quantitative corneal endothelial evaluation in intraocular lens implantation and cataract surgery
TRANSCRIPT
QUANTITATIVE CORNEAL ENDOTHELIAL EVALUATION IN
INTRAOCULAR LENS IMPLANTATION AND CATARACT SURGERY LAWRENCE W. HIRST, M.D., ROBERT C. SNIP, M.D.,
WALTER J. STARK, M.D., AND A. EDWARD MAUMENEE, M.D. Baltimore, Maryland
In 1968, Maurice1 described the specular microscope for laboratory examination of the corneal endothelium. Laing, Sand-strom, and Leibowitz,2 and Bourne, Mc-Carey, and Kaufman3 recently modified this system for human in vivo endothelial cell evaluation. Reports4-6 have subsequently been published, quantitating endothelial cell loss after various intraocular procedures. Average endothelial cell loss after routine cataract extraction has been reported as 8%4 to 12%,s and the average cell density loss after intraocular lens implantation varies from 28%4 to 62%.6 Reports to date have been limited by small patient numbers, differing intraocular lens types, different surgical techniques, and a wide spectrum of patient selection criteria.
We have reported a prospective study of the first 100 intraocular lens implants performed during a two-year trial period here.7 Of these, 33 patients were examined with the Syber clinical specular microscope before and after surgery, and the change in endothelial cell densities was calculated. During the same period, 26 patients who had had routine cataract extraction were similarly observed. The present paper reports the quantitative endothelial changes, as obtained with the clinical specular microscope, in these patients.
From the Wilmer Ophthalmological Institute, Johns Hopkins Hospital, Baltimore, Maryland. This work was supported in part by National Eye Institute, grant EY01302 (Dr. Stark).
Reprint requests to Walter J. Stark, M.D., Wilmer Institute, Johns Hopkins Hospital, 601 N. Broadway, Baltimore, MD 21205.
SUBJECTS AND METHODS
For intraocular lens implantation, patients were considered suitable candidates only if careful slit-lamp examination disclosed no evidence of corneal pathology. Corneal endothelial diseases such as cornea guttata were considered a contraindication for lens implantation. The patients scheduled for lens insertion were operated on by two surgeons (W.J.S. or A.E.M.) using the same surgical technique and the same intraocular lens, the Binkhorst iris-clip lens (Fig. 1). Of the first 100 intraocular lens patients, we studied 33 for endothelial cell density changes by clinical specular photomicroscopy. During the same period, 26 patients scheduled for routine cataract extraction, who demonstrated no preoperative corneal endothelial disease, were exam-
Fig. 1 (Hirst and associates). Binkhorst iris-clip lens, two weeks postoperatively.
775
776 AMERICAN JOURNAL OF OPHTHALMOLOGY DECEMBER, 1977
ined by the same observers using the clinical specular microscope. Additionally, eight patients who had already had the Binkhorst iris-clip lens implanted by one of the two aforementioned surgeons were assessed retrospectively for endothelial cell density changes by a comparison of the endothelium of the operated eye with that of the unoperated phakic eye.
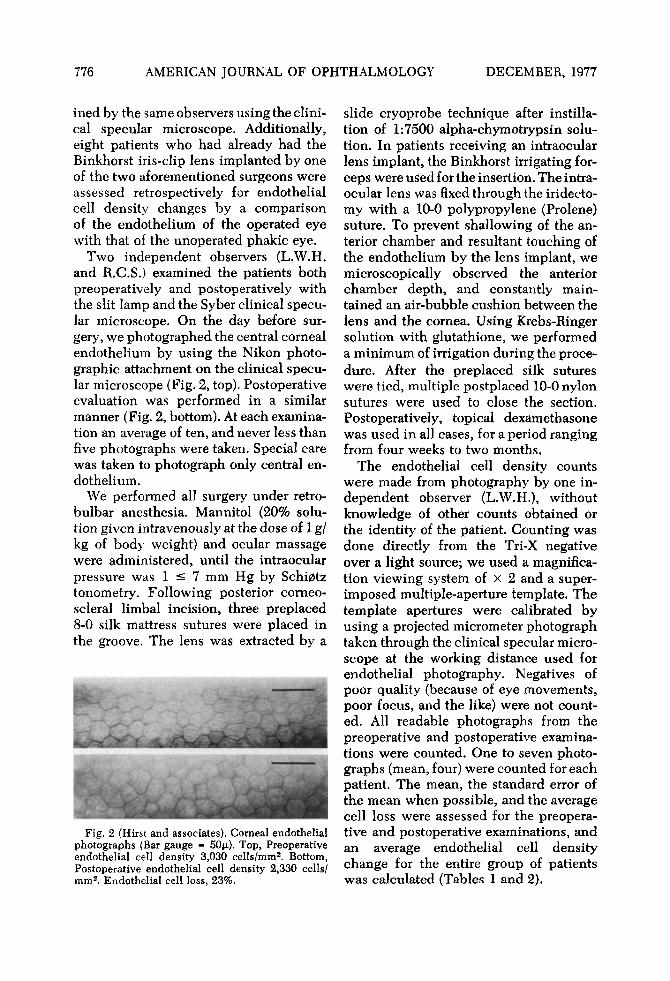
Two independent observers (L.W.H. and R.C.S.) examined the patients both preoperatively and postoperatively with the slit lamp and the Syber clinical specular microscope. On the day before surgery, we photographed the central corneal endothelium by using the Nikon photographic attachment on the clinical specular microscope (Fig. 2, top). Postoperative evaluation was performed in a similar manner (Fig. 2, bottom). At each examination an average of ten, and never less than five photographs were taken. Special care was taken to photograph only central endothelium.
We performed all surgery under retro-bulbar anesthesia. Mannitol (20% solution given intravenously at the dose of 1 g/ kg of body weight) and ocular massage were administered, until the intraocular pressure was 1 £ 7 mm Hg by Schi0tz tonometry. Following posterior corneo-scleral limbal incision, three preplaced 8-0 silk mattress sutures were placed in the groove. The lens was extracted by a
Fig. 2 (Hirst and associates). Corneal endothelial photographs (Bar gauge = 50μ). Top, Preoperative endothelial cell density 3,030 cells/mm2. Bottom, Postoperative endothelial cell density 2,330 cells/ mm2. Endothelial cell loss, 23%.
slide cryoprobe technique after instillation of 1:7500 alpha-chymotrypsin solution. In patients receiving an intraocular lens implant, the Binkhorst irrigating forceps were used for the insertion. The intraocular lens was fixed through the iridecto-my with a 10-0 polypropylene (Prolene) suture. To prevent shallowing of the anterior chamber and resultant touching of the endothelium by the lens implant, we microscopically observed the anterior chamber depth, and constantly maintained an air-bubble cushion between the lens and the cornea. Using Krebs-Ringer solution with glutathione, we performed a minimum of irrigation during the procedure. After the preplaced silk sutures were tied, multiple postplaced 10-0 nylon sutures were used to close the section. Postoperatively, topical dexamethasone was used in all cases, for a period ranging from four weeks to two months.
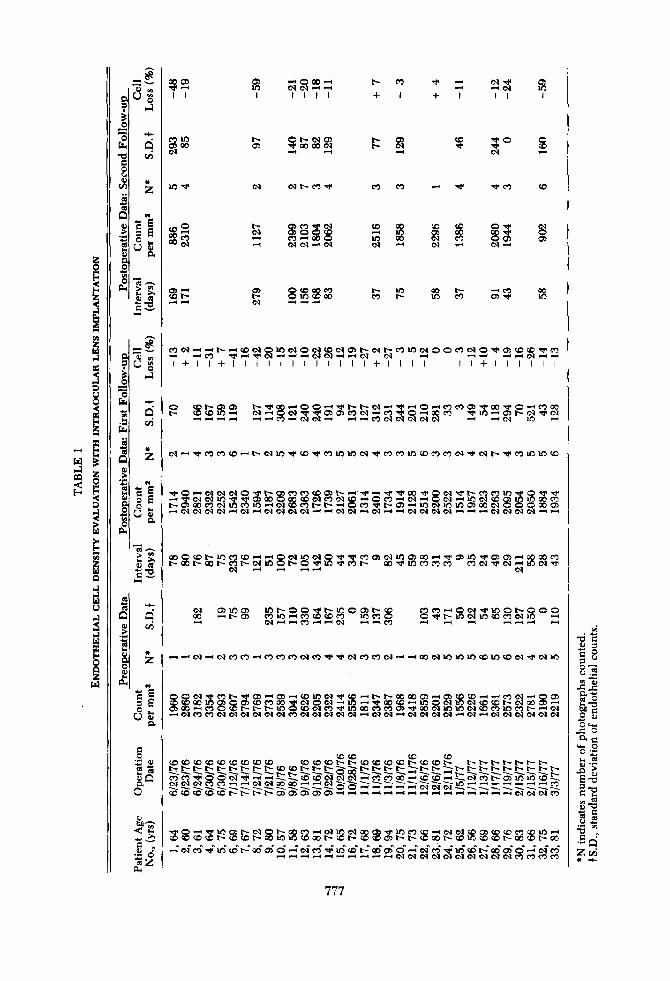
The endothelial cell density counts were made from photography by one independent observer (L.W.H.), without knowledge of other counts obtained or the identity of the patient. Counting was done directly from the Tri-X negative over a light source; we used a magnification viewing system of X 2 and a superimposed multiple-aperture template. The template apertures were calibrated by using a projected micrometer photograph taken through the clinical specular microscope at the working distance used for endothelial photography. Negatives of poor quality (because of eye movements, poor focus, and the like) were not counted. All readable photographs from the preoperative and postoperative examinations were counted. One to seven photographs (mean, four) were counted for each patient. The mean, the standard error of the mean when possible, and the average cell loss were assessed for the preoperative and postoperative examinations, and an average endothelial cell density change for the entire group of patients was calculated (Tables 1 and 2).
ί I I
Β S I
"o
II (0 vs U §
if Ü «
II q CO
E S
l! B O
o
P
0 0 05
I I
«5 w 05 00 CM
<2 in -» o ce -H CM <M - H » * I 1 I I + I + I I I
I > OS
O t - N O S ■* 00 00 CM <-H ~H
t -r-
05 <M
*̂ CO ■ »
Tf 0 ■V CM
05 W
S
S2 ss C t H CO t -
CM
OS
CSI
O Q CD (M CM -H ( N
8 CD 00 CO i n co 00
2 S i n ao CM " H
t ~ 10 t o t~-
cc CO 95 00 <M CO CM Ή
00 in
o ·» S3? (M —1
—' co <35 i ·
05
S
n M M H N H i O M O i o w o i M c o i M o i t - i s t - n i n w o o n c s i O ' i ' o x e e * « ~H »-HC0 ^ H ^ N - H ^ H H O Î W H P - I C S ! (M ~H -H .^ -I Mei H ^ H l + ll + l l l l l l l l l l l l + l l l l ll + l l l l l l
© $£<?05 t ~ . T ) < o o - H O O - ^ - * i ~ t ~ e M - ^ ' * ' - i o » - < c o c o o 5 - * o o - < j i o - < « c i o CM —1 © CM ■Ί· ■ * 05 05 CO <N —1 CO ■* O >-l 00 CO - * l f t — i OS t ~ CM ·9< <M _ _< ^-, _ H M O - « « O I r t — H * H C 0 < N O l < M < N e M - 4 1-1 CM
< M i - c ' q > c o r e c D - 4 t - < M i n - ^ ' c D - * c o i n i n i N r f c o c o i n c o c o c o < M - < * < M t ~ ' < j i c o i n i n c o
^ © ^ « Γ Μ Ο ί © ^ ^ Ο 5 « Ο < Ο « θ σ 5 ί ^ " Η · < ι < Μ · « < · ^ > 0 0 - * © £ Μ · < ) ' 1 - - Γ 0 Γ 0 ΐ η ' * © ' < Ϊ - > Ϊ ι
^ 3 c q « i n ^ » f c » » © o o c o c M r e c N ç p « © r e ^ c M « Q c M ^ i n c M « D œ i f t i n o o c o t ^ c * c c r e e q i n r e i n ^ e q « c r e t - t ~ - - H © c o ' ^ ' t - - 0 5 - H i n c N i n i n o 5 o o c M © © Q œ o 5 ^ C M C M e a c M ^ C M i ^ o q c < e < C M ' ^ - H < N t M « C i " ' - ^ C M < M C M e > l ^ < - H ' - i C M t M e M C M ' ^ ' - i
oo©cot-mcocD-4—ipcMin<M©'^'^|reo5CMW05oO'-i'^i05in'^'050>—«»opre t- 00 t- ce t- co r~ CM in © t- © ■* in ■* co t- 00 ·* in re co co re eq ·* CM -* in 59 ·* CM - 4 - H - H —1 <M
05 in 05 rt t - 05 i n r ~ © © " - f t - i n © o s c ~ ç p co i n - H co ce co re m e o © CJ ~H -H CO *■* - * <M ^ I r t C O
ç o c o — < © c M ' ^ > i n © t - © © © ©-<f t^ in c i m co co CM in -H
rt^ei^c^rere--<cococo<NcO'i'-*cMcocoei-^-4CiocMinioiocoincoc^-*cMio
8 © o i ^ r e i > ^ 0 5 ^ œ « c o w e M T r c p - H t - - i " - c o a o o 5 - H 0 5 c e c o - H > - - i c D c c i n ç » © c * c o r e c o 5 c v i © M ^ i n ^ ^ c o œ < - 4 i n © < M i n c N i c o c D œ o o ^ r e © c e t - t ^ t - i n © c D c M r e T p i n c « 5 r e « c S ^ c o ( M i n i o c M c B c o rtC«rorec*eqcicM«MtMco«McieMcMCM-4<sie>i-«cicM<Me>i.-4<N-*oj
CD-Hi—I CO CM -* © OS -' — — t- cM 00 05 H i nnt-rti» CM CM <M CM CM
CD CD CO CO COCDCOCOCOCOCDCOCO c O C O C D C ~ t - * C O C O C O C O r ~ C D C O t - - t ~ t ^ t - t ~ I s - l— t—
c o ~ r e ^ © " © c 7 ^ ^ ^ t t ^ S e M c q c j ^ c o " c o ~ c ? r t c o c c « t c M ~ c o " F ^ » i n Ä c o " f c £ ïS Σ ï w . r o - " ï * i o i lS iS 0 .SP .C l c ÎS i©~©*^ ï ^H" — ^ ^ o a e J o q i G ^ C l ^ C l ^ l c i d i J c B ' c o c o c o S P ï ^ î ^ t - œ œ œ œ o s r t ^ r t r t r f r t r t r t r t ^ S r t r t r t S c î c M c î c o
S c 5 ^ ^ i n o i t - c M © i ^ o o r e ^ c M i n c M c c c » T r i n r e c o « e M e M c o o 5 C D c o c o c o i n ' - i c o c D c e t ^ c D c o t ^ c o i n i n c o c n t ~ c o t - c D c e c » t ^ ^ c o c e t ^ c o i n c o c e t ^ o o c o t ^ o o -*" CM* co" ■*" in co" t-" 00" os" ©" —" c i re" ·*·" 10 CD" t-" ao" os" ©* -«" c i co* ■* in co" t-" 00" os ©* —î c i co"
Ή - < — i - 4 - < — i « - < ^ ~ H C M < N < M < N C M C M C M < N < N C M C 0 C O r e c O
777
778 AMERICAN JOURNAL OF OPHTHALMOLOGY DECEMBER, 1977
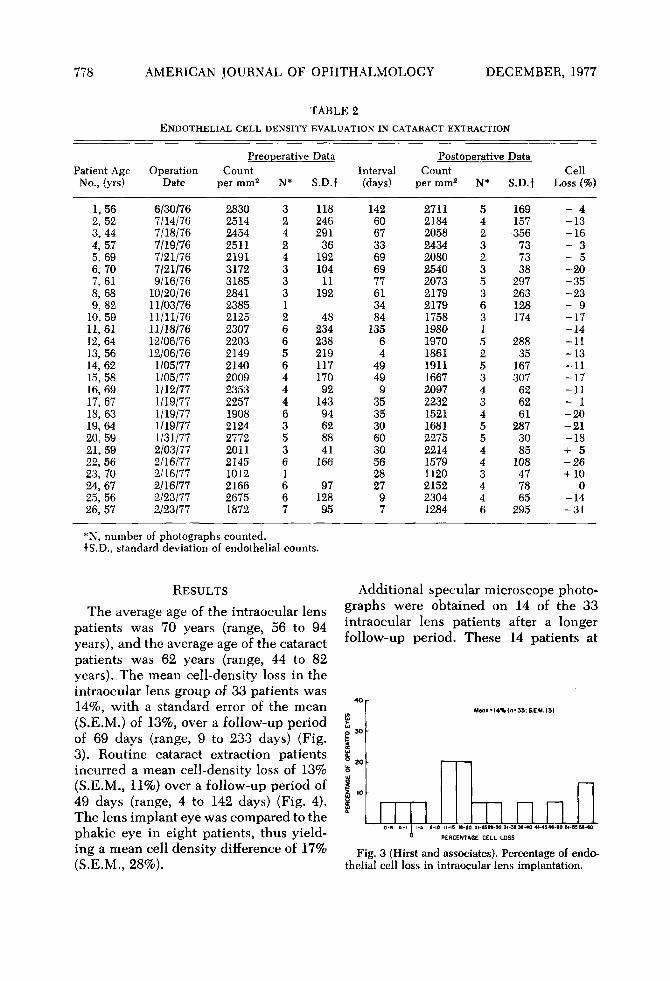
TABLE 2 ENDOTHELIAL CELL DENSITY EVALUATION IN CATARACT EXTRACTION
Patient Age No., (yrs)
1,56 2,52 3,44 4,57 5,69 6,70 7,61 8,68 9,82
10,59 11,61 12,64 13,56 14,62 15,58 16,69 17,67 18,63 19,64 20,59 21,59 22,56 23,70 24,67 25,56 26,57
Operation Date
6/30/76 7/14/76 7/18/76 7/19/76 7/21/76 7/21/76 9/16/76
10/20/76 11/03/76 11/11/76 11/18/76 12/06/76 12/06/76 1/05/77 1/05/77 1/12/77 1/19/77 1/19/77 1/19/77 1/31/77 2/03/77 2/16/77 2/16/77 2/16/77 2/23/77 2/23/77
Preoperative Count
per mm2
2830 2514 2454 2511 2191 3172 3185 2841 2385 2125 2307 2203 2149 2140 2009 2353 2257 1908 2124 2772 2011 2145 1012 2166 2675 1872
N*
3 2 4 2 4 3 3 3 1 2 6 6 5 6 4 4 4 6 3 5 3 6 1 6 6 7
Data
S.D.!
118 246 291
36 192 104
11 192
48 234 238 219 117 170 92
143 94 62 88 41
166
97 128 95
Interval (days)
142 60 67 33 69 69 77 61 34 84
135 6 4
49 49 9
35 35 30 60 30 56 28 27
9 7
Postoperative Count
per mm2
2711 2184 2058 2434 2080 2540 2073 2179 2179 1758 1980 1970 1861 1911 1667 2097 2232 1521 1681 2275 2214 1579 1120 2152 2304 1284
N*
5 4 2 3 2 3 5 3 6 3 1 5 2 5 3 4 3 4 5 5 4 4 3 4 4 6
Data
S.D.f
169 157 356 73 73 38
297 263 128 174
288 35
167 307 62 62 61
287 30 85
108 47 78 65
295
Cell Loss (%)
- 4 -13 -16 - 3 - 5 -20 -35 -23 - 9 -17 -14 -11 -13 -11 -17 -11 - 1 -20 - 2 1 -18 + 5 - 2 6 + 10
0 -14 - 3 1
*N, number of photographs counted. f S.D., standard deviation of endothelial counts.
RESULTS
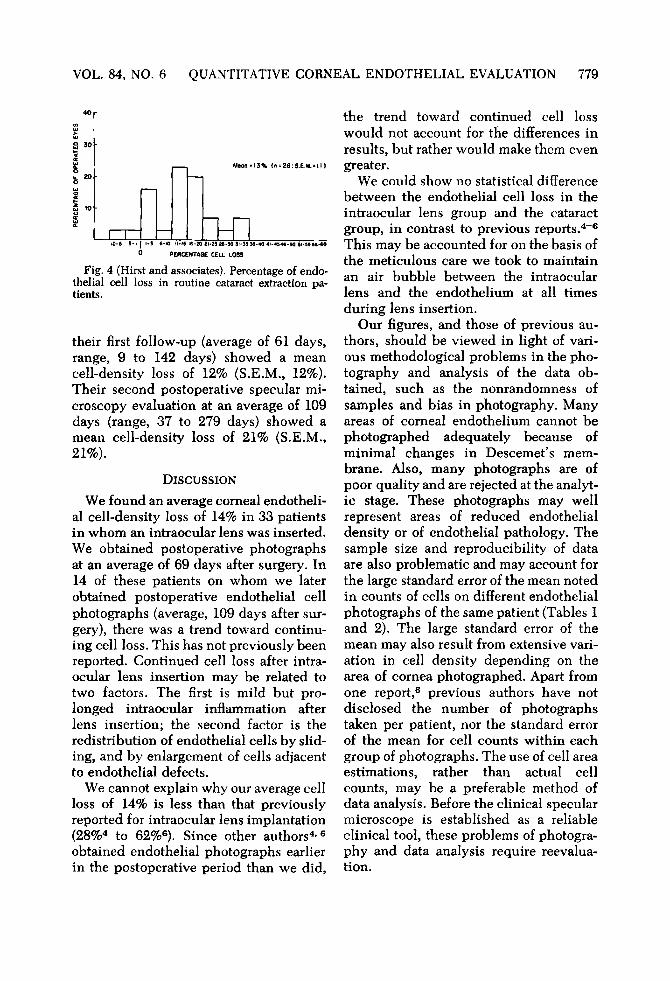
The average age of the intraocular lens patients was 70 years (range, 56 to 94 years), and the average age of the cataract patients was 62 years (range, 44 to 82 years). The mean cell-density loss in the intraocular lens group of 33 patients was 14%, with a standard error of the mean (S.E.M.) of 13%, over a follow-up period of 69 days (range, 9 to 233 days) (Fig. 3). Routine cataract extraction patients incurred a mean cell-density loss of 13% (S.E.M., 11%) over a follow-up period of 49 days (range, 4 to 142 days) (Fig. 4). The lens implant eye was compared to the phakic eye in eight patients, thus yielding a mean cell density difference of 17% (S.E.M., 28%).
Additional specular microscope photographs were obtained on 14 of the 33 intraocular lens patients after a longer follow-up period. These 14 patients at
Meoil'l4%ln = 33:S.E.M.I3)
10-6 9-1 l-S β'ΙΟ 1MB Ιβ-ÎO II-25M-30 31-55 38-40 41-45 « - 8 0 81-53 35-80 0 PERCENTi.CE CELL LOSS
Fig. 3 (Hirst and associates). Percentage of endothelial cell loss in intraocular lens implantation.
VOL. 84, NO. 6 QUANTITATIVE CORNEAL ENDOTHELIAL EVALUATION 779
Mran-13% <n<26:S.E.M.>ll)
cm 1-5 6-10 M-IS I 8 - » ΙΊ·23 2β-5θ 31-39 S6-40 4I-454C-90 »Ι-3336-CO
0 PERCENTAGE CELL LOSS
Fig. 4 (Hirst and associates). Percentage of endothelial cell loss in routine cataract extraction patients.
their first follow-up (average of 61 days, range, 9 to 142 days) showed a mean cell-density loss of 12% (S.E.M., 12%). Their second postoperative specular microscopy evaluation at an average of 109 days (range, 37 to 279 days) showed a mean cell-density loss of 2 1 % (S.E.M., 21%).
DISCUSSION
We found an average corneal endothelial cell-density loss of 14% in 33 patients in whom an intraocular lens was inserted. We obtained postoperative photographs at an average of 69 days after surgery. In 14 of these patients on whom we later obtained postoperative endothelial cell photographs (average, 109 days after surgery), there was a trend toward continuing cell loss. This has not previously been reported. Continued cell loss after intraocular lens insertion may be related to two factors. The first is mild but prolonged intraocular inflammation after lens insertion; the second factor is the redistribution of endothelial cells by sliding, and by enlargement of cells adjacent to endothelial defects.
We cannot explain why our average cell loss of 14% is less than that previously reported for intraocular lens implantation (28%4 to 62%e). Since other authors4·6
obtained endothelial photographs earlier in the postoperative period than we did,
the trend toward continued cell loss would not account for the differences in results, but rather would make them even greater.
We could show no statistical difference between the endothelial cell loss in the intraocular lens group and the cataract group, in contrast to previous reports.4 - 6
This may be accounted for on the basis of the meticulous care we took to maintain an air bubble between the intraocular lens and the endothelium at all times during lens insertion.
Our figures, and those of previous authors, should be viewed in light of various methodological problems in the photography and analysis of the data obtained, such as the nonrandomness of samples and bias in photography. Many areas of corneal endothelium cannot be photographed adequately because of minimal changes in Descemet's membrane. Also, many photographs are of poor quality and are rejected at the analytic stage. These photographs may well represent areas of reduced endothelial density or of endothelial pathology. The sample size and reproducibility of data are also problematic and may account for the large standard error of the mean noted in counts of cells on different endothelial photographs of the same patient (Tables 1 and 2). The large standard error of the mean may also result from extensive variation in cell density depending on the area of cornea photographed. Apart from one report,6 previous authors have not disclosed the number of photographs taken per patient, nor the standard error of the mean for cell counts within each group of photographs. The use of cell area estimations, rather than actual cell counts, may be a preferable method of data analysis. Before the clinical specular microscope is established as a reliable clinical tool, these problems of photography and data analysis require réévaluation.

780 AMERICAN JOURNAL OF OPHTHALMOLOGY DECEMBER, 1977
SUMMARY
We analyzed pre- and postoperative corneal endothelial photographs of 33 intraocular lens patients and found an average endothelial cell density loss of 14%. Twenty-six cataract patients, similarly examined, showed a 13% mean endothelial cell loss. In 14 of the intraocular lens patients, a second postoperative evaluation of the central endothelium, at a later date, revealed a trend toward continuing cell loss. Our results indicate fewer endothelial cells were lost after intraocular lens implantation than has been previously reported. This may be accounted for by our considering only patients with normal corneas for lens implantation, and by our constant maintenance of the anterior chamber with an air bubble during lens implant surgery.
REFERENCES 1. Maurice, D. M.: Cellular membrane activities
in the corneal endothelium of the intact eye. Experi-entia 24:1094, 1968.
2. Laing, R. A., Sandstrom, M. M., and Leibowitz, H. M.: In vivo photomicrography of the corneal endothelium. Arch. Ophthalmol. 93:143, 1975.
3. Bourne, W. M., McCarey, B. E., and Kaufman, H. E.: Clinical specular microscopy. Trans. Am. Acad. Ophthalmol. Otokryngol. 81:743, 1976.
4. Forstot, S. L., Blackwell, W. L., Jaffe, N. S., and Kaufman, H. E.; The effect of intraocular lens implantation on the corneal endothelium. Trans. Am. Acad. Ophthalmol. Otolaryngol. 83:195, 1977.
5. Bourne, W. M., and Kaufman, H. E.: Cataract extraction and the corneal endothelium. Am. J. Ophthalmol. 82:44, 1976.
6. : Endothelial damage associated with intraocular lenses. Am. J. Ophthalmol. 81:482,1976.
7. Stark, W. J., Hirst, L. W., Snip, R. C, and Maumenee, A. E.: A two-year trial of intraocular lenses at the Wilmer Institute. Am. J. Ophthalmol. Am. J. Ophthalmol. 84:769, 1977.