pulmonary function testing sandra b. weibel md thomas jefferson university
TRANSCRIPT
Pulmonary Function Testing
Sandra B. Weibel MD
Thomas Jefferson University
Indications
• Differential diagnosis of dyspnea
• Provides objective assessment of symptoms versus severity
• Determine fitness for surgery
• To guide therapy
• To follow the course of a disease

Physiologic classification of disease
• Obstructive Impairment- Airway limitation due to the resistive properties of the respiratory system
• Restrictive Impairment- Loss of volume capacity of the lung due to loss of air space units or inability to expand the respiratory system
Obstructive Processes
• L ocal obstruction
• A sthma
• C hronic bronchitis (COPD)
• E mphysema
Restrictive Processes
• P leural disease
• A lveolar filling processes
• I nterstial lung disease
• N euromuscular diseases
• T horacic cage abnormailites

Spirometry
• Most widely performed study and is important in initial screening of patients
• Easily and quickly performed in many settings

Types of spirometers
• Types include flow (pneumotach) or volume (water seal, rolling and diaphragm)
• Water seal device previoisly most commonly used in pulmonary function labs of the volume– Collect exhaled gas and act as a reservoir for
inhaled gas– Composed of a mouthpiece, bell system and a
pen on a rotating drum


Volume Displacement Spirometer

Flow Spirometry

Calibration of spirometer
• Warmed up and temperature controlled Barometric pressure and temperature recorded
• Volume calibration with 3L syringe (within 3%)
• Flow spirometer tested at 3 flow rates between 2 and 12L

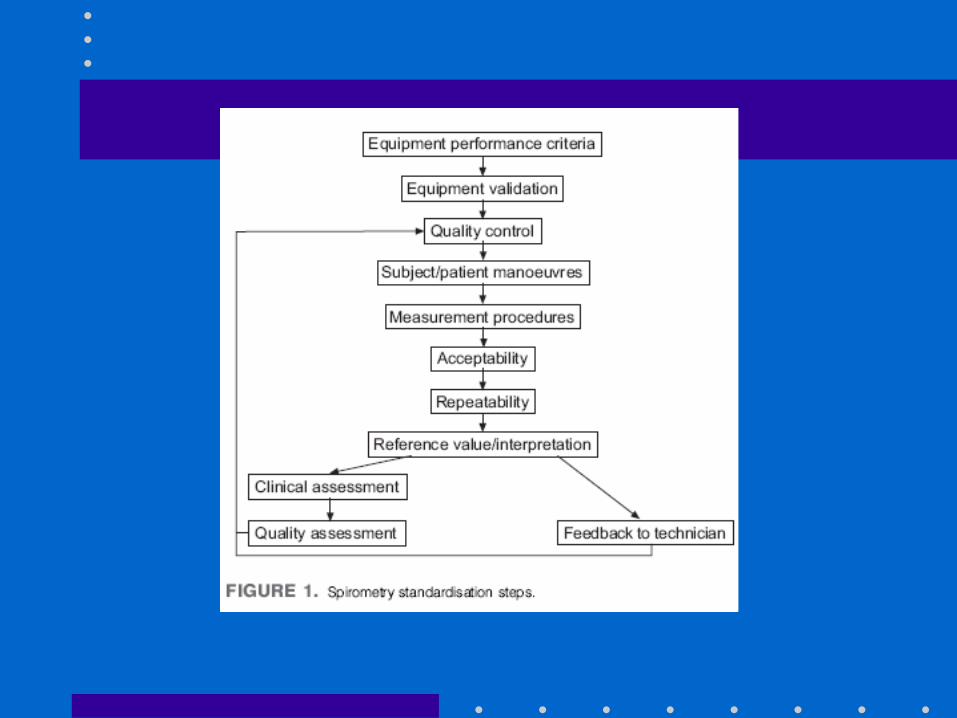
Quality Control
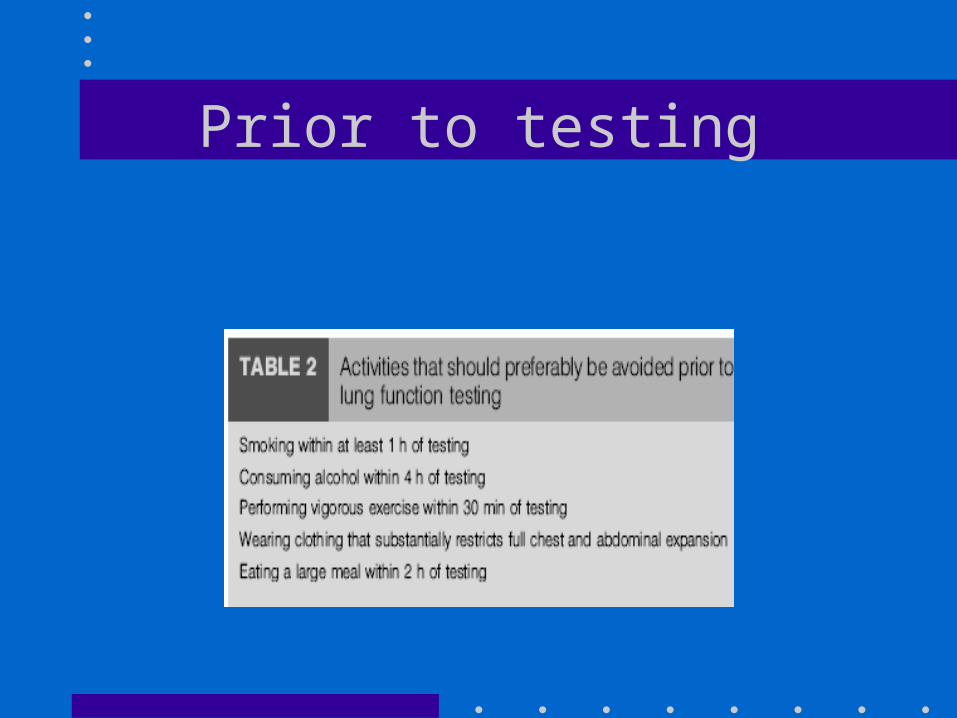
Prior to testing

Performing the maneuver
• It is a forced expiratory maneuver and the patient must be sitting upright in a chair with lips around a mouthpiece
• After a maximal inspiration, a forced and rapid expiration is made
• Quality of the maneuver needs to be assessed noting that the patient started at zero, had a maximal initial efffort and lasted 6 seconds.


Measurements
• FVC
• FEV1
• FEV1/FVC
• Also FEF25-75 and TET

FVC Measurement

FEV1 Measurement
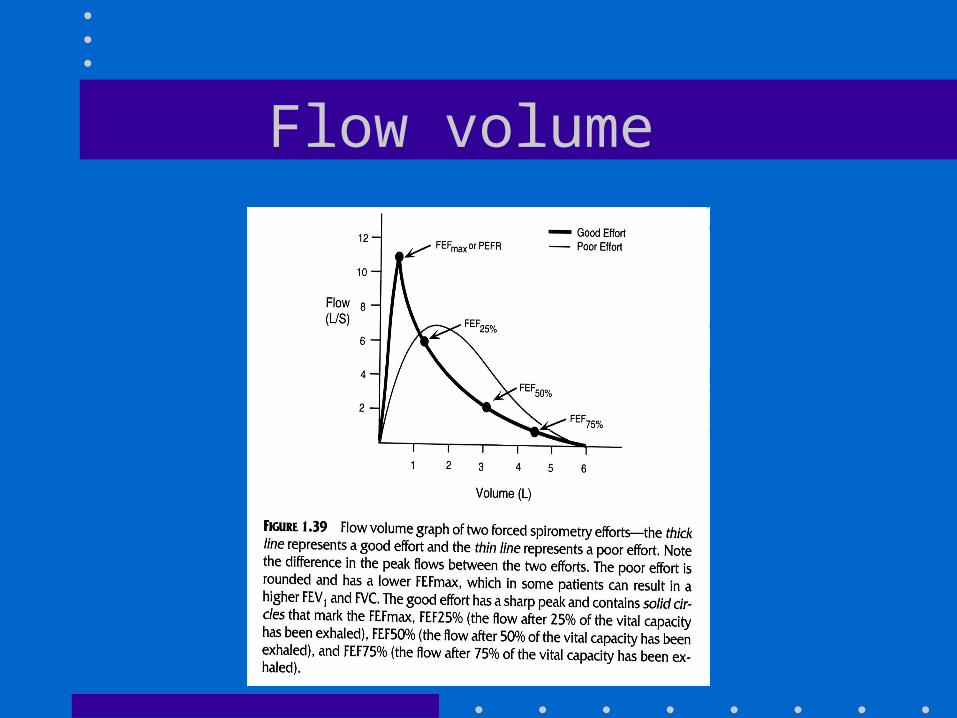
Flow volume

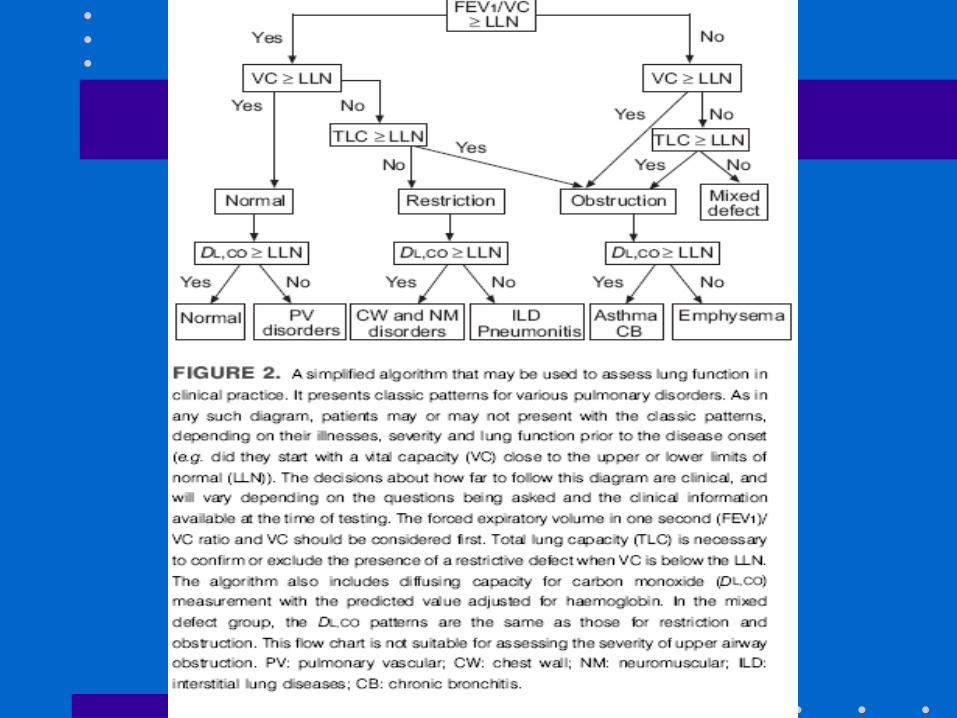
Interpretation
• First need to assess the quality of the maneuvers
• Choice of reference values
• Use of LLN
• Compare to previous tests
• Race adjustments
Interpretation
• Restrictive Lung– FVC AND FEV1
decreased
– FEV1/FVC normal
– FEV1 main distinguishing feature
• Obstruction– FEV1 decreased
– FVC Normal
– FEV1/FVC are low
Pitfalls in Interpretation
• Predicted need to fit your population
• Non Caucasians have lower lung volumes and this may need to be addressed
• Prior to interpretation the test needs to be assessed to see if it meets standards
• Machines need to be calibrated daily to ensure accuracy

Effort


Poor effort



Interpretation
• The patient’s data is compared to predicted
• Predicted values are obtained after studying populations of normal nonsmokers and then regression equations developed
• Regressions are based on sex, height, and age.

Predicted Values
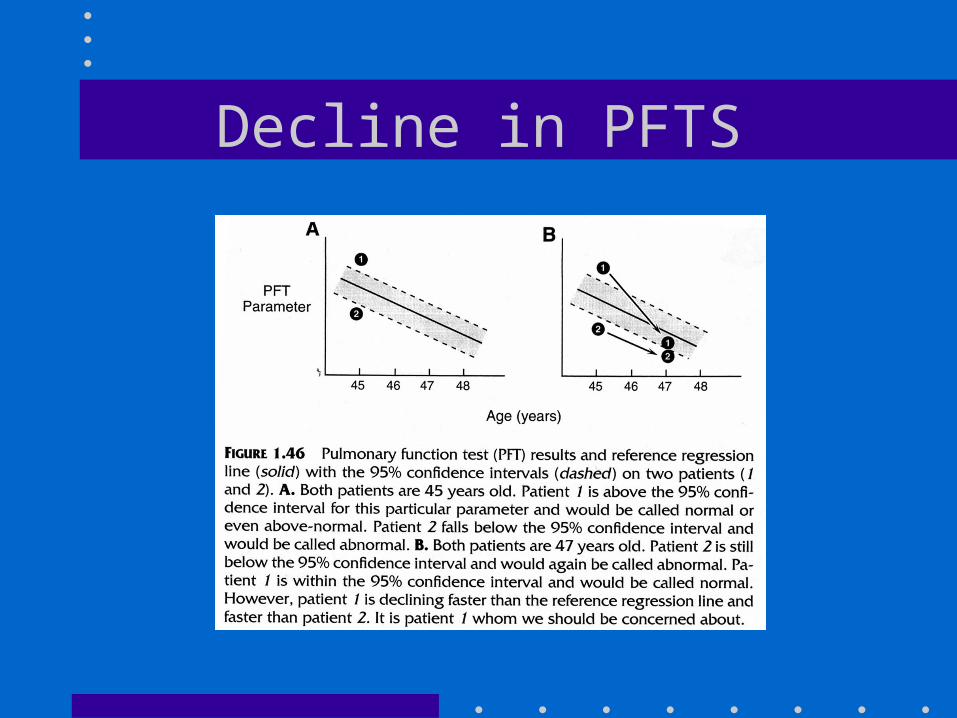
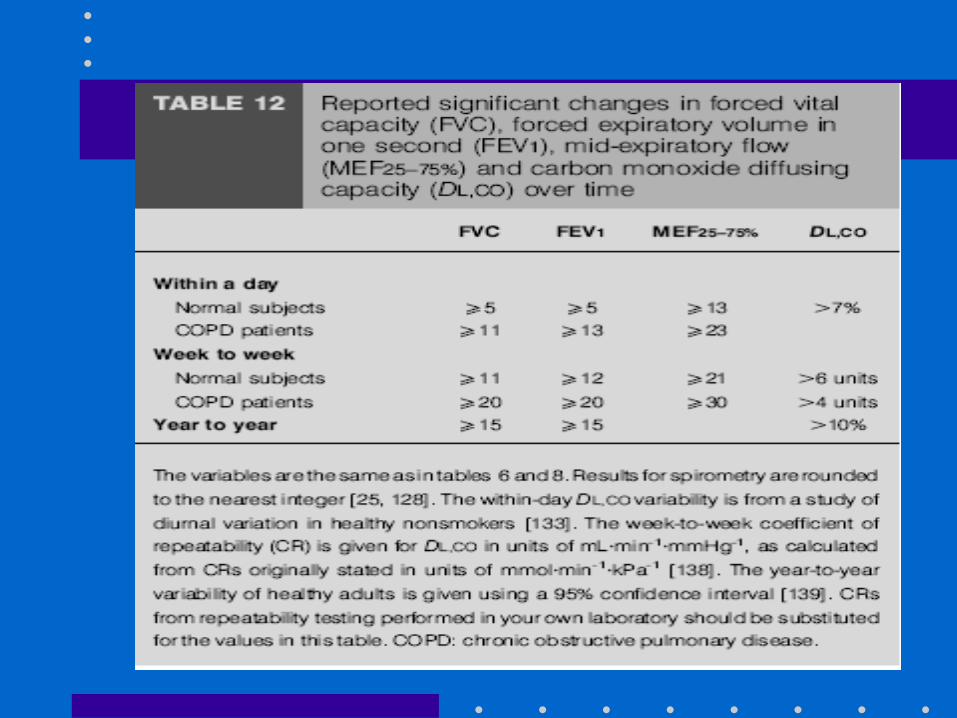
Decline in PFTS
References
• Many different ones used in past Knudson Crapo etc
• Current recommendation is NHANES III
• This studied over 7000 individuals
• Included Caucasians, blacks and Mexican Americans




Interpretaion
• Normal is > 80% of predicted– Mild impairment 65-79%– Moderate 50 -64%– Severe < 50%

Interpretations
Flow Volume Loops
• Inspiratory loops can also be obtained to evaluate for the presence of large airway obstruction
• Theory changes in pressure outside and inside the thoracic cage will cause changes in airway diameter
• These airway changes can cause a limitation to airflow if large enough
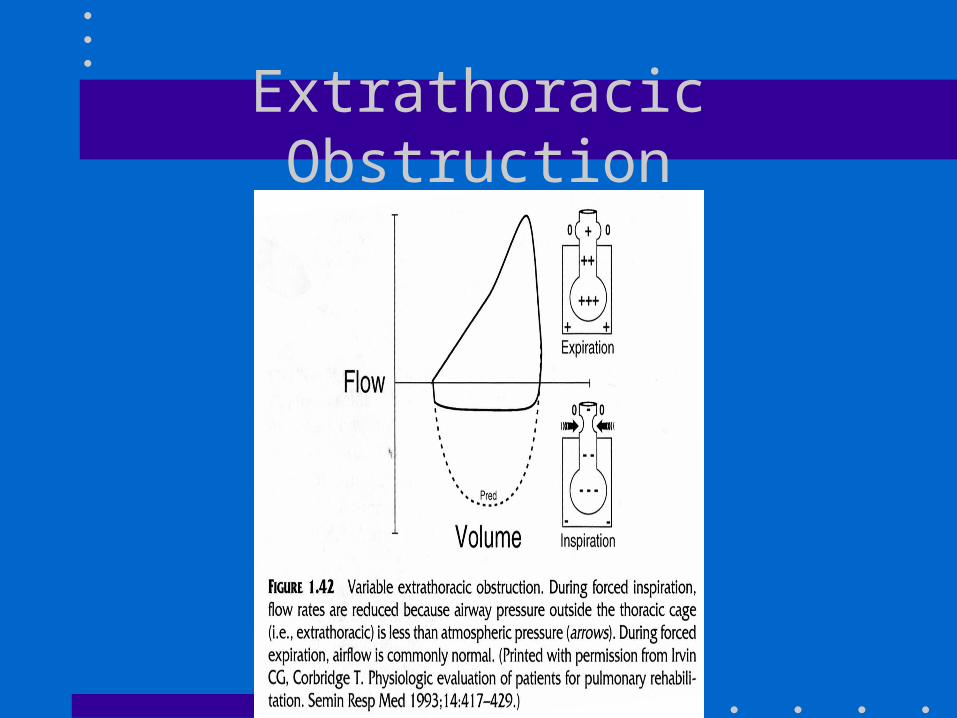
Extrathoracic Obstruction

Intrathoracic Obstruction
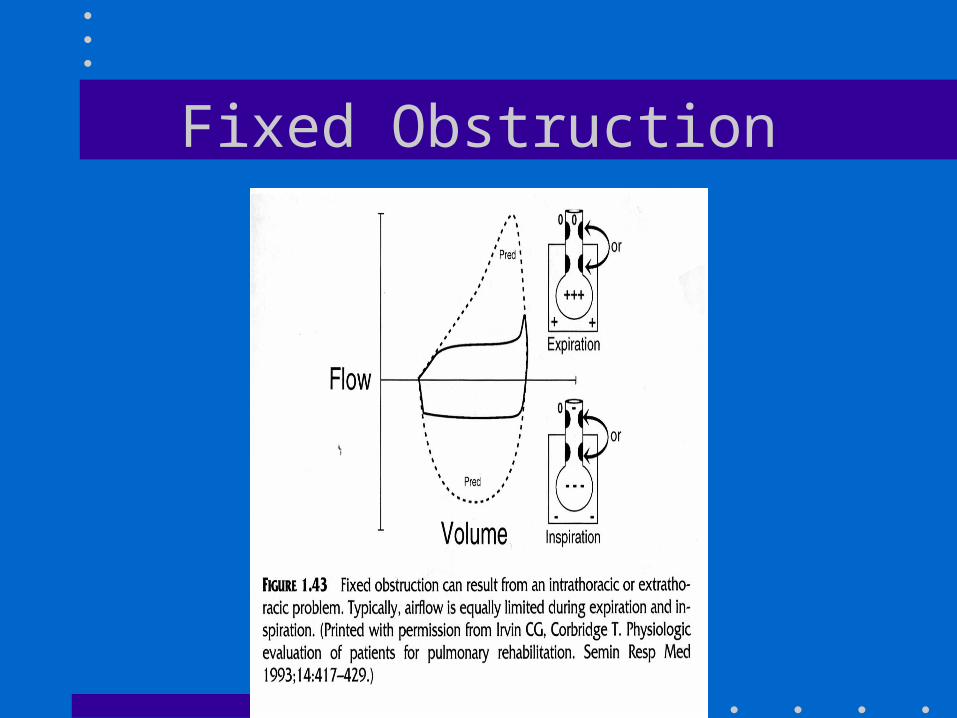
Fixed Obstruction
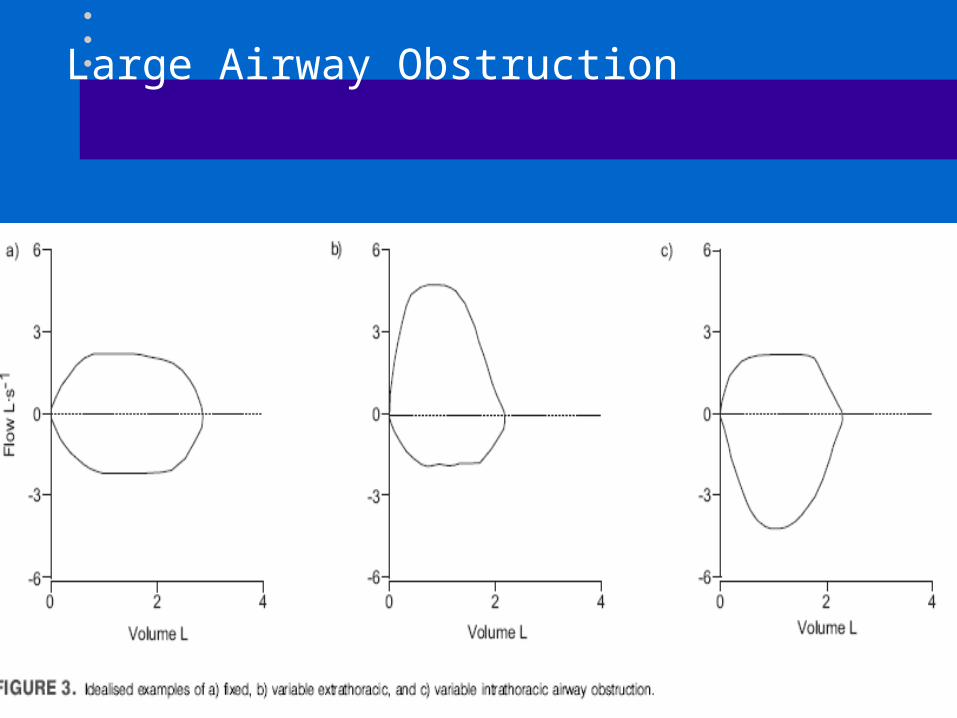
Large Airway Obstruction
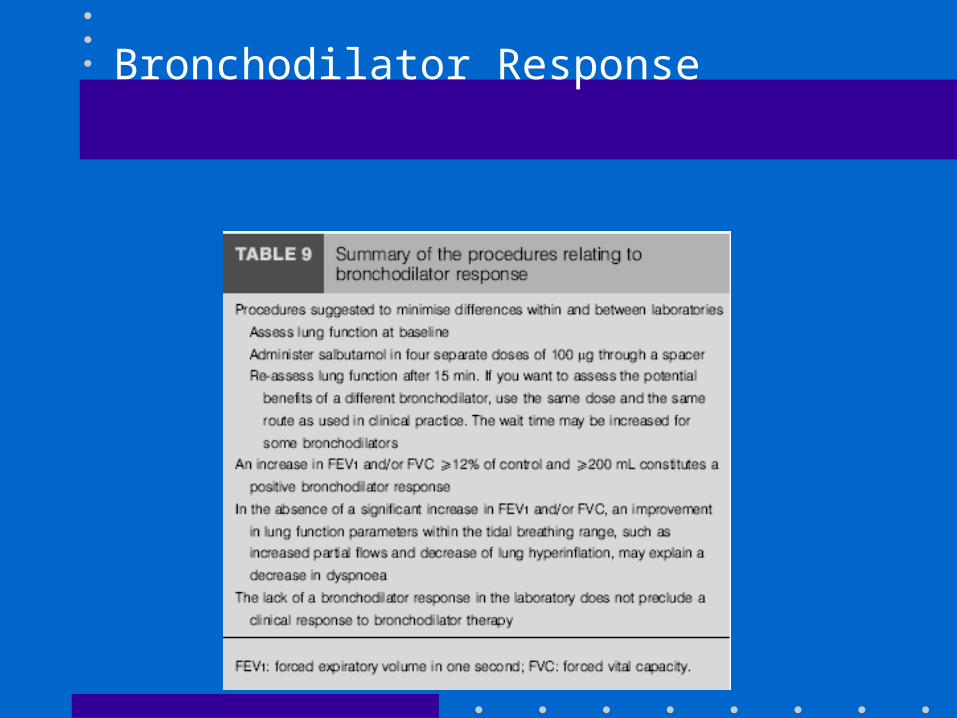
Bronchodilator Response

Bronchodilator testing
• No short acting agents for 4 hrs
• No long acting beta agonists for 12 hrs
• No theo for 12 hrs
• No smoking for 1 hr
• Beta agonist given recommended 4 puffs and wait 10-15 minutes later


Performance of the Maneuver
Peak Flow Measurements
• Convenient portable device for measuring peak expiratory flow in l/min
• May be less reliable than spirometry but easy to use and inexpensive
• Useful to follow the course of asthma and to possibly look and work exposure
• Technique

Lung Volumes
• May be measured by multiple methods
• Is important to understand what volumes the lung is composed of
• The total volume of the lung is TLC
• The subdivisions include ERV, IRV, TV,and RV
• Capacities are composed of 2 or more volumes.


Helium Dilution Technique
• Uses an inert gas, helium and by a closed circuit technique, allow it to come to equilibrium and FRC is measured
• May underestimate lung volumes in bullous lung disease



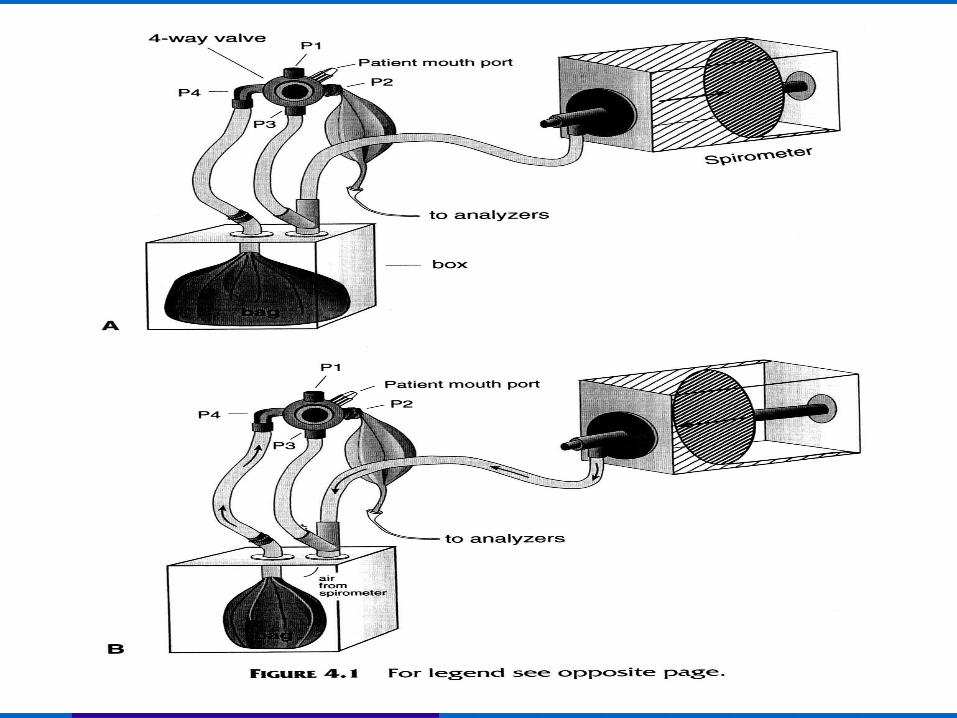
Nitrogen Washout
• Determine FRC by multiple breath open circuit nitrogen washout
• Involves having nitrogen in patients lung being washed out by inhaling 100% O2 for several minutes.
• Widely used, easy to perform but may underestimate bullous lung disease

Nitrogen Washout
• Performed by having the patient breath comfortably for several minutes and then turn in to 100% O2 at FRC.
• Monitor N2 concentrations and test ends when falls below 1%
• Easy to see leaks

Nitrogen Washout
• Concept is C1V1= C2V2– C1 = Nitrogen concentration at the start of the
test– V1 = FRC volume– C2 =N2 concentration in exhaled volume– V2 = Total exhaled volume during O2
breathing period– Nitrogen is measured by photoelectric principle

Body Plethsymography
• Is a sealed box with a fixed volume
• Uses Boyle’s Law that changes in pressure are brought about by changes in volume for the person seated in the box
• P1V1= P2V2

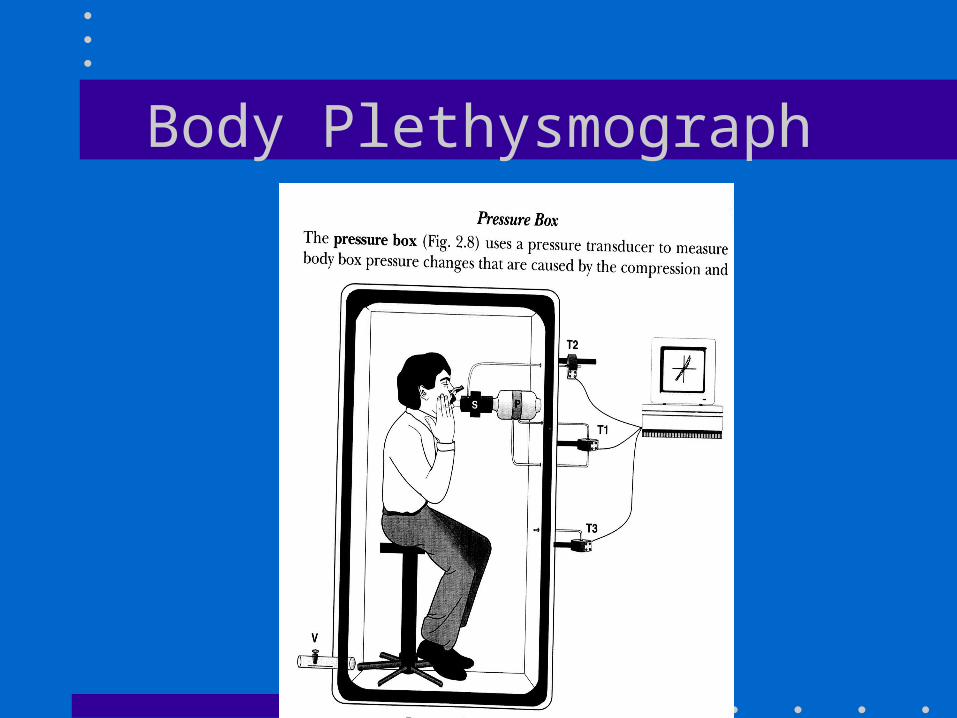
Body Plethysmograph

Lung volume measurements
• FRC is directly measured as well as SVC
• Other volumes and capacities can be calculated
• Lung volume measurements are important to confirm RLD
• TLC and RV the usual volumes assessed

Interpretation
• RLD– TLC is reduced in all
– Predicted values and interpret same as FVC and FEV1
• OLD– TLC can be increased
and is then called hyperinflation (120%)
– RV can be increased in asthma and COPD indicating air trapping

Diffusing Capacity
• Provides information about the transfer of gas between the alveoli and the pulmonary capillary bed
• It is the only noninvasive test of gas exchange
• Performed by a single breath technique and uses CO as the inert gas

Diffusing Capacity
• Diffusion of a gas is dependent of the area, the concentrations, the thickness of the membrane and the diffusing properties of the gas
• Diffusion is the rate at which a gas is transferred across the alveolar capillary membrane, the plasma, the RBC and ultimately combined with Hgb

Diffusing Capacity
• CO is typically used because it is freely diffusable
• It usually is not present in significant amounts in the blood except in some heavy smokers
• Helium or methane is also used to measure volume
• A single maximal inspiration is taken and held for 10 sec
Diffusing Capacity
• Normal result is >80%
• Can be reduced in interstitial diseases such as sarcoid or asbestosis
• Can be reduced also in emphysema or pulmonary vascular diseases
• False low measurements in anemia or lung resection and elevated in alveolar hemm
Summary
• Spirometry- Most commonly performed and useful screening test.
• Lung volumes- Can be measured several different ways. Are used to evaluate for restrictive disease and will also show air trapping
• Diffusing Capacity - Transfer of gas across the alveolar membrane

Selecting Tests
• Who should get what test
• Who cannot get certain tests
• Which method of lung volume testing
• Inpatients

Case 1
• A 25 year old female comes to your office complaining of chest tightness and shortness of breath with running.
• Exam is normal
• What tests would you order?

Spirometry
• Pre – FVC 2.64 90%
– FEV1 1.83 79%
– FEV1/FVC 69
– TET 5.0
– FEFmax 4.85 L/S
• Post– 3.12 106%
– 2.21 95% (18%)
– FEV1/FVC 71
– TET 5.5
– FEFmax 5.02 L/S
Case 2
• A 58 year old male presents to office complaining of dyspnea on exertion over the last 6 months. He has a dry cough but no other complaints. He has smoked 1ppd for 35 years and works in construction.

PFTS
• FVC 1.43 48%• FEV1 1.30 57%• FEV1/FVC 91• TLC 3.05 63%• RV1.53 68%
• Dsb 5.78 24%• Dsb(adj) 7.8 33%• VA 2.3 42%• D/VA 2.51 57%• Hsb 11.4