progression of keratoconus in patients wearing pancorneal toric edge rigid gas-permeable contact...
TRANSCRIPT

G
C
Pr
Wa
b
a
ARR1A
KCPKR
1
ip[bisd[
oN
1h
ARTICLE IN PRESS Model
LAE-681; No. of Pages 6
Contact Lens & Anterior Eye xxx (2013) xxx– xxx
Contents lists available at ScienceDirect
Contact Lens & Anterior Eye
jou rn al hom ep age : w w w.elsev ier .com/ locate /c lae
rogression of keratoconus in patients wearing pancorneal toric edgeigid gas-permeable contact lenses
ishal D. Ramdasa,b,∗, Charles J.W.C. Vervaeta
Department of Ophthalmology, Erasmus Medical Center, Rotterdam, The NetherlandsDepartment of Epidemiology, Erasmus Medical Center, Rotterdam, The Netherlands
r t i c l e i n f o
rticle history:eceived 20 August 2013eceived in revised form2 November 2013ccepted 26 November 2013
eywords:ontact lensancornealeratoconus progressionigid gas-permeable
a b s t r a c t
Purpose: To investigate the rate of progression of keratoconus in patients wearing pancorneal toric edgerigid gas-permeable contact lenses (pancorneal RGP-CL) compared to non-pancorneal RGP-CL. We alsoevaluated alterations in anterior chamber parameters with the progression of keratoconus and investi-gated the location of the cone in eyes with keratoconus.Methods: The current study was a retrospective study including patients with clinically evident kerato-conus from the outpatient clinic from the Department of Ophthalmology of the Erasmus Medical Center,Rotterdam, the Netherlands. Medical history and contact lens characteristics were documented. All par-ticipants underwent ophthalmic examination including corneal topography. Corneal topography wasrepeated at one of the consecutive visits of the patient. Patients were divided into two groups: thosewearing pancorneal RGP-CL and those wearing other contact lens types. As a measure of progression ofkeratoconus differences in corneal topography parameters between both groups were compared.Results: A total of 82 patients were included of which 42 had follow-up (mean 17.8 months) data. Wefound a significant difference in progression between eyes fitted with and without pancorneal RGP-CL (K-flat: p = 0.09, K-steep: p = 0.02, K-mean: p = 0.02, and K-minimum: p = 0.04). Compared with eyesfitted without pancorneal RGP-CL no significant difference in K-values was found for eyes fitted with
pancorneal RGP-CL during follow-up. Furthermore, a significant decrease in anterior chamber volume(p < 0.001) and corneal volume (p = 0.008) was found during follow-up. In 86.6% the location of the conewas located infero-temporal.Conclusions: Pancorneal RGP-CL have a better effect on stabilizing progression of keratoconus than non-pancorneal RGP-CL. The finding of an infero-temporal location of the cone in keratoconic corneas mayimprove results of contact lens fitting and surgical management.Britis
© 2013. Introduction
Keratoconus is an insidious progressive, often bilateral but typ-cally asymmetric [1], non-inflammatory ectasia of the cornea. Therevalence of keratoconus is 1 in ∼1800 in the general population2,3]. Keratoconus has been described more than 150 years ago [4],ut its etiology is still largely unknown [5,6]. Known risk factors
nclude atopy, many systemic and ocular diseases (e.g., Downyndrome, Leber’s congenital amaurosis, and connective tissue
Please cite this article in press as: Ramdas WD, Vervaet CJWC. Progressgas-permeable contact lenses. Contact Lens Anterior Eye (2013), http://dx.
isorders), and in 6–8% a positive family history of keratoconus3,7,8]. To date only a few (rare) genes have been identified [5,9].
∗ Corresponding author at: Departments of Ophthalmology and Epidemiol-gy, Erasmus Medical Center Rotterdam, PO Box 2040, 3000 CA Rotterdam, Theetherlands. Tel.: +31 10 7033691; fax: +31 10 7035105.
E-mail address: [email protected] (W.D. Ramdas).
367-0484/$ – see front matter © 2013 British Contact Lens Association. Published by Elsttp://dx.doi.org/10.1016/j.clae.2013.11.012
h Contact Lens Association. Published by Elsevier Ltd. All rights reserved.
Modifiable risk factors that may cause progression include eyerubbing and hard contact lens wear [10].
The irregular conical shape, i.e. curvature, of the cornea resultsin refractive errors (myopia and astigmatism) leading to signifi-cant visual impairment. The disease is highly variable in its course.Classically, the onset of keratoconus occurs at early adolescence,but it may also comment later in life. The visual impairment andtreatment of keratoconus, especially in younger adults, has a veryhigh impact on the quality of life [11,12]. Treatment modalities canbe conservative (spectacle correction, contact lenses) or surgical(graft surgery, intracorneal rings, corneal collagen cross-linking).Although the need for a corneal transplant can be reduced signifi-cantly with Riboflavin/Ultraviolet-A-induced collagen crosslinking[13], keratoconus is still one of the leading indications for corneal
ion of keratoconus in patients wearing pancorneal toric edge rigiddoi.org/10.1016/j.clae.2013.11.012
graft surgery [14]. The visual impairment-related quality of life andespecially the probability of corneal transplant (and subsequentregraft) strongly influence the economic burden of keratoconus inhealth care [15]. The lifetime need of a corneal transplantation,
evier Ltd. All rights reserved.

ING Model
C
2 act Len
ocT[fGccpittf[rs
canri
2
2
tRtl2t
a
2
farads
2
ttctdosTep
iaoti
ARTICLELAE-681; No. of Pages 6
W.D. Ramdas, C.J.W.C. Vervaet / Cont
ften deep anterior lamellar keratoplasty [16], is 10–20%; in otherases it can be delayed or avoided by using contact lenses [5,17].he first contact lens reports came from Germany around 188818]. Since than it has represented the most common and success-ul treatment option for early to moderate cases of keratoconus [5].ood results have been reported with fitting rigid gas-permeableontact lenses [19,20]. Pancorneal toric edge rigid gas-permeableontact lens (from here on called pancorneal RGP-CL) may removeressure, as the toric shape of this contact lens allows the bear-
ng toward the limbal area and may distribute pressure away fromhe cone to the rest of the cornea (see Section 2) [21]. The loca-ion of the cone can be a valuable predictor in finding the best fitor contact lenses, but also depends on the severity of keratoconus3,22]. Regarding the severity and progression of keratoconus ante-ior chamber parameters may be of clinical interest, but data arecarce [23].
The aim of the current study was to investigate whether pan-orneal RGP-CL wear can stabilize progression of keratoconusssessed with corneal topography, and whether this differs fromon-pancorneal RGP-CL. We also evaluated alterations in ante-ior chamber parameters with the progression of keratoconus andnvestigated the location of the cone in eyes with keratoconus.
. Methods
.1. Study population
The present study was performed at the outpatient clinic ofhe department of Ophthalmology of the Erasmus Medical Center,otterdam, the Netherlands. Medical records of patients with kera-oconus were checked. Patients were included if they underwent ateast one Pentacam scan. Baseline examination took place between007 and 2012. Patients who changed type of contact lens duringhe study were excluded.
The Medical Ethics Committee of the Erasmus Universitypproved the study.
.2. Ophthalmic examination
The ophthalmic examination was almost similar at baseline andollow-up and included measurement of the best-corrected visualcuity with the Snellen chart, slit lamp examination, corneal topog-aphy (Pentacam; Oculus Optikgeräte GmbH, Wetzlar, Germany),nd in some cases Javal-Schiötz ophthalmometer to confirm theiagnosis of keratoconus. All examinations were performed by theame investigator (CJWCV).
.3. Corneal topography
At the end of 2006 we upgraded to the Pentacam HR. The Pen-acam is a computerized videokeratoscope: it is a projection-basedopographer consisting of a Placido cone and a rotating Scheimpflugamera allowing high depth of focus and sharp picture. The rota-ional measuring procedure generates Scheimpflug images in threeimensions. It takes a maximum of 2 s to generate a complete imagef the anterior eye segment. Any eye movement is detected by aecond camera and corrected for in the process to some extent.he Pentacam calculates a 3-dimensional model of the anteriorye segment from as many as 25,000 (HR: 138,000) true elevationoints.
All Pentacam scans took place in dim-light conditions. Themage of the eye was observed on the monitor, brought into focus,
Please cite this article in press as: Ramdas WD, Vervaet CJWC. Progressgas-permeable contact lenses. Contact Lens Anterior Eye (2013), http://dx.
nd centered within the aiming circle with the help of markingsn the monitor. When a clear image was maintained and focused,he device took the Scheimpflug images automatically. Excellentntra- and interoperator reproducibility have been reported for the
PRESSs & Anterior Eye xxx (2013) xxx– xxx
Pentacam. Central corneal thickness values obtained with the Pen-tacam are similar to those obtained with ultrasound pachymetry[24].
The following parameters of the corneal topography wereanalyzed: pachymetry (measured at the apex, pupil, andthinnest/minimal value), irregularity indices (ISV [index of sur-face variance], IVA [index of vertical asymmetry], KI [keratoconusindex], CKI [center keratoconus index], IHA [index of heightasymmetry], IHD [index of height decentration], ABR [aberrationcoefficient]) [34] corneal volume (total, in the inner 3, 5 and 7 mmcircle), anterior chamber (depth, volume and angle), and K-values(K-flat, K-steep, K-mean, K-minimum). All K-values were calculatedas radius in mm. K-Flat is the flattest curvature from either thehorizontal or vertical meridian of the cornea, whereas K-steep isthe steepest of both (horizontal and vertical). K-Minimum repre-sents the minimum radius of the curvature, which is equal to thesteepest curvature anywhere on the cornea. Of these K-values onlyK-minimum is not necessarily located at the center of the cornea.
2.4. Contact lenses
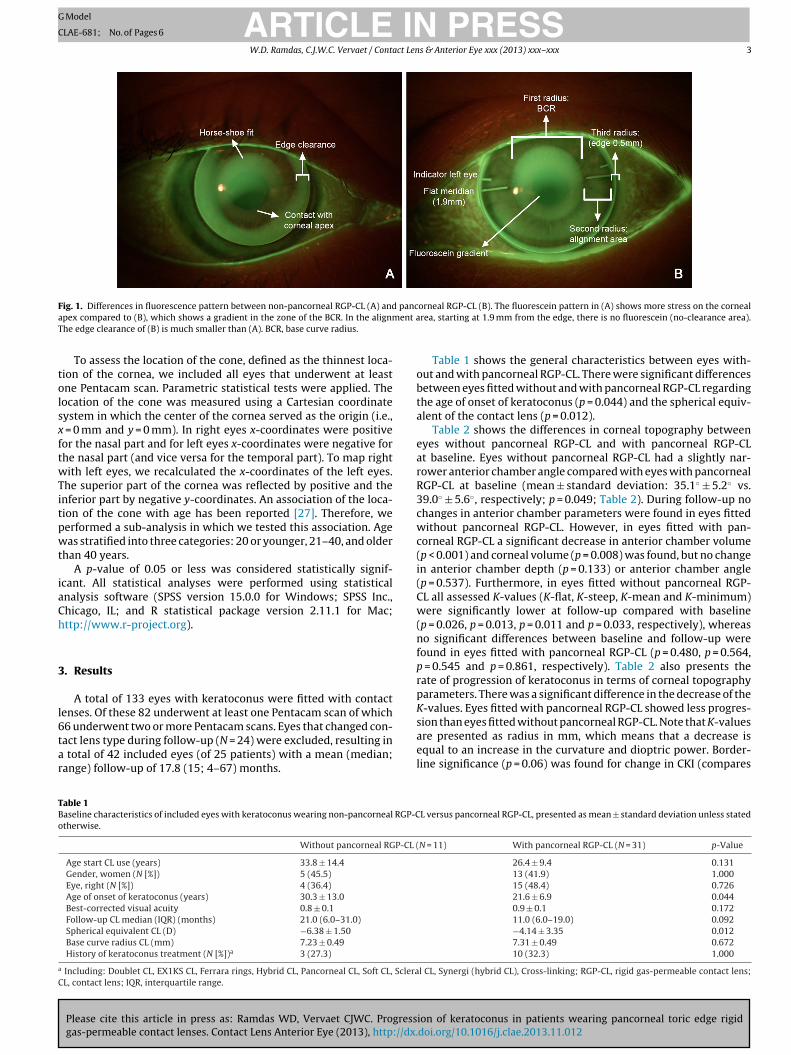
Fitting of contact lenses was tested and refined by analyzingfluorescence patterns behind a slitlamp [25]. Fig. 1 shows the dif-ference in fluorescein patterns between non-pancorneal RGP-CLand pancorneal RGP-CL. Designs of contact lenses for keratoconustypically have a smaller diameter to minimize stress on the cone.However, this may result in more mobility of the contact lens.Increasing the diameter reduces the mobility of the contact lens,but increases the risk of the contact lens getting vacuumed to thecornea.
Included contact lenses were: hybrid lens (Synergeyes; ML662,hard contact lens with a soft edge), SRF (scleral lens edge- andfronttoric), SRT (scleral lens edgetoric), TRT (triradial edgetoric),TRF (triradial edge- and fronttoric), and TRP (triradial edge- andfronttoric with prismstabilisation). The last three mentioned con-tact lenses are pancorneal toric edge rigid gas-permeable contactlenses (pancorneal RGP-CL). Details about the pancorneal RGP-CLand about the other contact lenses are described elsewhere [21,26].
A traditional method of fitting contact lenses in eyes with kera-toconus is by using lens designs with a small and steep optical zonein combination with a progressive flattening of peripheral curves.Over the years it became quite clear that as a result of blinkingand gaze excursions these contact lenses are mobile in vertical andhorizontal direction. Two negative side effects may occur: mechan-ical stress on the apex due to the flat periphery, and dry spots onthe cornea often seen in the 3–9 o’clock zone where the cornea isnot covered by a contact lens. The pancorneal RGP-CL investigatedin the current study copes with these issues. The aim of this con-tact lens was to achieve three goals [21]. First, the central area ofthe contact lens was elevated to avoid mechanical pressure on thecone. Secondly, the mobility of the contact lens on blinking or gazeexcursions was minimized by sizing up the diameter of the contactlens and using front stabilization to prevent rotational movementin cases of oblique meridians of cylindrical errors. Thirdly, the mostdifficult part, not to have the lens vacuumed to the cornea. All thefittings were done individually with a trial set.
2.5. Statistical analyses
Differences in baseline characteristics were analyzed withMann–Whitney U-tests and Fisher’s exact test (2-sided) statistics.
ion of keratoconus in patients wearing pancorneal toric edge rigiddoi.org/10.1016/j.clae.2013.11.012
Corneal topographic changes during follow-up were analyzed usingthe paired Wilcoxon-test. Differences in rate of change of cornealtopographic parameters between eyes fitted without and with pan-corneal RGP-CL were analyzed using the Mann–Whitney U-test.
ARTICLE IN PRESSG Model
CLAE-681; No. of Pages 6
W.D. Ramdas, C.J.W.C. Vervaet / Contact Lens & Anterior Eye xxx (2013) xxx– xxx 3
F panca ent aT
tolsxftwTitpwt
iaCh
3
l6tar
TBo
a
C
ig. 1. Differences in fluorescence pattern between non-pancorneal RGP-CL (A) andpex compared to (B), which shows a gradient in the zone of the BCR. In the alignmhe edge clearance of (B) is much smaller than (A). BCR, base curve radius.
To assess the location of the cone, defined as the thinnest loca-ion of the cornea, we included all eyes that underwent at leastne Pentacam scan. Parametric statistical tests were applied. Theocation of the cone was measured using a Cartesian coordinateystem in which the center of the cornea served as the origin (i.e.,
= 0 mm and y = 0 mm). In right eyes x-coordinates were positiveor the nasal part and for left eyes x-coordinates were negative forhe nasal part (and vice versa for the temporal part). To map rightith left eyes, we recalculated the x-coordinates of the left eyes.
he superior part of the cornea was reflected by positive and thenferior part by negative y-coordinates. An association of the loca-ion of the cone with age has been reported [27]. Therefore, weerformed a sub-analysis in which we tested this association. Ageas stratified into three categories: 20 or younger, 21–40, and older
han 40 years.A p-value of 0.05 or less was considered statistically signif-
cant. All statistical analyses were performed using statisticalnalysis software (SPSS version 15.0.0 for Windows; SPSS Inc.,hicago, IL; and R statistical package version 2.11.1 for Mac;ttp://www.r-project.org).
. Results
A total of 133 eyes with keratoconus were fitted with contactenses. Of these 82 underwent at least one Pentacam scan of which
Please cite this article in press as: Ramdas WD, Vervaet CJWC. Progressgas-permeable contact lenses. Contact Lens Anterior Eye (2013), http://dx.
6 underwent two or more Pentacam scans. Eyes that changed con-act lens type during follow-up (N = 24) were excluded, resulting in
total of 42 included eyes (of 25 patients) with a mean (median;ange) follow-up of 17.8 (15; 4–67) months.
able 1aseline characteristics of included eyes with keratoconus wearing non-pancorneal RGP-Ctherwise.
Without pancorneal RGP-CL (
Age start CL use (years) 33.8 ± 14.4
Gender, women (N [%]) 5 (45.5)
Eye, right (N [%]) 4 (36.4)
Age of onset of keratoconus (years) 30.3 ± 13.0
Best-corrected visual acuity 0.8 ± 0.1
Follow-up CL median (IQR) (months) 21.0 (6.0–31.0)
Spherical equivalent CL (D) −6.38 ± 1.50Base curve radius CL (mm) 7.23 ± 0.49
History of keratoconus treatment (N [%])a 3 (27.3)
Including: Doublet CL, EX1KS CL, Ferrara rings, Hybrid CL, Pancorneal CL, Soft CL, ScleraL, contact lens; IQR, interquartile range.
orneal RGP-CL (B). The fluorescein pattern in (A) shows more stress on the cornealrea, starting at 1.9 mm from the edge, there is no fluorescein (no-clearance area).
Table 1 shows the general characteristics between eyes with-out and with pancorneal RGP-CL. There were significant differencesbetween eyes fitted without and with pancorneal RGP-CL regardingthe age of onset of keratoconus (p = 0.044) and the spherical equiv-alent of the contact lens (p = 0.012).
Table 2 shows the differences in corneal topography betweeneyes without pancorneal RGP-CL and with pancorneal RGP-CLat baseline. Eyes without pancorneal RGP-CL had a slightly nar-rower anterior chamber angle compared with eyes with pancornealRGP-CL at baseline (mean ± standard deviation: 35.1◦ ± 5.2◦ vs.39.0◦ ± 5.6◦, respectively; p = 0.049; Table 2). During follow-up nochanges in anterior chamber parameters were found in eyes fittedwithout pancorneal RGP-CL. However, in eyes fitted with pan-corneal RGP-CL a significant decrease in anterior chamber volume(p < 0.001) and corneal volume (p = 0.008) was found, but no changein anterior chamber depth (p = 0.133) or anterior chamber angle(p = 0.537). Furthermore, in eyes fitted without pancorneal RGP-CL all assessed K-values (K-flat, K-steep, K-mean and K-minimum)were significantly lower at follow-up compared with baseline(p = 0.026, p = 0.013, p = 0.011 and p = 0.033, respectively), whereasno significant differences between baseline and follow-up werefound in eyes fitted with pancorneal RGP-CL (p = 0.480, p = 0.564,p = 0.545 and p = 0.861, respectively). Table 2 also presents therate of progression of keratoconus in terms of corneal topographyparameters. There was a significant difference in the decrease of theK-values. Eyes fitted with pancorneal RGP-CL showed less progres-
ion of keratoconus in patients wearing pancorneal toric edge rigiddoi.org/10.1016/j.clae.2013.11.012
sion than eyes fitted without pancorneal RGP-CL. Note that K-valuesare presented as radius in mm, which means that a decrease isequal to an increase in the curvature and dioptric power. Border-line significance (p = 0.06) was found for change in CKI (compares
L versus pancorneal RGP-CL, presented as mean ± standard deviation unless stated
N = 11) With pancorneal RGP-CL (N = 31) p-Value
26.4 ± 9.4 0.13113 (41.9) 1.00015 (48.4) 0.72621.6 ± 6.9 0.0440.9 ± 0.1 0.17211.0 (6.0–19.0) 0.092−4.14 ± 3.35 0.0127.31 ± 0.49 0.67210 (32.3) 1.000
l CL, Synergi (hybrid CL), Cross-linking; RGP-CL, rigid gas-permeable contact lens;
ARTICLE IN PRESSG Model
CLAE-681; No. of Pages 6
4 W.D. Ramdas, C.J.W.C. Vervaet / Contact Lens & Anterior Eye xxx (2013) xxx– xxx
Table 2Corneal topography: baseline and change after follow-up for eyes fitted without and with pancorneal RGP-CL, presented as mean ± standard deviation unless stated otherwise.
Baseline p-Value Change after follow-up p-Value
Withoutpancorneal RGP-CL(N = 11)
With pancornealRGP-CL (N = 31)
Withoutpancorneal RGP-CL(N = 11)
With pancornealRGP-CL (N = 31)
Pachymetry at apex (�m) 436 ± 68 470 ± 51 0.282 16.00 ± 64.54 −2.06 ± 13.96 0.735Pachymetry at pupil (�m) 452 ± 56 475 ± 49 0.429 12.36 ± 58.13 −1.16 ± 14.57 0.844Pachymetry minimal (�m) 421 ± 78 451 ± 50 0.498 4.82 ± 28.54 −1.00 ± 21.46 0.778
ISV 97 ± 55 77 ± 27 0.756 −2.55 ± 20.97 −1.77 ± 12.06 0.672IVA 1.05 ± 0.63 0.76 ± 0.30 0.308 −0.15 ± 0.30 −0.03 ± 0.21 0.269KI 1.29 ± 0.18 1.18 ± 0.12 0.104 −0.04 ± 0.08 −0.01 ± 0.06 0.163CKI 1.06 ± 0.06 1.05 ± 0.04 0.612 0.01 ± 0.02 0.00 ± 0.02 0.062IHA 28.4 ± 21.5 17.6 ± 12.3 0.163 9.22 ± 30.34 −3.08 ± 14.73 0.058IHD 0.10 ± 0.08 0.07 ± 0.04 0.155 −0.02 ± 0.07 −0.01 ± 0.02 0.822ABR 100 ± 0 100 ± 1 0.535 −1.09 ± 3.02 0.26 ± 1.18 0.322
Corneal volume (mm3) 54.6 ± 2.3 55.6 ± 6.3 0.222 0.51 ± 3.21 0.81 ± 1.51 0.445Inner 3 mm circle 3.3 ± 0.4 3.5 ± 0.3 0.336 0.08 ± 0.35 0.00 ± 0.12 0.888Inner 5 mm circle 9.8 ± 0.9 10.3 ± 1.0 0.295 0.21 ± 0.81 0.03 ± 0.28 0.978Inner 7 mm circle 21.8 ± 1.2 22.5 ± 2.3 0.163 0.15 ± 1.16 0.16 ± 0.55 0.535
AC depth (mm) 3.24 ± 0.65 3.27 ± 0.34 0.978 0.06 ± 0.32 −0.03 ± 0.11 0.412AC volume (mm3) 187 ± 36 194 ± 40 0.822 0.45 ± 20.82 −6.74 ± 9.54 0.735AC angle (◦) 35.1 ± 5.2 39.0 ± 5.6 0.049 −0.94 ± 3.41 −0.43 ± 4.03 0.823K-Flat (mm) 7.22 ± 0.75 7.49 ± 0.63 0.396 −0.11 ± 0.15 −0.02 ± 0.16 0.092K-Steep (mm) 6.81 ± 0.87 6.92 ± 0.50 0.714 −0.18 ± 0.22 −0.01 ± 0.15 0.020K-Mean (mm) 7.02 ± 0.80 7.21 ± 0.53 0.693 −0.15 ± 0.17 −0.01 ± 0.11 0.019K-Minimum (mm) 6.04 ± 0.93 6.42 ± 0.61 0.429 −0.17 ± 0.22 0.02 ± 0.25 0.041
R riancei rratio
cebc
tde(pal
Fip
GP-CL, rigid gas-permeable contact lens; CL, contact lens; ISV, index of surface vandex; IHA, index of height asymmetry; IHD, index of height decentration; ABR, abe
entral with peripheral cornea curvature) and IHA (height differ-nce between superior and inferior cornea) irregularity indicesetween eyes without pancorneal RGP-CL and eyes with pan-orneal RGP-CL.
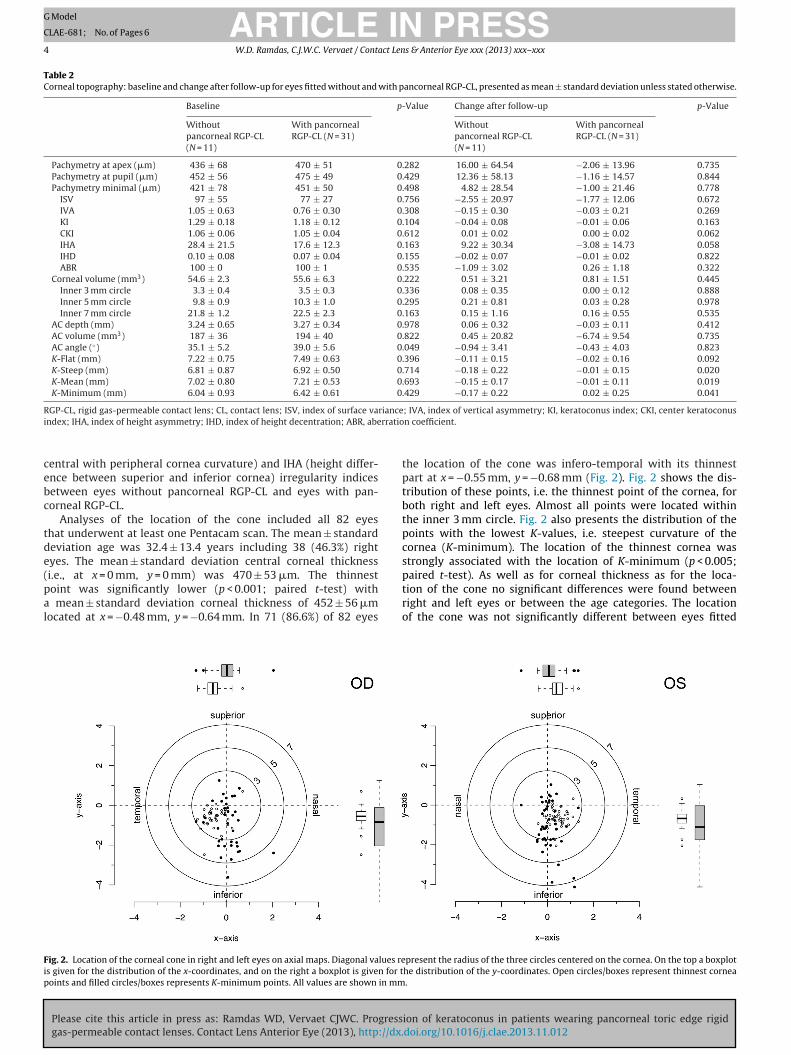
Analyses of the location of the cone included all 82 eyeshat underwent at least one Pentacam scan. The mean ± standardeviation age was 32.4 ± 13.4 years including 38 (46.3%) rightyes. The mean ± standard deviation central corneal thickness
Please cite this article in press as: Ramdas WD, Vervaet CJWC. Progressgas-permeable contact lenses. Contact Lens Anterior Eye (2013), http://dx.
i.e., at x = 0 mm, y = 0 mm) was 470 ± 53 �m. The thinnestoint was significantly lower (p < 0.001; paired t-test) with
mean ± standard deviation corneal thickness of 452 ± 56 �mocated at x = −0.48 mm, y = −0.64 mm. In 71 (86.6%) of 82 eyes
ig. 2. Location of the corneal cone in right and left eyes on axial maps. Diagonal values res given for the distribution of the x-coordinates, and on the right a boxplot is given for toints and filled circles/boxes represents K-minimum points. All values are shown in mm
; IVA, index of vertical asymmetry; KI, keratoconus index; CKI, center keratoconusn coefficient.
the location of the cone was infero-temporal with its thinnestpart at x = −0.55 mm, y = −0.68 mm (Fig. 2). Fig. 2 shows the dis-tribution of these points, i.e. the thinnest point of the cornea, forboth right and left eyes. Almost all points were located withinthe inner 3 mm circle. Fig. 2 also presents the distribution of thepoints with the lowest K-values, i.e. steepest curvature of thecornea (K-minimum). The location of the thinnest cornea wasstrongly associated with the location of K-minimum (p < 0.005;
ion of keratoconus in patients wearing pancorneal toric edge rigiddoi.org/10.1016/j.clae.2013.11.012
paired t-test). As well as for corneal thickness as for the loca-tion of the cone no significant differences were found betweenright and left eyes or between the age categories. The locationof the cone was not significantly different between eyes fitted
present the radius of the three circles centered on the cornea. On the top a boxplothe distribution of the y-coordinates. Open circles/boxes represent thinnest cornea.

ING Model
C
ct Len
wC
4
oRemcw
twsctrftmrohtsr(iNblbttl
wpmtis(
aascip[sfaRtw
wecpb
[
ARTICLELAE-681; No. of Pages 6
W.D. Ramdas, C.J.W.C. Vervaet / Conta
ithout pancorneal RGP-CL and eyes fitted with pancorneal RGP-L.
. Discussion
We found evidence that pancorneal RGP-CL had a better effectn stabilizing keratoconus than eyes fitted without pancornealGP-CL. We did not find any alteration in anterior chamber param-ters during follow-up. The thinnest part of the cornea was in theajority of eyes located infero-temporally of the cornea within the
entral 3-mm circle. As expected, the point of the thinnest corneaas strongly associated with the point with the steepest curvature.
Our findings of the location of the cone are in line withhose reported previously [27–29]. The corneal thickness in casesith keratoconus wearing contact lenses has been shown to be
ignificantly thinner in the infero-temporal area of the corneaompared with controls wearing contact lenses [30]. The infero-emporal position of the cone might be the consequence of eyeubbing habits, a risk factor for keratoconus [31]. We found no dif-erence between the age categories and the location of the cone,hough a temporal global cone pattern has been reported to occur
ore often in younger patients (<21 years of age) [27]. In the cur-ent study the location of the cone was defined as the thinnest pointf the cornea rather than the point with the steepest curvature. Inealthy eyes the former point is generally located at the center ofhe cornea. The position of the latter point, i.e. the point with theteepest curvature, has been reported to be more often at the infe-ior part of the cornea [31]. This is in agreement with our findingsFig. 2). One may comment that the location of the cone as definedn the current study may differ from the “true” location of the cone.onetheless, a poor correlation between thickness- and curvature-ased maps of the cornea has been described in determining the
ocation of the cone [29]. The thinnest point of the cornea may note equal to the steepest curvature, for example, the steep slope ofhe cone is not always located on the same side (Fig. 2). Therefore,hickness-based maps might give a more precise estimate of theocation of the cone of the cornea [29].
One study evaluated the effect of “normal” RGP-CL in patientsith contact lenses and compared the corneal topography withatients without contact lenses with a follow-up of around 20onths [32]. They showed that RGP-CL wear did not contribute
o the progression of keratoconus, which is in line with our find-ngs. However, the RGP-CL used in their study is not exactly theame as the pancorneal RGP-CL investigated in the current studysee Section 2).
Regarding the anterior chamber parameters, one study reported significant decrease in corneal volume and the anterior chamberngle, and an increase in anterior chamber depth in eyes with moreevere keratoconus [23]. Another study also reported a decrease inorneal volume in patients with keratoconus [33]. The decreasen corneal volume is in line with our findings in eyes fitted withancorneal RGP-CL and might be due to loss of corneal tissue33]. Nevertheless, in contrast to their findings we did not find aignificant difference in anterior chamber depth or angle duringollow-up. This may be explained by the relatively short follow-upnd small sample size (especially for eyes fitted without pancornealGP-CL) of the current study; however, follow-up was long enougho detect a significant progression of keratoconus in eyes fittedithout pancorneal RGP-CL.
One of the limitations of the current study is that patientsho changed type of contact lens during the study (N = 24) were
Please cite this article in press as: Ramdas WD, Vervaet CJWC. Progressgas-permeable contact lenses. Contact Lens Anterior Eye (2013), http://dx.
xcluded. This might have resulted in a selection bias, in that physi-ians are more likely to change the type of contact lens in eyes withrogressive keratoconus and as a consequence these eyes may haveeen excluded from the current study. Nonetheless, of the assessed
[
PRESSs & Anterior Eye xxx (2013) xxx– xxx 5
corneal topography variables only corneal volume showed a statis-tically significant difference at baseline between the excluded andincluded eyes. Therefore, it is not likely that this limitation wouldhave hampered the current results.
The ability to fit contact lenses in severe keratoconus may bethe result of a combination of corneal steepness/astigmatism andcorneal irregularity. Although eyes fitted without pancorneal RGP-CL were more myopic than eyes fitted with pancorneal RGP-CL,it is not obvious that the former group consisted of more severekeratoconus. When measured with corneal topography, cornealastigmatism increases strongly with disease severity indicatingthat patients with more severe keratoconus have not only steepercorneas but also higher corneal cylindrical errors. In the presentstudy eyes fitted with pancorneal RGP-CL had slightly higher refrac-tive errors. This suggests that the effect of the spherical power issmaller than the effect of the astigmatism. Moreover, there were nodifferences in K-values or irregularity values between eyes fittedwithout and with pancorneal RGP-CL.
Another limitation could be that five eyes underwent surgicaltreatment for keratoconus prior to inclusion in the current study.Of these, one was treated with Ferrara rings and subsequently fittedwith a non-pancorneal RGP-CL. The remaining four eyes were fittedwith a pancorneal RGP-CL, of which three underwent cross-linkingand one was treated with Ferrara rings. Excluding these five eyesdid not alter the presented results significantly.
In conclusion, compared with “normal” contact lenses pan-corneal RGP-CL may be a better treatment option in eyes with earlykeratoconus. Studies with longer follow-up are needed to assess thelong-term results of these contact lenses. The location of the conemay be clinically important for comfortable contact lens fitting, forbetter designs of contact lenses to reduce pressure of the contactlens on the cone, and for surgical management.
Financial support
None.
Conflict of interest
None.
References
[1] Chopra I, Jain AK. Between eye asymmetry in keratoconus in an Indian popula-tion. Clinical & Experimental Optometry: Journal of the Australian OptometricalAssociation 2005;88:146–52.
[2] Kennedy RH, Bourne WM, Dyer JA. A 48-year clinical and epidemio-logic study of keratoconus. American Journal of Ophthalmology 1986;101:267–73.
[3] Rabinowitz YS. Keratoconus. Survey of Ophthalmology 1998;42:297–319.[4] Nottingham J. Practical observations on conical cornea, and on the short
sight, and other defects of vision connected with it. London: J. Churchill;1854.
[5] Romero-Jimenez M, Santodomingo-Rubido J, Wolffsohn JS. Keratoconus: areview. Contact Lens & Anterior Eye: Journal of the British Contact Lens Asso-ciation 2010;33:157–66 [quiz 205].
[6] Sugar J, Macsai MS. What causes keratoconus. Cornea 2012;31:716–9.[7] Hallermann W, Wilson EJ. Genetic aspects of keratoconus (author’s transl).
Klinische Monatsblatter fur Augenheilkunde 1977;170:906–8.[8] Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory
corneal thinning disorders. Survey of Ophthalmology 1984;28:293–322.[9] Lu Y, Vitart V, Burdon KP, Khor CC, Bykhovskaya Y, Mirshahi A, et al. Genome-
wide association analyses identify multiple loci associated with central cornealthickness and keratoconus. Nature Genetics 2013;45:155–63.
10] Gasset AR, Houde WL, Garcia-Bengochea M. Hard contact lens wear asan environmental risk in keratoconus. American Journal of Ophthalmology
ion of keratoconus in patients wearing pancorneal toric edge rigiddoi.org/10.1016/j.clae.2013.11.012
1978;85:339–41.11] Cesnekova T, Skorkovska K, Petrova S, Cermakova S. Visual functions and
quality of life in patients with keratoconus. Ceska a slovenska oftalmologie:casopis Ceske oftalmologicke spolecnosti a Slovenske oftalmologicke spolec-nosti 2011;67:51–4.
ING Model
C
6 act Len
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLELAE-681; No. of Pages 6
W.D. Ramdas, C.J.W.C. Vervaet / Cont
12] Kymes SM, Walline JJ, Zadnik K, Gordon MO. Quality of life in keratoconus.American Journal of Ophthalmology 2004;138:527–35.
13] Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagencrosslinking for the treatment of keratoconus. American Journal of Ophthal-mology 2003;135:620–7.
14] Modis Jr L, Szalai E, Facsko A, Fodor M, Komar T, Berta A. Corneal trans-plantation in Hungary (1946–2009). Clinical & Experimental Ophthalmology2011;39:520–5.
15] Rebenitsch RL, Kymes SM, Walline JJ, Gordon MO. The lifetime economic burdenof keratoconus: a decision analysis using a Markov model. American Journal ofOphthalmology 2011;151:768–73, e2.
16] Keenan TD, Jones MN, Rushton S, Carley FM. Trends in the indications forcorneal graft surgery in the United Kingdom: 1999 through 2009. Archives ofOphthalmology 2012;130:621–8.
17] Smiddy WE, Hamburg TR, Kracher GP, Stark WJ. Keratoconus. Contact lens orkeratoplasty. Ophthalmology 1988;95:487–92.
18] Fick AE. A contact-lens. 1888 (translation). Archives of Ophthalmology1988;106:1373–7.
19] Wei RH, Khor WB, Lim L, Tan DT. Contact lens characteristics and con-trast sensitivity of patients with keratoconus. Eye & Contact Lens 2011;37:307–11.
20] Kamar S, Vervaet C, Luyten GP, Jager MJ. Pancorneal contact lens with a toricedge: a new concept in keratoconus. European Journal of Ophthalmology2011;21:685–90.
21] Ramdas WD, Vervaet CJ, Bleyen I. Corneal topography for pancorneal toricedge rigid gas-permeable contact lens fitting in patients with keratoconus,and differences in age and gender. Contact Lens & Anterior Eye: The Jour-
Please cite this article in press as: Ramdas WD, Vervaet CJWC. Progressgas-permeable contact lenses. Contact Lens Anterior Eye (2013), http://dx.
nal of the British Contact Lens Association 2013, http://dx.doi.org/10.1016/j.clae.2013.07.005.
22] Sorbara L, Dalton K. The use of video-keratoscopy in predicting contact lensparameters for keratoconic fitting. Contact Lens & Anterior Eye: Journal of theBritish Contact Lens Association 2010;33:112–8.
[
[
PRESSs & Anterior Eye xxx (2013) xxx– xxx
23] Emre S, Doganay S, Yologlu S. Evaluation of anterior segment parameters inkeratoconic eyes measured with the Pentacam system. Journal of Cataract andRefractive Surgery 2007;33:1708–12.
24] Barkana Y, Gerber Y, Elbaz U, Schwartz S, Ken-Dror G, Avni I, et al. Cen-tral corneal thickness measurement with the Pentacam Scheimpflug system,optical low-coherence reflectometry pachymeter, and ultrasound pachymetry.Journal of Cataract and Refractive Surgery 2005;31:1729–35.
25] Leung KK. RGP fitting philosophies for keratoconus. Clinical & Experimen-tal Optometry: Journal of the Australian Optometrical Association 1999;82:230–5.
26] Barnett M, Mannis MJ. Contact lenses in the management of keratoconus.Cornea 2011;30:1510–6.
27] Ertan A, Kamburoglu G, Colin J. Location of steepest corneal area of cone inkeratoconus stratified by age using Pentacam. Journal of Refractive Surgery2009;25:1012–6.
28] Colin J, Sale Y, Malet F, Cochener B. Inferior steepening is associatedwith thinning of the inferotemporal cornea. Journal of Refractive Surgery1996;12:697–9.
29] Demirbas NH, Pflugfelder SC. Topographic pattern and apex location of kerato-conus on elevation topography maps. Cornea 1998;17:476–84.
30] Pflugfelder SC, Liu Z, Feuer W, Verm A. Corneal thickness indices discriminatebetween keratoconus and contact lens-induced corneal thinning. Ophthalmol-ogy 2002;109:2336–41.
31] Kim H, Joo CK. Measure of keratoconus progression using Orbscan II. Journal ofRefractive Surgery 2008;24:600–5.
32] Hwang JS, Lee JH, Wee WR, Kim MK. Effects of multicurve RGP contact lensuse on topographic changes in keratoconus. Korean Journal of Ophthalmology
ion of keratoconus in patients wearing pancorneal toric edge rigiddoi.org/10.1016/j.clae.2013.11.012
2010;24:201–6.33] Mannion LS, Tromans C, O’Donnell C. Reduction in corneal volume with severity
of keratoconus. Current Eye Research 2011;36:522–7.34] Koller T, Iseli HP, Hafezi F, Vinciguerra P, Seiler T. Scheimpflug imaging of
corneas after collagen cross-linking. Cornea 2009;28(June 5):510–5.