public health accreditation board board of directors … 2012 phab board meeting material… ·...
TRANSCRIPT

Public Health Accreditation Board Board of Directors Meeting | April 10-12, 2012
Mansion on Forsyth Park | Savannah, GA
MEETING AGENDA FOR PARTNERS AND INVITED GUESTS
All meetings will be held in the Viennese Ballroom unless otherwise noted. Conference Line Phone Number: 1.866.734.7792 / Conference Line Access Code: 1076445#
Tuesday, April 10, 2012
5:40 pm Gather in the Hotel Lobby to Depart for Group Dinner for Board Members, Partners, Invited Guests,
and Spouses 6:00 pm Reception and Dinner with Remarks from Dr. Brenda Fitzgerald, Georgia State Health Officer (invited) LOCATION: Rocks on the River (102 West Bay Street, Savannah, GA 31401)
Wednesday, April 11, 2012
9:00 am Breakfast for Board Members, Partners, and Invited Guests 9:30 am Dialogue with Funding Partners
Liza Corso, Centers for Disease Control and Prevention
Pamela Russo, Robert Wood Johnson Foundation (via phone)
10:30 am Break 10:45 am Accreditation Program Update (Robin Wilcox, Chief Program Officer) [WRITTEN REPORT] 11:00 am Discussion of Multi-Jurisdictional Accreditation Application Procedures (Bud Nicola, Les Beitsch, Rex
Archer, Carol Moehrle, and Shirley Orr) [DISCUSSION ONLY]
12:30 pm Lunch 1:30 pm Think Tank Reports and Follow-up Discussion on Action Items
Interim Reports from the Workforce and California Think Tanks (Hugh Tilson and Kaye Bender) [VERBAL REPORTS]
Update on Scheduled and Pending Think Tanks (Kaye Bender) [WRITTEN REPORT] 3:00 pm Break 3:30 pm Integrating Primary Care and Public Health: Institute of Medicine Report (Fernando Guerra) 5:00 pm Adjourn 6:30 pm Dinner for the Finance and Accreditation Committees Only LOCATION: Marble Garden Courtyard
2012 PHAB Board of Directors Meeting Dates:
June 5-7, 2012 Seattle, WA (Accreditation Committee Meets June 5, 2012) September 25-27, 2012 Central Time Zone Location (Accreditation Committee Meets September 25, 2012)
November 27-29, 2012 Mountain Time Zone Location (Accreditation Committee Meets November 27, 2012)

March 28, 2012
To: Carol Moehrle, Chair
Board of Directors
From: Robin Wilcox
Chief Program Officer
Re: Program Update for the April Board Meeting
I am pleased to provide the Board of Directors with a report of the program activities of PHAB
since the December meeting of the Board of Directors.
1. Health Department Application Process
PHAB continues to receive Statements of Intent (SOI) and Applications from Health
Departments. As noted in the previous report to the Board, PHAB Accreditation Specialists
review and process these in a timely manner in order for an invoice to be generated. As of March
20, there are a total of 63 health departments in the e-PHAB system. That includes health
departments that are in the process of submitting their SOI, submitting their application,
uploading their documentation, and waiting for specifics concerning their site visit. Health
departments in the system include Tribal, state, and local health departments. Applicants include
health departments that serve urban, suburban, and rural populations.
In addition to processing SOIs and applications, PHAB Accreditation Specialists are reviewing
the documentation submitted by health departments with Accreditation Coordinators who have
completed the in-person training. The review by the Accreditation Specialists is to determine that
a sufficient type and volume of documentation has been submitted to proceed to the next step of
the accreditation process, review by a Site Visit Team. This completeness review includes
confirmation that documents are dated and signed and is a very detailed process. The
Accreditation Specialists are finding a significant number of documents that do not have dates
and/or department identification. The Accreditation Specialists are not assessing the
documentation for conformity with the measure or its documentation requirements; that is the
responsibility of the site visitors.

2
PHAB’s Accreditation Specialists continue their ongoing work to develop a detailed, step-by-
step Accreditation Specialist Procedures Manual as they complete steps in the accreditation
process and use parts of e-PHAB for the first time. This manual will serve to standardize actions
and communications as well as to provide an excellent training manual for future Accreditation
Specialists. PHAB will also use this material as we develop the Accreditation Reserve Corps.
The Accreditation Reserve Corps will be designed to provide PHAB with a surge capacity to
process health departments through the accreditation process when the workload exceeds the
capacity of the PHAB full time Accreditation Specialists. PHAB has hired a consultant to
develop a plan for the development, training, and management of a PHAB Reserve Corps. The
scope of work, to be completed by May 2012, is a plan that includes:
Recruitment;
Configuration of their assignments;
Training needs, based on the configuration of the assignments;
A projection of the numbers of required Reserve Corps members; and
Other considerations for the design, development, and management of a Reserve
Corps.
2. Applicant Health Department Training and Technical Assistance
In mid-December 2011, PHAB conducted a two-day training session for the Accreditation
Coordinators of the first group of health departments that had their application approved and
made their first fee payment. The training was very well received. It addressed:
a. Roles of participants in the accreditation process,
b. Selection and submission of documentation to PHAB (including the use of the e-
PHAB for the submission of documentation),
c. Interpretation of the PHAB Standards and Measures Version 1.0;
d. Preparation for the site visit, and
e. Legal, communication, and conflicts of interest issues.
A follow-up webinar concerning preparation for the site visit will be provided to this group of
health departments in 2012. PHAB plans to provide this Accreditation Coordinator training
quarterly and the next Accreditation Coordinator training, for the second cohort of health
department applicants, will be held in April, 2012.
PHAB has finalized the Accreditation Coordinator Handbook. This handbook guides
Accreditation Coordinators through the PHAB process and recommends ways to organize and
engage department staff in the accreditation process. The Handbook will also be useful to health
department directors as they determine whom they will appoint as their Accreditation
Coordinator. The draft Handbook was distributed to the Accreditation Coordinators in attendance
at the December training. They were asked to review the Handbook and provide feedback to
PHAB. The Handbook was revised and finalized in March 2012.

3
PHAB continues to provide regular technical assistance to health departments as they have
questions about the intent and interpretation of the PHAB Standards and Measures Version
1.0. We continue to organize the questions and their answers by domain, standard, and measure.
These questions and answers will, collectively, provide guidance for topics and issues to include
in webinars, site visitor training, site visit reviews, Accreditation Coordinator Training, and
future revisions to the standards and measures.
3. Site Visitors
The PHAB Site Visitor Guide has been rewritten to reflect feedback and recommendations
obtained through the beta test. A number of sections have been expanded to provide clarity and
additional support, including a new section that provides guidance on the review of
documentation. Site visitors are directed to the new sections of the PHAB Standards and
Measures Version 1.0 that state the purpose and significance of each measure. Scoring
assessment categories have been revised from three (Fully Demonstrated, Partially
Demonstrated, and Not Demonstrated) to four (Fully Demonstrated, Largely Demonstrated,
Slightly Demonstrated, and Not Demonstrated). Further definition of the programs that can be
used for accreditation purposes (as adopted in the PHAB Standards and Measures Version
1.0) is provided. Various guidance documents such as the Entrance Conference Talking Points
and the Interview Guide have been combined into the single document. The Site Visit Report
will look significantly different from the reports developed as part of the beta test. First, they will
be developed as part of e-PHAB. As approved by the Board, the report will include comments on
each measure but will not be in a narrative format. Site visitors will be guided to add
identifications of exemplary practices and opportunities for improvement, irrespective of the
scoring of the measure.
A group of site visitors for the health departments in the first group of applicants were selected
from the group of individuals who had been beta test site visitors. They have signed the PHAB
conflict of interest form and will sign the Site Visitor’s Agreement form. Site visitors will be
assigned to teams as health departments submit their documentation and it is deemed to be
complete by the Accreditation Specialists. Health departments will be provided the names of the
members of their Site Visit Team for their review for the identification of any conflicts of
interest.
A two-day training was held on March 20 and 21, 2012 for the first group of site visitors. The
purpose of the training was to instruct site visitors on how to:
Conduct a professional and informative health department site visit;
Implement PHAB’s site visit, review, and Site Visit Report development process;
Operate PHAB’s e-PHAB information system;

4
Accurately assess a health department’s conformity with the PHAB standards and
measures; and,
Write a comprehensive Site Visit Report that provides the PHAB Accreditation
Committee with information needed for them to make an appropriate accreditation
status decision.
The training was very well received. A training session for site visitors from the beta test group
will be held in May 2012 to accommodate some of the site visitor schedules that prevented them
from attending the March training session. This will complete the training for the beta test site
visitor group.
PHAB is working to further develop a pool of trained site visitors. We are reviewing several lists
of names of individuals who have been engaged with PHAB in order to identify potential site
visitor volunteers. We are also developing a call for volunteers, based on the same criteria that
were successfully used to select the beta test site visitors.
4. Education and Training
PHAB is developing webinars and training sessions in addition to the Accreditation Coordinator
training and the Site Visitor training. Specialized training will be provided to Site Visit Teams
that are scheduled to visit a state or local health department in a centralized state. A series of
three webinars will be made available on the PHAB’s website providing tips for the selection of
documentation. An introductory webinar for newly appointed Accreditation Coordinators is
being planned. PHAB is working with NIHB to develop a series of three webinars that target
Tribal health departments. These are planned for early summer. PHAB is assisting the Public
Health Sciences Department at the University of California in developing a webinar series that
will be held for local and state health department leaders in May.
5. Other Program Activities
PHAB revised the format of the policies and procedures for centralized states to be “user
friendly” for health departments. PHAB announced the availability of the PHAB Centralized
States Policies and Procedures Version 1.0 in its newsletter and six states have requested a
copy. PHAB further developed guidance for centralized state health departments that have no
local health departments but provide programs and services through local offices.
PHAB program staff are working closely with Liaison International through the development,
testing, and implementation of e-PHAB, including the development of process maps, the review
of e-PHAB components, health department scenario testing of system components, and the
identification of system issues that require resolution. Recent focus has been on the
operationalization of the completeness review module and the site visit module.

5
The Accreditation Policies and Procedures will be reviewed by the Accreditation Committee
during its first meeting scheduled for April 12.
5. Presentations and Abstracts Submitted Since the December 2011 Board Meeting
Presentations:
1. Public Health Accreditation: Tribal Collaboration and Action, Presentation to the NIHB
Board, Washington DC, January 23, 2012
2. State Public Health Accreditation. Presentation at the Alaska Public Health Association
Annual Meeting, Anchorage, AK, January 25, 2012.
3. Why Invest in Accreditation, Presentation at the NY State Associations of Counties
Annual Meeting, Albany, NY January 31, 2012
4. Public Health Accreditation, Presentation to the FDA Food Safety Project Advisory
Group and the NACCHO Food Safety Workgroup, Washington DC, February 1, 2012
5. Public Health Nursing in a Transformed Public Health System. Presentation to the RWJF
Public Health Nursing Forum. Princeton, NJ, February 8, 2012.
6. Public Health Accreditation. Presentation to the RWJF Thought Leaders Meeting,
Washington, DC, February 10, 2012.
7. Public Health Accreditation. Presentation to the Institute of Medicine Committee,
Washington, DC, February 14, 2012.
8. State Health Department Accreditation. Presentation to the Indiana State Department of
Health Performance Assessment Meeting, Indianapolis, IN, February 29, 2012.
9. Affecting Population Health Through a National Accreditation Strategy. Two
presentations at the University of Mississippi Medical Center Annual Research
Conference, Jackson, MS, March 1, 2012.
10. Health Department Collaborations with Nonprofit Hospitals: Community Health Needs
Assessments, panel at the Network for Public Health Law conference Legal Aspects of
Local Public Health Governance, Structure & Change, New Orleans, LA on March 5-6,
2012.
11. Accreditation: What Is It and Why Support It, Presentation to the Georgia State Board of
Health monthly meeting, Atlanta, GA, March 13, 2012
12. Public Health Accreditation. Presentation to the ASTHO State Health Officers
Networking Initiative. Washington, DC, March 13, 2012.
13. Public Health Accreditation. Presentation to the ASTHO/RWJF Quality Improvement
Initiative. Alexandria, VA, March 19, 2012.
14. CHAs and CHIPs and Accreditation, NACCHO CHA/CHIP In-person Training, Dallas,
TX, March 29, 2012
15. Public Health Accreditation. CDC Seminar, Atlanta, GA, April 3, 2012.

6
Abstracts Submitted:
1. Evaluating and Selecting Documentation for Accreditation Measures, Submitted on
February 10, 2012 for an APHA Learning Institute at the 2012 Annual Meeting, San
Francisco, CA
2. Partners in Preparation: Supporting Health Departments as They Get Ready for
Accreditation, Submitted on March 1, 2012 for the NNPHI 2012 Annual Conference,
New Orleans, LA
3. Public Health Accreditation: One Year Post Launch, Submitted to APHA for Invited
Session at the 2012 Annual Meeting, San Francisco, CA.
4. Achievements in Governance Engagement in Public Health Accreditation. Submitted to
NALBOH for their 20th
Annual Meeting in Atlanta, GA, August 2012.
Enclosures:
PHAB Site Visitor Guide Version 1.0
PHAB Centralized States Policies and Procedures Version 1.0

Site Visitor Guide
VERSION 1.0APPLICATION PERIOD 2011-2012
MARCH 2012
Public HealthAccreditation Board

Table of Contents
Introduction 1 I. Public Health Department Accreditation 2 II. Purpose of the Site Visit 3 III. Site Visit Team 4 1. Site Visit Team Roles and Responsibilities 4 a. Roles and Responsibilities of Site Visit Team Members 4 b. Roles and Responsibilities of the Site Visit Team Chair 4 2. Site Visit Team Composition 5 3. Site Visit Team Requirements 7 a. Conflicts of Interest 7 b. Professional and Ethical Behavior 8 c. Confidentiality 8 d. Intellectual Property 10 e. Interaction with Health Department Employees 10 f. Removal From the Site Visit Team 10 IV. e-PHAB 11 V. Site Visitor Training 12 1. Purpose and Objectives 12
2. Topics to be Covered 12
VI. Site Visit Preparation 14 1. Health Department Website 14
2. Preliminary Review of the Health Department’s Documentation 14
a. Organizational Team Meeting 15
b. First Review of Documentation 15
c. Team Review of Documentation 16
d. Pre-Site Visit Conference Call 16
3. Scheduling and Logistical Arrangements 17
4. Health Department Preparations 18
VII. Site Visit 19 1. Focus of the Site Visit 19
2. Site Visit Process 19

a. Other Site Visit Attendees 19
3. Site Visit Agenda 20
a. Site Visit Agenda Development 20
b. Site Visit Agenda Contents 20
VIII. Documentations Review Guidance 25 1. Documentation Assessment for Each Measure 25
2. Assessment Categories 26
3. Quality and Performance Improvement 27
4. Standards and Measures 27
5. Applicability of Public Health Department Accreditation Standards 28
6. Types and Formats of Documentation 28
7. Visual Observations of Documentation 30
8. Additional Interviews and Discussions 30
IX. Site Visit Report 33 1. Site Visit Report Contents 33
2. Process and Timeframes 34
X. Post-Site Visit 35 1. PHAB Accreditation Committee Accreditation Status Decision 35
2. Evaluation 35
3. Travel Reimbursement 35
Appendices 36 A. PHAB Site Visit Process 37
B. Site Visit Agenda Template 40
C. Entrance Conference Talking Points 43
D. Exit Conference Talking Points 45
E. PHAB Site Visitor Interview Guidance 46
F. PHAB Site Visitor Agreement Form 50
G. PHAB Travel Policies and Procedures 52
H. PHAB Travel Reimbursement Form 57

PHAB Site Visitor Guide Version 1.0
March 2012 Page 1
Introduction
The PHAB Site Visitor Guide Version 1.0 provides guidance to PHAB site visitors to address
the preparation for the site visit, the conduct of the site visit, and the development of the Site
Visit Report. The Site Visitor Guide not only reviews the steps in the overall health department
review process, it also provides guidance and guidelines for completing those steps and fulfilling
the responsibilities of a PHAB site visitor. The Site Visitor Guide addresses the key elements
of the roles and responsibilities of site visitors, the PHAB information system (e-PHAB), site
visitor training, conduct of the site visit, documentation review and assessment, the
development of the Site Visit Report, and evaluation responsibilities. PHAB site visitors are
encouraged to use and refer to the Site Visitor Guide throughout the implementation of their
assigned site visitor responsibilities.
The site visitors’ review of a health department consists of an assessment of the health
department to determine if it is in conformity with the measures and meets the standards
contained in the PHAB Standards and Measures Version 1.0. These are peer reviews
conducted by a team of PHAB-trained site visitors. Site visitors will use their public health
experience and expertise to make assessments of a health department’s conformity with the
PHAB Standards and Measures Version 1.0. Site visitors are strongly encouraged to also be familiar with and utilize other PHAB documents
and publications including the PHAB Standards and Measures Version 1.0; Guide to
National Public Health Department Accreditation Version 1.0; National Public Health Department Documentation Guidance Version 1.0; and PHAB Acronyms and Glossary of Terms Version 1.0. These documents may be accessed on the PHAB website:
www.phaboard.org.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 2
I. Public Health Department Accreditation
PHAB is the national accrediting organization for public health departments. A nonprofit
organization, PHAB is dedicated to advancing the continuous quality improvement of Tribal,
state, local, and territorial public health departments. PHAB is working to promote and protect
the health of the public by advancing the quality and performance of all public health
departments in the United States through national public health department accreditation.
PHAB’s vision is a high-performing governmental public health system contributing to a
healthier nation.
Applicants eligible for PHAB accreditation are governmental entities that have the primary
statutory or legal responsibility for public health in a Tribe, state, territory, or at the local level. To
be eligible, such entities must operate in a manner consistent with applicable federal, Tribal,
state, territorial, and local statutes.
The accreditation process and the PHAB standards and measures are intended to be flexible
and inclusive, accommodating many different configurations of governmental public health
departments at all levels - Tribal, state, local, and territorial. Applicants include: centralized and
decentralized state health departments; health departments that are part of a larger
governmental agency; health departments that may or may not have environmental public
health responsibility; regional and district health departments; and health departments that
share resources to fulfill particular functions.
Accreditation provides a means for a public health department to identify performance
improvement opportunities, enhance management, develop leadership, and strengthen
relationships with members of the community. The accreditation process will challenge the
health department to think about its roles and responsibilities and how it fulfills them. The
accreditation process will encourage and stimulate quality and performance improvement in the
health department.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 3
II. Purpose of the Site Visit
The site visit of a health department is a key and critical phase of the accreditation process.
The site visit provides a peer review by public health practitioners and other public health
experts. The site visit process includes off-site preliminary reviews of documentation submitted
by the health department to demonstrate conformity with each measure; on-site interviews and
discussions with health department staff; and on-site meetings with partner organizations,
community partners, and representatives of the health department’s governing entity. Following
the site visit, the site visitors develop the Site Visit Report based on the review of documentation
and on-site interviews and meetings at the health department. The Site Visit Report is the basis
for the accreditation status decision made by the PHAB Accreditation Committee.
The primary purpose of the site visit is to verify the information submitted to PHAB by the
applicant health department as evidence that it meets the standards and measures. Site
visitors will review this documentation to assess conformity with each measure. The site visit
provides the on-site operational context of the documentation.
The site visit is an opportunity for site visitors to supplement paper documentation with face-to-
face discussions and direct observations. Site visitors will ask questions about the
documentation and the structure and operation of the health department. The health department
will have an opportunity to describe its policies and procedures, relationships with the
community, the role of its governing entity, and other qualitative information. These discussions
will provide an opportunity for the Site Visit Team to understand the character and culture of the
health department.
During the beta test of the PHAB process, site visitors commented that the site visit provided “a
better understanding of the health department.” A beta test health department said that the site
visit was an opportunity for the Site Visit Team “to smell it and to taste it and to see how it
works,” rather than rely only on documentation to assess the health department. The site visit is
the opportunity to experience the health department and learn how it implements the Essential
Public Health Services.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 4
III. Site Visit Team
PHAB will establish and train a team of site visitors for each health department accreditation
applicant. Most Site Visit Teams will consist of three members. However, PHAB may elect to
assign more members where indicated by the size, breadth, or other particular characteristics of
the health department being reviewed. PHAB will designate one of the team members to be the
Site Visit Team Chair.
1. Site Visit Team Roles and Responsibilities a. Roles and Responsibilities of Site Visit Team Members Site Visit Team members are responsible for the completion of the following activities:
Attend PHAB’s in-person Site Visitor Training.
Review the health department’s website to learn about the health department
they will visit.
Coordinate with the other Site Visit Team members for documentation review
assignments. Each team member will be assigned Domains for in-depth review,
questions, and writing the Site Visit Report.
Log on to e-PHAB to review the health department’s descriptive information
provided by the health department in its e-PHAB application, review the health
department’s documentation, read the measure narratives submitted, and
preliminarily determine whether the documentation conforms to the measure.
Participate in a series of teleconferences with the Site Visit Team prior to the site
visit.
Conduct the site visit. Each of the members of the Site Visit Team will be
responsible for working to reach consensus on the assessment and comments
for each measure.
Develop the Site Visit Report. Each of the site visitors will participate in the
development of the report and write sections in accordance with Domain
assignments.
Site visitors are expected to:
Be present, attentive, and participatory in all training, team meetings, site visit
activities, and site visit interviews;
Arrive on time for training, conference calls, meetings, site visit sessions, and
other agree on times and not leave early;
Be prepared for all site visit activities; and
Contribute to the completion of the team’s charge including review of the health
department’s documentation, the development of site visit questions, the conduct
of site visit interviews, and the writing of the Site Visit Report.
b. Roles and Responsibilities of the Site Visit Team Chair One team member will be appointed by PHAB to be the Site Visit Team Chair. The Site
Visit Team Chair is charged with leading, managing and organizing team members to
facilitate completion of all Site Visit Team responsibilities. The Site Visit Team Chair has

PHAB Site Visitor Guide Version 1.0
March 2012 Page 5
the responsibility to facilitate group discussions, ensure that all team members are
heard, and develop group consensus. The Site Visit Team Chair is expected to establish
a professional, collegial, and comfortable atmosphere in all team meetings and during
the site visit.
Specifically, the Site Visit Team Chair is responsible to:
Work with the PHAB staff to schedule the pre-visit teleconference(s).
Lead all pre-site visit teleconference reviews and discussions concerning
documentation.
Ensure that discussions and interviews are based solely on the accreditation
subject.
Make Domain assignments for the team members.
Act as the spokesperson for the Site Visit Team.
Lead the work of the team on-site and lead all meetings involving Site Visit Team
members.
o Facilitate on-site executive sessions.
o Lead the entrance and exit conference and other sessions, as
appropriate.
o Convene the Site Visit Team to review the findings and to reach a
consensus on the scoring, comments, and conclusions.
Manage any conflicts that may arise between Site Visit Team members and/or
with health department representatives or guests.
Prepare the final Site Visit Report.
Assign each Site Visit Team member a portion of the Site Visit Report
to develop.
Manage a consensus process to incorporate feedback from all Site
Visit Team members into the Site Visit Report and coordinate the
development of the final report.
Give final approval of the Site Visit Report and submit it to PHAB. The
Site Visit Report is due to PHAB within two weeks of the conclusion of
the site visit.
Be available by phone to the PHAB Accreditation Committee during their
review of the Site Visit Report in order to answer any questions the
Committee may have.
2. Site Visit Team Composition Site Visit Teams will be multi-disciplinary with collective broad-based public health experience.
PHAB will employ a peer review model in the assignment of Site Visit Team members.
Site Visit Teams will include members with public health management experience (at
least five years) and knowledge about the delivery of governmental public health
services.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 6
PHAB will endeavor to include individuals with senior level, executive health department
management experience on Site Visit Teams. PHAB will seek to assign senior level
state health department managers (current or previous state health officials or senior
deputies) to state health department site visits; senior level local health department
managers (current or previous local health officials or senior deputies) to local health
department site visits; and senior level Tribal public health department managers
(current or previous Tribal public health officials or senior deputies) to Tribal public
health department site visits.
Site Visit Team members will be from the same geographic area (HHS Region) as the
applicant, to the extent possible. However, to ensure objectivity, site visitors will not be
from the same state as the applicant health department.
PHAB will seek to include site visitors with experience in similar public health system
structures as the health department being visited; i.e., centralized or decentralized, etc.
PHAB will determine when Site Visit Teams should include individuals with specific
experiences, including Tribal public health, environmental public health, public health
laboratory, and governance.
Site Visit Teams should include a member with Tribal experience when the site is a:
o Tribal public health department,
o State health department that has state and federally-recognized Tribes within the
state, and/or a
o Local health department that is included within the geographic composition of
Contract Health Service Delivery Areas*, as defined by the Indian Health Service.
*Contract Health Service Delivery Areas (CHSDAs) consist of a county which
includes all or part of a reservation, and any county or counties which have a
common boundary with the reservation.
When possible, a local health department representative may be assigned to a state
health department Site Visit Team and a state representative may be assigned to a local
Site Visit Team (from another state) to address communication and coordination of state
and local functions.
In addition to the appointed Site Visit Team, PHAB may enlist individuals with specific
expertise to review particular portions of the documentation submitted by a health
department. Examples of areas of expertise include emergency preparedness,
environmental public health, governance, Tribal public health, or public health laboratory
services. These volunteers will provide additional expert assessment and assist the Site
Visit Team in formulating questions for the site visit.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 7
3. Site Visitor Team Member Requirements Members of Site Visit Teams serve on a voluntary basis as PHAB’s representatives. Site Visit
Team members will not be compensated for their role as a site visitor. Travel expenses will be
covered by PHAB in accordance with PHAB’s Travel Policies. To become a Site Visit Team
member, an individual must attend PHAB’s in-person site visitor training session. In order to
maintain the status as a site visitor, an individual must (1) participate on a Site Visitor Team at
least one site visit a year, and (2) participate in an annual refresher training session. The
purpose of the annual refresher training session is to keep site visitors up-to-date on recent
changes and current practices related to PHAB accreditation. To accommodate site visitors’
schedules, two or more training sessions will be offered each year. Training dates will be
announced at least one month prior to the session. PHAB will offer the refresher training
programs and updates online.
a. Conflicts of Interest In their capacity as site visitors, volunteers must act at all times in the best interest of
PHAB. PHAB has an obligation to ensure that the organization maintains a biasfree
decision making process. All PHAB site visitors have an obligation to identify and
disclose actual, potential, and perceived conflicts of interest, and avoid the impact that
such conflicts of interest may create in the accreditation process.
A conflict of interest is a transaction or relationship which presents or may present a
conflict between an individual’s obligations to PHAB and an individual’s personal,
business, or other interests. A conflict of interest may arise when an individual has some
other interest that might suggest divided loyalty on the part of the individual between
obligations to PHAB, on one hand, and to some other organization or cause, on the
other. The “other interest” may arise from a transaction between PHAB and a third party,
or an individual's volunteer or paid relationship with a third party, which may compromise
his or her ability to provide unbiased and undivided loyalty to PHAB while serving in a
site visitor role.
Site visitors, when selected for their qualifications, will be asked to disclose any potential
conflicts of interest with any applicant health department. These conflicts may include,
but are not limited to, previous or current employment with a site; previous or current
consultation or other business arrangement with a site; family relationship with key
employees at a site; or any other relationship with a site that would afford the site visitor
access to information about that site other than that which is provided through the PHAB
accreditation process. A site visitor could still be able to serve as a member of a Site
Visit Team, but will not be assigned to review any site for which a conflict of interest
exists.
Site visitors will be expected to review PHAB’s Conflict of Interest (COI) Policy and
submit a confidential COI Disclosure Form prior to being approved as a site visitor. COI
form updates will be required annually thereafter. PHAB reserves the right to not select

PHAB Site Visitor Guide Version 1.0
March 2012 Page 8
or assign a site visitor if the conflict of interest is determined to create a barrier to
administering PHAB’s accreditation program.
b. Professional and Ethical Behavior Site visitors serve as representatives of PHAB. As such, site visitors will conduct
themselves in the highest professional and ethical manner at all times. Each team
member has valuable perspectives and contributions to make to the process. All site
visitors should be courteous and demonstrate respect and consideration for other team
members as well as to the health department staff and community representatives. In
the unlikely event that conflict arises during the site visit experience, the Site Visit Team
Chair will be asked to work to resolve the conflict. Assistance may be requested from the
PHAB staff as needed.
Site visitors are expected to never criticize any elements of the PHAB accreditation
process or standards and measures in the presence of health department staff or
members of the community. Site visitors are expected to never criticize health
departments’ operations, programs, or staff. Team discussions should be limited to
conformity to measures.
Site visitors are expected to dress in business attire during the site visit. PHAB will issue
each site visitor a “PHAB Official Site Visitor” badge to wear during the site visit to
identify themselves as members of the Site Visit Team. Additionally, some health
departments will require site visitors to wear a health department “visitor badge.”
c. Confidentiality The nature of the business and the purposes to be conducted and promoted by PHAB is
as follows:
To improve and protect the health of the public in the United States by
establishing and maintaining a national accreditation program designed;
To prepare and disseminate nationally accepted standards of quality and
encourage voluntary compliance with such standards for the accreditation of
Tribal, state, local, and territorial governmental public health departments;
To promote high performance and continuous quality improvement and
increase accountability among public health departments;
To identify and publicly recognize those public health departments that have
met nationally accepted standards of quality;
To make charitable contributions and grants to nonprofit organizations
exempt from federal income tax under Section 501(c)(3) of the Internal
Revenue Code of 1986, as the same may be amended or supplemented
(hereinafter referred to as the “IRC”), as well as governmental units and other
nonprofit organizations, that promote and further the purposes described in
Section 1 above; and

PHAB Site Visitor Guide Version 1.0
March 2012 Page 9
To exercise any other powers conferred upon corporations organized
pursuant to the provisions of the District of Columbia Nonprofit Corporation
Act.
PHAB is organized exclusively for charitable, educational, and scientific purposes,
including, for such purposes, the making of distributions to organizations exempt from
federal income tax under IRC Section 501(c)(3). The nature of the business that PHAB
is engaged in and the laws that guide the work of nonprofit organizations suggest that
PHAB have a policy related to confidentiality.
As with many nonprofit organizations, however, PHAB needs to find the right balance
between transparency and confidentiality. Some information, such as Form 990 required
by IRS, must be disclosed. Other information is shared with funders, stakeholders, and
the general public in order to demonstrate the organization’s positive impact on the
community. On the other hand, like most nonprofit organizations, PHAB operates in a
demanding and competitive environment.
Confidentiality is a basic element of the operation of PHAB. To protect the confidentiality
of its applicants as well as its board members, employees and the organization itself, all
information concerning these parties must be treated with extreme care. All members of
the board of directors, the staff, committees, volunteers and firms engaged by PHAB are
bound by this policy.
Except for confirming a successful completion of the accreditation process, information
pertaining to any public health department involved in exploring, seeking, or restoring
PHAB accreditation shall be kept strictly confidential. Only those authorized personnel
directly involved with a specific accreditation process shall discuss or have access to this
information. Information about PHAB finances, personnel issues, and discussions about
strategic issues related to the organization’s future should be treated as confidential and
should not be disclosed except as required by law or by funding sources, or as
authorized by the executive director. Care shall be exercised to ensure that
unauthorized individuals do not overhear discussion of confidential information.
During their service or employment, information and documents of a confidential and/or
privileged and proprietary nature may be obtained by PHAB board of director members,
committee members, employees, and others engaged by the organization. They must
understand and agree that such information must be kept confidential both during and
after their term of employment or service. They must recognize that PHAB has a
proprietary interest in any such information and/or documents and might be damaged as
a result of any disclosure or dissemination thereof.
Any such person as described above who purposely, or through a failure to exercise
reasonable care, divulges confidential or privileged information, whether during or after

PHAB Site Visitor Guide Version 1.0
March 2012 Page 10
his or her term of employment or service, is subject to appropriate discipline, including
termination or removal and possibly the pursuit of legal action.
Site visitors will be asked to sign an agreement that contains their commitment to
ensuring PHAB’s confidentiality policy is upheld.
d. Intellectual Property
Individual members of the Site Visit Teams may participate in the review, development,
modification and refinement of written documents and other forms of communication,
whether in print, electronic, or other format. All such information belongs and will belong
to PHAB. Site visitors are asked to completely, exclusively, and irrevocably assign to
PHAB the ownership of all copyrights and whatever intellectual property to which they
have contributed as a member of a PHAB site review team.
Site visitors will be asked to sign an agreement form that documents understanding and
compliance with of PHAB’s Intellectual Property policy.
e. Interaction with Health Department Employees Site visitors should present themselves in a friendly, courteous, and professional manner
as they interact with health department employees during the accreditation site visit. The
atmosphere set by the site visitors will do much to allay the natural anxiety that a health
department staff may have in being reviewed. However, site visitors should refrain from
social interactions (such as evening meals, etc.) with health department employees
while the review is being conducted. Site visitors should also not accept any gratuities
from health department employees.
f. Removal from the Site Visit Team Site visitors are expected to carry out their roles in a responsible, complete, and
professional manner. Site visitors may be removed and replaced by an alternative
volunteer if they fail to complete their assignments, are consistently late to or absent
from activities, or fail to abide by PHAB’s guidelines and policies. Site visitors will be
removed if they engage in illegal or unethical behavior.
The decision to remove site visitors will be made by the President/CEO of PHAB after
consultation with the applicant health department’s Accreditation Coordinator and other
members of the Site Visit Team. Removal of a site visitor could delay the accreditation
process; this decision will not be made casually.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 11
IV. e-PHAB e-PHAB is the electronic information system used in all phases of PHAB’s public health
accreditation process. It is a system that has been designed specifically for PHAB and tracks all
transactions in the accreditation process. e-PHAB allows for multiple users, each with a different
view depending on their role: health departments, site visitors, PHAB staff, and PHAB
Accreditation Committee members can all utilize different parts of e-PHAB to conduct their
accreditation activities. Health departments use e-PHAB to submit their Statement of Intent,
Application, and Documentation, and to receive their invoice(s). Site visitors use e-PHAB to
review the health department’s documentation and make initial assessments, develop the Site
Visit Report, and submit the Site Visit Report to PHAB. Site visitors will receive hands-on
training on the use of e-PHAB at the in-person training.
All pre- and post-site visit communications between the applicant health department and the
Site Visit Team will occur inside of e-PHAB and be facilitated by a PHAB staff person.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 12
V. Site Visitor Training All site visitors must attend PHAB’s site visitor training. This training will be an in-person training
session. 1. Purpose and Objectives The purpose of the site visitor training is to prepare volunteer site visitors to:
Conduct a professional and informative health department site visit;
Implement PHAB’s site visit, review, and Site Visit Report development process;
Operate PHAB’s e-PHAB information system;
Accurately assess a health department’s conformity with the PHAB standards and
measures; and
Write a comprehensive Site Visit Report that provides the PHAB Accreditation
Committee with sufficient information for them to make an appropriate accreditation
status decision.
Training objectives include:
Orient site visitors to PHAB, the accreditation process, and PHAB standards and
measures;
Describe the process of the site visit;
Describe, provide instruction, and demonstrate the use of e-PHAB in the review of
documentation, conduct of the site visit, and development of the Site Visit Report;
Define the roles and responsibilities of site visitors, Site Visit Team Chairs, the applicant
health department, and PHAB staff;
Provide an opportunity for dialogue with the PHAB Accreditation Specialists;
Review legal issues including confidentiality and conflict of interest;
Provide and review tools, guidance, and templates to be used by the Site Visit Team;
Provide site visitors an opportunity to practice the skills necessary to be a successful site
visitor; and
Define the process that PHAB uses to monitor inter-rater reliability.
PHAB will cover the travel expenses for the site visitors to attend the training, in accordance
with PHAB’s Travel Policies and Procedures (Appendix G).
2. Topics to be Covered Training for site visitors will provide an overview of PHAB, its processes, the standards and
measures, and PHAB’s commitment to quality and performance improvement. The entire
accreditation process will be reviewed to provide the site visitors an understanding of how the
site visit fits into the accreditation process and the importance of the site visit and the Site Visit
Report that the Site Visit Team will develop for the PHAB Board appointed Accreditation
Committee. The roles and responsibilities of the site visitor will be presented.
Training will include:
Review of the accreditation process;

PHAB Site Visitor Guide Version 1.0
March 2012 Page 13
Legal and communication issues;
Review of the site visit process;
Review of the standards, measures, and documentation requirements and guidance;
Instruction on the use of e-PHAB;
Guidance on evaluating the evidence provided by the applicant health department to
show conformity with the measure;
Instructions concerning the assignment of categories of demonstrated conformity for
each measure (Fully Demonstrated, Largely Demonstrated, Slightly Demonstrated, and
Not Demonstrated);
Inter-rater reliability measurement;
Instruction concerning the identification of areas of excellence and opportunities for
improvement;
Instructions on the development of the Site Visit Report; and
Hands-on group case study exercise to evaluate documentation and use e-PHAB.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 14
VI. Site Visit Preparation
After a Site Visit Team has been appointed, the Site Visit Team Chair has been designated by
PHAB, and the Site Visit Team members have completed site visitor training, the Site Visit
Team will be ready to begin preparing for the site visit of the health department they have been
assigned. In summary, each member of the Site Visit Team, and the team as a group, will
prepare for the site visit by: (1) agreeing on assignments of Domains for each team member;
(2) reviewing the documentation submitted by the health department; (3) preparing questions
and/or requests for additional documentation; and (4) reviewing answers and/or additional
documentation.
No member of the Site Visit Team will contact any staff or representative of the health
department prior to the site visit. All communication with the applicant health department will
occur through PHAB via e-PHAB.
The health department will submit its documentation to PHAB; these are the documents that the
health department has uploaded for each measure to provide evidence that measures have
been met. PHAB Accreditation Specialists will conduct a completeness review of the
documentation. If the documentation is deemed to be incomplete, the health department will
have an opportunity to upload additional documents.
The members of the Site Visit Team will begin their review when PHAB forwards to each site
visitor the e-PHAB link and instructions to access the health department’s documentation. Each
uploaded document may be accompanied by a description that the health department has
developed to provide context for the site visitor. Each measure may also contain Measure
Narrative, or text the health department provides to explain how all the documents, taken
together, provide evidence that the health department is in conformity with the measure.
Documentation will be organized by the Required Documentation for each measure in the
PHAB Standards and Measures Version 1.0.
1. Health Department Website Before beginning the review of documentation, each member of the Site Visit Team should
individually review the health department’s website. The website can provide a great deal of
background information on the governmental and reporting relationships, organizational
structure of the health department, population served, programs provided to the population, and
public health priorities as communicated to the public. The website will provide each team
member with a broad overview of the health department that they will be visiting.
2. Preliminary Review of the Health Department’s Documentation The documentation the health department submits serves as the primary source of information
about the health department and will be the basis for interviews and discussions conducted
during the site visit. It will also be the basis for the Site Visit Report, on which the PHAB
Accreditation Committee will base its accreditation determination.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 15
a. Organizational Team Meeting PHAB staff will schedule a planning teleconference call for the team to discuss the
process, make assignments, and clarify expectations of the process and roles of the Site
Visit Team. During this call the Site Visit Team Chair will assign each of the team
members a set of Domains for their review. Each Site Visit Team member will be
responsible for reviewing and assessing the documentation that was submitted to
demonstrate conformity with the measures in the Domains assigned to them. The Site
Visit Team will consider the work assignments and agree on a general time frame for the
next team call. The Site Visit Team will review the purpose of the next call, which will be
to review all of the documentation as a group and discuss impressions and questions.
During the next call they will also, as a group, identify any additional documentation they
would like to request and articulate questions for the health department’s response prior
to the site visit.
b. First Review of Documentation Each site visitor will be given access to e-PHAB and the Domains they have been
assigned. Each site visitor should review the health department’s application for
accreditation. The application provides an overview of the department including:
A description of the jurisdiction (urban, rural, suburban, or frontier),
The existence of Tribal government in the area served by the health
department,
The size of the department (population, budget, employees, and FTEs),
A description of the governing entity structure,
A list of public health programs,
The identification of additional physical sites or facilities that the health
department would like the Site Visit Team to consider visiting, and
A narrative developed by the health department that describes unique
characteristics such as structure, population served, governing entity, unique
services provided, etc.
Each site visitor will individually review the documentation for each of the measures in
the Domains they have been assigned. The site visitor will preliminarily gauge the
conformity of each measure as “Fully Demonstrated,” “Largely Demonstrated,” “Slightly
Demonstrated,” or “Not Demonstrated”. Each Site Visit Team member will make a
judgment for each measure based on his or her review and careful consideration of the
documentation and health department’s notes, and on his or her professional expertise.
As the individual site visitors work through the measures in the Domains that they have
been assigned, they will keep notes (using the e-PHAB note function) describing how
conformity was or was not demonstrated, areas of strengths, and opportunities for
improvement.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 16
c. Team Review of Documentation PHAB staff will work with the members of the Site Visit Team to schedule a team
teleconference. The purpose of this conference call will be to review the materials,
determine potential areas of non-conformity, identify missing documentation, and
formulate questions. More than one call may be needed, depending on the number and
complexity of the issues identified for group discussion.
Each Site Visit Team member will identify measures that received a preliminary
assessment of less than “Fully Demonstrated”. The Site Visit Team should discuss each
of these and, as a group, determine a pre-site visit team assessment. This team
assessment will be recorded in e-PHAB.
Based on these discussions, the Site Visit Team may develop a request for additional
documentation and/or may generate questions to ask the health department, pre-site
visit. These questions and/or requests will be forwarded to PHAB staff by the Site Visit
Team Chair, via e-PHAB. The health department will be provided no fewer than four
weeks to gather and submit additional documentation and to develop responses to
questions.
Any additional documentation that is accepted must have been developed, finalized, and
in use by the health department at or before the date of their original submission of
documentation to PHAB. That is, the health department may not submit documentation
that was developed or finalized between their original submission of documentation and
the pre-site request for additional documentation.
d. Pre-Site Visit Conference Call Four weeks after the documentation request and/or questions were forwarded to the
health department (or sooner, if possible, based on the health department’s response),
the Site Visit Team will conduct a third teleconference to prepare for the site visit. This
will be the final teleconference meeting of the Site Visit Team before the site visit.
In preparation for the call and for group discussion, each member will prepare and
organize a list of questions or issues to be raised during on-site interviews specific to the
documentation provided for the measures in the Domain they have been assigned.
Questions or issues may pertain to, for example:
Adequacy of documentation;
Appropriateness or relevance of documentation;
Documentation that is similar to, but not the same as, required
documentation;
Timeliness of the documentation, based on the timelines in the PHAB Standards and Measures Version 1.0;
Areas where clarification or explanation is required in order to understand
the applicability of the documentation;

PHAB Site Visitor Guide Version 1.0
March 2012 Page 17
Areas where clarification or explanation is required in order to understand
how the health department operationally meets the standards and measures;
and
Documentation for which additional samples will be requested (additional
program areas, additional examples, etc.).
In addition, the Site Visit Team will consider themes and trends in the pre-site visit
assessment of the health department’s conformity with the measures and prepare a list
of general questions or issues to be raised during the on-site interviews. These
questions or issues may be weaved into the Domain specific discussions as well as
raised during interviews with the health department’s leadership.
During this conference call the Site Visit Team will also review the site visit agenda and
review each team member’s roles and responsibilities. PHAB will provide an agenda that
will be organized by Domain (See Appendix B for the Agenda template). In addition, final
travel logistics and connections will be discussed during this call (see Section V, 3
below).
3. Scheduling and Logistical Arrangements PHAB staff will schedule the site visit at a time that is practical and agreeable for all parties
involved. The schedule of the site visit will allow sufficient time for the completion of the steps
described above.
PHAB staff will impress upon the health department’s Accreditation Coordinator the importance
of ensuring that all key staff involved in the accreditation application will be available for
interviews and meetings in accordance with the site visit agenda. This will include key staff from
any other agencies that provide public health services through agreements or contracts cited as
evidence of conformity to specific standards. It will also include representatives of the governing
entity and community partners.
PHAB staff will make all necessary travel arrangements and provide site visitors with travel
details. Site visitors should plan to depart from their starting location the day prior to the first day
of the site visit and arrive at the hotel for a team meeting that evening. Special travel needs or
requests should be communicated to PHAB upon acceptance of a site visit assignment,
including but not limited to dietary restriction or special travel or lodging needs. Members of Site
Visit Teams will share cell phone numbers so that they can communicate as they travel to the
site. PHAB will ask that each site visitor provide emergency contact information to be used if the
need arises.
Site visitor travel expenses for the site visit will be reimbursed by PHAB, in accordance with
PHAB’s Travel Policies and Procedures (Appendix G).

PHAB Site Visitor Guide Version 1.0
March 2012 Page 18
4. Health Department Preparations Health departments will be instructed by PHAB to prepare for the site visit. Health departments
will be instructed to:
Schedule a private meeting room to serve as “home base” for the Site Visit Team that
will be available to them for the duration of the site visit. Ensure that the room that is provided to the Site Visit Team contains a table that is large
enough for the team to sit with laptops and papers and to also conduct group interviews. Provide Wi-Fi internet access and appropriate passwords to the members of the Site
Visit Team. If Wi-Fi is not available, then the health department should set up four
laptops that are connected to the internet. Provide a working projector and screen in the meeting room so that the team may view
e-PHAB page or documentation together, at the same time. Ensure that the appropriate health department staff and partners have been notified and
will be available to the Site Visit Team.
Ensure that interviews are scheduled to be held in private offices or rooms.
Ensure that the health department director and Accreditation Coordinator will be
available for the duration of the site visit.
Notify the building receptionist to expect the Site Visit Team and know where to direct
them.
Health departments will be cautioned that they may not offer additional or more recent
documentation; they may only submit additional documentation in response to requests from the
Site Visit Team.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 19
VII. Site Visit
1. Focus of Site Visit The focus of the Site Visit Team is on gathering information to:
Understand the documentation received through e-PHAB and how it is applicable to
each measure,
Identify where documentation is missing or insufficient,
Learn about the operations of the health department,
Understand the culture of the health department,
Develop a sense of the health department’s effectiveness in addressing the Essential
Public Health Services,
Identify exemplary practices, and
Articulate department opportunities for improvement.
Validation of documentation is accomplished through interviews and discussions. Site Visit
Team members will make observations and draw conclusions. Site Visit Team members will
meet with a range of stakeholders, including various levels of health department staff,
representatives of the health department governing entity, representatives of partner
organizations, and representatives of community partners.
2. Site Visit Process Site visits will typically last two to three days, depending upon the size and complexity of the
health department, satellite sites, and the scope of the documentation. The site visit will consist
of an entrance and exit conference, a series of interviews, a walk-through, and Site Visit Team
executive sessions.
The Site Visit Team Chair will lead the work of the team on-site, act as spokesperson, and lead
all meetings involving Site Visit Team members. The Site Visit Team Chair will manage a
consensus process to incorporate all team members’ feedback and opinions into the Site Visit
Report. The Site Visit Team Chair will review and approve the Site Visit Report before it is
submitted to PHAB.
Each site visitor should take notes on discussions concerning the Domains to which they have
been assigned. They will be responsible for writing the portions of the site visit that relate to
those Domains.
a. Other Site Visit Attendees Health departments may invite observers or participants to the site visit. For example,
they may wish to invite a community partner to a portion of the site visit to speak about
how they work with the health department specific to a Domain or standard. They may
invite a consultant with whom they have been working to prepare for accreditation.
PHAB Accreditation Specialists will attend site visits. They will provide consultation and
any technical assistance as needed by the Site Visit Team concerning interpretation

PHAB Site Visitor Guide Version 1.0
March 2012 Page 20
and/or intent of standards, measures, and guidance for documentation; or concerning
the site visit process. They will be available to coordinate logistical assistance with travel
or other scheduling concerns.
3. Site Visit Agenda a. Site Visit Agenda Development PHAB has developed a standard site visit agenda that will be the template for all site
visit agendas. The order of the sessions and the times allotted for each of the interviews
and discussions may be altered to accommodate the needs of the health department
and the Site Visit Team. For example, a key health department staff person may have a
major or leadership role in more than one Domain. PHAB will work with the health
department to not schedule meetings on those Domains concurrently. PHAB will also
work with the health department to accommodate representatives of the governing
entity, partner organizations, or community partners.
PHAB will also work with the Site Visit Team to ensure that Domains requiring more
review time are allotted more time on the agenda. Any concurrent meetings will take into
account Domain assignments. There may be some Domains that the team determines
should be reviewed by the whole team, due to the number or complexity of issues. The
Team may consider visiting additional physical sites or facilities that the health
department would like the Site Visit Team to visit.
In addition to interviews and discussions based on Domains, the agenda will include
several general sessions: an entrance and exit conference and a walk through. The
agenda will also include Executive Sessions which are private meetings of the Team
without health department representation. (See description below.)
Site visitors should adhere to the site visit agenda and times as a means of respecting
the time and ongoing responsibilities of health department staff, governance
representatives, and any invited community stakeholders. Adhering to the PHAB
approved agenda also contributes to a more standardized process for all health
department applicants.
b. Agenda Contents The agenda will include the following specific sessions:
Pre-Visit Team Meeting The Site Visit Team will hold a team in-person meeting the evening prior to the
first day of the site visit. This meeting provides an opportunity for the team
members to become acquainted with each other and the PHAB Accreditation
Specialist, follow-up on review that has been completed and questions that have
been articulated since the team’s conference call, and raise any additional
concerns identified during the pre-site visit review process. All documentation
needs that have not been previously communicated to the Site Visit Team Chair
PHAB Site Visitor Guide Version 1.0
March 2012 Page 21
should be shared at this time. The Site Visit Team should review the site visit
agenda and the Site Visit Team Chair will advise the team of how s/he intends to
run the interviews and answer any questions posed by team members. Finally,
the Site Visit Team should review the plans for the development of the Site Visit
Report to ensure that each Site Visit Team member knows their responsibilities.
Entrance Conference The purpose the entrance conference is to make introductions, establish
expectations, and establish a collegial tone. Specifically, the meeting should
include the following items:
Introductions of Site Visit Team Chair and members, the health
department’s Accreditation Coordinator, the PHAB Accreditation
Specialist, and health department leadership (other health department
staff also present, as appropriate);
Review of the purpose of the site visit;
Review of the site visit process, agenda, and schedule;
Summary of the next steps (Site Visit Report, accreditation decision,
and notification);
Receive an overview of the health department; and
Discuss recent changes that impact on the health department about
which the Site Visit Team should be aware.
See Entrance Conference Talking Points (Appendix C).
Walk-through
A health department staff member will guide the Site Visit Team on a walk-
through of the physical facilities of the department. The walk-through may
include introductions of various health department staff. The purpose of the walk-
through is to provide the Site Visit Team with an overall picture of the health
department’s environment, atmosphere, and working conditions. Site Visit Team
members should note the general lay-out of the health department, the space
provisions, and records storage. If the health department operates a public health
laboratory and it is located in close proximity the central office of the health
department, the laboratory should be included in the walk-through. The Site Visit
Team should pay particular attention to areas listed in PHAB’s “Visual
Observation Guidance” (Appendix E).
Interviews and Document Review The majority of the site visit will consist of interviews and discussions. The
purpose of interviews is to confirm evidence provided by the documentation, gain
a context for the documentation, and improve understanding of what process and
procedures the documentation represents. The interviews provide the
opportunity to ask questions and clarify how the documentation demonstrates

PHAB Site Visitor Guide Version 1.0
March 2012 Page 22
conformity with the measure. The Site Visit Team should review any areas that
require clarification or explanation with the health department’s staff. It is vitally
important that the interviews and conversations stay on the subject matter related
to accreditation.
The Site Visit Team members will individually interview health department staff
concerning the documentation for the Domains that they have been assigned.
There may be some Domains that the team determines would be reviewed by
two or all members of the Site Visit Team due to the number or complexity of the
questions or if there is overlap of issues across Domains. This will have been
determined when the agenda was finalized with input from the Site Visit Team.
During general sessions and group interviews, team members are encouraged to
ask questions and participate in Site Visit Team dialogue across all standards,
even though each site visitor will have specific Domains of standards assigned to
them.
The Site Visit Team will interview a variety of individuals, including the senior
level management of the health department, program managers, representatives
of the governing entity, directors and/or staff of partner organizations,
representatives of community partners, and others. If the health department
operates a public health laboratory, the team should interview the director and/or
the Quality Assurance Officer of the laboratory.
Site visitors should seek to have open and frank discussions that clarify and
expand on information provided by the documentation. All interviews and
discussions should be conducted in a professional and cordial manner.
Interviews should be held in a private office or room so that the exchange of
information can be confidential. Interviewers should not make comments about
the information. They should not provide information about personal or
professional experiences or about other health departments. They should not
offer critiques or suggestions for improvements. These interviews are part of a
fact-finding process. (See the Interview Guidance, Appendix F for more
information.)
On-site Additional Documentation Members of the Site Visit Team may request additional documentation and
additional examples. The Site Visit Team may want to see documentation from
additional program areas to provide evidence of health department-wide
conformity with measures. The Site Visit Team may request additional
documentation to provide evidence of the measure being met as a standard way
of operating.
When documentation does not demonstrate conformity with a measure, the Site
Visit Team MAY NOT suggest specific types of documentation that might provide

PHAB Site Visitor Guide Version 1.0
March 2012 Page 23
stronger evidence of conformity with the measures. They may only ask for
additional documentation.
The health department MAY NOT OFFER additional documentation, but may
only respond to the Site Visit Team’s request for additional documentation. There
may be instances that a health department identifies more appropriate
documentation for a measure after they submit their documentation to PHAB.
However, PHAB will not accept additional documentation from a health
department unless specifically requested by a site visitor.
Any additional documentation that is accepted during the site visit must have
been developed, finalized, and in use by the health department at or before the
date of their original submission of documentation to PHAB. That is, the health
department may not submit documentation that was developed or finalized
between their original submission of documentation and the site visit.
Additional documentation accepted by the Site Visit Team must be submitted by
the health department electronically through e-PHAB. No paper documentation
will be accepted.
All requests for additional documentation from the Site Visit Team must be
communicated to the Accreditation Specialist on-site so they may re-open the
appropriate measures in e-PHAB for the Health Department. Site visitor requests
for additional documentation made during the site visit and the health
department’s responses must be submitted prior to the last executive session
that is scheduled immediately before the exit conference. After this time, the
health department’s Documentation Submission section in e-PHAB will be
locked.
Executive Sessions The agenda will include executive sessions throughout the visit. These sessions
are included to provide the Site Visit Team with opportunities to discuss their
observations and preliminary findings, and to evaluate its progress and make any
necessary revisions to the agenda or requests for information. Executive
sessions also provide opportunities to prepare clear and succinct comments for
end of day and for the exit conferences. These meetings ultimately serve as the
opportunity for the Site Visit Team to reach consensus on assessments for each
of the measures.
The Site Visit Team should hold an executive session at the end of day one. The
Site Visit Team should review the day’s work and findings and make any
changes to the agenda for day two that may be indicated. Additional questions
may be generated and more documentation may be identified for requests.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 24
The Site Visit Team should, during its executive sessions throughout the site
visit, reach consensus and begin the development of the contents of the Site Visit
Report. Before the exit conference, the Site Visit Team should come to
agreement about the findings. If there are differences in perceptions or
conclusions among the team, they should discuss them and reach a consensus
on the statement of findings.
The Site Visit Team may not make a recommendation regarding accreditation status during the visit, during the exit conference, or in the Site Visit Report.
Exit Conference
The Exit Conference is the final meeting of the site visit. The attendees will
probably be the same individuals who attended the Entrance Conference, though
the health department may wish to invite others. A health department may issue
an open invitation to all of the department staff to attend the Exit Conference.
The purpose of the Exit Conference is to review identified strengths, areas of
potential non-conformance and/or opportunities for improvement as known at the
conclusion of the site visit. The Site Visit Team will not make any recommendation regarding accreditation status during the site visit or during the exit conference. The exit conference points should be consistent with the content of the Site Visit Report. The health department should not be surprised by any differences in observations. (See Appendix
D for Exit Interview Talking Points.)
SITE VISITOR TIPS
Be thoroughly prepared. Read PHAB’s materials. Review the PHAB Standards and Measures
Version 1.0 and the National Public Health Department Accreditation Documentation Guidance Version 1.0.
Always remember that the purpose of public health department accreditation is quality and
performance improvement.
Create a professional, cordial atmosphere during the site visit among the Site Visit Team
members and with the health department.
Go to the site visit with an open mind.
Gather as much information as you can.
Be as specific as possible in the Site Visit Report, so the PHAB Accreditation Committee can
make a well informed determination of accreditation status.
Be aware that health departments can have unique organizational structures, may require
different operational approaches, and may meet the measures in various ways.
Review the PHAB travel reimbursement policies before you travel. (Save all receipts!)

PHAB Site Visitor Guide Version 1.0
March 2012 Page 25
VIII. Documentation Review Guidance Before the health department’s documentation is provided to site visitors for their review, a
PHAB Accreditation Specialist will review the health department’s documentation for
completeness. PHAB Accreditation Specialists will NOT assess the documentation for
conformity with the measure or its documentation requirements. Accreditation Specialists will:
Determine if documents are dated; they will not assess whether the documentation
meets the required timeframe;
Review the documentation for required signatures, department logos, or other evidence
of authenticity;
Determine if the required number of examples is submitted; and
Check with the health department to determine whether missing documentation was
intentional.
1. Documentation Assessment for Each Measure Site Visit Team members will review the documentation several times through the site visit
process:
Each team member will individually review the documentation for each measure in the
Domains they have been assigned. They will note all measures that are not clearly met.
The Site Visit Team will meet on a conference call and review issues identified through
the initial individual team members’ review. The Team will form questions and requests
for additional documentation that they will submit to PHAB. PHAB will contact the health
department for additional information, which the Site Visit Team will review prior to the
Site Visit.
A final review of documentation will occur during the Site Visit. The Site Visit Team may
request additional documentation during the Site Visit. The Site Visit Team may identify
“Areas of Excellence” and “Opportunities for Improvement” for each measure. At the end
of the site visit, a consensus assessment will be made by the Site Visit Team for the
development of the Site Visit Report.
To develop the Site Visit Report, the Site Visit Team will assess the documentation for each
measure and will assign one of four ratings, as described in Section 2 below. The Site Visit
Report will include written descriptions of how the documentation meets the requirements. It will
also note “Areas of Excellence” and “Opportunities for Improvement” for each measure. The
Site Visit Team may identify opportunities for improvement, even when a measure is “Fully
Demonstrated.”
When assessing documentation, the Site Visit Team should review the measure, the “Purpose”
of each measure, and the standard to ensure that the intent of the measure is being
demonstrated by the documentation. While the Site Visit Team is expected to look for
conformity with the specifics of the measures and required documentation, including the
required number of examples and timeframes for dates of documents, the priority of the team
should be to use their public health experience and expertise to ensure that the intent of the
measure is met. Some requirements for the number of examples or the timeframes of the

PHAB Site Visitor Guide Version 1.0
March 2012 Page 26
documentation may be open to interpretation. Site visitors should be flexible when considering
how the department demonstrates that it is in conformity with the requirements and the
measure.
The review of documentation is a qualitative, not quantitative. Assessment of conformity with
each measure will be based on the team members’ review and careful consideration of the
documentation and health department’s notes, and their careful review of the requirements and
guidance contained in the PHAB Standards and Measures Version 1.0. Assessment will be a
judgment call of the Site Visit Team based on the team members’ practical public health
experience with how a health department effectively operates, their public health expertise, and
their common sense interpretation of the intent of the requirements in the PHAB Standards and Measures Version 1.0. There will be no numerical score attached to the ratings. Numbers
or percentage of measures met or not met will not be calculated.
In assessing the documentation, the Site Visit Team should keep in mind the notion of “the letter
of the law versus the intent of the law.” The Site Visit Team should keep in mind that the “intent
of the law” of the PHAB Standards and Measures Version 1.0 is continuous quality
improvement. Accreditation through PHAB is not a regulatory process.
2. Assessment Categories The four categories of ratings for each measure are:
Fully Demonstrated: In the professional judgment of the Site Visit Team members,
documentation is assessed to be complete, providing evidence of conformity with all of
the required documentation and the measure is Fully Demonstrated.
Largely Demonstrated: In the professional judgment of the Site Visit Team members,
documentation is assessed to be close to complete and conformity with the measure is
Largely Demonstrated. For example:
Documentation is missing from less than half of multiple requirements for a
measure.
Documentation is missing from less than half of the elements or specified
characteristics of the required documentation.
There is evidence that the health department does not meet the measure in one
or more programs or sections of the department.
Slightly Demonstrated: In the professional judgment of the Site Visit Team members,
documentation is assessed to be minimal and conformity with the measure is only
Slightly Demonstrated. For example:
Documentation is provided for fewer than half of multiple required documentation
items for a measure.
Documentation is provided for fewer than half of the elements or specified
characteristics of the required documentation.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 27
There is evidence that the health department meets the measure in a small
selection of programs or sections of the department.
Not Demonstrated: In the professional judgment of the Site Visit Team members,
documentation is assessed as providing no evidence of conformity with the required
documentation and conformity with the measure is Not Demonstrated.
When the Site Visit Team develops the Site Visit Report, the team will include comments on the
documentation and how it meets the measure. The Site Visit Team may comment on any
measure, but must comment on measures that are rated less than “Fully Demonstrated.”
There is no measure that can be determined to be “not applicable.” All health departments are
to be assessed for all measures.
3. Quality and Performance Improvement The intent of the accreditation process is to encourage continuous quality improvement during
all phases of working towards and demonstrating conformity with the PHAB standards and
measures. Additionally, Domain 9 of the standards focuses on evaluation and continuous
improvement of health department processes, programs, and interventions. Site visitors,
therefore are charged with the identification of areas of excellence and opportunities for
improvement as they assess documentation. The site visit process is not limited to the
determination of conformity to the measures; it has been designed to also assist health
departments identify areas of improvement (even for measures that are met) and support areas
of excellence.
4. Standards and Measures
The PHAB Standards and Measures Version 1.0 provides guidance for Site Visit Teams as
they review documentation submitted by applicant health departments, conduct discussions with
health department staff during the site visit, and develop the Site Visit Report. Credibility in
accreditation results from consistent interpretation and application of defined standards and
measures.
The PHAB Standards and Measures Version 1.0 sets forth the Domains, standards,
measures, and required documentation adopted by the PHAB Board of Directors. The
document also provides guidance on the meaning and purpose of a measure and the types and
forms of documentation that are appropriate to demonstrate conformity with each measure.
There is a “Purpose” statement for each standard and measure, a “Significance” statement for
each measure, and narrative guidance specific to each required documentation item.
The PHAB Standards and Measures Version 1.0 provides assistance to site visitors as they
work to assess the documentation for conformity with the measures. PHAB site visitors must
pay close attention to this document when assessing if documentation demonstrates conformity
with a measure.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 28
5. Applicability of Public Health Accreditation Standards PHAB’s public health department accreditation standards address the array of public health
functions set forth in the ten Essential Public Health Services. Health department accreditation
standards address a range of core public health programs and activities including, for example,
environmental public health, health education, health promotion, community health, chronic
disease prevention and control, communicable disease, injury prevention, maternal and child
health, public health emergency preparedness, access to clinical services, public health
laboratory services, management/administration, and governance. Thus, public health
department accreditation gives reasonable assurance of the range of public health services that
a health department should provide.
While some public health departments provide mental health, substance abuse, primary care,
human, and social services (including domestic violence), these activities are not considered
core public health services under the ten Essential Public Health Services framework used for
accreditation purposes. PHAB’s scope of accreditation authority does not extend to these areas.
Documentation from these program areas are not generally accepted for public health
department accreditation. Similarly, documentation from health care facilities and professional
licensing programs and the administration of health care financing systems (e.g., Medicaid)
cannot be used for public health department accreditation purposes.
6. Types and Formats of Documentation Health departments vary in size, organizational structure, scope of authority, resources,
population served, governance, and geographic region. PHAB does not intend to be prescriptive
about how or what the health department does to meet the standards and measures. The focus
of the standards, measures, and required documentation is on “what” the health department
provides in services and activities, irrespective of the organizational structure.
Documents developed through a variety of methods are acceptable. Documentation may be, for
example:
Documents developed in-house by health department staff,
State health department documents used by local health departments and local health
department documents used by state health departments,
Documents developed by community partnerships or collaborations of which the health
department is a member,
Partners such as non-profits and academic institutions with which health departments
have working agreements, or
Purchase-of-service providers with which the health department has contracted.
The purpose of documentation review is to confirm that materials exist and are in use in the
health department being reviewed, regardless of who originated or developed the material.
Documentation should be representative of a variety of department programs. Both
administrative and program activities are appropriate for documentation to meet various
measures. Overall, documentation should demonstrate conformity in a variety of programs to

PHAB Site Visitor Guide Version 1.0
March 2012 Page 29
illustrate department-wide activity. Documentation should include programs that address chronic
disease. Documentation should address the needs of the population in the jurisdiction that the
health department has authority to serve.
Generally, types of documentation that are acceptable to demonstrate conformity include:
Examples of policies and processes: policies, procedures, protocols, standing
operating procedures, emergency response/business continuity plans, manuals,
flowcharts, organization charts, and logic models.
Examples of documentation for reporting activities, data, decisions: health data
summaries, survey data summaries, data analyses, audit results, meeting agendas,
committee minutes and packets, after-action evaluations, continuing education tracking
reports, work plans, financial reports, and quality improvement reports.
Examples of materials to show distribution and other activities: email, memoranda,
letters, dated distribution lists, phone books, health alerts, faxes, case files, logs,
attendance logs, position descriptions, performance evaluations, brochures, flyers,
website screen prints, news releases, newsletters, posters, and contracts.
Site visitors should also be aware that:
In many cases a single department document is required (for example, a department-
wide policy or procedure). Where documentation requires examples, health departments
must submit two examples, unless otherwise noted in the list of required documentation
or guidance for each measure.
Some measures require that “policies and procedures” or “protocols” be submitted. It
should be acknowledged that many times “policies and procedures” or “protocols” are
actually one document, a “policies and procedures manual.” Two examples may or may
not be required, depending on the specifics in the guidance.
Documentation submitted to demonstrate conformity to a measure does not have to be
presented in a single document; several documents may support conformity to a single
measure.
A single document may be relevant for more than one measure and may be submitted
multiple times.
Documentation must directly address the measure. When reviewing documentation, the
site visitor should carefully consider the standard and Domain in which the measure is
located, as well as the measure itself.
Centralized states and their local health department applicants may submit shared
documentation (specific training on these submissions will be provided to site visitors as
appropriate).
Further PHAB guidance concerning documentation can be found in the National Public Health Department Documentation Guidance Version 1.0.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 30
7. Visual Observations of Documentation In a few cases, where a document is excessively large (for example, Measure 11.1.4 A,
Required Documentation 1, a Human Resources Policies and Procedures Manual; Measure
2.1.5 A, Required Documentation 2, copy of laws), the health department may submit a table of
contents or a description of the document in e-PHAB. In these cases, the site visitors will need
to make a point of seeing the document during the site visit.
Visual observation may be needed to verify description of availability of documents to staff. For
example, a health department may say that the human resources policy and procedures manual
is accessible to staff in the reception area of the human resources department (Measure 11.1.1
A, Required Documentation 4, description of methods for staff access to department policies
and procedures). The Site Visit Team should confirm that the manual or policies are in fact
accessible to staff in that location.
On the other hand, the health department may say that a manual, policies, or position
descriptions are available to staff via an intranet (For example, Measure 11.1.2A, Required
Documentation 1, Confidentiality Policies Measure; 11.1.5 A, Required Documentation 3,
Position Descriptions). Site visitors should verify that the documents are available through the
intranet by being provided a demonstration during the site visit.
A few of the measures require direct visual observation.
Measure 3.2.1 A, Required Documentation 2: “Documentation of branding or
communication of presence of health department.”
The Site Visit Team should supplement the submitted documentation with visual
observations of signage inside and outside the health department.
Measure 3.2.5 A, Required Documentation 3: “Availability of assistive staff or technology
devices to meet ADA requirements.”
The Site Visit Team should supplement the submitted documentation with their visual
observations of TTY or other assistive technology.
Measure 11.1.7: “Maintain facilities that are clean, safe, accessible, and secure.”
The Site Visit Team should supplement the submitted documentation with their visual
observations of the facilities.
Measure 11.1.6 A, Required Documentation 1: “Demonstrate the use of technology to
support public health functions.”
The Site Visit team should supplement the documentation with their visual observations
of the use of technology.
8. Additional Interviews and Discussions Site visitors are encouraged to speak with representatives of the governing entity, partner
organizations, and community partners, as well as with health department staff. Some of these
conversations may be informal discussions, for example, during a walk-through of the
department. Other discussions will part of the formal site visit agenda.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 31
a. Community Partners The site visit agenda will include a meeting with representatives of community partners.
Community partners are the organizations, collations, partnerships, etc. with which the
health department coordinates to improve the health of the jurisdiction it serves.
Community partners may include for example, the school system, members of the faith
community, representatives of local businesses, recreational organizations, or private
citizens. This meeting will provide the site visitors with the opportunity to further assess
the health department’s conformity with measures that relate to, for example,
involvement in a partnership to develop the community health assessment (Measure
1.1.1), provision of data reports to communities (Measure 1.3.2), and general
engagement with the community (Domain 4). The health department will be responsible
for selecting and inviting community partners to participate in appropriate portions of the
site visit. The health department may choose to invite community representation to
participate in other agenda items, such as the discussion that addresses the
development of the community health assessment or the review of Domain 4.
b. Partner Organizations The site visit agenda will also include a meeting with representatives of partner
organizations. Partner organizations are those organizations with which the health
department has a formal relationship for the provision of public health activities. Partner
organizations may include, for example, an academic institution with which the health
department has a formal agreement (MOU, contract, etc.) to collect data and develop
data reports. A partner organization may be a school system with the health department
has a formal agreement for the provision of on-site immunization clinics or health
education sessions.
Partner organizations specifically include other levels of health departments in the state:
Tribal, state and local. That is, if the site visit is of a state health department, the site
visitors will meet with representatives of local, district or regional health departments in
the state. This will be required for both centralized and decentralized states. If health
departments of Federally Recognized Tribes are located in the jurisdiction served by the
health department being reviewed, then the Site Visit Team should meet with
representatives of some or all of the Tribes. Likewise, if the site visit is of a local health
department or Tribal health department, then the Site Visit Team should meet with
representatives of the state health department. These meetings will provide the site
visitors with the opportunity to further assess the health department’s conformity with
measures that relate to, for example, the distribution of health data profiles (Measure
1.4.2), the state’s provision of consultation, technical assistance and information
regarding disease outbreaks (State Measure 2.1.6), or collaboration for rapid detection,
investigation, and containment/mitigation of public health problems and hazards
(Measure 2.3.4). The health department will be responsible for inviting partner
organizations, including other level health departments, to participate in the site visit.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 32
c. Representatives of the Governing Entity The site visit agenda will also include a meeting with representatives of the health
department’s governing entity, if appropriate. In some cases the governing entity may be
a governor, mayor, or board of county commissioners, and they may or may not be
available for a meeting with the Site Visit Team; in such cases, the health department
should invite representatives of the governing entity. Meetings with representatives of
the governance entity will provide the site visitors with the opportunity to further assess
the health department’s conformity with measures that relate to, for example, informing
governing entities of the impact of policies (Measure 5.1.3), information to governance
concerning needed updates/amendments to laws and/or proposed new laws (Measure
6.1.2), and maintenance of capacity to engage the governing entity (Domain 12).

PHAB Site Visitor Guide Version 1.0
March 2012 Page 33
IX. Site Visit Report
1. Site Visit Report Contents The Site Visit Report provides the information on which the PHAB Accreditation Committee will
base its accreditation status decision. The Accreditation Committee will not review the health
department’s documentation. The Site Visit Report will be developed and submitted to PHAB in
e-PHAB. The Site Visit Report, for the most part, will be developed during the executive
sessions of the site visit.
The documentation submitted by the health department, along with site visit discussions, visual
observations, and additional information gathered, is the basis for the Site Visit Report. The Site
Visit Report should present a clear representation of the department, its areas of strength, and
opportunities for improvement.
The Site Visit Team will develop an “assessment” of the department on its conformity with each
measure. The Site Visit Team will indicate their consensus concerning whether the department
has “Fully Demonstrated,” “Largely Demonstrated,” “Slightly Demonstrated,” or “Not
Demonstrated” conformity with each measure. The Site Visit Report will include comments
concerning how the documentation meets the measure. The Site Visit Report may comments on
any measure, but must provide an explanation for the rating of any measure less than “Fully
Demonstrated.”
The Site Visit Report will also recognize areas of excellence and identify opportunities for
improvement for each measure. The Site Visit Report will include a summary statement
concerning the health department’s meeting of each standard, based on the conformity with the
standard’s measures and a summary statement of the health department’s performance of the
Domain, based on the meeting of the standards in that Domain.
Finally, the Site Visit Report will summarize its findings by providing their impression of the
health department by stating (1) the health department’s three greatest strengths, (2) the health
department’s three most serious challenges or opportunities for improvement, and (3) their
overall impression of the department as a functioning health department.
The Site Visit Team will not make any recommendation regarding accreditation status in the Site Visit Report. Site Visit Reports will not be made available as part of the public record.
They should be considered confidential.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 34
SITE VISIT REPORT DEVELOPMENT TIPS
Focus your review and discussions around the measures and the
documentation. Your assessment should address the provision of evidence of
meeting the measure and not other aspects of the department or its operations.
The narrative of the Site Visit Report should be concise and direct.
The Site Visit Report should be fair, balanced, accurate and comprehensive.
Your assessment and Site Visit Report will be the basis for the PHAB
Accreditation Committee’s accreditation status decision.
2. Process and Timeframes The Site Visit Team Chair is responsible for managing the development of the Site Visit Report.
Each Site Visit Team member will responsible for developing the sections of the Site Visit
Report that pertain to the Domains they were assigned. The Site Visit Team Chair will review
the entire Site Visit Report, ensure that summary narratives are complete, and submit it to
PHAB (through e-PHAB).
The Site Visit Report must be submitted by the Site Visit Team Chair to PHAB within two weeks of the completion of the site visit. PHAB staff may edit the Site Visit Report and will confer with the Site Visit Team Chair, if significant edits are made. The final edited Site Visit Report will be sent to the health department.
The health department will have thirty days to review the Site Visit Report and cite any factual errors.
Applicants cannot submit additional documentation of corrective action(s) after the written Site Visit Report is received, but before the accreditation decision is made. The only exception to this rule is if the submission of a document will correct a factual error in the Site Visit Report.
Health department comments will become part of the official record that will be forwarded to the PHAB Accreditation Committee.
PHAB Staff will forward the final Site Visit Report to the Accreditation Committee of the PHAB
Board.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 35
X. Post-Site Visit
1. PHAB Accreditation Committee Accreditation Status Decision The Site Visit Team Chair is expected to be available for participation (by phone) in the meeting
of the PHAB Accreditation Committee at which the Site Visit Report will be reviewed. The Site
Visit Team Chair will be notified of the date and time scheduled for discussion and should
provide PHAB staff a phone number at which s/he can be reached. The Site Visit Team Chair
should notify PHAB staff immediately if there are scheduling conflicts with the scheduled date
and/or time. Another member of the Site Visit Team may be asked to be available to the
Accreditation Committee, if the Site Visit Team Chair cannot be available. 2. Evaluation Approximately one week after the site visit, site visitors will receive an online evaluation. Site
visitors are asked to evaluate other Site Visit Team members, PHAB staff support and
coordination of the site visit process, and the site visit process itself. Evaluative feedback should
be thoughtful and constructive in nature. PHAB uses evaluation feedback to make decisions
about appointment of individuals to Site Visit Teams, to identify ways to better serve health
departments seeking PHAB accreditation, and to modify PHAB policies and procedures. Site
visitors may also be asked to participate in inter-rater reliability assessments as appropriate.
3. Travel Reimbursement Site Visit Team members must submit signed Travel Reimbursement Forms (Appendix H)
with corresponding receipts to PHAB within 15 days after the travel has been completed. PHAB will not reimburse vouchers received which are older than 60 days or those that occur
after the end of a grant cycle. Travel is reimbursed in accordance with PHAB’s Travel Policies
and Procedures (Appendix G). Reimbursement must be requested using the PHAB Travel
Reimbursement Form.

PHAB Site Visitor Guide Version 1.0
March 2012 Page 36
Appendices
A. PHAB Site Visit Process
B. Site Visit Agenda Template
C. Entrance Conference Talking Points
D. Exit Conference Talking Points
E. PHAB Site Visitor Interview Guidance
F. PHAB Site Visitor Agreement Form
G. PHAB Travel Policies and Procedures
H. PHAB Travel Reimbursement Form
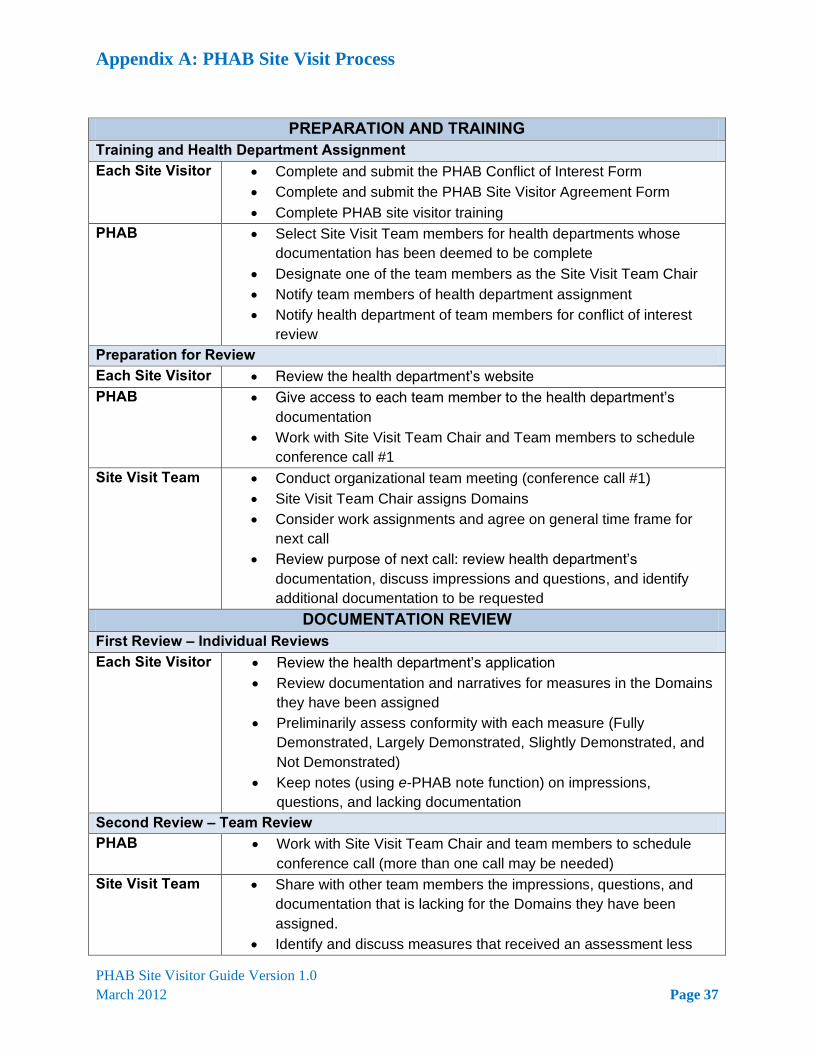
Appendix A: PHAB Site Visit Process
PHAB Site Visitor Guide Version 1.0
March 2012 Page 37
PREPARATION AND TRAINING Training and Health Department Assignment Each Site Visitor Complete and submit the PHAB Conflict of Interest Form
Complete and submit the PHAB Site Visitor Agreement Form
Complete PHAB site visitor training
PHAB Select Site Visit Team members for health departments whose
documentation has been deemed to be complete
Designate one of the team members as the Site Visit Team Chair
Notify team members of health department assignment
Notify health department of team members for conflict of interest
review
Preparation for Review Each Site Visitor Review the health department’s website
PHAB Give access to each team member to the health department’s
documentation
Work with Site Visit Team Chair and Team members to schedule
conference call #1
Site Visit Team Conduct organizational team meeting (conference call #1)
Site Visit Team Chair assigns Domains
Consider work assignments and agree on general time frame for
next call
Review purpose of next call: review health department’s
documentation, discuss impressions and questions, and identify
additional documentation to be requested
DOCUMENTATION REVIEW First Review – Individual Reviews Each Site Visitor Review the health department’s application
Review documentation and narratives for measures in the Domains
they have been assigned
Preliminarily assess conformity with each measure (Fully
Demonstrated, Largely Demonstrated, Slightly Demonstrated, and
Not Demonstrated)
Keep notes (using e-PHAB note function) on impressions,
questions, and lacking documentation
Second Review – Team Review PHAB Work with Site Visit Team Chair and team members to schedule
conference call (more than one call may be needed)
Site Visit Team Share with other team members the impressions, questions, and
documentation that is lacking for the Domains they have been
assigned.
Identify and discuss measures that received an assessment less

Appendix A: PHAB Site Visit Process
PHAB Site Visitor Guide Version 1.0
March 2012 Page 38
than “Fully Demonstrated”
Prepare a list of questions and requests for additional
documentation (focus on measures that have been “Partially
Demonstrated” and “Not Demonstrated”)
Recommend revisions to site visit agenda template, considering the
focus of questions and areas for discussions with the health
department
Health Department
Within four weeks, reply to the Site Visit Team’s questions and
requests for additional documentation
Work with PHAB to finalize site visit agenda
PHAB Finalize site visit agenda (taking into account Site Visit Team’s
priority focus areas, team members’ Domain assignments, health
department staff assignments, and community members’ and
governing entity’s schedules.
Schedule site visit and make travel arrangements
Third Review – Final Pre-Site Visit Review Site Visit Team List questions/issues for site visit
Identify themes and trends
Discuss final travel logistics and connections
SITE VISIT
Pre-Visit Team Meeting (Evening before site visit ) Site Visit Team Review site visit agenda
Raise any additional documentation needs or questions and
concerns
Review roles and plans for conducting meetings
Review process for the development of the Site Visit Report
Site Visit (Two days) Site Visit Team
Conduct:
Entrance Conference
Walk through
Interviews
Document review
Executive sessions
Exit Conference
Complete:
Assessment of measures
Identification of areas of excellence and opportunities for
improvement
SITE VISIT REPORT Develop Draft Site Visit Report Each Site Visitor For the most part, during the site visit Executive Sessions:
Assess measures in assigned Domains

Appendix A: PHAB Site Visit Process
PHAB Site Visitor Guide Version 1.0
March 2012 Page 39
Note areas of excellence and opportunities for improvement
Site Visit Team Chair
Reach consensus on: three greatest strengths, three most serious
challenges or opportunities for improvement, and the team’s overall
impression of the department as a functioning health department
Complete Site Visit Report and submit to PHAB within two weeks of
the completion of the site visit
Site Visit Report Review and Submission to PHAB Board PHAB May edit the Site Visit Report and send it Site Visit Team Chair for
review if recommended changes or questions substantial
Site Visit Team Chair
Review edited Site Visit Report to ensure content has not been
altered
PHAB Send edited Site Visit Report to health department
Health Department
Respond to PHAB within thirty days (citing any factual errors)
PHAB Forward the final Site Visit Report to the Accreditation Committee
Site Visit Team Chair
Site Visit Team Chair is available by phone during the Accreditation
Committee discussion, in case the Committee has questions or
requires clarification
POST-SITE VISIT Site Visitors Complete evaluation and submit to PHAB (within two weeks)
Submit travel reimbursement form and receipts within fifteen days of
the completion of the site visit
Complete other evaluations and provide feedback, as requested by
PHAB

Appendix B: Site Visit Agenda Template
PHAB Site Visitor Guide Version 1.0
March 2012 Page 40
This Site Visit Agenda Template is provided as a sample of a typical health department site visit. The template sets forth the agenda items that are to be included in every site visit. The Site Visit Agenda Template is not intended to be the absolute, unalterable agenda for every site visit. It is intended to be flexible to meet the specific needs of the Site Visit Team based on their review of the documentation. For example, the Site Visit Team may wish to spend less time on one particular Domain and more time on another, based on the volume of questions they have. The order and grouping of concurrent sessions to review documentation by Domain will need to be revised to accommodate the assignments of Domains to members of the Site Visit Team, so that no member is expected to attend two different Domain sessions at the same time. There are, however, a few agenda items that should never shift. Every site visit will begin with an entrance conference and end with an exit conference. After the entrance conference, the Site Visit Team will meet with health department staff to review the health department’s Community Health Assessment (CHA) and Community Health Improvement Plan (CHIP) and the standards and measures that relate to them. This will provide the site visitors an overview of the population served by the health department, plans to address the population’s health needs, and the health departments collaborative relationship with the community in the development and implementation of the CHA and CHIP. Immediately after the meeting concerning the CHA and CHIP, the Site Visit Team will meet with health department staff to review the department’s strategic plan and the standard and measures that relate to it. The health department staff may or may not be the same staff people that met with the Site Visit Team to review the CHA and CHIP. Review of the strategic plan will provide the Site Visit Team with an overview of the health department’s strategies, objectives, and plans to address the implementation of the CHIP and other organizational issues. Also, every site visit will include a meeting with representatives of community partners, a meeting with representatives of the governing entity, and a meeting with the health department director. The placement of these three meetings on the agenda may be repositioned to accommodate the schedules of community partners, the governing entity, and the health department director. Every agenda will also include several Executive Sessions, during which the Site Visit Team will meet to discuss their findings and prepare their Site Visit Report. The Site Visit Agenda Template is intended to be flexible to also meet the staffing and organizational structure of the health department. The order of the Domains may need to be shifted, based on a staff person’s area of responsibility and expertise. The order of other agenda items may also be adjusted. Specifically, the meetings with representatives of community partners and governing entities may need to be scheduled at different times than those proposed on this template. The health department is responsible for selecting the department staff that will attend each session. Likewise, they will be responsible for inviting representatives of their governing body and community partners.
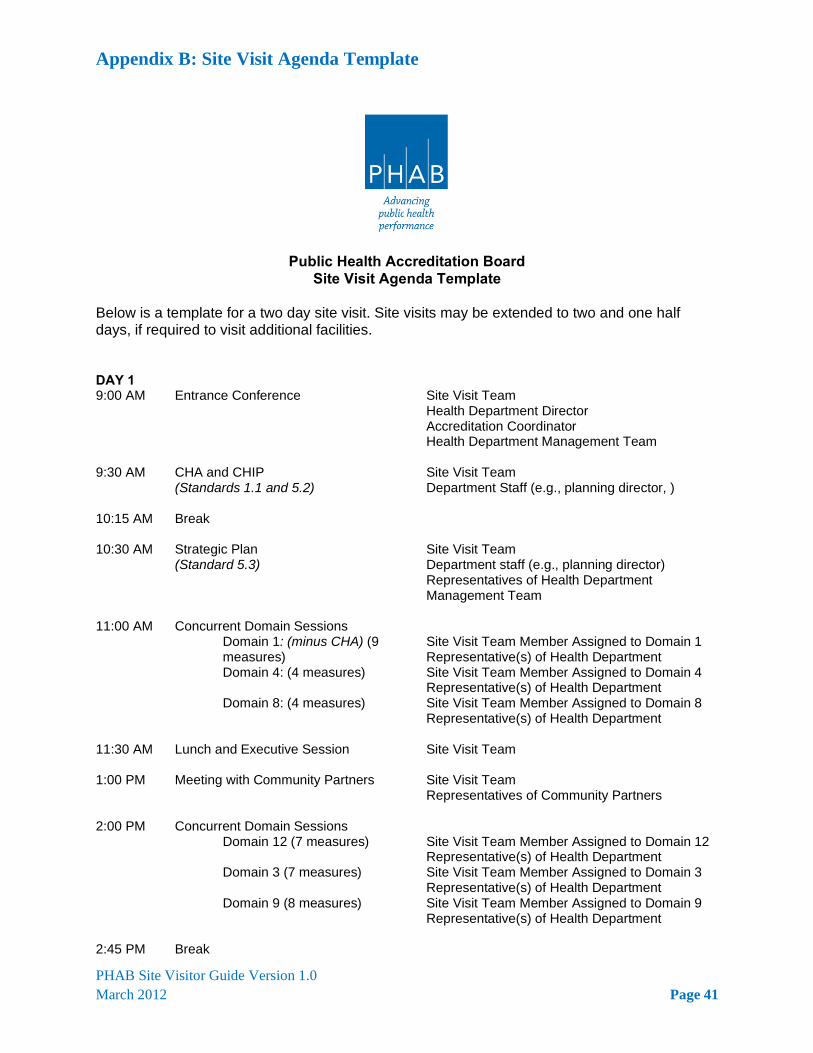
Appendix B: Site Visit Agenda Template
PHAB Site Visitor Guide Version 1.0
March 2012 Page 41
Public Health Accreditation Board Site Visit Agenda Template
Below is a template for a two day site visit. Site visits may be extended to two and one half days, if required to visit additional facilities. DAY 1 9:00 AM Entrance Conference Site Visit Team
Health Department Director Accreditation Coordinator Health Department Management Team
9:30 AM CHA and CHIP (Standards 1.1 and 5.2)
Site Visit Team Department Staff (e.g., planning director, )
10:15 AM Break
10:30 AM Strategic Plan (Standard 5.3)
Site Visit Team Department staff (e.g., planning director) Representatives of Health Department Management Team
11:00 AM Concurrent Domain Sessions Domain 1: (minus CHA) (9
measures) Site Visit Team Member Assigned to Domain 1 Representative(s) of Health Department
Domain 4: (4 measures) Site Visit Team Member Assigned to Domain 4 Representative(s) of Health Department
Domain 8: (4 measures)
Site Visit Team Member Assigned to Domain 8 Representative(s) of Health Department
11:30 AM Lunch and Executive Session Site Visit Team
1:00 PM Meeting with Community Partners Site Visit Team Representatives of Community Partners
2:00 PM Concurrent Domain Sessions Domain 12 (7 measures) Site Visit Team Member Assigned to Domain 12
Representative(s) of Health Department Domain 3 (7 measures) Site Visit Team Member Assigned to Domain 3
Representative(s) of Health Department Domain 9 (8 measures) Site Visit Team Member Assigned to Domain 9
Representative(s) of Health Department
2:45 PM Break

Appendix B: Site Visit Agenda Template
PHAB Site Visitor Guide Version 1.0
March 2012 Page 42
SITE VISIT AGENDA TEMPLATE CONTINUED
3:00 PM Concurrent Domain Sessions Domain 2 (17 Measures) Site Visit Team Member Assigned to Domain 2
Representative(s) of Health Department Domain 6 (10 Measures) Site Visit Team Member Assigned to Domain 6
Representative(s) of Health Department Domain 11 (11 Measures)
Site Visit Team Member Assigned to Domain 11 Representative(s) of Health Department
4:00 PM Executive Session
Site Visit Team
5:00 PM Adjourn
DAY 2 9:00 AM Executive Session
Site Visit Team
9:30 AM Concurrent Sessions Domain 7 (6 measures) Site Visit Team Member Assigned to Domain 7
Representative(s) of Health Department Domain 10 (6 measures) Site Visit Team Member Assigned to Domain 10
Representative(s) of Health Department Domain 5 (minus CHIP and SP)
(6 measures)
Site Visit Team Member Assigned to Domain 5 Representative(s) of Health Department
10:15 AM Break
10:30 AM Meeting with Representatives of Governing Entity
Site Visit Team Representative(s) of Governing Entity
11:30 AM Lunch and Executive Session
Site Visit Team
1:30 PM Meeting with Director of Health Department
Site Visit Team Health Department Director
2:30 PM Executive Session and Site Visit Report Development
Site Visit Team
3:30 PM Exit Interview
Site Visit Team Accreditation Coordinator Health Department Management Team Other Health Department Staff (invited by Health Department)
4:30 PM Adjourn

Appendix C: Entrance Conference Talking Points
PHAB Site Visitor Guide Version 1.0
March 2012 Page 43
The purpose the entrance conference is to establish a collegial tone, review the objectives and schedule of the site visit, and discuss any recent changes in the department about which the site visit team should be aware. Below are topics that should be addressed during the entrance conference.
Thank the health department for their support of public health department
accreditation, the work that they have dedicated to the process, and their hospitality.
Conduct introductions of the Site Visit Team Members, PHAB Accreditation Specialist,
health department leadership and staff, Health Department Accreditation Specialist, and others (that may be invited by the health department).
Describe PHAB’s conflicts of interest and confidentiality policies.
o Each PHAB site visitor has completed a Conflict of Interest Disclosure Form. o The health department has had an opportunity to review the names of their site
visitors and to indicate to PHAB any real or perceived conflict of interest. o PHAB and its site visitors will not share any information about the health
department, its application, and its documentation; the Site Visit Team’s interviews, review of documentation, findings, or impressions; or the health department’s accreditation status. When a health department receives full five-year accreditation, PHAB will notify the health department and then post the name of the health department on the PHAB website as public notice of the achievement. Site visitors have signed a confidentiality agreement with PHAB not to discuss their specific health department review with anyone other than PHAB staff, Accreditation Committee members (as requested) or their team members.
Review the purpose of the site visit. It is an opportunity:
o For the health department to be reviewed by peer public health practitioners. o For PHAB site visitors to verify the documentation submitted to PHAB by the
health department. o For site visitors to request further and additional documentation. (Documentation
that was created after the submission of the department’s documentation to PHAB will not be considered by the site visit team.)
o For discussion and explanation. o For the site visitors to supplement paper documentation with face-to-face
discussions and direct observations.
Review the site visit process, agenda, and schedule. o Verbally “walk through” the agenda and schedule. o State that the Accreditation Coordinator need not attend every interview, though
they must be available to the Site Visit Team for the duration of the visit. o Review the accommodations for the meetings (private meetings, conference
room for the Site Visit Team, rest rooms, soda and water vending machines, etc.)
Review the Site Visit Team’s process and guidelines for documentation review.
o Note that the team may not have time to review documentation for all measures with the health department; they will focus on missing documentation, perceived deficiencies, and questions.

Appendix C: Entrance Conference Talking Points
PHAB Site Visitor Guide Version 1.0
March 2012 Page 44
o Explain the four categories to be used for ranking each measure. Explain that numerical values will NOT be assigned to each ranking.
o Explain that a primary purpose of the site visit is to identify opportunities for improvement for the health department’s continuous quality improvement.
o Explain that the Site Visit Team will not make suggestions of actions or activities to address opportunities for improvement. The Site Visit Report may identify opportunities for improvement.
o Make it clear that the team will NOT recommend accreditation status at any time. o Explain that the site visit schedule includes an exit conference during which the
team will provide their overall impressions; review strengths, areas of potential non-conformance, and opportunities for improvement; and highlight observed strengths.
o The exit conference will be consistent with the final Site Visit Report findings.
Invite the health department leadership to provide an overview of the health
department, its programs, its structure, the population it serves, or any other pertinent information the health department would like the Site Visit Team to know.
Ask if there have been any changes or developments in the department since it
submitted its application for accreditation to PHAB about which the site visitors should know.

Appendix D: Exit Conference Talking Points
PHAB Site Visitor Guide Version 1.0
March 2012 Page 45
The exit conference is the last on-site session conducted by the Site Visit Team. The purpose of the exit conference is to provide the health department with a general summary and review of the site visit. It is an opportunity to provide feedback concerning the team’s assessment of strengths and opportunities for improvement. The health department director and the Accreditation Coordinator must attend the exit conference. The health department may invite others to attend the exit conference, if they wish including: department staff, representatives of their governing entity, representatives of community partners and partner organizations, and others.
Stress that the goal of the accreditation process is quality and performance improvement and that a culture of continuous quality improvement is the ideal.
Provide the team’s general impressions of the department’s conformity with the
PHAB standards and measures. o Share identified strengths, exemplary practices, unique or innovative methods. o Share identified opportunities of improvement. (Do not share suggestions for
ways to improve.)
Remind the health department of PHAB’s confidentiality policy.
Review the next steps of the accreditation process.
o The site visit team will submit its Site Visit Report to PHAB. o PHAB will share the Site Visit Report with the health department for a 30-day
review for inaccuracies. o At its next quarterly meeting, the PHAB Accreditation Committee will review the
Site Visit Report and determine the health department’s accreditation status.
Remind the health department that the Site Visit Team will not make any recommendation regarding accreditation status during the site visit, during the exit conference, in the Site Visit Report, to staff of PHAB, to members of the PHAB Board of Directors, or the PHAB Accreditation Committee.
Thank the members of the health department for their hospitality, time, and efforts of
all of their staff and partners. Thank the Accreditation Coordinator specifically.

Appendix E: PHAB Site Visitor Interview Guidance
PHAB Site Visitor Guide Version 1.0
March 2012 Page 46
I. INTRODUCTION The site visit is an opportunity to for the site visitors to ask specific questions and request further explanation in support of conducting the accreditation review. The health department will have an opportunity to present its structure and operation; describe its relationship with the community; explain the role and structure of its governing entity, and provide other qualitative information. This Guide presents general advice concerning the conduct of interviews during the site visit as well as provides sample questions for the Site Visit Team consideration. The purpose of the site visit interviews is to verify evidence provided by the documentation and to provide the opportunity to ask questions, request additional information, and clarify how the documentation provides the required evidence. The site visitors should review with the department’s staff any areas that require clarification or explanation. Each Site Visit Team should develop a list of specific questions appropriate for the department based on their review of the documentation that the health department submitted and the team has reviewed. The Site Visit Team should develop questions for specific Domains and individual and group interviews (i.e., health director, representatives of the governing entity, community partners). Interview questions should not relate to any subject matter that is not covered in the
PHAB Standards and Measures Version 1.0. II. GENERAL INTERVIEW GUIDANCE Interviews should be conducted in a professional and cordial manner. While site visitors will have a list of questions that they have developed to ask or issues to be covered, they should attempt to conduct the interview in a relaxed, conversational manner. Interviews should be held in a private room so that exchange of information can be maintained as confidential. Questions should be designed to gain information and understanding.
Questions should be clear, concise, and nonthreatening. Questions should be open ended to provide opportunities for descriptions and explanations. Questions should not imply values or judgments.
Site visitors should be active listeners, be observant, and check for understanding.
Site visitors should be aware of “clues” and attempt to follow up on what is not being said. Site visitors should be aware of body language and non-verbal feedback. Site visitors should allow time for the complete answer and not rush the person being interviewed.
Follow-up comments can often be revealing. Site visitors should encourage the person they are interviewing to provide additional information.
There are several methods that can be employed to encourage the provision of additional information:
Silent Probe An effective way to encourage someone to elaborate is to do nothing at all; just pause and wait. It suggests that you are waiting, listening for what they will say next.

Appendix E: PHAB Site Visitor Interview Guidance
PHAB Site Visitor Guide Version 1.0
March 2012 Page 47
Overt Encouragement Overt encouragement could be as simple as saying "Uh-huh" or "OK" after the respondent completes a thought. Try to do so in a way that does not imply approval or disapproval of what they said.
Elaboration You can encourage more information by asking for elaboration. For instance, ask "Would you like to elaborate on that?" or "Is there anything else you would like to add?"
Ask for Clarification Sometimes, you can elicit greater detail by asking the respondent to clarify what they said.
Repetition Repeat what you heard. This may elicit additional information as well as confirm your understanding.
Site visitors should not make evaluation comments about the information provided during an interview. They should not offer information about personal experiences, other professional experiences, or other health departments. They should not offer suggestions for improvements during the interviews. At the end of each interview, site visitors should always thank the person for their time, hospitality, and contributions to the site visit and accreditation process.
III. SAMPLE QUESTIONS The questions that the Site Visit Team poses during the site visit should be based on the Site Visit Team’s review of the health department’s documentation, the team’s preliminary assessment of the documentation, and the team’s need for additional information or clarification. The sample questions presented in this guide are suggestions for consideration by the Site Visit Team; they are not required.
A. General Questions a. What are the health department’s (or program’s) most significant contributions to
the health of the community? b. What are the health department’s (or program’s) strengths? c. What are the biggest challenges that the health department (or program) faces? d. What is the department’s (or program’s) relationship with the community?
B. Entrance Conference (See Appendix C, Entrance Conference Talking Points)
a. Have there been changes in the department since the department submitted your documentation?
b. Describe the governmental public health system in your community/state. c. Describe the department’s organizational structure. d. What significant public health services are provided by other organizations? How
does the health department coordinate with those organizations? e. (Local) What other public health resources exist in your community? How does
the health department coordinate with them?

Appendix E: PHAB Site Visitor Interview Guidance
PHAB Site Visitor Guide Version 1.0
March 2012 Page 48
f. What issues/topics/explanations should the Site Visit Team be aware of and/or keep in mind as they conduct the site visit?
C. Meetings On the CHA/CHIP/SP a. Describe how the community health assessment (CHA) was developed.
i. What was the overall process? ii. How was the community involved? iii. Do you have indications that the community uses the CHA for planning,
coordinating services and activities, sharing resources, funding applications, or other uses?
b. How was the community health improvement plan (CHIP) developed? i. What was the overall process? ii. How was the community involved? iii. How is the community involved in its implementation? iv. Do you have indications that the community uses the CHIP for their
program planning, coordinating services and activities, sharing resources, funding applications, or other uses?
v. Does the CHIP translate into the department’s annual budget? vi. Does the CHIP impact on resource requests or allocations? Is it
considered in setting priorities for grant applications or funding requests? c. How was the department’s strategic plan developed?
i. Who in the department was involved in its development? ii. How was the governing entity involved in its development? iii. How is it used by programs and leadership? iv. Does the strategic plan translate into the annual budget? v. Does the strategic plan impact on resource requests or allocations? Is it
considered in setting priorities for grant applications or funding requests?
D. Health Department Director a. Describe the public health system structure in your Tribe/state/community.
i. What is unique about the public health system and structure? ii. Describe how your health department fits within the Tribal/state/local
overall government structure. iii. Describe your department’s relationship with other public health
departments (Tribal/state/local health department(s)). b. Describe the department’s relationship with its governing entity.
i. Describe how the department and the governing entity work together on public health issues.
ii. Describe how does the department educates the governing entity about the mission and role of the department.
c. Describe the department’s relationship with the community. i. What is the department’s policy or process for working with the
community? How do programs obtain community input? ii. What examples are there of collaboration and partnership with the
community? d. How is the community health assessment and community health improvement
plan used? i. How does the health department use these documents? ii. Are there indications that the community uses the improvement plan for
priority setting, resource allocation, or other purposes?

Appendix E: PHAB Site Visitor Interview Guidance
PHAB Site Visitor Guide Version 1.0
March 2012 Page 49
e. How is the department’s strategic plan used?
E. Governing Entity Representatives a. Describe the relationship of the governing entity with the health department.
i. Describe the process for information exchange. ii. Describe the process for decision making.
b. Describe the working relationship of the governing entity with the community. i. How does the governing entity obtain community input?
c. What was the governing entity’s role in the development of the health department’s strategic plan?
i. What is the governing entity’s role in promoting and monitoring its implementation?
F. Community Partners a. Describe the relationship of the health department with the community at large.
i. How well does the community understand the mission and role of the department?
ii. How does the department communicate with the community? b. Describe your organization’s relationship with the health department.
i. In what areas does your organization partner and collaborate with the health department?

Appendix F: PHAB Site Visitor Agreement Form 2011-2012
PHAB Site Visitor Guide Version 1.0
March 2012 Page 50
Public Health Accreditation Board Site Visitor Agreement Form 2011-2012
Site Visitor Responsibilities As a site visitor of health departments on behalf of the Public Health Accreditation Board (PHAB), I will:
• be present, attentive, and participatory in all training, team meetings, site visit activities, and site visit interviews;
• arrive on time for training, conference calls, and meetings, and not leave early; • be prepared for all site visit activities; • be responsive to requests for information, comments, and feedback from PHAB; and • contribute to the completion of the team’s charge including review of the department’s
documentation submitted, preparation for and conduct of the site visit, and the completion of the team’s Site Visit Report.
Professional Conduct As a volunteer site visitor for the public health department accreditation program, I represent PHAB during all portions of the site visit process. As a site visitor, I will conduct myself in the highest professional and ethical manner at all times. I will be courteous and demonstrate respect and consideration for other team members, the health department, and department governance and community representatives. As a site visitor, I will not criticize any elements of the PHAB accreditation process or standards and measures in the presence of health department staff or members of the community. I will not criticize health departments’ operations, programs, or staff.
Confidentiality I will respect the confidential nature of the accreditation process. I will treat all information obtained through the accreditation review process as confidential, including the name of any health department to which I am assigned. I will not discuss information about the health department site or any of its documentation with others not involved in the PHAB accreditation process. Travel Liability In consideration of my position as a site visitor, I, being 21 years of age or older, do hereby release, forever discharge and agree to hold harmless PHAB and the officers, directors, employees, members, subsidiaries, agents, successors and assigns thereof, from any and all liability, claims or demands for personal injury, sickness or death, as well as property damages and expenses, of any nature whatsoever which may be incurred, directly or indirectly, now or in
Appendix F: PHAB Site Visitor Agreement Form 2011-2012
PHAB Site Visitor Guide Version 1.0
March 2012 Page 51
the future, by reason of my participation and travel as a site visitor, including that caused solely or in part by the fault (including but not limited to negligence, gross negligence and/or recklessness) of the above- named parties. Furthermore, I hereby assume all risk of personal injury, sickness, death, damage and expense as a result of participation in recreation and work activities related to my participation and travel as a site visitor. Further, authorization and permission is given to PHAB to furnish and hereby release liability of transportation, food and lodging provided to me. This Release and Waiver of Liability shall be binding on my heirs, executors, administrators, successors, and assigns. I hereby indemnify PHAB, its officers, directors, employees, members, subsidiaries, agents, successors and assigns, from and against all claims, liabilities and expenses, including reasonable attorney’s fees, which may result from my acts, omissions or breach of this Agreement. As a PHAB accreditation site visitor, I have read, understand and agree to the Site Visitor Agreement. I have been given information in the following PHAB policies and procedures and agree to abide by them in the conduct of my activities before, during and after the accreditation site visit.
PHAB Site Visitor Guide Version 1.0
PHAB Conflict of Interest Policy and Disclosure Form
Content of this Site Visitor Agreement Form herein
______________________________________ Name (Please print)
______________________________________ ________________________
Signature Date
Approved February 2012

Appendix G: PHAB Travel Policies and Procedures
PHAB Site Visitor Guide Version 1.0
March 2012 Page 52
See separate document attached.

1 of 4
PHAB | 1600 Duke Street, Suite 440 | Alexandria, VA 22314 | 703.778.4549 | www.phaboard.org
Public Health Accreditation Board Travel Policies and Procedures
As the national public health accrediting body, the Public Health Accreditation Board (PHAB) has a need for people from all over the country to travel for PHAB business. All travel being reimbursed by PHAB must have prior approval. PHAB cannot reimburse travel expenses paid by another party. The following set of policies and procedures are used to assist PHAB Board of Directors, work group, committee members, site visitors, advisory groups, and staff in obtaining reimbursement for travel expenses. Questions should be directed to the contact for the project for which the travel occurred. The phone number for PHAB is 703-778-4549.
Reimbursement Policy Transportation 1. Air travel must be completed using the least expensive fare available. Flight arrangements must be made through Executive Travel Associates and every attempt should be made to book travel at least 14 days in advance. Our representative is Kathy Rosnick and she can be reached at [email protected] or 202-828-0102, Kathy will be given approval by PHAB to charge tickets to the PHAB account. You must obtain pre-approval from PHAB to purchase your ticket directly from another agency or from the airlines. 2. Travel by railway can also be used, using the most direct route, and should not exceed the least expensive air travel via the most direct economy air route. 3. Automobile mileage will be reimbursed at the current government rate per mile, not to exceed the cost by the most direct economy air route. The cost for the most direct (no more than one stops and/or flight change) economy air route includes any fees charged by airlines and the cost of ground transportation to and from the airport. Travelers should provide the actual mileage driven on the expense form and document departure and arrival locations. 4. Other ground transportation expenses, such as parking, taxi, bus, shuttles, etc. whether incurred at point of departure or upon return, will be reimbursed providing original receipts are submitted. Please note that car rental will not be allowed without prior approval by PHAB. PHAB will not reimburse for extra insurance purchased if the traveler’s automobile insurance covers rental vehicles driven during business use. 5. The cost of checking the first piece of luggage will be reimbursed, but the traveler is responsible for the costs associated additional checked bags.

2 of 4
PHAB | 1600 Duke Street, Suite 440 | Alexandria, VA 22314 | 703.778.4549 | www.phaboard.org
Lodging Reimbursement will be based on the actual amount paid for lodging. It is expected that the cost will be as close as possible to the federal daily maximum for that geographic area. Items such as personal telephone calls, non-meal room service items (e.g., movies, bar) and spa services are considered to be personal expenses and will not be reimbursed. If hotel reservations need to be cancelled, it is the traveler’s responsibility to notify the hotel directly to avoid “no show” charges. Travellers are expected to avoid overnight stays if morning travel (i.e., travel that begins at 6:00 a.m. or later) is feasible and reasonable. Meals and Incidental Expenses Reimbursement will be made up to a maximum per Diem of $100, including tax and gratuities. This is designed to cover the cost of purchasing meals while traveling and to cover small incidental expenses such as non-meal tips. The $100 will be reduced by the cost of the meals which the traveler does not have to purchase while traveling. This restriction includes both meals which are furnished by PHAB and meals that do not need to be purchased because the traveler is not traveling at a time that a meal would occur. Gratuities are expected to be in the 15-20% range. Should the travel schedule need to be broken down to separate individual meals, the meal per diem guidelines are:
Breakfast: $15.00 Lunch: $20.00 Dinner: $60.00 Incidentals $ 5.00
Please do not exceed the maximum total meal per Diem of $100 for the meals you purchased while on travel. PHAB will not reimburse for meals outside the dates and times of the approved travel. Meal receipts are required regardless of the amount.
How to Obtain Reimbursement 1. Complete the PHAB Travel Expense Voucher. See Instructions below for more information on how to complete the form. 2. Attach ORIGINAL receipts for lodging, air, ground, meals, and other related expenses for which reimbursement is being requested. These receipts should be taped to an 8½” by 11” sheet of paper (using multiple sheets if necessary). All purchases must be documented with an original receipt.

3 of 4
PHAB | 1600 Duke Street, Suite 440 | Alexandria, VA 22314 | 703.778.4549 | www.phaboard.org
3. Submit Travel Expense Vouchers with corresponding receipts to PHAB within 15 days after the travel has been completed. PHAB will not reimburse vouchers received which are older than 60 days or those that occur after the end of a grant cycle. The Vouchers should be sent to the PHAB Chief Administrative Officer for payment. Payments will be made by the on a biweekly basis. Please note that following the above procedures will expedite the reimbursement process.
Instructions for Completing the Travel Expense Voucher
PHAB staff will complete the “Please return to:” and “no later than:” sections of the form prior to distributing the form to travelers. Traveler Information Section Enter the name, phone and fax numbers, email, and mailing address for the traveler. This is the address to which reimbursement checks will be sent. Name of Meeting Enter the name of the meeting attended with enough descriptive information to provide audit detail, i.e. “Standards Development Workgroup Meeting” or “PHAB Board Meeting,” not just “PHAB Meeting.” Site visitors should note the name of the accreditation site visit, i.e. “Millet County Health Department Site Visit”. Dates of Trip Enter the dates of the trip, from the beginning of the travel to the return. This is the duration of the travel being reimbursed by PHAB. Time of Departure and Time of Return Indicate when the traveler departed for the trip and when the traveler returned from the trip. These times are used to calculate per diem expenses. Description of Expenses Section
Air/Rail: Enter the amount of air or rail tickets if purchased directly by the individual traveler. These expenses must be pre-approved for reimbursement by PHAB staff prior to the trip. Include any service fee charged in this section.
Taxi/Bus/Ground transportation: Enter the amount of ground transportation expenses. PHAB encourages the use of shared-ride vans and shuttles to reduce travel expenses whenever possible. This includes subway fares and other public transport expenses.
Garage Parking/Tolls: Enter amount of parking expenses and tolls.
Personal Car Mileage: In the box marked “Personal car mileage” enter the total number of miles driven using personal vehicles. PHAB will reimburse for these miles at the current allowable rate (Refer to the IRS website for the current mileage rate). In the “From/To” box, indicate where the personal miles were accumulated (i.e., “Washington DC to BWI airport, BWI airport to PHAB Office”

4 of 4
PHAB | 1600 Duke Street, Suite 440 | Alexandria, VA 22314 | 703.778.4549 | www.phaboard.org
or other description of departure and arrival points). Document of actual mileage is desirable (i.e., Yahoo! or MapQuest mileage totals) but not required.
Hotel/Motel expenses: Enter allowable hotel or motel costs, or other costs of lodging.
Phone/Telegrams/Fax: Enter expenses for allowed, business-related fax and phone costs.
Per diem section: Enter the actual dollar amount claimed for each meal that was not provided to you during the trip. Incidentals may be claimed for gratuities paid and other incidental expenses during your travel. RECEIPTS are REQUIRED.
Rental cars. Enter rental car expenses if approved prior to the trip by PHAB staff.
Other expenses: Enter the amount of other reimbursable expenses incurred and describe these expenses in the box provided on the form. If additional space is necessary, attach another sheet of paper.
Total Expenses Enter the total expenses for each row and column in the appropriate spaces provided. Double check the Total Expenses prior to submission. Balance Due Enter the amount due to the traveler. Traveler Signature The traveler must sign and date the voucher to obtain reimbursement. PHAB The PHAB Chief Administrative Officer will sign the voucher after checking for allowable expenses, checking the totals and assigning the voucher the appropriate code. Project Charge Instructions This box is for PHAB staff use only. Note: Interpretation or expansion of these policies and procedures will be conducted by referring to the Robert Wood Johnson Foundation or Centers for Disease Control Travel Guidelines, depending on the source of the reimbursement funds.
Policy Effective September 15, 2009 Updated February 2012
Appendix H: PHAB Travel Reimbursement Form
PHAB Site Visitor Guide Version 1.0
March 2012 Page 57
See separate document attached.

Please return to:
Travel Reimbursement Form
TRAVELER INFORMATION
Name of Traveler/Payee:
Phone Number:
Fax Number:
Email address: Time of Return:
SUN MON TUES WED THURS FRI SAT TOTAL
1. Air/Rail (REQUIRES PRE-APPROVAL IF PURCHASED INDIVIDUALLY)
2. Taxi/Bus/Ground Transportation
3a. Personal Mileage (ENTER TOTAL MILES TRAVELED) -
3b.Enter Dollar Amount Claimed for Mileage ($0.55 x MILEAGE)
4. Garage Parking/Tolls
5. Hotel Expenses
6. Phone/Telegrams/Fax/Internet
7a. Breakfast (Max $15)
7b. Lunch (Max $20)
7c. Dinner (Max $60)
7d. Incidental per diem (Max $5)
8. Rental car (REQUIRES PRE-APPROVAL)
9. Rapid Transit/Metro
10. Registration
11. Other Expenses (PLEASE EXPLAIN BELOW) INSERT
TOTAL EXPENSES TOTAL
Personal Car Mileage
Total Miles = From/To?
11. Other Expenses (DESCRIBE BELOW)
G/L Code Amount
SIGN HERE
Traveler Signature Date
Budget Manager ApprovalDate
Second Staff Approval (if required) Date
Note: Failure to submit travel reimbursement in time specified may result in forfeiting your claim for reimbursement.
Dates of Trip:
Time of Departure
no later than:
PROJECT CHARGE INSTRUCTIONS
Advance amount (if issued)Project Code
Total Expenses
Chief Administrative Officer
Street Address:
City, State, Zip Code
Name of Meeting:
Please complete this form, attach all receipts, sign it, and return it to the Chief Administrative Officer, PHAB, 1600 Duke Street, Suite 440
Alexandria, VA 22314 within 15 days of completing the travel.
Description of Expense
Balance Due
Date advance issued:

This publication was supported through grant funding from the Robert Wood Johnson Foundation (RWJF) and Cooperative Agreement #5U38HM000415-04 from the Centers for Disease Control and Prevention (CDC). Its contents are solely the
responsibility of the authors and do not necessarily represent the official views of the CDC or RWJF.
Copyright © 2012 Public Health Accreditation Board. All rights reserved.

1
CENTRALIZED STATES
Policies and Procedures V 1.0
Adopted by the PHAB Board of Directors December 2011
Definition of Centralized State
A centralized health department is defined, for the purposes of PHAB accreditation, as a state public health organizational structure that
operates all or most of the local health departments. Centralized health departments have a central office that provides administrative, policy,
managerial direction, and support. The local health departments in centralized states are organizationally a part of the state health department.
Employees are state employees, except for those in independent local public health departments, usually in one or more major city or county in
the state.
Types of Applicants
Where the state or territorial health department operates local and/or regional health department(s), a single local or regional applicant or a
number of individual applicants may choose to apply together.
Categories of centralized state PHAB accreditation applications are:
1. State health department application
This is a single health department application.
2. Local health department application
This is a single health department application.
3. State health department application for some or all local health departments in the state
If a state applies for one or more of its local health departments, the application review, site visit and accreditation
determination will be coordinated, concurrent, and performed as for one unit. (It is essential that health departments considering
this category of application have a conversation with PHAB prior to submitting their Statement of Intent so that all aspects of the
application category may be fully described.)
4. District or regional application as a local health department
Where state law (statutes, regulations, rules, executive orders, ordinances, case law, and codes) defines a district or region with
multiple counties, working together to deliver services and/or perform functions, will be treated as one health department.
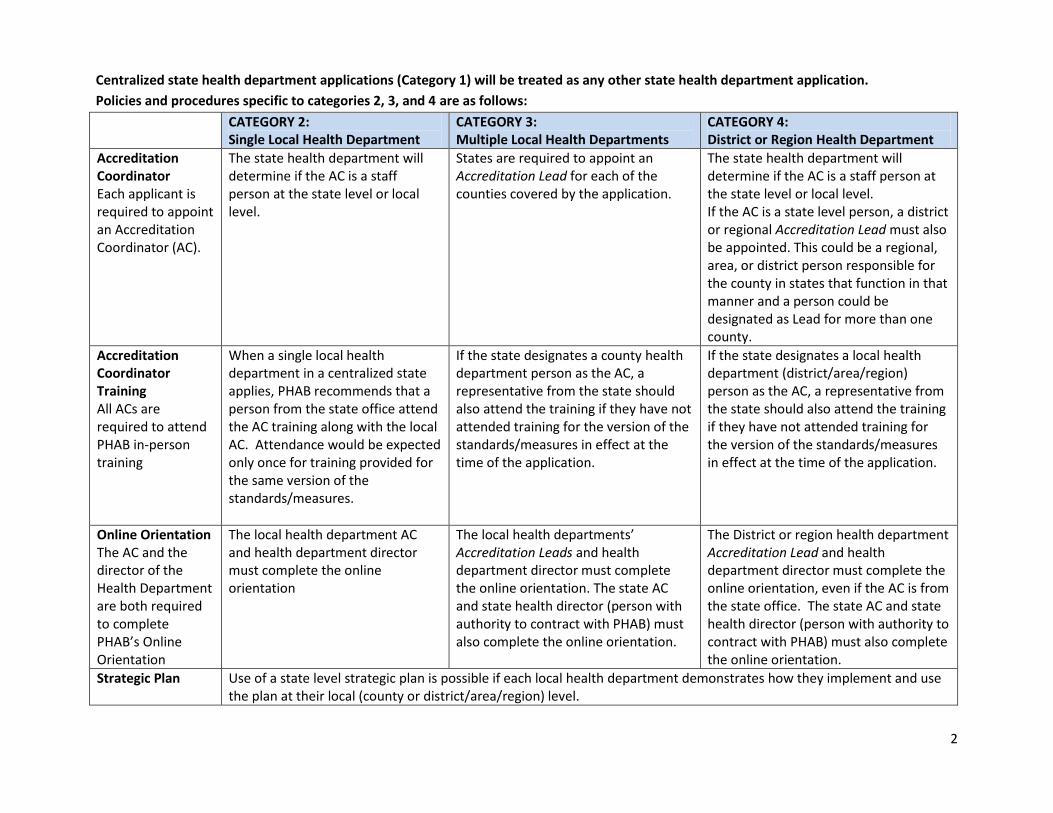
2
Centralized state health department applications (Category 1) will be treated as any other state health department application.
Policies and procedures specific to categories 2, 3, and 4 are as follows:
CATEGORY 2: Single Local Health Department
CATEGORY 3: Multiple Local Health Departments
CATEGORY 4: District or Region Health Department
Accreditation Coordinator Each applicant is required to appoint an Accreditation Coordinator (AC).
The state health department will determine if the AC is a staff person at the state level or local level.
States are required to appoint an Accreditation Lead for each of the counties covered by the application.
The state health department will determine if the AC is a staff person at the state level or local level. If the AC is a state level person, a district or regional Accreditation Lead must also be appointed. This could be a regional, area, or district person responsible for the county in states that function in that manner and a person could be designated as Lead for more than one county.
Accreditation Coordinator Training All ACs are required to attend PHAB in-person training
When a single local health department in a centralized state applies, PHAB recommends that a person from the state office attend the AC training along with the local AC. Attendance would be expected only once for training provided for the same version of the standards/measures.
If the state designates a county health department person as the AC, a representative from the state should also attend the training if they have not attended training for the version of the standards/measures in effect at the time of the application.
If the state designates a local health department (district/area/region) person as the AC, a representative from the state should also attend the training if they have not attended training for the version of the standards/measures in effect at the time of the application.
Online Orientation The AC and the director of the Health Department are both required to complete PHAB’s Online Orientation
The local health department AC and health department director must complete the online orientation
The local health departments’ Accreditation Leads and health department director must complete the online orientation. The state AC and state health director (person with authority to contract with PHAB) must also complete the online orientation.
The District or region health department Accreditation Lead and health department director must complete the online orientation, even if the AC is from the state office. The state AC and state health director (person with authority to contract with PHAB) must also complete the online orientation.
Strategic Plan
Use of a state level strategic plan is possible if each local health department demonstrates how they implement and use the plan at their local (county or district/area/region) level.

3
CATEGORY 2: Single Local Health Department
CATEGORY 3: Multiple Local Health Departments
CATEGORY 4: District or Region Health Department
CHA/CHIP
The local health department must submit a CHA and CHIP with their applications
Each of the county health departments included in the application is required to submit a CHA and a CHIP. The state level CHA and CHIP could be used only if it contains information detailing information specific to the local health department jurisdictions and the population they serve; describes active local community participation; includes locally collected information and/or data to supplement that collected for the state level CHA/CHIP; and sets forth policies and plans specific to each local health department jurisdiction.
The district/region health department is required to submit a CHA and a CHIP. The state level CHA and CHIP could be used only if it contains information detailing information specific to the district/region health department jurisdiction and the population it serves; describes active local community participation; includes locally collected information and/or data to supplement that collected for the state level CHA/CHIP; and sets forth policies and plans specific to the district/region health department jurisdiction.
Application: Health Department Descriptions Applications require the department’s budget amount, number of employees and FTEs, and size of population.
County data should be submitted. Health department descriptive data should be shown separately for each county included in the application.
Data should be totaled for the jurisdiction covered by the application.
Application: Letter of Support
Local health directors must submit a letter of support for the application covering their department.
Standards and Measures
Compliance with local-level standards must be demonstrated for local health department.
Compliance with local-level standards must be demonstrated for each local unit. Examples from each county included in the application should be submitted where needed to indicate compliance.
Compliance with local-level standards must be demonstrated for district/region health department.

4
CATEGORY 2: Single Local Health Department
CATEGORY 3: Multiple Local Health Departments
CATEGORY 4: District or Region Health Department
State Developed Documentation PHAB Documentation Guidance includes provisions for documentation developed by a larger governmental unit.
Once a measure is met with documentation by any level health department (state, county, district/area/region) within a centralized state, that documentation is accepted as meeting the measure for all health departments in that state for that PHAB application cycle. (For example, if documentation is deemed to meet a measure at a state level, it is automatically deemed to meet the measure at local, regional, or district levels, in that state, within that application cycle.) However, each level health department must demonstrate how that documentation deemed to meet the measure is applied and operationalized at the level of application. State policies will be assumed to apply to all local health departments included within the application, with any exceptions noted by the applicant.
Documentation Examples
If the sites are disparate in operations, geography, population, etc., the state should submit documentation from a variety of health department sites or programs that represent the different types of sites included in the application. For example, large/small, rural/urban, service delivery types. Including staff from each site in a group meeting during the site visit is desirable.
Governance (Domain 12)
Local, district, area and regional level health departments in a centralized state (that do not operate as independent entities) are covered by the state governance structure. Interaction with the state level health department concerning governance issues must be demonstrated. Interaction with any local governmental entities that have a partial role in local health department operations (local fee authority for example) must also be demonstrated.
Site Visit Team Members
When a local, district, area or regional health department applies at the same time as the state level health department in a centralized state (separate applications), there should be some overlap of SV team membership, if applications are submitted within the same application period and standards version. The SV team chair for SV’s to health departments in centralized states should be from a centralized state.

5
CATEGORY 2: Single Local Health Department
CATEGORY 3: Multiple Local Health Departments
CATEGORY 4: District or Region Health Department
Site Visit Team Size The number of members of the site visit team would be the normal number: 3 -4.
SV team size should vary according to the number of counties and geographic distance involved. Flexibility in use of additional members and visit days is needed.
Site Visit Schedule When both the state and a local health department in a centralized state apply for accreditation at the same time, (these will be separate applications), it is recommended that the state be scheduled to have its site visit before the local health department.
If the local health department is advanced in the application process, the local can be scheduled for a site visit and completed first, with the state’s approval.
If the district/region health department is advanced in the application process, the district/region health department can be scheduled for a site visit and completed first, with the state’s approval.
Sites Visited Site visitors should select a variety of health department sites that represent the different types of sites included in the application to visit. For example, large/small, rural/urban, different service delivery types. Including staff from each site in a group meeting during the site visit is desirable.
Site Visit Report There will be separate sections for each local health department covered by the application, to the extent that the documentation speaks to local situations, especially for opportunities for improvement and best practices.

March 28, 2012
TO: Carol Moehrle, Chair
Board of Directors
FROM: Bud Nicola, Chair
Board Multi-jurisdictional Ad Hoc Committee
RE: Report of the Multi-jurisdictional Ad Hoc Committee of the Board
Since the appointment of the board’s Multi-jurisdictional (MJD) Ad Hoc Committee (Les
Beitsch, Rex Archer, Carol Moehrle, and myself), we have met by phone on two occasions. The
first meeting held on February 3, 2012 was to familiarize the committee with the proposed
review procedures developed by the expert panel and distributed to the Board in December 2011.
The second meeting, held on March 26, 2012, focused on developing a better understanding of
the context for this accreditation application category. Pat Libbey, Shirley Orr, and Pamela
Russo joined us for that meeting to provide some examples of multi-jurisdictional sharing of
public health services and to assist us in identifying some of the issues that PHAB should
consider.
The committee has determined that this issue is much more complex than we had envisioned
when the application category was first created. We are also aware that there have been no
Statements of Intent or Accreditation Applications submitted to PHAB in this category as of yet.
Therefore, the committee recommends that the full board take some time during the April board
meeting to discuss these issues further. We also recommend deferring any official action on the
procedures until the June board meeting. Shirley Orr will be joining the Board for the discussion,
and Pamela Russo will participate by phone.
Past Board Actions
The Board has previously approved the following items related to this topic:
1. Multi-jurisdictional as an accreditation application category.
2. The following definition of multi-jurisdictional for accreditation purposes:
Entities that meet the definition of a tribal or local health department may apply jointly
for PHAB accreditation if some essential services are provided by formally sharing

resources and the sharing of resources can be clearly demonstrated (p.12, PHAB Guide
to National Public Health Department Accreditation, Version 1.0).
For multi-jurisdictional applications, the partnering health departments, which could be
two or more health departments, will apply as a single entity. The partnering health
departments must select one lead health department to apply on behalf of all partners.
The partnering health departments must submit a memorandum of understanding (MOU)
or similar documentation describing in detail the multi-department relationship. The
relationship must be that of the health departments working together to deliver services
and/or perform functions over the combined jurisdiction. It cannot be simply an “of
convenience” or paper-only relationship to apply for accreditation. The business and
working relationship of multi-jurisdictional applicants must be well established and well
defined (p. 13, PHAB Guide to National Public Health Department Accreditation,
Version 1.0).
The Board had also approved the establishment of a Multi-jurisdictional Think Tank to
further explore the accreditation issues and to develop recommendations to the Board for
implementation. Because of her former experience in the Kansas Department of Health
(where a lot of work in developing multi-jurisdictional approaches to shared services has
occurred), Shirley Orr was contracted to lead this body of work. Given the small number
of health departments with this experience, the original idea of a think tank developed
into a smaller expert panel with the same charge. Their recommendations were prepared
for the December 2011 board meeting because it was anticipated that PHAB would have
some early MJD applicants. Given time constraints and the complexity of the MLD issue,
the topic was tabled until the April meeting, and the recommendation was made to
appoint an ad-hoc committee of the board to lead further work.
Requests for the April Meeting
1. Formal decisions continue to be deferred pending additional board discussion on the
issues.
2. The Board should devote some time at the April meeting to discuss the context for
this application category. Some questions to be considered, although not all inclusive,
are:
The original intent for creating the MJD application category was to address some of the accreditation concerns of small health departments. Is this still an
appropriate strategy? If not, is there a better alternative?
Is PHAB’s role to help transform local public health in areas with limited
resources so that a growth in shared services is an expected outcome?
Does PHAB know what the potential demand for MJD accreditation is for the future?
How does PHAB ensure that health departments reviewed under the MJD category are reviewed equitably?

Are there any special considerations with regard to the fee schedule (this decision was also tabled)?
What should PHAB’s messages be with regard to the MJD application
category while the issue is still under review?
Thank you for the opportunity to provide this report. I look forward to the discussion at the
upcoming board meeting.

March 28, 2012
TO: Carol Moehrle, Chair
Board of Directors
FROM: Kaye Bender, President/CEO
RE: Think Tank Report
Since PHAB has completed the initial stages of development of the accreditation materials, tools
and processes that are being used in this accreditation cycle, we now have fewer volunteers
engaged in the developmental work of PHAB. Over 400 individuals assisted us in the early
stages, a major factor in PHAB’s success to date. One of the ways that we continue to engage
partners across the country is through participation in the various think tanks. PHAB uses the
current think tank process as a means for marketing accreditation to additional health
departments and other stakeholders (such as additional federal agencies, public health program
representatives, and partner organizations) and to obtain input into future versions of the
standards and measures and accreditation process. Participation in the think tanks by board
members is vital to a sound process, and I thank those board members who have committed to
assist us in those efforts.
The purpose of this report is to provide the Board with an update on the planned think tanks
previously approved by the Board.
Think Tanks Held in This Quarter
1. The Workforce Think Tank was held on March 7-8, 2012 in Alexandria, VA. The
Workforce Think Tank purpose and outcomes are to identify strategies for public health
leadership engagement in the workforce aspects of accreditation; to discuss the
relationship between the PHAB accreditation standards and public health workforce
competencies; to identify strategies to strengthen the PHAB accreditation standards and
measures in the area of workforce development and to develop ideas to inform future
public health workforce and accreditation research. Hugh Tilson facilitated the meeting,
which was also attended by Paul Halverson as a board liaison. Representatives from CDC
and HRSA, as well as a number of public health organizations, universities, health
departments and others engaged in workforce development attended. A verbal report of
the Workforce Think Tank will be provided at the April meeting. We anticipate holding a
follow-up session with the same group later in 2012 or early 2013.
2. The California Think Tank is being held on March 29, 2012 in Sacramento, CA. The
purpose of this think tank is consider motivations, incentives, issues, challenges, and

concerns of health departments in California that would influence their participation in
PHAB accreditation; and, to provide consultation and recommendations to PHAB
regarding the application of the PHAB accreditation process, and standards and measures
as they pertain to public health departments in the state of California. Board members
Fernando Guerra, Bill Riley, Les Beitsch, and Wilma Wooten have planned to attend the
meeting, as are a number of health department and public health organizational
representatives from California. Jennifer Jimenez serves as PHAB’s consultant to this
think tank and has performed a lot of outreach and educational activities to various
stakeholders in the California area prior to the session. A verbal report will be provided at
the April board meeting. We anticipate holding another session with this group later in
2012 or early 2013.
Think Tanks Scheduled for the Next Quarter
The following think tanks are scheduled for the upcoming months. I have also noted the board
member liaisons beside each think tank name, based on individual board member requests.
1. Maternal Child Health Think Tank – In partnership with the Association of Maternal
Child Health Programs, PHAB has scheduled the MCH Think Tank for May 3, 2012 in
San Francisco, CA. The purpose of this think tank is to discuss the relationship between
the PHAB standards and measures and the MCH performance standards and measures; to
identify strategies to strengthen the PHAB standards and measures in the areas of
maternal and child health; to identify strategies to ensure MCH leadership engagement in
health department accreditation readiness activities; and, to identify related program areas
managed by health departments that also serve the MCH population (such as WIC and
Children with Special Health Care Needs). Board member liaisons are Hugh Tilson, Les
Beitsch, and Fernando Guerra.
2. Emergency Preparedness Think Tank –In partnership with CDC, PHAB has tentatively
planned the Emergency Preparedness Think Tank for June 12-13, 2012 in Atlanta. The
purpose of this think tank is under development, but will be similar to the other think tank
purposes. Board member liaisons are Alonzo Plough, Bill Riley and Joe Finkbonner.
3. Informatics Think Tank – In partnership with the Public Health Informatics Institute and
CDC, PHAB has tentatively planned the Informatics Think Tank for the latter part of
June 2012 (working around many other planned national meetings), in Atlanta. The
purpose is also under development at this time. Board member liaisons are Carol
Moehrle, Hugh Tilson, and Ed Harrison.
Think Tanks Pending Final Planning
Approved Think Tanks that are pending final planning include Chronic Disease and
Communication Science. PHAB has recently secured a commitment from the Association of
Chronic Disease Directors to partner with us in planning the Chronic Disease Think Tank.
Developmental work has begun on planning for the Territorial Think Tank. PHAB’s partners for
that work include ASTHO and PIHOA.
In addition to those already mentioned in this report, we also expect to hold second think tank
sessions with the large city/metro group later in 2012 or early 2013. Thank you for the
opportunity to provide this report. I look forward to the discussion at the April board meeting.

For more information visit www.iom.edu/primarycarepublichealth
Primary Care and Public Health Exploring Integration to Improve Population Health
Although primary care and public health share a goal of promoting the health and well-being of all people, these two disciplines historically have operated independently of one another. Problems that stem from this sepa-ration have long been recognized, but new opportunities are emerging for bringing the sectors together in ways that will yield substantial and lasting improvements in the health of individuals, communities, and populations. In recognition of this potential, the Centers for Disease Control and Pre-vention (CDC) and the Health Resources and Services Administration (HRSA), both agencies of the Department of Health and Human Services (HHS), asked the Institute of Medicine (IOM) to convene a committee of experts to examine the integration of primary care and public health. The United Health Founda-tion also provided support for the study. The IOM committee presents its findings and recommendations in Pri-mary Care and Public Health: Exploring Integration to Improve Population Health.
Principles of SuccessAs part of its study, the IOM committee identified and analyzed past and cur-rent efforts to integrate primary care and public health. Put simply, primary care focuses on providing medical services to individual patients with imme-diate health needs. Public health focuses on offering a broader array of ser-vices across communities and populations that collectively will help people to be healthy. The committee finds that the types of interactions between the two sectors are so varied and dependent on local circumstances, such as the avail-
Although primary care and public health share a goal of promot-ing the health and well-being of all people, these two disciplines historically have operated indepen-dently of one another.
REPORT BRIEF MARCH 2012

2
FIGURE: Degrees of Primary Care and Public Health Integration
ability of resources and differences in health chal-lenges, that it is not possible to prescribe a specific model or template for how integration should look. Instead, it identifies a set of core principles derived from successful integration efforts. The core principles include a common goal of improving population health, as well as involv-ing the community in defining and addressing its needs. Strong leadership that works to bridge dis-ciplines, programs, and jurisdictions; sustainabil-ity; and the collaborative use of data and analysis are the other principles. While the committee regards all of these principles as ultimately necessary for successful integration of primary care and public health, it concludes that integration can start with any of the principles. Beginning is more important than waiting until all of the requisite components are in place. Moreover, the committee notes that the time is right for action. There is a growing recogni-tion that the current model of investment in the nation’s health system is unacceptable, and the dramatic rise in health care costs has led many stakeholders to explore innovative ways of reduc-ing costs and improving health. Research findings also continue to clarify the importance of social and environmental determinants of health and the effect of primary prevention. An unprecedented wealth of health data is providing new means to understand and address community-level health concerns. In addition, passage of the Patient Pro-tection and Affordable Care Act (ACA) provides
new opportunities to encourage integration to occur, changing the way the nation improves health.
Scope of IntegrationThe committee acknowledges that integration of primary care and public health can occur on a continuum (see Figure). While it stresses the need to move away from isolation, where the sectors work in separate silos, the committee does not advocate for complete merger. Rather, it identifies degrees of integration that can be used to achieve better health results: mutual awareness, coopera-tion, collaboration, and partnership. When there is mutual awareness, primary care and public health are informed about each other and each other’s activities. Cooperation denotes some sharing of resources, such as space, data, or personnel. Collaboration is more intense and involves joint planning and execution, with both sectors working together at multiple points to carry out a combined effort. Partnership implies integration on a programmatic level, with the two sectors working so closely together that, from the individual’s perspective, there is no separation. In practice, every community will be differ-ent, and not all will be able to achieve true part-nership. In some communities, achieving mutual awareness will mark a significant step forward. However, it will be useful to strive for greater integration when possible.

3
others about best practices related to the integra-tion of primary care and public health, and con-vening stakeholders at the national and regional levels to share best practices for integration. The CDC and HRSA should join forces to develop the workforce needed to support the inte-gration of primary care and public health. Among needed actions, the CDC and HRSA should work with the Centers for Medicare and Medicaid Ser-vices (CMS) to identify regulatory options for graduate medical education funding that give pri-ority to provider training in primary care and pub-lic health settings and specifically support pro-grams that integrate primary care practice with public health. They also should develop training grants and teaching tools that can prepare the next generation of health professionals for more integrated clinical and public health functions. HHS should focus on improving the integra-tion of primary care and public health through its existing programs as well as new initiatives being developed as a result of the ACA. For example, the CMS Innovation Center can use its focus on improving community health to support pilot projects that better integrate primary care and public health. Some health data that doctors col-lect from patients already are used to help improve public health. To bolster that effort, the Office of the National Coordinator for Health Information Technology should consider developing popu-lation measures that support the integration of community-level clinical and public health data. At a broader level, HHS should work with its agencies to develop a national strategy and invest-
There is a growing recognition that the current model of investment in the nation’s health system is unac-ceptable, and the dramatic rise in health care costs has led many stakeholders to explore innovative ways of reducing costs and improv-ing health.
Framework for ActionWith these principles as a framework for action, the committee proposes an array of recommen-dations whose implementation would assist the CDC, HRSA, and HHS in creating an environ-ment that would foster broader integration of pri-mary care and public health. At the agency level, the CDC and HRSA should take steps to connect staff, funding, and data at the regional, state, and local levels. The agencies should create opportunities for staff to build relationships with each other and local stakeholders by taking advantage of opportuni-ties to work through the 10 regional HHS offices, state primary care offices and association organi-zations, state and local health departments, and other mechanisms. In addition, the committee recommends that the agencies inventory health and health care databases in order to create a consolidated platform for sharing and displaying local population health data that could be used by communities. The CDC and HRSA also should work together to create research and learning networks that disseminate best practices in order to foster and support the integration of primary care and public health to improve population health at the state and local levels. The agencies should support the evaluation of existing local and regional mod-els of primary care and public health integration, and they should support the development of new models of integration. Such efforts should include working with the Agency for Healthcare and Research Quality’s Action Networks to educate

The Institute of Medicine serves as adviser to the nation to improve health. Established in 1970 under the charter of the National Academy of Sciences,
the Institute of Medicine provides independent, objective, evidence-based advice to policy makers, health professionals, the private sector, and the public.
Copyright 2012 by the National Academy of Sciences. All rights reserved.
500 Fifth Street, NW Washington, DC 20001
TEL 202.334.2352 FAX 202.334.1412
www.iom.edu
Committee on Integrating Primary Care and Public Health ment plan for creating a primary care and public health infrastructure robust enough and appropri-ately integrated to enable the agencies to play their appropriate roles in furthering the nation’s popula-tion health goals.
ConclusionThe challenges in integrating primary care and public health are great—but so are the opportuni-ties and rewards. The IOM report offers the most detailed portrait yet of the current landscape for integrating, along with principles that can serve as a roadmap to move the nation toward a more effi-cient health system. The status quo of siloed enter-prises is not good enough. Moving along a path of integration will promote better health and well-being for all Americans. f
Consultants
Sara RosenbaumGeorge Washington University School of Public Health and Health Services, Washington, DC
Philip Sloane University of North Carolina, Chapel Hill
Katrina DonahueUniversity of North Carolina, Chapel Hill
Federal Funds Information for States Washington, DC
Rona Briere Briere Associates, Inc., Felton, PA
Study Sponsors
Centers for Disease Control and Prevention Health Resources and Services Administration United Health Foundation
Monica N. FeitStudy Director
Joshua JosephAssociate Program Officer
Trevonne WalfordResearch Associate
Andrés GaviriaSenior Program Assistant (from August 2011)
Katherine McGrawSenior Program Assistant (until August 2011)
Rachel MirianiIntern, Summer 2011
Rose Marie MartinezDirector, Board on Population Health and Public Health Practice
Study Staff
Paul J. Wallace (Chair)Senior Vice President and Director, Center for Comparative Effectiveness Research, The Lewin Group, Falls Church, VA
Anne M. Barry Deputy Commissioner, Minnesota Department of Human Services, St. Paul
Jo Ivey Boufford President, New York Academy of Medicine, New York
Shaun Grannis Director and Principal Investigator for DRI-ICE and Assistant Professor, Department of Family Medicine, Indiana Center of Excellence in Public Health Informatics, Regenstrief Institute, Inc., Indianapolis
Larry A. Green Epperson-Zorn Chair for Innovation in Family Medicine, University of Colorado at Denver
Kevin Grumbach Professor and Chair, Department of Family and Community Medicine, University of California, San Francisco, and Chief, Family and Community Medicine, San Francisco General Hospital
Fernando A. Guerra Public Health Consultant and Director of Health, City of San Antonio and the San Antonio Metropolitan Health District, Texas
James Hotz Clinical Services Director/Medical Director, Albany Area Primary Health Care, GA
Alvin D. Jackson Director (Former), Ohio Department of Health, Fremont
Bruce E. LandonProfessor of Health Care Policy, Department of Health Care Policy, Harvard Medical School, Boston, MA
Danielle LaraqueChair, Department of Pediatrics, Maimonides Medical Center, Brooklyn, NY
Catherine G. McLaughlin Senior Research Fellow, Mathematica Policy Research, Ann Arbor, MI
J. Lloyd MichenerProfessor and Chairman, Department of Community and Family Medicine, and Director, Duke Center for Community Research, Duke University Medical Center, Durham, NC
Robert L. PhillipsDirector, Robert Graham Center, American Academy of Family Physicians, Washington, DC
David N. SundwallClinical Professor of Public Health, School of Medicine in the Division of Public Health, University of Utah, Salt Lake City
Mary WellikCommunity Health Services Administrator (Retired), Olmsted County Public Health Services, Rochester, MN
Winston F. WongMedical Director, Community Benefit Disparities Improvement and Quality Initiatives, National Program Office, Kaiser Permanente, Oakland, CA