psychophysiological responses to anger provocation among asian indian and white men
TRANSCRIPT

Psychophysiological Responses to Anger ProvocationAmong Asian Indian and White Men
Sonia Suchday and Kevin T. Larkin
To examine cultural differences in response to anger provocation, affective, cognitive,behavioral, and cardiovascular responses to social confrontation, role plays weremeasured in 20 Indian male immigrants in the United States and 40 White men. Par-ticipants engaged in 2 interactions with a nonacquiescent male confederate and wereinstructed to suppress or express their anger in counterbalanced order. Followingeach role play, participants state anger, and resentful and reflective cognitions per-taining to anger were assessed. Participants’ videotaped behavioral responses wereassessed for problem-solving skills and negative and positive verbal and nonverbalbehaviors. Blood pressure and heart rate (HR) responses were recorded throughoutthe session. Results revealed that Indian participants used more introspective strate-gies comprising of repression and rational coping self-statements to anger provoca-tion than their White counterparts. White participants experienced significantlyhigher HR responses and showed more awareness of physiological sensation com-pared to the Indian participants, but only when asked to exhibit their anger. Indianparticipants had a faster diastolic blood pressure (DBP) recovery when allowed toengage in anger inhibition (which is a culturally determined mode of functioning)compared to when they had to exhibit anger before inhibiting it. White men showed aheightened cardiac response to anger expression, something not seen among Indianmen. Indian men, in contrast, exhibited delayed DBP recovery from anger expressionand increased introspective cognitive strategies when asked to engage in anger exhi-bition, a behavior not congruent with their culture of origin.
Key words: anger expression, culture, cardiovascular reactivity, coping self-state-ments, role-play assessment
Prevalence of coronary heart disease (CHD) is on therise in the Indian subcontinent as a function of increasedlife expectancy, increasing urbanization, and poorchildhood nutrition (Reddy, 1999). In addition to otherrisk factors, people from India are particularly prone toinsulin resistance and central obesity, which cannot betotally explained by health behaviors including activitylevel, cigarette smoking, and alcohol intake (Hodge etal., 1996). Despite the increasing prevalence of CHDamong Indians, research on behavioral predispositions,which render individuals vulnerable to the developmentof CHD, has lagged behind efforts using White samples.Research using primarily White samples from theUnited States, for example, has shown that the experi-
ence and expression of anger is associated with the de-velopment and exacerbation of CHD (e.g., Siegman,1993; Smith, 1992) and hypertension (e.g., Everson,Goldberg,Kaplan, Julkunen,&Salonen,1998). Inaddi-tion to the association between anger expression andCHD observed among samples in the United States, ele-vated blood pressure response to anger provocation inthe laboratory has been hypothesized as a mechanismthat may help explain how the experience and expres-sion of anger might lead to the development of CHD(Krantz & Manuck, 1984). Accordingly, persons whoexperience anger intensely and express it overtly mayexhibit exaggeratedheart rate (HR)orbloodpressure re-sponses to anger provocation, which in turn increasestheir risk for CHD (Smith, 1992).
In the United States, considerable attention hasbeen given to examining the relation between anger ex-pression and cardiovascular response to stress (e.g.,Faber & Burns, 1996; Miller, Dolgoy, Friese, & Sita,1996; Siegman, 1993; Siegman & Snow, 1997; Vogele,Jarvis, & Cheeseman, 1997; Vogele & Steptoe, 1992).Among these studies, however, no consistent patternhas been observed; some observed exaggerated cardio-
71
International Journal of Behavioral Medicine2004, Vol. 11, No. 2, 71–80
Copyright © 2004 byLawrence Erlbaum Associates, Inc.
Sonia Suchday, Clinical Health Psychology, Albert Einstein Col-lege of Medicine/Yeshiva University/Ferkauf Graduate School ofPsychology and Kevin T. Larkin, Department of XXX, West VirginiaUniversity.
Correspondence concerning this article should be addressedto Sonia Suchday, Clinical Health Psychology, Albert EinsteinCollege of Medicine/Yeshiva University, Ferkauf Graduate Schoolof Psychology, 1300 Morris Park Avenue, Bronx, NY 10461.E-mail:[email protected]

vascular responses to stress among persons who sup-press anger in comparison to those who express anger(Vogele & Steptoe, 1992; Vogele et al., 1997) and oth-ers showed exaggerated cardiovascular reactions tooccur among anger-expressive persons (Miller et al.,1996; Siegman, 1993; Siegman & Snow, 1997). A re-cent longitudinal study (Everson et al., 1998) sup-ported both of these bodies of literature by showingthat both anger expression and suppression result in thedevelopment of hypertension over a 4-year period. Ac-cording to the authors, regardless of anger expressionstyle, it is the festering resentment that accompaniesanger that is responsible for increased vulnerability todisease.
Despite accumulation of data on multiple dimen-sions of modes of anger expression among predomi-nantly White persons in the United States, little isknown about the universality of cardiovascular reactiv-ity to anger provocation. Specifically, little is knownabout how anger expression is correlated with cardio-vascular responses to provocation in the laboratoryamong Asian Indians. Because the prevalence of CHDwithin the Indian subcontinent is increasing (Reddy,1999), the examination of behavioral risk factors in thispopulation is worthy of inquiry.
Studies using inhabitants of the Indian subcontinenthave identified various personal traits that have beenshown to be correlated with CHD, including findingsthat Indian CHD patients in contrast to non-CHD con-trols (a) were more likely to have a neurotic personality(assessed by the Eysenck Personality Inventory), (b)tended to be emotionally overresponsive during stress(Shukla, 1995), and (c) were more likely to display theType A behavior pattern (Kaushik, Mukhopadhyay,Sheik, & Goel, 1994). In another study using an Indiansample, hyperreactivity to mental arithmetic and mir-ror drawing distinguished controls from hypertensivepatients (Basu, 1991). In this regard, findings on be-havioral risk factors for CHD have been shown to bequite similar for inhabitants of both India and theUnited States. However, when anger as a construct wasexamined among Indian participants, a significant in-verse correlation between anger-in and anger-out wasobserved, which differed from how participants fromthe United States scored on anger expression scales(Sharma, Krishna, & Spielberger, 1996). Among In-dian respondents, components of anger expression(i.e., anger inhibition and anger exhibition) fell on acontinuum of anger expression, whereas among partic-ipants in the United States, anger-in and anger-out typ-ically are conceived as orthogonal dimensions. Also,among Indians, risk of cardiovascular disease wasmore closely associated with anger-in rather than an-ger-out modes of anger expression (Sharma et al.,1996). Contrary to the findings of Sharma et al.,Forgays, Richards, Forgays, and Sujan (1999) reportedthat male college students from the United States, Aus-
tralia, and India did not differ on self-report measuresof anger and anger expression. The only difference ob-served among the three groups was that Indian men re-ported fewer somatic symptoms compared to youngmen from the United States and Australia. However,neither of these studies examining differences in angerexpression between Indian and White samples at-tempted to assess cardiovascular or behavioral re-sponse to anger provocation. In sum, although compar-isons of anger expression between Indian and Whitesamples appear to warrant further exploration, empiri-cal work examining cardiovascular and behavioral re-sponses to anger provocation among Indian sampleshas been scarce. Because anger suppression is cultur-ally reinforced but also is associated with increasedrisk for CHD in Indian samples, it is likely that furtherexamination of the experience and expression of angeramong Indians may elucidate behavioral risk factor el-ements unique to the Indian culture.
Immigration poses an additional and potent chronicstressor for Indian men who might already be at risk forCHD (Reddy, 1999). On immigrating to Western cul-tures where anger expression is normative, the cultur-ally reinforced style of anger suppression among In-dian men may become even less adaptive. Preliminarydata from the United Kingdom has shown that SouthAsians have a higher prevalence of CHD compared tothe native population, which may be related to stressresulting from immigration (Farooqi, Nagra, Edgar, &Khunti, 2000). In one recent study where cardiovascu-lar response to stress was assessed among immigrantsfrom South Asia, Indians residing in Singapore withhigh levels of trait anger were more likely to evidenceelevated systolic blood pressure (SBP) responses tocomputer tasks regardless of whether they were ha-rassed or not harassed during the task compared to Chi-nese men residing in Singapore (Bishop & Robinson,2000). In this study, Chinese men experienced elevatedblood pressure responses to provocation, but onlywhen harassed during the computer task. In sum, thestress associated with immigration has been shown tobe related to both exaggerated blood pressure re-sponses to stress and anger suppression and that thesefindings may not be unique to immigrants from India.
Because of the complexity of the effects of culturaldifferences between native and immigrant populations,a comprehensive measurement of responses, includingaffective, cognitive, behavioral, and cardiovascular re-sponses, provides an optimal method for identifyingdifferences in anger expression among culturally di-verse groups.
Despite the heterogeneity of culture in both Indiaand the United States, there are certain universal valuesthat distinguish them from each other, specifically, theemphasis placed on collectivism and interpersonal re-lationships among Eastern cultures and the focus on in-dividualism and personal achievement in the Western
72
SUCHDAY AND LARKIN

world (Miller & Bersoff, 1992; Oyserman, Coon, &Kemmelmeier, 2002; Sahoo & Bidyadhar, 1995). Inaddition, the philosophical beliefs prevalent in Easterncultures, which emphasize acceptance of adversity asan inevitable part of life and as an opportunity for spiri-tual growth, differ from Western values that focus onactive coping with stress and overcoming adversity.
Traditionally, Western values have emphasized in-dividualism as a focus on achievement and rights oversocietal obligations (Hofstede, 1980). An implicationof the individualistic values in the West is a belief in thecontrol exerted by individuals in the determination oftheir fate and the value placed on the attainment of in-dividuals’ potential (personally, socially, and profes-sionally) and freedom of emotional expression (Diener& Diener, 1995; Triandis, 1995). In contrast, Easterncultures are more likely to uphold a collectivistic valuesystem that focuses on individuals subsuming individ-ual achievement in favor of societal good, with impor-tant behaviors directed toward the achievement of thegroup (Triandis, 1995). Indian society, in particular,has been described as practicing vertical collectivismwith an emphasis on traditional, hierarchical systemsof authority (Triandis & Suh, 2002). An implication ofcollectivistic values is the acceptance of fate as prede-termined and restraint in emotional expression as ameans of maintaining harmony within society(Oyserman et al., 2002).
In this study an attempt was made to reconstruct situ-ations that both native and foreign students typically en-counter during their collegiate education, which may beparticularly stressful for immigrant students who havethe added burden of interacting with members of a cul-ture thatdiffers fromtheirown.Moreover, Indianpartic-ipants may place a significantly higher value on inter-personal relations compared to their Westerncounterparts (Miller, 1984), and hence, anger expres-sion (which is not a prosocial emotion for them) may beparticularly problematic. To examine whether re-sponses to anger provocation differed between nativeWhite and immigrant Indian male college students, re-sponses were measured to two interpersonal confronta-tion scenes, one in which they were instructed to expresstheir anger openly and the other in which they wereinstructed to hide or suppress their anger. It was hypoth-esized that response differences would be observedbetween the White and Indian students, with Indian par-ticipants reacting with greater arousal to anger provoca-tion when requested to express their anger openly thanwhen instructed to refrain from anger expression.
Methods
Participants
Participants were 40 White men and 20 Asian In-dian men. Participants were excluded from the experi-
ment if they were taking any medication that affectedthe cardiovascular system, including beta blockers,anxiolytics, and sympathomimetics.
Assessment of Affective Responses
State anger. The state form of the State and TraitAnger Scale (STAS; Spielberger, 1988), assesses af-fective responses to perceived insult, injury, unfair-ness, or frustration in the environment. In this study,the STAS served as a measure of anger experiencedduring each of the interpersonal tasks.
Awareness of physiological responses. The Phys-iological Sensations Checklist (Sturges & Goetsch,1996) was used to assess awareness of physiological ex-perience. Participants’self-report of HR increase or de-crease (in bpm) during the preceding task was obtainedfollowing each task.
Arousal and anxiety. Participants also rated theextent of arousal and anxiety experienced during thepreceding interpersonal task on a 10-point Likert scaleranging from 1 (no arousal/anxiety) to 10 (most arous-al/anxiety).
Assessment of Cognitive Responses
Cognitive responses were assessed using the AngerCognitions Inventory (Suchday & Desiderato, 1991),which is a 27-item, 4-point Likert scale inventory ofself-statements assessing the cognitive correlates ofanger. Participants rated the frequency with whicheach self-statement occurred during the immediatelypreceding role-play situation. Four subscale scoreswere obtained for each participant: Rational Coping,Repression/Distancing, Victimization, and Self Righ-teousness. Additional details about the inventory canbe obtained in Suchday and Larkin (2001).
Assessment of Behavioral Responses
Behavioral responses to both interpersonal taskswere coded using a modified version of the Marital In-teraction Coding System (Hops, Mills, Patterson, &Weiss, 1972). Based on previous work by Wiedner andWeiss (1980), individual response codes were groupedinto five categories: positive and negative nonverbalmotor behaviors, positive and negative verbal contentof the interaction, and problem solving. Details aboutthe scoring procedures are provided in Suchday andLarkin (2001).
73
RESPONSES TO ANGER PROVOCATION

Assessment of CardiovascularResponses
Blood pressure (SBP and diastolic, DBP) was ob-tained via an IBS SD-700A automated sphygmoma-nometer (Industrial Biomedical Sensors, Waltham MA)at 1-min intervals during the role play and recovery fol-lowing the role play, and at 2-min intervals during restperiods. An occluding cuff positioned over the brachialartery of the participant’s nondominant arm was used.Cuff inflation and deflation was controlled by a micro-processor; resulting SBPs and DBPs were digitally dis-playedandrecordedbya laboratoryassistant.Threesur-face electrodes attached to the collarbone and lowerchest of each participant transmitted wave forms to anelectrocardiogram (ECG) preamplifier and charted on aGrass Model 7 polygraph (Grass Instruments, Quincy,MA) and provided a measure of HR.
Experimental Tasks
In this investigation, participants engaged in two roleplays that have been used in previous investigations toelicit anger (Larkin, Frazer, & Semenchuk, 1996;Larkin, Semenchuk, Frazer, Suchday, & Taylor, 1998;Suchday & Larkin, 2001). In each role play, participantswere asked to resolve a conflict with a White male con-federate introduced as another participant. In the NoiseScene, theconfederateplayed the roleofaneighborwhorefused to turn down loud music in his apartment in onevignette. In the other vignette (the Mess Scene), the con-federate played the part of an inconsiderate roommatewho refused to clean the apartment despite repeated re-quests. The confederate responded to the participants’requests fora resolutionwithasetof structuredresponseprompts, which got increasingly nasty (see Larkin et al.,1998). The same confederate was used during both roleplays and was instructed not to reach a compromise dur-ing either vignette. Participants were asked to exhibitand inhibit their anger toward the confederate during thetwo role plays in counterbalanced order. Both interac-tions with the confederate were videotaped using a JVCcamcorder.
Procedure
Participants signed up for a single 1-hr laboratorysession and refrained from consuming any alcohol, nic-otine, or caffeine for 2 hr before the laboratory session.This was confirmed via self-report before beginning thelaboratory session. Following consent, a brief explana-tionof the studywasprovided.Electrodeswereattachedas explained previously, and the participant was intro-duced to the male confederate. The participant com-pleted the state form of the STAS to determine an initiallevel of state anger after the confederate left the room.The role play commenced following a 20-min period of
relaxation in which the last 6 min were recorded as theinitial rest period; HR was measured continuously andblood pressure was measured at 2-min intervals duringall rest periods throughout the procedure.
The participant was presented with a description ofthe first vignette and instructions to inhibit or exhibithis anger following the rest period. The confederatethen entered the room and the 3-min role play beganwith a standard prompt delivered by the confederate,followed by a 3-min recovery period. A second 6-minrest period occurred next, followed by instructions forthe second role play. Participants who exhibited theiranger during the first interaction were asked to inhibitit, and participants who inhibited their anger during thefirst interaction were asked to exhibit it openly duringthe second scenario. The second scene was also fol-lowed by a 3-min recovery period. After each role play,the participant completed the STAS, the AngerCognitions Inventory (ACI), and the self-report ratingsbased on his experience during the preceding role play.The confederate left the room during this period. Fol-lowing both role plays, all recording apparatuses weredetached. The participants were then debriefed and in-formed about the purpose of the study.
Results
Demographic Measures
Demographic data, depicted in Table 1, revealedthat the Indian men were significantly older than theWhite men, p < .0001. Self-reported anger expressiondid not differ across the two groups; however, the An-ger-Out score from Spielberger et al.’s Anger Expres-sion Inventory (Spielberger, 1988) was significantlylower among Asian Indian participants than theirWhite counterparts.
Data Analysis
The primary analytic method used in this investiga-tion was a 2 × 2 × 2 Group (White, Indian) × Order (in-hibited anger role play first or second) × Role Play (ex-
74
SUCHDAY AND LARKIN
Table 1. Means (and Standard Deviations) forDemographic Measures Among White and Asian IndianMen
Whitea Asian Indianb
M SD M SD
Age (yrs)** 20.27 2.84 24.95 1.66Anger in 18.60 4.93 18.11 3.89Anger out* 17.45 4.64 14.95 2.82Anger expression –1.15 8.63 –3.22 4.41
an = 40. bn = 20.*p < .05, **p < .0001.
hibited anger scene, inhibited anger scene) mixedfactors design. All analyses were calculated controllingfor age and anger-in/anger-out scores (STAXI anger ex-pression subscales), because those variables reflectedsignificant group differences during recruitment. For allthree cardiovascular indexes (i.e., HR, SBP, and DBP),analysis of covariance (ANCOVA) was used, adjustingfor respective pretask resting levels. For analyses of re-covery data, ANCOVAs also included task level as anadditional covariate. For purposes of presenting datapertinent to thehypothesesof this study,onlysignificantGroup main effects or any interactions with Group arepresented. The confidence level adopted for all analyseswas .05 and significant interactions were followed upusing F tests for simple main effects.
Self-Reported Measures of Affectiveand Cognitive Response
There was a significant Group × Role Play interac-tion for the ANCOVA on self-reported measures ofchange in HR, F(1, 50) = 8.56, p < .005. Mean compar-isons showed that among White participants, there wasa significantly greater participant report of HR increaseduring anger exhibition compared to anger inhibition,p < .0001 (see Table 2). Similar differences in detectingHR during the two role plays were not observed amongIndian participants. No group differences were ob-served on measures of state anger, arousal, or anxiety.
There was a significant main effect for Group on theanalysis on rational coping self-statements, F(1, 50) =4.46; p < .04. Asian Indian participants reported theuse of significantly greater cognitive self-statements
indicative of rational coping (M = 8.0) than White par-ticipants (M = 7.1). Likewise, Indian participants usedsignificantly greater repression self-statements (M =6.2) than their White counterparts (M = 3.6) duringboth role plays, F(1, 50) = 11.40; p < .002 (see Table2). No group differences were observed on Victimiza-tion or Self-Righteousness.
Behavioral Measures
There were no significant differences in behavioraldimensions between White and Asian Indian partici-pants (see Table 2).
Cardiovascular Measures
Resting cardiovascular levels. Indian partici-pants had lower resting SBP (M = 113.4 mm Hg) com-pared to their White counterparts (M = 120.6 mm Hg),F(1, 50) = 5.42, p < .02, regardless of the order of taskpresentation. Mean blood pressures during rest, roleplay, and recovery periods are reported in Table 3.
The ANOVA on resting HR revealed a significantGroup × Order × Role Play interaction, F(1, 50) = 4.48,p < .04. Analysis of simple main effects, however,failed to reveal any significant differences betweengroups. Post hoc contrast analyses revealed that themean resting HR of all White men (M = 77.0 bpm) washigher than the mean resting HR of Indian men (M =71.3 bpm), p < .03, except for the rest period prior toanger expression among Indian participants who ex-hibited anger first (M = 75.3).
75
RESPONSES TO ANGER PROVOCATION
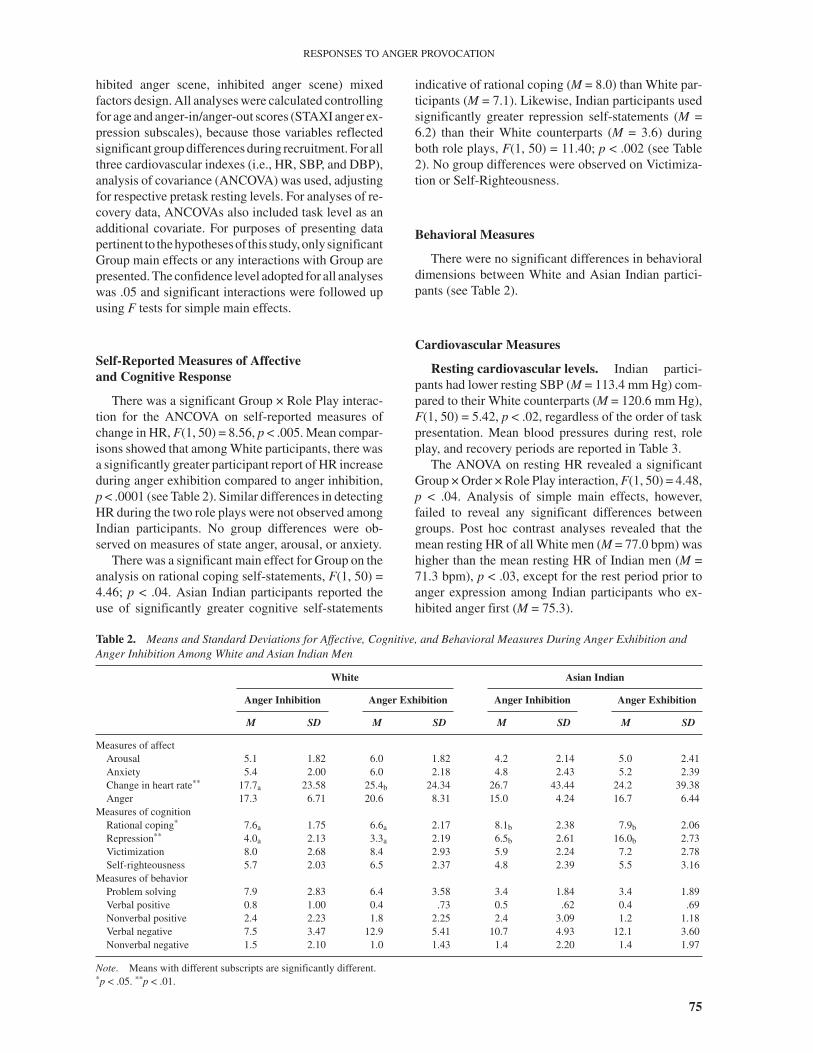
Table 2. Means and Standard Deviations for Affective, Cognitive, and Behavioral Measures During Anger Exhibition andAnger Inhibition Among White and Asian Indian Men
White Asian Indian
Anger Inhibition Anger Exhibition Anger Inhibition Anger Exhibition
M SD M SD M SD M SD
Measures of affectArousal 5.1 1.82 6.0 1.82 4.2 2.14 5.0 2.41Anxiety 5.4 2.00 6.0 2.18 4.8 2.43 5.2 2.39Change in heart rate** 17.7a 23.58 25.4b 24.34 26.7 43.44 24.2 39.38Anger 17.3 6.71 20.6 8.31 15.0 4.24 16.7 6.44
Measures of cognitionRational coping* 7.6a 1.75 6.6a 2.17 8.1b 2.38 7.9b 2.06Repression** 4.0a 2.13 3.3a 2.19 6.5b 2.61 16.0b 2.73Victimization 8.0 2.68 8.4 2.93 5.9 2.24 7.2 2.78Self-righteousness 5.7 2.03 6.5 2.37 4.8 2.39 5.5 3.16
Measures of behaviorProblem solving 7.9 2.83 6.4 3.58 3.4 1.84 3.4 1.89Verbal positive 0.8 1.00 0.4 .73 0.5 .62 0.4 .69Nonverbal positive 2.4 2.23 1.8 2.25 2.4 3.09 1.2 1.18Verbal negative 7.5 3.47 12.9 5.41 10.7 4.93 12.1 3.60Nonverbal negative 1.5 2.10 1.0 1.43 1.4 2.20 1.4 1.97
Note. Means with different subscripts are significantly different.*p < .05. **p < .01.
Cardiovascular reactivity to provocation. ForHR response, there was a significant Group × RolePlay interaction, F(1, 49) = 4.35, p < .04. Analysis ofsimple main effects revealed that adjusted mean HRduring anger expression was significantly higher thanadjusted mean HR during anger inhibition amongWhite participants, p < .02. Indian participants’ ad-justed mean HRs did not differ during the two roleplays.
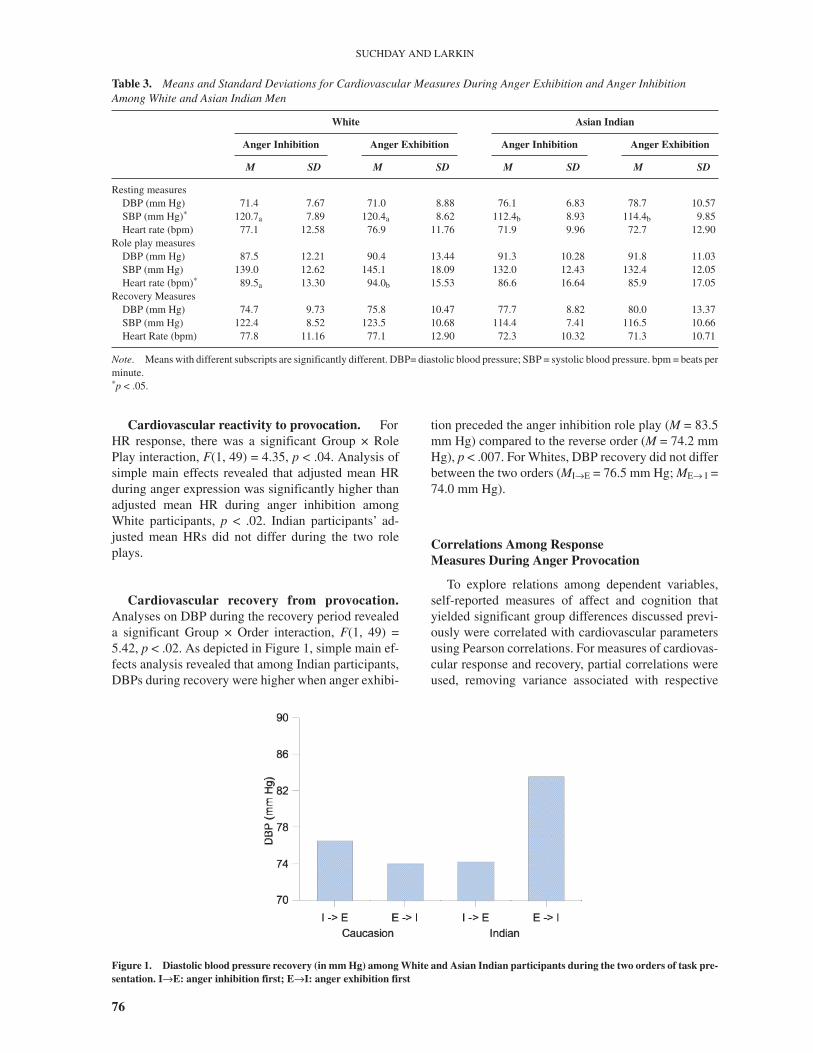
Cardiovascular recovery from provocation.Analyses on DBP during the recovery period revealeda significant Group × Order interaction, F(1, 49) =5.42, p < .02. As depicted in Figure 1, simple main ef-fects analysis revealed that among Indian participants,DBPs during recovery were higher when anger exhibi-
tion preceded the anger inhibition role play (M = 83.5mm Hg) compared to the reverse order (M = 74.2 mmHg), p < .007. For Whites, DBP recovery did not differbetween the two orders (MI→E = 76.5 mm Hg; ME→ I =74.0 mm Hg).
Correlations Among ResponseMeasures During Anger Provocation
To explore relations among dependent variables,self-reported measures of affect and cognition thatyielded significant group differences discussed previ-ously were correlated with cardiovascular parametersusing Pearson correlations. For measures of cardiovas-cular response and recovery, partial correlations wereused, removing variance associated with respective
76
SUCHDAY AND LARKIN
Table 3. Means and Standard Deviations for Cardiovascular Measures During Anger Exhibition and Anger InhibitionAmong White and Asian Indian Men
White Asian Indian
Anger Inhibition Anger Exhibition Anger Inhibition Anger Exhibition
M SD M SD M SD M SD
Resting measuresDBP (mm Hg) 71.4 7.67 71.0 8.88 76.1 6.83 78.7 10.57SBP (mm Hg)* 120.7a 7.89 120.4a 8.62 112.4b 8.93 114.4b 9.85Heart rate (bpm) 77.1 12.58 76.9 11.76 71.9 9.96 72.7 12.90
Role play measuresDBP (mm Hg) 87.5 12.21 90.4 13.44 91.3 10.28 91.8 11.03SBP (mm Hg) 139.0 12.62 145.1 18.09 132.0 12.43 132.4 12.05Heart rate (bpm)* 89.5a 13.30 94.0b 15.53 86.6 16.64 85.9 17.05
Recovery MeasuresDBP (mm Hg) 74.7 9.73 75.8 10.47 77.7 8.82 80.0 13.37SBP (mm Hg) 122.4 8.52 123.5 10.68 114.4 7.41 116.5 10.66Heart Rate (bpm) 77.8 11.16 77.1 12.90 72.3 10.32 71.3 10.71
Note. Means with different subscripts are significantly different. DBP= diastolic blood pressure; SBP = systolic blood pressure. bpm = beats perminute.*p < .05.
Figure 1. Diastolic blood pressure recovery (in mm Hg) among White and Asian Indian participants during the two orders of task pre-sentation. I→E: anger inhibition first; E→I: anger exhibition first

resting levels. Cognitive and affective measures werenot significantly correlated with cardiovascular mea-sures among Indian participants. Among White partic-ipants, rational coping was positively correlated withresting blood pressure before the anger inhibition roleplay (rSBP = .49, p < .001; rDBP = .46, p < .002; rHR
=.48, p < .002) and anger expression role play (rSBP =.41, p < .009; rDBP = .45, p < .003; rHR = .34, p < .04).Rational coping and repression were both correlatedwith HR reactivity during the anger inhibition roleplay, r = .38, p < .02 and r = .53, p < .001, respectively.In addition, rational coping was positively correlatedwith DBP reactivity during the anger inhibition inter-action (r = .36, p < .02). Repression was positively cor-related with SBP recovery (r = .41, p < .01) and HR re-covery (r = .34, p < .04) following the anger inhibitionrole play. Cardiovascular reactivity and recovery asso-ciated with the anger exhibition role play were not sig-nificantly correlated with any cognitive or affective re-sponse.
Discussion
Congruent with expectations, some differenceswere observed regarding responses to anger provoca-tion between White and Asian Indian men. Spe-cifically, White participants reported a greater increasein self-reported HR and actual HR during anger exhibi-tion in contrast to the anger inhibition role play. Thisdifference between anger exhibition and inhibition wasnot observed among the Indian participants in eitheractual or perceived HR. The correspondence betweenthese two modes of measuring HR provide rather com-pelling evidence that HR response among Whites ismuch greater during exhibition of anger than anger in-hibition, a phenomenon not observed among Indianparticipants.
These findings indicate that Indian participants maybe less responsive to expressing anger compared toWhite students, consistent with data from a South Af-rican study comparing Indians, Blacks, and Whites(Spangenberg, Shuda, & Robbertze, 1997). In thisstudy, White participants scored the highest of thethree groups on the Type A behavior pattern, an identi-fied risk factor for CHD and were also more prone toCHD compared to the other two groups. To the extentthat HR response to stress may be an indicator of riskfor CHD, Whites were shown to be at greater risk forCHD than Indian participants in our study. These find-ings also imply that Indian participants are equally re-sponsive to both anger expression and anger inhibition,in contrast to the differential response observed amongWhite students. These findings are similar to the pat-tern of responses among Indian participants observedby Bishop and Robinson (2000). In this study, Indianparticipants showed no differential response during
situations in which participants were harassed or notharassed while engaging in a laboratory stressor, incontrast to Chinese participants who evidenced differ-ential responses between the two conditions.
Interestingly, self-reported change in HR was notcorrelated with actual change in HR during either ofthe two role plays for either of the two groups—Whitesor Asian Indians. Participants, regardless of their coun-try of origin, were not particularly accurate predictorsof the actual extent of HR arousal that the anger provo-cation evoked. This is not particularly surprising, giventhat participants were engaged in a very active interac-tion during the time that they were presumably detect-ing these HR increases.
The link between CHD and anger expressionamong Indians, however, may occur via another physi-ological pathway and not via hyperresponsiveness ofHR to provocation. It is also possible that, given theemphasis on interpersonal harmony within the Indianculture, Indian participants may have been less willingto engage in an experimental situation requiring the ex-perience and expression of anger. Instead, they mayhave adopted learned patterns of not responding tocontrived anger provocation tasks or seeking alterna-tive modes of expressing emotion rather than reactingto the provocation. This was partly evidenced by theIndian participants’use of introspective cognitive strat-egies that were aimed at monitoring and coping withtheir reactions during anger provocation rather than ex-pressing their anger openly. In general, Indian partici-pants used significantly greater coping self-statementsthan White participants, including rational coping andrepression self-statements.
An interesting observation comparing the two groupsin this study was that Indian participants experienceddelayed DBP recovery when anger exhibition was thefirst role play compared to the opposite order, a findingnot observed among White participants. Among Indianparticipants in this study, if anger inhibition is indeed acultural norm, permitting them to experience this formof anger expression first enabled these participants torecover from the interactions more quickly. When In-dian participants were instructed to engage in the non-preferred anger exhibition first, delayed recovery forthe remainder of the experiment was noted.
Delayed cardiovascular recovery following provo-cation may explain the pathway by which Indian par-ticipants may be at risk for cardiovascular disorders.Given the emphasis on harmonious interpersonal inter-actions within the Indian culture, people may have lim-ited practice in reacting to and recovering from provo-cation. However, as we go about the business of living,provocation is inevitable. If Indian participants’cardio-vascular systems are unable to recover quickly follow-ing provocation, chronic elevations of blood pressuremay render individuals vulnerable to future cardiaccomplications.
77
RESPONSES TO ANGER PROVOCATION

The difference between White participants experi-encing enhanced HR reactivity during provocation andIndian participants experiencing delayed DBP recov-ery may perhaps allude to different hemodynamicpathways by which daily life stress renders the twogroups vulnerable to the development of CHD. AmongWhite participants, the tendency to experience elevatedcardiac responses to stress may describe a pattern ofhyperresponsivity to stress in their lives. Indian partici-pants, on the other hand, may react less intensely onmeasures of cardiac responsivity but tend to maintainelevated levels of DBP for extended periods of timefollowing stress, suggesting a vasoconstrictive re-sponse profile. These differences are further evidencedby the significant group difference in resting SBP.White participants had significantly higher restingSBP than Indian participants, but Indian participantshad higher (although not significantly) resting DBPsthan Whites. Although exploratory, these findings sug-gest differing cardiovascular pathways through whichWhites and Asian Indians are at risk for CHD.
The lack of behavioral differences between the twogroups is similar to findings from a previous studycomparing anger-in versus anger-out participants (Such-day & Larkin, 2001). Perhaps the behavior of both In-dian and White groups is influenced more by the in-structions given to them by the experimenter ratherthan their preferred behavioral styles. It is possible thatexternal behavior is more easily influenced by situa-tional demands in the laboratory whereas physiologi-cal, affective, and emotional responses are more easilyinfluenced by underlying individual or cultural differ-ences. Moreover, both the Indian and White partici-pants were enrolled in graduate or undergraduate pro-grams, in which there is a culture of behavingaccording to certain defined behavioral norms estab-lished by an academic institution.
Cultural Differences in Responseto Anger Provocation
Differences in cardiovascular response and recov-ery from stress may reflect cultural differences in theexpression of anger between persons raised in Indiaversus North America. Regardless of the heterogeneityof the participants from the two countries of origin ex-amined in this study, certain universal values underlieEastern and Western thought. Assertive expression ofdispleasure is a Western value and, therefore, may beuncomfortable for people of Asian Indian origin forwhom inhibition of anger is shaped. The elevated car-diovascular response to anger expression and delayedrecovery following anger expression both emphasizethe discomfort (to the extent that emotional discomfortis accompanied by cardiovascular arousal) experi-enced by Indian participants when engaging in cultur-ally discordant behavior.
The use of rational coping and repression self-state-ments was positively correlated with cardiovascularmeasures during resting, reactivity, and recovery peri-ods among White participants but not Asian Indianparticipants. Resting cardiovascular measures ob-tained before both role plays were positively correlatedwith rational coping. This appears to suggest that phys-iological arousal while waiting or in anticipation of thetasks by White men is associated with increased ratio-nal coping observed later during the task itself. Thus,increased cardiovascular arousal during anticipation ofinteraction tasks may serve as a marker for the prepara-tory cognitive coping activity used during subsequenttasks. However, because cognitive activity was notmeasured during the resting period in this study, thishypothesis remains for future research to examine. Thesignificant correlations between rational copingself-statements and HR and DBP reactivity to the angerinhibition role play indicate that the association be-tween this form of thinking and cardiovascular arousalwas maintained during the task that involved more ofan introspective approach. A comparable associationwas not observed during anger expression, when it islikely that participants focused more on using effectivebehavioral expressions of anger rather than introspec-tive means of coping with anger.
There was also evidence that the cognitive strategyof repression is related to both HR reactivity and mea-sures of SBP and HR recovery from the anger inhibi-tion role play. Similar to the findings on rational cop-ing, this form of cognitive activity was associated withincreased arousal and delayed recovery from the expe-rience of anger, again, only for the anger inhibitioncondition. Rather than reflecting effortful coping,however, it is likely that these associations represent afailure to cope adequately with the experience of angerunder conditions of anger inhibition, resulting in sus-tained cardiovascular arousal.
Of note, is the finding that the only associations ob-served between cognitive and cardiovascular measureswere observed during the anger inhibition role plays en-countered by the White men. The profile of the Asian In-dian men showed no association between cognitive andphysiological measures for either task. It is possible thattheuseof repressionand rational copingself-statementsrepresents a salient cultural trait related to the commonuse of introspective strategies among Indians. As de-scribed earlier, emotional expression is not reinforcedfor dealing with provocation among Indians. Hence,they may habitually use cognitive coping strategies thatdo not require them to expend as much effort in dealingwith anger inhibition as their White counterparts, whoevidenced strong associations between cognitive strate-giesandcardiovascularparameters throughout the labo-ratory session—resting, reactivity, and recovery, partic-ularly during the anger inhibition role play. It is possiblethat their elevated cardiovascular measures during the
78
SUCHDAY AND LARKIN

laboratory session may reflect the additional effort re-quired by White participants to use introspective strate-gies and to engage in a coping style that is not used fre-quently within Western culture.
Although the two groups did not differ on the totalanger expression score, Indian participants scored sig-nificantly lower than White participants on the an-ger-out scale. When correlations between anger-in andanger-out were computed for each group, there was anegative correlation between anger-in and anger-outamong White participants (r = –.63, p < .0001). An-ger-in and anger-out were not correlated among Indianparticipants. These data are contradictory to Sharma etal.’s (1996) data that found that anger-in and anger-outwere negatively correlated among Indian participants.White participants, according to Sharma et al.’s (1996)data responded to the anger expression subscales as or-thogonal dimensions. The reasons for this contradic-tion are unclear. However, these data clearly illustrate aneed for further investigation of the construct of angeramong Indian participants.
Conclusions
The findings of this study may be regarded as pre-liminary given the small sample size. However, theyraise intriguing possibilities that warrant future inquirypertaining to behavioral differences among ethnicgroups and their associated CHD risk. With a largersample, it may be possible to delineate specific re-sponse styles (e.g., the increased use of coping self-statements among people of Asian Indian descentcompared to Whites) that may then be positively corre-lated with measures of health. This study tested amethod for examining hypotheses regarding the as-sessment of the effects of prolonged inhibition of an-ger. This within-subject method of data collection andanalysis may help us explore the negative conse-quences of more enduring states of anger inhibition,such as that which occurs in schools, places of work,social organizations, neighborhood societies, and dailylife. Membership in all of these institutions requiresome anger inhibition to get along. It is possible thatprolonged inhibition of anger may actually teach peo-ple an alternative way of functioning, as their cardio-vascular system adjusts and develops a homeostaticbalance to the situation. On the other hand, lack of ad-aptation may also lead to prolonged periods of vigi-lance and cardiovascular responding that may be harm-ful over time, resulting in cardiovascular disease.
References
Basu, R. (1991).Hyperreactivity and essential hypertension: A be-havioural approach. Journal of the Indian Academy of AppliedPsychology, 17, 86–92.
Bishop, G. D., & Quah, S. H. (1998). Reliability and validity of mea-sures of anger/hostility in Singapore: Cook-Medley Ho Scale,STAXI, and Buss-Durkee Hostility Inventory. Personality andIndividual Differences, 24, 867–878.
Bishop, G. D., & Robinson, G. (2000). Anger, harassment, and car-diovascular reactivity among Chinese and Indian men in Singa-pore. Psychosomatic Medicine, 62, 684–692.
Diener, E., & Diener, M. (1995). Cross-cultural correlates of life sat-isfaction and self-esteem. Journal of Personality & Social Psy-chology, 68, 653–663.
Everson, S. A., Goldberg, D. E., Kaplan, G. A., Julkunen, J., &Salonen, J. T. (1998). Anger expression and incident hyperten-sion. Psychosomatic Medicine, 60, 730–735.
Faber, S. D., & Burns, J. W. (1996). Anger management style, degreeof expressed anger, and gender influence cardiovascular recov-ery from interpersonal harassment. Journal of Behavioral Med-icine, 19, 31–53.
Forgays, D. K., Richards, J. C., Forgays, D. G., & Sujan, S. (1999).Examination of the AHA!-illness relation in male and femaleuniversity students from Australia, India, and the United States.International Journal of Behavioral Medicine, 6, 64–77.
Farooqi, A., Nagra, D., Edgar, T., & Khunti, K. (2000). Attitudes tolifestyle factors for coronary heart disease amongst SouthAsians in Leicester: A focus group study. Family Practice, 17,293–297.
Hodge, A. M., Dowse, G. K., Collins, V. R., Alberti, K. G.,Gareeboo, H., Tuomilehto, J., & Zimmet, P. Z. (1996). Abdomi-nal fat distribution and lipid levels only partially explain ad-verse cardiovascular risk profile in Asian Indians. Journal ofCardiovascular Risk, 3, 263–270.
Hops, H., Mills, T. A., Patterson, G. R., & Weiss, R. L. (1972). Mari-tal interaction coding system. Eugene, OR: Oregon ResearchInstitute.
Hofstede, G. (1980). Culture’s consequences. Beverly Hills, CA:Sage.
Kaushik, S. S., Mukhopadhyay, A., Sheik, K., & Goel, S. K. (1994).A comparative study of male and female CHD patients on somepsychophysical correlates. Indian Journal of Clinical Psychol-ogy, 18, 49–53.
Krantz, D. S., & Manuck, S. B. (1984). Acute psychophysiologicalreactivity and risk of cardiovascular disease: A review andmethodological critique. Psychological Bulletin, 96, 435–464.
Larkin, K. T., Frazer, N. L., & Semenchuk, E. M. (1996). Physiologi-cal, affective, and behavioral responses to interpersonal conflictamong males from families with different levels of cohesionand adaptability. Journal of Psychopathology and BehavioralAssessment, 18, 239–254.
Larkin, K. T., Semenchuk, E. M., Frazer, N. L., Suchday, S., & Tay-lor, R. L. (1998). Cardiovascular and behavioral responses tosocial confrontation: Measuring real-life stress in the labora-tory. Annals of Behavioral Medicine, 20, 294–301.
Miller, J. G. (1984). Culture and the development of everyday socialexplanation. Journal of Personality & Social Psychology, 46,961–978.
Miller, J. G., & Bersoff, D. M. (1992). Culture and moral judgment:How are conflicts between justice and interpersonal responsi-bilities resolved? Journal of Personality & Social Psychology,62, 541–554.
Miller, S. B., Dolgoy, L., Friese, M., & Sita, A. (1996). Dimensionsof hostility and cardiovascular response to interpersonal stress.Journal of Psychosomatic Research, 41, 81–95
Oyserman, D., Coon, H. M., & Kemmelmeier, M. (2002). Re-thinking individualism and collectivism: Evaluation of theoreti-cal assumptions and meta-analyses. Psychological Bulletin,128, 3–72.
Reddy, K. S. (1999). Primordial prevention of coronary heart diseasein India: Challenges and opportunities. Preventive Medicine,29, S119–S123.
79
RESPONSES TO ANGER PROVOCATION

Sahoo, F. M., & Bidyadhar, S. (1995). A cultural validation ofneed-saliency model: An empirical investigation in a non-West-ern context. Psychological Studies, 40, 120–125.
Sharma, S., Krishna, A., & Spielberger, C. D. (1996). Anger and anxi-ety in hypertensive patients in India. In C. D. Spielberger, I. G.Sarason, J. M. T. Brebner, E. Greenglass, P. Laungani, & A. M.O’Roark (Eds.), Stress and emotion: Anxiety, anger, and curios-ity (Vol.16,pp.261–268).Tampa:UniversityofSouthFlorida.
Shukla, P. R. (1995). Personality traits and coronary heart disease(CHD) patients. Journal of Personality & Clinical Studies, 11,83–86.
Siegman, A. W. (1993). Cardiovascular consequences of expressing,experiencing, and repressing anger. Journal of BehavioralMedicine, 16, 539–569.
Siegman, A. W., & Snow, C. W. (1997). The outward expression ofanger, the inward experience of anger and cardiovascular reac-tivity: The role of vocal expression. Journal of Behavioral Med-icine, 20, 29–45.
Smith, T. W. (1992). Hostility and health: Current status of a psycho-somatic hypothesis. Health Psychology, 11, 139–150.
Spangenberg, J. J., Shuda, S., & Robbertze, U. C. (1997). Type A be-havior and hostility in final year South African students. SouthAfrican Journal of Psychology, 27, 30–36.
Spielberger, C. D. (1988). State Trait Anger Expression Inventory.Odessa, FL: Psychological Assessment Resources.
Sturges, L. V., & Goetsch, V. L. (1996). Physiological reactivity andheart beat awareness in anxiety sensitivity. Journal of AnxietyDisorders, 10, 283–294.
Suchday, S., & Desiderato, O. (1991, April). Factor analysis of ananger cognitions inventory. Paper presented at the 13th An-nual Meeting of The Society for Behavioral Medicine, NewYork.
Suchday, S., & Larkin, K. T. (2001). Biobehavioral responses tointerpersonal conflict during anger expression among anger-in and anger-out males. Annals of Behavioral Medicine, 23,282–290.
Triandis, H. C. (1995). Individualism and collectivism. Boulder, CO:Westview.
Triandis, H. C., & Suh, E. M. (2002). Cultural influences on person-ality. Annual Review of Psychology, 153, 133–160.
Vogele, C., Jarvis, A., & Cheeseman, K. (1997). Anger suppression,reactivity, and hypertension risk: Gender makes a difference.Annals of Behavioral Medicine, 19, 61–69.
Vogele, C., & Steptoe, A. (1992). Emotional coping and tonicblood pressure as determinants of cardiovascular re-sponses to mental stress. Journal of Hypertension, 10,1079–1089.
Weider, G. B., & Weiss, R. L. Generalizability theory and the codingof marital interactions. Journal of Consulting Clinical Psychol-ogy, 48, 469–477, 1980.
80
SUCHDAY AND LARKIN