pregnancy after perinatal loss: the relationship between anxiety and prenatal attachment
TRANSCRIPT
JOGNN CLINICAL STUDIES
Pregnancy After Perinatal Loss: The Relationship Between Anxiety and -
Prenatal Attdchrnent Deborah Armstrong, R N, M S N , Marianne Hutti, WHNP-C, DNS
= Objective: To determine the difference be- tween levels of pregnancy-specific anxiety and pre- natal attachment in a group of pregnant women who previously had a late pregnancy loss and a group of primiparous women of similar gestational age. To also determine the relationship, i f any, between anx- iety and prenatal attachment in both groups.
Design: A nonrandom, comparative descrip- tive design.
Setting: Participants recruited from medical of- fices, childbirth classes, and perinatal support groups and newsletters.
Participants: A convenience sample of 31 ex- pectant mothers (1 5 primiparae and 16 who previ- ously experienced a late pregnancy miscarriage, still- birth, or neonatal death). Both groups of women were in the 2nd or 3rd trimester of their current pregnancy.
Main Outcome Measures: Anxiety was mea- sured using the Pregnancy Outcome Questionnaire; prenatal attachment was measured using the Prena- tal Attachment Inventory.
Results: The loss group showed significantly greater levels of anxiety and significantly lower levels of prenatal attachment compared with a group of pri- miparous women of a similar gestational age.
Conclusions: Women who experienced a pre- vious late pregnancy loss had a higher level of anxiety related to concerns about the pregnancy and decreased prenatal attachment with the child in the current preg- nancy. Women in their first pregnancy had decreased anxiety compared with the loss group. Higher levels of prenatal attachment also were shown in the primipa- rous group. JOGNN, 27, 183-1 89; 1998.
Accepted: April 1997
Perinatal loss continues to be a complicated, shat- tering experience in the lives of parents and families at a time when the happiness of a new birth is an- ticipated. Some researchers estimate the incidence of early miscarriage (before 20 weeks gestation) to be 10-20 miscarriages per 100 pregnancies, and of late pregnancy loss to be 2 per 100 pregnancies (Woods & Esposito, 1987).
Past clinical studies focused on grief re- sponses after perinatal loss and interventions to fa- cilitate adaptation for the parents a t the time of the loss (Hutti, 1988; Kirkley-Best & Kellner, 1982; Leon, 1986). However, that research did not focus on the effects of grieving on the mother during a subsequent pregnancy or on the relationship of anxiety to concerns about the current pregnancy and prenatal attachment with the fetus.
Many studies support the theory that the at- tachment process between mother and fetus begins well before birth (Cranley, 1981; Muller, 1993; Rubin, 1977). Attachment theories state that the affectional tie between a mother and her infant is essential for enhancing the child’s early survival and later capacity for getting along with others (Bowlby, 1969).
With perinatal loss, parents may grieve for many years. When these couples become pregnant again, they may continue mourning their lost child while simultaneously attempting to develop bonds of attachment with their new unborn infant. Some mothers, to protect themselves from future painful involvements, hold back from making an emo- tional investment with the new child. The loss of an infant is such 3 traumatic experience for most women that it can produce severe anxiety when another pregnancy is contemplated. Davis, Stew-
MarchlApril 1998 JOGNN 283
art, ;ind Harmon ( 1989) determined that mothers felt more ii 11 xi o LI s d ~i r i n g a s u hseq ti en t pregnancy than d u r - ing an!. pregnancy before their perinatnl loss. I n a study by (:ovington nnd Tlieut ( I W 3 ) , some women stated that even though they understood tlie cause of tlie loss, this k n ()wl ed gc did not co m p I e te I y ease the i I- an s i e t y .
Tlieut, I'ederson, Zaslow, ~ i n d Rahinovich ( 19S8) compared 2.5 expectant couples who experienced a pre- vious pregnancy loss with 3 1 first-time expectant couples to determine whether the level of pregn"ncy-specific anx- iety was greater i n couples who had experienced the loss than i n those who had not. The results of their study indicated increased maternal anxiety in a pregnancy af- ter a perinatal loss. I t is important to assess the relation- ship between anxiety kind prenatal attachment in a preg- nancy subsequent to 11 perinntal loss if increased anxiety can lead to decreased attachment.
N u r s e s must be aware of the difficult
emotions that can accompany grief after a
perinatal loss. The anxiety mothers often
experience during a subsequent pregnancy may
be overwhelming.
Nurses must be aware of the difficult eniotions that can accompany grief after a perinatal loss. The unique and increased anxiety mothers often experi- ence during a subsequent pregnancy may be over- whelming. If this heightened anxiety can interfere with prenatal attachment in a subsequent pregnancy, it is important for health care providers to assess the cli- ent's obstetric history to provide support, assess the impact of increased anxiety, and give reassurance about tlie development o f this vital relationship be- tween mother and her new infant.
The purpose of the current study was to examine the relationship between anxiety-related concerns about the pregnancy and the development of prenatal attach- ment. Differences were explored i n levels of pregnancy- specific anxiety of a group of expectant mothers during their 2nd or 3rd trimester who had experienced a pre- vious loss compared with a group of first-time expectant mothers of similar gestational age. We sought to deter- mine whether anxiety related to concerns about the preg- nancy was greater during a pregnancy subsequent to a perinatal loss and whether there were differences in lev- els o f prenatal attachment betwecn tlie two study groups.
The relationship between heightened anxiety, if present, and the development of p renn t a I R t tach men t he t wee n the expectant mother and her new intant also ivere ex3 i n ined .
Literature Review
Bowlby ( 1969) stated that during the course of healthy development, attnchnient behaviors lead to the development of affectional bonds. Ruhin ( 1977) pro- posed that the affectional tie between a mother and child that is obvious at birth is developed and structured diir- ing pregnancy. She contended that the intt'rriction oh- served in the early days and months ot an infunt's life is a consequence of prebirth experiences. These experi- ences prompt the mother to develop an emotional tie to her infant.
Per in a ta I I oss i nc I LI des i n i scn r r i a gc ( ea r I y or I ate ) , stillbirth, or neonatal death within the first 28 days of life. The lack of concrete evidence of the pregnancy or the child's existence after a perinatal loss may make it difficult for the parents to mourn their loss. Parents mourn not only the death of their infant, but part of their own mortality and dreams and hopes for the future re- lated to the child (Harrigan, Naber, Jensen, Tse, & Perez, 1993).
Davis et al. (1989), in a study of 24 mothers ex- periencing a subsequent pregnancy after a periiiatal loss, found that 23 of 24 mothers felt more anxious during the pregnancy subsequent to the loss than during any previous pregnancy before the loss. This anxiety was experienced regardless of how soon the pregnancy oc- curred after the loss and may be specific rather than generalized. Gaffney ( 1986) showed significant inverse correlations between state (temporary) anxiety and tlie overall Maternal-Fetal Attachment Scale (Cranley, 198 1 ). However, whereas some studies showed an inverse corre- lation between anxiety and attachment (Avant, 1980; Blumberg, 1980; Gaffney, 1986), othei- researchers pro- posed that increased prenatal anxiety indicates that the mother is developing an emotional relationship with her unborn child (Brazelton & Keefer, 1982; Leifer, 1977).
The results of a study by Theut et al. (1988) indi- cated increased anxiety related to their pregnancy in mothers who experienced a previous pregnancy loss. Us- ing a tool developed to contrast specific pregnancy- related anxiety (Pregnancy Outcome Questionnaire) with generalized measures of anxiety and depression, this research showed that for their sample, perinatal loss was associated with specific rather than generalized anx- iety during a subsequent pregnancy. Theut et al. (1988) theorized that "anxiety and depression of sufficient se- verity can interfere with tlie parents' ability to ~ O C L I S on the process of the new pregnancy, the developing fetus,
283 JOGNN Volirriie 27, Niniiher 2
J t i d t ti e ps y c hol og ica I process i ti vo I ved i n attach me tit ” (p . 289).
Methods The convenience sample of 3 1 expectant mothers
was recruited to participate in the current study through private medic a 1 practices, chi Id b i r t h c 1 asses, and perinatal support groups such as SHARE; and support group newsletters such a s Helping Hands, the Counselor Connection, ii n d SHARE’S newsletter . The study population was difficult to locate because the women were required to have experienced a previous loss late in pregnancy and be i n the second half of a s 11 b seq i i e n t pregnancy . In i t i a I attempts to 1 oca te s t i i d y g r o 11 p pa r t i c i pants with i n medic a I practices an d c I i n ics were not successful because of a lack of referrals. However, as volunteers were recruited through peri- natal support groups and their newsletters, referrals were obtained. All control group participants were re- ferred by medical offices and clinics, but only one s t LI d y gro u p pa r t i c i pa n t w a s r ec r 11 i te d from this so II rce .
Sixteen participants had experienced miscarriage in the 2nd trimester, stillbirth, or early neonatal death during a previous pregnancy. The other 15 mothers comprised a comparison group experiencing their first pregnancy of a similar gestational age. Both groups were i n the 2nd or 3rd trimester of their current pregnancy.
Both groups of women received a full description of the research study and its purpose. All participants signed consent forms before the study began. Question- naires were mailed to participants after they received a complete description of the study in person or by tele- phone. Each participant completed a demographic ques- tionnaire, Prenatal Attachment Inventory (Muller, 1993), and the Pregnancy Outcome Questionnaire (Theut et al., 1988).
Muller ( 1993) developed the Prenatal Attachment Inventory (PAI) based on Bowlby’s (1 969) theory of at- tachment. The PA1 is a 21-item instrument; responses are made on a four-point Likert-type scale and range from “almost always” to “almost never.” Evidence of reli- ability was obtained using Cronbach’s alpha coefficient of internal consistency. Cronbach’s alpha for the PA1 scale for this study was .93. Muller tested the validity of the PA1 during its development by comparing items on this scale with items on the Maternal-Fetal Attachment Scale (Cranley, 1981).
The Pregnancy Outcome Questionnaire (POQ) (Theut et a l . , 1988) was developed to examine pregnancy-specific anxiety. The items of the POQ were derived from interviews with parents who had expe- rienced a perinatal loss and were based on the areas of
concern they expressed. According to the authors, each item is intended to apply to first-time expectant parents and those who had a previous pregnancy. The POQ consists of 15 items with responses scored on a four-point Likert scale ranging from “almost all the time” to “almost never.” The alpha coefficients for the POQ were .80 for the mothers and .80 for the fathers, indicating acceptable internal consistency. Cronbach’s alpha for the mothers in both groups for this study was .89. Measurenients of validity were not reported for the POQ. Sample items for both questionnaires are shown in Table 1.
Means were compared to determine whether there was a significant difference related to anxiety and prenatal attachment between the previous peri- natal loss group and the first-time mothers. The Kruskal-Wallis test (equivalent to chi square) was used to evaluate differences between groups for anxiety and attachment. This nonparametric test was chosen be- cause the distribution of data was nonnornial. Spear- man Rho correlations were then performed to deter- mine the relationship between the levels of anxiety and prenatal attachment for the two groups and the rela- tionship, if any, between anxiety and attachment for both groups.
Results Both groups consisted of mothers currently preg-
nant in their 2nd or 3rd trimester. The mean age of all subjects was 29 years, and their mean educational level was 15 years. Sixty-eight percent of the subjects were employed and worked an average of 33 hours per week. Income levels for 66% of the subjects in both groups was $45,000 or greater. All but one of the participants were married, and 68% of the women in both groups planned their current pregnancy (see Table 2 for a more detailed description of how the two groups differed in relation to demographic data).
Results of the Kruskal-Wallis test for anxiety be- tween the groups showed significant differences between groups on the POQ for anxiety a t the .01 level. The Krus- kal-Wallis test measures of significance on the PA1 dif- fered significantly in attachment between the groups ( p = .0482). More information on means and value ranges for both groups is provided in Table 3.
In addition, correlations between the two groups for the relationship between heightened anxiety and prenatal attachment indicated that prenatal attach- ment, although not statistically significant, was de- creased when anxiety was increased in the previous loss group. Although significant correlations could not be demonstrated for the primiparous group of women, when anxiety levels increased, prenatal attachment also increased (see Table 4).
MarchlApril 1998 JOG” 185

TABLE 1 Sample Itenis Froin the Pregnancy Attachment Invent0 y and the Pregnancy Oiitconie Questionnaire
Sample Items From the Prenatal Attachment Inventory“ I imagine calling the baby by name. I think that my baby already has a personality. I imagine what part of the baby I’m touching. I feel love for the baby. I know the baby hears me.
Sample Items From the Pregnancy Outcome Questionnaire
I feel confident that my pregnancy will proceed without any special problems. I worry about whether my nervousness over this pregnancy will have some effect on the outcome. I feel worried about the health of my new baby. I have hesitated to tell others about my pregnancy. I feel overwhelmed because of the anxieties related to this pregnancy.
a Responses are made on a Likert-type scale with choices ranging from “almost always” to “almost never.”
Responses are made on a Likert-type scale with choices ranging from “almost all the time” to “almost never.” Note. From “Development of the Prenatal Attachment Inventory,” by M. Muller, 1993, Western]ournal of Nursing Research 15 ( 2 ) . Adapted with permission of the author; and from “Pregnancy Sub- sequent to Perinatal Loss: Parental Anxiety and Depression,” by s. Theut, F. Pederson, M. Zaslow, and B. Rabinovich, 1988, Journal of the American Academy of Child and Adolescent Psychiatry, 27. Adapted with permission of the author.
Discussion
The results of this study show an increase in preg- nancy-specific anxiety as measured by the POQ (Theut et al., 1988) in a group of upper middle class, highly educated, married women who had experienced a peri- natal loss in a previous pregnancy. The loss group also demonstrated significantly less prenatal attachment, which can be a difficult developmental task for these mothers to achieve. In conversations and letters returned with some of the questionnaires sharing stories of their losses, the women expressed differences in attitudes to- ward the children they were carrying. Some mothers ex- pressed feelings of great awareness of their unborn child’s activities and seemed to actively seek opportuni- ties to create memories of this child. Other mothers ex- pressed the desire to distance themselves and not become too closely involved with their unborn child. Women who had experienced a previous loss expressed the feel- ing that this pregnancy was unlike any before the loss. “Although I am thrilled about this pregnancy, the stress
and anxiety can be overwhelming. So few understand the anxiety after loss,” one mother wrote.
W o r n e n who had experienced a previous
loss expressed the feeling that their subsequent
pregnancy was unlike any before the loss.
Although the loss group showed decreased attach- ment and increased levels of anxiety, the correlation be- tween these two variables was not significant. These find- ings represent an intriguing trend. Lack of significance may be due to the small sample size, or there may be n o relation between anxiety and attachment.
Currently, no generalizations can be made about a relationship between anxiety and attachment. However, further study of this relationship is warranted, with larger, more diverse populations to examine the possible relationships between heightened pregnancy-related anxiety and prenatal attachment. Other studies have in- dicated that anxiety in general can interfere with a
TABLE 2 Deniogrrzphic Data for Both Grotips
Group 1 (Previous Loss)” Mean age = 31.5 years Mean years of education = 15.69 Employment: 56.3% employed; 43.8% not employed Mean hours worked per week if employed, 33.3 hours Income: $25,000 to $45,000 = 20%; >$45,000 = 80% Planned pregnancy: yes = 87.5%; no = 12.5%
Group 2 (First Pregnancy)b Mean age = 26 years Mean years of education = 14.67 Employment: 80% employed; 20% not employed Mean hours worked per week if employed, 33.92 hours Income: <$25,000 = 7.1%; $25,000 to $45,000 =
Planned pregnancy: yes = 46.7%; no = 53.3% 42.9%; >$45,000 = 50%
All participants in this group were married. All but one of the participants in this group were married.
186 JOGNN Volttine 27, Number 2
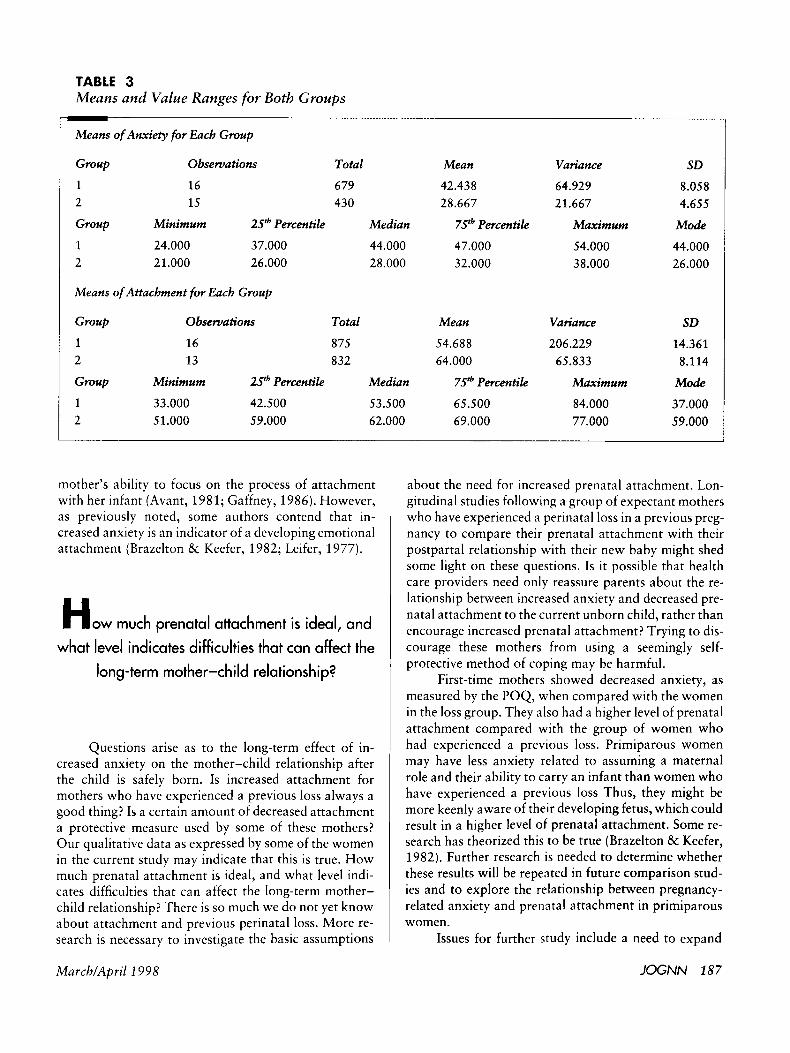
TABLE 3 Means and Value Ranges for Both Groups
MarchlApril 1998
Mean
42.438 28.667
7 . P Percentile
47.000 32.000
Mean
54.688 64.000
7.P Percentile
65.500 69.000
Variance
64.929 21.667
Maximum
54.000 38.000
Variance
206.229 65.833
Maximum
84.000 77.000
SD
8.058 4.655
Mode
44.000 26.000
SD
14.361 8.114
Mode
37.000 59.000
about the need for increased prenatal attachment. Lon- gitudinal studies following a group of expectant mothers who have experienced a perinatal loss in a previous preg- nancy to compare their prenatal attachment with their postpartal relationship with their new baby might shed some light on these questions. Is it possible that health care providers need only reassure parents about the re- lationship between increased anxiety and decreased pre- natal attachment to the current unborn child, rather than encourage increased prenatal attachment? Trying to dis- courage these mothers from using a seemingly self- protective method of coping may be harmful.
First-time mothers showed decreased anxiety, as measured by the POQ, when compared with the women in the loss group. They also had a higher level of prenatal attachment compared with the group of women who had experienced a previous loss. Primiparous women may have less anxiety related to assuming a maternal role and their ability to carry an infant than women who have experienced a previous loss Thus, they might be more keenly aware of their developing fetus, which could result in a higher level of prenatal attachment. Some re- search has theorized this to be true (Brazelton & Keefer, 1982). Further research is needed to determine whether these results will be repeated in future comparison stud- ies and to explore the relationship between pregnancy- related anxiety and prenatal attachment in primiparous women.
Issues for further study include a need to expand
JOG" 187
Means o f Anxieiy for Each Group
Group Observations Total
1 16 679 2 15 430
Group Minimum 2.5" Percentile Median
1 24.000 37.000 44.000 2 21.000 26.000 28.000
Means of Attachment for Each Group
Group Observations Total
1 16 8 75 2 13 832
Group Minimum 2.P Percentile Median
1 33.000 42.500 53.500 2 51.000 59.000 62.000
mother's ability to focus on the process of attachment with her infant (Avant, 1981; Gaffney, 1986). However, as previously noted, some authors contend that in- creased anxiety is an indicator of a developing emotional attachment (Brazelton & Keefer, 1982; Leifer, 1977).
H o w much prenatal attachment is ideal, and
what level indicates difficulties that can affect the
long-term mother-child relationship?
Questions arise as to the long-term effect of in- creased anxiety on the mother-child relationship after the child is safely born. Is increased attachment for mothers who have experienced a previous loss always a good thing? Is a certain amount of decreased attachment a protective measure used by some of these mothers? Our qualitative data as expressed by some of the women in the current study may indicate that this is true. How much prenatal attachment is ideal, and what level indi- cates difficulties that can affect the long-term mother- child relationship? There is so much we do not yet know about attachment and previous perinatal loss. More re- search is necessary to investigate the basic assumptions
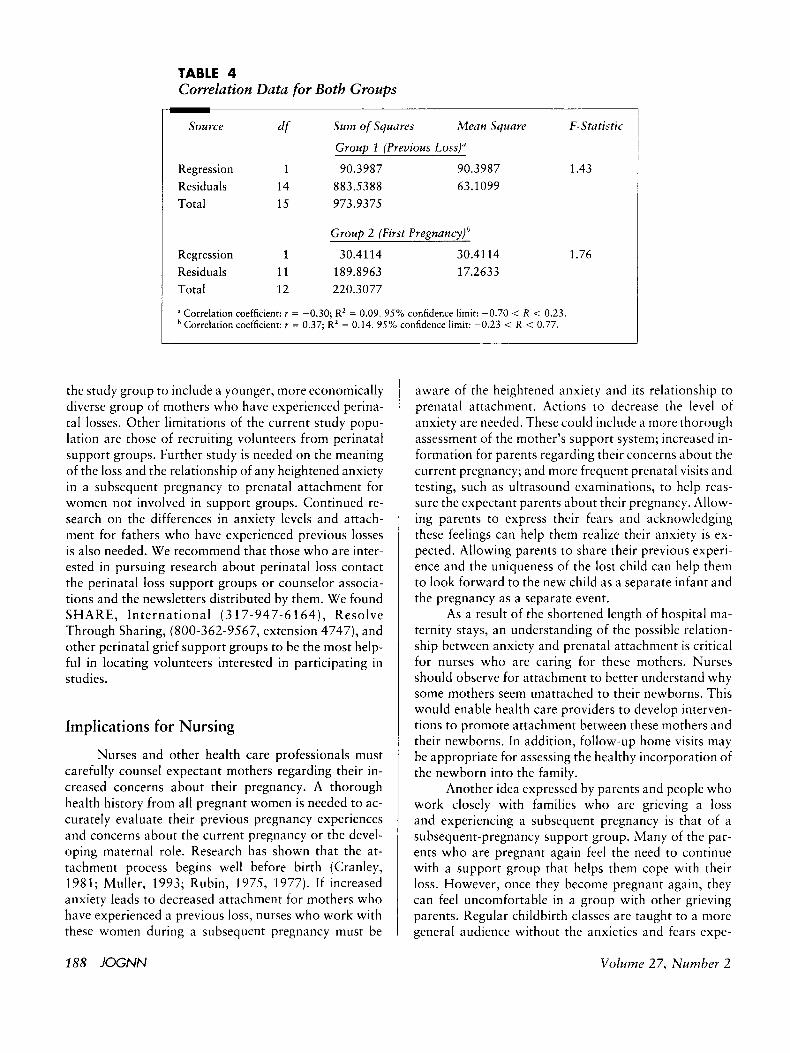
TABLE 4 Correlation Data for Both Groups
Sou rce df SMill of Squares Mean Sqtiare F-Statistic
Group 1 (Previous Loss)"
Regression 1 90.3987 90.3987 1.43 Residuals 14 883.5388 63.1099 Total 15 973.9375
Group 2 (First Pregnancy)"
Regression 1 30.4114 30.41 14 1.76 Residuals 11 189.8963 17.2633 Total 12 220.3077
Correlation coefficient: r = -0.30; R' = 0.09. 95% confidence limit: -0.70 < R < 0.23. Correlation coefficient: r = 0.37; R' = 0.14. 95% confidence limit: -0.23 < R < 0.77.
the study group to include a younger, more economically diverse group of mothers who have experienced perina- tal losses. Other limitations of the current study popu- lation are those of recruiting volunteers from perinatal support groups. Further study is needed on the meaning of the loss and the relationship of any heightened anxiety in a subsequent pregnancy to prenatal attachment for women not involved in support groups. Continued re- search on the differences in anxiety levels and attach- ment for fathers who have experienced previous losses is also needed. We recommend that those who are inter- ested in pursuing research about perinatal loss contact the perinatal loss support groups or counselor associa- tions and the newsletters distributed by them. We found SHARE, Internat ional ( 3 17-947-6 164) , Resolve Through Sharing, (800-362-9567, extension 4747), and other perinatal grief support groups to be the most help- ful in locating volunteers interested in participating in studies.
Implications for Nursing
Nurses and other health care professionals must carefully counsel expectant mothers regarding their in- creased concerns about their pregnancy. A thorough health history from all pregnant women is needed to ac- curately evaluate their previous pregnancy experiences and concerns about the current pregnancy or the devel- oping maternal role. Research has shown that the at- tachment process begins well before birth (Cranley, 1981; Muller, 1993; Rubin, 1975, 1977). If increased anxiety leads to decreased attachment for mothers who have experienced a previous loss, nurses who work with these women during a subsequent pregnancy must be
aware of the heightened anxiety and its relationship to prenatal attachment. Actions to decrease the level of anxiety are needed. These could include a more thorough assessment of the mother's support system; increased in- formation for parents regarding their concerns about the current pregnancy; and more frequent prenatal visits and testing, such as ultrasound examinations, to help reas- sure the expectant parents about their pregnancy. Allow- ing parents to express their fears and acknowledging these feelings can help them realize their anxiety is ex- pected. Allowing parents to share their previous experi- ence and the uniqueness of the lost child can help them to look forward to the new child as a separate infant and the pregnancy as a separate event.
As a result of the shortened length of hospital ma- ternity stays, an understanding of the possible relation- ship between anxiety and prenatal attachment is critical for nurses who are caring for these mothers. Nurses should observe for attachment to better understand why some mothers seem unattached to their newborns. This would enable health care providers to develop interven- tions to promote attachment between these mothers and their newborns. In addition, follow-up home visits may be appropriate for assessing the healthy incorporation of the newborn into the family.
Another idea expressed by parents and people who work closely with families who are grieving a loss and experiencing a subsequent pregnancy is that of a subsequent-pregnancy support group. Many of the par- ents who are pregnant again feel the need to continue with a support group that helps them cope with their loss. However, once they become pregnant again, they can feel uncomfortable in a group with other grieving parents. Regular childbirth classes are taught to a more general audience without the anxieties and fears expe-
188 JOG" Volume 27, Number 2

I-ienced by parents who have had a perinatal loss. T h e need exists for a suppor t g r o u p of parents who a r e ex- periencing the same difficulties of mourning their lost child while dealing with the anxieties a n d hopes t h a t the new pregnancy brings. Some special “subsequent preg- nancy after loss” suppor t g roups a re being s tar ted t o a n - swer this need. By expanding such groups, nurses could assist these parents in dealing with their anxieties a n d promote the vital developing relationship between par- ents a n d their newborn.
REFERENCES
Avant, K. ( 1 98 1 ). Anxiety as a potential factor affecting ma- ternid attachment. Jotrrnol of Obstetric., Gynecologic-, L i d NeoniltL71 Nirrsing, 10 . 416-419.
Bocvlby, J . ( 1969). At t~ ichnz~nt aiid loss, idirnze I : AttLichnzent, New York: Basic Books.
Blumberg, N. L. (1980). Effects of neonatal risk, maternal at- titude, and cognitive style on early postpartum adjust- ment. Joirrnal of Almortnal Psychology, 6’9, 139- 1 50.
Brazelton, T. B., & Keefer, C. H. (1982). The early-mother child relationship: A developmental view of woman as mother. In M. Notham & C. Nadelson (Eds.), The 1~~on1411 pLitient: Concepts of femininity and the life cycle (pp. 95-109). New York: Plenum Press.
Covington, S., tl: Theut, S. (1993). Reactions to perinatal loss: A qualitative analysis of the national maternal and infant health survey. American Jotrrnal of Orthopsychiatry,
Cranky, M. (1981). Development of a tool for the measure- ment of maternal attachment during pregnancy, Nursing Research, .30(5), 28 1-284.
Davis, D., Stewart, M., tl: Harmon, R. (1989). Postponing pregnancy after perinatal death: Perspectives on doctor advice. Joirrnal of Anzerican Academy of Child 6 Ado- lesrent Psyclii~ztry, 28, 481-487.
Gaffney, K. ( 1986). Maternal-fetal attachment in relation to
63(2) , 215-222.
self-concept and anxiety. M ~ z t ~ , ~ ~ z ~ i l - C l i i l ~ 1 Nursing Jcnrr-
Harrigan, B., Naber, M., Jensen, K., Tse, A,, & Perez, D. ( 1993 j. Perinatal grief: Response to the loss of an infant.
Hutti, M. ( 1988). Perinatal loss: Assisting parents to cope.
Kirkley-Best, E., & Kellner, K. (1982). The forgotten grief: A review of the psychology o f stillbirth. A ~ n i ~ r i ~ m / o ~ f r n d i of Orthopsychiatry, 5 2 ( 3 ) , 420-429.
Leifer, M. ( 1977). Psychological changes accompanying prcg- nancy and motherhood. Gcnctir Psyshology Mono- gr~ipbs , 95, 55-96.
Leon, I.G. ( 1986). Psychodynamics of perinatal loss. Psycbia- try, 49, 3 12-324.
Muller, M. (1993). Development of the prenatal attachment inventory. Western Joi.rrnd of Nursing ReseLzrch, 1.7(2),
Rubin, R. (1975). Maternal tasks of pregnancy. Materrzai- Child Nursing Journal, 4, 143-153.
Rubin, R. (1977). Binding-in in the postpartum period. M~rternal-Child Nursing Josrrizal, 6 , 67-75.
Theut, S., Pederson, F., Zaslow, M., 81 Rabinovich, B. (1988). Pregnancy subsequent to perinatal loss: Parental anxiety and depression. ]oiirn~7/ of the Anierzcan Accrderriy of Child and Adolescent Psychiatry, 2 7 ( 3 j , 289-292.
Woods, J., 81 Esposito, J. (1987). Pregnancy loss: Medical ther- apeutics rind practical considerations. Baltimore: Wil- liams & Wilkins.
nal, I5(2) , 9 1 - 10 1.
NEOllcitrll NCtiLjOrk. 12 (5 ) , 2.5-3 I .
]OlfI’lZi7/ of EilZc>rgejzc.)f NItrSifzg, 14(6), 338-34 1 .
199-215.
Deborah Smith Armstrong is a doctoral student in the College of Nursing a t the Universiiy o f Kentucky, Lexington.
Marianne Hopkins Hutti is a professor and coordinator, Women’s Health Nurse Practitioner Program, University of Louisville School of Nursing, and a women’s health nurse practitioner with Partners in Women’s Health, Louisville, KY.
Address for correspondence: Deborah S . Armstrong, RN, MSN, 6902 Watford Court, Louisville, KY 40222.
MarchlApril 1998 JOG“ 189