premature ovarian insufficiency eshre guidelines, 2015
TRANSCRIPT

PREMATURE
OVARIAN INSUFFICIENCY
ESHRE Guidelines,
2015
Aboubakr Elnashar
Benha university,
Egypt ABOUBAKR ELNASHAR

CONTENTS
1.DEFINITION
2.PREVALENCE
3.CAUSES
4.DIAGNOSIS
5.MANAGEMENT OF SEQUALAE
5
ABOUBAKR ELNASHAR

1. DEFINITION
Terminology:
“Premature ovarian insufficiency” should be used to more effectively reflect its heterogeneous nature.19b
ABOUBAKR ELNASHAR

Define
Clinical syndrome
Depletion of follicular activity before the age of 40.
Characterized by:
1. Menstrual disturbance
amenorrhea or
oligomenorrhea
2. Raised gonadotropins
3. Low E2
ABOUBAKR ELNASHAR
2. PREVALENCE
In the general population
1%.
Ethnicity may affect the prevalence.
To reduce the incidence {long-term health consequences } • gynaecological surgical practice • lifestyle – smoking • modified tt for malignant and chronic diseases.
ABOUBAKR ELNASHAR

Cigarette smoking and POI
No causal relation
There is a relation to early menopause.
: women who are prone to POI should be advised
to stop smoking.
ABOUBAKR ELNASHAR

Relatives of women with POI
Relatives of women with the fragile-X premutation
should be offered genetic counseling.
ABOUBAKR ELNASHAR

Relatives of women with non-iatrogenic POI
•No proven predictive test to identify women that
will develop POI
•No established POI preventing measures
•Potential benefit of fertility preservation: unclear
•Potential risk of earlier menopause should be
taken into account when planning a family.
ABOUBAKR ELNASHAR

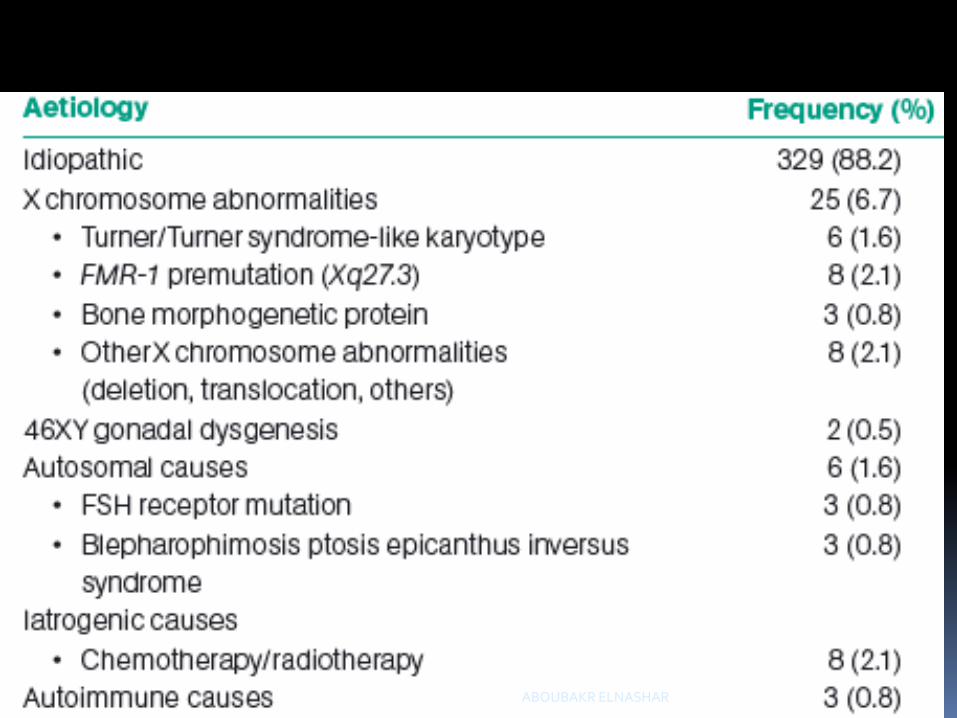
3. CAUSES
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

Aetiology of premature ovarian failure cases managed at the West London Menopause and PMS 387 Centre, London, UK (Maclaran and Panay, 2011 ).
ABOUBAKR ELNASHAR

4. DIAGNOSIS
Symptoms
strogen deficiency
below the age of 40 ys.
with oligomenorrhea or amenorrhea
ABOUBAKR ELNASHAR

Investigations for diagnosis
1. Cycle irregularly for at least
4 months +
Oligo/amenorrhea:
2. An elevated FSH level
> 25 IU/l on 2 occasions > 4
weeks apart.
ABOUBAKR ELNASHAR

Investigations for causes
1. Chromosomal analysis should be performed in
all.
{Gonadectomy should be recommended for all
women with detectable Y chromosomal
material}.
Fragile-X premutation testing is indicated.
The implications of the fragile-X premutation
should be discussed before the test is
performed. Permission from the patient to perform the test
Autosomal genetic testing is not indicated,
unless there is evidence suggesting a specific
mutation (e.g. BPES). ABOUBAKR ELNASHAR

Fragile-X testing is indicated in all women with POI, {1. establish the causation of POI
2. it has major implications for herself and her family}.
1. Family members ±carriers: developing POI and
a risk of having (grand)children with fragile-X
syndrome.
2. Patient: risk of fragile-X-associated
tremor/ataxia syndrome (FXTAS), a late onset
neurological problem
ABOUBAKR ELNASHAR
2. Screening for 21OH-Ab (or alternatively
adrenocortical antibodies (ACA))
{if +ve: an endocrinologist for testing of adrenal
function and to rule out Addison’s disease}.
ABOUBAKR ELNASHAR

3. Screening for thyroid (TPO-Ab) antibodies.
{if positive: TSH should be measured /y}.
If 21OH-Ab/ACA and TPO-Ab are negative:
No indication for re-testing later in life, unless signs
or symptoms of these endocrine diseases develop.
ABOUBAKR ELNASHAR

Routine screening for diabetes
insufficient evidence
Infection screening
No indication
Unexplained or idiopathic POI.
In a significant number of women with POI
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

5. MANAGEMENT OF SEQUELAE 1. REDUCED LIFE EXPECTANCY
2. SMALL CHANCE OF SPONTANEOUS PREGNANCY.
3. OBSTETRIC RISKS
4. REDUCED BMD
5. INCREASED RISK OF CVD
6. PSYCHOLOGICAL WELLBEING / QUALITY OF LIFE
7. SEXUAL DYSFUNCTION
8. GENITO-URINARY SYMPTOMS
9. DETRIMENTAL EFFECT ON NEUROLOGICAL
FUNCTION
10. VASOMOTOR SYMPTOMS
ABOUBAKR ELNASHAR

1. REDUCED LIFE EXPECTANCY
{CVD}.
Advise to reduce CVD risk factors
not smoking
Regular exercise
Maintaining a healthy weight.
ABOUBAKR ELNASHAR

2. SMALL CHANCE OF SPONTANEOUS
PREGNANCY.
Women with POI should be advised to use
contraception if they wish to avoid pregnancy.
ABOUBAKR ELNASHAR

Fertility interventions
No interventions that have been reliably shown to
increase ovarian activity and natural conception
rates.
Oocyte donation is an established option for
fertility.
oocyte donation from sisters has a higher rate of cycle cancellation. In women with established POI, the opportunity for fertility preservation is missed.
ABOUBAKR ELNASHAR

3. OBSTETRIC RISKS
idiopathic POI or most forms of chemotherapy:
No higher obstetric or neonatal risk than in the
general population.
Radiation to the uterus:
high risk of obstetric complications: should be
managed in an appropriate obstetric unit.
Turner Syndrome
very high risk of obstetric complications: should be
managed in an appropriate obstetric unit with
cardiologist.
ABOUBAKR ELNASHAR

Oocyte donation pregnancies high risk: should be managed in an appropriate obstetric unit. Antenatal aneuploidy screening should be based on the age of the oocyte donor. A cardiologist should be involved in care of pregnant women who have received anthracyclines and/or cardiac irradiation.
ABOUBAKR ELNASHAR

Assessment for fitness for pregnancy
Women presenting for oocyte donation who are suspected of having POI should be fully investigated prior to oocyte donation thyroid and adrenal function as well as karyotype. Pregnancy in some women can be of such high risk that clinicians may consider oocyte donation to be life threatening and therefore inappropriate
ABOUBAKR ELNASHAR

Women previously exposed to anthracyclines,
high dose cyclophosphamide or mediastinal
irradiation
ECG prior to pregnancy.
Those who are identified to have impaired
cardiac function or structural abnormalities should
be referred to a cardiologist.
ABOUBAKR ELNASHAR

Women with Turner Syndrome
cardiologist with a specialist interest in adult
congenital heart diseas
general medical and endocrine examination.
Women with POI
blood pressure
renal function
thyroid function assessed prior to pregnancy.
ABOUBAKR ELNASHAR

4. REDUCED BMD
Particularly in the early years after onset.
An increased risk of fracture later in life
ABOUBAKR ELNASHAR

Bone protection and improvement
1. Healthy lifestyle:
weight-bearing exercise
avoidance of smoking
maintenance of normal body weight
2. A balanced diet will contain the recommended
intake of calcium and vitamin D.
3. Dietary supplementation
in women with inadequate vitamin D status and/or calcium intake, and may be of value in women with low BMD.
ABOUBAKR ELNASHAR

4. Estrogen replacement
{maintain bone health: prevent osteoporosis: reduce
the risk of fracture}.
5. Other pharmacological tts
Bisphosphonates, should only be considered with
advice from an osteoporosis specialist.
Particular caution applies to women desiring pregnancy.
ABOUBAKR ELNASHAR

Monitoring bone in women with POI
Measurement of BMD at initial diagnosis
DEXA should be performed where there are additional risk factors but
may not be of value in all women with a new diagnosis of POI where
estrogen replacement is initiated early.
Repeated measurement of BMD If BMD is normal and adequate systemic estrogen replacement is commenced, the value of repeated DEXA scan is low.
ABOUBAKR ELNASHAR

If a diagnosis of osteoporosis is made and estrogen replacement or other therapy initiated, BMD measurement should be repeated after 5 years. A decrease in BMD should prompt review of estrogen replacement therapy and of other potential factors. Review by a specialist in osteoporosis may be appropriate.
ABOUBAKR ELNASHAR

5. INCREASED RISK OF CVD
Behavioural change to decrease risk:
stopping smoking
regular weight-bearing exercise
healthy weight
Turner Syndrome:
cardiologist with expertise in congenital heart
disease
ABOUBAKR ELNASHAR
Is estrogen replacement cardio-protective?
HRT
with early initiation is strongly recommended in
POI to control future risk of CVD
should be continued at least until the estimated
normal age of menopause.
ABOUBAKR ELNASHAR

Cardiovascular risk factors to be screened in women
with POI or Turner Syndrome (Bondy and Turner Syndrome Study Group, 2007; Turtle, et al., 2013).
ABOUBAKR ELNASHAR

6. PSYCHOLOGICAL WELLBEING / QUALITY OF
LIFE
Psychological support
Psychological and lifestyle interventions
ABOUBAKR ELNASHAR

7. SEXUAL DYSFUNCTION
Routinely inquire about sexual function
Management of sexual dysfunction
Estrogen replacement:
normalising sexual function.
Local estrogen:
to treat dyspareunia.
Testosterone:
some women with POI and sexual dysfunction
but long-term efficacy and safety are unknown.
Lubricants:
vaginal discomfort
dyspareunia for women not using HRT.
ABOUBAKR ELNASHAR

8. GENITO-URINARY SYMPTOMS
Treatment
Local estrogens
effective
may be given in addition to systemic HRT.
ABOUBAKR ELNASHAR

9. DETRIMENTAL EFFECT ON NEUROLOGICAL
FUNCTION
on cognition should be discussed when planning hysterectomy and/or
oophorectomy under the age of 50 years, especially for prophylactic reasons. Management
Estrogen replacement:
reduce the possible risk of cognitive impairment
For at least up to the age of natural menopause.
ABOUBAKR ELNASHAR

10. VASOMOTOR SYMPTOMS
lifestyle measures
Exercise
cessation of smoking
maintaining a healthy weight to reduce possible
risks for cognitive impairment
HRT
for the tt of VMS.
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

Risks of HRT
No increase risk of breast cancer before the age of
natural menopause.
An intact uterus:
progestogen in combination with estrogen therapy
{endometrial protection}
ABOUBAKR ELNASHAR

HRT
17-β estradiol
preferred to EE or conjugated equine estrogens.
Synthetic progestogens
preferred, until safety data on the ability of
micronized progestogens to adequately protect the
endometrium from the mitogenic effects of estrogen.
Route:
According to patient preference
ABOUBAKR ELNASHAR

Monitoring
Clinical review annually
Routine monitoring tests
Not required
±if specific symptoms or concerns.
Turner Syndrome:
HRT throughout the normal reproductive lifespan
ABOUBAKR ELNASHAR

Contraindications
Breast cancer survivors. BRCA gene mutation or
after breast cancer
ABOUBAKR ELNASHAR

Not contraindication
1. women carrying BRCA1/2 mutations but without
personal history of breast cancer after
prophylactic BSO.
2. Surgically induced menopause because of
endometriosis:
E/P or tibolone
at least up to the age of natural menopause
3. Post-menopausal women after hysterectomy and
with a history of endometriosis:
Avoid unopposed E. However, the theoretical benefit of avoiding disease reactivation and malignant transformation of residual disease should be balanced against
the increased systemic risks associated with combined E/P or tibolone.
ABOUBAKR ELNASHAR

4. Migraine:
changing dose, route of administration or regimen
if migraine worsens during HRT.
5. Hypertension
transdermal E2 is the preferred method of delivery
6. History of prior VTE
haematologist prior to commencing HRT.
Transdermal E2 is the preferred route
7. Obesity or overweight:
Transdermal E2 is the preferred method
8. Fibroids
ABOUBAKR ELNASHAR

Androgen
supported by limited data
long-term health effects are not clear yet.
evaluated after 3-6 months
should be limited to 24 months.
ABOUBAKR ELNASHAR

Induction of Puberty:
17β-estradiol
starting with low dose at the age of 12 with a
gradual increase over 2 to 3 years. In cases of late diagnosis and for those girls in whom growth is not a concern, a modified regimen of E2 can be considered.
Transdermal E2
: more physiological estrogen levels: preferred.
COC:
contra-indicated for puberty induction.
Cyclical progestogens
Start after at least 2 years of estrogen or when
breakthrough bleeding occurs.
ABOUBAKR ELNASHAR

Estrogen substitution therapy in adolescence (Bondy and Turner Syndrome Study Group, 2007)
ABOUBAKR ELNASHAR

263 lectures
1. My scientific
page on face
book: 3622
members
2. Slide share: 1259
followers
ABOUBAKR ELNASHAR