pregnancy and heart - bryan health · pregnancy and heart disease objectives •to recognize the...
TRANSCRIPT

9/2/2015
1
Clyde Meckel MD, FACC, FSCAI
Bryan Heart
9-5-15
Pregnancy and Heart Disease
Objectives •To recognize the physiological changes
that occur during pregnancy
•To identify risk factors for adverse
maternal and fetal outcomes
•To recognize that cardiovascular risks
extend into the postpartum period
•To manage cardiac conditions during
pregnancy
A 25 year old asymptomatic woman is referred for
evaluation of a murmur noted during the early second
trimester of pregnancy. She has no history of cardiac
disease. Physical examination confirms a pulse of 95
beats per minute, blood pressure of 110/85 mmHg, a II/VI
systolic ejection murmur at the left sternal border and an
apical S3. What is the most likely cause of this murmur?
(A) M
oder
ate ao
rtic stenos
is
(B) T
ricu
spid re
gurg
itat
ion
(C) S
ever
e pul
mona
ry stenos
is
(D) P
hysiol
ogic m
urm
ur
(E) Bicusp
id aor
tic va
lve wit...
0% 0% 0%0%0%
A. (A) Moderate aortic stenosis
B. (B) Tricuspid regurgitation
C. (C) Severe pulmonary stenosis
D. (D) Physiologic murmur
E. (E) Bicuspid aortic valve with
severe aortic stenosis

9/2/2015
2
Cardiovascular Changes in
Pregnancy
CV Exam During Pregnancy
NORMAL
•Brisk carotid upstrokes
•Mildly elevated JVP
•Systolic ejection murmur at LSB
•Mammary souffle
•S3 gallop
•Mild pedal edema
•Varicose veins
NOT NORMAL
•Lung rales
•Diastolic murmur
•Holosystolic murmur
•Fixed split S2 •S4
Changes in Existing Murmurs•Stenotic lesions will get louder due to increased
preload and cardiac output
•Regurgitant lesions will get softer due to
decreased systemic vascular resistance
•A murmur from a ventricular septal defect also
gets softer due to decreased SVR

9/2/2015
3
Hemodynamic Changes Labor &
Delivery Labor:
↑ Cardiac output
↑ Heart rate
↑ Blood pressure
↑ Venous return
↑ Circulating blood volume
with uterine contraction
Post-partum:
Autotransfusion from placenta
↑ preload and CO
Cardiac Output (L/min) Hunter S. Br Heart J 1992
Pregnancy is a Hypercoaguable
State •Many hematological changes occur
↑ Clotting factors (VII, VIII, X, vWF)
↑ Platelet adhesion
↑ PAI-1, PAI-2 (produced by placenta)
↓ Fibrinolysis (due to ↑ fibrinogen)
↓ protein S activity
Brenner B. Thrombosis Research 2004
James A. Hematology 2009
Prepregnancy Risk Assessment
Cardiovascular disease does not preclude pregnancy,
but it poses increased risk to mother and fetus
• 37% of women denied having been told they were at
increased risk of complications
• Only 50% had received contraceptive counseling
Kovacs A. J Am Coll Cardiol 2008

9/2/2015
4
Why Risk Stratification is
Important
•Increased morbidity and mortality associated with
pregnancy
•Up to 20% maternal cardiac complications in women
with congenital heart disease
•Rates of hypertensive syndromes, such as
preeclampsia, are increasing
•Deaths attributable to maternal cardiac conditions have
increased in the past decade
Berg C. J. Obstet Gynecol 2009
Maternal Cardiovascular Risk
The 8th Report of Confidential Inquiries into Maternal Deaths in the UK
Greutmann M. European Heart Journal 2012
An 22 yr old woman is referred to clinic to discuss the
option of future conception. She has a history of “heart
disease” which was surgically repaired in infancy. In
performing your evaluation, which of the following factors
poses the highest risk of maternal cardiac complications
associated with pregnancy?
A. Restrictive ventricular septal
defect
B. Left ventricular ejection
fraction of 30%
C. Moderate aortic regurgitation
w/ normal systolic function
D. Palpitations with occasional
ventricular couplets
E. Bicuspid aortic valve with
aortic stenosis and a peak
F. LVOT gradient of 25 mmHg Restrict
ive v
entr
icula
r septa
...
Left ventr
icula
r eje
ctio
n fra
c...
Modera
te a
ortic
regu
rgitati.
.
Palpita
tions
with o
ccas
ional..
.
Bicusp
id a
ortic valv
e with a
ort..
LVOT g
radie
nt of 2
5 m
mHg
17% 17% 17%17%17%17%

9/2/2015
5
Maternal Cardiac Risk Factors
• Prior cardiac event
• NYHA Class >II or cyanosis
• Left heart obstruction
• Left ventricular dysfunction
Mnemonic15 (Aortic valve area <1.5 cm2) 20 (Mitral valve area <2.0 cm2) 30 (LVOT peak grad >30 mm Hg) 40 (LVEF <40%)
Siu S. Circulation 2001
Late Cardiovascular Events
NYHA class or cyanosis
Cardiac event during pregnancy
Subaortic ventricular dysfunction
Subpulmonary ventricular dysfunction
Left heart obstruction
Balint O. Heart 2010
High Risk Patients
WHO III• Mechanical valve
• Systemic right ventricle
• Fontan circulation
• Other complex congenital heart disease
• Aortic dilation 40-45 mm in Marfan syndrome
• Aortic dilation 45-50 mm in aortic disease
associated with bicuspid aortic valve
• Pulmonary arterial hypertension of any
cause
• Severe systemic ventricular dysfunction
(NYHA III-IV)
• Previous peripartum cardiomyopathy
with any residual impairment of left
ventricular function
• Severe mitral stenosis, severe
symptomatic aortic stenosis
• Marfan syndrome with aorta dilated
>45 mm
• Aortic dilation >50 mm in aortic disease
associated with bicuspid aortic valve
• Native severe coarctation
WHO IV
(pregnancy contraindicated)
Significantly increased risk of maternal
mortality or severe morbidity
Regitz-Zagrosek V. European Heart J 2011
9/2/2015
6
A 35 yr old woman with a history of peripartum
cardiomyopathy returns 18 months following the birth of
her child. She desires a second pregnancy. She is
asymptomatic, on no medications and her
echocardiogram reveals a left ventricular ejection fraction
of 30%. What is your recommendation?
A. (A) Proceed with pregnancyB. (B) Start an ace-inhibitor and
proceed with pregnancyC. (C) Obtain a cardiac MRI and if her
EF is improved, proceed with pregnancy
D. (D) Proceed with pregnancy with echos every trimester
E. (E) Counsel against pregnancy
(A) P
roce
ed with
pre
gnan
cy
(B) S
tart an a
ce-in
hibito
r and...
(C) O
btai
n a ca
rdia
c M
RI a
nd ..
(D) P
roce
ed w
ith p
regn
ancy
...
(E) C
ounse
l aga
inst
pre
gnan
cy
0% 0% 0%0%0%
Peripartum Cardiomyopathy
• Onset of heart failure in the last month of pregnancy through
5 months postpartum
• No other etiology identified
• No prior history of heart disease
• Demonstrable impairment in left ventricular systolic function:
-Echocardiogram: LVEF <45%, SF <30%
Demakis J. Circulation 1971
Pearson G. JAMA 2000
Major cause of pregnancy related deaths in
the United States
Pathogenesis of PPCM
Silwa K. Lancet 2006
9/2/2015
7
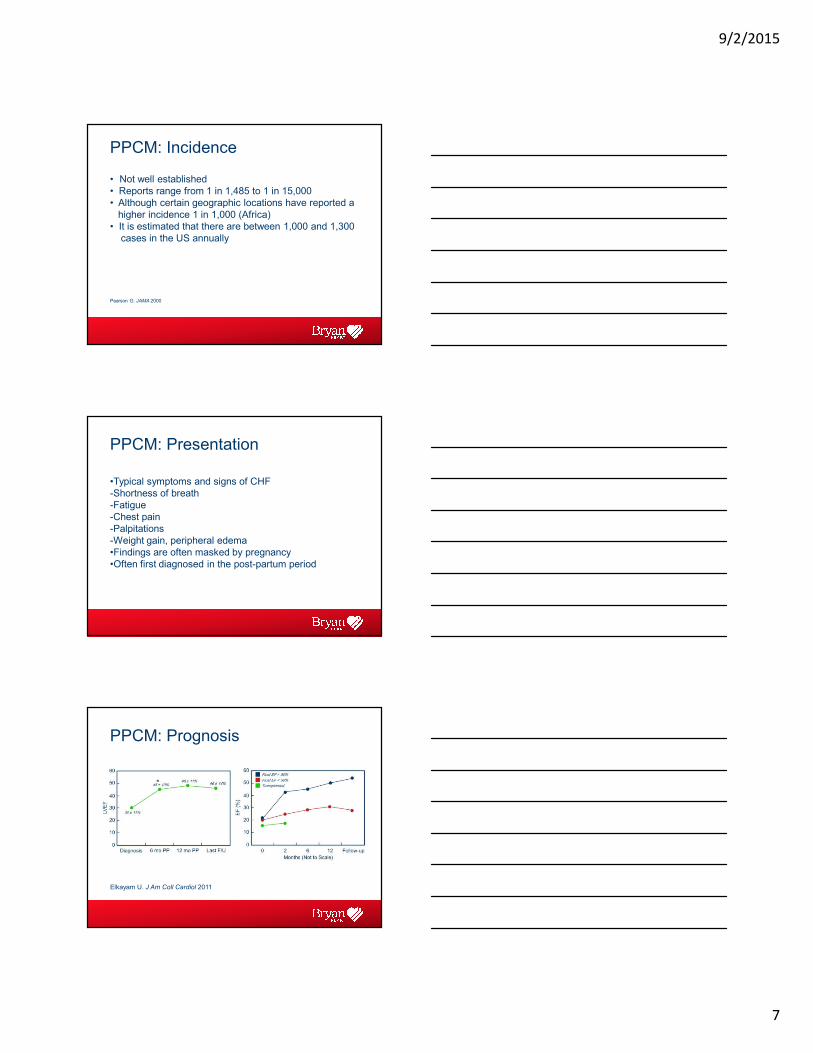
PPCM: Incidence
• Not well established
• Reports range from 1 in 1,485 to 1 in 15,000
• Although certain geographic locations have reported a
higher incidence 1 in 1,000 (Africa)
• It is estimated that there are between 1,000 and 1,300
cases in the US annually
Pearson G. JAMA 2000
PPCM: Presentation
•Typical symptoms and signs of CHF
-Shortness of breath
-Fatigue
-Chest pain
-Palpitations
-Weight gain, peripheral edema
•Findings are often masked by pregnancy
•Often first diagnosed in the post-partum period
PPCM: Prognosis
Elkayam U. J Am Coll Cardiol 2011

9/2/2015
8
Risk Factors and Management
Homans D. NEJM 1985
Elkayam U. Circulation 2005
Elkayam U. J Am Coll Cardiol 2011
Risk factors:
–Multiple gestation
–Advanced maternal age
–Pregnancy induced HTN
–Tocolytic therapy
Management:
–CHF management
–Consider anticoagulation due
to ↑ risk of thrombosis
–Deliver baby as soon as fetal
lungs are mature
Onset of PPCM:
PPCM: Recovery of LV Function
Fett J. Mayo Clin Proc 2005 Elkayam U. J Am Coll Cardiol 2011
•It is difficult to predict who will have recovery of function
•Subsequent pregnancies are associated with significant
morbidities
A 22 year old woman who is 25 weeks pregnant presents
with dizziness. On evaluation, her pulse is 150 and blood
pressure is 80/50 and an electrocardiogram confirms atrial
flutter. What is your initial management?
A. (A) Intravenous adenosine
B. (B) Intravenous beta-blocker
C. (C) Oral calcium channel
blocker
D. (D) Intravenous amiodarone
E. (E) DC cardioversion
(A) I
ntrave
nous adenosi
ne
(B) I
ntrave
nous beta
-blo
cker
(C) O
ral c
alciu
m channel b
lo...
(D) I
ntrave
nous am
iodaro
ne
(E) D
C ca
rdio
vers
ion
0% 0% 0%0%0%

9/2/2015
9
Arrhythmias
• Incidence of both atrial and
ventricular arrhythmias increase
during pregnancy
• Physiological changes in pregnancy
alter the absorption, excretion and
plasma concentration of
antiarrhythmic drugs
• All antiarrhythmic drugs are
myocardial depressants
-Use the lowest effective doses
• DC cardioversion is safe
Hypertension in Pregnancy
• Definition: SBP ≥140 mmHg or DBP ≥90 mmHg
• ~5% of women have pre-existing HTN
• ~10% develop HTN after 20 weeks gestation
• Common therapies: labetalol, methyldopa, nifedipine
-Hospitalization: SBP ≥170mmHg or DBP≥ 110mmHg
Women with hypertension during pregnancy are at increased risk for long-term vascular events
Classification of HTN• Pre-existing HTN (≈5%)
-Prior to 20 weeks gestation
• Pregnancy induced HTN (≈10%)
-Increase in systolic (≥30 mmHg) and diastolic (≥15 mmHg)
-After 20 weeks gestation & resolution by 6 weeks
postpartum
• HELLP syndrome
-Hemolytic anemia, elevated liver enzymes, low platelets
-10-20% of women with preeclampsia
-After 20 weeks gestation & resolution by 6 weeks
postpartum
• Eclampsia
-Tonic clonic seizures Seely E. N Engl J Med 2011

9/2/2015
10
Preeclampsia
• A systemic vascular disorder
• New onset of hypertension and
proteinuria during the 2nd half of
pregnancy
• Occurs in 3-5% of pregnancies
• Sustained systolic or diastolic
blood pressure ≥140 or ≥90
mmHg, respectively, with
concurrent proteinuria ≥ 0.3 grams
in 24 hrs
Cardiac Output (L/min)
Powe C. Circulation 2011
A 21 year old woman with Marfan syndrome and an aortic
root of 4.8 cm presents in the 2nd trimester of pregnancy.
You counsel her that:
A. (A) She should start a beta-blocker, be followed closely for strict BP control and monthly echocardiograms
B. (B) She is not at an increased risk for aortic complications following pregnancy
C. (C) Future pregnancies should be avoided due to the risk of aortic dissection
D. (D) An ace-inhibitor should be started immediately, as she is beyond the 1st trimester
E. (E) The chance that her child will have Marfan syndrome is <50%
(A) S
he should
start
a b
eta-b
...
(B) S
he is n
ot at a
n incr
eased ..
.
(C) F
uture
pre
gnanci
es shou..
(D) A
n ace
-inhib
itor s
hould b
...
(E) T
he ch
ance
that h
er child
...
0% 0% 0%0%0%
Connective Tissue Disorders
Pregnancy increases the risk of long-term aortic complications in women
with Marfan syndrome
Class Ia
•Counsel about the risk of aortic dissection and the heritable nature of the
condition
•Strict blood pressure control
•Monthly/bimonthly echo measurements of the ascending aorta
Class IIa
•It is reasonable to replace the aortic root and ascending aorta if the
diameter >4.0 cm in Marfan syndrome
•Fetal delivery via cesarean section is reasonable for patients with
significant aortic enlargement, dissection, or severe aortic valve
regurgitation
Hiratzka L. J Am Coll Cardiol 2010

9/2/2015
11
Valvular Heart Disease
• Stenotic lesions are not well tolerated
• Mitral stenosis: ↑ heart rate and ↓ diastolic filling results
in ↑ LA pressure and pulmonary edema
• Management: maintain sinus rhythm, beta-blockers,
diuretics, invasive strategies only if severe compromise
• Prosthetic heart valves: specific challenges
No pregnancy in a woman with a mechanical valve is safe
•Warfarin is recommended for all pregnant patients with a mechanical valve
in the 2nd and 3rd trimesters
•Warfarin should be discontinued with initiation of UFH before a planned
vaginal delivery
•Low dose aspirin (75-100 mg/day) is recommended in the 2nd and 3rd
trimesters for pregnant women with both mechanical valve or bioprosthesis
•Continuation of warfarin during the 1st trimester of pregnancy is reasonable if
the dose is <5mg/day
Nishimura R. Circulation 2014
Class IA
Class IIA
Endocarditis in Pregnancy
• Rare, yet life-threatening
• High maternal mortality rate, between 11 and 33%
• Death due to emboli, heart failure
• Highest maternal mortality for aortic valves
• Rheumatic heart disease cases declining, IVDA cases
increasing
• High fetal mortality, between 15 and 33%
• Most common species: Streptococcus
Campuzano K Arch Gynecol Obstet 2003
Kebed Y Mayo Clinic Proc 2014

9/2/2015
12
Question 6A 43 yr old woman who is 30 weeks pregnant presents
with chest pressure and shortness of breath. She is a
smoker, and is on medical therapy for HTN and
diabetes. Her electrocardiogram is shown here:
A 43 yr old woman who is 30 weeks pregnant presents
with chest pressure and shortness of breath. She is a
smoker, and is on medical therapy for HTN and diabetes
What is your initial management?
A. (A) Serial troponins and observation
B. (B) Coronary angiography
C. (C) Thrombolysis D. (D) Cardiac MRI with
viability E. (E) Start aspirin and
deliver the baby (A
) Ser
ial t
roponin
s an
d obs.
..
(B) C
oronar
y an
giogr
aphy
(C) T
hrom
bolysis
(D) C
ardia
c M
RI with
via
bility
(E) S
tart
asp
irin a
nd deliv
er ...
0% 0% 0%0%0%
Acute Myocardial Infarction
• Acute MI in pregnancy in rare
• Must rule out coronary artery dissection
• Case fatality rate is between 5 and 37%
• Risk factors include:
- Hypertension - Diabetes
- Age > 30 yrs - Smoking
- Thrombophilia - Tranfusions
- Postpartum infection
• Occurrence up to 6 weeks postpartum
James A. Circulation 2006
Ladner H. Obstet Gynecol 2005

9/2/2015
13
Cardiopulmonary bypass during
Pregnancy
• Results in utero-placental hypoperfusion
• Maternal outcomes are similar to cardiac surgery in non-
pregnant women
• Poor fetal outcomes (up to 33% mortality): fetal mortality
improved if CPB is delayed
• Perfusion strategy to ensure adequate placental
homeostasis includes high-flow, high-pressure,
normothermia and brief CPB time
Kapoor MC. Ann of Cardiac Anesthesia 2014
John AS. et al. Ann Thorac Surg 2011
Resuscitation Guidelines:
Cardiac Arrest
• Place the patient in the full left-lateral position to relieve
possible compression of the inferior vena cava
• Give 100% oxygen
• Establish IV access above the diaphragm
• Assess for hypotension
• Consider & treat reversible causes
• Emergency cesarean section may be considered at 4
minutes after onset of maternal cardiac arrest if there is no
return of spontaneous circulation
(Class IIb, LOE C)
AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Vanden Hoek T. Circulation 2010
It’s Not Just the Mother…
• Adverse Obstetric Outcomes -Higher rates of premature rupture of membranes, post-
partum hemorrhage
• Adverse Neonatal Outcomes -Higher rates of preterm birth, small for gestational age
neonates, respiratory distress, intraventricular hemorrhage
and death
-Congenital heart disease in the offspring

9/2/2015
14
Summary• Physiologic changes are dramatic during pregnancy and
delivery
• Established maternal cardiac risk factors include:
-Prior event, poor functional capacity, cyanosis
-Elevated pulmonary vascular resistance, connective tissue
disorders
Mnemonic
15 (Aortic valve area < 1.5 cm2)
20 (Mitral valve area < 2.0 cm2)
30 (LVOT peak gradient > 30 mm Hg)
40 (Systemic ventricular EF < 40%)
• These risks extend into the postpartum period
• Women with cardiac events in pregnancy have a higher risk
of cardiac complications later in life
ReferencesHunter S, Robson, SC. Adaptation of the maternal heart in pregnancy. Br Heart J. 1992;68:540-543.
Brenner B. Haemostatic changes in pregnancy. Thrombosis Research 2004; 114: 409-414.
James AH. Pregnancy-associated thrombosis. Hematology AM Soc Hematol Educ Program. 2009; 277-285.
Kovacs A. et al. Pregnancy and contraception in congenital heart disease: what women are not told. J Am
Coll Cardiol 2008; 52(7):577-578.
Berg CJ et al. Overview of maternal morbidity during hospitalization for labor and delivery in the United
States: 1993-1997 and 2001-2005. Obstet Gynecol 2009; 113(5): 1075-1081.
Greutmann M. et al. The ROPAC registry: a multicentre collaboration on pregnancy outcomes in women with
heart disease. European Heart Journal 2012: doi:10.1093.
Siu S et al. Prospective multicenter study of pregnancy outcomes in women with heart disease. Circulation
2001; 104(5): 515-521.
References
Balint OH et al. Cardiac outcomes after pregnancy in women with congenital heart disease. Heart
2010;96(15):1223-1226.
Regitz-Zagrosek V. et al. ESC Guidelines on the management of cardiovascular diseases during pregnancy:
the Task Force on the Management of Cardiovascular Disease during Pregnancy of the European Society of
Cardiology. European Heart Journal 2011; 32(24): 3147-3197.
Demakis J, Rahmimtoola SH. Peripartum Cardiomyopathy. Circulation 1971; 44(5): 964-968.
Pearson, GD et al. Peripartum cardiomyopathy: National Heart Lung and Blood Institute and Office of Rare
Diseases (National Institutes of Health) workshop recommendations and review. JAMA 2000; 283(9): 1183-
1188.
Silwa K. et al. Peripartum cardiomyopathy. Lancet 2006; 368(9536): 687-693.
9/2/2015
15
ReferencesElkayam U. Clinical characteristics of peripartum cardiomyopathy in the United States: diagnosis, prognosis,
and management. J Am Coll Cardiol 2011; 58(7): 659-670
Elkayam U. et al. Pregnancy-associated cardiomyopathy: clinical characteristics and a comparison between
early and late presentation. Circulation 2005; 111(16): 2050-2055.
Homans D. et al. Peripartum cardiomyopathy. N Engl J Med 1985; 312(22): 1432-1437.
Fett J. et al. Five-year prospective study of the incidence and prognosis of peripartum cardiomyopathy at a
single institution. Mayo Clin Proc 2005; 80(12):1602-1606
Seely EW, Ecker J. Clinical practice: Chronic hypertension in pregnancy. N Engl J Med 2011; 365(17): 439-
446.
Powe CE et al. Preeclampsia, a disease of the maternal endothelium: the role of antiangiogenic factors and
implications for later cardiovascular disease. Circulation 2011. 123(24):2856-2869.
Hiratzka L. et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis
and management of patients with thoracic aortic disease. A Report of the American College of Cardiology
Foundation/American Heart Association Task Force on Practice Guidelines, American Association for
Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular
Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional
Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine. J Am Coll Cardiol
2010;55(14):e27-e129.
References
Nishimura R. et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A
Report of the American College of Cardiology/American Heart Association Task
Force on Practice Guidelines. Circulation. 2014 Jun 10;129(23):e521-643.
Campuzano K. Bacterial endocarditis complicating pregnancy: case report and systematic review of the
literature. Arch Gynecol Obstet. 2003 Oct;268(4):251-5.
Kebed Y. Pregnancy and Postpartum Infective Endocarditis: A Systemic Review. Mayo Clinic Proc. 2014:
89(8): 1143-1152.
James A. et al. Acute myocardial infarction in pregnancy: A United States population-based study. Circulation
2006; 113: 1564-1571.
Ladner HE. et al. Acute myocardial infarction in pregnancy and the puerperium: a population-based study.
Obstet Gynecol 2005;105(3):480-4.
Kapoor MC. et al. Cardiopulmonary Bypass in Pregnancy. Ann of Cardiac Anesthesia. 2014; 17:33-39.
John A. et al. Cardiopulmonary Bypass During Pregnancy. The Annals of Thoracic Surgery 2011; 91 (4):
1191-1196.
References
Vanden Hoek et al. Part 12: Cardiac Arrest in Special Situations: 2010 American Heart Association Guidelines
for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010; 122(suppl
3):S829-S861.
*Donnelly et al. The immediate and long-term impact of pregnancy on aortic growth rate and mortality in
women with Marfan syndrome. J Am Coll Cardiol 2012;60:224-229.
*Hilfinker-Kleiner D et al. A cathepsin D-cleaved 16 kDa form of prolactin mediates postpartum
cardiomyopathy. Cell 2007;128(3): 589-600.
*Stergiopoulos K et al. Pregnancy in patients with pre-existing cardiomyopathies. J Am Coll Cardiol 2011;
58(4):337-350.
*Khairy P et al. Pregnancy outcomes in women with congenital heart disease. Circulation 2006; 113 (4):517-
524.
*Roos-Heselink JW et al. Outcome of pregnancy in patients with structural or ischaemicheart disease : Result
of a registry of the European Society of Cardiology. Eur Heart J. epub 2012.
*Denotes articles not included in presentation, but contains helpful information.