prognostic factors in papillary carcinoma of the thyroid
TRANSCRIPT

Prognostic Factors in Papillary Carcinoma of the Thyroid Anne-Marie Schindler, MD,* Guy van Melle, PhD,t Beatrice Evequoz, MD,$ and Bianca Scazziga, MD$
In a retrospective study of 119 patients, followed for 1 to 30 years after treatment of a papillary carcinoma of the thyroid, the authors searched for possible prognostic factors of the risk of recurrence. Microcarcinomas, anaplastic tumors and Hiirthle cell carcinomas were excluded from the study. In a univariate analysis, age (> 45 years), sex (male), loss of histologic differentiation, size (> 3 cm), presence of carcinomatous lymphangitis, extrathyroid extension, and presence of metastasis at diagnosis were associated with a higher recurrence rate; type of growth and multifocality were not significant. In a multivariate analysis (logistic regression), age, size, and carcinomatous lymphangitis were significant predictors for women, whereas metastasis at diagnosis and cystic growth were significant for men. Cancer 68:324-330,1991.
APILLARY CARCINOMA Of the thyroid was “unsur- P passed as a clinical subject of debate” for Frazell and Foot in 1958.’ Since then, the papillary form has been defined and clearly separated from its follicular counterpart; their respective characteristics have been laid down by the World Health Organization.2 Since then, also, numerous clinical and pathologic investigators have looked at the biology of this relatively slow growing but sometimes unpredictable tumor and have tried to deter- mine the elements of prognostic significance. The majority of these studies are based on a univariate a n a l y ~ i s . ~ - ~ ~
During the last decade, multivariate analysis has been intr~duced.~’-~’ Factors such as sex, age, size, extension, and presence of metastasis at diagnosis are generally men- tioned, but no complete agreement has yet been reached as to their significance. In 1982 Tscholl-Ducommun and Hedinger (TDH) proposed a histologic clas~ification~~ in which the degree of differentiation correlated well with clinical behavior. This classification represents a gradual
From the *Institut Universitaire de Pathologie, the tInstitut Univer- sitaire de MCdecine Sociale et PrCventive, Division Statistique, and the SDCpartement de MCdecine Interne. Division d’Endocrinologie, Centre Hospitalier Universitaire Vaudois, UniversitC de Lausanne, Lausanne, Switzerland.
The authors thank Professors C. Hedinger and J. Costa for their valu- able advice, Mrs. E. Haller for preparing the graphs, and Mrs. A. Lauper for typing the manuscript.
Address for reprints: Anne-Mane Schindler, MD, Institute of Pathol- ogy, Bugnon 25, Lausanne. 10 1 1, Switzerland.
Accepted for publication December 1. 1990.
loss of differentiation from class I to class 111. Their find- ings have not yet been confirmed by others.
In the current study, a multivariate analysis was applied to data obtained from a primarily morphologic approach of the papillary carcinoma of the thyroid. The I 19 patients studied constitute a particularly homogeneous group, fol- lowed up to 30 years by the same clinician (B.S.) and whose surgical specimens were practically all analyzed at the same institution and reviewed by the same pathologist (A.M.S.). Only the usual type of papillary carcinoma of the thyroid was considered, excluding microcarcinomas (< 1 cm), anaplastic carcinomas with a papillary com- ponent as well as papillary tumors of Hurthle cell type. The indolent course of microcarcinomas and the very ag- gressive behavior of anaplastic tumors being well estab- lished, both types are outside the scope of this study; the oncocytic or Hiirthle cell type has yet to be studied on a large enough scale to identify it either as a separate entity or as a simple variant of the usual form.
Materials and Methods
The population studied was chosen from a clinical contingency of patients operated upon for carcinoma of the thyroid with a final histologic diagnosis of papillary or folliculopapillary carcinoma. Patients with a clinical follow-up of at least 1 year were eligible for the study; microcarcinomas (< 1 cm), undifferentiated carcinomas and oncocytic papillary tumors were excluded. The longest follow-up was 30 years; the mean was 8.3 years. At the
324

No. 2 PAPILLARY CARCINOMA OF THE THYROID - Schindler et al. 325
end of the study, four patient categories were defined: (1) living free of tumor since the operation; (2) living free of tumor after a recurrence; (3) living with tumor; and (4) having died of papillary carcinoma.
Of the four patients who died of other causes during the study none had presented a recurrence; they were considered free of tumor, which was confirmed at autopsy in two of four cases.
All pathology specimens were reviewed and a ques- tionnaire (shown in Table I ) of 60 items of possible clinical and morphologic importance was completed for each pa- tient. Size and type of tumor growth were determined in the light of the original macroscopic description. Histo- logic determination was based on nine cytologic and nine morphologic criteria, whereas type and degree of invasion were established using seven criteria; these are enumerated in Table 1. Extrathyroid extension was determined on macroscopic evaluation by the surgeon and/or on micro-
TABLE 1. Questionnaire
Case identification Macroscopic findings
Type of growth
Size
Cytologic features Histologic findings
Architecture
Grading
Invasiveness
Metastases
Associated thyroid disease
Treatment Surgical
Medical
FOIIOW-UP Recurrences
Endpoint
ID no., sex, age
Cystic, solid with expansile margin,
< 2, < 3, < 4, < 6, > 6 cm
Nucleus
stellate scar
Ground glass, grooved, overlap, irregular outlines, atypia, hyperchromasia, mitosis
Cytoplasm Clear versus dense Papillary versus follicular
predominence, colloid, psammoma bodies or calcifications, interstitial sclerosis, loss of stroma, lymphoid infiltrate, focal solid versus diffuse solid cell sheets
Classification according to Tscholl- Ducommun and Hedir~ger~~
Tumor capsule, adjacent thyroid, intrathyroidal and/or perithyroidal lymphangitis, satelite nodules or multifocality, bilateral disease, extrathyroidal extension, vascular invasion
Local lymph node: one, two or more distant; diagnosis on metastasis
Goiter, adenoma, hyperplasia, chronic thyroiditis
Tumoriectomy, lobectomy, subtotal thyroidectomy, total thyroidectom y
None, TSH suppression, radioactive iodine. external radiation
Local thyroidal, cervical lymph nodes,
Cured, living with disease (recurred), distant
dead of disease
TSH: thyroid stimulating hormone.
TABLE 2. Clinical Evolution of the Study Group
No. Age (yr) Sex
92 F/27 M Total 119 45.0 19 F/18 M Cured 91 43.5 13 F/9 M Recurrences 22 50.3
Cured 5 38.8 4F/1 M Persistent disease 8 41.9 4 F/4 M Dead 9 58.8 5 F/4 M
scopic evidence. Presence or absence of lymph node me- tastasis was ascertained; associated benign thyroid disease was noticed. Each case was classified according to TDH.
Briefly, well-differentiated carcinomas (class I) show well-developed fine papillae with a delicate vascular axis, the nuclei being of the “ground glass” type, with cyto- plasmic pseudoinclusions, partially arranged like tiles on a roof. Stellate scars, lymphoplasmocytic inflammatory reaction, and cyst formation are frequent findings. Ab- sence of “ground glass” nuclei forms the subclass Ib, purely follicular architecture the subclass Ic. Loss of his- tologic uniformity, presence of solid cell sheets and nuclear polymorphism constitutes the moderately differentiated carcinomas, subdivided into subclass IIa if stellate scars, inflammatory reaction or cystic change are present, and into IIb if these elements are altogether absent. Poorly differentiated carcinomas (class 111) show a majority of microfollicular areas, devoid of colloid; they resemble the so-called “proliferating Langhans’ goiter” but contain clearly differentiated papillary structures. They lack the conspicuous giant and spindle-cell growth of undifferen- tiated carcinomas, as well as mitoses, necrosis, and mas- sive vascular invasion.
For statistical evaluation, a logistic regression analysis was used; factors which are significantly associated with the biologic behavior of this tumor as assessed by tumor recurrence, were sought for and their respective impor- tance evaluated. In addition, the time to recurrence was described using a Kaplan-Meier survival analysis.
Results
The general profile and clinical outcome of the popu- lation studied is shown in Table 2. Of a total of 119 pa- tients studied, 92 were women, giving a 3.4 female/male ratio. The mean age of 45.0 years is similar for both sexes (44.5 years for women, 45.6 years for men), the median being 42 years.
All I19 patients underwent surgical treatment intended to be curative; types of operations included lobectomy, and subtotal and total thyroidectomy, with or without adenectomy. Ninety-seven patients (8 1.5%) were free of tumor at the end of the study, but 30 of them (30.9%) were followed for less than 5 years. The group of patients

326 CANCER July 15 199 1 Vol. 68
TABLE 3. Details on Patients With Recurrences
Localization and time of Gross recurrence (years after diagnosis)
Age extrathyroid Years of Final outcome Sex (vr) extension observation T LN D TDH class
~ ~ ~ ~ ~ ~ ~ ~ ~
Curred F 18 - 16 7 8 Ia F 55 14 7 IIa F 10 - 16 3 IIa F 64 - 10 5 I11 M 47 - 2 I 111
-
Living with F 80 - 4 2 3 IIa disease F 22 - 30 30 IIa
F 66 Yes 7 7 Ila F 60 - 15 14 111 M 42 - 1 1 Ia M 22 - 4 2 3 IIa M 26 - 18 4; 5 9; 13; 16 IIa M 65 Yes 2 I 111
Died of disease F 63 - 6 6 la F 45 - I5 1 10 Ila F 45 - 6 6 4; 5 IIa F 15 Yes 7 7 IIb F 63 Yes 3 2 3 111 M 70 1 1 IIa M 44 - 18 II 1 1 IIa M 57 Yes 2 2 I11 M 67 Yes 4 4 111
-
T: thyroid bed; LN: lymph nodes, regional; D: distant metasteses; TDH: Tscholl-Ducomrnun and Hedinger.”
with recurrence had a mean age of 50.3 years, compared with 43.5 years for those without. This higher mean age is found in patients whose recurrence was not cured (mean age, 47.9 years) or had led to death (mean age, 58.8 years), whereas patients whose recurrence was cured had a mean age of 38.8 years. For those older patients the sex ratio is near 1.
Details on patients with recurrence are listed in Table 3. Excepting one patient (second female patient living with disease), whose recurrence after 30 years is more evocative of a new disease than of actual recurrence, it is seen that the interval between primary operation and first recurrence varied from 1 to 14 years, the mean being 4.5 years. Twenty-one of the 22 patients with recurrence(s) were reoperated and/or treated with radioactive iodine, the aim being once more curative. Five ofthem have been considered free of tumor at the end of the study, eight
TABLE 4. Recurrence Rate and Age According to the Tscholl-Ducommun and Hedinger Classification
Males Females Recurrence Mean age TDH class (rec/no.) (rec/no.) Total no. rate (’70) (YO
la I 14 2/24 28 10.7 41.6 Jc 0 O / I I I 1 0 30. I
IIa 4/11 6/36 47 21.3 42.9 Ilb 01 1 218 9 22.2 42.2
I I I 4/11 3/13 24 29.2 59.4
rec: recurrence; TDH: Tscholl-Ducommun and Hedinger?8
others were found living with tumor and nine had died of the carcinoma. Table 3 also shows sites and multiplicity of the recurrences as well as the longevity of some patients with multiple recurrences, one patient having lived with recurrences for 16 years. In addition, Table 3 reveals the possibility of curing metastatic disease, even when present at distant sites. Gross extrathyroid extension was found in only six patients with recurrence, although it was pres- ent in 13 others who did not recur.
Table 4 shows the recurrence rate for each one of the TDH classes. The subgroup Ic, which corresponds to the purely follicular type of papillary carcinoma, contains only women and shows not a single case of recurrence. This group also has the lowest mean age (30.8 years). The tran- sition from well (class Ia) to moderately differentiated carcinomas (classes IIa and IIb) results in the doubling of the recurrence rate, whereas mean ages are comparable. Between class I1 and class 111 the increase in risk is not so marked (from 22% to 29%); however, the mean age rises from 42 to 59 years.
The results of a univariate analysis of all the variables of interest in the questionnaire are presented in Table 5. Their effect on the recurrence rate is expressed as relative risk and their univariate significance is shown. It is seen that the rate for those younger than 45 years is 13.6%, and older than that age, 24.5%. Men show recurrences more than twice as frequently as women. The loss of dif- ferentiation triples the recurrence rate. Cystic growth, a relatively rare occurrence in the current series (1 2.774,
327 No. 2 PAPILLARY CARCINOMA OF THE THYROID Schindler et al.
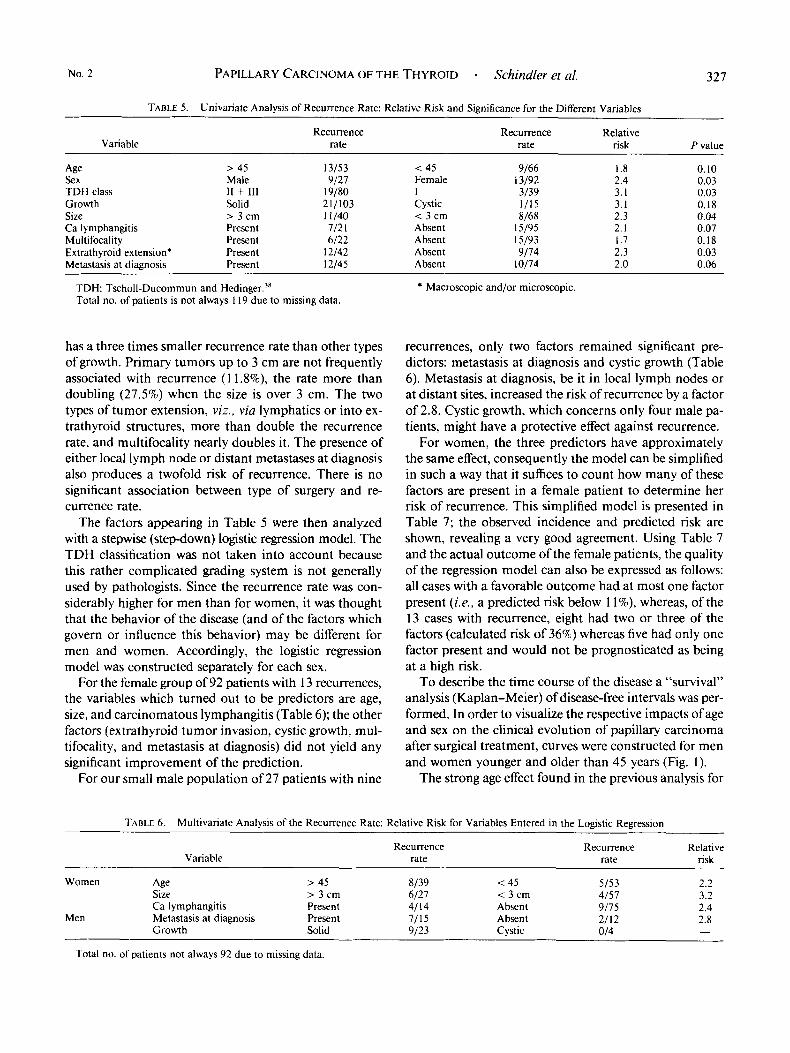
TABLE 5. Univanate Analysis of Recurrence Rate: Relative Risk and Significance for the Different Variables
Recurrence Recurrence Relative Variable rate rate risk P value
Age > 45 13/53 < 45 9/66 I .8 0.10 Sex Male 9/27 Female 13/92 2.4 0.03 TDH class I1 + 111 19/80 I 3/39 3. I 0.03 Growth Solid 211103 Cystic 1/15 3.1 0.18 Size > 3 cm 1 1/40 < 3 cm 8/68 2.3 0.04 Ca lymphangitis Present 712 1 Absent 15/95 2. I 0.07 Multifocality Present 6/22 Absent 15/93 I .7 0.18 Extrathyroid extension* Present 12/42 Absent 9/74 2.3 0.03 Metastasis at diagnosis Present 12/45 Absent 10174 2.0 0.06
TDH: Tscholl-Ducommun and Hedi~~ger .~’ Total no. of patients is not always 1 I9 due to missing data.
has a three times smaller recurrence rate than other types of growth. Primary tumors up to 3 cm are not frequently associated with recurrence ( 1 1.8%), the rate more than doubling (27.5%) when the size is over 3 cm. The two types of tumor extension, viz., via lymphatics or into ex- trathyroid structures, more than double the recurrence rate, and multifocality nearly doubles it. The presence of either local lymph node or distant metastases at diagnosis also produces a twofold risk of recurrence. There is no significant association between type of surgery and re- currence rate.
The factors appearing in Table 5 were then analyzed with a stepwise (step-down) logistic regression model. The TDH classification was not taken into account because this rather complicated grading system is not generally used by pathologists. Since the recurrence rate was con- siderably higher for men than for women, it was thought that the behavior of the disease (and of the factors which govern or influence this behavior) may be different for men and women. Accordingly, the logistic regression model was constructed separately for each sex.
For the female group of 92 patients with I3 recurrences, the variables which turned out to be predictors are age, size, and carcinomatous lymphangitis (Table 6); the other factors (extrathyrojd tumor invasjon, cystic growth, mul- tifocality, and metastasis at diagnosis) did not yield any significant improvement of the prediction.
For our small male population of 27 patients with nine
* Macroscopic and/or microscopic.
recurrences, only two factors remained significant pre- dictors: metastasis at diagnosis and cystic growth (Table 6). Metastasis at diagnosis, be it in local lymph nodes or at distant sites, increased the risk of recurrence by a factor of 2.8. Cystic growth, which concerns only four male pa- tients, might have a protective effect against recurrence.
For women, the three predictors have approximately the same effect, consequently the model can be simplified in such a way that it suffices to count how many of these factors are present in a female patient to determine her risk of recurrence. This simplified model is presented in Table 7; the observed incidence and predicted risk are shown, revealing a very good agreement. Using Table 7 and the actual outcome of the female patients, the quality of the regression model can also be expressed as follows: all cases with a favorable outcome had at most one factor present (i.e., a predicted risk below I I%), whereas, of the 13 cases with recurrence, eight had two or three of the factors (calculated risk of 36%) whereas five had only one factor present and would not be prognosticated as being at a high risk.
To describe the time course of the disease a “survival” analysis (Kaplan-Meier) of disease-free intervals was per- formed. In order to visualize the respective impacts of age and sex on the clinical evolution of papillary carcinoma after surgical treatment, curves were constructed for men and women younger and older than 45 years (Fig. 1).
The strong age effect found in the previous analysis for
TABLE 6 . Multivariate Analysis of the Recurrence Rate: Relative Risk for Variables Entered in the Logistic Regression
Recurrence Recurrence Relative Variable rate rate risk
Women Age > 45 8/39 < 45 5/53 2.2 Size > 3 c m 6/27 < 3 cm 4/57 3.2 Ca lymphangitis Present 4/14 Absent 9/75 2.4
Men Metastasis at diagnosis Present 1/15 Absent 2/12 2.8 - Growth Solid 9/23 Cystic 014
Total no. of patients not always 92 due to missing data.

328
50 - 40-
30 - 20 - 10 - 0
CANCER July 15 1991 Vol. 68
................
0 7 r . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 15 20 25 30 10
TABLE 7. Simplified Model of the Recurrence Rate for Women Based on Three Factors: Age > 45 Years,
Size > 3 cm, and Carcinomatous Lymphangitis
No. of factors present Observed risk Percent Calculated risk ('70)
0 2/34 5.9 2.3 1 4/34 11.8 10.4
2 or 3 712 I 33.3 36.2
the female patients is clearly visible: at 10 years of obser- vation the cumulative proportion of disease-free women is about 97% for those aged 45 years or younger and 66% for those. older than 45 years; after 20 years the proportions are, respectively, 70% and 50%. Similarly, the absence of age effect for men may be noticed; however, the figure suggests that this lack of age effect may be due to the fact that old men were not followed beyond 7 years.
The difference between sexes is quite marked and it appears that disease-free intervals of young men are nearly superposable to those of older women.
Discussion
Our overall recurrence rate of 19.7% is high compared with the 6.6% of the Mayo Clinic series, as calculated by Vickery et or to the 1 1 % of the Lahey Clinic," but is comparable with the 18.7% in the M. D. Anderson Hospital" and the 18% in Villejuif." Our recurrence rate is high in spite of a short follow-up period for nearly one third of this series. The difference between series is due, in part, to different types of patients: specialized oncology centers tend to see more advanced disease and few mi- crocarcinomas, the proportion of which is frequently not stated. If we had included all microcarcinomas from this series, the recurrence rate would have dropped to 13.9%.
The mean duration of our follow-up (8.3 years) is com- parable with many studies, but cannot compete with the 18.3 years of the Mayo C l i n i ~ . ~ ~ , ~ '
Our cumulated proportions of patients free of disease is comparable with those of the series by Carcangiu et al. from Italyz3 with 81.2% for women and 64.7% for men, at 10 years of observation. With only nine deaths in our series, no statistical evaluation of survival rate and its de- terminants was performed, recurrence being considered the endpoint for our study. Authors who compared factors associated with recurrence and those related to death10.23xz6.3z did not find significant differences.
In our study the 22 patients with recurrences had a mean age of 50.3 years; those without recurrence, 43.5 years. In the current series, the mean age at diagnosis was 38.8 years for the group which was cured after treatment of their recurrence, compared with 47.9 years for those living with disease and 58.8 for those. having died oftumor, confirming the findings of other authors that the curability
of a recurrence is dependent on the age at diagno-
Univariate analysis shows the age effect in virtually all series, be it in thyroid carcinomas in general or in the differentiated forms. No consensus has been reached as to the time of changeover from a slow growing to a more aggressive type of tumor. It seems to be somewhere be- tween the ages of 40 and 50 years. In the current series, the risk of recurrence for women remained about the same for both age limits and showed a threefold recurrence rate at higher ages. For men, the risk of recurrence was 1.7 times higher when the age limit was set at 40 years, but lost all age effect when set at 50 years, which is likdy due to small numbers in this group.
With a recurrence rate of 33.3% in men compared with 14.1 % in women, a strong sex effect is demonstrated in the current series, which is in concordance with most studies, with few exceptions7~12~16~28~30~31 where men fared no worse than women.
The value of the degree of differentiation in papillary carcinoma in relation to tumor aggressiveness is a con- troversial point. In the second edition of the World Health Organization on thyroid tumors ( 1 988),2 histologic dif- ferentiation in papillary carcinoma is denied any proven influence on clinical behavior. We tried to apply the TDH classification to our material. The current series confirms the influence of differentiation on clinical evolution, the well-differentiated form exhibiting the best prognosis. In group I11 it is difficult to separate the effect of poor dif- ferentiation from that of advanced age. The bulk of the population belongs to the moderately differentiated class. In the Mayo Clinic series,25 the authors have pooled both well-differentiated and moderately differentiated cases into grade I. However, since the recurrence risk doubles with the passage from well to moderate differentiation we think
sis. 10,23,26.32
W u) iz b E P
L
v, 0
W W
p H
80
............................ 511..111111._
YEARS
FIG. I . Disease-free interval curves grouped by age and sex. -: Men 145 years of age; - - - -: men >45 years of age; - - - -: women 545 years of age; - * * . : women >45 years of age.

No. 2 PAPILLARY CARCINOMA OF THE THYROID - Schindler et a[. 329
it preferable to keep the TDH classification of well-dif- ferentiated, moderately, and poorly differentiated carci- nomas and clearly separate the latter from anaplastic car- cinomas with papillary foci. We would, however, abolish the subgroups proposed by TDH, with the exception of the purely follicular type of papillary carcinomas, a par- ticularly favorable subgroup of the well-differentiated ones.
Cystic growth, present in 15 cases (12.6%), turned out to be associated with a favorable clinical outcome. Mac- roscopically, cystic papillary tumors have been called ad- enomas in the original fascicle of the Armed Forces In- stitute of Pathology on thyroid tumors,3y reflecting its rel- atively benign behavior. Carcangiu et al.23 find marked cystic changes in 9.1% oftheir cases and find a statistically significant clinical benefit associated with it. It is possible that tumors with cystic growth are comparable with those with total encapsulation, the particularly favorable prog- nosis of which has been pointed out by Vickery4' and Schroder rt d4' Our study being retrospective, we could not determine the totally encapsulated cases with any de- gree of certainty. Both types of tumors may have a better prognosis for analogous reasons: both are delimited by a capsule and have a low potential of invading and dis- rupting it. In the current series, the group of follicular type papillary tumors (TDH class Ic) stands equally out for its benign behavior, none of the 11 cases having re- curred. This tumor, too, is frequently encapsulated-six of 1 1 cases in the current series-and might derive its good prognosis from the same source.
Approximately two thirds of our patients had tumors measuring 3 cm or less. For them, the rate of a recurrence was 1 1.8% whereas it rose to 27.5% for those with tumors larger than 3 cm.
Ontai and Straehle~,*~ in their study in Hawaii, also found the 3 cm limit to be significant. In the analyses of Frauenhoffer et and Simpson et al.35 the delimitating size was found to be 4 cm, whereas all other studies in- cluding size as a prognostic factor allow only the so-called occult type (up to 1.5 cm) into the prognostically favorable group. 1') 2 v ' l The differences might be explained by a varying proportion of microcarcinomas in these series. Only when they are few in number ( 1 170 in the series of Simpson and associate^^^) can the impact of size above 1.5 cm be evaluated, which constitutes one ofthe reasons, for which we eliminated them altogether.
Carcinomatous lymphangitis was present in 22.1 % of our cases and implied seven of our 22 patients with re- currence, thus yielding a relative risk of recurrence of 2.1. This type of local invasion did not favor recurrences in the thyroid bed, the seven recurrences being equally dis- tributed at local and distant sites.
The effect of multifocality, a factor probably closely related to carcinomatous lymphangitis, was not significant
in our series. In the series of Cady et al. l o as well as Car- cangiu et multifocality was of prognostic value in increasing the risk of recurrence and the mortality rate.
Extrathyroid extension, which is frequently found as a
increased the risk of recurrence by a factor of 2.3 in our series, but lost its influence when studied within the mul- tivariate regression model.
The presence of metastases at diagnosis, of which 40 cases were in local lymph nodes and five at distant sites, shows a twofold recurrence risk. Lymph node status is a controversial predictor and appears to have variable sig- nificance depending on the clinical setting, a positive status having no deleterious effect when present in young patientslo3l3 or when associated with intrathyroid tumor.3h Distant metastases have an unequivocally negative influ- ence on O U ~ C O ~ ~ . ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ * But even at this stage, disease can be brought to a standstill in a large number of cases: in 70% of patients younger than 40 years and in 10% older than that age according to the M. D. Anderson Hos- pital series.44 In the current series, two patients younger than age 20 years, with pulmonary metastases, are free of disease after more than 15 years follow-up, whereas seven patients older than 40 years have persistent disease or have died of it.
In our multivariate analysis, age (> 45 years), size (> 3 cm) and presence of carcinomatous lymphangitis re- mained significant predictors for women, metastases at diagnosis and cystic growth for men. This difference in prognostic factors between the two sexes is of interest and will need to be confirmed. It is not excluded that it is an artifact due to the small numbers in our male population, rendering the interpretation of our results difficult. The female population is, however, large enough and a simple model is proposed to assess the risk of recurrence for a female patient based on age, tumor size, and carcino- matous lymphangitis: in the absence of any factor the risk is quite small (2% to 3%), with one of these factors the risk is roughly 10% and about one third of the women with more than one factor may be expected to develop a recurrence.
deleterious factor for s u r v ~ v a ~ , 5 . X . 1 4 . ~ 8 ~ ~ Y . 2 3 . ~ 5 . 2 ~ . 2 X , 3 0 , ~ l , 3 5 . 4 3
REFERENCES
I . Frazell EL. Foote FW. Papillary cancer of the thyroid. Cumw 1958;
2 . Hedinger C . Histological Typing ofThyroid Tumors, ed. 2. Berlin: Springer, 1988; 21-23 (International Histological Classitication of Tu- mors, vol. I I ).
3 . Tollefsen HR. DeCosse JJ, Hutter RVP. Papillary carcinoma of the thyroid: A clinical and pathological study of 70 fatal cases. C'nrwr 1964: 17: 1035-1044.
4. Meissner WA. Warren S. Tumors of the Thyroid Gland. Wash- ington: US Armed Forces Institute of Pathology, 1969: 70-84.
5. Woolner LB, Thyroid carcinoma: Pathologic classification with data on prognosis. S~~wziri N i d A f d 197 I : 1:48 1-50?,
6. Tollefsen HR, Shah JP, Huvos AG. Papillary carcinoma of the
11:895-922.

330 CANCER July I5 1991 Vol. 68
thyroid: Recurrence in the thyroid gland after initial surgical treatment. Am J Surg 1972; 124:468-472.
7. Simonin R, Grisoli J, Heim J, San Marco JL. Serment G. Le pron- ostic du cancer thyroidien: Expkrience personnelle. Ann Endocrin (Paris)
8. Franssila KO. Prognosis in thyroid carcinoma. Cancer 1975; 36:
9. BeaugiC JM, Brown CL, Doniach I, Richardson JE. Primary ma- lignant tumours of the thyroid: The relationship between histological classification and clinical behaviour. Br J Sitrg 1976; 63: 173- 18 1.
10. Cady B, Sedgwick CE. Meissner WA. Bookwalter JR. Romagosa V , Werber J. Changing clinical, pathologic, therapeutic, and survival patterns in differentiated thyroid carcinoma. Ann Surg 1976; 184:541- 553.
11. Gardet P, Parmentier C, Gerard-Marchant R el a/. Differentiated cancers of the thyroid: Course after treatment with special reference to frequency and chronology of first relapse for 470 treated patients. Ann Radio/ 1977; 20:831-840.
12. Franssila KO. Outcome in papillary carcinoma of the thyroid. Ann Chir Gvnaecol 1978: 67:49-57.
13. Harwood J , Clark OH, Dunphy JE. Significance of lymph-node metastasis in differentiated thyroid cancer. A m J Surg 1978; 136:107- 110.
14. Cady B. Sedgwick CE. Meissner WA, Wool MS, Salzman FA, Werber J. Risk factor analysis in differenciated thyroid cancer. Cancer 1979; 43:810-820.
15. Howard RB, Truels WP. Thyroid cancer: Thirty-year review of 201 cases. Am J Surg 1979: I38:934-938.
16. Friedmann M, Skolnik E, Baim HM. Becker SP. Katz AH. Man- travadi RVP. Thyroid carcinoma. Laryngoscope 1980: 90: 199 1-2003.
17. Hofstidter F, Unterkircher S. Histologische Kriterien zur Prognose der Struma maligna. Palhologe 1980; 1:79-85.
18. Krisch K, Depisch D. Jakesz R, Keminger K, Kokoschka R. Das papillare Schilddriisenkarzinom. Wien K/in Wochenschr 1980; 92: I I3- 118.
19. Mazzaferri EL, Young RL. Papillary thyroid carcinoma: A 10 year follow-up report of the impact of therapy in 576 patients. Am J Med 1981; 70:511-518.
20. Samaan NA, Maheshwari YK, Nader S et a/. Impact of therapy for differenciated carcinoma of the thyroid: An analysis of 706 cases. J Clin EndocrinolMefah 1983; 56:l 131-1 138.
21. Christensen SB. Ljungberg 0, Tibblin S. Thyroid carcinoma in Malmo 1960-1977: Epidemiologic, clinical and prognostic findings in a defined urban population. Cancer 1984; 53:1625-1633.
22. Donohue JH. Goldfien SD, Miller TR. Abele JS, Clark OH. Do the prognoses of papillary and follicular thyroid carcinomas differ? Am JSitrg 1984; 148:168-172.
23. Carcangiu ML, Zampi G. Pupi A, Castagnoli A, Rosai J. Papillary carcinoma of the thyroid: A clinicopathologic study of 241 cases treated at the University of Florence, Italy. Cancer 1985: 55:805-828.
24. Ontai S, Straehley CJ. The surgical treatment of well-differentiated carcinoma of the thyroid. Am J Surg 1985; 5 1:653-657.
25. McCohaney WM, Hay ID. Woolner LB. van Heerden JA, Taylor WF. Papillary thyroid cancer treated at the Mayo Clinic. 1946 through 1970: Initial manifestations, pathologic findings, therapy, and outcome. Mayo Clin Proc 1986; 61:978-996.
1974; 351483-484.
1138-1 146.
26. Rossi RL, Cady B, Silverman ML. Wool MS. Homer TA. Current results of conservative surgery for differentiated thyroid carcinoma. Wor/d J Surg 1986: l0:6 12-622.
27. Byar DP. Green SB, Dor P et a/. A prognostic index for thyroid carcinoma: A study of the EORTC Thyroid Cancer Cooperative Group. Eur JCancer 1979: 15:1033-1041.
28. Wanebo HJ. Andrews W. Kaiser DL. Thyroid cancer: Some basic considerations. Am J Surg I98 I ; 142:474-479.
29. Fourquet A, Asselain B, Joly J. Cancer de la thyroide: Analyse multidimensionnelle des facteurs pronostiques. Ann Endocrinol (Paris)
30. Ladurner D, Seeber G, Hofstadter F. Das papillare Schilddriisen- carcinom: Prognose und prognostische Faktoren. Longenbecks Arch Chir
31. Tennvall J, Biorklund A. Moller T. Ranstam J, Akerman M. Prognostic factors of papillary, follicular and medullary carcinomas of the thyroid gland: Retrospective multivariate analysis of 2 16 patients with a median follow-up of I 1 years. .4cla Radio/ Oncol 1985; 24:17- 24.
32. Tubiana M, Schlumberger M. Rougier P ei a/. Long-term results and prognostic factors in patients with differentiated thyroid carcinomas. Cancer 1985; 55:794-804.
33. Bacourt F, Asselain B, Savoie JC el a/. Multifactorial study of prognostic factors in differentiated thyroid carcinoma and a re-evaluation of the importance of age. Br JSurg 1986; 73:274-277.
34. Hay ID, Grant CS, Taylor WF, McConahey WM. Ipsilateral lo- bectomy versus bilateral lobar resection in papillary thyroid carcinoma: A retrospective analysis of surgical outcome using a novel prognostic scoring system. Surgery 1987: 102:1088-1095.
35. Simpson WJ, McKinney SE, Carruthers JS, Gospodarowicz MK, Suttcliffe SB, Panzarella T. Papillary and follicular thyroid cancer: Prog- nostic factors in 1.578 patients. Am J hfed 1987: 83:479-488.
36. Vickery AL, Wang CA, Walker AM. Treatment of intrathyroidal carcinoma of the thyroid. Cancer 1987; 60:2587-2595.
37. Smith SA, Hay ID, Goellner JR, Ryan JJ, McCohaney WM. Mortality from thyroid carcinoma: A case-control study of 56 lethal cases. Cancer 1988: 62: I38 I - I 388.
38. Tscholl-Ducommun J. Hedinger CE. Papillary thyroid carcinomas: Morphology and prognosis. Virchows '4rc.h [ A ] 1982: 396: 19-39,
39. Warren S, Meissner WA. Thyroid Tumors. Washington, DC: US Armed Forces Institute of Pathology, 1953; 36-39.
40. Vickery AL. Thyroid papillary carcinoma: Pathological and phil- osophical controversies. A m J Slug Patho/ 1983; 7:797-807.
4 I . Schroder S, Bocker W, Dralle H. Kortmann KB, Stern C. The encapsulated papillary carcinoma ofthe thyroid: A morphologic subtype of the papillary thyroid carcinoma. Cuncer 1984; 54:90-93.
42. Frauenhoffer CM, Patchefsky AS, Cobanoglu A. Thyroid carci- noma: A clinical and pathologic study of 125 cases. Cuncer 1979; 43: 24 14-242 I .
43. Cody HS, Shah JP. Locally invasive, well-differenciated thyroid cancer: Twenty-two years experience at Memorial Sloan-Kettering cancer center. Am JSurg 1981; 142:480-483.
44. Samaan NA. Schultz PN. Haynie TP. Ordonez NG. Pulmonary metastasis of differenciated thyroid carcinoma: Treatment results in 10 I patients. J Clin Endocrinol Metab 1985; 60:376-380.
1983; 44: 12 1-1 26.
1984; 363~43-55.