procedural sedation
TRANSCRIPT
Procedural SedationKate Donaghy
26th March 2015
-American College of Emergency Physicians
“Procedural sedation and analgesia refers to the
technique of administering sedatives or dissociative
agents with or without analgesics to induce an
altered state of consciousness that allows the
patient to tolerate painful or unpleasant procedures
while preserving cardiorespiratory function.”
When Use it?
Fracture reduction
Joint Relocation
Wound management
Abscess I+D
DC cardioversion
Why Use it?
Avoid theatre
Cost saving: £614 (
$1164) for P.S. vs OT
Pain saving, anxiety-
relieving
Alternatives
Local anaesthetic direct
infiltration
Nerve blocks
Bier’s Block
GA
Text
PolicyGuidelines from collaboration of Australian and New Zealand
College of Anaesthetists (ANZCA), ACEM, etc
Levels of Sedation (ASA)
Minimal Sedation
Moderate Sedation (‘Conscious sedation’)
Deep Sedation
General Anaesthesia
Dissociative Sedation
The Ideal agent
Predictable induction and maintenance of sedation
prompt recovery
minimal recall
no complications
Often an opioid analgesic with a sedative and
amnesic agent
Options
Nitrous Oxide
Propofol
Ketamine
Midazolam
Etomidate
Opioids in combination
Combination eg Ketamine-
Propofol
Propofol
Benefits: rapid onset and recovery
Onset: 30-60sec; Peak 60-120sec, Duration 3-10min
Contraindication: allergy to egg and soy
Caution:haemodynamically unstable, elderly
SEs: hypotension, bradycardia, resp depression, pain on
infusion
No analgesic properties: give with an opioid
Dose: 0.5-2mg/kg
Midazolam
Anxiolytic, sedative, amnesic. No analgesia
Reversible
onset 1-5min, peak 10-15min, duration 1-2.5hrs
SEs: hypotension, resp depression, paradoxical reaction
Dose: 0.025-0.05mg/kg titrated to 0.4mg/kg max
caution: avoid alcohol and mental-alert activities for
24hrs
Nitrous Oxide
Inhalational: amnesia, sedation, analgesia
Fast induction
Contraindication: pneumothorax, bowel obstruction
Caution: diffusion hypoxia: O2 for 20min after
SEs: vomiting
Dose: mask inhalation: 30-70%, safety valve, if pt overly
sedated, mouth piece falls

Ketamine
Dissociative Anaesthetic
IV: Onset 1-2min, peak 2-3min, duration 5-15min
Benefits: Increase HR and BP, maintain airway reflexes, bronchodilator
SEs: laryngospasm, emergence reactions, oral secretions, reduce seizure
threshold, vomiting, resp depression, ???raised ICP
Good for children more than adults
Contraindications: schizophrenia, raised IOP, (URTIs)
Warn parents re stare; pleasant dreams!, room quiet
Dose: 0.5-1.5mg/kg IV, 2-4mg/kg IM
Etomidate
Acts on GABA receptor
onset 20-60sec, peak 1min, duration 3-8min
limited effects on cardiovascular function
good for altered myocardial contractility and raised ICP
SEs: n+v, pain at injection site, myoclonus, adrenocortical
suppression?
Dose: 0.1-0.15mg/kg
Opioids
Morphine 0.05-0.1mg/kg every 5-15min
onset 1-2.5min, peak 10-20min, duration 1-4hrs
SEs: n+v, dizziness, injection site pain, agitation, flushing,
paraesthesia
Fentanyl 1-2mcg/kg
onset immediate, peak 1-3min, duration 30-60min
SEs: resp depression, rigidity (rapid IV), brady and
hypotension, dizzy, n+v, diaphoresis
Ketofol
Ketamine - emergence reactions in adults, emesis
Propofol - hypotension and respiratory depression
combination to give sedation that is closer to ideal,
avoid opioid use with propofol
RCTs suggest ketofol no better than propofol
Australia
EMA - Procedural Sedation Practices - 2011
Propofol used in 2/3 cases (adults 94%)
65% ketamine use was in children
Half of pts did not have pre-procedural analgesia:
oligoanalgesia is an issue
Morphine:Fentanyl 4:1
Methods
Assessment
Preparation
Procedure
Aftercare
Assessment
Patient: HPC, PMHx, DHx, Allergies, prev anaesthetics, loose teeth,
exercise tolerance, LMP
Fasting status
Airway grade: Mallampati score
CVS/Resp exam
Review results
Department Status
Consent
Cautions
elderly, children <2yr
heart, lung, Cerebrovascular, renal, liver disease
morbid obesity, OSA, difficult AW
cardiovascular compromise, severe anaemia
potential for aspiration e.g. Pregnant
anaesthetic adverse events previously
ASA grades P4-5
Preparation
At least 3 appropriately trained staff (1 for drugs and AW, 1 proceduralist,
assistant) (AW, ALS competent)
Procedure Room appropriate, lighting
oxygen (FM, NC)
BMV apparatus, airways, intubation equip, suction
crash cart, defibrillator
medications, emergency drugs
monitoring (cardiac, pulse oximeter, capnography, BP)
Emergency Plan
Procedure
IVC, positioning
Pre-oxygenation
Baseline observations
Medications
Monitoring, depth of
sedation
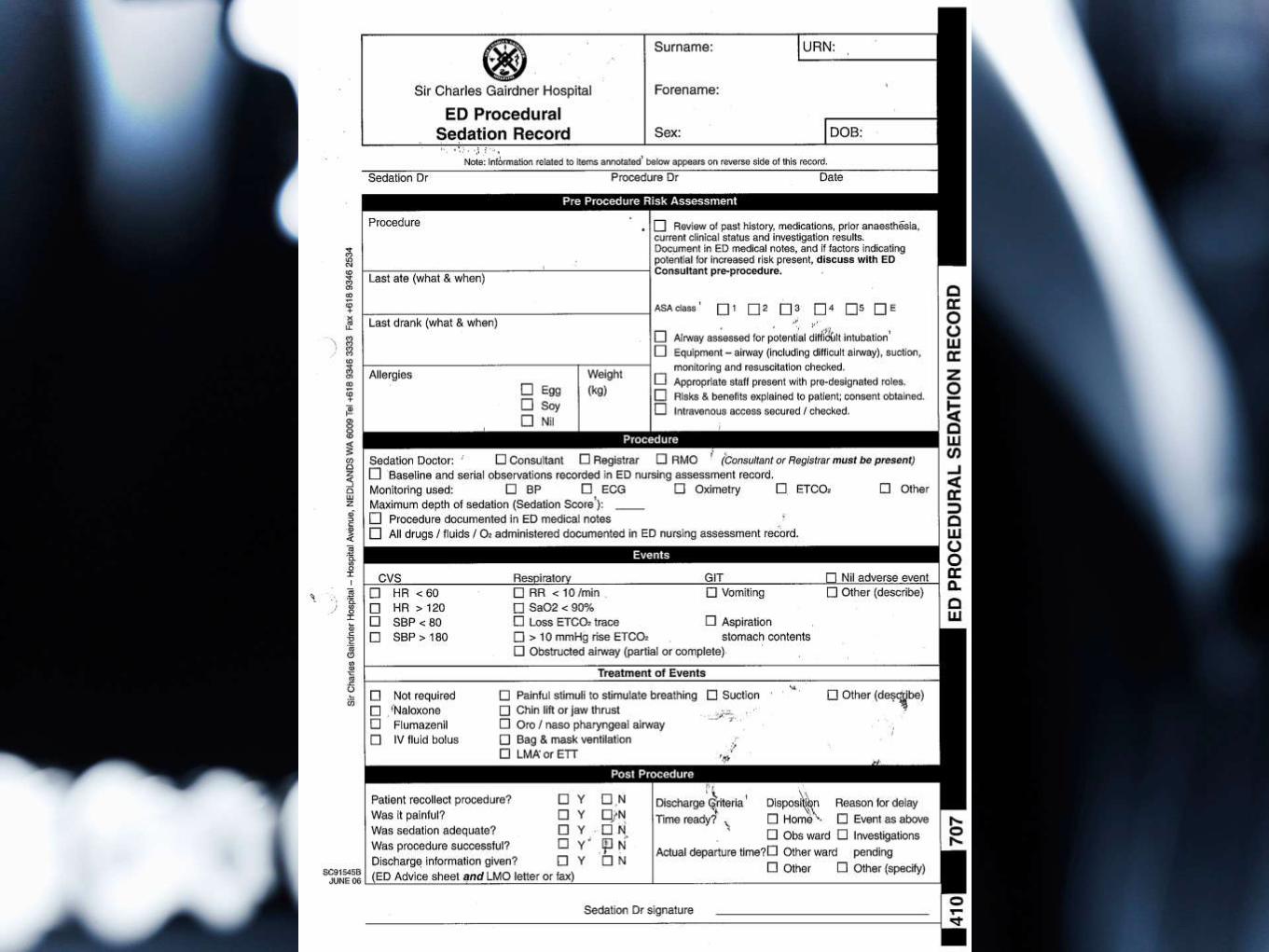
Aftercare
Documentation: drugs, IVF, monitoring, rescue
interventions, complications
Recovery: Doc present until spont respiration, stable vitals,
protective reflexes, sedation level 2
Further recovery: fully awake, obs, pain, dressing,
mobilising, E+D, voided
discharge to responsible adult
advice: E+D, analgesia, driving/machinery/decisions
Complications
Sedation related events common: 1 in 5
Vomiting, aspiration, hypo/hypertension,
brady/tachycardia, hypoventilation, desaturation,
obstructed airway
Adverse outcomes rare
Higher risk (resp): age, level of sedation, premed,
sedation drug (person in charge)
Managing Complications
Resp Depression: stimulation, airway manoeuvres, BMV, Airways
Hypotension: IVF, elevate legs, metaraminol
Laryngospasm: 100% O2 with mask, tight seal, closed expiratory valve ->
positive pressure
manually ventilate
Break laryngospasm - Larson’s point
Deepening sedation - propofol
suxamethonium IV or IM
Intubate
Controversies
Fasting status? 2+6 or no evidence of decreased aspiration?
Capnography? prevent hypoxia but no difference in outcome
How many doctors? 1 or 2?
Supplemental Opioids? Respiratory depression vs catecholamine
surge
Nasal NIV?? - AJEM 2015
Conclusion
Essential skill for ED
trainees
Know of policies and
departmental
credentialing
Choose your patient
Anticipate complications
ReferencesAustralian and New Zealand College of Anaesthetists (ANZCA) (2014) Guidelines on Sedation and/or Analgesia for Diagnostic and
Interventional Medical, Dental or Surgical Procedures. [Online]. Available at: http://www.anzca.edu.au/resources/professional-
documents/pdfs/ps09-2014-guidelines-on-sedation-and-or-analgesia-for-diagnostic-and-interventional-medical-dental-or-surgical-
procedures.pdf (Accessed: 24/3/15).
Bell A, Taylor DM et al. (2011) 'Procedural sedation practices in Australian Emergency Departments', Emergency Medicine
Australasia, 23, pp. 458-465.
Godwin SA, Burton JH et al. (2014) 'Clinical Policy: Procedural Sedation and Analgesia in the Emergency Department', Annals of
Emergency Medicine, 63, pp. 247-258.
Boyle A, Dixon V et al. (2010) 'Sedation of children in the emergency department for short painful procedures compared with
theatre, how much does it save? Economic evaluation', Emergency Medicine Journal, 28, pp. 383-386.
Andolfatto G, Abu-Laban RB et al (2012) 'Ketamine-Propofol Combination (Ketofol) Versus Propofol Alone for Emergency
Department Procedural Sedation and Analgesia: A Randomized Double-Blind Trial', Annals of Emergency Medicine, 59(6), pp. 504-
512.
Miner JR, Moore JC et al (2013) 'Randomized Clinical Trial of the Effect of Supplemental Opioids in Procedural Sedation with
Propofol on Serum Catecholamines', Academic Emergency Medicine, 20(4), pp. 330-337.
Strayer RJ, Caputo ND (2015) 'Noninvasive ventilation during procedural sedation in the ED: a case series', American Journal of
Emergency Medicine, 33, pp. 116-120.
Taylor DM, Bell A et al. (2011) 'Risk factors for sedation-related events during procedural sedation in the emergency department',
Emergency Medicine Australasia , 23(), pp. 466-473.