pulmonary thromboembolism specific situations
DESCRIPTION
Pulmonary thromboembolism specific situations. Dr.E.Shabani. Symptom. Dyspnea 73 percent Pleuritic chest pain 66 percent Cough 37 percent Hemoptysis 13 percent. Signs. - PowerPoint PPT PresentationTRANSCRIPT

PULMONARY THROMBOEMBOLISM SPECIFIC SITUATIONS
Dr.E.Shabani
SYMPTOM
Dyspnea 73 percent Pleuritic chest pain 66 percent Cough 37 percent Hemoptysis 13 percent
SIGNS
Tachypnea 70 percent Rales 51
percent Tachycardia 30 percent Fourth heart sound 24 percent Accentuated pulmonic component of second heart sound 23 percent Circulatory collapse 8 percent

CLASSIC RISK FACTORS AND PHYSIOLOGIC FINDINGS FOR PULMONARY EMBOLISM
Surgery within previous 4 wk requiring general anesthesia
Unilateral leg or arm swelling Trauma within previous 4 wk requiring
hospitalization Hemoptysis Pulse rate >100 beats/min Pulse oximetry reading <95%
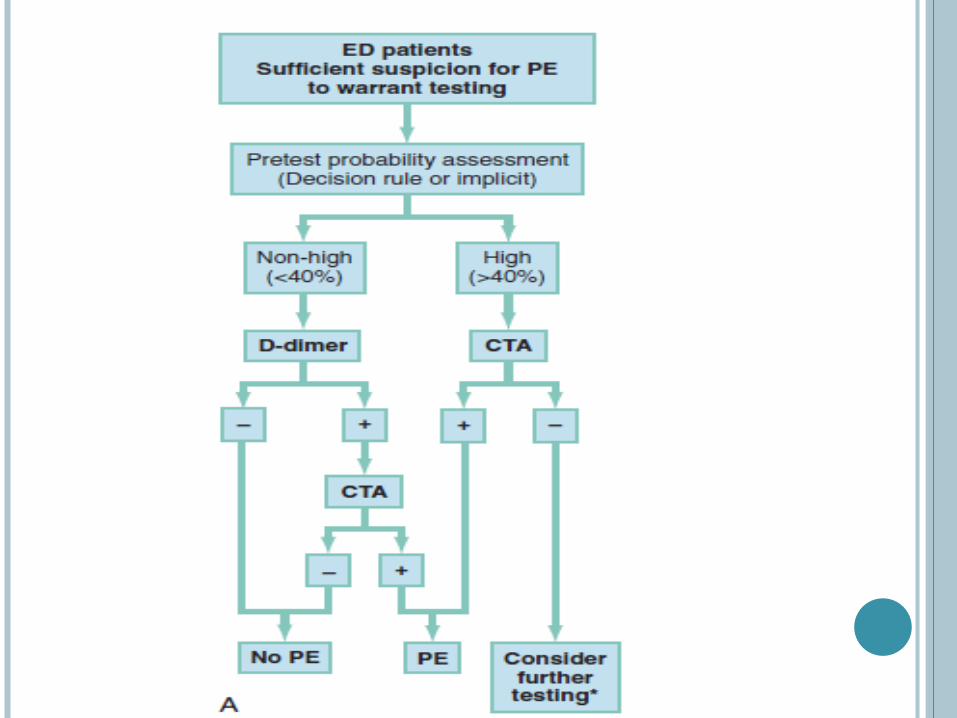
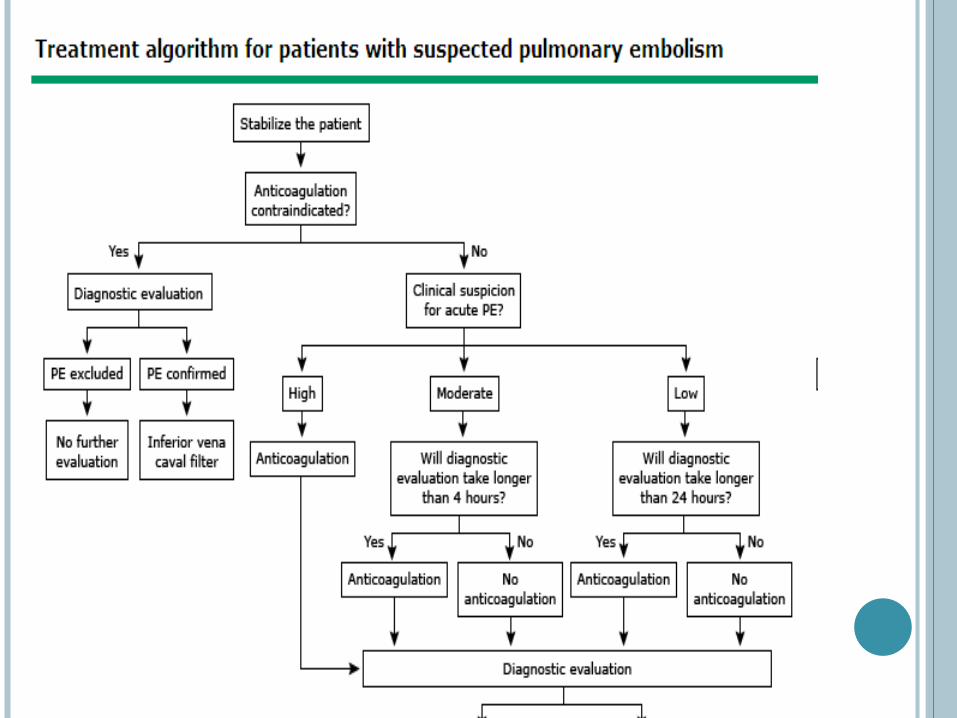
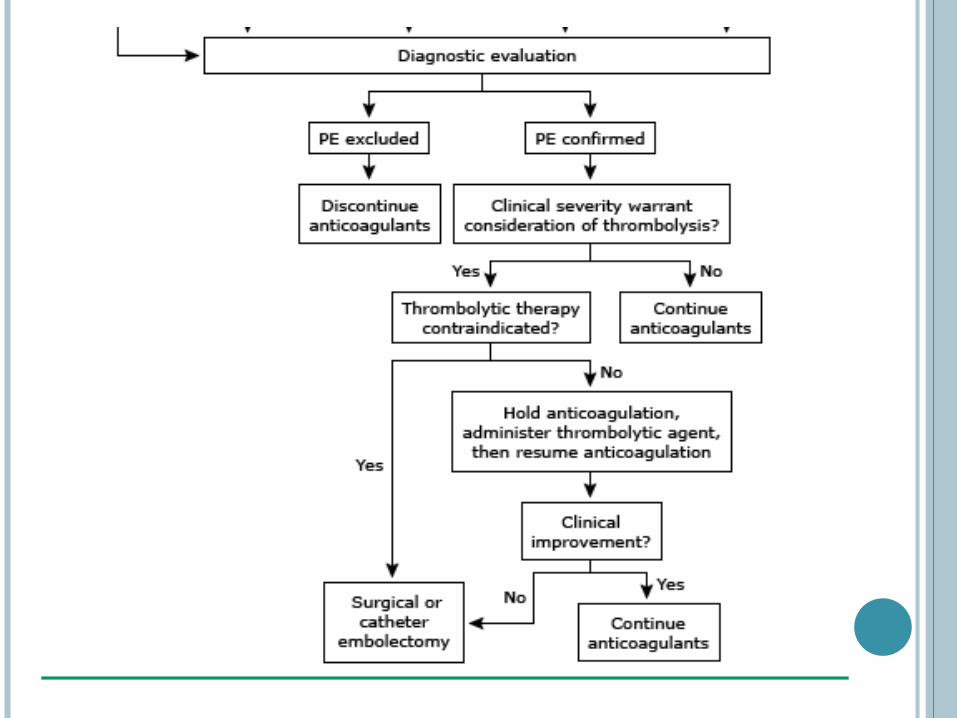
DIAGNOSIS
CXR :
useful to suggest alternative diagnoses Unilateral basilar atelectasis Hampton’s hump Unilateral lung oligemia (Westermark’s sign)
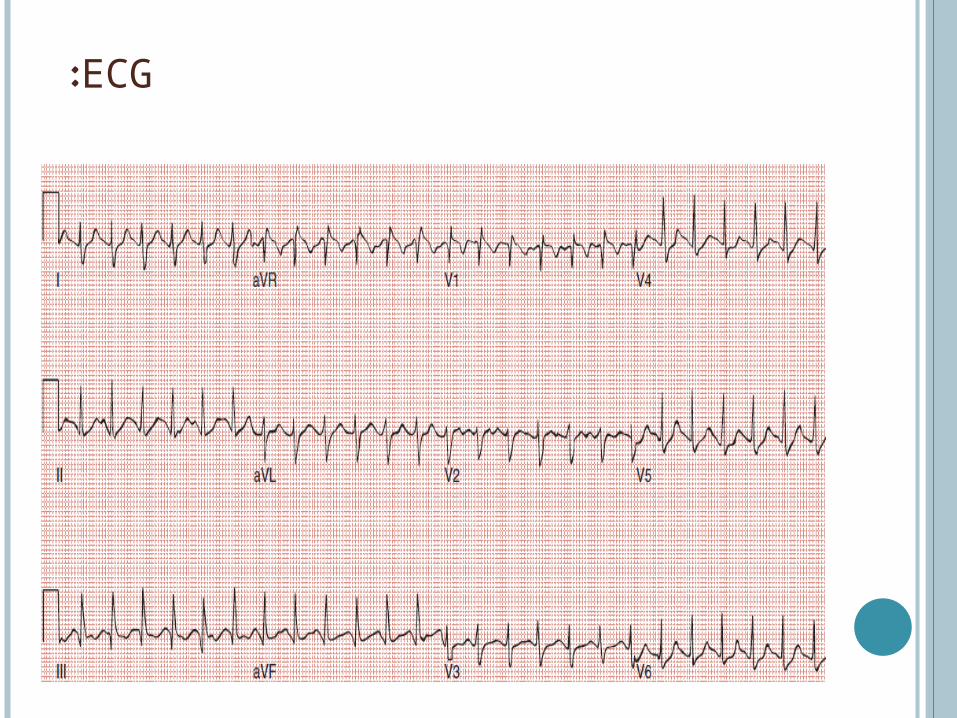
ECG:

WELLS CRITERIA
Clinical symptoms of DVT (leg swelling, pain with palpation) 3.0
Other diagnosis less likely than pulmonary embolism 3.0
Heart rate >100 1.5 Immobilization (≥3 days) or surgery in the
previous four weeks 1.5 Previous DVT/PE 1.5 Hemoptysis 1.0 Malignancy 1.0



WHEN WE DO NOT HAVE ACCESS TO IMAGING
A 50 years old smoker woman with previous DVT come to ED complaining of dyspnea she has edema on one of her legs and is also tachycardic and hypoxic
what SHOULD we do?

Start anticoagulant, (If the patient has no contraindication).

RULING OUT PULMONARY EMBOLISM IN PREGNANT PATIENTS
A 25 years old pregnant woman comes to ED complaining of dyspnea, she is tachycardic and hypoxic, she is not febrile has no respiratory tract infection lungs auscultation appears normal.

Pregnancy is associated with both PTE and also predictable elevated D-dimer even in the absence of PTE.
Pulmonary V/Q scan is safe in pregnancy. Chest CT delivers less energy than that is
known as teratogenic threshold, but recent evidence suggest that even small amount of radiation to young brain is associated with subtle cognitive deficit later in life.

1: try to rule out PTE by D-dimer, if negative in low risk patients the diagnosis would be excluded.
2: as an additional margin of safety a negative venous doppler ultrasound can lower the probability by about half.
3: a normal V/Q scan rule out diagnosis. 4: a high probable V/Q scan establishes
diagnosis and heparin can be initiated. 5: if V/Q scan is neither diagnostic nor normal
then further imaging

EVALUATING OF OBESE PATIENT
A 48 y/o man comes to ED with dyspnea and PTE is suspected the patients weight is 180 kg! :-S
This weight is above the weight that our scanner can tolerate.

Venous ultrasound ,although suboptimal in obese patients, can occasionally provide positive evidence of DVT and clinch the diagnosis.
Another option is to initiate antcoagulant based on moderate to high pretest probability and a D-dimer which exceeds 1000 ng/ml.

SUSPECTED PTE IN A PATIENT ALREADY GETTING TREATMENT FOR PREVIOUS PTE
A 72 y/o man bedridden because of an lumbar vertebral injury for a while he had got PTE in the course of his treatment, and was on Warfarin after a while his dyspnea came back and one of the most probable diagnosis was PTE.
If INR is in therapeutic range (1.5-2.5), and the patient has normal V/S, is relatively comfortable, does not have had syncope, and has no changes suggestive of pulmonary HTN on EKG, follow up imaging is not needed. Other causes of chest pain must be considered and if no alternative diagnose is established symptom therapy with NSAIDs is safe and reasonable in patients complaining of chest pain

WHAT IF THE COMPLAINT IS IN DYSPNEA AT REST!!!??
Repeat pulmonary vascular imaging and echocardiography.
If the patient is symptomatic and there is evidence of unresolved filling defect or and pulmonary HTN, should be admitted to a program that offers pulmonary thrombectomy.