preimplantation genetic diagnosis pgd
DESCRIPTION
Preimplantation genetic diagnosis PGD. Maha M. El- hallaq Master of Biotechnology. Tube Babies. 1_ Intra - vaginal Culture. - PowerPoint PPT PresentationTRANSCRIPT

Preimplantation genetic diagnosis
PGD
Maha M. El-hallaqMaster of Biotechnology
Tube Babies
1_ Intra - vaginal Culture
• Summed up this way that after collecting the eggs are placed with sperm in a tube containing a special material for the growth of embryos Culture Media, then this tube is placed in the vagina and hold it in place by a special payment. Still repayment and the tube from the vagina after 24-48 hours, and examine the components inside the tube to make sure conceive. The fertilized embryo is transferred to the uterus.
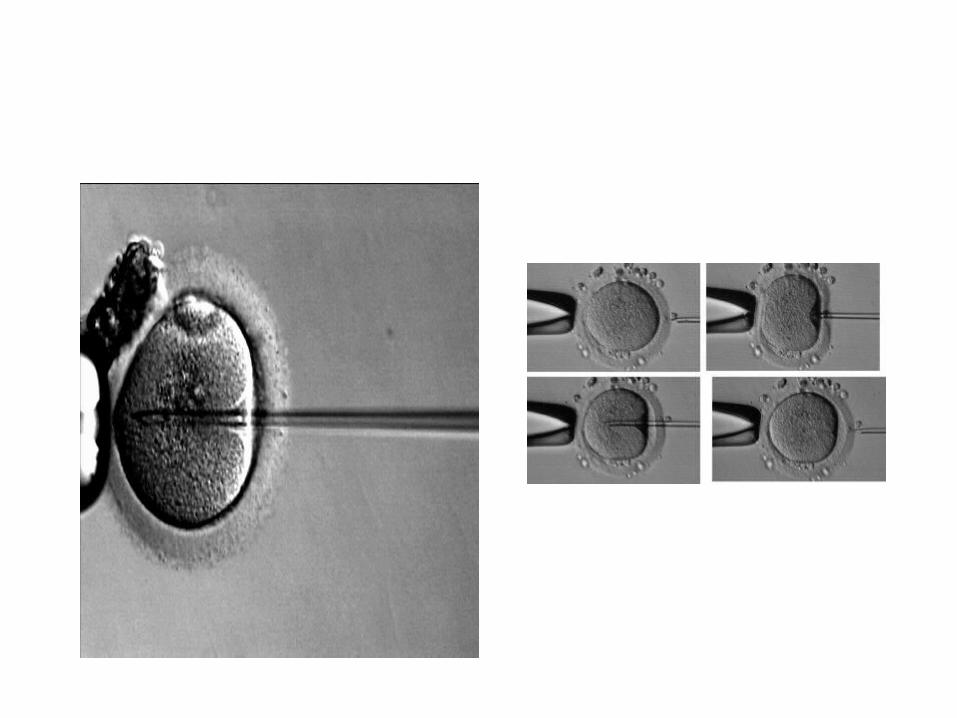
2_Intra cytoplasmic sperm injectionICSI
• This method is ideal and favorite now a very successful especially for men who complain of the lack of sperm significantly. As well as when the type of sperm is good. The main enter the sperm directly into the cytoplasm of the cell and using sperm and only one other than the way IVF that are put thousands of sperm on the egg and are in this way injection egg after removing cells prosecution her fine needle very inject sperm into the egg any inside cytoplasm.
Used in:
When there are too few sperm in the semen. When fertilization fails in a way that IVF. when the movement of sperm is weak . Statistics have shown that the rate of cases in which
they conducted the operation successfully about 70% as statistics have shown that the eggs fertilized in this way and transferred to the mother be a success rate of live births in the same way IVF rate and possibly more in some .
3_ In Vitro FertilizationIVF
• Is to fertilize the egg with sperm in a test tube after taking mature eggs from the ovary to be placed with good sperm only after fertilization until it gets washed. The fertilized egg then returned (embryos) to the mother. This process takes from two - five days and this method gives the best option to choose the best embryos to be transferred to the mother after fertilized outside the womb.
Who are the right couples are treated in a manner IVF ??
Wife is capable of producing eggs and the pair product of sperm.
Women who are Fallopian tubes have closed or damaged so as not to allow the sperm to reach the egg fertilized.
The men who are infertile due to a lack of or low sperm movement .
Women between 35-40 years to be able to get a child where the probationary period in front of them short-term.
Cases of infertility is not known why. Men who have generated antibodies to the sperm
“Anti-sperm Antibody”. When one of the parents are carriers of a genetically
transmitted disease .
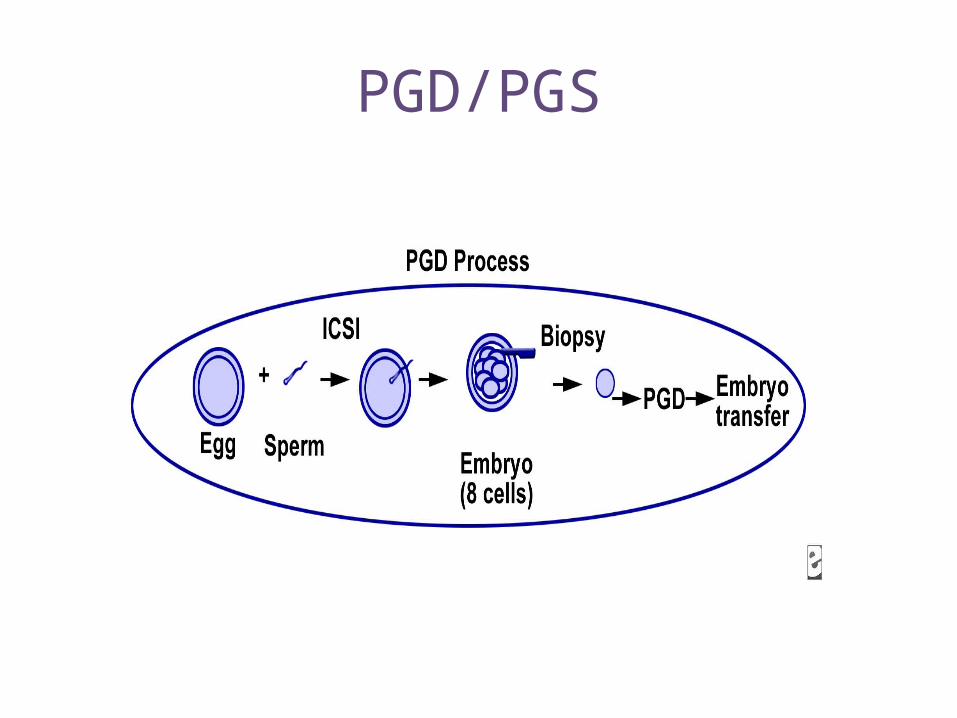
PGD/PGS
Preimplantation genetic diagnosis (PGD)
It is the beginning of the end of genetic disease… Dr. Perry Phillips
PGD
• Preimplantation genetic diagnosis is a technique used to identify genetic defects in embryos created through in vitro fertilization (IVF) before pregnancy.
• (PGD) refers specifically to when one or both genetic parents has a known genetic abnormality and testing is performed on an embryo to determine if it also carries a genetic abnormality.
History
• Edwards and Gardner successfully performed the first known embryo biopsy on rabbit embryos in 1968. In humans, PGD was developed in the United Kingdom in the mid 1980s as an alternative to current prenatal diagnoses.Initially, PGD revolved around determination of gender as an indirect means of avoiding an X-linked disorder. In 1989 in London, Handyside and colleagues reported the first unaffected child born following PGD performed for an X-linked disorder.
• As of 2006, more than 15,000 PGD cycles have been reported. PGD is currently available for most known genetic mutations.
Primary candidates for PGD
• Couples with a family history of X-linked disorders (Couples with a family history of X-linked disease have a 25% risk of having an affected embryo [half of male embryos].)
• Couples with chromosome translocations, which can cause implantation failure, recurrent pregnancy loss, or mental or physical problems in offspring
• Carriers of autosomal recessive diseases (For carriers of autosomal recessive diseases, the risk an embryo may be affected is 25%.)
• Carriers of autosomal dominant diseases (For carriers of autosomal dominant disease, the risk an embryo may be affected is 50%.)
Advantages for the Procedure
• The Pre-Implantation Genetic Diagnosis technique is performed before pregnancy begins. This avoids "the stress, emotional trauma and subsequent moral dilemma" of amniocentesis.
• Some adults who know that they are carriers of a genetically transmitted disease decide to not have children. The Pre-Implantation Genetic Diagnosis procedure allows them to have a healthy child with full assurance that it would not be carrying that disease
• If the procedure became widespread, the incidence of many diseases and a great deal of human suffering would be reduced. Many genetic diseases cause a great deal of suffering in children and enormous family stress.
Conditions diagnosed using PGD
• PGD should be offered for 3 major groups of disease:
• (1) sex-linked disorders• (2) single gene defects• (3) chromosomal disorders
* Sex-linked disorders
• X-linked diseases are passed to the child through a mother who is a carrier or affected fathers .
• Sex-linked recessive disorders include hemophilia, fragile X syndrome, most neuromuscular dystrophies (currently, >900 neuromuscular dystrophies are known), and hundreds of other diseases. Sex-linked dominant disorders include Rett syndrom, incontinentia pigmenti, pseudohyperparathyroidism, and vitamin D–resistant rickets.
**Single gene defects
• PGD is used to identify single gene defects such as cystic fibrosis, Tay-Sachs disease, sickle cell anemia, and Huntington disease. Although progress has been made, some single gene defects, such as cystic fibrosis, have multiple known mutations. In cystic fibrosis, only 25 mutations are currently routinely tested. Because most of these rare mutations are not routinely tested, a parent without any clinical manifestations of cystic fibrosis could still be a carrier. This allows the possibility for a parent carrying a rare mutation gene to be tested as negative but still have the ability to pass on the mutant cystic fibrosis gene.
• PGD can also be used to identify genetic mutations like BRCA -1, which does not cause a specific disease but increases the risk of a set of diseases.
***Chromosomal disorders
• The last group includes chromosomal disorders in which a variety of chromosomal rearrangements, including translocations, inversions, and deletions, can be detected using fluorescent in situ hybridization (FISH). FISH uses telomeric probes specific to the loci site of interest. Some parents may have never achieved a viable pregnancy without using PGD because previous conceptions resulted in chromosomally unbalanced embryos and were spontaneously miscarried.
What Are The Concerns Of PGD?
The following are considered concerns or disadvantages associated with the use of PGD:
• Many people believe that because life begins at conception and that the destruction of an embryo is the destruction of a person. In practice, the PGD procedure usually results in a small number of discarded embryos.
• While PGD helps reduce the chance of conceiving a child with a genetic factor, it can not completely eliminate this risk. In some cases, further testing done during pregnancy is needed to ascertain if a genetic factor is still possible.
• Although genetically present, some resulting diseases only generate symptoms when carriers reach middle age.
preimplantation genetic screening (PGS)
Preimplantation genetic screening (PGS) refers to
techniques where embryos from presumed chromosomally normal genetic parents are screened for aneuploidy.
Indications for Preimplantation Genetic Screening
• Most early pregnancy losses can be attributed to aneuploidy. • Women of advanced maternal age• Couples with history of recurrent pregnancy loss• Couples with repeated IVF failure These patient populations are at risk of failure with IVF because
of a high proportion of aneuploid embryos. PGD is believed to decrease this risk by selecting chromosomally normal embryos that have a higher chance of implantation.

How Is The PGD/PGS Performed?
How Is The PGD/PGS Performed?
1_ Ovarian stimulation is needed in order to produce multiple eggs. During the 8- to 14-day hormonal stimulation period, frequent ultrasonographic examinations and laboratory tests are performed to monitor the development and maturation of follicles (egg-containing ovarian cysts).
2_ The eggs are then cultured for a few hours after their retrieval to allow for final maturation to occur. For the PGD/PGS procedure at a later stage of embryonic development, intracytoplasmic sperm injection (ICSI) is preferred. In this manner, ICSI prevents the chance of polyspermy and the accidental acquisition of “extra” chromosomal material from the sperm
3_ Sperm for purposes of egg fertilization are typically obtained from the male partner by masturbation on the day of egg retrieval.
4_ The morning after ICSI, the eggs are examined for signs of fertilization, which is determined by the presence of 2 pronuclei, representing the male and female contribution to the embryo.
5_ Embryos continue to divide into multicellular entities. Three days after egg retrieval, when the embryo is normally at the 6-10 cell stage, the embryos can be prepared for a cleavage-stage biopsy. Normal development includes progression to the 2-4 cell stage two days after egg retrieval, and, after three days, usually 6-10 cells.

Biopsy Techniques
Most clinics perform a cleavage-stage embryo biopsy. However, one of the following 3 techniques can be used for PGD:
1_Polar body biopsy• Polar body biopsy works only for female chromosomal
disorders. The mature metaphase II egg extrudes a single polar body. This polar body can be removed and tested, providing information on only the chromosomal content of the egg.
• Because only information about the mother can be obtained by analyzing polar bodies, chromosomal abnormalities occurring after fertilization (when the sperm meets the egg) are not detected.
• This technique is infrequently used .
2_Cleavage-stage embryo biopsy• The most common approach for PGD/PGS is to biopsy a single
blastomere from day 3 embryos; this allows extraction of a single blastomere from a developing embryo. The removal of the blastomere is a technically challenging procedure.
• Removal of blastomere from an 8-cell embryo (cleavage-stage embryo).
• Before extracting the single cell from a 6-10 cell embryo, the embryo is incubated in calcium- and magnesium-free medium for approximately 20 minutes in order to reduce blastomere-to-blastomere adherence.

cell embryo, on Day 3 after IVF, ready to be biopsied. It is held in place on a micromanipulatorwith a holding pipette.
2. The zona drilling pipette is used to drill a hole through the shell of the embryo ( the zona) using acid Tyrode's.
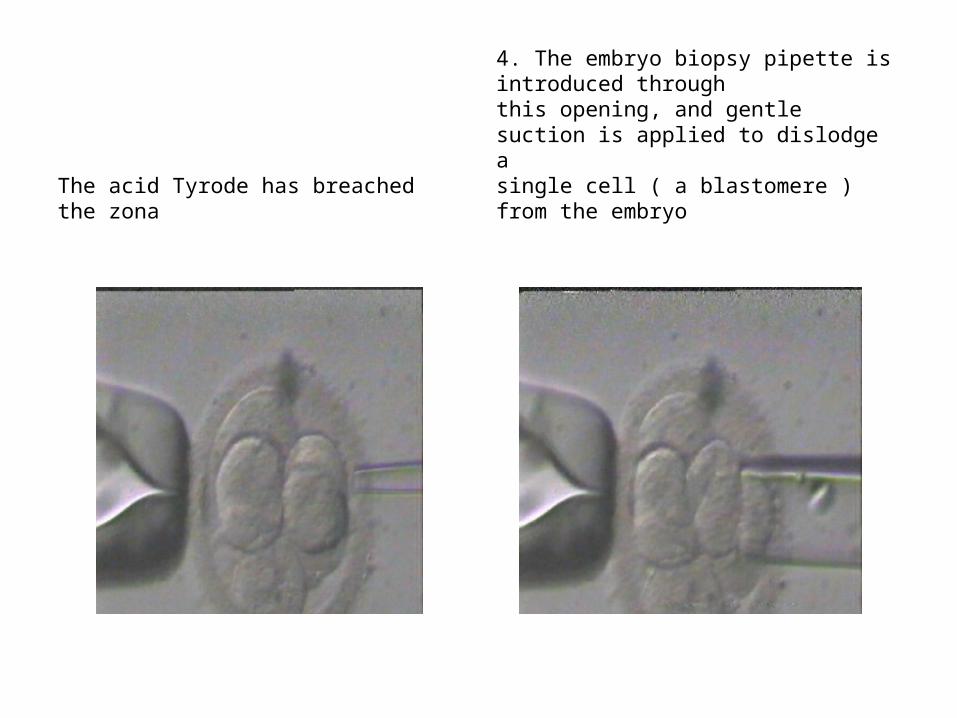
The acid Tyrode has breached the zona
4. The embryo biopsy pipette is introduced throughthis opening, and gentle suction is applied to dislodge asingle cell ( a blastomere ) from the embryo
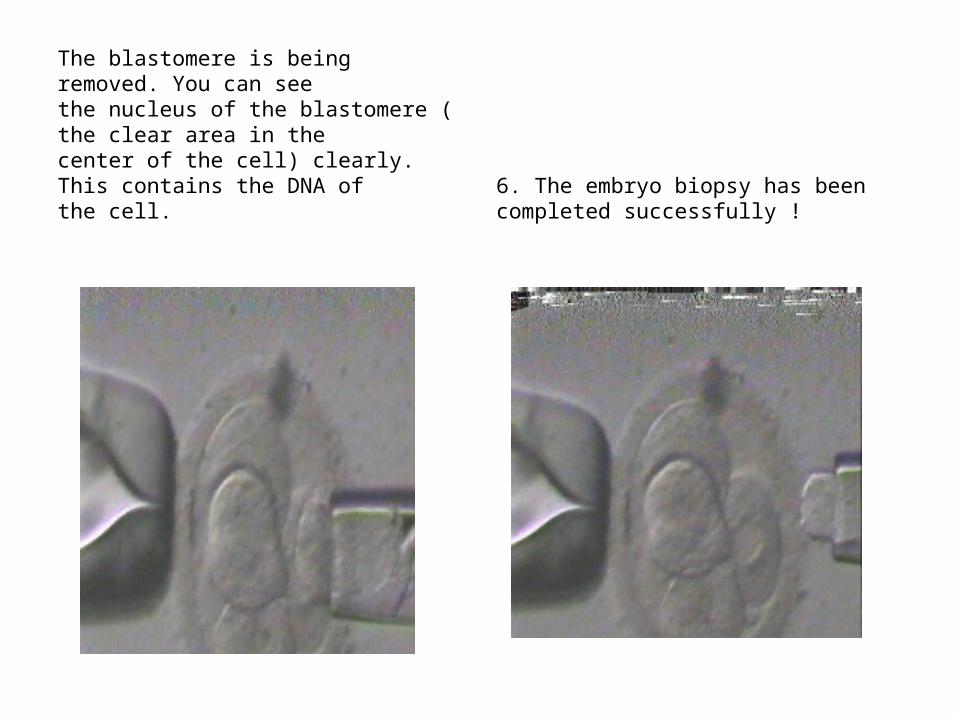
The blastomere is being removed. You can see the nucleus of the blastomere ( the clear area in thecenter of the cell) clearly. This contains the DNA ofthe cell.
6. The embryo biopsy has been completed successfully !
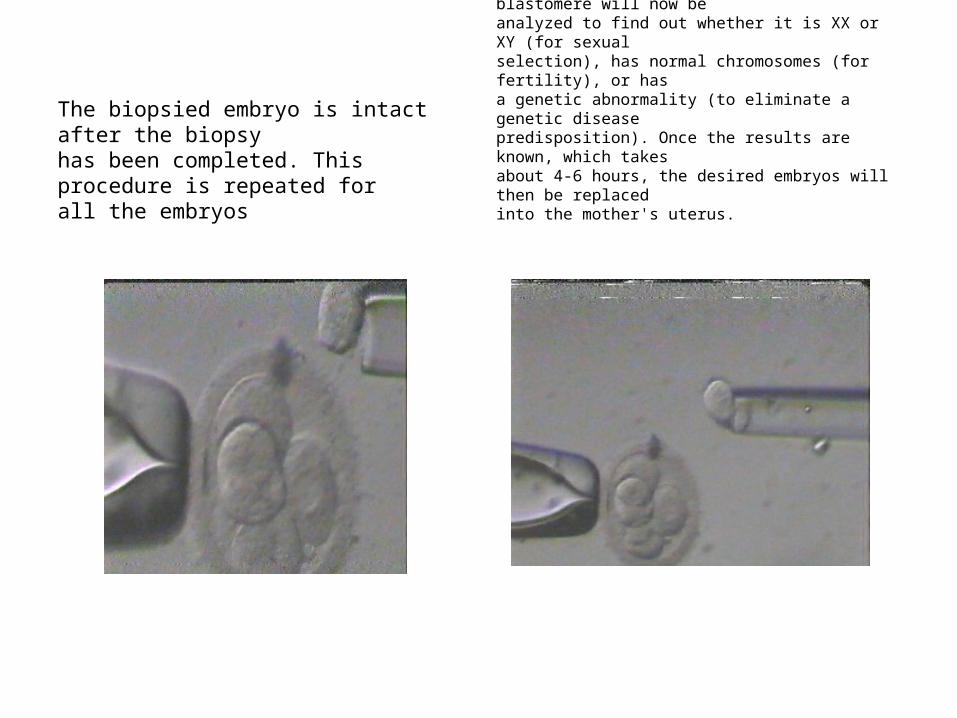
The biopsied embryo is intact after the biopsy has been completed. This procedure is repeated for all the embryos
8. The biopsied embryo is now returned to the incubator for further culture. The blastomere will now be analyzed to find out whether it is XX or XY (for sexualselection), has normal chromosomes (for fertility), or hasa genetic abnormality (to eliminate a genetic diseasepredisposition). Once the results are known, which takesabout 4-6 hours, the desired embryos will then be replacedinto the mother's uterus.
3_Blastocyst biopsy• Blastocyst formation begins on day 5 post-egg retrieval and is
defined by the presence of an inner cell mass and the outer cell mass or trophectoderm. At this stage of development, the embryo is formed of more than 100 cells. A hole is breached in the zona pellucida in a similar manner as described for a cleavage-stage embryo biopsy, and cells are removed from the trophectoderm using a fine biopsy pipette. The inner cell mass is left undisturbed.
• A limitation of this procedure is the potential acquisition of cells from the trophectoderm that are not representative of the developing embryo (inner cell mass) due to mosaicism (having multiple different types of cell lines). In addition, genetic/aneuploidy testing is completed approximately 24-48 hours of the embryo biopsy; due to the limited viability of embryos in the laboratory (≤6 d after egg retrieval), many embryos do not survive until the time of embryo transfer. Therefore, biopsied blastocysts must be frozen.
Genetic Testing
Polymerase Chain Reaction ( PCR)
Fluorescence in situ hybridization (FISH)
Polymerase chain reactionpcr
• PCR is a relatively fast and convenient way to test DNA. The method has been used in a variety of preimplantation genetic testing protocols
• Only one cell should be amplified; however, if another cell or piece of DNA enters the tube, it is also amplified. ICSI must be used to minimize this problem and to ensure that no excess sperm are present (paternal contamination) and that all the cumulus cells have been removed (maternal contamination).

• Errors in PCR can result in misdiagnoses leading to an affected embryo being transferred or the discarding of a normal embryo. One error is caused by a phenomenon known as allele dropout. This refers to the preferential amplification of one allele over another during the PCR process and is mainly a problem for PGD of dominant disorders or when 2 different mutations are carried for a recessive disorder and only one mutation is being analyzed. In autosomal dominant diseases, the risk of transferring an affected embryo is 11% and 2% for recessive disorders.
Fluorescence in situ hybridization
• FISH is used for the determination of sex for X-linked diseases, chromosomal abnormalities, and aneuploidy screening. FISH is used more commonly in PGS secondary due to its utility as an aneuploidy screen. Probes bind to a particular chromosome.
• Each probe is labeled with a different fluorescent dye. These fluorescent probes are applied to the cell biopsy sample and are expected to attach to the specific chromosomes.
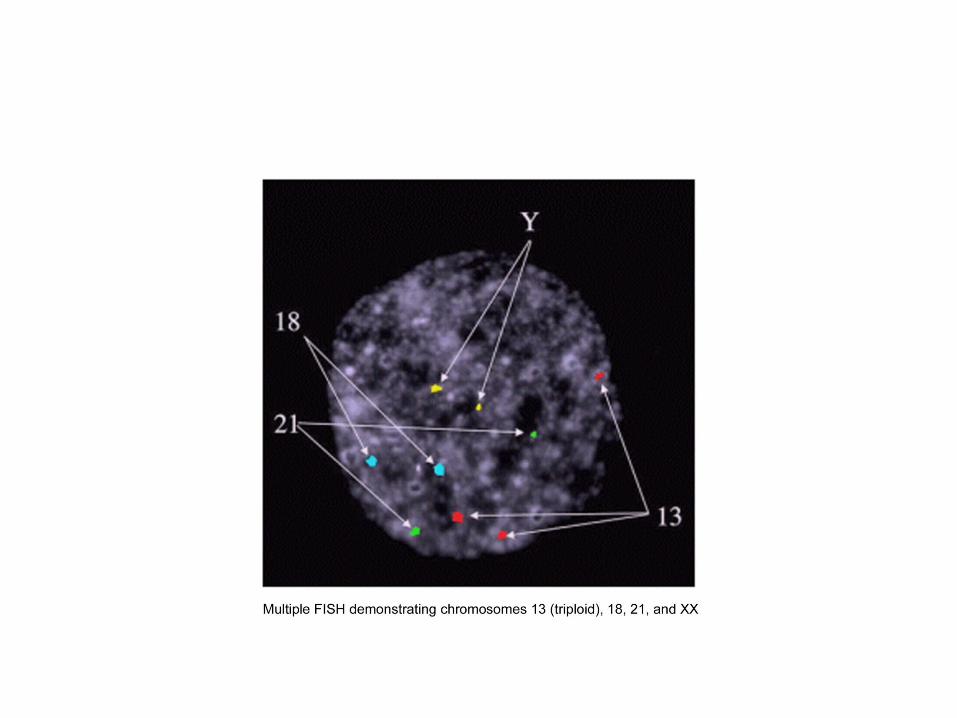
• They can be visualized under a fluorescent microscope. The number of chromosomes of each type (color) present in that cell is counted. The geneticist can thus distinguish normal cells from abnormal cells, such as those with aneuploidy
• Chromosomes that can be analyzed with FISH probes include X, Y, 1, 13, 16, 18, and 21.
A summary of PGD applications categorized by PCR or FISH
• Polymerase chain reaction categorizes the following:• Single gene defects in autosomal disease• Single gene defects in male infertility• Identification of sex in X-linked diseases• Fluorescence in situ hybridization (preferred because PCR
bears the risk of misdiagnosis caused by contamination) categorizes the following:
• Aneuploidy screening in women of advanced maternal age• Aneuploidy screening for male infertility• Identification of sex in X-linked diseases• Recurrent miscarriages caused by parental translocations
PGD/PGS IN GAZA COMUNITY

RECOMMENDATION