profile of learning opportunities - … · this profile of learning opportunities is a document...
TRANSCRIPT
PROFILE OF LEARNING
OPPORTUNITIES
NORTHUMBRIA HEALTHCARE NHS FOUNDATION TRUST
ENDOSCOPY DEPARTMENT NTGH
June 2010 Author:- Lyndsey Fieldson
Link Mentor:- Sylvia Chaplin

GUIDANCE FOR PRACTICE PLACEMENT EDUCATORS AND STUDENTS.
This profile of learning opportunities is a document that details learning opportunity within your placement. This file is a growing and dynamic document, with staff and students being responsible for keeping it updated and relevant for their clinical area. It is intended that practice placement educators and students utilise this resource to select appropriate learning opportunities to help students meet their specified competencies. It is expected that students will use this file as a resource and be proactive in identifying their learning needs. Many of these learning opportunities will take place with a variety of professionals including other allied health professionals, district nurses, health visitors, public health nurses, specialist nurses and practice nurses. This resource gives an overview of the inter agency and multi professional contacts which students may encounter during their placement, however not all of these opportunities will be accessible.
On the first day of practice placement within primary care, the student must have an induction into their practice area. Please ensure that the induction checklist is completed and retained in this portfolio. Following placements, student evaluation forms should be retained in the practice area. These should be used to reinforce good practice placement education and developmental opportunities. Please retain student evaluations (with students permission) in this portfolio for audit purposes.
(Copyright Newcastle and North Tyneside PCT - Lynn Dracup December 2003)
CONTENTS
1. AREA PROFILE.
2. LEARNING ZONES.
3. LEARNING OPPORTUNITES.
4. ADDITIONAL LEARNING OPPORTUNITIES SPECIFIC
TO AREA OF PRACTICE.
5. REFERRAL PATHWAYS
6. RELEVANT STANDARDS OF PRACTICE
7. RELEVANT INFORMATION FOR STUDENTS
8. READING LIST
AREA PROFILE.
CLINICAL AREA (DESCRIPTION)- ENDOSCOPY -
LOCATION
NTGH Endoscopy unit comes under the surgical Directorate of Northumbria Healthcare NHS Foundation Trust. We are situated on the main corridor between Pathology and Surgical Day Unit North Tyneside General Hospital. The department has two treatment rooms and 12 recovery bays. Patients undergoing gastroscopy, sigmoidoscopy, colonoscopy, bronchoscopy and ERCP are cared for by endoscopy staff. We also have specialist nurse clinics in the Out Patients Department which we staff. Patients who attend the unit can access the department via four routes:- Open Access Referred directly from their own GP Waiting List Referred directly from their own GP Urgent Referrals Patients seen within 2 weeks of referral
from GP Emergency Referrals Patients who have already been admitted To hospital All members of staff within the endoscopy unit follow strict guidelines which are set out clearly by the British Society of Gastroenterologists. Sister Maureen Carmichael manages Endoscopy Services here and at Wansbeck General Hospital, Sister Marshall manages this unit on a daily basis, supported by Staff Nurses, Health Care Assistants, Endoscopy Technicians and Clerical Staff.
TELEPHONE NUMBER—01912932580
SHIFT PATTERNS
The unit operates Monday to Friday 8am – 6pm, shift patterns are negotiated with your mentor. Off duty is organised 3 weeks in advance and even though you will remain supernumerary for the duration of your placement, you will be expected to request specific off duty in advance, as all other staff.
PHILOSOPHY OF CARE-
Endoscopy staff work as a team to create a safe and friendly
environment, maintaining high standards of Nursing Care at
all times.
Our Aim is to:-
Provide a holistic approach to patients care, involving
relatives, friends and carers.
To treat each patient as an individual, respecting their
privacy, dignity and beliefs.
To share knowledge and promote health education
To involve all members of the multidisciplinary team to
provide the best care and treatment for our patients.
Finally we are committed to provide excellent service.
Please feel free to question any member of staff about any
concerns you may have.
PRACTICE PLACEMENT EDUCATORS--
Sister Sandra Marshall
Staff Nurse Debra Morrow
Staff Nurse Valerie Greenwood
Staff Nurse Shirley Douthwaite
Staff Nurse Fiona Antcliffe
Staff Nurse Sylvia Chaplin
Staff Nurse Jill Gascoigne
NAMED PERSON RESPONSIBLE FOR POLO –
Staff Nurse Sylvia Chaplin
POLO REVIEW DATE—
June 2011
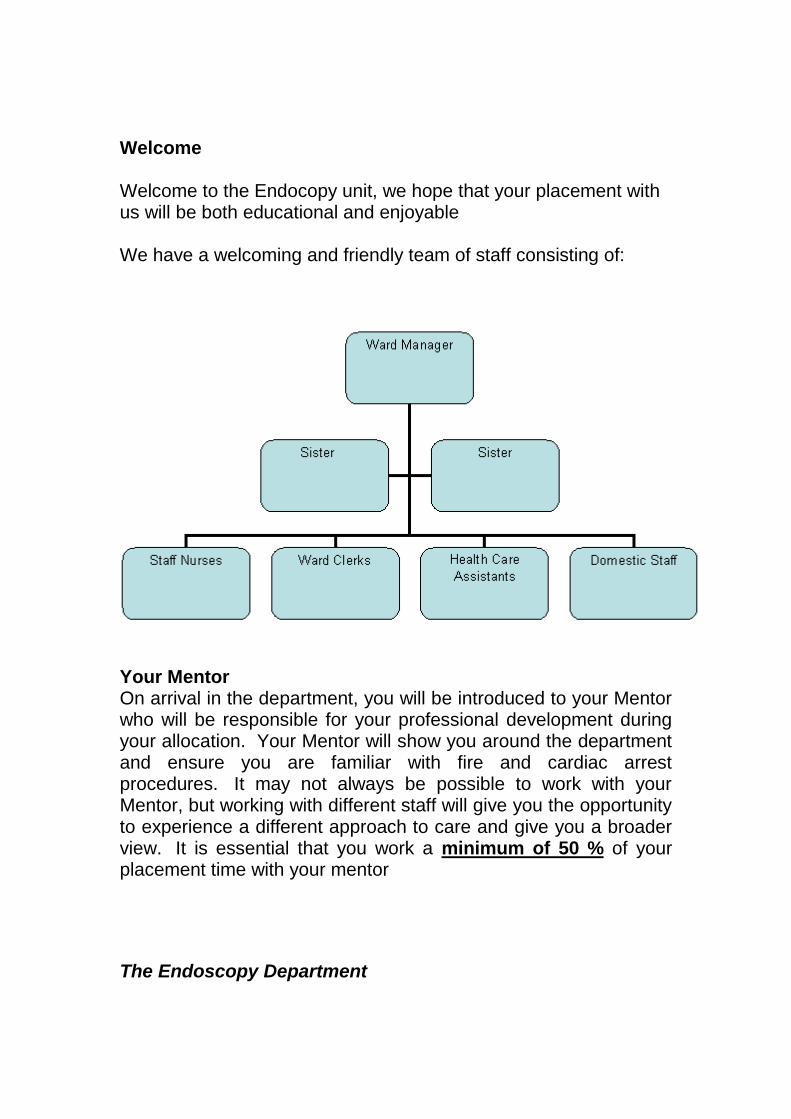
Welcome Welcome to the Endocopy unit, we hope that your placement with us will be both educational and enjoyable We have a welcoming and friendly team of staff consisting of:
Your Mentor On arrival in the department, you will be introduced to your Mentor who will be responsible for your professional development during your allocation. Your Mentor will show you around the department and ensure you are familiar with fire and cardiac arrest procedures. It may not always be possible to work with your Mentor, but working with different staff will give you the opportunity to experience a different approach to care and give you a broader view. It is essential that you work a minimum of 50 % of your placement time with your mentor
The Endoscopy Department
The Endoscopy Unit sees approximately 7000 patients per year, the majority of which are outpatients, but an inpatient service is also provided. The endoscope is an expensive, complex piece of equipment with channels enabling the use of instruments to take biopsies on therapeutic procedures. The endoscope is connected to a processor, which supplies the light and air supply. The processor is able to transmit an image onto the monitor in much the same way as a TV camera transmits images. This is why many patients call the test ―having the camera‖ An Endoscopy procedure can be described as either diagnostic (when a cause for a patients symptoms may be discovered) or therapeutic (where treatment can be administered to ease the patients problem/disease) The term ―endoscopy‖ literally means, ―to look in and see‖. It is a generic term and can describe a variety of procedures. It is a term, which is widely used, therefore may cause some confusion. For that reason, it is preferable to use specific terminology, ie: Gastroscopy, Colonoscopy and Flexible Sigmoidoscopy, to accurately describe the area to be looked at ENDOSCOPY EXPECTATIONS OF STUDENTS
We expect all students allocated to the department to arrive on time, if you are going to be late please call and let staff know as soon as possible
If you are going to be off sick, please telephone the department as soon as possible, speak to either Sylvia Chaplin (Link Mentor) or Sandra Marshall (Sister), informing them why you are off sick and when you hope to return to placement. You must also let the department know when you will be resuming work.
Please ensure that you contact the university sick line and report your sickness absence
We do expect you to be on time for your shift — therefore you must contact the ward if you are going
to be late or absent
Whilst on placement you will be required to wear surgical scrubs (provided by the unit), please adhere to the trust dress policy, including:-
Minimal jewellery should be worn, if any, one pair of stud earrings and a single wedding band with no stones. Do not wear wrist watches or anything else on your wrists and arms.
Your trust identification badge is to be worn at all times whilst on duty.
Sensible shoes need to be worn (flat, soft rubber soles, covered toes).
YOU MUST NOT WEAR WORK SHOES OR UNIFORMS
OFF HOSPITAL GROUNDS.
Most importantly, to attend the department and demonstrate a professional manner, a willingness to learn, making the most of every learning experience available.
EMERGENCY ALARM CALLS AND NUMBERS
FIRE ALARM Every Friday the fire alarms will sound at an intermittent tone as a test procedure. If the alarm sounds at any other time this would indicate a real fire could be in progress and immediate action must be taken. It is EVERY-ONES responsibility to ensure all doors and windows are shut and remain so until the stand down is given. If the alarm sounds with a continuous unbroken tone, this would indicate the fire is close to your working area and requires urgent investigation and the possibility of evacuation of all staff, patients and relatives. You will be given full direction by the nurse in charge if this occurs.
CALL 2222 (Speak to operator and state: Fire,
Endoscopy, North Tyneside Hospital CRASH CALL In the event of a cardiac arrest on the ward, your first line of action is to summon assistance from other members of staff. Your mentor will outline your expected role as a student during your initial interview and staff at the time will support you during any action taken.
CALL 2222 (Speak to operator and state: Cardiac
Arrest, Endoscopy, North Tyneside Hospital North
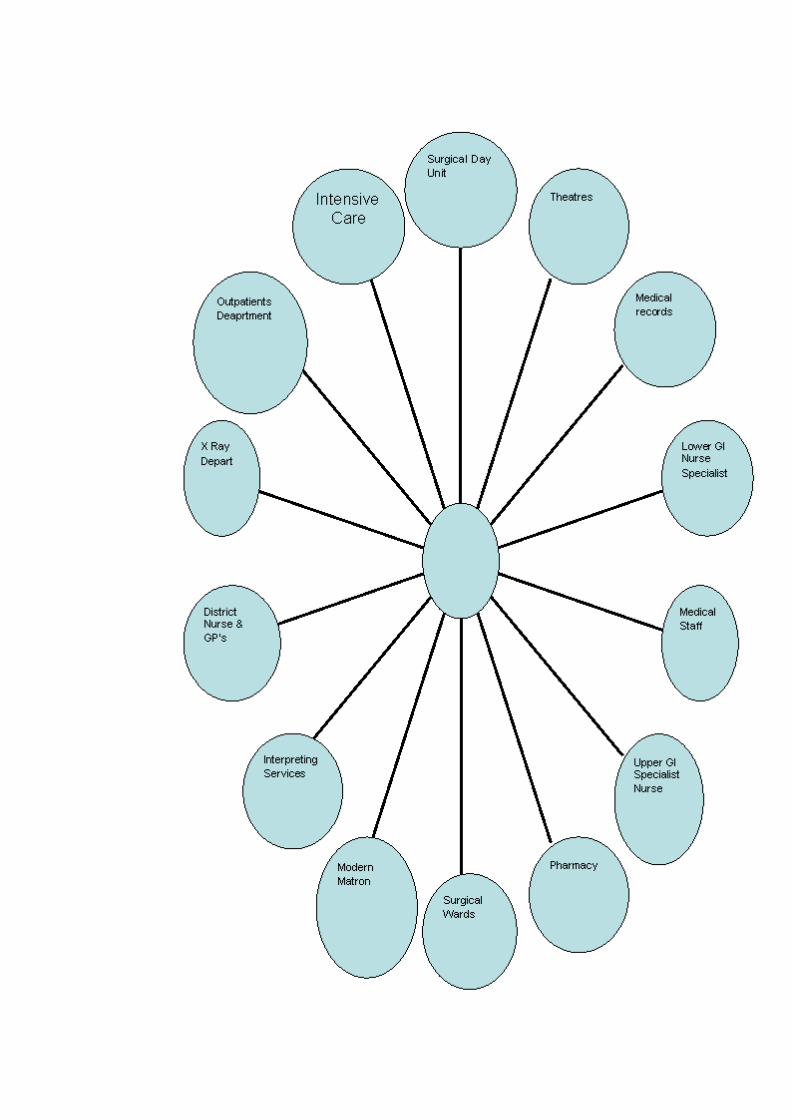
LEARNING ZONES.
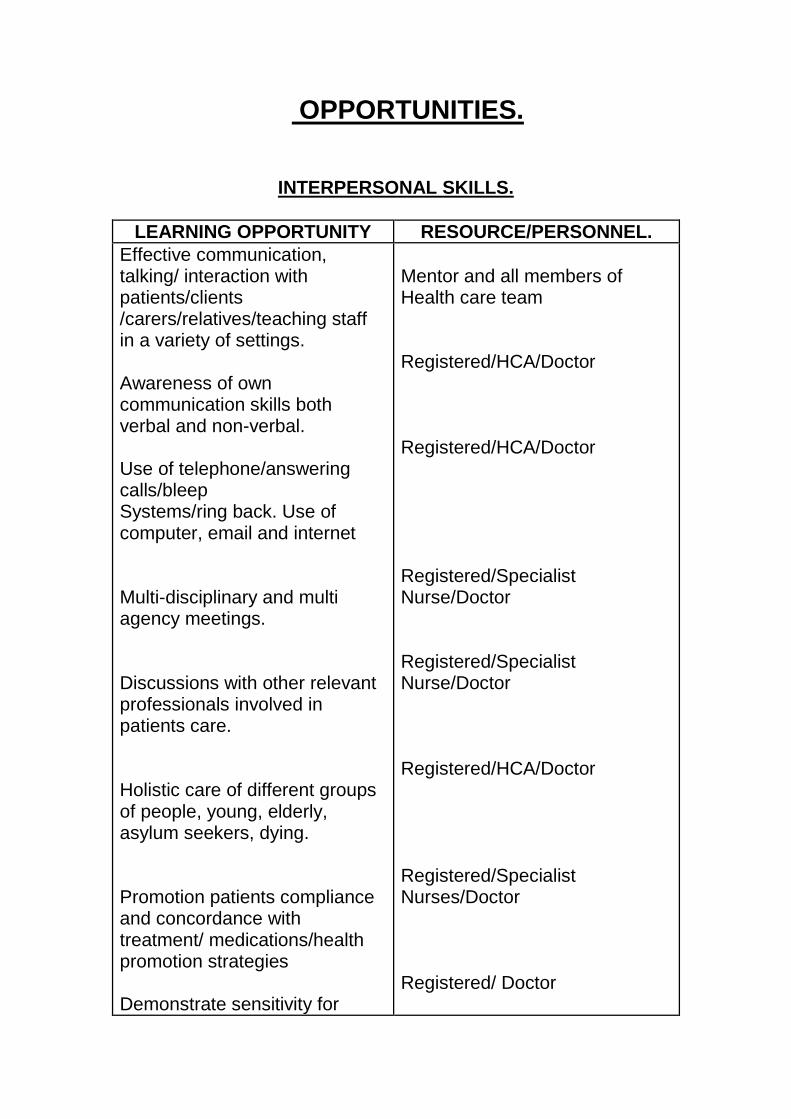
OPPORTUNITIES.
INTERPERSONAL SKILLS.
LEARNING OPPORTUNITY RESOURCE/PERSONNEL.
Effective communication, talking/ interaction with patients/clients /carers/relatives/teaching staff in a variety of settings. Awareness of own communication skills both verbal and non-verbal. Use of telephone/answering calls/bleep Systems/ring back. Use of computer, email and internet Multi-disciplinary and multi agency meetings. Discussions with other relevant professionals involved in patients care. Holistic care of different groups of people, young, elderly, asylum seekers, dying. Promotion patients compliance and concordance with treatment/ medications/health promotion strategies Demonstrate sensitivity for
Mentor and all members of Health care team Registered/HCA/Doctor Registered/HCA/Doctor Registered/Specialist Nurse/Doctor Registered/Specialist Nurse/Doctor Registered/HCA/Doctor Registered/Specialist Nurses/Doctor Registered/ Doctor
patients/carers in relation to distressing information. Support and enable patients/carers/groups and communities to take action and prioritise health needs. Demonstrate effective communication between primary care networks. Experiences with clients from a variety of ethnic backgrounds and asylum seekers
Registered/HCA/Doctor Registered/Specialist Nurses/Doctor Registered/Specialist Nurse/Doctor Interpreting services.
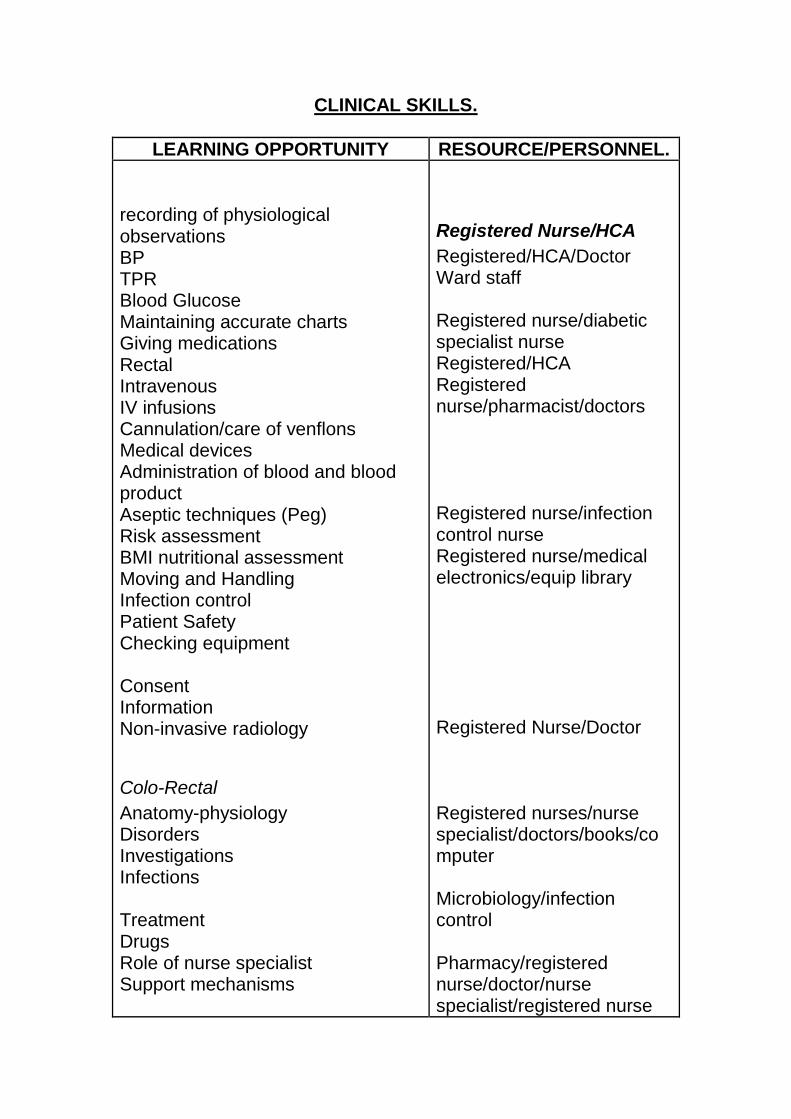
CLINICAL SKILLS.
LEARNING OPPORTUNITY RESOURCE/PERSONNEL.
recording of physiological observations BP TPR Blood Glucose Maintaining accurate charts Giving medications Rectal Intravenous IV infusions Cannulation/care of venflons Medical devices Administration of blood and blood product Aseptic techniques (Peg) Risk assessment BMI nutritional assessment Moving and Handling Infection control Patient Safety Checking equipment Consent Information Non-invasive radiology
Colo-Rectal
Anatomy-physiology Disorders Investigations Infections Treatment Drugs Role of nurse specialist Support mechanisms
Registered Nurse/HCA
Registered/HCA/Doctor Ward staff Registered nurse/diabetic specialist nurse Registered/HCA Registered nurse/pharmacist/doctors Registered nurse/infection control nurse Registered nurse/medical electronics/equip library Registered Nurse/Doctor Registered nurses/nurse specialist/doctors/books/computer Microbiology/infection control Pharmacy/registered nurse/doctor/nurse specialist/registered nurse
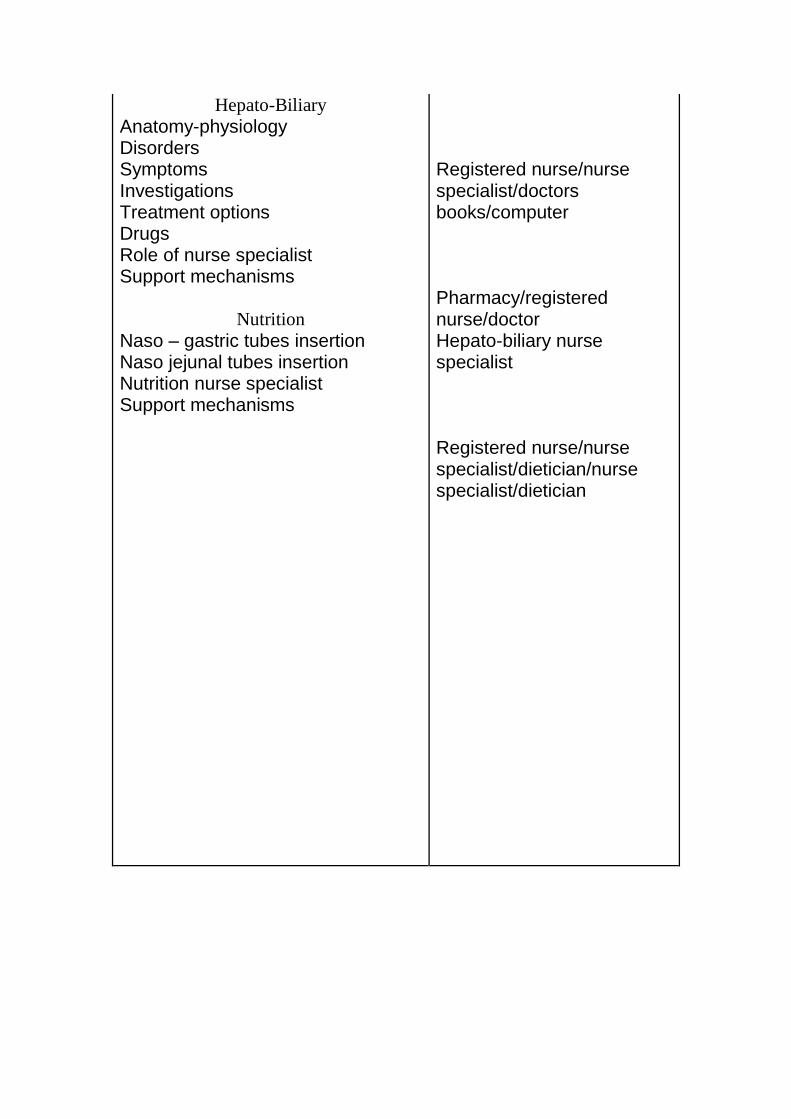
Hepato-Biliary
Anatomy-physiology Disorders Symptoms Investigations Treatment options Drugs Role of nurse specialist Support mechanisms
Nutrition
Naso – gastric tubes insertion Naso jejunal tubes insertion Nutrition nurse specialist Support mechanisms
Registered nurse/nurse specialist/doctors books/computer Pharmacy/registered nurse/doctor Hepato-biliary nurse specialist Registered nurse/nurse specialist/dietician/nurse specialist/dietician
HEALTH PROMOTION OPPORTUNITIES.
LEARNING OPPORTUNITY RESOURCE/PERSONNEL.
Healthy life style in relation to
Smoking cessation Alcoholic liver disease Bowel disorders Cancer Obesity Diabetes Eating for a healthy heart Drug and alcohol abuse Promotion of exercise Healthy heart
Patient information leaflets and Health Promotion unit
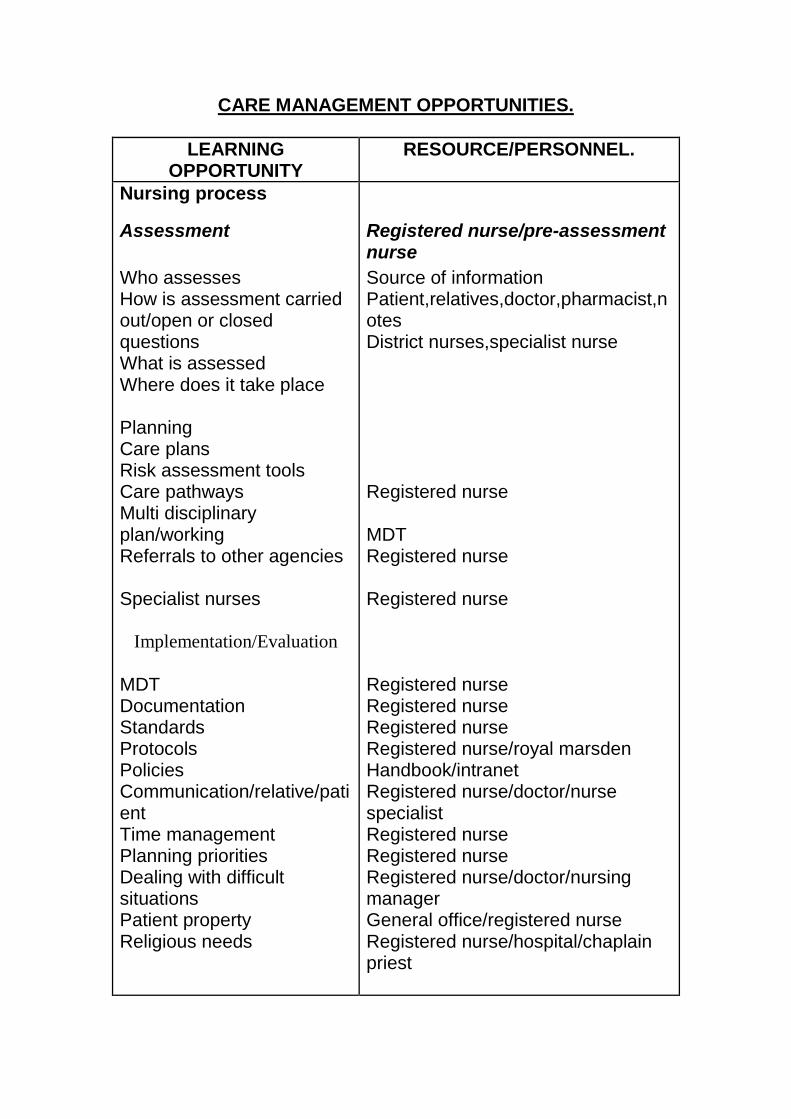
CARE MANAGEMENT OPPORTUNITIES.
LEARNING OPPORTUNITY
RESOURCE/PERSONNEL.
Nursing process
Assessment
Who assesses How is assessment carried out/open or closed questions What is assessed Where does it take place Planning Care plans Risk assessment tools Care pathways Multi disciplinary plan/working Referrals to other agencies Specialist nurses
Implementation/Evaluation
MDT Documentation Standards Protocols Policies Communication/relative/patient Time management Planning priorities Dealing with difficult situations Patient property Religious needs
Registered nurse/pre-assessment nurse
Source of information Patient,relatives,doctor,pharmacist,notes District nurses,specialist nurse Registered nurse MDT Registered nurse Registered nurse Registered nurse Registered nurse Registered nurse Registered nurse/royal marsden Handbook/intranet Registered nurse/doctor/nurse specialist Registered nurse Registered nurse Registered nurse/doctor/nursing manager General office/registered nurse Registered nurse/hospital/chaplain priest
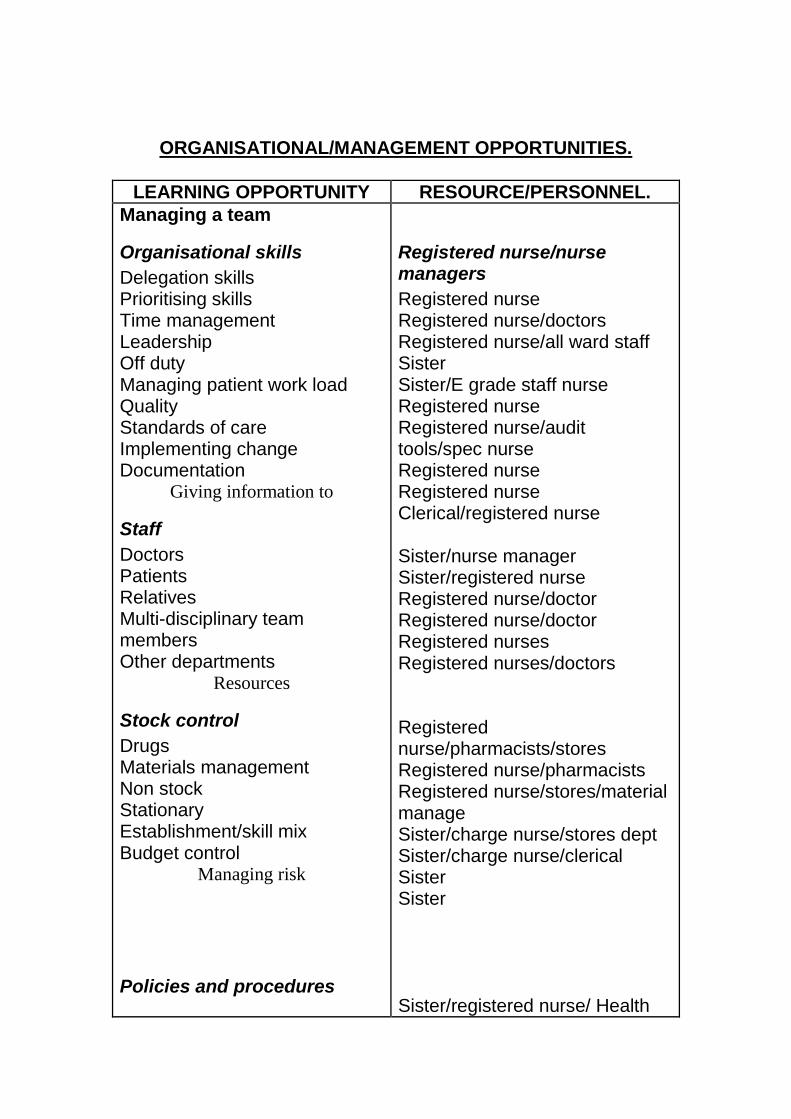
ORGANISATIONAL/MANAGEMENT OPPORTUNITIES.
LEARNING OPPORTUNITY RESOURCE/PERSONNEL.
Managing a team
Organisational skills
Delegation skills Prioritising skills Time management Leadership Off duty Managing patient work load Quality Standards of care Implementing change Documentation
Giving information to
Staff
Doctors Patients Relatives Multi-disciplinary team members Other departments
Resources
Stock control
Drugs Materials management Non stock Stationary Establishment/skill mix Budget control
Managing risk
Policies and procedures
Registered nurse/nurse managers
Registered nurse Registered nurse/doctors Registered nurse/all ward staff Sister Sister/E grade staff nurse Registered nurse Registered nurse/audit tools/spec nurse Registered nurse Registered nurse Clerical/registered nurse Sister/nurse manager Sister/registered nurse Registered nurse/doctor Registered nurse/doctor Registered nurses Registered nurses/doctors Registered nurse/pharmacists/stores Registered nurse/pharmacists Registered nurse/stores/material manage Sister/charge nurse/stores dept Sister/charge nurse/clerical Sister Sister Sister/registered nurse/ Health
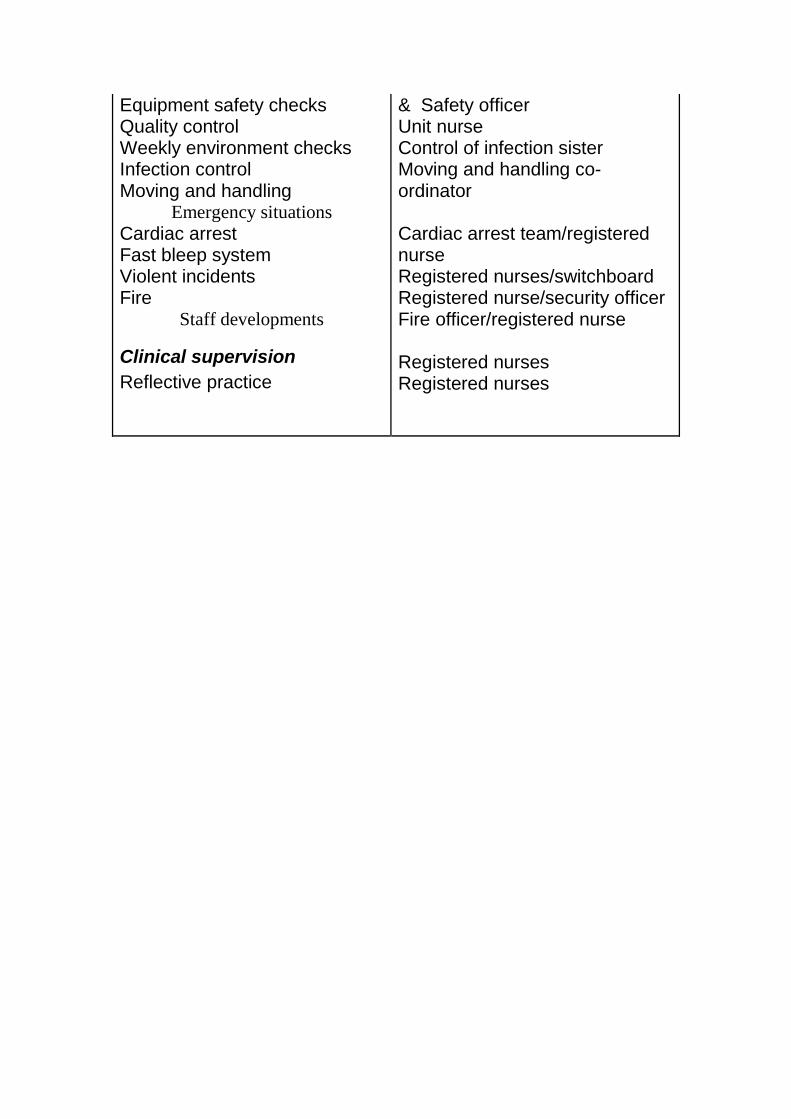
Equipment safety checks Quality control Weekly environment checks Infection control Moving and handling
Emergency situations
Cardiac arrest Fast bleep system Violent incidents Fire
Staff developments
Clinical supervision
Reflective practice
& Safety officer Unit nurse Control of infection sister Moving and handling co-ordinator Cardiac arrest team/registered nurse Registered nurses/switchboard Registered nurse/security officer Fire officer/registered nurse Registered nurses Registered nurses
ADDITIONAL LEARNING OPPORTUNITIES SPECIFIC TO AREA OF PRACTICE.
LEARNING OPPORTUNITY RESOURCE/PERSONNEL.
REFERRAL PATHWAYS.
RELEVANT STANDARDS OF PRACTICE
RELEVANT INFORMATION FOR STUDENTS
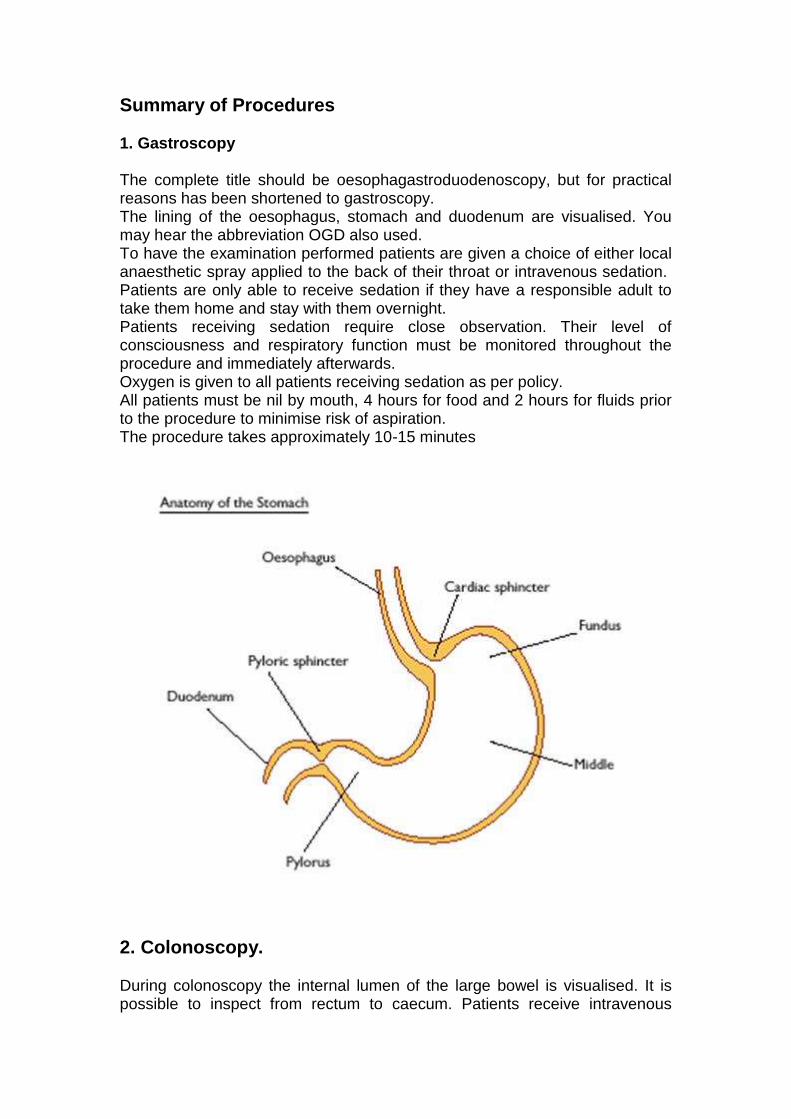
Summary of Procedures 1. Gastroscopy The complete title should be oesophagastroduodenoscopy, but for practical reasons has been shortened to gastroscopy. The lining of the oesophagus, stomach and duodenum are visualised. You may hear the abbreviation OGD also used. To have the examination performed patients are given a choice of either local anaesthetic spray applied to the back of their throat or intravenous sedation. Patients are only able to receive sedation if they have a responsible adult to take them home and stay with them overnight. Patients receiving sedation require close observation. Their level of consciousness and respiratory function must be monitored throughout the procedure and immediately afterwards. Oxygen is given to all patients receiving sedation as per policy. All patients must be nil by mouth, 4 hours for food and 2 hours for fluids prior to the procedure to minimise risk of aspiration. The procedure takes approximately 10-15 minutes
2. Colonoscopy. During colonoscopy the internal lumen of the large bowel is visualised. It is possible to inspect from rectum to caecum. Patients receive intravenous
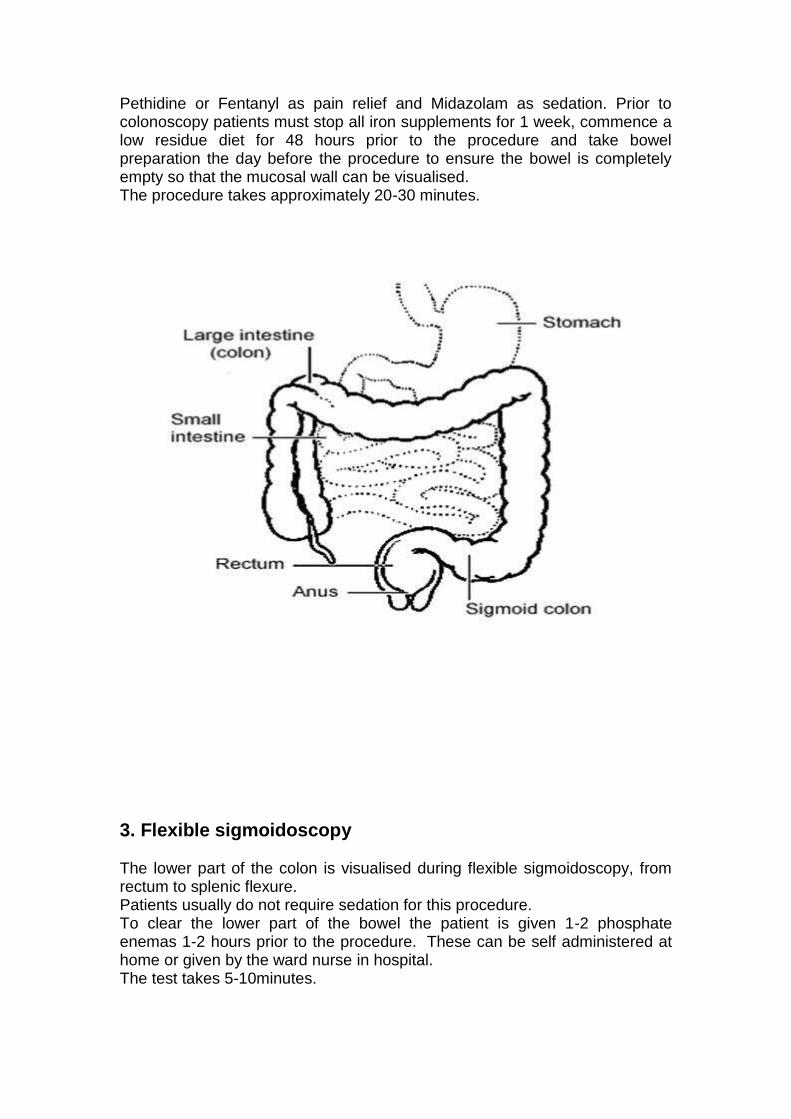
Pethidine or Fentanyl as pain relief and Midazolam as sedation. Prior to colonoscopy patients must stop all iron supplements for 1 week, commence a low residue diet for 48 hours prior to the procedure and take bowel preparation the day before the procedure to ensure the bowel is completely empty so that the mucosal wall can be visualised. The procedure takes approximately 20-30 minutes.
3. Flexible sigmoidoscopy The lower part of the colon is visualised during flexible sigmoidoscopy, from rectum to splenic flexure. Patients usually do not require sedation for this procedure. To clear the lower part of the bowel the patient is given 1-2 phosphate enemas 1-2 hours prior to the procedure. These can be self administered at home or given by the ward nurse in hospital. The test takes 5-10minutes.
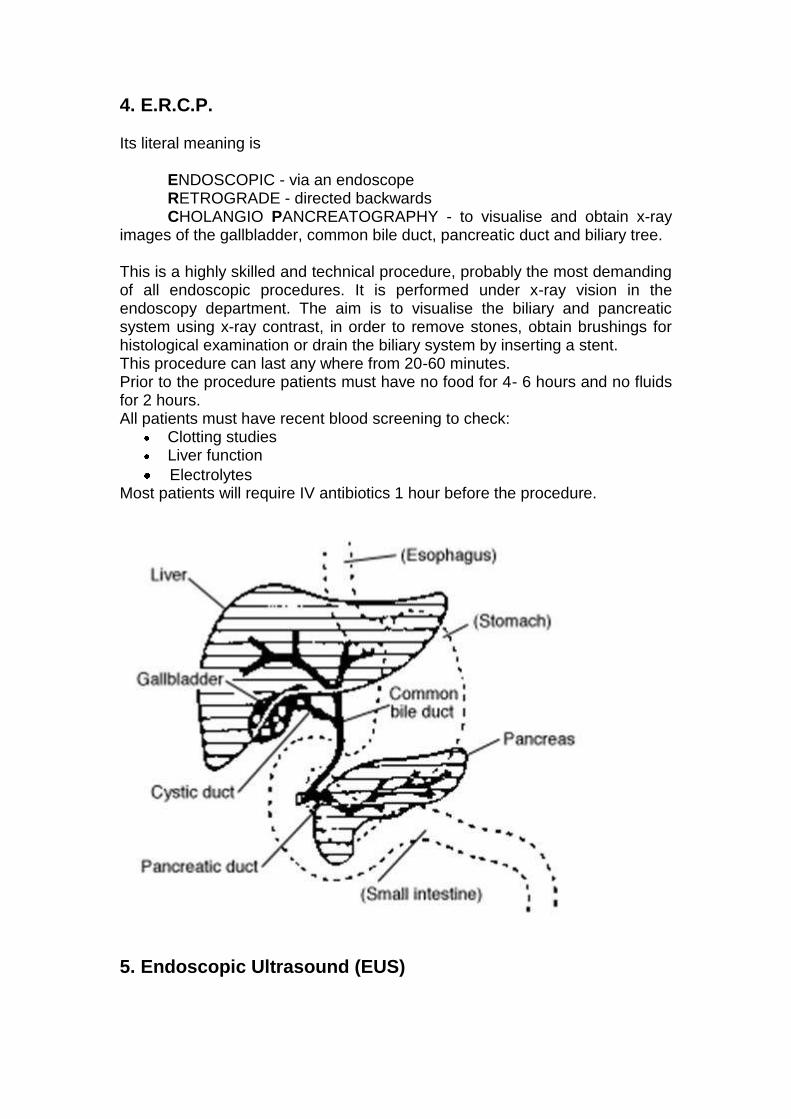
4. E.R.C.P. Its literal meaning is
ENDOSCOPIC - via an endoscope RETROGRADE - directed backwards CHOLANGIO PANCREATOGRAPHY - to visualise and obtain x-ray
images of the gallbladder, common bile duct, pancreatic duct and biliary tree. This is a highly skilled and technical procedure, probably the most demanding of all endoscopic procedures. It is performed under x-ray vision in the endoscopy department. The aim is to visualise the biliary and pancreatic system using x-ray contrast, in order to remove stones, obtain brushings for histological examination or drain the biliary system by inserting a stent. This procedure can last any where from 20-60 minutes. Prior to the procedure patients must have no food for 4- 6 hours and no fluids for 2 hours. All patients must have recent blood screening to check:
Clotting studies Liver function
Electrolytes Most patients will require IV antibiotics 1 hour before the procedure.
5. Endoscopic Ultrasound (EUS)
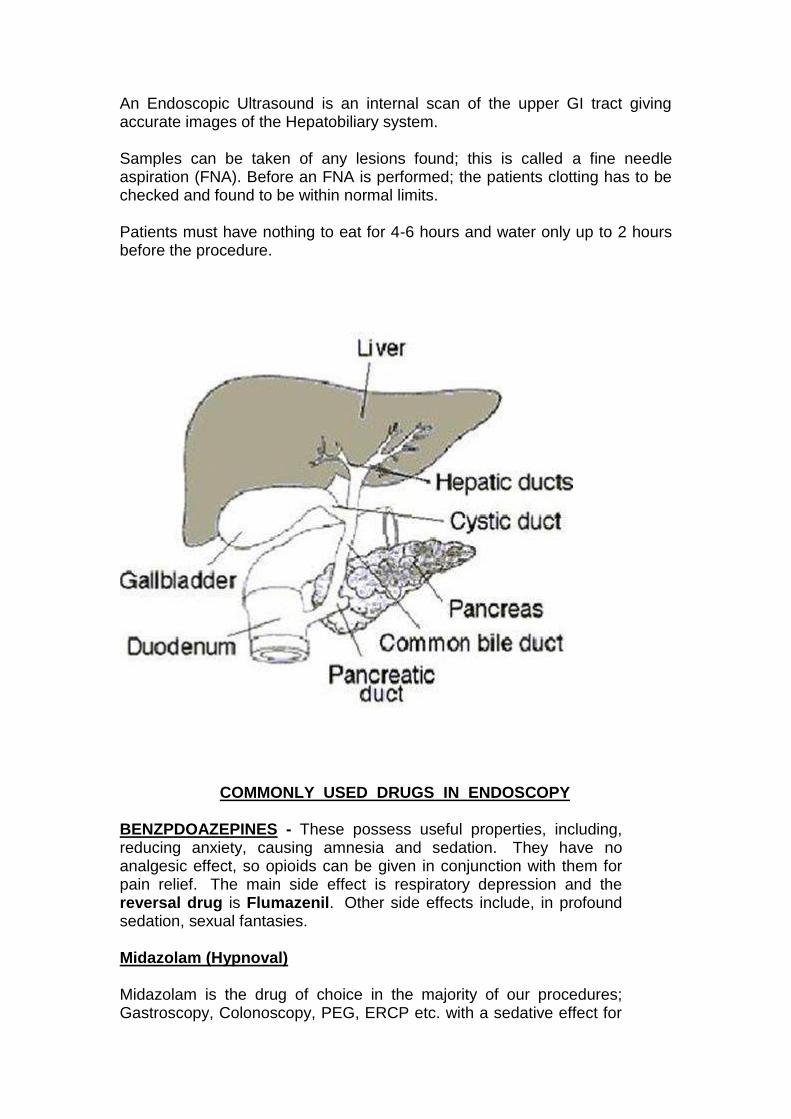
An Endoscopic Ultrasound is an internal scan of the upper GI tract giving accurate images of the Hepatobiliary system. Samples can be taken of any lesions found; this is called a fine needle aspiration (FNA). Before an FNA is performed; the patients clotting has to be checked and found to be within normal limits. Patients must have nothing to eat for 4-6 hours and water only up to 2 hours before the procedure.
COMMONLY USED DRUGS IN ENDOSCOPY
BENZPDOAZEPINES - These possess useful properties, including, reducing anxiety, causing amnesia and sedation. They have no analgesic effect, so opioids can be given in conjunction with them for pain relief. The main side effect is respiratory depression and the reversal drug is Flumazenil. Other side effects include, in profound sedation, sexual fantasies.
Midazolam (Hypnoval)
Midazolam is the drug of choice in the majority of our procedures; Gastroscopy, Colonoscopy, PEG, ERCP etc. with a sedative effect for
up to 24 hours. Midazolam has a faster recovery time than other Benzodiazepines.
Given IV. Draw up 1 ampoule in 5 ml labelled syringe. Concentration is 10mg/5ml – 2mg/1ml.
Diazepam (Diazemuls)
Diazepam is the preference of some doctors for ERCP. It is longer acting and can have a second period of drowsiness after several hours. It comes ready prepared as a white emulsion.
Given IV. Draw up 2x10mg ampoules into a 5ml labelled syringe. Concentration is 5mgs in 1ml.
OPIOIDS - Opoids are used to relieve moderate to severe pain. The main side effects include nausea, vomiting, constipation, drowsiness, hypotension and respiratory depression. The reversal drug is Naloxone (Narcan).
Pethidine
Pethidine is given during Colonoscopy and ERCP. Produces prompt short lasting analgesia.
Given IV. Draw up 1 ampoule in a 2ml labelled syringe. Concentration is 50mg/1ml.
Fentanyl
Fentanyl is the preference of some doctors for Colonoscopy. It is very quick acting.
Given IV. Draw up 1 ampoule in 2ml labelled syringe. Concentration is 100mcg in 2mls, 50mcg in 1ml. REVERSAL DRUGS - Used as antagonists. Both Naloxone and Flumazenil have shorter half life that the drugs they reverse, and the patient is at risk of becoming re-sedated.
Flumazenil (Anexate)
Flumazenil is used to reverse Benzodiazepines. It is short acting and may need to be repeated.
Given IV. Draw up 1 ampoule in 5ml labelled syringe. Concentration is 500mcgs in 5mls, 100mcgs in 1ml.
Naloxone (Narcan)
Naloxone is used to reverse Opioid drugs. It is short acting and may need to be repeated.
Given IV. Draw up 1 ampoule in 2ml labelled syringe. Concentration is 400mcg in 1ml.
ANTISPASMODICS
Used to relax the gut during therapeutic procedures and Colonoscopy by reducing peristalsis and spasm.
Hyoscine Butylbromide (Buscopan)
The side effects include bradycardia and tachycardia: therefore it should not be used for patients who have recently had an MI, or cardiac rhythm disturbances.
Given IV. Draw up I or 2 ampoules, depending on the dose required, in a 2ml labelled syringe. Concentration is 20mg in 1ml
Glucagon
Glucagon inhibits gut motility and tends to be used when Buscopan is contraindicated. Caution must be given to diabetic patients, as it is a hyperglycaemic agent. Glucagon comes in a ready prepared ―hypokit‖.
Given IV. The pack contains a syringe containing water and a vial of powder to be reconstituted, inject the water into the vial and then draw it up into a normal syringe so that the needle can be removed in order to be given IV. Concentration is 1 unit (1mg) in 1ml.
LOCAL ANAESTHETICS Lidocaine Throat Spray (Xylocaine) Lidocaine is used for Gastroscopy patients who do not want to be sedated. It works by numbing the mouth and throat. The loss of sensation may make swallowing difficult and reassurance is given to the patient that swallowing and breathing remain the same. This effect can last for up to one hour and the patient is kept nil by mouth for one hour to reduce the risk of aspiration.
READING LIST