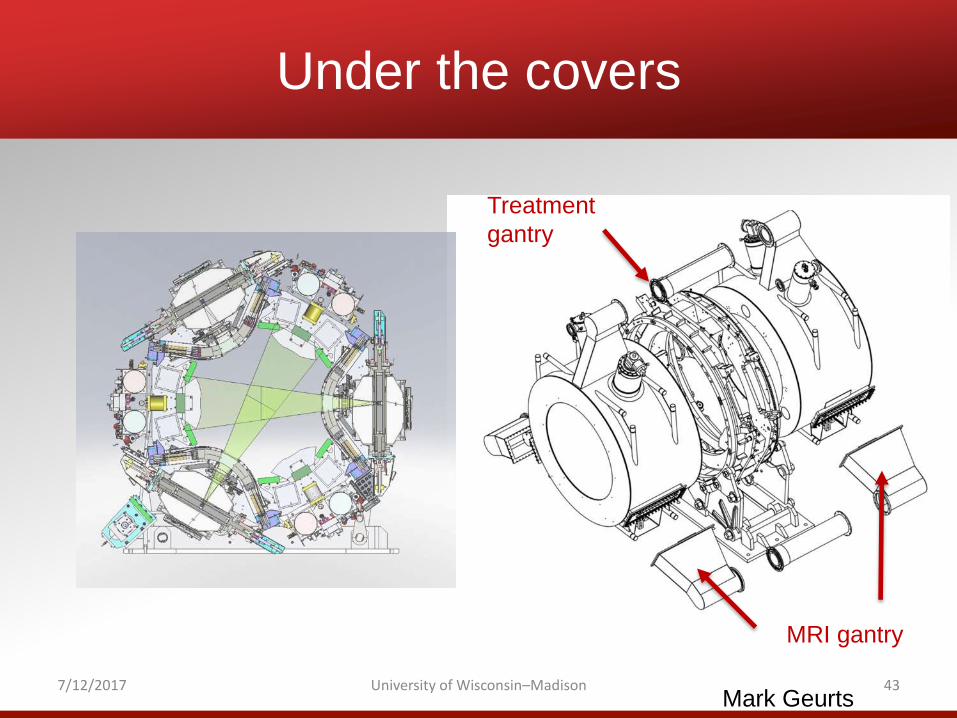
Under the covers
7/12/2017 University of Wisconsin–Madison 43
Treatment
gantry
MRI gantry
Mark Geurts
Comparison
Standard Daily Pretreatment imaging
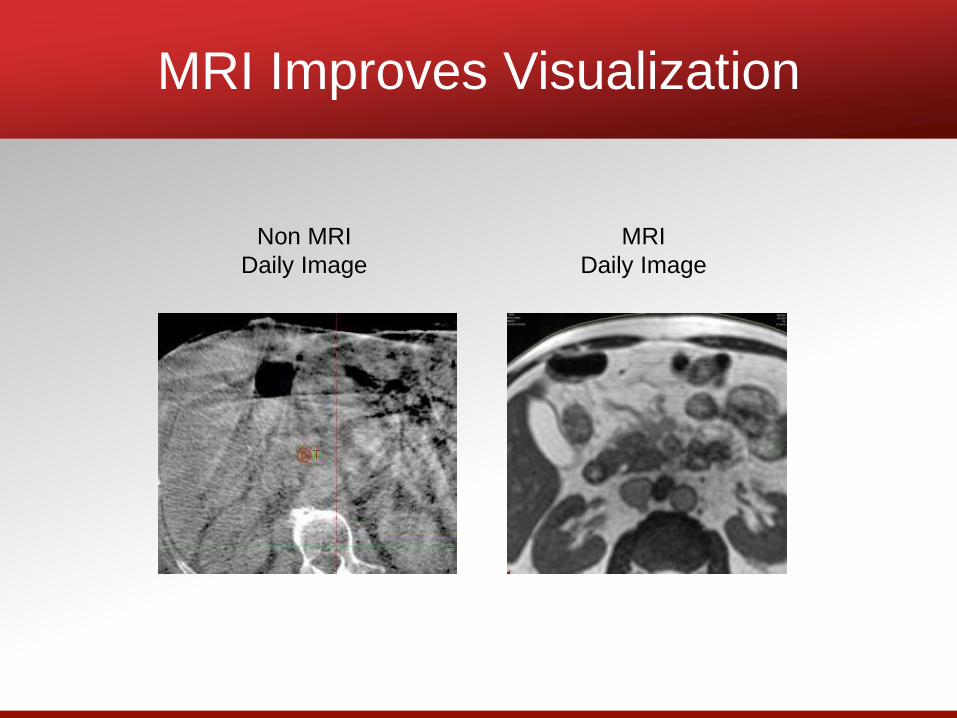
MRI Improves Visualization
Non MRI
Daily Image
MRI
Daily Image
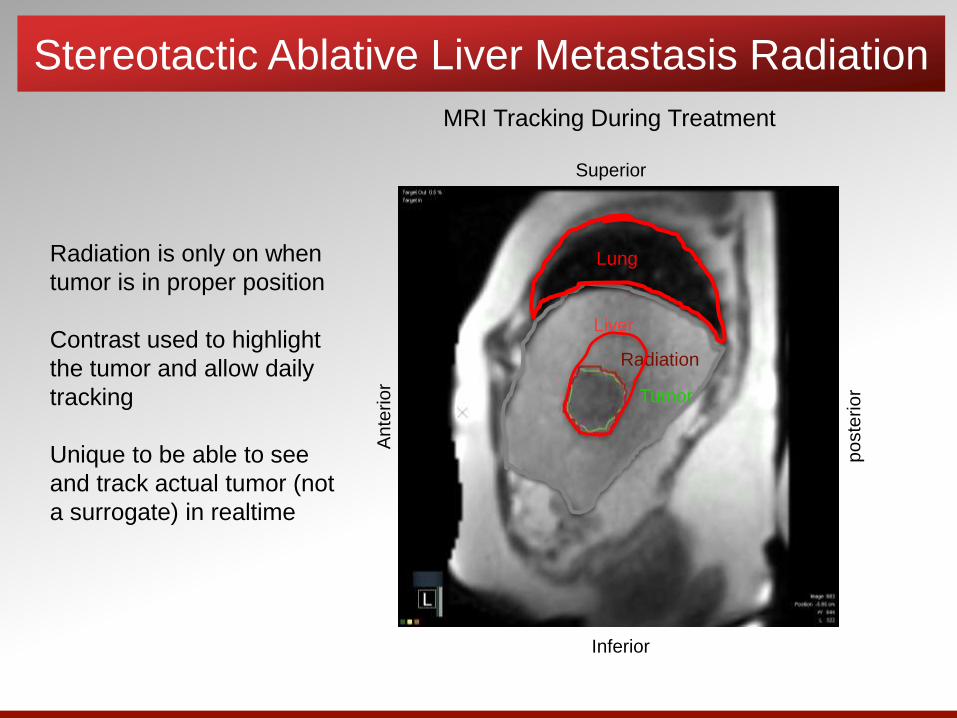
Stereotactic Ablative Liver Metastasis Radiation
Radiation is only on when
tumor is in proper position
Contrast used to highlight
the tumor and allow daily
tracking
Unique to be able to see
and track actual tumor (not
a surrogate) in realtime
MRI Tracking During Treatment
An
terio
r
po
ste
rio
r
Lung
Liver
Radiation
Tumor
Superior
Inferior
Summary
• Advantages of MRI Guided Radiation
• Soft Tissue Resolution• Improved alignment/targeting
• Confidence using high dose near critical organs
• Motion management –Breath hold and Tracking
• Decreased normal tissue/increase tumor dose
• Improve image quality
• Intra-treatment Response Assessment
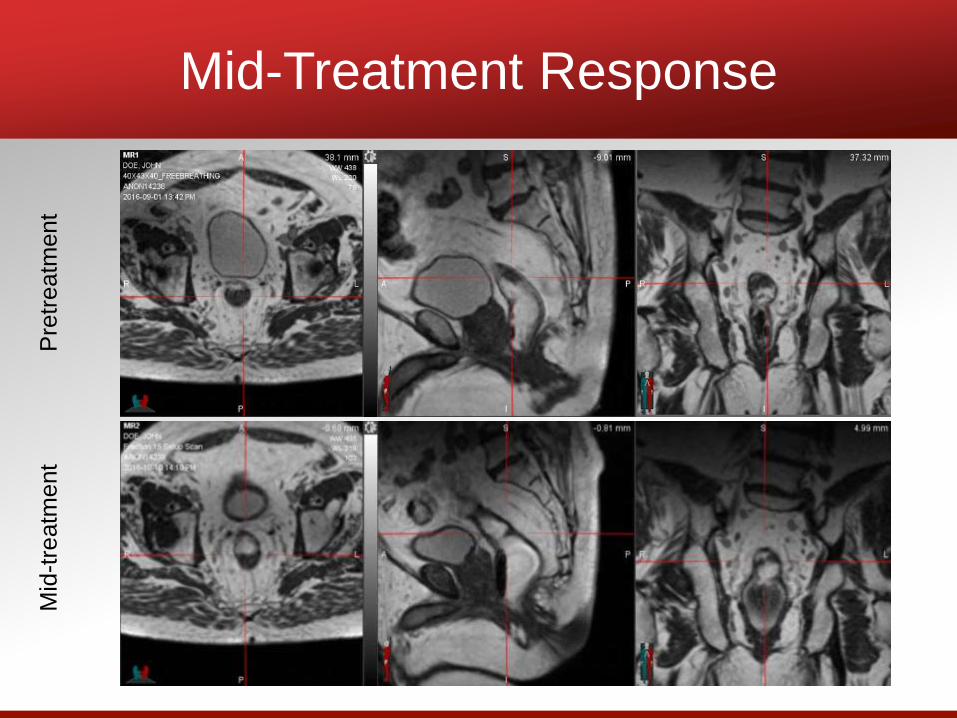
Mid-Treatment ResponseP
retr
eatm
ent
Mid
-tre
atm
ent
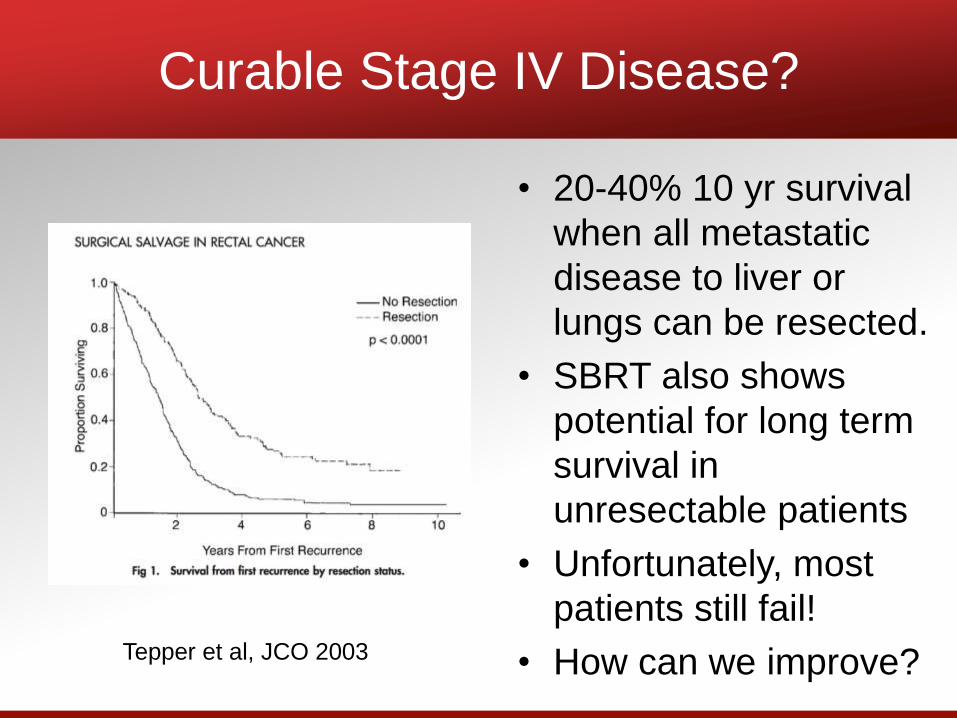
Curable Stage IV Disease?
• 20-40% 10 yr survival
when all metastatic
disease to liver or
lungs can be resected.
• SBRT also shows
potential for long term
survival in
unresectable patients
• Unfortunately, most
patients still fail!
• How can we improve?Tepper et al, JCO 2003
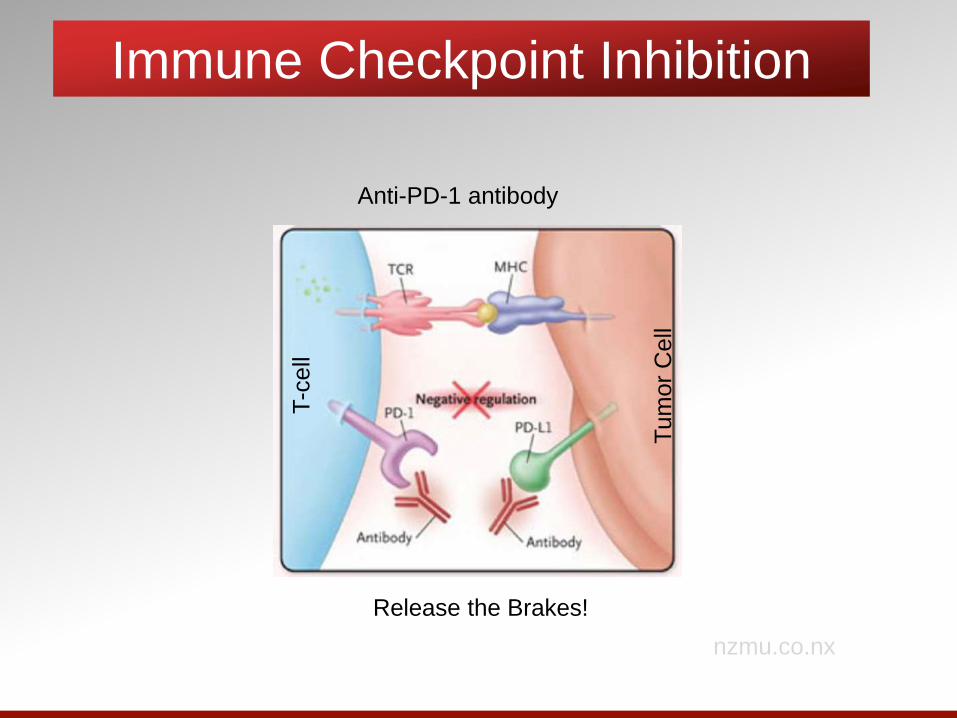
Immune Checkpoint Inhibition
nzmu.co.nx
Anti-PD-1 antibody
T-c
ell
Tum
or
Cell
Release the Brakes!
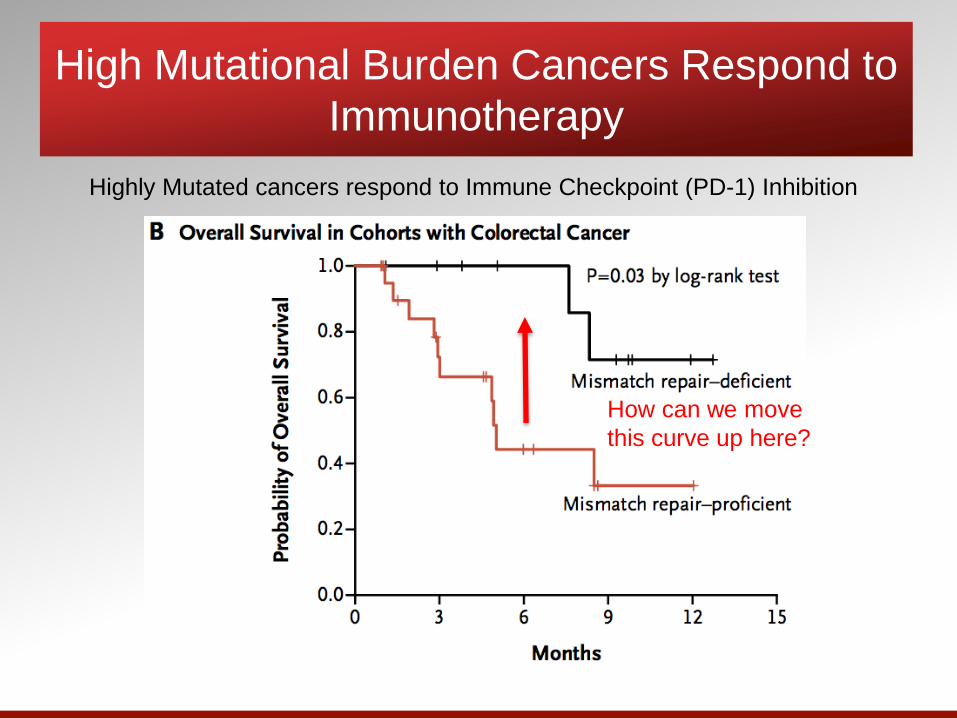
High Mutational Burden Cancers Respond to
Immunotherapy
Highly Mutated cancers respond to Immune Checkpoint (PD-1) Inhibition
How can we move
this curve up here?
Radiation Effects on Tumor
Microenvironment
• New Mutations Created
• New Antigens Expressed
• Dying Tumor Cells
• Release Antigens
• Pro-Inflammatory Cytokines
• Chemokines to attract immune cells
• Remove Immunosupressive Immune
Cells
• Macrophages, Regulatory T-cells
SBRT and immunotherapy in colorectal cancer
patients with liver confined metastasis and
completely resectable disease.
Dustin Deming MD
Michael Bassetti MD PhD
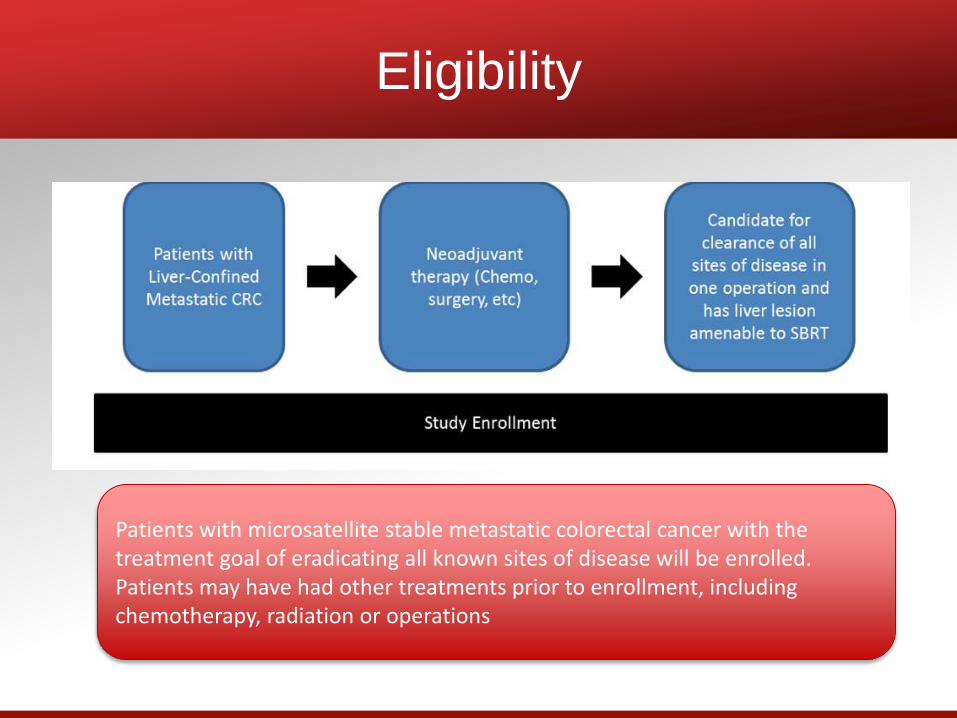
Eligibility
Patients with microsatellite stable metastatic colorectal cancer with the treatment goal of eradicating all known sites of disease will be enrolled. Patients may have had other treatments prior to enrollment, including chemotherapy, radiation or operations
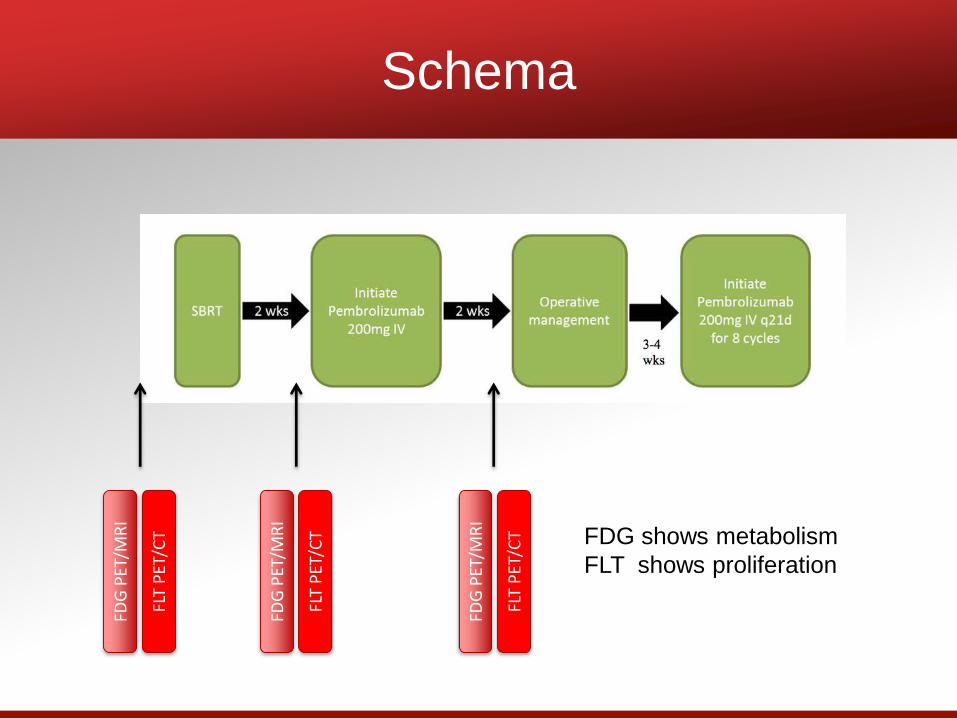
SchemaFD
G P
ET/M
RI
FLT
PET
/CT
FDG
PET
/MR
I
FLT
PET
/CT
FDG
PET
/MR
I
FLT
PET
/CT FDG shows metabolism
FLT shows proliferation
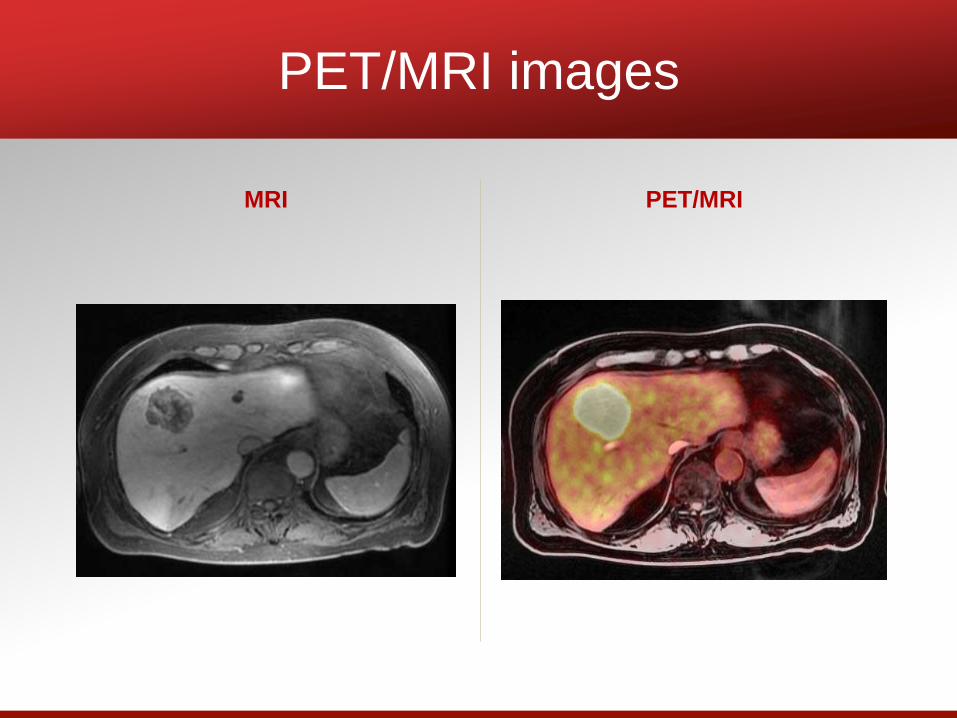
PET/MRI images
MRI PET/MRI
Conclusions
• Radiation can stimulate a T cell response
in colorectal tumors
• The trial is using this response with an
immune checkpoint inhibitor to attempt to
help the body recognize the CRC as
foreign and attack it.
• Surgery after SBRT to clear any remaining
metastasis and give immune therapy best
chance to work against remaining possible
microscopic cancer cells
Conclusions
• Radiation plays an important role in localized
rectal cancer management
• Stereotactic radiation is an effective, non-
invasive option for treatment of metastatic
lesions.
• MRI guided radiation allows accurate treatment
and easy assessment of intra-treatment
response for individually tailored radiation
therapy
• Immotherapy is very exciting, but currently
ineffective for the majority of CRC patients. We
are currently looking for ways to help the
immune system target CRC.
Thank You

Question & Answer:
SNAP A #STRONGARMSELFIE
Bayer HealthCare will donate $1 for every photo posted (up to $25,000).
Flex a “strong arm” & post it to Twitter or Instagram! (Use the hashtag!) #strongarmselfie

Contact Us!