psoriasis recent advances and existing therapy in psoriasis
TRANSCRIPT

RECENT ADVANCES IN PSORIASIS
DR. SIDDHARTHA DUTTAMAMC, New Delhi

contents Introduction Etiology Pathophysiology Current treatment options Challenges When to switch? Newer targets New molecules limitations Summary

Introduction “Psora” means itch Term used since 133 AD, earlier was grouped with
leprosy until 19th century In 1881, Thin described psoriasis Psoriasis is a chronic inflammatory immune-
mediateddisease of skin and joints affecting around 0. 5-1% ofchildren and 2- 3% of adults worldwide

Psoriasis A chronic, non-contagious disease of the
skin, in which silvery white masses of epidermic scales are attached, more or less firmly to a reddish vascular base
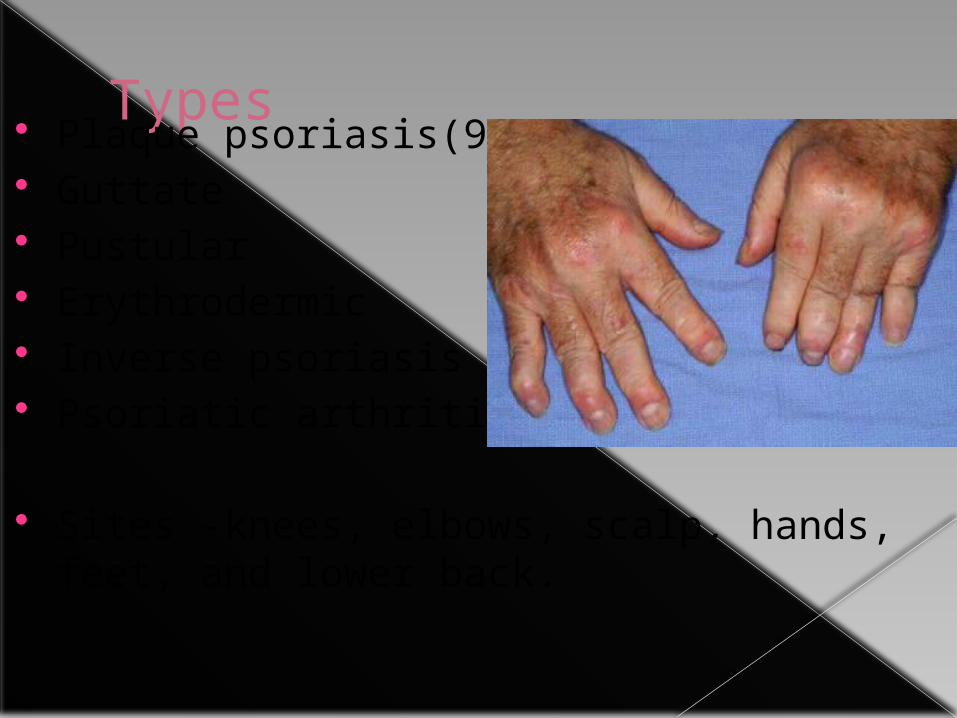
Types Plaque psoriasis(90%) Guttate Pustular Erythrodermic Inverse psoriasis Psoriatic arthritis
Sites -knees, elbows, scalp, hands, feet, and lower back.

ETIOLOGY
Idiopathic Stress Genetic(HLA-cw6) local trauma(koebner phenomenon) Infections (streptococcus, HIV) Drugs (beta-blockers, lithium, chloroquine) Sunlight Alcohol & smoking

Skin in normal vs psoriasis

Current treatment Topical corticosteroids Vitamin D analogues Anthralin Coal tar Retinoids Light therapy (phototherapy) Oral therapy

DRUG M.O.A INDICATION
LIMITATIONS
CORTICOSTEROID
binds to cytosolic receptors modulates the regulatory proteins & silencing gene transcription for proinflammatory proteins
Ps Thinning of the skin, telangiectasia, diabetes, hypertension and HPA suppression
VIT D ANALOUGUES• Calcipotriene• Calcitriol
Binds to cytoplasmic receptor & translocates into nucleusregulates transcription of genes, cell differentiation and causes inhibition of cell proliferation and inflammation
Ps Skin irritation, rednessRarely increased urinary calcium level
ANTHRALIN(dithranol)
induce release of ROS with an inhibiting effect on proliferation of keratinocytes and leucocytes
Ps discolouration of hair, irritates the skin and it stains virtually anything it touchesdithranol-induced dermatitis
COAL TAR ↓ DNA replication & makes the skin more sensitive to UV light(?)
Ps messy, stains clothing and bedding, and has a strong odour

DRUG M.O.A INDICATION
LIMITATIONS
METHOTREXATE
DHFRase inhibitor PsPsA
Myelosuppression, mucositis Hepatotoxicity, pul fibrosis, Nephotoxic, neurotoxic
CYCLOSPORINE Inhibits the activation of NFAT &inhibition of gene transcription of of IL-2 by t cells
Ps Nephrotoxicity, hepatotoxicity, HTN, DM, neurotoxicity, hirsutismrisk of infection increases
RETINOIDS normalizes DNA activity in skin cells and may decrease inflammation
Ps skin irritation, increase sensitivity to sunlightC/I- pregnancy & lactation
PHOTOTHERAPY
Induces apoptosis & enhanced transcription and expression of IL-10 in keratinocytes
Ps redness, itching and dry skin
PUVA(2 to 3 sessions a week)
Psoralen sensitizes the skin to uv raysMore aggressive therapy
Ps headache, burning and itchingwrinkled skin, freckles & skin cancer

Challenges long-term safe control of psoriasis remains a problem Cumulative toxic effects are a limitation of classical
treatment Traditional topical therapy, phototherapy systemic
therapy has low compliance among patients Past decade, treatment development has been based
on mechanisms of pathogenesis Pathogenesis-based treatments with a selective and
focused action are likely to cause fewer side-effects

National Institute for Health and Care Excellence (NICE)
The recommendation are
Patients being considered for treatment withbiologics should have severe disease defined by a total psoriasis area and severity index (PASI) score of 10 or more (20 for infliximab)
Ineligible for phototherapy or traditionalsystemic treatment due to contraindications, intolerance or previous treatment failure

PSORIASIS
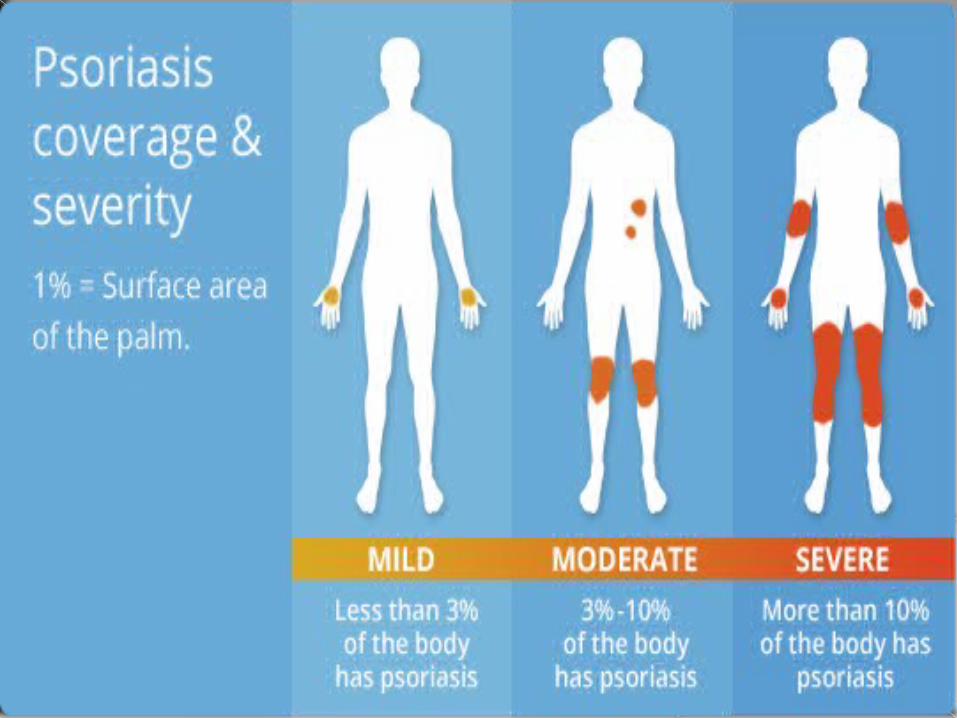
MODERATE TO SEVERE
(>15% BSA)
nUVB/PUVAMethotrexateCyclosporinretinoids
MILD TO MODERATE(<10% BSA)Vitamin
D analogueRetinoidCoal-tar Corticost
eroid Dithranol
BIOLOGICS
1ST LINE
2ND LINE
3rd LINE

BIOLOGICSANTI TNF α AGENTS IL-17 A INHIBITORSINFLIXIMAB SECUKINUMABETANERCEPT IXEKIZUMABADALIMUMAB CERTOLIZUMAB GOLIMUMAB JAK INHIBITOR TOFACITINIBIL-12 & IL-23 INHIBITORS PDE4 INHIBITOR USTEKINUMAB APREMILAST APILIMODIL-17 A RECEPTOR INHIBITOR MISC.BRODALUMAB ALEFACEPT ITOLIZUMAB

Drug targets
brodalumab

Anti TNF α agents INFLIXIMAB ETANERCEPT ADALIMUMAB CERTOLIZUMAB GOLIMUMAB

INFLIXIMAB Ist biologic, approved by FDA in sept 2006 Chimeric anti–TNF-α MAb 5 mg/kg as IV infusion at 0, 2 and 6 weeks followed by
a every 8 weeks thereafter Ist 3 infusion under supervision Adverse effects-Infusion reaction within 1-2 hours after Ab administration The development of ANA and rarely a lupus-like syndrome RA, Chohn’s, UC, Ank. spond Off label- Behcet’s disease

Etanercept FDA approved in jan 2002 TNF α receptor fusion protein Lesser efficacy than infliximab S.C. inj twice weekly 50mg/week C/I- Multiple sclerosis, CHF,
immunosuppression, hepatitis B RA, Ank spond

Adalimumab FDA approved in oct 2005 for PsA & in 2008 for
plaque psoriasis S.C inj 40mg once weekly every other week Better efficacy than infliximab & etanercept C/I- CHF,Multiple sclerosis T.B, immunosupression S/e- lymphoma, lupus like syndrome Malignancy rate is lower RA, Chohn’s, UC, Ank. spond

Certolizumab FDA approved in sept 2013 for PsA S.C inj 400 mg taken at week 0,week2,week4 then
every 2 weeks thereafter 78.4 % vs 6% with placebo S/E- T.B, CHF, lupus like syndrome, hep b reactivation easy bruising RA, Crohn’s
Golimumab FDA approved in april 2009 for PsA S.C, 50 mg once a month S/e- T.B, increased risk of infection, increased risk of bruising &bleeding CHF, lymphoma, lupus like syndrome, hepatotoxicity RA

IL-12 & IL-23 INHIBITORS
Ustekinumab Apilimod

Ustekinumab FDA approved in sept 2009 for PsA in sept 2013 for
plaque psoriasis Human MAb that targets the p40 subunit of both
interleukin (IL)-12 and 23 Inj S.C Two initial doses at week 0 and week 4, then once
every 12 weeks Efficacious than most TNF a agents 74% vs 57% with etanercept Dose- 45mg for 220 lb or less 90 mg for > 220 lb C/I- T.B, lymphoma & PML

Apilimod Phase 3 p19 subunit of both interleukin (IL)-12
and 23 Administered Orally Apilimod 70 mg daily achieved a PASI-50 at
12 weeks

IL-17 A INHIBITORS SECUKINUMAB IXEKIZUMAB

Secukinumab FDA approved in jan 2015 Anti-IL-17A monoclonal antibody Efficacious than etanercept 82.8 % vs. 44% 300mg/dose S.C Inj once a week for first 5 weeks, then every 4 weeks thereafter Screened for latent T.B Nasopharyngitis, headache, diarrhoea, URI,
rarely neutropenia

IXEKIZUMAB FDA approved on 22 march 2016 for Ps Phase 3 for PsA 68 to 71 % achieved virtually clear skin (PASI 90) 35 to 42 % saw complete resolution(PASI 100) at week
12 87 percent vs. 41 percent for PASI 75 with etanercept Inj S.C. 160mg stat then 80 mg every 2 week

IL-17 A RECEPTOR INHIBITOR
BRODALUMAB

Brodalumab Anti IL-17 receptor A MAb for the treatment of
moderate to severe plaque psoriasis Phase 3 development The week 12 PASI 100 response rates were significantly higher with 210 mg of brodalumab than with ustekinumab (44% vs. 22%) Neutropenia were higher than with ustekinumab


Tofacitinib Oral Janus kinase inhibitor Phase 3 Aprroved for RA in 2012

ALEFACEPT Fusion protein Fda approved in jan 2003 for psoriasis

LFA-3 portion of alefacept binds to CD2 on T lymphocyte
blocks the interaction between LFA-3 and CD2 and interfering with T-cell activation
15 mg IM or 7.5 mg IV per week S/E- lymphopenia, skin cancers, lymphomas, hepatotoxicity

Apremilast Inhibitor of PDE4 March 2014, the US FDA approved apremilast
for psoriatic arthritis

Inhibition of IL-2, IL-4, IL-13, IFN- g, TNF- a Effective and well tolerated in clinical trials
in psoriasis (phase III) 30mg BD Better than etanercept, but less potent than cyclosporine S/e- diarrhoea, nausea, URI, headache & wt loss Has been linked to depression and suicidal thoughts

Itolizumab Anti CD-6 MAb Blocks the signaling and differentiation of T cells into
Th1 & Th 17 Pre-clinical studies have shown It inhibits intracellular
mitogen-activated protein kinase (MAPK) and signal transducer and activator of transcriptor3 (STAT-3) which are involved in intracellular signaling pathways triggered by CD6
Downregulates gene transcription of pro-inflammatory cytokines and adhesion molecules

Available as 25 mg/5 mL vials for (IV) injection (brand name Alzumab™)
Administered as IV infusion 1.6 mg/kg once every 2 weeks for 12 weeks & 1.6 mg/kg once in 4 weeks until 24 weeks S/e- infusion reaction, URI, UTI, lymphopenia Risk of infection is less No data on cancers


Recent modulation in phototherapy Narrow band UVB therapy(311-313 nm) More effective than broadband UVB treatment Usually administered 2 to 3 times a week until the skin improves, then maintenance may require only weekly sessions Narrow band UVB therapy may cause more severe and longer lasting burns

Goeckerman therapy –Combination of UVB treatment and coal tar treatment The two therapies together are more effective than either
alone because coal tar makes skin more receptive to UVB light Once in three-week, inpatient basis Safe and reliable, even in patients unresponsive to other conventional
therapies Results in long-term remissions
Targeted phototherapy The excimer laser—recently approved by FDA for treating chronic, localized psoriasis Emits a high-intensity beam of ultraviolet light B (UVB)

Drugs in pipeline Voclosporin phase 3 Calcineurin inhibitor AN2728 phase 1 PDE-4 inhibitor Baricitinib phase 2 JAK inhibitor ASP015K phase 2 JAK inhibitor Ruxolintinib phase 1 JAK inhibitor CNTO 1959 phase 2 Anti-iL-23 (p19) MK-3222 phase 3 Anti-iL-23 (p19) SCH900222 phase 2 Anti-iL-23 (p19) APG2305 phase 2 Anti-iL-23 receptor

Limitations Biologics do not cure Ps or PsA but can relieve
symptoms and may help to prevent further joint damage
High cost(3000$ to 6000$ per month), a challenge especially for early intervention
Risk of infection is 20 to 40% higher than methotrexate
CHF, MS, lupus- Most of the people improved after stopping treatment, indicates the biologic drug was the cause
Cancers of the breast, colon, skin, lymphoma Long-term risks of the biologics have not been
identified yet


THANK YOU